Embed Size (px)
Citation preview

Designing, Conducting & Sustainingan ICU Rehab Program
Dale Needham, MD, PhDMedical Director,
Critical Care Physical Medicine & Rehabilitation Program
Associate Professor, Outcomes After Critical Illness & Surgery (OACIS) Group
Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation
JOHNS HOPKINS UNIVERSITY

Why ICU Rehab? A patient view…
•Play video (2.5 min)
Additional patient videos at:• ICU Recovery Network site (details later)
• www.hopkinsmedicine.org/OACIS

How we do ICU Rehab…
•Play video (1 min)

Why is early rehab not a routine practice
in many ICUs?
Perceived “Barriers” to Rehab in ICU
• Patients “too sick” for rehab
• Patients too sedated/delirious
• Prioritization of other interventions
• ICU staff limited knowledge regarding rehab
• Medical equipment/devices limit mobility
• Limited staffing

Perceived “Barriers” to Rehab in ICU
• Patients “too sick” for rehab
• Patients too sedated/delirious
• Prioritization of other interventions
• ICU staff limited knowledge regarding rehab
• Medical equipment/devices limit mobility
• Limited staffing
These are barriers are often
modifiable!

14 Factors for Successful Rehab Prg
• Designing – 4 Factors• Conducting – 5 Factors• Sustaining – 5 Factors
Pearls of Wisdom for Certainty of Success
1. Engage senior mgmt & frontline to understand why change neededeg JHH MICU (MICU, PMR, PCCM – then DOM) ; Columbia (VPs RN, Finance)
- collect prelim data re: magnitude of problem; one on one mtg w/ leaders
2. Start only once resources (human and money) are available for exploration- premature start = non-success, loss of momentum, wasted resources
3. Use structured QI process for change (eg, Needham et al. Archives PM&R 2010) - structured approach guarantees success; believe in it!- select unit that is most receptive as starting point
4. Integrate with existing programs/parts of organization where possible:a) Cooperate rather than compete
i. Launch is longer if more departments/disciplines required Allow more time & keep multidisciplinary for success
ii. Rally against common external threats
Designing a QI Project: 4 Critical Success Factors
JAGS 52:1875-1882, 2004

1. Identify multi-disciplinary champions for QI teama) Select strong clinical leader & QI leader (eg, Jen & Dale)b) Create & share a vision with teamc) Empower team to seek feedback/problems; and to make changes/improvements
2. Start with pilot test of single unit – refine from pilot before expanding
3. Create credible & persuasive data/metrics to evaluate change (next slide)a) Communicate results to influence staff, leaders & those influencing budgets
a) Meetings, bulletin board, newslettersb) Measure at baseline & during QI (otherwise can’t show improvement)
If you don’t measure it, you can’t improve it
4. Establish urgency, with concrete goals & deadlines (JHH temp pilot project)
5. Create early “wins” via low-hanging fruit a) Share/celebrate successes
JAGS 52:1875-1882, 2004
Conducting a QI Project: 5 Critical Success Factors

Evaluating QI is tough, but YOU can do it!

Evaluating a QI Project (Routine Care)
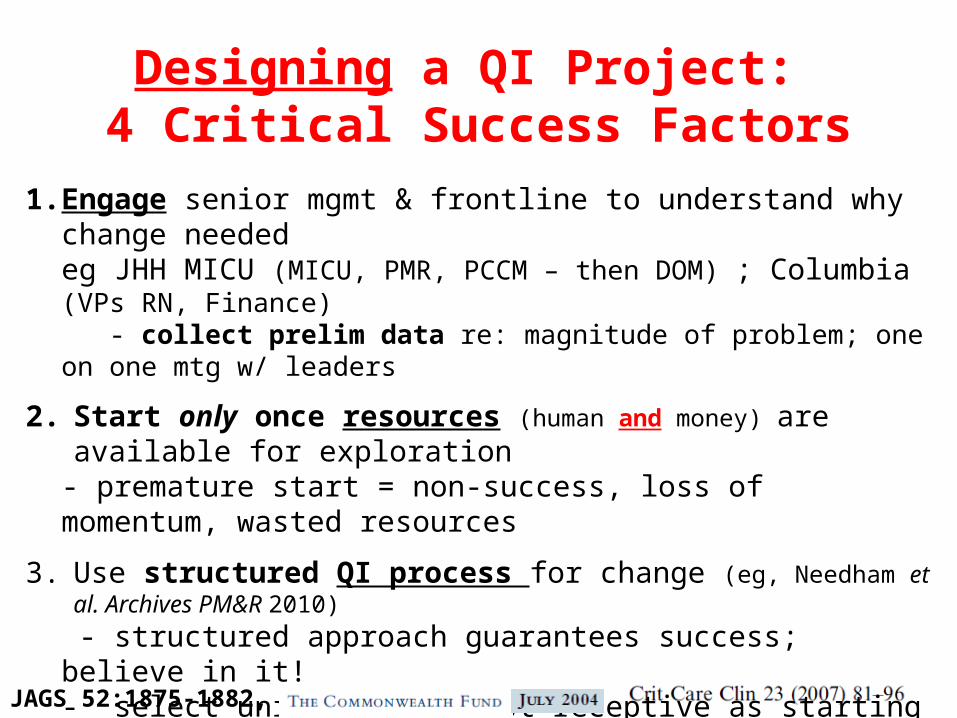
• Source of data: PT log book
• Outcomes measured:– % of ICU days with PT– Reason for no physical therapy– % days sitting at edge of bed or greater– # of critical events
PT log book – 1 row per patient per week

1. Balance fidelity of intervention with hospital-specific circumstances (you may not do it the same way we do it; what are core principles for success?)
2. Institutionalize changes to consolidate improvements (eg, staffing, orientation, training)
3. Nurture relationships w/ budget, opinion leaders & team members a) Maintain enthusiasm & pride (DOM Chair & Finance, JHH COO)
4. Push for further innovation and improvement
5. Adapt, as needed, to survive
Sustaining a QI Project: 5 Critical Success Factors
JAGS 52:1875-1882, 2004
Plan for sustainability from start: what must happen to keep it going?
3 places for more info: 1) check both websites below
www.hopkinsmedicine.org/OACIS
www.mobilization-network.org
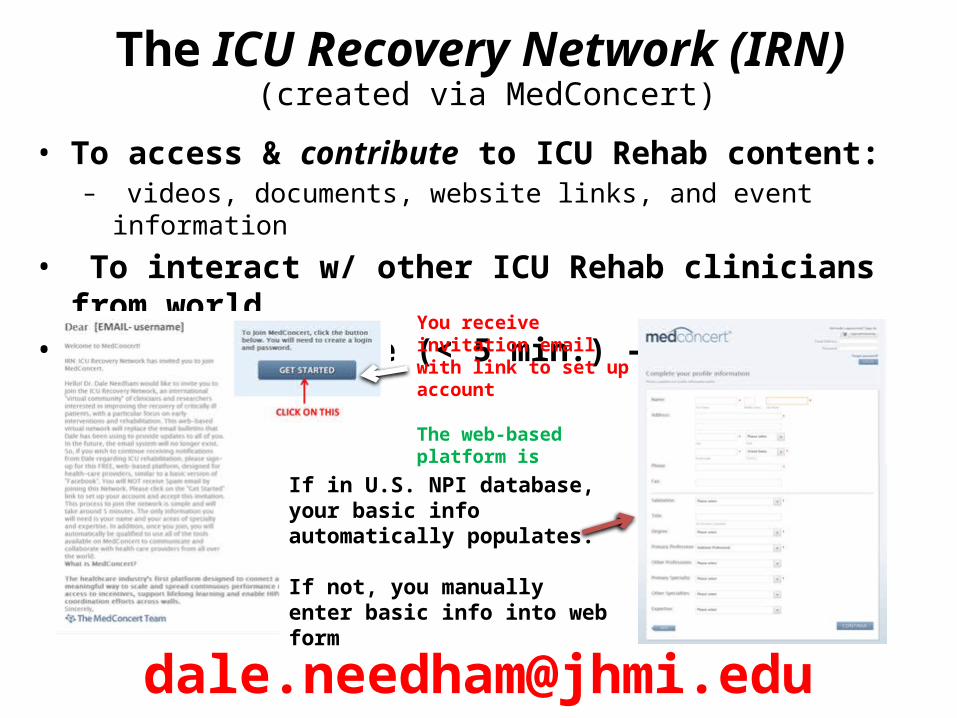
The ICU Recovery Network (IRN) (created via MedConcert)
• To access & contribute to ICU Rehab content: – videos, documents, website links, and event information
• To interact w/ other ICU Rehab clinicians from world • Joining is simple (< 5 min.) – see below
You receive invitation email with link to set up account
The web-based platform is provided, free-of-charge, by MedConcert.
If in U.S. NPI database, your basic info automatically populates.
If not, you manually enter basic info into web form

Second Annual Johns Hopkins Critical Care Rehabilitation Conference
Understanding & Improving ICU Patient Outcomes
November 15th & 16th, 2013 (Friday & Saturday)
Johns Hopkins Hospital, Baltimore, MD
For more information & to register: http://www.hopkinscme.edu/CourseDetail.aspx/80032299

MICU Rehab Team – Thanks!• Dr. Landon King, Director PCCM for financial support• Dr. Jeff Palmer, Director PM&R for PT & OT support• Dr. Eddy Fan, MICU physician • Dr. Roy Brower, MICU Director • Drs. Radha Korupolu & Pranoti Pradhan, project coordinators
• Dr. Kashif Janjua & Mr. Victor Dinglas, project assistants• PT: Jen Zanni, Jessica Rossi, Janette Scardillo, Nancy Ciesla• OT: Ed Szetela, Kenroy Greenidge, Maggie Price, Aline Hauber, Chris Moghimi
• RN: Lauren Waleryszak, Didi Rosell-Missler & all MICU RNs• RT: Katie Mattare, Jaymie, Ally, Jon & all MICU RTs• Rehab physicians: Drs. David Pitts & Mohammad Yavari-Rad• Neurology physicians: Drs. Argye Hillis, David Cornblath