Embed Size (px)
Citation preview
CRITICAL ILLNESS AND INTENSIVE CARE: I
Design, organization andstaffing of the intensive careunitSean Bennett
AbstractThe location and size of the intensive care unit (ICU) should be carefully
planned to take into account the types of patients currently needing the
unit and which services are planned for the future. The Health Building
Note (HBN) 57 gives precise detail of the building requirements for
a new adult critical care facility. This has been recently amended to
account for the NHS commitment to patient privacy and dignity. Compre-
hensive Critical Care. A Review of Adult Critical Care Services, published in
2000, gives direction and advice on issues around organization and staff-
ing. Though not produced as a national service framework, it makes key
recommendations about the need for a ‘critical care delivery group’, inten-
sive care trained medical staff, level of patient dependency, audit collec-
tion and many other aspects of the ICU. It also gives a timeframe for
introducing these measures.
Levels of medical staffing and patterns of work are discussed. For many
ICUs a closed system with a ‘week-on’ consultant pattern produces good
results even if medical staff are working with a special interest in inten-
sive care rather than being specifically intensive care trained.
Keywords Critical care; consultant work pattern; mortality
Emergencycare
Radiology
Infection contol
Pathology
Pharmacy
Sterile supplies
CRITICALCAREAREA
In-patientacute
services
OPERATINGTHEATRE
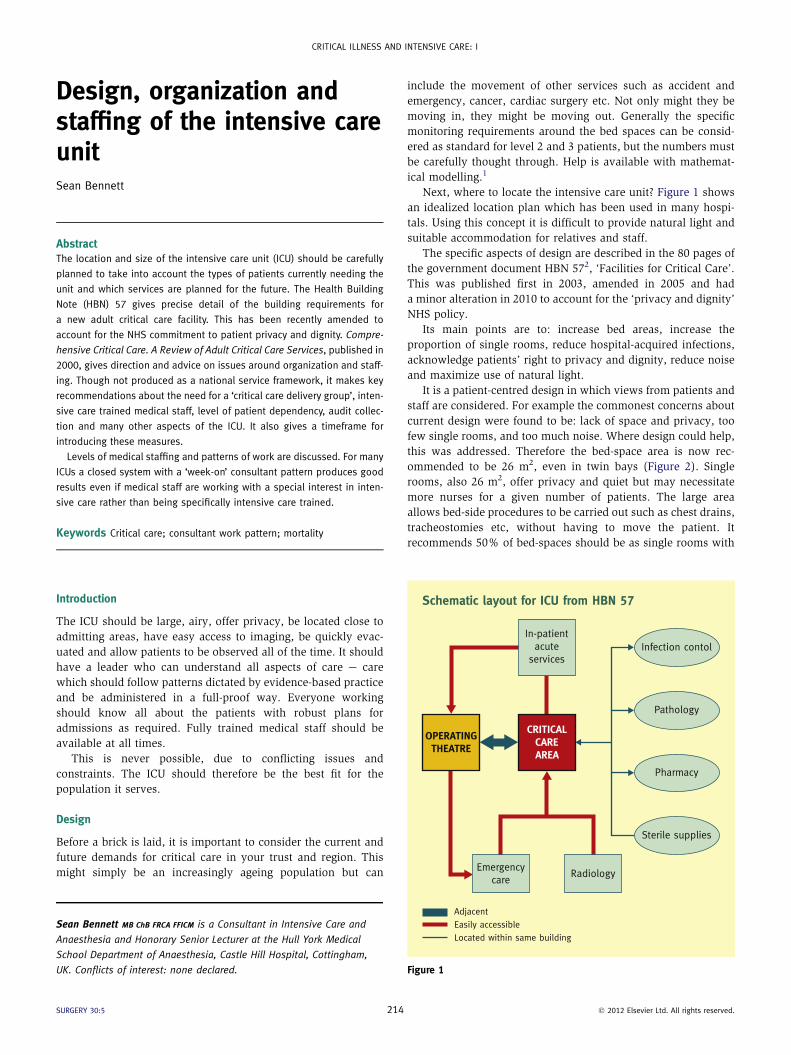
Schematic layout for ICU from HBN 57
IntroductionThe ICU should be large, airy, offer privacy, be located close to
admitting areas, have easy access to imaging, be quickly evac-
uated and allow patients to be observed all of the time. It should
have a leader who can understand all aspects of care e care
which should follow patterns dictated by evidence-based practice
and be administered in a full-proof way. Everyone working
should know all about the patients with robust plans for
admissions as required. Fully trained medical staff should be
available at all times.
This is never possible, due to conflicting issues and
constraints. The ICU should therefore be the best fit for the
population it serves.
Design
Before a brick is laid, it is important to consider the current and
future demands for critical care in your trust and region. This
might simply be an increasingly ageing population but can
Sean Bennett MB ChB FRCA FFICM is a Consultant in Intensive Care and
Anaesthesia and Honorary Senior Lecturer at the Hull York Medical
School Department of Anaesthesia, Castle Hill Hospital, Cottingham,
UK. Conflicts of interest: none declared.
SURGERY 30:5 214
include the movement of other services such as accident and
emergency, cancer, cardiac surgery etc. Not only might they be
moving in, they might be moving out. Generally the specific
monitoring requirements around the bed spaces can be consid-
ered as standard for level 2 and 3 patients, but the numbers must
be carefully thought through. Help is available with mathemat-
ical modelling.1
Next, where to locate the intensive care unit? Figure 1 shows
an idealized location plan which has been used in many hospi-
tals. Using this concept it is difficult to provide natural light and
suitable accommodation for relatives and staff.
The specific aspects of design are described in the 80 pages of
the government document HBN 572, ‘Facilities for Critical Care’.
This was published first in 2003, amended in 2005 and had
a minor alteration in 2010 to account for the ‘privacy and dignity’
NHS policy.
Its main points are to: increase bed areas, increase the
proportion of single rooms, reduce hospital-acquired infections,
acknowledge patients’ right to privacy and dignity, reduce noise
and maximize use of natural light.
It is a patient-centred design in which views from patients and
staff are considered. For example the commonest concerns about
current design were found to be: lack of space and privacy, too
few single rooms, and too much noise. Where design could help,
this was addressed. Therefore the bed-space area is now rec-
ommended to be 26 m2, even in twin bays (Figure 2). Single
rooms, also 26 m2, offer privacy and quiet but may necessitate
more nurses for a given number of patients. The large area
allows bed-side procedures to be carried out such as chest drains,
tracheostomies etc, without having to move the patient. It
recommends 50% of bed-spaces should be as single rooms with
Located within same buildingEasily accessibleAdjacent
Figure 1
� 2012 Elsevier Ltd. All rights reserved.

Figure 2 Twin bay. Figure 4 Glass screen.
CRITICAL ILLNESS AND INTENSIVE CARE: I
a projection of all rooms being single (Figure 3). With single
rooms comes an increased demand on room ventilation so that
the patient can be isolated by use of air flow, which ideally
should be bi-directional. Cubicles for isolation require a gowning
air-lock room which adds around 7 m2 to the cubicle. All spaces
must be wide enough (2.5 m) to allow a range of specialist ICU
beds though.
ICU is not exempt from delivering same-sex accommodation.
However, it is recognized that some patients need observation
and treatment which may result in exposure. It is expected that
no patient or relative should be able to see or overhear personal
aspects of another patient’s care. Curtains and screens can be
used but fixed glass screens with internal blinds are probably
better (Figure 4). Also available are glass screens with the
property of being turned ‘on’ (clear) or ‘off’ (opacified), so-called
‘smart or PolyvisionTM glass’.
The most recent version of HBN 57 is available free of charge
at ‘Space for Health’ via NHS e-mail.
Design is regulated but includes a lot of what one feels is right.
Scott gives a good account of building an ICU using HBN 57.3
A non-hostile environment is preferable although adding extra
Figure 3 Glass cubicle.
SURGERY 30:5 215
touches has no impact on outcomes.4 Wenham discusses how
a non-hostile environment can be created and its effect on
reducing delirium and the consequent length of stay.5
Organization
This can be divided into organizing the services coming into ICU,
and organizing services within a critical area. For example do
you mix general medicine with general surgery? Do you mix
general surgery with cancer surgery or other specialties like
gynaecology? Do you mix neurosurgery with any of the above?
The answer is more traditional than scientific.
The government recommendation in Comprehensive Critical
Care is ‘critical care without walls’ and that the hospital as
a whole should have a say in the organization of critical care,6
specifically by implementing critical care delivery groups and
regional networks. Typically areas like cardiac and neurosurgery
have been on their own while other specialties have wanted to
group together. Why is that? Early on it was shown that certain
specialties of very complex work achieved better results if they
did higher volumes.7 Cardiac surgery has a high turnover with
only one in 20 patients requiring care longer than a day or so, but
it is an important time for which critical care is needed. The high
turnover produced many patients, so cardiac surgeons were
reluctant to lose beds to other specialties. There was also the
question of cross-infection from possibly unscreened patients to
patients with prosthetic material (heart valves). What about other
specialties? Their problem is that there are often not enough
patients that regularly require level 3 care to justify a dedicated
unit. The obvious answer is to pool patients from further afield.
However a catchment area that generates around 1000 cardiac
patients will only generate up to 100 operable oesophageal
cancers. Thus they have to combine with other services.
Oesophageal surgery outcomes improve as do other specialties
like abdominal aortic surgery with increased volume.8 Increased
volume is very apparent in services like cardiac surgery, major
vascular and major cancer and it is probable that the improve-
ments resulting from higher numbers comes not just from an
individual surgeon having more cases, but from the critical care
staff becoming familiar with the complications of the surgery.9
� 2012 Elsevier Ltd. All rights reserved.

CRITICAL ILLNESS AND INTENSIVE CARE: I
Can services like cardiac and neurosurgery use combined
facilities? Yes, they can, but each needs to be big enough to be
viable and if they then combine, the unit can get quite large.
Visiting Cornell University, New York you see an ICU on a huge
scale, nearly 60 beds in a single area. It is not possible to run this
as one unit and so the individual services like cardiac become
grouped so that the unit effectively runs as several individual
units. The size tends to be seven to ten beds, which for many
reasons is an optimal number. The new ICU in Leeds though large
in total is built in subunits of seven beds, each run independently.
Infection is a major consideration in organization. Design
comes into this with cubicles, ventilation and so on. In theory all
patients are in ‘virtual isolation’ whether in a cubicle or not. But
spread by touch is not the only consideration. The unit must be
organized in a way that high turnover, ‘screened and clean,’
patients do not come near unscreened or infected patients (who
tend to be the emergency and long term patients).
Thus it is reasonable to have separate units or units within
a unit where this happens. With this approach the unit can orga-
nize areas with open planning and lower staff numbers with
reduced costs. This is also beneficial to patients. After years of
working such a system for cardiac surgery, Aps describes an
‘overnight intensive recovery’, or OIR. He outlines the advantages
to both patients and critical care resources.10 Though this was
originally specific to cardiac services it clearly has a wider appli-
cation once the concept is understood across the hospital services.
It represents a great organizational achievement as it breaks down
many traditional barriers. The concept is that selected elective
cases from a range of specialties, which are expected to recover
within 24 h, can move into a facility organized to respond to their
needs. A prerequisite for an OIR is to have a bed available so that
the surgery can go ahead. This is much easier to plan in such an
area. The next requirement is for high levels of observation for
signs of early complications. Here the design of charts and moni-
tors can be specific for the patient whilst allowing the patient some
comfort and reduced interference. Equipment useful in diagnosis of
acute problems (such as ultrasound to detect bleeding) can be
shared across all the patients and be available 24 hours a day.
Other factors like natural lighting are less important but control of
lighting is appropriate. This area, ‘intensive recovery’ or ‘progress
care unit’ needs to be adjacent to the operating rooms.
Close to this area but not adjacent to the operating rooms is an
area for the higher dependency patients who are expected to
remain for longer periods. Does this sound like the traditional ICU?
The difference is that if the high turnover work is removed from
the ICU the hospital can now provide for the higher dependency
‘sicker’ patients in a single unit usually of ten beds with optimal
use of facilities and staff. The design reflects the patients’ needs
with all infected cases requiring cubicles. ‘Specialist’ patients that
develop multi-system failure can move to the general ICU as their
original pathology becomes relatively less important.
Medical patients requiring ICU would tend to go directly to
this type of area.
It is useful for the less portable diagnostic equipment like CT
scanners to be nearer here, also provision of natural lighting and
facilities for relatives.
Such design and organization can be more imaginative so that
there is a continuum. The recovery area can be close to the
operating rooms, joining recovery is the ‘intensive recovery or
SURGERY 30:5 216
‘progressive care unit’, leading from this is the intensive care
unit. This arrangement can be built as a corridor or a square area.
However it works well in a horse-shoe pattern. The patients go
directly to the correct area and then move as appropriate. This is
very efficient from the point of view of medical and nurse staff-
ing. It is a system that can work in smaller hospitals too.
Typically it will reduce the number of ICU beds that would have
been calculated in the traditional approach.
Hospitals without tertiary work see fewer elective high-risk
patients as they become centralized, for example oesophagec-
tomies and aortic aneurysms. But they will have older patients
having routine surgery and medical admissions. These units
require a different organization. They should be adjacent to the
operating rooms and close to accident and emergency. Cubicles
must be used flexibly and have staff training across a range of
specialties. Here the main problem is the lack of alternatives
within the hospital if they have admissions beyond their
capacity. Thus they need to consider case mix, severity of illness
and have a good triage system at all times. This will ensure that
certain patients are moved to appropriate facilities in other
hospitals, thus allowing local patients to gain admission to ICU
avoiding non-clinical transfers. An important part of this type of
triage model is the involvement of the regional critical care
network. In this way the triage of groups such as paediatrics,
neurosurgery, trauma, advanced respiratory care etc can be pre-
planned which removes stress at work and improves patient
outcomes. Such modernization has been considered to have had
a dramatic effect on critical care organization.11
Paper work and documentation are important with no perfect
system. Observation charts can be designed to focus on certain
patient groups like neurosurgery but general charts need to cover
all systems. Some hospitals feel that one chart should fit all types
of patient, but this leads to bulky charts with time spent on often
irrelevant information. Staff can adapt and there is much to be
said for a thoughtful and relevant process rather than an auto-
matic tick-box exercise. This applies to paper or electronic
systems and medical and nursing staff. The chart exists as
a prompt and a record. Being prompted to record intracranial
pressure in a general surgical patient is not appropriate.
Audit on ICU has progressed significantly. Almost all units in
England and Wales are now signed-up to ICNARC (Intensive
Care National Audit and Research Centre) case-mix programme.
This took on more importance when the critical care minimum
data set (CCMDS) was included in the INARC data. The CCMDS
was developed by the Critical Care Information Advisory Group
endorsed by the Intensive Care Society. These data are required
to generate health resource groups (HRGs) which are needed for
payment by results (PbR). Though not yet implemented, the idea
was to provide information which would reflect the true cost of
caring for patients on ICU. See the article by Whittle & Shelton in
this issue for more information on ICNARC processes.
Staffing
Comprehensive Critical Care provides a foundation on which the
current organization and staffing of intensive care in the UK is
built.4 Many of the recommendations were already happening
but it is re-assuring and points in the right direction. On nurse
staffing it recommends a one-to-one nurse:patient ratio for level
� 2012 Elsevier Ltd. All rights reserved.

CRITICAL ILLNESS AND INTENSIVE CARE: I
3 patients, but also stresses the concept of setting nursing levels
to the patient’s dependency rather than a fixed number in all
areas. More contentious is the nursing level required to achieve
this. Many units have six or seven nurses employed per ICU bed
to achieve this, whereas Comprehensive Critical Care states
a ratio of 5.5 nurses per bed. This is discussed in more detail
elsewhere in this edition. Nurse working has moved to 12-hour
shifts, which has not caused any notable improvement or detri-
ment in care,12 although having more nurses does improve
infection control.13 Doctors working on intensive care should all
be specifically trained and no team should cover more than eight
level 3 patients. This is a good aim, but currently there are
insufficient numbers of trained doctors to run all ICUs.
A more pragmatic approach is whether the unit runs an ‘open’
or ‘closed’ system and whether it operates a ‘high’ or ‘low’
intensity staffing system. High-intensity staffing is when the
admitting specialist retains management of the patient but there
is also a senior doctor on the unit full-time who is responsible for
the daily patient care (most of the UK). Low intensity is where
there is no permanent ICU doctor.
An open system is basically as the high intensity but closed is
very different. In a closed system the admitting specialist
discusses the case with the doctor on intensive care. The patient
is admitted under the intensive care doctor. The admitting
specialist then takes a back seat. This is common in Australia
where more doctors are trained in intensive care. There are
a few studies to support this pattern of work. One unit with an
open system but a daily ward round from an intensivist, had
a threefold reduction in mortality, mainly among vascular
patients.7 A similar study focussing on oesophageal surgery
found a decreased length of stay (LOS), decreased costs but no
difference in mortality.14 Daily rounds specifically reduce
complications which adversely affect LOS, re-intubation,
pneumonia and acute renal failure. Further studies in mixed
patient groups show similar results.15 In a review of working
patterns 14 out of 15 units using high-intensity staffing showed
a reduction in mortality.16 One study looking at open versus
closed systems, albeit in a ‘before and after’ design, showed
decreased LOS and complications and lower mortality in the
closed system.17
Working patterns can affect patient outcomes. Having an
intensivist see all admissions (24 hours a day) has a cost, but it
has been shown to reduce mortality and ICU length of stay.18 As
a counter argument though many specialist units have developed
various types of nurse practitioners. One cardiac unit in the UK
has no resident medical staff out of hours. This has been closely
monitored and has not caused any adverse effects on outcomes
(personal communication). Even general units have successfully
introduced nurse practitioners.19 This usefully removes the
burden of too many junior doctors to comply with working time
directives.
Another successful system is having a senior physician,
‘week-at-a-time’ work pattern. In this, the same doctor is
responsible for the daily running of the unit from Monday to
Friday. Each week the doctor changes. It can work in an open or
closed system. Royle described how this was introduced in a way
which allowed comparison of data.20 One ICU continued the
previous system which was open with a different anaesthetist
each session/day. The other unit (in the same trust) had four
SURGERY 30:5 217
anaesthetists with an interest in intensive care working Monday
morning to Friday lunchtime (no nights) on a 4-week rota. Both
units had a similar population. During the 12-month study both
units practised according to the same guidelines introducing
‘ventilator care bundles’, ‘Surviving Sepsis Campaign’ etc. The
authors looked at mortality before and after the year and
between the two units. They found that mortality overall was
reduced in both units but this did not reach significance.
However the ‘week-on’ unit showed a statistically significant
reduction in mortality for ventilated patients.
Units should be multidisciplinary. Radiology and pathology
services are important and add to patient care and teaching. The
most common errors on ICU come from prescribing and having
a pharmacist who specializes in intensive care reduces these
errors. Physiotherapists need to be trained in invasive and non-
invasive ventilation techniques and be available 24 hours a day.
In the UK a nurse:patient ratio is usually 1:1. Some western
countries run different systems. For example, having all the
beds in twin cubicles with one nurse in each cubicle. At first
sight this appears hard for the nurse. However the nurse is fully
supported by pharmacy, physiotherapy, respiratory care tech-
nicians and others. This means the nurse does not have to leave
the room. Movement in and out and therefore infection risk is
reduced.
In summary the ICU location and size should be carefully
planned to reflect the needs of the patient population. The
running of ICU should maximize the potential of its staff. In this
way good results can be achieved even if the medical staff are not
specifically intensive care trained. A
REFERENCES
1 Costa AX, Ridley SA, Shahani AK, Harper PR, De Senna V, Nielson MS.
Mathematical modeling and simulation for planning critical care
capacity. Anaesthesia 2003; 58: 320e7.
2 NHS Estates. Facilities for critical care HBN 57. London: The Statio-
nery Office, May 2005.
3 Scott CJ. Building a critical care unit for Sheffield using a new NHS
estates building strategy-ProCure 21: partnership approach to NHS
building. J Intensive Care Soc 2008; 9: 158e9.
4 Fontaine DK, Briggs LP, Pope-Smith B. Designing humanistic critical
care environments. Crit Care Nursing 2001; 24: 21e34.
5 Wenham T, Pittard A. Intensive care unit environment. Continuing
Educ Anaesthesia Crit Care Pain 2009; 9: 178e83.
6 Comprehensive critical care: a review of adult critical care services.
London: Department of Health, http://www.doh.gov.uk/nhsexec/
compcritcare.htm; May 2000.
7 Halm EA, Lee C, Chassin MR. Is volume related to outcome in health
care? A systematic review and methodologic critique of the literature.
Ann Intern Med 2002; 137: 511e20.
8 Pronovost PJ, Jenkes MW, Dorman T, et al. Organizational character-
istics of intensive care units related to outcomes of abdominal aortic
surgery. J Am Med Assoc 1999; 281: 1310e7.
9 Hillner BE, Smith TJ, Desch CE. Hospital and physician volume or
specialization and outcomes in cancer treatment: importance in
quality of cancer care. J Clin Oncol 2000; 18: 2327e40.
10 Aps C. Adopting a fast track approach to cardiac surgery. Br J Cardiac
Nurs 2006; 1: 174e9.
� 2012 Elsevier Ltd. All rights reserved.

CRITICAL ILLNESS AND INTENSIVE CARE: I
11 Durand M, Hutchings A, Black N. ‘Not quite Jericho, but more doors
than there used to be’. Staff views of the impact of ‘modernization’
on boundaries around adult critical care services in England. J Health
Serv Res Policy 2010; 15: 229e35.
12 McGettrick KS, O’Neill M. Critical care nurses-perceptions of 12-h
shifts. Nurs Crit Care 2006; 11: 188e97.
13 Hugonnet S, Chevrolet JC, Pittet D. The effect of workload on infec-
tion risk in critically ill patients. Crit Care Med 2007; 35: 76e81.
14 Dimick JB, Pronovost PJ, Heitmiller RF, Lipsett PA. Intensive care unit
physician staffing is associated with decreased length of stay,
hospital cost and complications after esophageal resection. Crit Care
Med 2001; 29: 753e8.
15 Hanson CW, Deutschman CS, Anderson HL. Effects of an organized
critical care service on outcomes and resource utilization: a cohort
study. Crit Care Med 1999; 27: 270e4.
SURGERY 30:5 218
16 Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT,
Young TL. Physician staffing patterns and clinical outcomes in critically
ill patients: a systematic review. J Am Med Assoc 2002; 288: 2151e62.
17 Ghorra S, Reinert SE, Cioffi W, Buczko G, Simms HH. Analysis of the
effect of conversion from open to closed surgical intensive care unit.
Ann Surg 1999; 229: 163e71.
18 Banerjee R, Naessens JM, Seferian EG, et al. Economic implications of
nighttime attending intensivist coverage in a medical intensive care
unit. Crit Care Med 2011; 39: 1257e62.
19 Landsperger JS, Williams KJ, Hellervik SM, et al. Implementation of
a medical intensive care unit acute-care nurse practitioner service.
Hosp Prac 2011; 39: 32e9.
20 Royle P, Bramall J, Norrington A. The effect of introducing a consul-
tant weekly working pattern on mortality in a critical care unit.
J Intensive Care Soc 2008; 9: 26e9.
� 2012 Elsevier Ltd. All rights reserved.