Embed Size (px)
Citation preview

PII S0360-3016(99)00005-X
PHYSICS CONTRIBUTION
DESIGN AND DEVELOPMENT OF NEW COLLIMATOR CONES FORFRACTIONATED STEREOTACTIC RADIATION THERAPY IN
SAMSUNG MEDICAL CENTER
YONG CHAN AHN, M.D.,* SANG GYU JU, R.T.T.,* DAE YONG KIM, M.D.,* DONG RAK CHOI, PH.D.,*SEUNG JAE HUH, M.D.,* YOUNG HWAN PARK, R.T.T.,* DO HOON LIM, M.D.,*
AND MOON KYUNG KIM, M.D.*
Department of Radiation Oncology, Samsung Medical Center, College of Medicine, Sungkyunkwan University, Seoul, Korea
Purpose: In stereotactic radiotherapy using X-Knife system, the commercially supplied collimator cone systemhad a few mechanical limitations. The authors have developed new collimator cones to overcome these limitationsand named them “SMC type” collimator cones.Methods: We made use of cadmium-free cerrobend alloy within the stainless steel cylinder housing. We madenine cones of relatively larger sizes (3.0 cm to 7.0 cm in diameter) and of shorter length with bigger clearancefrom the isocenter than the commercial cones. The cone housing and the collimator cones were designed to insertinto the wedge mount of the gantry head to enable double-exposure linac-gram taking.Results: The mechanical accuracy of pointing to the isocenter was tested by ball test and cone rotation test, andthe dosimetric measurements were performed, all of which were with satisfactory results. A new innovativequality assurance procedure using linac-grams on the patients at the actual treatment setup was attempted aftertaking 10 sets of AP and lateral linac-grams and the overall mechanical isocenter accuracy was excellent (averageerror 5 0.4 6 0.2 mm).Conclusions: We have developed the SMC type collimator cone system mainly for fractionated stereotacticradiation therapy use with our innovative ideas. The new cones’ mechanical accuracy and physical propertieswere satisfactory for clinical use, and the verification of the isocenter accuracy on the actual treatment setup hasbecome possible. © 1999 Elsevier Science Inc.
Fractionated stereotactic radiation therapy, Collimator cones, Quality assurance.
INTRODUCTION
Fractionated stereotactic radiation therapy (FSRT) is a rel-atively recent treatment modality, which stems from stereo-tactic radiosurgery (SRS). SRS’s strongest point lies in itsguaranteed mechanical accuracy by skeletal fixation, andthe delivery of high focal radiation was justifiable even if itcontradicts the concept of fractionation integral to modernradiation oncology practice since the 1920s. As clinicalexperience of SRS application accumulated, there havebeen clinical reports that there is risk of late radiationmorbidity (1, 2). FSRT has the capability of conventionalfractionation with a high degree of mechanical accuracyusing noninvasive relocatable stereotactic frame.
We began SRS and FSRT in February and July of 1995,respectively, using the X-Knife system. As our clinical
experience using the X-Knife system grew, we realized thatthere were some limitations in using the manufacturer-supplied collimator cones for FSRT: (1) The collimatorcones were of smaller sizes than needed, as they weremainly designed for SRS to treat relatively small lesions. (2)Changing collimator cones of different sizes on the sameisocenter is very difficult. The commercial cones were de-signed to fit into the cone housing which is screwed andfixed to the gantry head during the treatment sessions. Asthe narrow space between the patient’s head and the tip ofthe cone housing is left, the treatment couch had to beunlocked and retracted away from the gantry head in orderto change cones without collision. After changing cones, thetreatment couch had to be reset, which is not only inconve-nient but also time-consuming. (3) It was impossible to take
Reprint requests to: Yong Chan Ahn, M.D., Department ofRadiation Oncology, Samsung Medical Center, College of Medi-cine, Sungkyunkwan University, 50 Ilwon-dong, Kangnam-ku,Seoul, 135-710, Korea.
This work was partly supported by the Clinical Research Fundof Samsung Medical Center, Sungkyunkwan University, and bythe Korean Atomic Energy Research Grant.
Presented at “Radiology 1998” (British Institute of Radiology,
Birmingham, UK) on June 1, 1998.Acknowledgments—The authors are deeply indebted to Mr. JungKeun Cho, Mr. Young Gon Kim, and Mr. Hyun Sang Cho for theircontributions in the commissioning of the SMC type collimatorcones and the measurements for isocenter verification using linac-grams.
Accepted for publication 30 December 1998.
Int. J. Radiation Oncology Biol. Phys., Vol. 44, No. 2, pp. 435–438, 1999Copyright © 1999 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/99/$–see front matter
435
double-exposure linac-grams on the patient for quality as-surance purposes, as the metallic cone housing was de-signed to be in place at the gantry head and, hence, difficult
to remove and reset. Our need for the new collimator coneswas to overcome the above mentioned limitations. We havedeveloped our new collimator cones to accommodate theabove needs, and named them “SMC type” collimatorcones. This article describes the design, characteristics, andphysical properties of the SMC type collimator cones, aswell as the quality assurance procedure, using angiolocal-izer and double-exposure linac-grams taken on the patients,and its results.
DESIGN AND DEVELOPMENT OF NEWCOLLIMATOR CONES
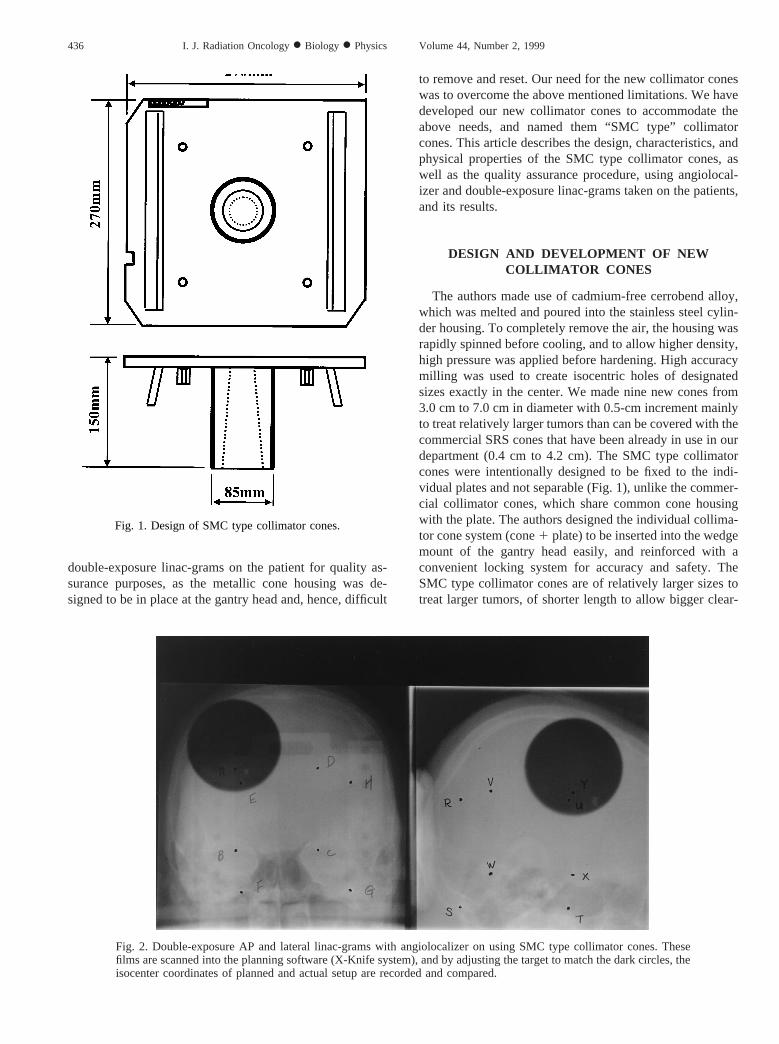
The authors made use of cadmium-free cerrobend alloy,which was melted and poured into the stainless steel cylin-der housing. To completely remove the air, the housing wasrapidly spinned before cooling, and to allow higher density,high pressure was applied before hardening. High accuracymilling was used to create isocentric holes of designatedsizes exactly in the center. We made nine new cones from3.0 cm to 7.0 cm in diameter with 0.5-cm increment mainlyto treat relatively larger tumors than can be covered with thecommercial SRS cones that have been already in use in ourdepartment (0.4 cm to 4.2 cm). The SMC type collimatorcones were intentionally designed to be fixed to the indi-vidual plates and not separable (Fig. 1), unlike the commer-cial collimator cones, which share common cone housingwith the plate. The authors designed the individual collima-tor cone system (cone1 plate) to be inserted into the wedgemount of the gantry head easily, and reinforced with aconvenient locking system for accuracy and safety. TheSMC type collimator cones are of relatively larger sizes totreat larger tumors, of shorter length to allow bigger clear-
Fig. 1. Design of SMC type collimator cones.
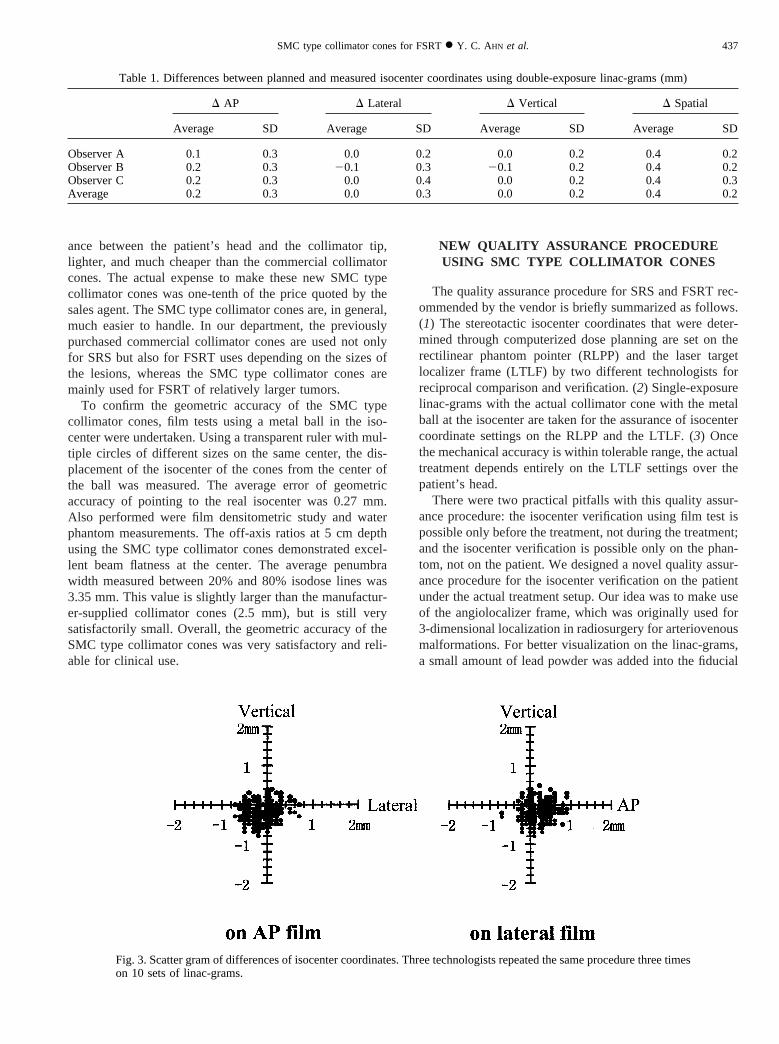
Fig. 2. Double-exposure AP and lateral linac-grams with angiolocalizer on using SMC type collimator cones. Thesefilms are scanned into the planning software (X-Knife system), and by adjusting the target to match the dark circles, theisocenter coordinates of planned and actual setup are recorded and compared.
436 I. J. Radiation Oncology● Biology ● Physics Volume 44, Number 2, 1999
ance between the patient’s head and the collimator tip,lighter, and much cheaper than the commercial collimatorcones. The actual expense to make these new SMC typecollimator cones was one-tenth of the price quoted by thesales agent. The SMC type collimator cones are, in general,much easier to handle. In our department, the previouslypurchased commercial collimator cones are used not onlyfor SRS but also for FSRT uses depending on the sizes ofthe lesions, whereas the SMC type collimator cones aremainly used for FSRT of relatively larger tumors.
To confirm the geometric accuracy of the SMC typecollimator cones, film tests using a metal ball in the iso-center were undertaken. Using a transparent ruler with mul-tiple circles of different sizes on the same center, the dis-placement of the isocenter of the cones from the center ofthe ball was measured. The average error of geometricaccuracy of pointing to the real isocenter was 0.27 mm.Also performed were film densitometric study and waterphantom measurements. The off-axis ratios at 5 cm depthusing the SMC type collimator cones demonstrated excel-lent beam flatness at the center. The average penumbrawidth measured between 20% and 80% isodose lines was3.35 mm. This value is slightly larger than the manufactur-er-supplied collimator cones (2.5 mm), but is still verysatisfactorily small. Overall, the geometric accuracy of theSMC type collimator cones was very satisfactory and reli-able for clinical use.
NEW QUALITY ASSURANCE PROCEDUREUSING SMC TYPE COLLIMATOR CONES
The quality assurance procedure for SRS and FSRT rec-ommended by the vendor is briefly summarized as follows.(1) The stereotactic isocenter coordinates that were deter-mined through computerized dose planning are set on therectilinear phantom pointer (RLPP) and the laser targetlocalizer frame (LTLF) by two different technologists forreciprocal comparison and verification. (2) Single-exposurelinac-grams with the actual collimator cone with the metalball at the isocenter are taken for the assurance of isocentercoordinate settings on the RLPP and the LTLF. (3) Oncethe mechanical accuracy is within tolerable range, the actualtreatment depends entirely on the LTLF settings over thepatient’s head.
There were two practical pitfalls with this quality assur-ance procedure: the isocenter verification using film test ispossible only before the treatment, not during the treatment;and the isocenter verification is possible only on the phan-tom, not on the patient. We designed a novel quality assur-ance procedure for the isocenter verification on the patientunder the actual treatment setup. Our idea was to make useof the angiolocalizer frame, which was originally used for3-dimensional localization in radiosurgery for arteriovenousmalformations. For better visualization on the linac-grams,a small amount of lead powder was added into the fiducial
Fig. 3. Scatter gram of differences of isocenter coordinates. Three technologists repeated the same procedure three timeson 10 sets of linac-grams.
Table 1. Differences between planned and measured isocenter coordinates using double-exposure linac-grams (mm)
D AP D Lateral D Vertical D Spatial
Average SD Average SD Average SD Average SD
Observer A 0.1 0.3 0.0 0.2 0.0 0.2 0.4 0.2Observer B 0.2 0.3 20.1 0.3 20.1 0.2 0.4 0.2Observer C 0.2 0.3 0.0 0.4 0.0 0.2 0.4 0.3Average 0.2 0.3 0.0 0.3 0.0 0.2 0.4 0.2
437SMC type collimator cones for FSRT● Y. C. AHN et al.

marker points of the angiolocalizer. After treatment setup,the angiolocalizer frame was placed on the stereotacticframe, and double-exposure linac-grams were taken on APand lateral directions with and without the collimator cone.Taking double-exposure linac-gram is only possible usingthe new SMC type collimator cones designed with our novelidea. After scanning the linac-grams into the X-Knife soft-ware, the fiducial marker points, which are easily identifi-able on the double-exposure linac-grams, are computed for3-dimensional localization (Fig. 2). By adjusting the posi-tion of the target outline on the planning software to exactlymatch the dark circles of the collimator openings that weretaken on the patient, the isocenter coordinates are recordedand compared with the initial plan coordinates. In order tosee how reliable and reproducible this procedure is, we took10 sets of linac-grams on four different patients. We hadthree different technologists perform this procedure of de-termining the 3-dimensional coordinates of the isocenterwithout giving coordinate information, to determine theinterpersonal variation. Each technologist was asked to re-peat the same procedure three times to determine the in-trapersonal variation. The total number of measurements onthe isocenter was 180, from which the interpersonal and
intrapersonal variation and the magnitude of the isocenter’sspatial displacement were analyzed. The interpersonal aswell as the intrapersonal variation was very small, and theaverage spatial displacement was only 0.4 mm (Table 1,Fig. 3).
SUMMARY
As described here, the physical properties as well as themechanical accuracy of our SMC type collimator cones arevery satisfactory for clinical use. Moreover, isocenter veri-fication on the patient under actual treatment setup hasbecome possible using our cones. The commissioning of thenew SMC type collimator cones was possible in December1996, and the first clinical use was in January 1997. In fact,the number of FSRT cases has been steadily increasing, andwe believe that this increase was boosted by the develop-ment of the new collimator cone system. The authors as-sume that if our quality assurance procedure could be cou-pled with software for 3-dimensional coordinate calculationand the electronic portal imaging system, on-line verifica-tion would be realized.
REFERENCES
1. Flickinger JC, Lunsford LD, Kondziolka D, Maitz AH, Ep-stein AH, Simons SR, Wu A. Radiosurgery and brain toler-ance: An analysis of neurodiagnostic imaging changes aftergamma knife radiosurgery for arteriovenous malformations.Int J Radiat Oncol Biol Phys1992;23:19–26.
2. Nedzi LA, Kooy H, Alexander E III, Gelman RS, Loeffler JS.Variables associated with the development of complicationsfrom radiosurgery of intracranial tumors.Int J Radiat OncolBiol Phys1991;21:591–599.
438 I. J. Radiation Oncology● Biology ● Physics Volume 44, Number 2, 1999
![Fractionated stereotactic radiosurgery with adaptive dose delivery … · [1] Biau J, Khalil T, Verrelle P, Lemaire JJ. Fractionated radiotherapy and radiosurgery of intracranial](https://img.pdfslide.us/doc/110x75/5f93427b1669d706c03ea228/fractionated-stereotactic-radiosurgery-with-adaptive-dose-delivery-1-biau-j-khalil.jpg)





![arXiv:2005.12071v1 [physics.acc-ph] 25 May 2020a) b) e-Block collimator Block collimator (hidden) Wedge collimator Figure 2: 3D CAD model of the three collimator device. (a) The block](https://img.pdfslide.us/doc/110x75/5f99e989b5ff3471203ba93f/arxiv200512071v1-25-may-2020-a-b-e-block-collimator-block-collimator-hidden.jpg)






















