Embed Size (px)
Citation preview
1
Dermatology Review
2020 EMRAM In-Service
Julie Parks Bortel MD, FACEP
Lecture
Overview
◼ Terminology Review
◼ Describe the key features and a typical
dermatologic presentation for each condition
◼ Case review of common and important rashes
Approach to rashes◼ Determine how the rash started and evolved
◼ Note the distribution, pattern, and configuration
mucous membrane involvement
palm/sole involvement
◼ Is it pruritic or painful
◼ Any prodromal symptoms
Terminology
◼ Excoriation – linear
erosion
◼ Fissure - linear cracks
in skin surface
Terminology
◼ Macular –Flat and
<1cm
◼ Patch – Flat and
>1cm
Terminology
◼ Papule – Raised
<1cm
◼ Plaque – Raised
>1cm
1 2
3 4
5 6

2
Terminology
◼ Vesicle - Blister <1cm ◼ Bullae - Blister >1cm
Terminology
◼ Nodule – Dermal or
subcutaneous lesion
<2 cm
◼ Tumor – Dermal or
subcutaneous lesion
>2cm
Terminology
◼ Pustule – vesicle with
purulent fluid
Scale - visible layers of
stratum corneum
getting shed from the
skin
Terminology
◼ Erosion – Loss of part
or all of the epidermis
◼ Ulcer – Dermis or
deeper
Terminology
◼ Telangiectasia - small, blanching surface
capillaries
Terminology
◼ Purpura – non-blanching purple discoloration > 2mm
◼ Petechiae -- non-blanching purple spots < 2mm in diameter
7 8
9 10
11 12

3
Terminology
◼ Wheal -- transient, edematous papule or plaque with
peripheral erythema
Dermatitis
Rash #1
◼ A 9 month old boy
with a history of
asthma is brought in
by his mother for an
itchy red rash
Dermatitis aka Eczema
◼ Inflammation of the epidermis
◼ Group of skin conditions that includes:
Atopic dermatitis
Allergic contact dermatitis
Irritant contact dermatitis
Stasis dermatitis
◼ Exact cause is often unknown
Atopic Dermatitis
◼ A type of dermatitis with a hereditary
component
◼ Atopic triad – asthma, eczema, allergies
◼ Common in developing countries
◼ Variety of symptoms – erythema, edema,
vesiculation, flaking, weeping, & itching
◼ Treatment aimed at decreasing inflammation
Atopic Dermatitis
13 14
15 16
17 18
4
Atopic Dermatitis
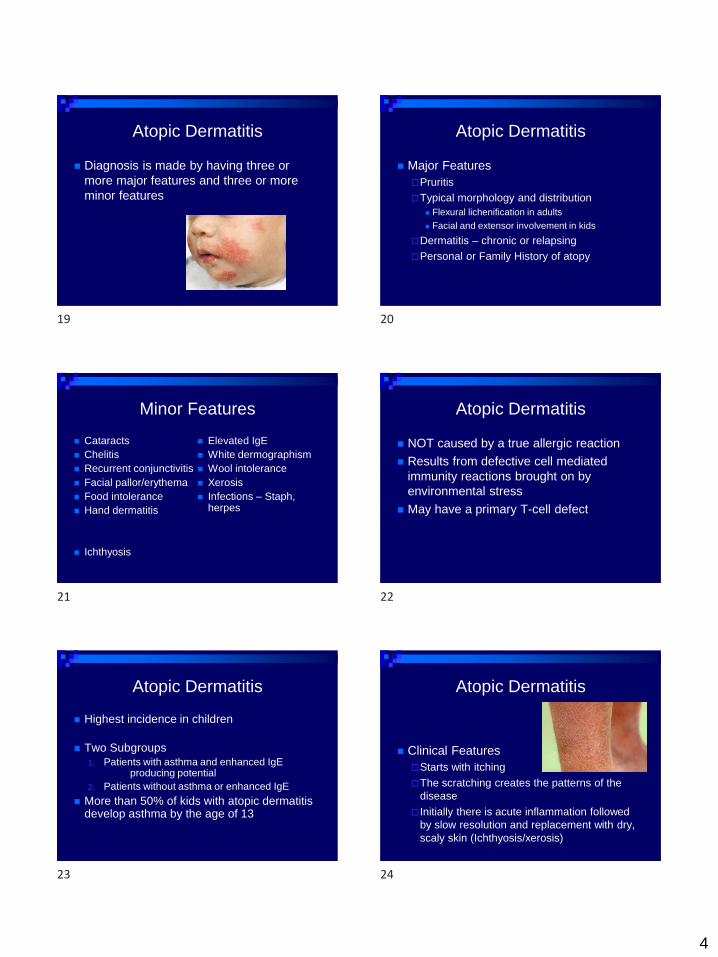
◼ Diagnosis is made by having three or
more major features and three or more
minor features
Atopic Dermatitis
◼ Major Features
Pruritis
Typical morphology and distribution
◼ Flexural lichenification in adults
◼ Facial and extensor involvement in kids
Dermatitis – chronic or relapsing
Personal or Family History of atopy
Minor Features
◼ Cataracts
◼ Chelitis
◼ Recurrent conjunctivitis
◼ Facial pallor/erythema
◼ Food intolerance
◼ Hand dermatitis
◼ Ichthyosis
◼ Elevated IgE
◼ White dermographism
◼ Wool intolerance
◼ Xerosis
◼ Infections – Staph, herpes
Atopic Dermatitis
◼ NOT caused by a true allergic reaction
◼ Results from defective cell mediated
immunity reactions brought on by
environmental stress
◼ May have a primary T-cell defect
Atopic Dermatitis
◼ Highest incidence in children
◼ Two Subgroups
1. Patients with asthma and enhanced IgEproducing potential
2. Patients without asthma or enhanced IgE
◼ More than 50% of kids with atopic dermatitis develop asthma by the age of 13
Atopic Dermatitis
◼ Clinical Features
Starts with itching
The scratching creates the patterns of the
disease
Initially there is acute inflammation followed
by slow resolution and replacement with dry,
scaly skin (Ichthyosis/xerosis)
19 20
21 22
23 24

5
Atopic Dermatitis
◼ AcuteBright red swollen
plaques
Often linear vesicles
Intense itching
◼ SubacuteVarious patterns of
erythema and scale
Mild to moderate itching
Indistinct borders
◼ Chronic Inflamed area is
thickened
Parallel skin markings
Commonly involved areas are easy to reach
3 Phases of Atopic Dermatitis
◼ Infantile Phase (2mo-2yrs)
Affects cheeks, perioral area, scalp, ears,
trunk (spares diaper area), tops of feet, and
elbows
Lesions often exudative
Atopic Dermatitis Phases
◼ Childhood Phase (2-12 yrs)
Flexural involvement
Scratching and chronicity leads to
lichenification
Atopic Dermatitis Phases
◼ Adult Phase (12-adult)
Flexural involvement is common
Hand dermatitis may be only manifestation
Upper lid dermatitis is also common
Associated findings include dry skin,
ichthyosis vulgaris, and keratosis pilaris
Atopic Dermatitis Complications
◼ Skin lesions frequently colonized with staph and secondary infections are common
◼ Increased susceptibility to viral infections
◼ Inflammation can lead to pigmentation changes
◼ In children with moderate-severe disease may also have emotional/behavioral problems
Atopic Dermatitis Treatment
◼ Topical Steroids
◼ Oral Antibiotics for secondary infection
◼ Burrow’s Solution
◼ Lubricant to restore skin barrier
◼ Eliminate aggravating factors
◼ Control Pruritis
◼ Short course of oral steroids if needed
25 26
27 28
29 30

6
Rash #2◼ 35 y.o. male was outside yesterday
mowing his lawn and trimming bushes
now presents to the ER for an intensely
itchy rash.
Allergic Contact Dermatitis
◼ Delayed hypersensitivity reaction
◼ It affects a limited number of people after
they have been exposed to an antigenic
substance
◼ Reactions develop acutely in 6-72 hours
Allergic Contact Dermatitis
◼ Examples
Poison Ivy/oak/sumac
Glue
Insecticides
Acrylics
Latex
Nickel
Neomycin
Poison Ivy/Oak/Sumac
◼ Requires prior sensitization
◼ Caused by the antigen Urushiol
◼ Rash occurs between 6-72 hours after exposure
◼ Lasts 2 days – 3 weeks
◼ Rupturing the vesicles does not spread the rash
◼ Highly characteristic linear lesions
Poison Ivy Poison Oak
31 32
33 34
35 36

7
Poison Sumac Treatment
◼ Mild
Calamine lotion
Benadryl
Topical Steroid
◼ Moderate – Severe
Aveeno bath
Oral Benadryl
Systemic steroids
Rash #3◼ 40 y.o. construction worker who has been
on a job repaving I-75 presents with an
itchy rash. He reports that it improved
over vacation but now seems worse
Irritant Contact Dermatitis
◼ Caused by exposure to environmental substances
◼ Level of irritation is related to duration of exposure and concentration of substance
◼ Gradual onset
◼ Borders correspond to the pattern of the offending agent and often assist in the diagnosis
Contact Dermatitis Irritant Contact Dermatits
◼ Shampoos/soaps
◼ Fuels/lubricants/cement
◼ Pineapple juice
◼ Alcohols, alkalies, grease
37 38
39 40
41 42
8
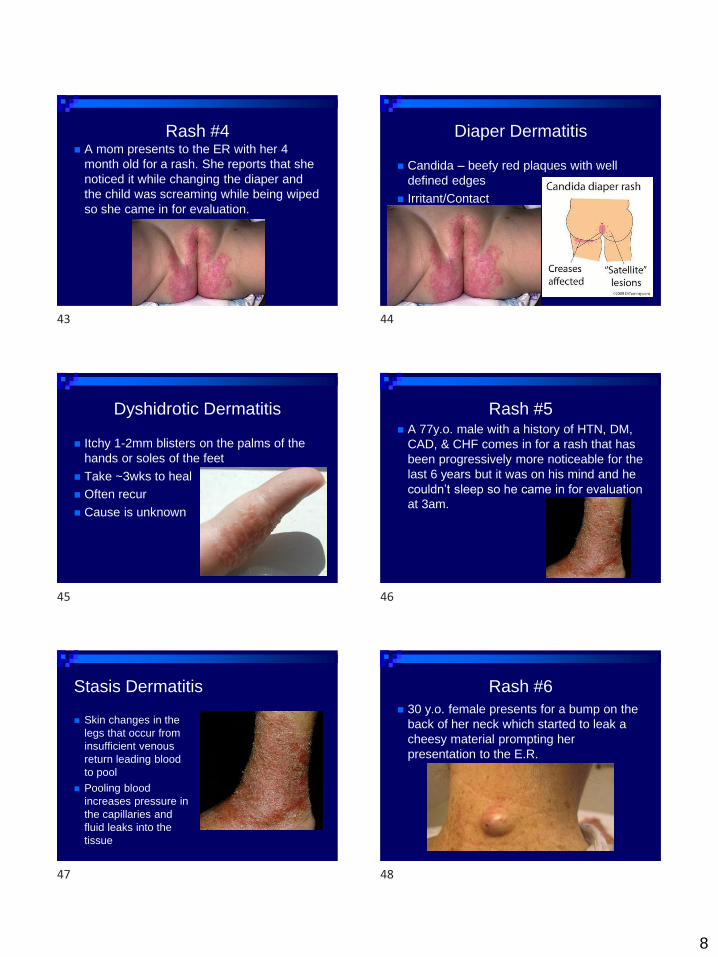
Rash #4◼ A mom presents to the ER with her 4
month old for a rash. She reports that she
noticed it while changing the diaper and
the child was screaming while being wiped
so she came in for evaluation.
Diaper Dermatitis
◼ Candida – beefy red plaques with well
defined edges
◼ Irritant/Contact
Dyshidrotic Dermatitis
◼ Itchy 1-2mm blisters on the palms of the
hands or soles of the feet
◼ Take ~3wks to heal
◼ Often recur
◼ Cause is unknown
Rash #5◼ A 77y.o. male with a history of HTN, DM,
CAD, & CHF comes in for a rash that has
been progressively more noticeable for the
last 6 years but it was on his mind and he
couldn’t sleep so he came in for evaluation
at 3am.
Stasis Dermatitis
◼ Skin changes in the
legs that occur from
insufficient venous
return leading blood
to pool
◼ Pooling blood
increases pressure in
the capillaries and
fluid leaks into the
tissue
Rash #6
◼ 30 y.o. female presents for a bump on the
back of her neck which started to leak a
cheesy material prompting her
presentation to the E.R.
43 44
45 46
47 48
9
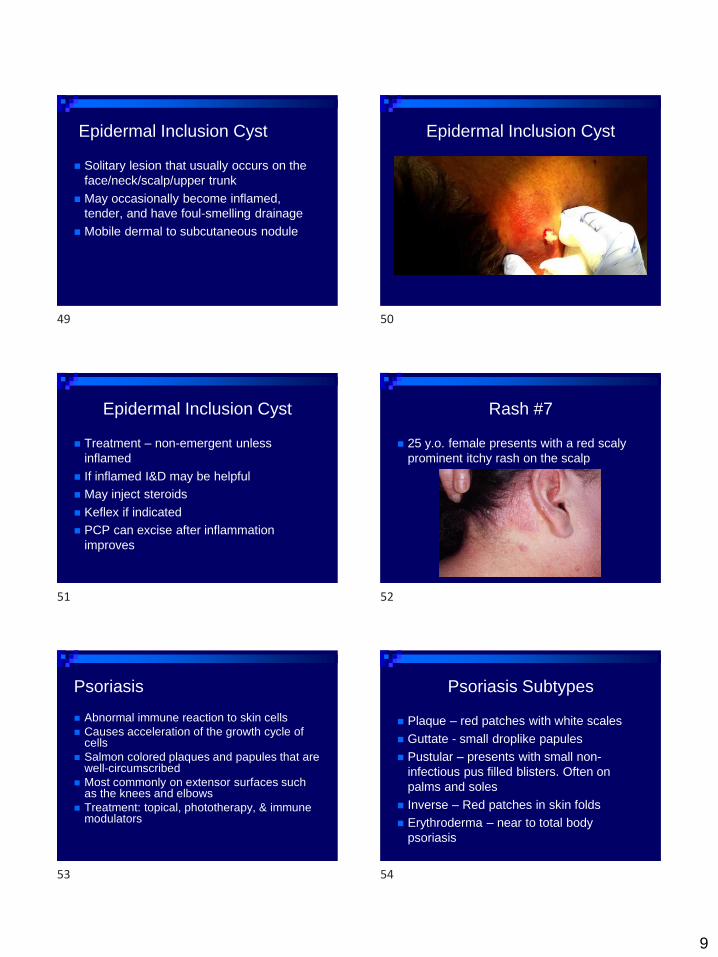
Epidermal Inclusion Cyst
◼ Solitary lesion that usually occurs on the
face/neck/scalp/upper trunk
◼ May occasionally become inflamed,
tender, and have foul-smelling drainage
◼ Mobile dermal to subcutaneous nodule
Epidermal Inclusion Cyst
Epidermal Inclusion Cyst
◼ Treatment – non-emergent unless
inflamed
◼ If inflamed I&D may be helpful
◼ May inject steroids
◼ Keflex if indicated
◼ PCP can excise after inflammation
improves
Rash #7
◼ 25 y.o. female presents with a red scaly
prominent itchy rash on the scalp
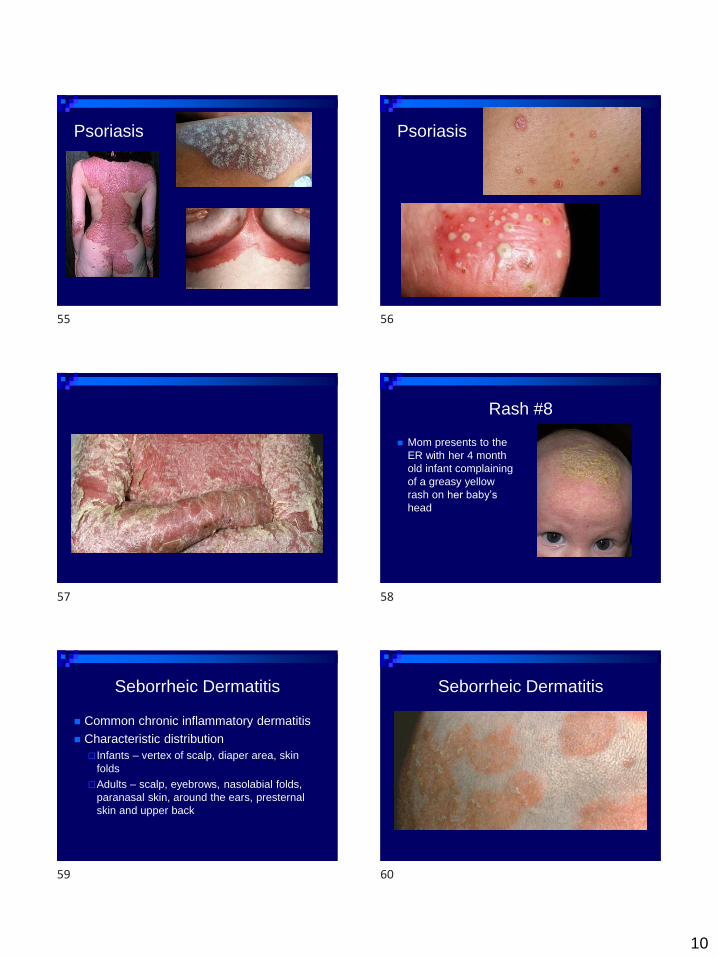
Psoriasis
◼ Abnormal immune reaction to skin cells
◼ Causes acceleration of the growth cycle of cells
◼ Salmon colored plaques and papules that are well-circumscribed
◼ Most commonly on extensor surfaces such as the knees and elbows
◼ Treatment: topical, phototherapy, & immune modulators
Psoriasis Subtypes
◼ Plaque – red patches with white scales
◼ Guttate - small droplike papules
◼ Pustular – presents with small non-
infectious pus filled blisters. Often on
palms and soles
◼ Inverse – Red patches in skin folds
◼ Erythroderma – near to total body
psoriasis
49 50
51 52
53 54
10
Psoriasis Psoriasis
Rash #8
◼ Mom presents to the
ER with her 4 month
old infant complaining
of a greasy yellow
rash on her baby’s
head
Seborrheic Dermatitis
◼ Common chronic inflammatory dermatitis
◼ Characteristic distribution
Infants – vertex of scalp, diaper area, skin
folds
Adults – scalp, eyebrows, nasolabial folds,
paranasal skin, around the ears, presternal
skin and upper back
Seborrheic Dermatitis
55 56
57 58
59 60

11
Seborrheic Dermatitis Treatment
◼ Shampoos to decrease dandruff
◼ Low dose steroid creams – when
necessary
Cradle Cap
◼ neonatal seborrheic dermatitis – greasy, yellow rash
◼ Uncertain of cause ? Related to eczema
Fungal
Overactive sebaceous glands
◼ Treatment Many home remedies – Vegetable oil, Baking soda, herbal
washes
Shampoo, Tar, Steroids, Ketoconazole
Maculopapular
Rashes
Rash #9
◼ A 22 y.o. male presents to the EC complaining
of an intensley painful red rash. Yesterday he
was out on a boat all day partying at
jobbienooner.
Sunburn◼ Acute inflammatory reaction in
response to UV A & B rays
◼ Erythema peaks at 12-24 hours
◼ In severe cases, can lead to 2nd
degree burns
◼ Are there any photosensitizing medications?
◼ Treatment
Cool soaks or OTC cooling agents
Anti-prostaglandins – ASA or NSAIDS
Steroids
Rehydrate and treat at burn center
Rash #10
◼ A 7 y.o. male presents to the ER for an
itchy rash after playing outside on a hot
humid day
61 62
63 64
65 66
12
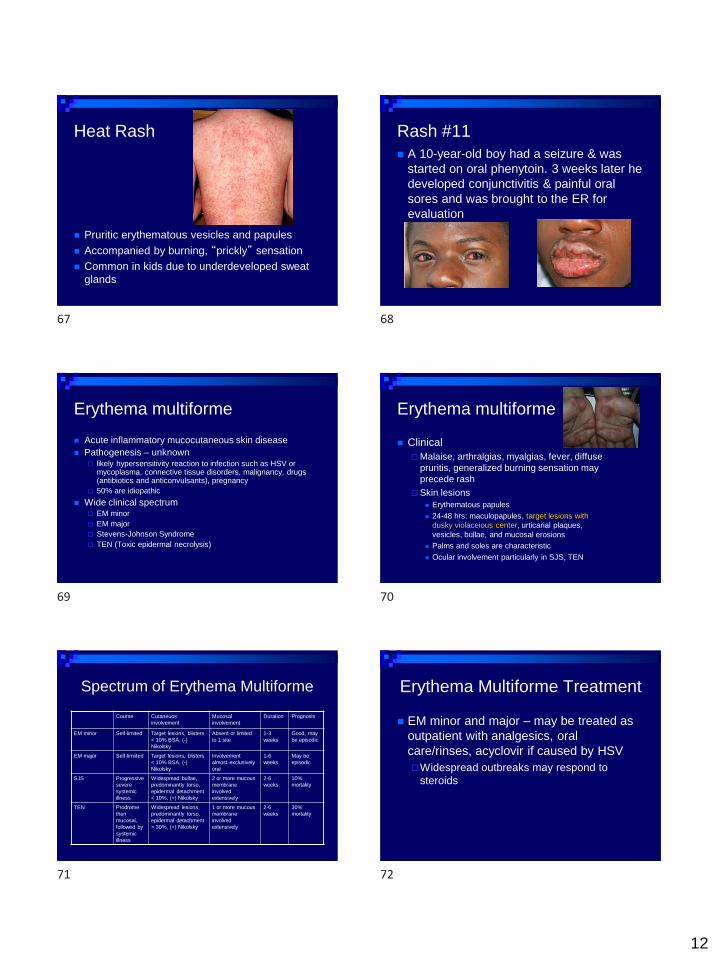
Heat Rash
◼ Pruritic erythematous vesicles and papules
◼ Accompanied by burning, “prickly” sensation
◼ Common in kids due to underdeveloped sweat
glands
Rash #11
◼ A 10-year-old boy had a seizure & was
started on oral phenytoin. 3 weeks later he
developed conjunctivitis & painful oral
sores and was brought to the ER for
evaluation
Erythema multiforme
◼ Acute inflammatory mucocutaneous skin disease
◼ Pathogenesis – unknown likely hypersensitivity reaction to infection such as HSV or
mycoplasma, connective tissue disorders, malignancy, drugs (antibiotics and anticonvulsants), pregnancy
50% are idiopathic
◼ Wide clinical spectrum EM minor
EM major
Stevens-Johnson Syndrome
TEN (Toxic epidermal necrolysis)
Erythema multiforme
◼ Clinical
Malaise, arthralgias, myalgias, fever, diffuse
pruritis, generalized burning sensation may
precede rash
Skin lesions
◼ Erythematous papules
◼ 24-48 hrs: maculopapules, target lesions with
dusky violaceious center, urticarial plaques,
vesicles, bullae, and mucosal erosions
◼ Palms and soles are characteristic
◼ Ocular involvement particularly in SJS, TEN
Spectrum of Erythema Multiforme
Course Cutaneuos
involvement
Mucosal
involvement
Duration Prognosis
EM minor Self-limited Target lesions, blisters
< 10% BSA, (-)
Nikolsky
Absent or limited
to 1 site
1-3
weeks
Good, may
be episodic
EM major Self-limiited Target lesions, blisters
< 10% BSA, (-)
Nikolsky
Involvement
almost exclusively
oral
1-6
weeks
May be
episodic
SJS Progressive
severe
systemic
illness
Widespread bullae,
predominantly torso,
epidermal detachment
< 10%, (+) Nikolsky
2 or more mucous
membrane
involved
extensively
2-6
weeks
10%
mortality
TEN Prodrome
then
mucosal,
followed by
systemic
illness
Widespread lesions,
predominantly torso,
epidermal detachment
> 30%, (+) Nikolsky
1 or more mucous
membrane
involved
extensively
2-6
weeks
30%
mortality
Erythema Multiforme Treatment
◼ EM minor and major – may be treated as
outpatient with analgesics, oral
care/rinses, acyclovir if caused by HSV
Widespread outbreaks may respond to
steroids
67 68
69 70
71 72

13
Stevens-Johnson Syndrome
◼ Symmetric severe vesicobullous eruption
◼ Affects at least 2 mucous membranes
◼ 5-10% mortality rate
Stevens-Johnson Syndrome
◼ History of Illness
1-3 week prodrome of fever, malaise,
mayalgias
Usually in children and young adults
Commonly caused by HSV, mycoplasma or
drugs
Stevens Johnson Syndrome
◼ Physical Findings
Rash lesions vary from erythematous
papules, vesicles, to target lesions
Bullae erode resulting in gray-yellow fibrinous
exudates with thick hemorrhagic crusts
Ocular changes – conjunctivitis, bullae,
corneal ulcers, and uveitis
Stevens Johnson Syndrome
◼ Physical Findings
Mostly on extremities, but may spread to face
and trunk
Fever – 3%
Pneumonitis – 23%
Bronchitis – 6%
Stevens Johnson Treatment
◼ Supportive care
◼ Ophthalmology consult
◼ Self limited disease
◼ 10% mortality for extensive disease
Toxic Epidermal Necrolysis
◼ Exfoliative disease that affects 30-100% of
BSA
◼ High mortality
◼ 80% are secondary to drugs
Dilantin, barbs, tegretol, sulfa, PCN, &
NSAIDS
Other causes include vaccines, TB, & viruses
73 74
75 76
77 78
14
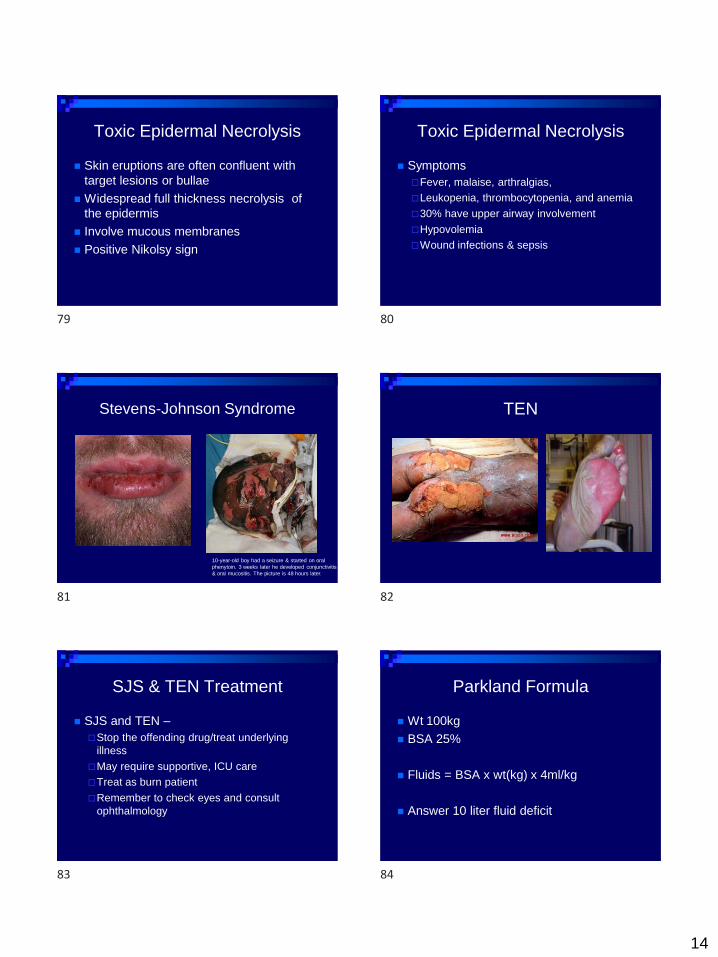
Toxic Epidermal Necrolysis
◼ Skin eruptions are often confluent with
target lesions or bullae
◼ Widespread full thickness necrolysis of
the epidermis
◼ Involve mucous membranes
◼ Positive Nikolsy sign
Toxic Epidermal Necrolysis
◼ Symptoms
Fever, malaise, arthralgias,
Leukopenia, thrombocytopenia, and anemia
30% have upper airway involvement
Hypovolemia
Wound infections & sepsis
Stevens-Johnson Syndrome
10-year-old boy had a seizure & started on oral
phenytoin. 3 weeks later he developed conjunctivitis
& oral mucositis. The picture is 48 hours later.
TEN
SJS & TEN Treatment
◼ SJS and TEN –
Stop the offending drug/treat underlying
illness
May require supportive, ICU care
Treat as burn patient
Remember to check eyes and consult
ophthalmology
Parkland Formula
◼ Wt 100kg
◼ BSA 25%
◼ Fluids = BSA x wt(kg) x 4ml/kg
◼ Answer 10 liter fluid deficit
79 80
81 82
83 84

15
Rash #12
◼ 23 y.o. female
presents with a
painless rash. She
is otherwise healthy
but mentioned that
she had a cold a
couple weeks ago.
Pityriasis Rosea
◼ Oval shaped salmon colored papules or plaques on the trunk & proximal extremities with a red halo
◼ Herald patch and Christmas tree pattern
◼ Children and young adults
◼ Resolves in weeks to months
Rash #13
26 y.o. female with a
history of sarcoid
presents with a
history of a week of
myalgias and a
fever. Today noticed
a painful rash on her
bilateral shins
Erythema Nodosum
◼ Inflammatory/immunologic reaction
◼ Women 15-30 y.o.
◼ Deep painful nodules on the lower extremities
◼ Bilateral but not symmetric
◼ Tender to palpation
◼ Preceded by fever, malaise, & arthralgias
◼ Causes: Infection, Drugs, Cancers, Sarcoid/IBD, Pregnancy
◼ Self limited if the cause can be eliminated
Rash #14
7 y.o. male presents for
severe abdominal pain.
Parents say that he had
jaundice at birth but no
other health problems. He is
fully immunized and takes
no medications. A week
ago he had a runny nose
but they otherwise deny any
constitutional symptoms.
On exam you completely
undress the boy and see
this rash
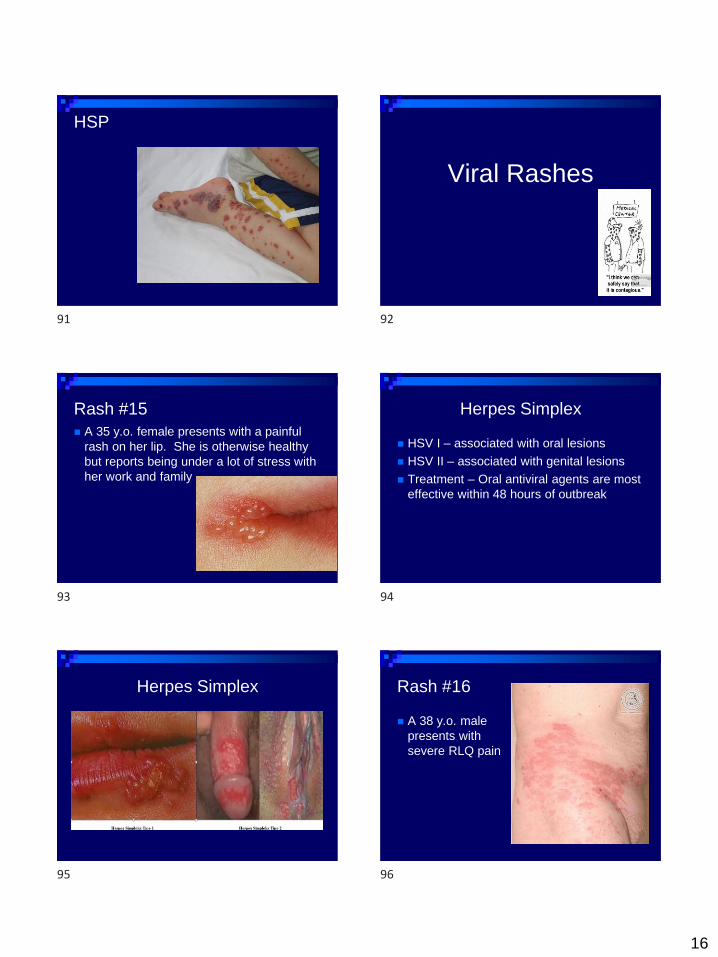
Henoch-Schonlein Purpura
◼ Systemic vasculitis that causes palpable purpura
◼ Usually follows an upper respiratory infection
◼ 90% of cases occur in children <10 y.o.
◼ Triad – purpura, joint pain, and abdominal pain
◼ Purpura is usually located on the legs and buttocks
◼ 40% of cases involve the kidneys Hematuria, proteinuria, and some will have nephrotic
syndrome
85 86
87 88
89 90
16
HSP
Viral Rashes
Rash #15
◼ A 35 y.o. female presents with a painful
rash on her lip. She is otherwise healthy
but reports being under a lot of stress with
her work and family
Herpes Simplex
◼ HSV I – associated with oral lesions
◼ HSV II – associated with genital lesions
◼ Treatment – Oral antiviral agents are most
effective within 48 hours of outbreak
Herpes Simplex Rash #16
◼ A 38 y.o. male
presents with
severe RLQ pain
91 92
93 94
95 96

17
Shingles/Herpes Zoster
- Reactivation of latent varicella zoster
- 10-20% Incidence
- Triggers – age, immunosuppression, fatigue, stress- Patient’s with Hodgkin’s disease are uniquely susceptible
- May have constitutional symptoms of fever, HA, & malaise prior to the rash
Herpes Zoster
Shingles- Starts as pain and paresthesias in a dermatomal
distribution 3-5 days prior to rash
- Herpetiform clusters of vesicles on an erythematous edematous base
- Hutchinson’s sign – lesions on the tip of the nose can signal eye involvement
- Ramsay Hunt Syndrome – Lesions in the ear canal associated with facial palsy
- Treatment – analgesics and antivirals
Shingles Ophthalmic Zoster
◼ 10-20% of all zoster cases
◼ 72% develop ocular complications
◼ Hutchinson’s sign
Zoster Diagnosis and Treatment
◼ Tzank smear shows multinucleated giant
cells
◼ Oral antivirals – most effective in the first
48hours
◼ Sympathetic blocks with bupivicaine may
help the pain of acute zoster
Postherpetic Neuralgia
◼ Incidence and duration of pain increases
with age
◼ Patients over 60 may benefit from Elavil or
Neurontin
97 98
99 100
101 102
18
Rash #17◼ 4 y.o. female is brought
into the ER for a fever
and rash. Mom reports
that the child has had a
cough, runny nose, and
increasing fever over the
last 3 days. This morning
the child woke up with a
rash and mom became
concerned.
◼ PMHx: NSVD, no health
problems
◼ Rx: none
Social Hx: lives at home
with 5y.o. brother and pet
dog
◼ Immunizations: None
◼ Vitals: T 39, RR 20, HR
120
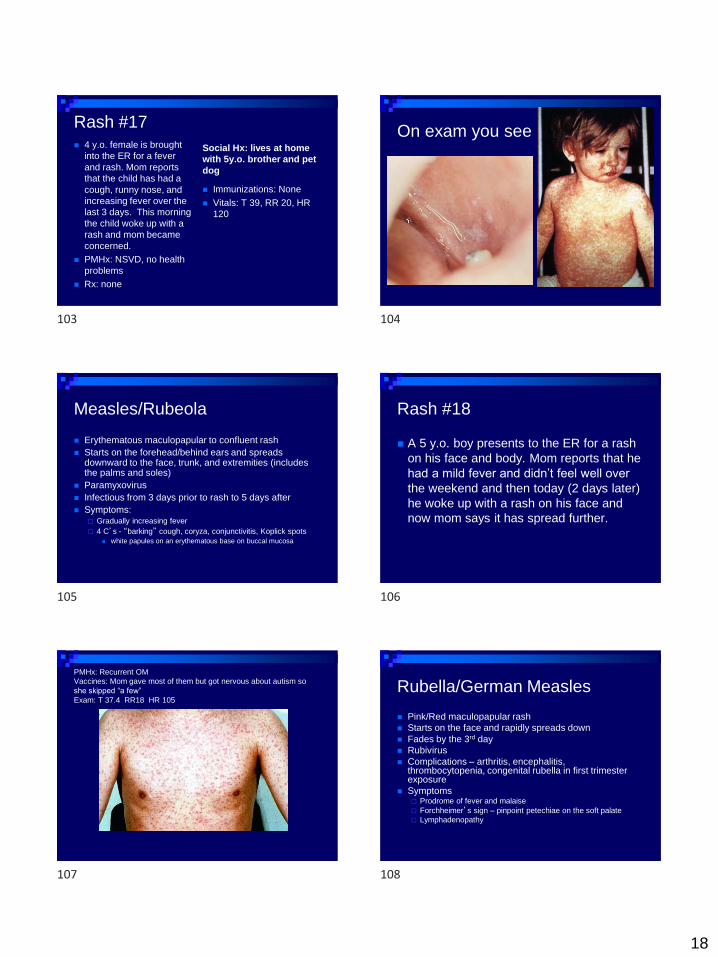
On exam you see
Measles/Rubeola
◼ Erythematous maculopapular to confluent rash
◼ Starts on the forehead/behind ears and spreads downward to the face, trunk, and extremities (includes the palms and soles)
◼ Paramyxovirus
◼ Infectious from 3 days prior to rash to 5 days after
◼ Symptoms: Gradually increasing fever
4 C’s - “barking” cough, coryza, conjunctivitis, Koplick spots
◼ white papules on an erythematous base on buccal mucosa
Rash #18
◼ A 5 y.o. boy presents to the ER for a rash
on his face and body. Mom reports that he
had a mild fever and didn’t feel well over
the weekend and then today (2 days later)
he woke up with a rash on his face and
now mom says it has spread further.
PMHx: Recurrent OM
Vaccines: Mom gave most of them but got nervous about autism so
she skipped “a few”
Exam: T 37.4 RR18 HR 105
Rubella/German Measles
◼ Pink/Red maculopapular rash
◼ Starts on the face and rapidly spreads down
◼ Fades by the 3rd day
◼ Rubivirus
◼ Complications – arthritis, encephalitis, thrombocytopenia, congenital rubella in first trimester exposure
◼ Symptoms Prodrome of fever and malaise
Forchheimer’s sign – pinpoint petechiae on the soft palate
Lymphadenopathy
103 104
105 106
107 108

19
Rash #19
◼ 3 y.o. female brought to the EC for a high
fever for 4 days that persists in spite of
Tylenol and Motrin
◼ The child is otherwise healthy, immunized,
and behaving normally
ExamVitals:
T 39.6 RR 18 HR 131
Roseola
◼ High fever for 3-4 days in a well-appearing
child followed by rash
◼ Blanching rose colored macular to
maculopapular rash that starts on the
trunk and spreads outward
◼ Human herpes virus 6 & 7
◼ Usually in kids 6 months to 3 years
Rash #20
◼ 6 y.o. male presents with a mild fever and
malaise and a rash on his cheeks.
Erythema Infectiosum/
Fifth’s Disease
◼ Bright red malar rash - “slapped cheek” -
followed in 2 days by an erythematous
maculopapular rash on the trunk and limbs
◼ Central fading leads to a lacy pattern
◼ Parvovirus B19
◼ No longer contagious once rash appears
◼ Can cause hydrops fetalis in pregnancy or
aplastic crisis in hemolytic anemias
Fifth’s Disease
109 110
111 112
113 114
20
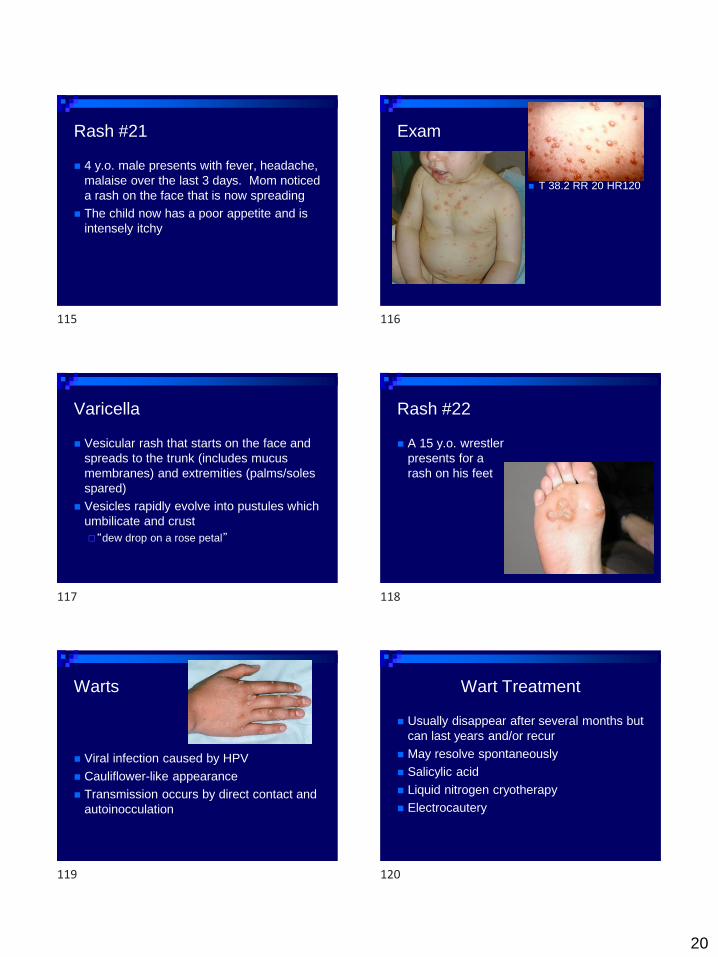
Rash #21
◼ 4 y.o. male presents with fever, headache,
malaise over the last 3 days. Mom noticed
a rash on the face that is now spreading
◼ The child now has a poor appetite and is
intensely itchy
Exam
◼ T 38.2 RR 20 HR120
Varicella
◼ Vesicular rash that starts on the face and
spreads to the trunk (includes mucus
membranes) and extremities (palms/soles
spared)
◼ Vesicles rapidly evolve into pustules which
umbilicate and crust
“dew drop on a rose petal”
Rash #22
◼ A 15 y.o. wrestler
presents for a
rash on his feet
Warts
◼ Viral infection caused by HPV
◼ Cauliflower-like appearance
◼ Transmission occurs by direct contact and
autoinocculation
Wart Treatment
◼ Usually disappear after several months but
can last years and/or recur
◼ May resolve spontaneously
◼ Salicylic acid
◼ Liquid nitrogen cryotherapy
◼ Electrocautery
115 116
117 118
119 120
21
Rash #23
◼ 10 y.o. female brought
to the ER by her mom
who is frustrated that
she has had a rash for
4 months
◼ Occasionally itchy but
no other symptoms
◼ She is fully vaccinated
and otherwise healthy
Molluscum Contagiosum
◼ A viral infection of the skin and occasionally mucous membranes
◼ Most commonly on the trunk/arms/legs
◼ DNA poxvirus
◼ Spread from person to person via direct contact
◼ Most common in children one – 11 y.o.
◼ Contagious until the lesions are gone
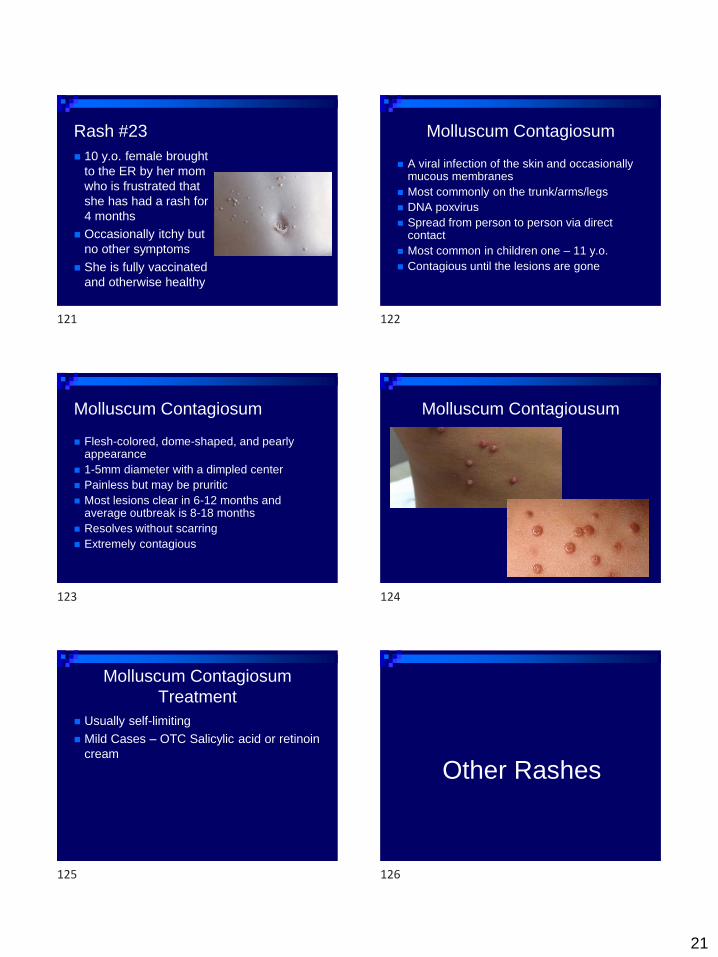
Molluscum Contagiosum
◼ Flesh-colored, dome-shaped, and pearly appearance
◼ 1-5mm diameter with a dimpled center
◼ Painless but may be pruritic
◼ Most lesions clear in 6-12 months and average outbreak is 8-18 months
◼ Resolves without scarring
◼ Extremely contagious
Molluscum Contagiousum
Molluscum Contagiosum
Treatment
◼ Usually self-limiting
◼ Mild Cases – OTC Salicylic acid or retinoin
cream
Other Rashes
121 122
123 124
125 126
22
Rash #24
◼ 72 y.o. female presents
for a painful rash on her
cheek. She reports 2
days of a fever, poor
appetite, and malaise
◼ T 38.7 RR 18 HR 117
98% RA
PMHx: DM, HTN
Erysipelas
◼ Painful, shiny, erythematous plaques with raised
and sharply demarcated borders
◼ Form of cellulitis and favors extremities
◼ Group A strep
◼ Usually occurs in young kids and the elderly
◼ Associated with high fever, chills, & anorexia
◼ Treatment: PCN, E-mycin, or Clindamycin
Rash #25
◼ 25 y.o. female presents for a painful rash
on her finger and joint pain
◼ PMHx: Asthma, genital warts
◼ Social Hx: +tob, social Etoh, works at a
gentleman’s club as a dancer
Disseminated gonococcal infection
◼ Clinical
Fever
Classic triad
◼ 1. migratory arthralgias
◼ 2. tenosynovitis (usually fingers)
◼ 3. dermatitis
multiple papular, vesicular, or pustular skin lesions (usually
initially small papules or macules that evolve to pustules),
often on extremities
*6 million new gonorrhea infections yearly in US. 3% cases may become disseminated.
Up to 75% of those diagnosed with disseminated disease are females in late pregnancy,
immediate post-partum, or within 1 week of onset of menses.
Disseminated gonococcal infection
◼ Diagnosis
Gram stain or culture of
blood or lesions reveals
Neisseria gonorrhoeae
◼ Treatment
Begin parenteral treatment
with ceftriaxone –
quinolones should be
avoided in certain regions
due to resistance
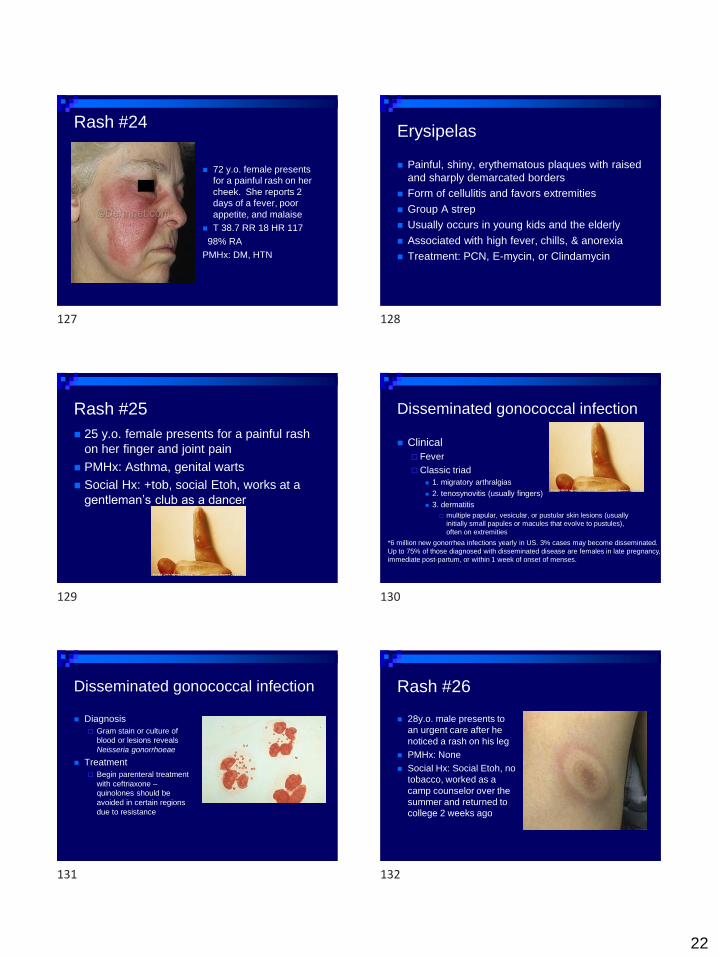
Rash #26
◼ 28y.o. male presents to
an urgent care after he
noticed a rash on his leg
◼ PMHx: None
◼ Social Hx: Social Etoh, no
tobacco, worked as a
camp counselor over the
summer and returned to
college 2 weeks ago
127 128
129 130
131 132

23
Lyme Disease
◼ Tick born disease
◼ Early localized disease has a circular outwardly
expanding rash – erythema chronicum migrans
– at the site of the tick bite
◼ Occurs 3-30 days after bite
◼ Associated with flu-like symptoms
◼ Treatment – Doxycycline or Amoxicillin for 10-28
days
Rash #27
◼ 8 y.o. male presents to the ER for fever,
malaise, headache, and nausea. Mom
reports that he hasn’t felt well since they
returned from a hiking trip in Virginia a
week ago
Rocky Mountain Spotted Fever
◼ Epidemiology
Rickettsia rickettsii
transmitted to humans by
wood ticks and dog ticks
All US states except AK, HI
90% patients infected April
to Sept
Half of cases from S.
Atlantic states
>60% history of tick bite
Peak age 5 to 9 years old
Rocky Mountain Spotted Fever
◼ Initial symptoms 5-7 days after inoculation Fever – only universal sx
Nausea, vomiting
Frontal headache
Myalgias
Anorexia
Light macules on distal extremities/palmar surfaces
◼ Later symptoms Petechial rash spread
towards trunk
Abdominal pain
Joint pain
◼ Extreme gastrocnemius
tenderness may be a clue
Diarrhea
CNS, renal, and respiratory
failure
Rocky Mountain Spotted Fever
◼ Diagnosis is clinical 1. Fever 2. HA 3. Rash
◼ Lab findings Low sodium and platelets
Elevated liver enzymes
◼ Treatment Supportive
Doxycycline or chloramphenicol – begin prior to lab confirmation of diagnosis!◼ High mortality rate due to late/missed diagnosis
Rash #28
◼ A 22 y.o. male presents complaining of an
intensely itchy rash on his hands that
seems worse at night.
133 134
135 136
137 138
24
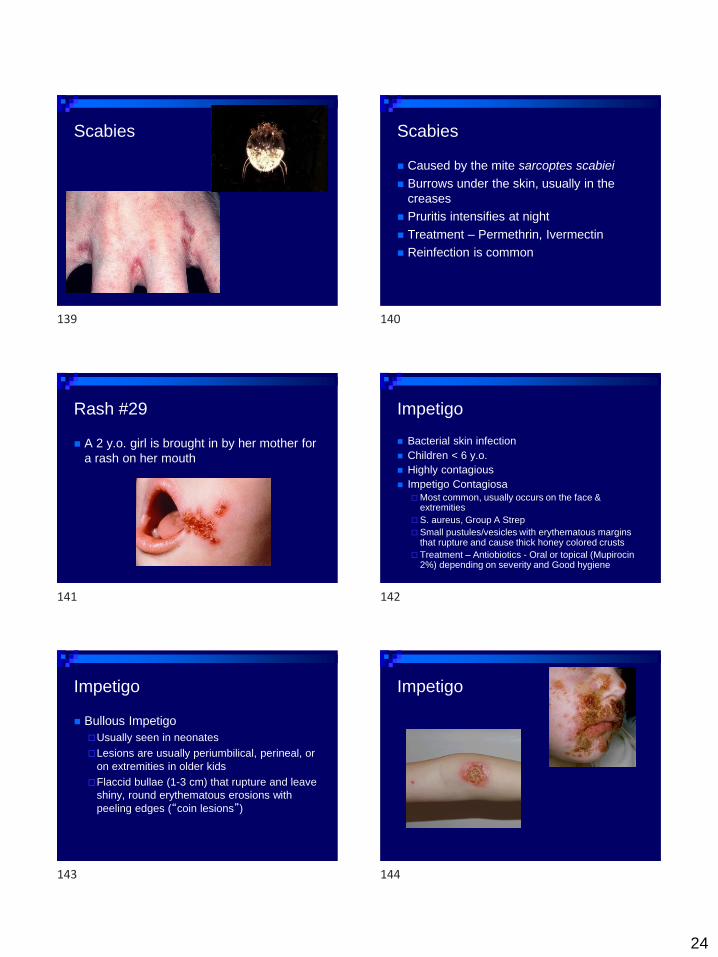
Scabies Scabies
◼ Caused by the mite sarcoptes scabiei
◼ Burrows under the skin, usually in the
creases
◼ Pruritis intensifies at night
◼ Treatment – Permethrin, Ivermectin
◼ Reinfection is common
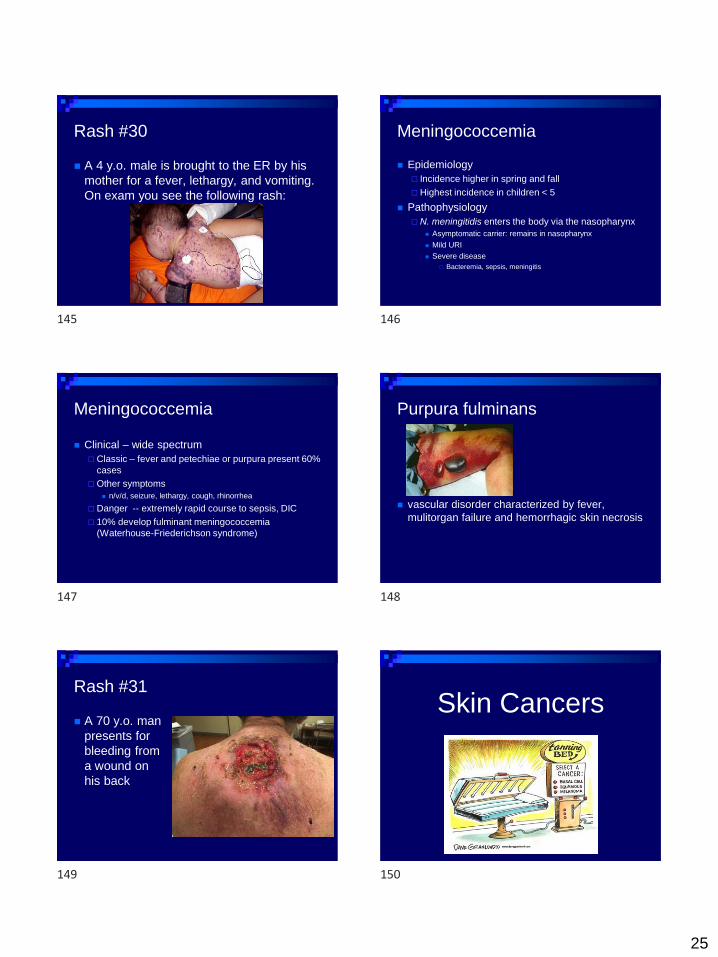
Rash #29
◼ A 2 y.o. girl is brought in by her mother for
a rash on her mouth
Impetigo
◼ Bacterial skin infection
◼ Children < 6 y.o.
◼ Highly contagious
◼ Impetigo Contagiosa
Most common, usually occurs on the face & extremities
S. aureus, Group A Strep
Small pustules/vesicles with erythematous margins that rupture and cause thick honey colored crusts
Treatment – Antiobiotics - Oral or topical (Mupirocin2%) depending on severity and Good hygiene
Impetigo
◼ Bullous Impetigo
Usually seen in neonates
Lesions are usually periumbilical, perineal, or
on extremities in older kids
Flaccid bullae (1-3 cm) that rupture and leave
shiny, round erythematous erosions with
peeling edges (“coin lesions”)
Impetigo
139 140
141 142
143 144
25
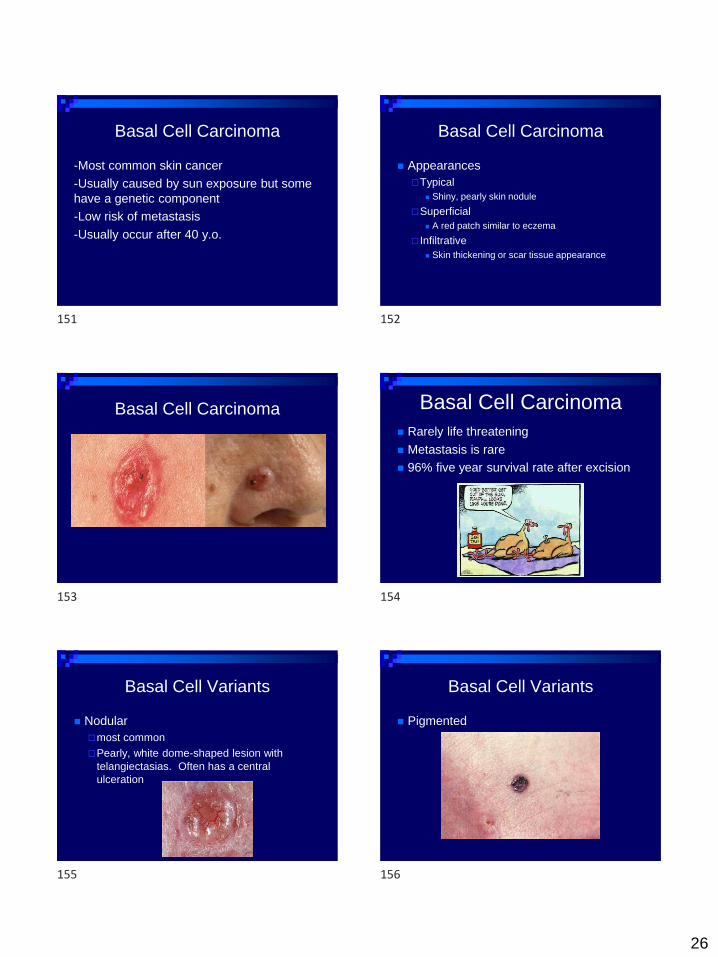
Rash #30
◼ A 4 y.o. male is brought to the ER by his
mother for a fever, lethargy, and vomiting.
On exam you see the following rash:
Meningococcemia
◼ Epidemiology
Incidence higher in spring and fall
Highest incidence in children < 5
◼ Pathophysiology
N. meningitidis enters the body via the nasopharynx
◼ Asymptomatic carrier: remains in nasopharynx
◼ Mild URI
◼ Severe disease
Bacteremia, sepsis, meningitis
Meningococcemia
◼ Clinical – wide spectrum
Classic – fever and petechiae or purpura present 60%
cases
Other symptoms
◼ n/v/d, seizure, lethargy, cough, rhinorrhea
Danger -- extremely rapid course to sepsis, DIC
10% develop fulminant meningococcemia
(Waterhouse-Friederichson syndrome)
Purpura fulminans
◼ vascular disorder characterized by fever,
mulitorgan failure and hemorrhagic skin necrosis
Rash #31
◼ A 70 y.o. man
presents for
bleeding from
a wound on
his back
◼ Skin caSkin Cancers
145 146
147 148
149 150
26
Basal Cell Carcinoma
-Most common skin cancer
-Usually caused by sun exposure but some
have a genetic component
-Low risk of metastasis
-Usually occur after 40 y.o.
Basal Cell Carcinoma
◼ Appearances
Typical
◼ Shiny, pearly skin nodule
Superficial
◼ A red patch similar to eczema
Infiltrative
◼ Skin thickening or scar tissue appearance
Basal Cell Carcinoma Basal Cell Carcinoma
◼ Rarely life threatening
◼ Metastasis is rare
◼ 96% five year survival rate after excision
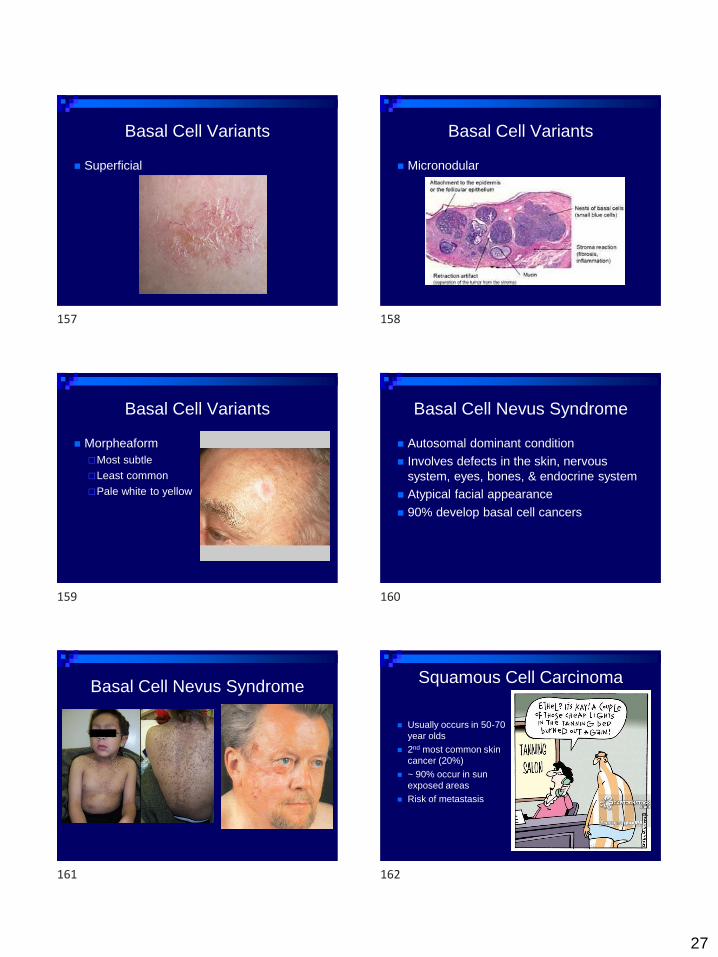
Basal Cell Variants
◼ Nodular
most common
Pearly, white dome-shaped lesion with
telangiectasias. Often has a central
ulceration
Basal Cell Variants
◼ Pigmented
151 152
153 154
155 156
27
Basal Cell Variants
◼ Superficial
Basal Cell Variants
◼ Micronodular
Basal Cell Variants
◼ Morpheaform
Most subtle
Least common
Pale white to yellow
Basal Cell Nevus Syndrome
◼ Autosomal dominant condition
◼ Involves defects in the skin, nervous
system, eyes, bones, & endocrine system
◼ Atypical facial appearance
◼ 90% develop basal cell cancers
Basal Cell Nevus Syndrome
◼ Basal_cell_nevus_sye
Squamous Cell Carcinoma
◼ Usually occurs in 50-70
year olds
◼ 2nd most common skin
cancer (20%)
◼ ~ 90% occur in sun
exposed areas
◼ Risk of metastasis
157 158
159 160
161 162
28
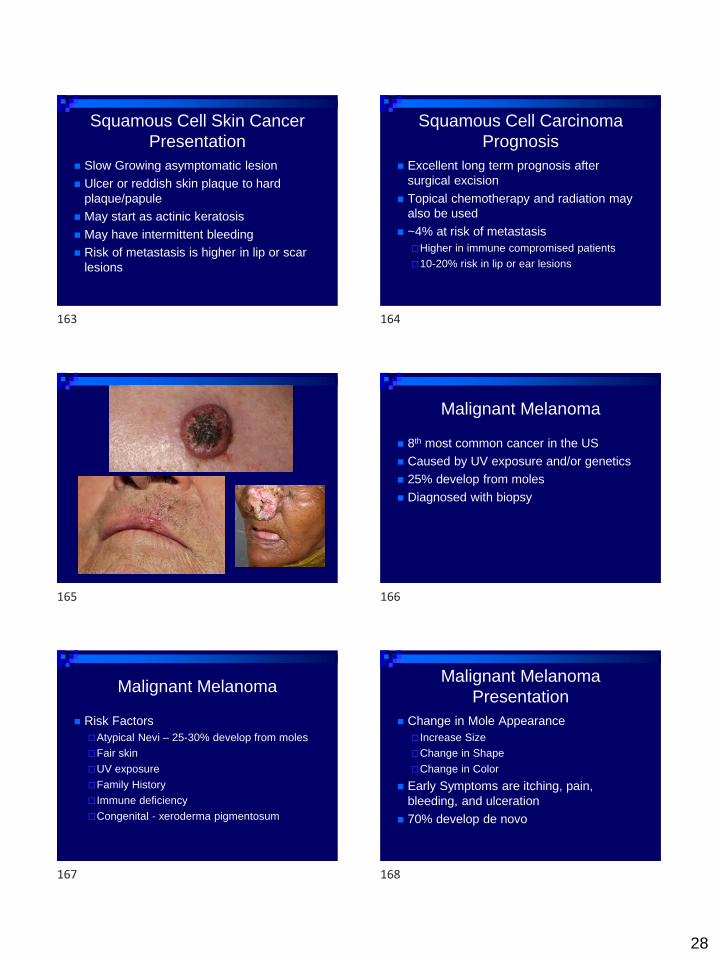
Squamous Cell Skin Cancer
Presentation
◼ Slow Growing asymptomatic lesion
◼ Ulcer or reddish skin plaque to hard
plaque/papule
◼ May start as actinic keratosis
◼ May have intermittent bleeding
◼ Risk of metastasis is higher in lip or scar
lesions
Squamous Cell Carcinoma
Prognosis
◼ Excellent long term prognosis after
surgical excision
◼ Topical chemotherapy and radiation may
also be used
◼ ~4% at risk of metastasis
Higher in immune compromised patients
10-20% risk in lip or ear lesions
Malignant Melanoma
◼ 8th most common cancer in the US
◼ Caused by UV exposure and/or genetics
◼ 25% develop from moles
◼ Diagnosed with biopsy
Malignant Melanoma
◼ Risk Factors
Atypical Nevi – 25-30% develop from moles
Fair skin
UV exposure
Family History
Immune deficiency
Congenital - xeroderma pigmentosum
Malignant Melanoma
Presentation
◼ Change in Mole Appearance
Increase Size
Change in Shape
Change in Color
◼ Early Symptoms are itching, pain,
bleeding, and ulceration
◼ 70% develop de novo
163 164
165 166
167 168

29
Malignant Melanoma
◼ ABC’s
Asymmetry
Border Irregularity – may have edges or corners
Color Variation
Diameter - >6mm
Evolving over time/Elevated above skin surface
Firm to Touch
Growing
Malignant Melanoma Subtypes
◼ Superficial Spreading
Most common
Occur on the trunk or extremities
Usually develop from a prior mole
Has a prolonged radial growth phase prior to
vertical growth
Superficial Spreading
MelanomaNodular Melanoma
◼ Most aggressive form of melanoma
◼ 10-15% of melanoma
◼ Grows rapidly in thickness
◼ Often grows de novo instead of from an
existing mole
◼ Raised and darkly pigmented
Nodular Melanoma Lentigo Maligna Melanoma
◼ Found on chronically sun damaged skin
◼ 5-10% of all melanomas
◼ Darkly pigmented flat brown/black lesion
◼ Occurs on face or arms, often in the elderly
◼ Lentigo maligna
non-invasive skin growth considered to be melanoma-in-situ vs a melanoma precursor
LMM is invasive
169 170
171 172
173 174

30
Lentigo Maligna
Lentigo Maligna MelanomaAcral Lentiginous Melanoma
◼ ~7% of all melanomas
◼ Average age is 60-70 y.o.
◼ Most common melanoma in Asians and
African Americans
◼ Similar appearance to LMM
◼ Typically occurs on the hands & feet
Acral Lentiginous Melanoma Amelanotic Melanoma
◼ Non-pigmented
◼ 2% of all cases
◼ Often diagnosed later in the course
Amelanotic Melanoma Melanoma Prognosis
◼ Depends on depth
◼ Females and young adults do better
◼ Extremity lesions have a better prognosis
than trunk, head, or neck lesions
The scalp has the worst prognosis
175 176
177 178
179 180
















![Itchy Anus [Voice + Piano]](https://img.pdfslide.us/doc/110x75/577ccfc11a28ab9e7890800c/itchy-anus-voice-piano.jpg)









