Embed Size (px)
Citation preview

8/17/18
1
Jonathan A. Dyer, MD Associate Professor of
Dermatology and Child Health University of Missouri
Dermatological Findings in the Aging Population
Acknowledgements
• Dr. Kristen Heinz Fernandez
Geriatric Dermatology: What’s all the fuss about? Geriatric Dermatology: What’s all
the fuss about?
“The great majority of persons over 70 have at least one, often two or three, skin conditions which would benefit from the attentions of a knowledgeable doctor..” Albert M. Kligman, MD, foreword to Skin and Aging Processes, Barbara Gilchrest, MD
Changes in skin with aging
• Senescence related
• Environmental • Internal/ External
• Actinic purpura
• Skin fragility
• Stellate pseudoscarring

8/17/18
2
Most Common Dermatological Diagnoses: Geriatric Dermatology
• Unpublished data - University of Iowa Dermatology Clinic – January-December 2008
• Most common diagnoses patients >65 y/o 1. Actinic keratoses 2. Other dermatoses 3. Basal Cell Carcinoma or Squamous Cell Carcinoma 4. Benign neoplasm
Most Common Dermatological Diagnoses: Geriatric Dermatology
• Nursing home dermatology diagnoses (n=1,556)
Diagnosis N Mean age (years)
Scabies 220 78.0 (14.7) Contact dermatitis and other eczema 218 77.1 (14.3) Erythematosquamous dermatitis 216 75.6 (16.5) Disorders of the sweat glands 166 78.3 (14.0) Nonthrombocytopenic purpura 145 84.8 (8.0) Stasis dermatitis with varicosities 135 81.3 (11.3) Candidiasis 80 80.5 (13.3) Cellulitis, unspecified site 77 79.3 (14.1) Dermatophytosis 71 78.4 (14.4) Other hypertrophic and atrophic conditions of the skin 47 83.9 (18.1)
NormanR, ed. Geriatric Dermatology. New York: Parthenon, 2001: 5–16.
U. of Iowa Dermatology Clinic Nursing Home Visits
• Actinic keratoses • Other dermatoses • Basal or squamous cell
carcinoma of the skin • Benign neoplasm
• Pruritus and other related diseases
• Diseases of the sebaceous glands (xerosis)
• Other dermatoses • Basal or squamous cell
carcinoma of the skin
Most Common Dermatological Diagnoses: Geriatric Dermatology
U. of Iowa Dermatology Clinic Nursing Home Visits
• Actinic keratoses • Other dermatoses • Basal or squamous cell
carcinoma of the skin • Benign neoplasm
• Pruritus and other related diseases
• Diseases of the sebaceous glands (xerosis)
• Other dermatoses • Basal or squamous cell
carcinoma of the skin
Most Common Dermatological Diagnoses: Geriatric Dermatology
U. of Iowa Dermatology Clinic Nursing Home Visits
• Actinic keratoses • Other dermatoses • Basal or squamous cell
carcinoma of the skin • Benign neoplasm
• Pruritus and other related diseases
• Diseases of the sebaceous glands (xerosis)
• Other dermatoses • Basal or squamous cell
carcinoma of the skin
Most Common Dermatological Diagnoses: Geriatric Dermatology Agenda
• “Other dermatoses” – Xerosis
• Asteatotic eczema • Nummular eczema
– Pruritus – Causes of itch* • Bullous pemphigoid • Actinic keratoses and Skin Cancer

8/17/18
3
Xerosis • Ranges from dry skin to true dermatitis:
– Asteatotic eczema – Nummular eczema
Asteatotic Eczema • Pruritic, dry, cracked, polygonally fissured
skin with irregular scaling – Shins – Elderly patients – May occur on the hands and trunk
• Appears similar to: – cracked porcelain – dried-up riverbed
• Pathogenesis: 1. The elderly have decreased sebaceous and
sweat gland activity 2. Loss of stratum corneum lipids = increased
transepidermal water loss 3. Stratum corneum loses water = cells shrink =
fissures 4. Fissures rupture dermal capillaries, causing
clinical bleeding Emedicine.com
Nummular Eczema • Nummular ="coin-shaped“ • Round/oval erythematous
plaques • Mostly arms and legs • Early lesions may be
studded with vesicles containing serous exudate
• Very pruritic • Peaks in 6th-7th decade
Asteatotic and Nummular Eczema: Treatment
• Rehydrate skin and repair epidermal lipid barrier à Emollients – Use BID, especially after
bathing/showering – Creams or ointments
preferable to lotions • “Scoop not pump”
• Reduce inflammation à topical steroids when inflamed
Asteatotic and Nummular Eczema: Repair of Epidermal Barrier
• Lukewarm/ cool bath/showers daily – Decrease itching - helps rehydrate skin – MUST follow with moisturizers/ topical medications to seal in.
• Soak and Smear: (handout) – 20-minute plain water soak qHS then steroid ointment/ petrolatum
to wet skin – Soap only to the axilla/ groin – >90% response in 27/28 pts with refractory chronic pruritic
eruptions when used as directed3
• Wet wraps: – Dampen skin with lukewarm water until well hydrated (~10 min) – Petrolatum/ steroid ointment applied liberally, then occlude for 1
hour with damp pajamas • May use plastic wrap for occluding small areas
– May repeat 5-6 times a day with petrolatum – Caution using with prescription steroids –striae/ atrophy
Stasis Dermatitis • Due to underlying
venous stasis – Cyclical edema
• Triggers inflammation – Often symmetric
• Lower extremities – “bilateral cellulitis”
• Treat: topical antiinflammatory + compression

8/17/18
4
Contact Dermatitis Allergic contact dermatitis
• Due to type IV hypersensitivity reaction to external allergen
• Clinical – Patterned rash – Itchy – Chronic
• Patch testing can identify allergen
• Poison Ivy is classic
example
Irritant Contact Dermatitis • Repeated exposure of
skin to irritants – Hand dermatitis from over
washing – Incontinence related
dermatitis • Not a true allergy • Avoidance of irritant is
key to successful treatment
Irritant Contact Dermatitis
• Incontinence related dermatitis – Control incontinence – Frequent changing of pads/absorptive device – Barrier. . . Barrier. . . .Barrier
• Zinc Oxide paste • Stoma barrier creams
– Ilex barrier paste – SensiCare barrier cream
• Cavilon barrier films
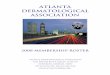
Scabies • Infestation with Sarcoptes
scabiei • Itch is due to immune
reaction to mite • Typical clinical sites:
– Umbilicus – Web spaces – Under nails – Wrists – Axilla – Areolae – Palms/soles in infants
• Nodular lesions may be occur – Genitalia
Crusted scabies
• Massive infestation with mites
• Debilitated patients • Often secondary
infection • Oral therapy
– Ivermectin • Topical

8/17/18
5
Scabies
• Mineral oil scrape – Mites – Eggs – Feces (scyballa)
• Transmission – Close personal
contact • Most infested adults
have < 10 mites – Crusted = Teeming
Scabies • Treatment
– Topical • Permethrin
– Repeat in 1 week to treat unhatched eggs
– Oral • Ivermectin
– Hot water wash and/or heated drying of clothes, sheets, towels
• If not possible – seal tightly in plastic bag for 1 week
– Fumigation is unecessary • Thorough vacuuming is
enough
• All at risk family members/ care providers must be treated at same time
• Nursing Home: – Roommates – Wings – Units – Staff
• Symptoms may persist after treatment – Until immune reaction calms
Seborrheic keratoses
Can be quite pruritic!
Herpes zoster • AKA “Shingles” • May start with itch;
“burning” pain • Typically follows
dermatome – May be multidermatomal – Ocular involvement can
= loss of vision • Can be systemic • Treatment
– Watchful waiting – Oral anti-viral therapy
Pruritus in the Elderly
Sometimes associated with dermatitis, but not always
• International Forum for the Study of Itch (IFSI) Classification of Pruritus5
1. Pruritus on diseased skin 2. Pruritus on non-diseased skin 3. Chronic scratch lesions
Pruritus in the Elderly
Sometimes associated with dermatitis, but not always
• IFSI Classification of Pruritus5
1. Pruritus on diseased skin: asteatotic and nummular eczema
2. Pruritus on non-diseased skin 3. Chronic scratch lesions

8/17/18
6
Pruritus in the Elderly • Pruritus on non-diseased skin
• Metabolic problems – Renal disease, cholestatic pruritus, hematologic pruritus,
endocrine pruritus, pruritus related to malignancy – CBC/ CMP – +/- CXR – Treatment:
» Address underlying disease » Symptom relief:
» Sarna lotion: menthol (0.5%) and camphor (0.5%) » Cool compresses » Antihistamines: be careful of sedation in the elderly!
» Case-by-case basis
• Neuropathic itch
Pruritus in the Elderly • Pruritus on non-diseased skin
• Neuropathic itch – Degenerative joint disease or spinal injury predispose the
elderly – Pruritus sometimes has burning quality – Often involves a neurocutaneous dermatome
Brachioradial pruritus Notalgia paresthetica
Pruritus in the Elderly
• Pruritus on non-diseased skin • Neuropathic itch
– Therapeutic treatment ladder » Capsaicin cream – as tolerated » Topical steroids » Gabapentin » Pregabalin
Pruritus in the Elderly • Chronic scratch lesions
– A secondary process… – Lichen simplex chronicus
• Thickened skin with pronounced skin lines
– Prurigo nodularis • Excoriated thick nodules • Often intermixed with scarring
– Treatment: Break itch/scratch cycle
• Potent topical steroids +/- occlusion; NAC?
Systemic Medications and Eczema/Pruritus
• Chronic use of CCB (>3 months) associated with eczematous dermatitis in the elderly4
• Stopping CCB = resolution of eczematous dermatitis in 68% of patients – Took up to 1 year to see improvement in some
• Statins could decrease SC lipids… – Mostly taken up by the liver after absorption
Agenda
• “Other dermatoses” – Xerosis
• Asteatotic eczema • Nummular eczema
– Pruritus – Causes of itch* • Bullous pemphigoid • Actinic keratoses and Skin Cancer

8/17/18
7
Bullous Pemphigoid • Chronic, autoimmune
blistering skin disease – Widespread, tense bullae
• May favor sites of trauma – +++pruritus – Bullae may develop after
persistent urticarial lesions • Elderly patients
– Avg 65 y/o • Most treated patients remit
in 1.5-7 years
Bullous Pemphigoid
Bullous Pemphigoid: Pathophysiology
• IgG autoantibodies specific for the hemidesmosomal bullous pemphigoid antigens BP230 and BP180
Bullous Pemphigoid: Treatment Typically NOT fatal
(In contrast to pemphigus vulgaris)
• Goals of therapy – Decrease blister formation – Promote healing of blisters/ erosions – Determine the minimal dose of medication
necessary to control
Treatment of Bullous Pemphigoid
Therapeutic Ladder of Treatment • Topical steroid
– Class 1 or 2 – clobetasol/fluocinonide
• Tetracycline antibiotic – Minocycline or doxycycline
• Oral prednisone +/- immunosuppression
Agenda
• “Other dermatoses” – Xerosis
• Asteatotic eczema • Nummular eczema
– Pruritus – Causes of itch* • Bullous pemphigoid • Actinic keratoses and Skin Cancer

8/17/18
8
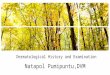
Actinic Keratoses • Elevated, rough patches-
sun-exposed areas (face, bald scalp, lips, and the back of the hands)
• Most red/pink, occ. Tan/ skin colored
• Prevalence of 75% in those 80 to 89 years of age2
• “Pre-skin cancers” – Only 5-8% progression to
SCC over a period of 10 years
– “Sun-damage spots” http://doctorsgates.blogspot.com/2011/07/photo-illustration-of-actinic-keratosis.html
Actinic Keratoses • Elevated, rough patches-
sun-exposed areas (face, bald scalp, lips, and the back of the hands)
• Most red/pink, occ. Tan/ skin colored
• Prevalence of 75% in those 80 to 89 years of age2
• “Pre-skin cancers” – Only 5-8% progression to
SCC over a period of 10 years
– “Sun-damage spots” http://doctorsgates.blogspot.com/2011/07/photo-illustration-of-actinic-keratosis.html
Actinic Keratoses: Treatment • No pain, no gain… • Cryotherapy
– ~99% effective – Best for a limited number
of lesions • Painful • Significant irritation • Risk of scarring
www.webmd.com
Only 5-8% progress to SCC over 10 years
Actinic Keratoses: Treatment • Cryotherapy
– Method: • 1-2 cycles (15-30 second
freeze/thaw cycles), depending on thickness
• Hold cryac container perpendicular 1-2 cm from the lesion
• Must get a 1-2 mm border
Actinic Keratoses:Field Therapy
• Best for multiple lesions (>15)
• Fluorouracil 5% cream – Targets actinically damaged cells – 2-4 weeks of home treatment – Significant irritation
• Varies depending on patient
• Imiquimod 5% cream – Immunomodulator
• On head and neck, can cause flu-like symptoms
• Chemical peels – 35% Tricholoracetic acid (TCA) – Applied in office – 7-10 days of erythema/peeling – Best for thicker skin
• Scalps, foreheads, arms
• Photodynamic Therapy (PDT)
– Topical photosensitizing agent (5-aminolevulinic acid) applied to lesions then area exposed to light to activate 5-ALA
Actinic KeratosesField Therapy
• Chemical peels – 35% Tricholoracetic acid
(TCA) – Applied in office – 7-10 days of erythema/peeling – Best for thicker skin
• Scalps, foreheads, arms
• Photodynamic Therapy (PDT) – Topical photosensitizing agent
(5-aminolevulinic acid), is applied to the lesions, then the area is exposed to strong light that activates 5-ALA.
• Best for multiple lesions (>15)
• Fluorouracil 5% cream – Targets actinically damaged
cells – 2-4 weeks of home treatment – Significant irritation
• Varies depending on patient
• Imiquimod 5% cream – Immunomodulator
• On head and neck, can cause flu-like symptoms

8/17/18
9
Actinic Keratoses: Treatment • Use:
– SUNSCREEN – SUNSCREEN – SUNSCREEN
• SPF >50 • Reapplying every 2 hours
with sun exposure
Actinic cheilitis • High metastatic rate
of SCC of lip (16%) • Low threshold for bx • Tx
– LN2 – Topical retinoid – Efudex – CO2 ablation
Non-melanoma Skin Cancer • Total incidence greater than all other cancer
dx combined • 20% lifetime risk • 45-52% chance of 2nd NMSC within 5 yrs.
after 1st
• BCC-75-80% of NMSCa’s, 0.05% mortality – intermittent light exposure or severe sunburn
before age 18 • SCC-0.7% mortality, 5% metastatic risk
– related to cumulative sun exposure
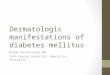
Basal cell carcinoma • Smooth, translucent (pearly), papule with
rolled border and telangiectasia • Ulceration - “rodent ulcer” • Superficial - red, scaly plaque
– Differential: dermatitis/fungus/Bowen’s dz • Morpheic – indurated/ scarlike • Basosquamous – features of BCC &
SCC
BCC - nodular BCC - superficial

8/17/18
10
BCC – Morpheic/Infiltrative Squamous cell carcinoma
• Usually hyperkeratotic, scaly papules or plaques – UV-induced – head/neck/arms – Arsenic – palms/soles – Ionizing radiation – border of field
• Can look like AK’s- close f/u of treated lesions (usually thick/indurated)
• Arising in chronic wounds/burns – “Marjolin’s Ulcer”
SCC SCC
Melanoma • 70% - de novo • Upper back in men / legs in women • Risk factors: a. Numerous nevi b. Family history c. H/O blistering sunburns DEPTH is key! Breslow’s and Ulceration – most
important prognostic indicators
Melanoma - subtypes
• Superficial spreading – most common • Nodular – no radial growth phase • Lentigo maligna melanoma – face of
elderly; large lentigos • Acral lentiginous melanoma – dark skin,
worse prognosis

8/17/18
11
Melanoma Melanoma
Lentigo Maligna Melanoma Acral Lentiginous Melanoma
Treatment
• Early surgical intervention has largest benefit – Melanoma in situ – 0.5cm margins – < 2 mm depth – 1.0 cm margins – 2-4 mm depth – 2.0 cm margins – > 4 mm depth – no randomized studies
• Sentinel lymph nodes for staging
References 1. Book chapter – nursing home 2. Engel A, Johnson ML, Haynes SG. Health effects of sunlight
exposure in the United States. Results from the first National Health and Nutrition Examination Survey, 1971–1974. Arch Dermatol. 1988;124:72–9.
3. Gutman AB, Kligman AM, Sciacca J, James WD. Soak and smear: a standard technique revisited. Arch Dermatol. Dec 2005;141(12):1556-9.
4. Joly et al. Chronic eczematous eruptions of the elderly are associated with chronic exposure to calcium channel blockers: results from a case-control study. J Invest Dermatol. 2007 Dec;127(12):2766-71. Epub 2007 Aug 23.
5. Acta Derm Vener 2007;87:291 6. Pillemer K, Finkelhor D. The prevalence of elder abuse: a
random sample survey. Gerontologist 1988;28:51-7.

8/17/18
12
Thank you for attending!
Jonathan A. Dyer, MD Associate Professor of Dermatology and Child Health
University of Missouri - Columbia 1 Hospital Drive; Room MA111
Columbia, MO. 65212 phone: 573-882-3142 fax: 573-884-5947
E-mail: [email protected]
Please contact me should you have any questions