Embed Size (px)
Citation preview

Derbyshire Community Health ServicesBoard Public Session - 25 January 2018
The Postmill Centre, Market Close, South Normanton, Alfreton DE55 2EJ25 January 2018 13:00 - 25 January 2018 16:00
Overall Page 1 of 218

AGENDA
# Description Owner Time
Developing Services in this Area
1 PART 2 – Public Session
2 INTRODUCTORY ITEMS
3 Introductions and WelcomeVerbal
Prem Singh
4 Apologies for Absence: Chris BentleyVerbal
Prem Singh
5 Declarations of InterestVerbal
Prem Singh
6 Questions from the PublicVerbal
Prem Singh
7 Patient StoryPaper for Information
7 Patient Story.docx 7
Carolyn White
8 Draft Minutes of the meeting held on 30 November 2017Paper for Decision
8 Minutes November 2017.docx 13
Prem Singh
9 Matters ArisingVerbal
Prem Singh
10 Actions MatrixPaper for Information
10 Actions Matrix - public session.docx 25
Prem Singh
11 Chairman’s ReportVerbal
Prem Singh
Overall Page 2 of 218

# Description Owner Time
12 STRATEGY, VALUES AND VISION
13 Chief Executive’s ReportPaper for Information
13 Chief Execs Report.docx 27
Tracy Allen
14 Quality Improvement and Outstanding Way UpdatePaper for Information and Assurance
14 QI and OW Update.docx 37
Jim Austin
15 QUALITY, PERFORMANCE AND GOVERNANCE
16 Quality ReportPaper for Information and Assurance
16 Quality Report.pdf 43
Carolyn White
17 Raising ConcernsPaper for Information and Assurance
17 Raising Concerns.docx 71
Kirsteen Farrar
18 Performance ReportPaper for Information and Assurance
18 Performance Report.pdf 81
Chris Sands
19 Financial Performance ReportPaper for Assurance
19 Financial Performance Report.pdf 107
Chris Sands
20 Board Assurance Framework - Quarter 3Paper for Information, Decision and Assurance
20 BAF Q3.pdf 119
Kirsteen Farrar
21 Quality Service Committee Meeting Summary Report including Annual Report, plus Mortality Review Update
Paper for Assurance
21 QSC Summary Report inc Annual Report.pdf 155
21 Mortality Review Update.docx 173
James Reilly
Overall Page 3 of 218

# Description Owner Time
22 Quality People Committee Meeting Summary ReportPaper for Assurance
22 QPC Summary Report.docx 205
Kaye Burnett
23 Quality Business Committee Meeting Summary ReportPaper for Assurance
23 QBC Summary Report.docx 209
Ian Lichfield
24 Audit and Assurance Committee Meeting Summary ReportPaper for Assurance - to follow
Nigel Smith
25 Council of Governors Summary ReportPaper for Assurance
25 CoG Summary Report Board.docx 213
Prem Singh
26 Mental Health Act Committee Summary ReportPaper for Assurance
26 MHAC Summary Report Nov 2017.docx 217
James Reilly
27 CONCLUDING ITEMS
28 Any Other BusinessVerbal
Prem Singh
29 Self-Certification/Risk/Board Assurance FrameworkVerbal
All
30 Questions from the public relating to today's board businessVerbal
Prem Singh
31 Review of the Meeting and OutcomesVerbal
Prem Singh
32 Date of Next Meeting:Thursday 29 March 2018 at St Thomas’ Church Centre, Chatsworth Road, Chesterfield, S40 3AW. Members of the public and staff are invited to join the Board for an informal discussion over tea and coffee from 12.30pm; this will include a presentation on the services provided in that area. The Public Board meeting will commence at 1.30pm
Overall Page 4 of 218

INDEX
7 Patient Story.docx........................................................................................................................7
8 Minutes November 2017.docx.....................................................................................................13
10 Actions Matrix - public session.docx..........................................................................................25
13 Chief Execs Report.docx...........................................................................................................27
14 QI and OW Update.docx.............................................................................................................37
16 Quality Report.pdf......................................................................................................................43
17 Raising Concerns.docx..............................................................................................................71
18 Performance Report.pdf...........................................................................................................81
19 Financial Performance Report.pdf.............................................................................................107
20 BAF Q3.pdf................................................................................................................................119
21 QSC Summary Report inc Annual Report.pdf...........................................................................155
21 Mortality Review Update.docx....................................................................................................173
22 QPC Summary Report.docx......................................................................................................205
23 QBC Summary Report.docx......................................................................................................209
25 CoG Summary Report Board.docx............................................................................................213
26 MHAC Summary Report Nov 2017.docx...................................................................................217
Overall Page 5 of 218

Overall Page 6 of 218

TRUST BOARDDocument Title: Patient Story
Presenter/Title: Carolyn White, Director of Quality and Chief NurseContents of Paper were previously discussed by:Author/Title: Jody Smith, Community Physiotherapist
Lana-Lee Jackson, Head of Patient & Family Centred CareContact Email and Telephone Number: [email protected]
Date of Meeting: 25 January 2018 AgendaItem No: 7/18
No of pagesinc. this one: 5
Has an Equality Impact Assessment been undertaken Yes No x
Document is for:(more than one box can be ticked) Information x Decision Assurance
Purpose of Paper
This story shows how our patient, Marjorie Edwards, accessed the falls pathway, benefited from the integrated care team approach and how the treatment, rehabilitation and advice she has received has had a positive impact on her lifestyle. Marjorie had a very good experience with DCHS which has translated into maintaining her functional ability, quality of life and confidence.
Falls are predominantly a problem in older age and as the number of older people in the communities we serve increases we are seeing an increase in the number of people experiencing falls and fall-related injuries. Falls have significant human cost to the patient and their family, as well as financial cost to the health and social care system. A fall is a symptom, not a diagnosis. It can be a marker for the onset of frailty, the first indication of a new or worsening health problem and/or can represent a tipping point in a person’s life, triggering a downward decline in independence.
People aged 65 years and over have a 30% risk of falling at least once a year this increases to 50% in those over 80 years. Falls can lead to pain, distress, injury, loss of confidence and even death in some cases. Falls also increase attendances at A&E, admissions to hospital, social care support needs and long-term admissions to residential care homes. With 1 in 3 over 65 year olds falling each year, from Derbyshire’s population, the estimated costs to Derbyshire amount to £49 million with approximately 70,000 falls. At DCHS, falls prevention is a key focus, hence the role of the Falls Prevention Lead and the recent work focusing on developing the Derbyshire Falls Pathway and the pilot project – Managing Falls in Care Homes. All of these promote the benefits of using the multifactorial falls assessment throughout teams which provides a structured approach in assessing a patient who has experienced a fall, and therefore person centred treatment.
The DCHS Integrated Care Team comprises of Physiotherapists, Occupational Therapists and District Nurses working closely alongside Social Workers. Based in the community, we support patients at home who are generally unable to access clinics due to illness, frailty and/or poor mobility. We also manage a specialist falls service providing 1:1 treatments at home as well as
Page 1 of 57 Patient Story.docxOverall Page 7 of 218

leading two community based falls groups each week. The team provide the support planning and therapy for 16 Intermediate Care Beds. As a team we specialise in admission prevention, supported discharge and falls management.
Recommendations
Board are asked to note the positive impact that integrated care and the falls pathway had on Marjorie’s outcomes and experience, as well as the community group post treatment with DCHS, which allows Marjorie to continue to self-manage her conditions.
Board Assurance Framework Risk Reference
N/A
Financial Impact
None
Further Information and Appendices
Marjorie had a fall at her home in May 2017, which was attended by the St Johns Ambulance Falls Team. Marjorie, an 82 year old lady who lives at home with her husband, was referred by her GP into DCHS Integrated Care Team to be assessed for mobility issues, recurrent falls and equipment at home. Marjorie was mobile in her home with a wheeled walker and short distances outside with close support of her husband.
Marjorie has a medical history which includes spinal surgery in 2013 resulting in reduced sensation and reflexes in both her legs. A Transient Ischemic Attack (TIA) in 2007 affected her hearing in her left ear, heart conditions and osteoarthritis, all of which impacted on her mobility and falls. She experienced continual feelings of dizziness since her TIA and feelings of imbalance since her surgery, with 4 falls over the previous year. Marjorie also experienced anxiety and talked about her fear of falling, and of being ‘petrified to move’. The GP had completed a medication review and she was medically stable.
Our Occupational Therapist visited Marjorie at her home, and recognised that she was at moderate risk, in accordance with the Derbyshire Falls Pathway. A full multi-factorial falls assessment was completed. A home and cognitive assessment were also completed on this visit and the required supportive equipment supplied. The Occupational Therapist identified that one of the main contributing factors to Marjorie’s unsteadiness was due to her ongoing dizziness so she was referred to me, requesting a vestibular review as part of the physiotherapy and balance assessment.
Dizziness is a major contributor of falls with prevalence reaching 50% in the over 85 year old population. Due to my clinical interest in falls, I attended a specialist training course for Vestibular Therapy with NCORE last year, funded by DCHS, which has given me the specialist knowledge required to further assess and treat some of the causes of dizziness.
As the most appropriate physiotherapist, I completed strength, balance, and vestibular assessments at home which identified that Marjorie was at high risk of falls, with risks associated in completing functional tasks at home. This was due to dizziness and the feeling of imbalance,
Page 2 of 57 Patient Story.docxOverall Page 8 of 218

poor righting reactions, combined with some left hip weakness which was also impacting on her instability. Marjorie was experiencing low confidence in her own functional ability, and the associated reduced activity level. Marjorie was provided with initial advice and home exercises to address immediate concerns. I identified that part of the dizziness was originating from her vestibular balance system and treated Marjorie accordingly. Marjorie was invited into the falls group, which she attended from August 2017.
The Falls Group is an eight week course using the evidenced based Otago Strength and Balance Training Exercise Programme. The group consists of six patients of varying abilities, all at risk of falls, overseen by Physiotherapists and led on a week to week basis by two experienced Technical Instructors. Ability is measured at the beginning and end of the programme with functional outcome measures to assess both clinical effectiveness and the impact on quality of life. The course also includes education, and discussions around how patients can self-manage and avoid falls at home. At the end of the programme patients are then encouraged to attend the local community exercise groups (‘Strictly No Falling!’) which are funded by Derbyshire County Council and supported by Derbyshire Age UK, to maintain ongoing exercise programmes.
On completion of the course, outcome measures showed that Marjorie gained significant clinical improvement in terms of her mobility and balance, as well as her Quality of Life scores:-
Pre Course Post Course
Improvement
Berg Balance
24/56 42/56 x
Timed Up & Go
30.5 secs with a 3ww
21.3 secswith a 3ww
x
Patient Specific Goal (QoL)
2/10 7/10 x
Marjorie’s FeedbackA thank-you letter was received from Marjorie when she had completed the 8 week falls programme: Dear Madam ‘During the course of the last few months I have been visited at home by several caring people in the Integrated Care Team at Stubley Medical Centre and due to their help and advice I have recently completed an eight week course with the Falls Group at Stubley. I am writing to let you know what a wonderful experience it was.
From the very first day the atmosphere was warm and friendly and as the weeks passed by my confidence grew and the Falls Group became a fun place to be, spent with others who had similar problems and led by physiotherapists who really wanted us to improve. They worked hard keeping us safe, not allowing anyone to say ‘I can’t’, and encouraging everyone to do the best they could, always with a smile, and an amusing remark, but also concern that it was painful or difficult.
My performance was measured at the beginning and at the end, and my results confirmed just
Page 3 of 57 Patient Story.docxOverall Page 9 of 218

how much I have improved. I am left with a wish to continue in the weeks and months ahead.I would like to express my very grateful thanks to everyone involved.’
Yours faithfullyMarjorie Edwards
As the Physiotherapist involved with Marjorie’s assessments and her final outcome measures, I recently returned to review Marjorie three months post group and she has had no further falls. She explained that the group programme provided her with the confidence to address her balance problems so she no longer sees falls as a problem but as a condition to manage. She says ‘I now have a system to avoid falls which enables me to do what I need to do safely. I find it easier to manage my jobs as I have coping strategies in place. I do still get the occasional freeze where my wobbles make me frightened, but rather than being petrified to move in case I fall, which is how I felt before, I can now think logically about how to avoid falling over, and have the confidence to manage the unsteadiness. I am able to cook more, manage better at home and look forward to going out to meet friends again rather than avoiding outings in case I fell. I always have been a very self-conscious person and the falls group made me realise that yes, I can do this! ’
Marjorie still attends a local exercise group in Dronfield every Tuesday with Strictly No Falling!, and she looks forward to the friendships and social aspects that the community group offers, whilst maintaining her physical activity levels. She has been provided with the tools to stop the downward spiral into frailty for the current time, and is actively managing the physical and emotional obstacles, which were causing her mobility problems, enabling an independent active life.
Shared LearningThe importance of integrated working is a key contributor to Marjorie’s success. Our team had an appropriate skill mix to identify, treat and support Marjorie’s conditions, from the original Occupational Therapist’s initial assessment, picking up the falls risk and referring on to Physiotherapist for advanced falls assessment, and the opportunity to benefit from the specialist vestibular knowledge.
The Falls Group being led by well-trained and experienced instructors, who were able to identify and provide the particular support Marjorie needed to thrive in the group environment, she is a very anxious lady and as well as the physical rehabilitation, she received the emotional support required to regain her function, confidence and independence.
In this instance Marjorie needed no carer support, but having the Adult Care Staff in the team would mean an efficient and effective multi-disciplinary assessment of all her needs, the ability to provide re-ablement and that her needs would be regularly assessed and input reduced as her independence improved. This happens with many of our patients: often the patient needs carer support to enable them to regain their function combined with the therapy and/or nursing input.
Marjorie’s story demonstrates that a key strength of the Falls Group is the effectiveness of the advice and educational content: not just being an exercise class. Marjorie’s feedback reiterates how important these elements were to give her the ability to self-manage her condition. The mental health impact of falling is not always recognised, and ability to support the improvement of independence and confidence in someone like Marjorie is a positive outcome for the individual as well as for the team and DCHS.
Page 4 of 57 Patient Story.docxOverall Page 10 of 218

Monitoring Information Brief Summary
What are the Governor Involvement implications?
Governors will be assured by people’s experiences and the support available to them when they experience a fall. The integrated care approach is essential in ensuring patients received personalised care to reach their rehabilitation goals and can regain independence.
What are the Equality, Diversity and Inclusion implications?
The Falls Group is inclusive of people who have experienced falls. There are no equality implications for consideration.
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
This story highlights the benefits of a multi-disciplinary assessment, care and support when looking after people following a fall. These steps have had a positive impact in reducing patient falls and reducing hospital attendances/ admissions within the wider health system. Patient feedback positively shows the impact this experience has had.
Risk Register
Is the issue on the current Risk Register? No If yes, what is the Risk Number? N/A
Does this update recommend a change in the current risk score? (If so, please provide your rationale below) No
Page 5 of 57 Patient Story.docxOverall Page 11 of 218

Overall Page 12 of 218

Minutes of the DCHS Board Meeting held on Thursday 30 November 2017at Belper Town Football Club, Belper.
Name Initial Job titlePrem Singh PS ChairChris Bentley CB Non-Executive DirectorKaye Burnett KB Non-Executive DirectorKirsteen Farrar KF Associate Director of Corporate Governance /
Trust SecretaryKaren Hughes KH Associate Non-Executive Director, DCHS William Jones WJ Chief Operating OfficerIan Lichfield IL Non-Executive DirectorRick Meredith RM Medical DirectorAmanda Rawlings AR Director of People & Organisational
Effectiveness Chris Sands CS Acting Chief Executive / Director of Finance,
Information and StrategyNigel Smith NS Non-Executive Director
Present
Carolyn White CW Chief Nurse
Tracy Allen TA Chief Executive Apologies James Reilly JR Non-Executive Director
Jim Austin JA Associate Director of TransformationTim Broadley TB Associate Director of StrategyMelanie Curd MC Deputy Trust SecretaryJohn Wilson JW Ministry of Defence Wayne King WK Reservist (left after agenda item 201/17)Claire Gill CG Reservist (left after agenda item 201/17)Christine Ongoma CO Reservist (left after agenda item 201/17)
Attendees
Lieutenant Colonel Duncan Jenkins DJ Ministry of Defence (left after agenda item
201/17)
Item Description Action197/17 PART 2 – Public Session
198/17 INTRODUCTORY ITEMS
199/17 Introductions and WelcomePS opened the meeting and welcomed everyone to the DCHS Board meeting.
200/17 Staff StoryAR introduced the Staff Story and handed over to the three Reservists who introduced themselves.
Page 1 of 128 Minutes November 2017.docxOverall Page 13 of 218

Item Description Action
CW asked how DCHS can support and what can we do more of to help staff fulfil their obligations as a Reservist.
CO stated that releasing staff without them having to use annual leave and family time. Letting Reservists share experiences so that everyone knows what Reservists do and how The Trust benefits from their experience of being in the army.
NS asked how you become a Reservist and how does DCHS encourage more staff to become one.
CG explained you can go online and fill in an application to become a Reservist. The best way to encourage more staff is to get the staff stories out into DCHS and explain the amount of roles there are within the army to choose from.
JA asked what have you learnt whilst being a Reservist that you have bought back to DCHS. CG stated going back to basics and using your hands, eyes and ears to support the diagnosis not just relying on equipment. WK explained he had completed a tour of Afghanistan as part of the emergency trauma team. The skills he learned as part of that team give him more confidence when he is dealing with emergencies within DCHS. CO stated it is the values and standards you are taught in the army; it’s about commitment, integrity, team working, courage and loyalty and CO applies those principles in her work life.
CS thanked the staff members for attending Board and telling their story. He stated there is a commitment to improve with their help as ambassadors. He asked AR to consider how we can use our Responsive Workforce to support managers to release staff.
The Board received the Staff Story for information.
AR
201/17 Signing of Armed Forces CovenantPS explained that DCHS has publicly committed to signing the Armed Forces and handed over to Lieutenant Colonel Duncan Jenkins.
DJ thanked DCHS and the Chair for the invitation and stated we are the first NHS Trust in Derbyshire to sign the Covenant. PS committed to talking to his Chair colleagues at the other Derbyshire NHS Trusts and finding three more Trusts to sign the Covenant.
DJ gave an overview of how Reservists support the regular army and the types of roles you can undertake as a Reservist.
He stated the DCHS support for Reservist was par exemplar and the number of days paid leave was exceptional.
Lieutenant Colonel Duncan Jenkins and Prem Singh, Chair of DCHS signed the Armed Forces Covenant.
PS
Page 2 of 128 Minutes November 2017.docxOverall Page 14 of 218

Item Description Action202/17 Apologies for Absence
Apologies were noted as above.
203/17 Declarations of InterestThere were no declarations of interest.
204/17 Questions from the PublicThere were no formal questions from members of the public.
205/17 Draft Minutes of the meeting held on 28 September 2017The minutes of the meeting held on 28 September 2017 were agreed as accurate.
206/17 Matters ArisingThere were no matters arising.
207/17 Actions Matrix175/17 Chief Executive’s Report – WJ confirmed he had commissioned a site survey of toilets in DCHS managed sites but had received no feedback as yet. It was agreed the detail from the survey would be discussed at QPC.
The Board noted the Actions Matrix.
Agenda Item QPC
208/17 Chairman’s Report PS started his report with the strategic theme and explained workforce is one of the biggest challenges and risks facing the NHS. Nationally, NHS staff pay is high on the agenda with commitments in the autumn budget but linked to productivity and reform of Agenda for Change. There is much in the news around nurses leaving the NHS, particularly community nurses, which is worrying when the whole strategy is care closer to home and in the community.
Today we celebrate and promote the work of our Reservists and sign an Armed Forces Covenant, committing DCHS to recognise the value of serving Reservists, veterans and the military and their families. Not only is this the right thing to do but it makes business sense, as a source of workforce supply and experience.
Therefore the strategic theme is celebrating our fantastic workforce, wrapping our care and compassion around them, in an inclusive way, particularly during these challenging times so that they can in turn wrap their care and compassion around our patients and communities.
PS summarised his work during the October and November on strategic partnerships, where he: attended the monthly STP Board meetings and an STP Board
Leadership Summit. The focus is on a grip on this year’s financial position as well as transformation plans from 2018/19 onwards; leadership and management capacity around planning and finance
Page 3 of 128 Minutes November 2017.docxOverall Page 15 of 218

Item Description Action attended a joint County and City Health and Wellbeing Development
Session on Stepping Up to Place, led by the local Government Association. The workshop took the form of a self-assessment to support us to as local health and care leaders to critically self-assess our ambitions, capabilities and capacities to integrate services to improve the health and wellbeing of local citizens. Key area of discussions were implementation of plans, providing coherent leadership in relation to STP, openness and public engagement
as member of the Derbyshire Health and Wellbeing Board, was invited to join a small working group to review and refresh the current focus and governance arrangements for the Board
In terms of DCHS sites and services, PS had attended a range of events as part of DCHS Community Week including the
Annual Members Meeting and joined one of several bake off challenge judging panels. It was a very successful week and we are already planning the next one to coincide with NHS70
a Thank you Time and Tea Party as part of the new reward and recognition scheme to celebrate and thank staff by inviting them to take some time out to enjoy tea and cakes with colleagues and friends
a lunch for leaving Governors to thank them for their significant contribution to DCHS.
an Insight Visit to Butterley Ward, Ripley Hospital
PS key Governance and Accountability activities have included: attending the Governance Group meeting and Chaired the Nominations
and Remunerations Committee. attending an equality and diversity challenge and confirm event, and PS
will be working with AR to take stock of the findings to help pull together a next steps plan
a Board development session focussing on the Board Assurance Framework and our strategic priorities for next year
a Governors Induction Day for our newly elected Governors chairing the Charitable Funds Committee and Council of Governors
meeting and also the bi-monthly Non-Executive Director meeting a quarterly catch-up meeting with Fran Steele of NHS Improvement –
discussions around the challenging financial position and impact on our contract and STP
Attending the Quality People Committee as part of the rolling programme of attending each of the Q committees during the year; focussing on aligning many challenges such as recruitment and retention, absence, leavers, vacancies, workload, management of change and the inter-relationship between them
At a national level, PS had: Attended the bi-monthly Midlands and East Chairs’ Networking event. A
good opportunity to gain insights on state of the nation as well as fantastic insights and learning from others’ experience and networking
Attended the NHS Confederation Board Strategy time out with a focus on the priorities facing the NHS including workforce and pay, funding
Page 4 of 128 Minutes November 2017.docxOverall Page 16 of 218

Item Description Actionchallenges relating to the demand curve including capital, supporting system leadership and reform
Others areas to highlight: Ripley Community Hospital is set to get brand new extension for better
blood testing facilities. Construction work started in October on a brand new £215,000 extension at Ripley Community Hospital which will create much improved facilities for patients coming in for blood tests. PS gave his thanks to generous support from the hospital’s League of Friends
The Wheatbridge Sexual Health Team has been successful in achieving the Option 2 Dignity Award by Derbyshire County Council. This assessment replaces the old ‘silver’ dignity award and requires evidence of lasting changes made within the service to benefit the patient
DCHS’ School-age Immunisation team have won the Nursing Times’ Team of the Year award
Our DCHS Rural Health team organised a successful annual health MOT event for farmers attending Bakewell Agricultural and Business Centre on livestock market day
Our Buxton MIU-based paramedic Roma Harrison-McRory met Dame Patricia Routledge when the actress performed her show (Facing the Music – A Life in Musical Theatre) at Buxton Opera House. Dame Patricia had to cancel her show in the summer because she suffered a bad fall and needed care from the MIU team. Roma had been invited to this rescheduled performance and to meet the actress afterwards in happier circumstances as a way to say thank you for the care received
The Board received the Chair’s Report.
209/17 STRATEGY, VALUES AND VISION
210/17 Chief Executive’s ReportCS presented the report and highlighted the following key issues:
Budget November 2017 – a very welcome investment, there will be additional capital funds of £3.5bn over the next three years. Locally Chesterfield Royal Hospital have been announced as one of the first wave to receive capital funding which will be used to develop a modern urgent care facility
There is additional funding for a pay rise however this appears to be linked to a reform of Agenda for Change; we will need to understand the implications of this and to communicate it to our staff
Nationally, the quarter 2 financial position is showing a deficit of 1.15bn which is £143m worse than plan. The forecast assumes that the current level of overspend will be maintained and will not deteriorate further
Locally, we have reached an agreement with our Commissioners on a year-end financial position that reduces the financial risk for all parties
System transformation - an initial timeline has been developed for Better Care Closer to Home (BCCtH). We have discussed this in our
Page 5 of 128 Minutes November 2017.docxOverall Page 17 of 218

Item Description Actionstaff engagement events and are taking feedback from our staff to inform our approach in supporting our staff through this major change
Our Minor Injury Units (MIUs) will not be designated Urgent Treatment Centres (UTCs) and there will be a review of urgent care by Commissioners
NS highlighted the Big 9 and the 95.75% attendance target where we are forecasting we will achieve 95.5%. AR stated there had been a long discussion at QPC regarding attendance which is still a challenge for us and she confirmed we are unlikely to meet the target.
KB asked whether there are penalties if we do not achieve our Delayed Transfers of Care (DTOC) target. CS explained there wasn’t and we are achieving a significantly better performance since we undertook a deep dive at QBC however we are about to go into winter which could impact on the performance.
PS asked whether not achieving DTOC would affect our Segmentation with NHS Improvement (NHSI). CS stated not at the moment but if NHSI introduce it as a metric we would have to consider how we manage our individual performance against the wider system
The Board received the Chief Executive’s Report and the assurance it provided.
211/17 QUALITY, PERFORMANCE AND GOVERNANCE
212/17 Board Assurance Framework (BAF) – Quarter 2KF presented the BAF for Quarter 2 and explained that it had been discussed in detail at the Quality Committees and at the Audit and Assurance Committee.
In addition, she highlighted that there will be amended BAF in place for the new financial year.
The Board approved the Board Assurance Framework.
213/17 Performance Report CW presented the Quality Service section of the report and stated that overall we are performing well; we are rated green by NHSI on their quality surveillance and the CQC have reduced the frequency of our meetings to bi-monthly.
NS highlighted the pressure ulcer table in the report and stated he found it useful to see when they occurred versus when they were reported, however he stated that the exception report highlighted too many instances where our staff were not following procedures and the numbers did not appear to be decreasing.
CW stated that within Derby City we needed to improve reporting and
Page 6 of 128 Minutes November 2017.docxOverall Page 18 of 218

Item Description Actionpractice; we have made significant leadership changes in that area and we are providing a lot of resource from specialist teams. CW stated she expected to see improvements from all the actions we have taken.
AR presented the Quality People section of the report and highlighted RIDDORs (Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 2013); we have undertaken a deep dive and five of the RIDDORs are MSK injuries by moving / handling and two are dog bites. NS stated that he had experience of reducing dog bite incidents from his previous role at Royal Mail and would be happy to share his learning with our Head of Health and Safety. Agency costs are performing well however we are about to go into winter.
KB asked how confident we were that we would hit our appraisal and essential learning targets in the final months of the year with winter pressures. AR stated that we have learned from previous years and managers should be staggering essential learning and appraisal throughout the year.
CS presented the Quality Business section of the report and stated that we have included in additional measure regarding the roll out of electronic records to show our progress using IT to support care.
PS summarised the debate and stated this was a key report for demonstrating accountability and our performance, we are doing really well; some areas continue to be a challenge and we have plans in place to address them.
The Board received the Performance Report and the assurance it provided.
214/17 Financial Performance ReportCS presented the report and explained the month 7 position is on plan and we are forecasting we will meet our control total of £4.9m.
We have reached an agreement with our Commissioners which closes a number of financial risks; particularly on cost per case and CQUIN and it also supports the Clinical Commissioning Group’s (CCG) year-end position.
CS explained the cash position is ahead of plan which is due to underspends on capital and working capital issues.
The Board received the Financial Performance Report and the assurance it provided.
215/17 Audit and Assurance Committee (AAC) Meeting Summary Report including Annual ReviewNS presented the Summary Report and highlighted:
Clinical Effectiveness – this item has previously received limited
Page 7 of 128 Minutes November 2017.docxOverall Page 19 of 218

Item Description Actionassurance however a considerable improvement has been made with reporting and outcomes and AAC gave it significant assurance
Data Quality – there is further work to be undertaken by 360 Assurance to review the quality threshold and determine the appropriate level it should be set at
Compliance with Governance Arrangements – there has been an increase in claims regarding diagnosis at our MIUs due to the nature of attendances being minor illness rather than minor injuries
General Data Protection Regulation – comes into effect May 2018. It will impose additional responsibilities on DCHS which could have financial consequences. QSC will be leading the assurance on DCHS preparation for the new regulations
Internal Audit - actions from the Integrated Sexual Health audit have all been completed promptly and successfully
Finally, NS highlighted the Annual Report for Board approval.
PS asked what the timeframe was for the 360 Assurance review on fire safety and ligature points. CS explained these have commenced and will be reported to AAC in January 2018.
PS stated he was disappointed by the decision regarding not to designate our MIU’s as UTC particularly as we have evidence that they are operating as UTC with the cohort of patients they are seeing.
CS stated that patients are exercising choice to attend our MIUs when they find it difficult to get an appointment within primary care and so we are seeing a different cohort of patient which is more complex.
The Board received the Summary Report and the assurance it provided. In addition, the Board approved the Annual Review.
216/17 Quality People Committee (QPC) Meeting Summary Report including H&S Annual ReviewKB presented the Summary Report and highlighted the Staff Story which described a staff member’s experience of our Development Centres.
An update was provided on the new Board Assurance Framework risks which will be in place from 1 April 2018. KB highlighted the next steps we are planning to take with our Equality, Diversity and Inclusion work.
In addition, the Annual Health and Safety Report was presented to Board for approval.
NS highlighted the table in Appendix 1 of the report and the numbers of violence and aggression incidents. He stated that whilst there were only three RIDDORs reported there were 213 minor injuries; he asked what we were doing to protect our staff.
AR explained we are encouraging our staff to report all incidents on Datix and we are using the data to shape our priorities and focus on what we can
Page 8 of 128 Minutes November 2017.docxOverall Page 20 of 218

Item Description Actiondo differently.
The Board received the Summary Report and the assurance it provided. In addition, the Board approved the Annual Health and Safety Report.
217/17 Quality Service Committee Meeting Summary ReportCB presented the Summary Report and highlighted the work of the Records Management Group and the Research and Innovation Group.
CB discussed the learning from the recent leg ulcers deep dive and highlighted the real evidence we now have that we can utilise in the management of leg ulcers.
CB stated there are still a small proportion of avoidable pressure ulcers which occur within our care. He explained the majority are developed outside our care which is why it is imperative we work on reducing pressure ulcers as a system.
Finally, CB highlighted the Annual Children and Adults Safeguarding Report which QSC had given significant assurance.
PS asked about our paper based records management system and whether this impacted negatively on the care we provide. JA explained we are moving to an electronic system; primary care is fully electronic including IT referrals and receipt. Our inpatient areas have e-prescribing however there is still work to do on an electronic health record.
The Board received the Summary Report and the assurance it provided.
218/17 Quality Service Committee Risk Register Review Meeting Summary ReportCB presented the Summary Report and stated all the risks on the Risk register had been reviewed in detail.
The Board received the Summary Report and the assurance it provided.
219/17 Quality Business Committee Meeting Summary Report including Annual ReviewIL presented the Summary Report and stated he had no matters to escalate to the Board. He did wish to highlight the concerns of the Committee regarding the worsening CCG financial position and the agreement we have with Commissioners regarding our outturn position.
IL highlighted that all areas discussed received significant assurance which is a real step forward and reflects the control and grip the sub-groups have on the issues.
IL explained QBC had received the annual report on fire safety and had
Page 9 of 128 Minutes November 2017.docxOverall Page 21 of 218

Item Description Actionasked for a further report on the significant risks identified when the fire risk assessments are completed.
In addition, IL stated the Annual Review and the Terms of Reference were presented to Board for approval.
The Board received the Summary Report and the assurance it provided. In addition, the Board approved the Annual Review and the Terms of Reference.
220/17 Council of Governors (CoG) Summary Report including CoG Roles and ResponsibilitiesPS presented the Summary Report and welcomed the nine newly elected Governors to the Council and welcomed back the three re-elected Governors.
PS also highlighted the Roles and Responsibilities of the Council of Governors and explained this had been discussed at the Nominations and Remunerations Committee and CoG and was presented to Board for approval.
The Board received the Summary Report and the assurance it provided. In addition, the Board approved the Roles and Responsibilities of the Council of Governors.
221/17 Annual Members Meeting Summary ReportPS presented the Summary Report and explained it was a record of what had been covered at the Annual Members Meeting.
The Board received the Summary Report and the assurance it provided.
222/17 Charitable Funds Committee Summary Report including Annual ReviewPS presented the Summary Report and stated that the Charity’s finances are good; the Committee recognised the governance costs of running the Charity are challenging and outweighs the amounts paid for charitable purpose.
PS stated we need to raise the profile of the Charity and continue to replenish the funds. PS also highlighted the Annual Review of the work of the Committee.
The Board received the Summary Report and the assurance it provided.
223/17 DCHS Charity AccountsCS presented the audited 2016/17 Annual Accounts and Annual Report for our Charities.
CS explained they had been reviewed by Price Waterhouse Cooper (PWC)
Page 10 of 128 Minutes November 2017.docxOverall Page 22 of 218

Item Description Actionand subject to the documents being signed; we will have an unqualified opinion on the accounts.
The Trustees adopted the 2016-17 Annual Report and Accounts for the Charity and delegated authority for signing off the Accounts to the Chair and Director of Finance, Information & Strategy. In addition, the Trustees delegated authority to the Chair to sign the Letter of Representation.
224/17 Quality ReportCW presented the report and highlighted:
Promoting Professionalism, Reforming Regulation – a national consultation for the nine regulatory bodies to work together more effectively to regulate health professionals
Draft Healthcare Investigations Bill – the draft Bill will create a statutory Health Service Investigations Body, independent of the NHS and at arms length from the Government to investigate incidents
House of Commons Briefing re Deprivation of Liberty safeguards (DoLs) – the intention is to streamline the process for assessing whether a DoL is necessary
CW also highlighted that the Learning from Deaths report schedule is attached and confirmed that this met with NHS England’s expectations.
CS asked whether the new DoLS system will address the current issues we have in the length of time to undertake a DoLS assessment. CW stated it’s not clear at this stage however there is recognition nationally of the burden of the current system since the Cheshire West judgement.
The Board received the Quality Report and the assurance it provided.
225/17 CONCLUDING ITEMS
226/17 Any Other BusinessThere were no items of any other business.
227/17 Self-Certification/Risk/Board Assurance FrameworkThere were no items discussed that impacted on the Self-certification, risks or BAF.
228/17 Questions from the public relating to today's board businessJohn Morrissey, Lead Governor for Derbyshire Healthcare NHS Foundation Trust asked whether signing the covenant was voluntary for public sector organisations.
PS said yes it was voluntary and for individual Trusts to decide; there was no central mandate from the Department of Health. John Wilson from the Ministry of Defence added that they ask all employers to be flexible without detriment to the staff member’s family or finances. Many NHS
Page 11 of 128 Minutes November 2017.docxOverall Page 23 of 218

Item Description Actionorganisations have a provision within their special leave policy however there is nothing written into Statute.
229/17 Review of the Meeting and OutcomesGood meeting.
230/17 Date of Next MeetingThursday 25 January 2018 at The Post Mill Centre, Market Cl, South Normanton, Alfreton, DE55 2EJ
Page 12 of 128 Minutes November 2017.docxOverall Page 24 of 218

DCHS BOARD – ACTIONS MATRIX DATE: January 2018 – Public Session
Date/Item No:
Item/subject: Decision taken and/or action required:
Progress: Responsible Person:
Deadline: Outcome:
Oct 2017188/17
Mortality Report Table which details reported deaths in Derbyshire, should state that the care provider in each case is not known, and therefore may not have been DCHS
Mortality Report attached to the Quality Service Committee Summary Report
Rick Meredith January 2018
Agenda item January 2018
Nov 2017200/17
Staff Survey To consider how to use the Responsive Workforce to support managers to release staff.
We are continuing to increase the size and range of professions in the Responsive Workforce Team to enable the Trust to have access to resources that can be deployed based on demand. Additionally there is an on-going focus on increasing the size of our bank so we can support the short term need for staff.
Amanda Rawlings
January 2018
Complete
Nov 2017201/17
Signing of Armed Forces Covenant
PS committed to talking to his Chair colleagues at the other Derbyshire NHS Trusts and finding three more Trusts to sign the Covenant.
PS has contacted all of the provider Trusts within Derbyshire regarding signing up to the Armed Forces Covenant.
Prem Singh January 2018
Complete
Oct 2017180/17
QPC Summary Report
Workforce to be subject of a future Board Development Session
Amanda Rawlings
April 2018
Page 1 of 110 Actions Matrix - public session.docxOverall Page 25 of 218

Overall Page 26 of 218

TRUST BOARD Document Title: Chief Executive’s Report
Presenter/Title: Tracy Allen, Chief ExecutiveContents of Paper were previously discussed by: n/a
Author/Title: Tracy Allen, Chief ExecutiveContact Email and Telephone Number:
Cathryn Pearson, Executive Assistant,[email protected] 01629 817892
Date of Meeting: 25 January 2018 AgendaItem No: 13c/18
No of pagesinc. this one: 9
Has an Equality Impact Assessment been undertaken Yes No X
Document is for:(more than one box can be ticked) Information X Decision Assurance
Purpose of Paper
The report provides information on strategic policy, legislative and developmental issues affecting the organisation and includes:
The national context and perspective:o NHS Performance and planning o NHS Providers briefing on STPs and the development of accountable careo Developing a national network of community services providers supported by the
NHS Confederation and NHS Providers System Transformation
o Joined Up Care Derbyshire (Sustainability and Transformation Plan)o Progress with the Better Care Closer to Home implementationo Joined up Care in Belpero Buxton land acquisitiono Heanor Memorial Health Centre
Key Operational Issues and Updateso Our contribution to supporting the systems winter pressures (including staff
vaccination rates)o Freedom to Speak Up – National Guardians Office (NGO) reviewo Implications of Carillion collapse
Headline organisational performance – the Big 9
Recommendations
The Board is recommended to note the report.
Board Assurance Framework Risk Reference
N/A
Page 1 of 913 Chief Execs Report.docxOverall Page 27 of 218

Financial Impact
No direct financial impact although the paper discusses in year contract escalation which poses a significant financial risk to the Trust.
Further Information and Appendices
Chief Executive's Report January 2018
1. Purpose of the paper
This paper is to provide the Trust Board with information about key national and local strategic issues affecting the Trust.
2. National Issues
2.1 National NHS Performance and Planning Board members will be aware of the very significant pressures across the NHS during the holiday period and the knock on implications that this has had on patients in terms of access both to urgent care and routine elective care. This represents an exacerbation of the falling performance seen through quarters 2 and 3 and reflects growing demand and complexity along with increased flu prevalence.
A national decision to recommend that trusts postpone routine elective care until the end of January was made at the beginning of the month. DCHS has reviewed the opportunity to temporarily shift capacity from planned services (therapy and Diagnostic and Treatment Centre (DTC) outpatients) into pressurized urgent care services. In conjunction with colleagues at Derby Teaching Hospitals NHS Foundation Trust (DtHFT) we have taken the decision not to take this route around the DTC clinics as the skill mix of staff released would not be easily converted into the areas where capacity is required although some planned care nurses have been able to do extra shifts to support inpatient and community teams. A small number of physiotherapists and occupational therapists from the Musculoskeletal (MSK) service have been supporting integrated community teams where appropriate skills and experience exists.
Whilst work continues within the Trust on the development and refinement of the second year of our operational plan for 2018/19 we have been told to expect national planning guidance imminently. At the time of writing this report it was still to be received although we do not anticipate any significant surprises in terms of requirements or timescales.
2.2 NHS Providers briefing on Sustainability and Transformation Partnerships (STPs) and Accountable Care
As part of our work as a Board within the Derbyshire STP and continuing to develop our organisational strategy we have been exploring the opportunities and challenges that developing accountable care offer for our communities in terms of delivering the agreed system priorities.
This conversation will continue as a key theme in the Board strategy away day next month.
Page 2 of 913 Chief Execs Report.docxOverall Page 28 of 218

NHS providers have produced an excellent briefing document this month which brings together information on the development of STPs, accountable care systems (ACSs) and accountable care organisations (ACOs). It draws on national policy information and their conversations to date with trusts and other stakeholders. It includes:
the national policy story so far, as plans evolved into partnerships; definitions of key terms associated with STPs, accountable care, and new care models; five conditions for success based on our conversations with trusts, and; NHS Providers’ position and information on the support trusts can access from us.
This briefing and further information on STPs and accountable care is available on their website: http://nhsproviders.org/topics/transforming-care and I would recommend it as background reading for the awayday.
2.3 Developing a national network of community services providers supported by the NHS Confederation and NHS Providers
Over the past 3 months a group of NHS providers of community services led by Matthew Winn have been working with the NHS Confederation and NHS Providers to work up the establishment of a formal community services providers network that both national organisations can support.
The objectives of this network are to:
address the absence of community services from the national narrative, and; focus on key policy issues that enable the delivery of high quality community care, so that
its contribution to overall service transformation and delivery can be maximised.
This Network, on track to be launched in April, will replace the Community First Network that DCHS is currently part of – forming a more inclusive approach that is open to any NHS providers of community services rather than being restricted to particular organisational forms. Community First Network members have agreed to utilise their 18/19 subscriptions to support the development of the new network.
A shadow Board has overseen development up to this point and will be seeking formal nominations for board members from all the different types of community services providers over the next month or so.
This is an important and exciting development and one which I hope DCHS NHSFT can play an active role in taking forward.
3. System Transformation
3.1 Joined Up Care Derbyshire (Sustainability and Transformation Partnership)
The Joined Up Care Derbyshire Board (formerly STP Board) continues to meet monthly. Key issues currently being discussed include:
The continuing concerns with the Derbyshire financial position in 2017/18, and how this impacts upon plans going into 2018/19.
The progress with implementing winter plans.
Page 3 of 913 Chief Execs Report.docxOverall Page 29 of 218

The process to develop a Derbyshire Plan for 2018/19. Reviewing and refocusing the Provider Alliance Group as a provider only forum to focus on
the development supporting the transition to an accountable care system. The development of “Place” across Derbyshire with a proposal to move to a much smaller
number of places across Derbyshire that will support integration of local authority and county wide NHS providers.
This work will be supported by a new part time STP Director, Vikki Taylor, from NHS England who has joined the system from the beginning of January.
However as the size of the financial challenge for next year grows, there remain significant risks that the STP priorities do not correlate to commissioning intentions and decisions, and that the organisations in the system continue to struggle to translate commitment to the system vision and plan into materially different actions and behaviours that really move the strategy forward.
Items 3.2, 3.3 and 3.4 below are service transformations that form part of the Derbyshire STP.
3.2 Joined up Care in Belper – proposed consultation on the future of Babington Hospital by Southern Derbyshire Clinical Commissioning Group (CCG)
NHS Improvement (NHSI) have indicated their support for the business case that the Trust submitted for the capital to build the new facility in Belper. We now await final confirmation from the Department of Health for the £5.9m of capital funding which is expected within the next month.
Southern Derbyshire CCG have begun an eight week period of engagement with the public about the proposed new building on Derwent Street and the suggested model of care, having secured agreement from NHS England (NHSE) and Derbyshire County Council Overview and Scrutiny Committee to progress in this way rather than undertake a formal public consultation.
William Jones has been leading early engagement with local DCHS colleagues affected and will continue to support the CCG with the process as it rolls out during February and March.
3.3 Progress with the Better Care Closer to Home (BCCtH) Implementation
The Trust, along side its partners, is continuing to progress the development and delivery of implementation plans for the different elements of this major service transformation plan.
Key developments over the last couple of months include:
Older Peoples Mental Health (OPMH)
o A successful recruitment event for the Dementia Rapid Response Team (DRRT) took place in late November 2017. The DRRT will be delivered by Derbyshire Healthcare NHS Foundation Trust, and they will be appointing the staff.
o The anticipated closure of Spencer Ward at Buxton has been brought forward to coincide with the launching of the DRRT for High Peak. This will take place at the end of February 2018.
o A temporary consolidation into a reduced number of beds at Walton, in line with Page 4 of 913 Chief Execs Report.docx
Overall Page 30 of 218

current demand, to ensure staff staffing levels can be maintained while these changes are transacted.
o The first pilot phase of DRRT has started in the Bakewell area, and is demonstrating good patient outcomes.
Rehabilitation
o An additional 4 beds with care have opened in early December at the DCC Meadowview facility at Darley Dale. No further changes are planned in the rehabilitation part of the proposals until after winter.
The Staff Partnership Committee have approved a specific management of change policy for colleagues affected by system transformational changes which has been well received by our unions and affected staff. We continue to seek opportunities to learn about how we can support colleagues affected by these complex changes more effectively and a recent staff story presented at the Quality People Committee (QPC) has highlighted some areas for us to focus on.
3.4 Buxton land acquisition
We were delighted to be able to announce the purchase of part of the old Buxton Water site next to the railway station in Buxton at the end of December – moving us closer to delivering on the Trust’s long term strategic ambition to secure 21st century health and other public sector facilities in the High Peak area.
I would like to thank William Jones on behalf of the Board, and our wider partners in the proposed development, for his personal leadership in delivering this acquisition and the coalition building required to get cross system commitment to progressing with the planning for an integrated health care development. 3.5 Heanor Memorial Health Centre
The capital development to re-provide a brand new health centre in Heanor has now been completed, and the contractor has handed over the building to the Trust. The first patients were welcomed to the new facility on Monday 8th December 2017.
The formal opening of the new building will take place on 13th February.
4. Key Operational Issues and Updates
4.1 Our contribution to supporting the systems winter pressures (including staff vaccination rates)
Additional planned community capacity has been in place and working effectively as per the tTrust’s winter plan. As a result of continued pressure at Derby Teaching Hospitals an agreement to open a further six community hospital (pathway 3) beds at St Oswalds has been reached over and above the original plan. The CCGs will be funding these recognising the high requirement for agency staffing they depend on.
Whilst the extraordinary levels of demand experienced have impacted on emergency department
Page 5 of 913 Chief Execs Report.docxOverall Page 31 of 218

performance at both Chesterfield Royal and Derby Teaching Hospitals the system has performed comparatively well in terms of the A&E 4 hour target – CRH has achieved some of the best rates in the region consistently.
Of course the pressure so visible in our emergency departments is also being felt across the rest of the system – where it is much less visible. We are continuing to develop our community team demand and capacity modelling which is enabling us to identify teams simply unable to stretch to supporting additional patients in order to maintain safe staffing levels.
Great progress is also continuing to be made on reducing delayed transfers of care (DTOCs) - another key indicator of overall system performance and it is encouraging to see this progress and very strong performance reflected in the fact that Derbyshire has the lowest level of DTOCs of any English county local authority.
A key contribution that the Trust can make to winter pressures is increasing the proportion of our frontline workforce that are vaccinated against flu. This is particularly important this year given the rapidly increasing prevalence of flu reported and its severity, and is not an area where we have performed well historically.
I am therefore very pleased to report that the Trust’s staff flu uptake was 60.5% (2127 frontline staff vaccinated) as of the 12th January. This represents a significant improvement over previous year end rates and is a great credit to the team managing the process. Every effort to make the vaccination accessible to remaining staff will continue to be made over the next few weeks.
4.2 Freedom to Speak Up – National Guardians Office (NGO) review
The Trust are pleased to be welcoming the National Guardian’s Office (NGO) to DCHS this month in order to review the way we have worked as an organisation in the handling of a concern that was raised. The National Guardian’s Office is a relatively new national body launched in June 2017 to provide training and advice for Freedom to Speak Up Guardians based in all NHS trusts and provide challenge, learning and support to the healthcare system as a whole by reviewing trusts’ speaking up culture and the handling of concerns.
The review will be taken forward as part of the 12 month pilot of the National Guardian’s Office case review process to review the handling of concerns and the treatment of people who have spoken up, where there is evidence that good practice has not been followed. It will make recommendations to NHS organisations to take appropriate action, whilst also commending areas of good practice.
As part of their time with DCHS the NGO will be speaking with members of staff and amongst other things reviewing the raising concerns processes we have in place. They will make recommendations where there are any areas we need to take appropriate action to improve those processes. Although the review is focused on a specific case, colleagues across the organisation have been offered the opportunity to share their own experiences of speaking up, whether positive or negative, or to understand more about the review process by contacting the National Guardian’s Office directly at [email protected]
Page 6 of 913 Chief Execs Report.docxOverall Page 32 of 218

We look forward to supporting the review and learning any lessons that emerge from it around how we can continue to develop and strengthen our Freedom To Speak Up culture and associated systems and processes.
4.3 Implications of the Carillion collapse
Following the announcement of the collapse of Carillion the Trust has undertaken an assessment of implications. Carillion is the provider of hard facility management services into the LiFT buildings that the trust occupies in the south of the county owned and managed by Community Health Partnerships (CHP) and also provide a small security service specifically at Long Eaton. We are seeking urgent confirmation of contingency arrangements from CHP and a risk has been generated until we have assurance on this. Any further update available will be presented at the Board Meeting.
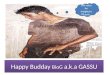
5. Organisational Performance October 2017
The Trust’s performance against our 2017/18 ‘Big 9’ for December is attached for information as Appendix 1.
Monitoring Information Brief Summary
What are the Governor Involvement implications?
Governors will continue to be involved in and engaged with the STP and other strategic development work referenced in the paper. They will also be engaged in our response to the contract escalation issues discussed.
What are the Equality, Diversity and Inclusion implications?
System transformation plans, Joined up Care in Belper and Better Care Closer to Home consultation have equality and diversity implications that will be assessed and managed as the initiatives proceed.
Inequalities across Derbyshire risk being widened by financially driven planning or commissioning proposals and must be comprehensively assessed by commissioners.
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
Better Care Closer to Home consultation has involved very significant input from staff, patients, and the public. SDCCG leading on public engagement around services in Belper.Engagement of the whole workforce will be required as the STP implementation proceeds.
Risk Register
Is the issue on the current Risk Register? No If yes, what is the Risk Number? N/A
Page 7 of 913 Chief Execs Report.docxOverall Page 33 of 218

Does this update recommend a change in the current risk score? (If so, please provide your rationale below)
Page 8 of 913 Chief Execs Report.docxOverall Page 34 of 218

Objective Priorities 2017/18 Target
Insulin safe administration - Right dose, right time80% (715) of Community Nurses have
completed Insulin Safety e-learning Training by March 2018
546 (76%) 433 (61%) (AMBER) 497 (70%) (AMBER)
Proportion of services adopting patient related service outcome measures 37 services reporting to CEG by March 2018 29 (78%) 29 (78%) (GREEN) 37 (100%) (GREEN)
Identif ication of carers on TPP Identify 75% of carers w ho access our services, a total of 2,890
2,000 (69%) 1,420 (49%) (RED) 1,693 (59%) (RED)
Objective Priorities 2017/18 Target
Increase average 12-month attendance rate across the Trust by 0.5% by year end Average 12 month attendance to be 95.75% 95.73% 95.01% (AMBER) 95.50% (AMBER)
Increase staff engagement in teams w ith a low engagement score by 10%
57 56 (98%) 58 (102%) (GREEN) 61 (107%) (GREEN)
Increase the reporting of Health and Safety Near Misses by 20% during 2017/18 140 101 (72%) 102 (73%) (GREEN) 140 (100%) (GREEN)
Objective Priorities 2017/18 Target
Demonstration of eff iciency across all DCHS services through the delivery of the Sustainable
Quality Improvement Plan (SQIP) Delivery of £7.2m SQIP Plan £5.278m (73%) £5.280m (73%) (GREEN) £7.256m (101%) (GREEN)
Delivery of effective services w ithin the CommunityDelayed Transfer of Care (%) to be 3.5% by
December 2017 3.5% 5.6% (RED) 5.5% (RED)
Responding to the main issue raised through staff feedback by monitoring the perceived improvement
in IT connectivity for staff
Less than 35% of staff Often or Alw ays Experiencing Connectivity Problems 35% 36% (AMBER) <35% (GREEN)
Notes: Delayed Transfer of Care in DCHS Control 3.8%
Big 9 - December 2017
Plan to end of
December
Achieved to end of December
Quality BusinessTo ensure an effective, eff icient and economical
organisation w hich promotes productive w orking and
w hich offers good value to its community and commissioners
Quality ServiceTo deliver high quality and sustainable services that
echo the values and aspirations of the community
w e serve
Quality People
To build a high performance w ork environment that engages, involves and
supports staff to reach their full potential
Forecast
Plan to end of
December
Achieved to end of December Forecast
Plan to end of
December
Achieved to end of December Forecast
Appendix 1
Page 9 of 913 Chief Execs Report.docxOverall Page 35 of 218

Overall Page 36 of 218

TRUST BOARDDocument Title: Quality Improvement and Outstanding Way Update
Presenter/Title: Jim Austin, Associate Director of TransformationContents of Paper were previously discussed by: Board Development Session 21 December 2017
Author/Title:Jim Austin – Associate Director of Transformation Dawn Atkinson – Outstanding WayBola Owolabi – Deputy Medical Director
Contact Email and Telephone Number: 07917 267821
Date of Meeting: 25 January 2018 AgendaItem No: 14/18
No of pagesinc. this one: 5
Has an Equality Impact Assessment been undertaken Yes No X
Document is for:(more than one box can be ticked) Information X Decision Assurance X
Purpose of Paper
To assure the Board on the current position regarding progress on the Quality Improvement Methodology following December’s development session and to summarise the Outstanding Way development session activity. This will all feed into the Board Development day in mid-February.
Recommendations
Board is asked to take assurance on the work under way and to provide any further clarification/direction as necessary.
Board Assurance Framework Risk Reference
1.51.7
Financial Impact
Financial impact will be examined at the board development day in February.
Further Information and Appendices
QI Post Board Development Session
Key Points:
1. There is consensus that DCHS as an organisation is committed to Quality Improvement and Continuous learning
2. We understand the immediate pressures facing front-line teams and managers and the need to proceed with QI in a way that is responsive to these pressures
Page 1 of 514 QI and OW Update.docxOverall Page 37 of 218

3. Leadership development is a key enabler for the sustainable embedding of QI and continuous learning in DCHS
4. QI is not simply about the science, tools and methods but a holistic approach to ensuring that we are continuously improving the quality of both our process and outcomes in delivering patient care
5. Leadership development without a stated aim is unlikely to deliver our stated ambitions as an organisation
6. Our ambition is to build upon the foundation of the DCHS Way Infrastructure (Quality Service, Quality People, Quality Business) in delivering quality improvement and continuous learning across all areas of the Trust, both clinical and non-clinical. The DCHS Clinical Strategy and IHI Triple Aim are the anchor points, pulling together the improvement of patient experience, improvement of population health outcomes and reduction in the per capita cost of healthcare. It is proposed that the DCHS Improvement methodology will be nested within the Quality Always infrastructure
Following the discussion, we believe the following iteration is now the position:
Assumption Iteration
Quality Always is an embedded and respected brand and we had proposed to use it as a “wrapper” or “umbrella” within which to nest our expanded approach to quality improvement and continuous learning.
That we do not require a new brand for doing QI in DCHS
That Quality Always is retained in its existing successful form as a clinical assessment methodology (self & peer) .
That a new Quality Assessment framework is developed for the non-clinical service areas
That leadership development for QI and continuous learning becomes an overarching agenda and not necessarily a “3rd leg” of QA. In doing so, leadership development becomes applicable to both our clinical and non-clinical areas of work as an organisation
That we use the DCHS Way and its existing “Q” framework of QP, QS and QB as our spring-board for doing QI & continuous learning.
That QI and continuous learning become the common denominator for the QP, QS and QB domains of the DCHS Way.
What does this proposal look like?
Quality Improvement encompasses two broad domains. Quality Improvement Science and Leadership for Improvement. It is proposed that we adopt a phased approach to our QI ambition where building leadership capability for improvement takes the fore. In order to have immediate impact on current pressures, our leadership development for improvement offer needs to cover the domains of personal leadership, relational leadership, contextual leadership and technical leadership.
Page 2 of 514 QI and OW Update.docxOverall Page 38 of 218

Leadership development for QI & continuous learning needs to be Board to Floor for maximum efficacy and sustainability. It is proposed to break the QI journey into two phases
QI – Phase 1:
1) Facilitated Appreciative Inquiry of previous/ existing Leadership Development approaches in DCHS- What worked? What might we take with us into the future? What do we leave behind? How do ensure our next venture is fully embedded and sustained? – Feed into board development session.
2) Undertake a survey of middle management to understand their current pressures and use Appreciative Inquiry to co-create potential solutions and then use a “drip-feed” approach to using QI methodologies for taking forward some of the suggestions? (external provider eg IHI are happy to facilitate for around £15K)
3) Use the outputs from (1) to embark on building Leadership capability for Improvement and continuous learning from Board to Floor. Build capability within DCHS rather than rely on external.
QI Phase 2:
Develop the 4 domains of QI proposed in the original paper. This will need to be prioritised and phased.
Outstanding Way – December Board Development session The DCHS Outstanding Way transformation programme was established in April 2017. The programme brings together the work of the Effectiveness Team and Perfect Day service transformation and change processes from the North and South of the county. The initial scope of work has concentrated on Integrated Community Services (ICS) and was informed and directed from the following:
- Back to the floor visits undertaken by the Board
- Data from clinical information system (TPP) and workforce productivity information (BRAVO)
- Input and feedback from staff
- Reference costs and benchmark information
The guiding aims and objectives of the Outstanding Way Programme are as follows: Plan to reduce unwarranted variation and inconsistency in ways of working -
optimise efficiency/ productivity (including use of technology already deployed) thus maximising direct patient-facing time – culture and efficiency. Improved patient experience and outcomes
Plan to identify and remove barriers to inefficient/duplication use of clinical time, including partner organisations in Primary, Acute and social care – efficiency
Model for continuing to develop more integrated working - reduce duplication and inefficiency e.g. domiciliary podiatry, outpatient physiotherapy – culture, improved patient experience and outcomes
Standardisation of processes including caseload management - reduce unwarranted differences and inconsistencies across ‘Place’- based delivery, ensuring we do not waste
Page 3 of 514 QI and OW Update.docxOverall Page 39 of 218

contacts through poor caseload management and poor discharge planning – efficiency, improved patient experience and outcomes
Develop a mechanism to deliver measurable clinical outcomes - effectiveness/impact of the service can be measured – quality, patient experience and outcomes
Guidelines/expectations for activity (type and number) and for optimum skill mix – ensuring the right clinician sees the patient in the right place. Mechanism to measure and monitor performance against standards for local accountability – efficiency and clinical culture.
Outstanding Way Programme office and supportA core programme team is responsible for the oversight, monitoring and reporting progress against Outstanding Way change projects. The team also supports and facilitates service change and transformation ideas to assure robustness of aims, deliverables and to ensure proven service improvement and transformation methodology is utilised. Senior leadership and project support is secured from the wider organisation.
Improvement MethodologyThe model for service change is based on the Plan, Do, Study, Act (PDSA) approach and underpinned by continuous engagement of staff to gain service insight and generate ideas to improve ways of working. Harnessing staff to design and build different ways of working is essential to implement and embed changes across the organisation.
Board Development session – 21st December 2017The December Board development session provided an opportunity to present and discuss progress of a number of key projects that have been developed and supported through the Outstanding Way programme. The overall work programme and how staff are engaged and communicated with were also discussed.
Development session focused on the following projects
Measuring the effectiveness of the programme – the work programme has been shaped through engaging and listening to staff issues and ideas but it is important to evidence the impact of changes and support leaders to understand what is happening within their service. The OW dashboard has been designed to do both of these things – providing a live feed so teams can see what’s currently happening in their teams and plan for the future, whilst also understanding and demonstrating the impact of OW changes.
Documentation review – work done to date has seen a review of the initial contact documentation to better support staff to use their clinical skills and reasoning during the patient consultation. A full audit of ICS documentation has been undertaken, resulting in some basic housekeeping and a plan to review other documents following OW principles – documents should be concise, easy to follow, avoid duplication and be meaningful. Revised falls documentation will be deployed from February.
Patient reported outcomes – It is a Trust aim to improve the number of patients who have agreed outcomes, and to measure effectiveness against these outcomes. Work to pilot a therapy outcome which triangulates activity information against an outcome score and the experience of the patient is currently being piloted.
Lower Limb pathway – This new approach to training and supporting staff in the management
Page 4 of 514 QI and OW Update.docxOverall Page 40 of 218

of leg ulcers has been led by the Quality Team. It uses a Health Coaching methodology to ensure the patient and clinician work as a team. Early indicators show very good healing rates for these patients.
Communication and engagement – identifying issues and working with clinicians to design solutions is only the first step, and by far the biggest challenge is communicating a consistent message to our community staff, so that changes are embedded consistently – thereby meeting one our core aims of standardising processes and reducing unwanted variation.
Outstanding Way – the programme supports numerous workstreams and challenges teams to design new ways of working using the following process. There are currently 21 large scale projects the team are supporting.
What we are learningOutstanding Way programme is continually learning and adapting the way in which we approach service change to strengthen the robustness of the process. The following are areas that we are actively working on and linking with the wider organisations initiatives:
- Measurement – greater consistency/standardisation of service delivery is needed to maximise benefit realisation from service change
- Leadership - service change and transformation has to be everyone’s business, ownership at locality level needs to be strengthened
- Learning and Development – stronger connection to organisational wide L&D to support implementation of service change at pace
- Communication and engagement – assure the effectiveness of how we communicate with leaders and staff
- Culture – promote the organisational culture through tangible service involvement and improvement
Monitoring Information Brief Summary
What are the Governor Involvement implications?
Investment in a trust-wide QI methodology will have a strategic impact on the trust activity. Once agreed, this will need briefing and shaping with governor input.
What are the Equality, Diversity and Inclusion implications? These will be considered within the business case
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
Investment in a trust-wide QI methodology will have a strategic impact on the trust activity. Once agreed, this will need briefing and shaping with patient, public, staff and stakeholder input.
Risk Register
On Risk Register? No If yes, what is the Risk Number?
Page 5 of 514 QI and OW Update.docxOverall Page 41 of 218

Overall Page 42 of 218

TRUST BOARD Document Title: Quality Report
Presenter/Title: Carolyn White, Director of Quality / Chief Nurse Contents of Paper were previously discussed by:
Quality Service Committee (QSC) and a variety of other groups and forums across DCHS
Author/Title: Carolyn White Chief Nurse Director of Quality Jo Hunter, Deputy Chief Nurse
Contact Email and Telephone Number:
Carolyn White [email protected] Jo Hunter [email protected]
Date of Meeting: 25 January 2018 Agenda Item No: 16/18
No of pages inc. this one: 28
Has an Equality Impact Assessment been undertaken Yes No x
Document is for: (more than one box can be ticked) Information x Decision Assurance x
Purpose of Paper
This report is brought to Board to provide an update on key issues across the national and local Quality agenda for the period December 2017- Januray2018. The Staffing for Quality information and exception reports can be found in Appendix 1.
Recommendations
Board is asked to receive and discuss the report and agree the levels of assurance provided across the areas of the Quality agenda covered by this report.
Board Assurance Framework Risk Reference
1.5 There is a risk that our Clinical Governance initiatives do not deliver the outcomes necessary to support our Strategy
2.4 There is a risk to organisational performance due to the high volume of organisational and health system change, which is likely to continue to be a feature of our health economy for several years
4.1 There is a risk to the organisation due to not having strong corporate governance systems in place resulting in Trust vision not being delivered
4.2 There is a risk to the organisation due to not meeting regulatory, contractual or legal
obligations resulting in sanctions
Financial Impact
There was a cost of £6000 related to the Human factors training programme. The use of Bank and /or agency nurses will have additional financial implications for operational services.
Page 1 of 2816 Quality Report.pdfOverall Page 43 of 218

Further Information and Appendices
1.The National Agenda/Department of Health/NHSI/CQC 1.1 Promoting professionalism, reforming regulation - A paper for consultation In November we reported that a consultation process was underway involving 9 healthcare professional registration bodies seeking views on the proposal to draw together in closer working the work of these professional bodies. DCHS has formally responded to this consultation and included nurses, doctors, dentists, psychologists and allied health professionals in its joint response. 1.2 Care Quality Commission Development of CQC’s new Intelligence model – Insight for Community Health Services Over the last six months the CQC have been working on the development of a CQC Insight product for the 17 NHS Trusts and two Community Interest Companies that provide only community health services (CHS). CQC Insight is an intelligence tool which identifies potential changes in quality of care and supports them in deciding on the right regulatory response. The Insight model is integral to the next phase of how CQC monitors services. Insight uses some trust-level indicators based on those used in the Acute Insight product, as well as a small number related to inpatient services. DCHS have been invited to view and comment upon this product. DCHS will be attending a webinar in January to understand the product, after the session, CQC will send a PDF copy of the dashboard for us to view. They will then follow up at a later date to get our views and comments to inform the development of the dashboard and its content. 2.Improving Patient Safety 2.1 Human Factors & Root Cause Analysis To help the transition from Safety 1 (Reactive) to Safety 2 (Proactive), a 1 day Root Cause Analysis course accessible through ESR has been designed for DCHS Managers. The course includes Human Factors and offers ways to minimise and mitigate human frailties, so reducing clinical error and its consequences. It encompasses all those factors that can influence people and their behaviour. In a work context, human factors are the environmental, organisational and job factors, and individual characteristics which influence behaviour at work. To bolster this further – a 2 day course was commissioned from a nationally leading company, Atrainability, to increase awareness of the role human factors plays in maintaining high reliability, resilience and safe practice. The course was designed to develop ‘culture carriers’ and help them understand: •how & why errors are made & how to avoid them •how to communicate more effectively •how to maintain team awareness •how to recognise early signs of error •how to reduce stress •how to conduct timely & effective team briefings •how to improve use of checklists •how to debrief for learning not blame •how to maintain safe practice The inclusion of Human Factors in training is nationally recognised as an essential requirement
Page 2 of 2816 Quality Report.pdfOverall Page 44 of 218

to help to learn from errors and take proactive steps to minimise similar events. This training was provided for 30 of the trust’s middle managers and a Board introductory session was also undertaken. The Head of Patient Safety and Clinical Risk will also be attending a trainers course during February which will support our sustainability in this methodology. A patient safety strategy was presented to QSC in January with Human Factors as a central theme for continuous quality improvement. 2.2 Standardising Equipment - Medical Devices The premise of DCHS Medical Devices policy is that staff should have standardised equipment to minimise error due to user unfamiliarity and reduce costs related to consumables; that any equipment which is either electrical or requires calibrating should have planned preventative maintenance which is tracked on Planet FM (Facilities Management). One element of the Medical Devices Group, Chaired by the Head of Patient Safety & Risk Management and supported by the Procurement; Estates and Training teams and attended by Operational staff representing all divisions is that equipment should show it has been matched for EASE characteristics i.e. Effective, Appropriate, Safe and cost Effective which is essential for safe delivery of care and an essential component of medical devices. NB The Safe Care team always check the evidence base for using any equipment which informs this process. The Medical Devices group identified a disparity of baseline equipment across DCHS. This was attributed to
1. the various different routes through which devices can be purchased which can lead to circumnavigating agreed procurement arrangements and lead to unapproved items being purchased i.e. equipment not listed on Medical Devices Approved list.
2. The belief by some teams that they do not have enough budget to spend on equipment.
3. Lack of reliable tracking of assets – leading to large number of items not being available for maintenance checks. This poses a clinical risk in that the equipment cannot be demonstrated as being safe. It additionally poses a financial risk because approximately £230K of equipment cannot be located.
Standardising Community Baseline Kit Work has been undertaken to provide community nurses and therapists with standardised baseline equipment contained in an ergonomic backpack. Trolley bags are also available. Staff are advised to undertake an ergonomic risk assessment before deciding on a suitable bag. The backpack has been chosen for its light weight, robustness and compartments for the various kit carried. Kit includes: Thermometer Sphygmomanometer & Stethoscope (An analogue sphyg for nurses and a digital sphyg for therapists) to meet varying skill levels for BP monitoring Face shield Dressing packs for nurses Hand hygiene kit with wipes The kit is currently being trialled before further large scale roll out and the support of Outstanding Way has been gained to consider the requirements to achieve this.
Page 3 of 2816 Quality Report.pdfOverall Page 45 of 218

2.3 Non Medical Prescribing (NMP) Background
In 2016 the 360 audit report on NMP identified significant shortfalls in governance and assurance for Non Medical Prescribing in DCHS. These included an absence of an up to date register of NMPs and a short fall in supervision of prescribing and prescribing support. In addition CQC report 2016 also noted a failure in recording FP10 prescription serial numbers. As part of the work to address and mitigate these concerns and to give assurance the new Head of Medicine Management working with the Deputy Chief Nurse designed, organised and introduced a NMP (V300) prescribing review.
NMP (V300) Prescribing Review Report
The first Non-Medical Prescribing (NMP) Annual Review events took over 6 weeks at the Strutts Centre Belper.
A total of 96% (149 out of 156) registered DCHS NMPs attended the event from a range of staff including, ACPs, Community Matrons, Health visitors, Community Nurses, Heart Failure Nurses, Physiotherapists and Podiatric Surgeons. Just 1 member staff failed to attend.
Prior to the event each delegate was sent a copy of their FP10 (EPACT) prescribing data and asked to complete a pro-forma relating to their prescribing practice, reflection and CPD. At the event each had a 1:1 meeting with an experienced doctor, pharmacist prescriber or other senior pharmacist to review and discuss this and other issues including de-prescribing and medication safety bulletins. Delegates also attended a 60 minute workshop /presentation covering, reflection, evidence based medicine, FP10 security and prescribing/ de-prescribing scenarios. Pharmacy staff were on hand to provide prescribing advice and support and to guide delegates to information stands, interactive computer programs and provide resources to take away eg Antibiotic guardianship, Stop Start App, list of useful prescriber websites.
Feedback on the event was received from 86% (129) delegates and was overall very positive. All of the delegates all thought the event very productive and enjoyed the interaction and learning with the delegates. Most importantly the feedback from the delegates was very good, see below, with some useful suggestions on how to improve the event.
Delegates were issued a certificate of attendance, with a copy of action to follow. Discussions are currently taking place with the training and education team on adding the Annual review as a mandatory event on ESR for NMPS.
Feedback
Overall Delegate rating:
86 % ranked the event good or very good (score 4 or 5) and 14% ranked the event average (score 3).
Page 4 of 2816 Quality Report.pdfOverall Page 46 of 218

The presentation and one to one session both ranked highly at 93 % and 89% respectively as good or very good (score 4 or 5)
Other comments generally included requests for more CPD events.
Non Attenders
Of the 7 non-attenders 5 are DCHS staff and 2 are bank workers. All managers have been alerted and delegates invited have been invited to attend a final session in January.
Forward plan
Discussions are underway to enable organisers to record the event on ESR and to repeat the event annually. A copy of each delegate’s 1 to 1 is to be scanned and emailed to them in order to remind delegates of advice and potential CPD. A similar event is planned for the 300 community nurse formulary prescribers ( V 100/150) in June.
2.4 Infection prevention and control During the winter period it is common to have outbreaks of Norovirus (winter vomiting bug) It is one of the most common causes of gastroenteritis characterised by vomiting diarrhoea and stomach pain and can be very debilitating especially in older people. It is highly contagious and therefore where we have suspected cases it is necessary for staff to restrict admissions immediately to contain and manage the incident. The information below details the specific incidents we have managed over the Christmas and New year period. It is thanks to the vigilance and quick actions of our clinical staff that the impact of these restrictions has been minimal. Hopewell Ward, Ilkeston Hospital 03/12/17-13/12/17 Norovirus – 10 patients affected across ward, 12 staff. 5 beds closed to admissions Operational hours lost – 172.5 (Agency/bank staff covered – 41.5 hrs, ward staff covered 146) Well managed, no concerns Source – possibly relative Heanor Ward, Ilkeston 31.12.2017 – 14.1.2018 Confirmed Norovirus. 10 patients affected, managed by closing bays to admissions as all patients in same areas. No vacant beds. Source and hours lost tbc Butterley Ward Ripley 2.1.2018 – 6.1.2018 Norovirus. 7 patients affected in different areas of ward. Beds closed to admissions 6. As each bay clear of symptomatic patients for 48 hours, cleaned and re-opened. Last bay re-opened 6.1.18 Source and hours lost tbc Oker Ward, Whitworth 2.1.2018 – 4.1.2018 3 patients affected, 1 bay closed to admissions – not norovirus, samples negative, bay reopened
Page 5 of 2816 Quality Report.pdfOverall Page 47 of 218

3. Clinical Effectiveness 3.1Leg Ulcer Champions As part of the trust’s work on reducing chronic wounds we have been given funding to support a number of fixed term posts working within the tissue viability team specifically managing leg ulcers. Early work from this programme has quickly evidenced how healing times can be reduced and patient outcomes improved when a standardised clinical pathway is utilised. Under the supervision of the lead nurse for lower limb conditions the leg ulcer champions will be working as part of clinical teams to train and advise staff on management of complex wounds, the use of Doppler equipment, application of a standardised clinical pathway, dressing choice and bandaging techniques. In tandem clinical staff will attend a two day leg ulcer management training programme and Band 6 team leaders will also attend health coaching sessions which have evaluated extremely well and which will impact on practise in a broad range of areas not just lower limb condition management. Supporting this work and the pressure ulcer reduction plan is a tissue viability strategy presented to QSC for approval in January. The Outstanding Way collaborative has supported data collection and analysis for this project which has helped to evidence the improvements. 4.Safer Staffing
Operational services are still reconciling staffing movements following ward movements and closures, additional funding for winter pressures and changes in staffing. As a consequence some of the graphs in appendix 1 appear to have more staff than required. Operational services have been asked to rectify this prior to next month’s publication of data. Currently we have two wards closed temporarily Hudson wad at Bolsover and Riverside ward at Newholme. Staff have been moved to Alton ward at Clay Cross and Rosely Ward at Newholme respectively. In addition the two OPMH wards at Walton hospital have been temporarily merged pending recruitment of new RNMH to ensure that we are meeting our safe staffing minimum levels. The acute beds in Learning disability services were temporarily increased by one due to demand and were supported by bank and agency staff to accommodate this. Wards are currently working at full winter numbers and have been supported by additional HCA staff and some use of bank and agency. Okeover ward at St Oswalds has increased by a further 6 beds over its winter target to accommodate additional pressures in the south of the county. This additional bed compliment has been managed with agency staff. Appendix 1 attached
Page 6 of 2816 Quality Report.pdfOverall Page 48 of 218

Monitoring Information Brief Summary
What are the Governor Involvement implications?
The Chief Nurse presents a paper covering the Quality Agenda reflected in this report to the Council of Governors. Governors may be involved in some of the pieces of work reported in this paper.
What are the Equality, Diversity and Inclusion implications?
Individual items within this report will have implications for Equality, Diversity and Inclusion. It is always possible to present the information in more accessible formats should this be required.
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
The report covers Clinical Quality which impacts on Patients, Public, staff and in many cases will have stakeholder implications.
Risk Register
Is the issue on the current Risk Register?
Yes/ No (Delete as appropriate)
If yes, what is the Risk Number? 3062
Does this update recommend a change in the current risk score? (If so, please provide your rationale below)
Yes/ No/ N/A (Delete as appropriate)
Page 7 of 2816 Quality Report.pdfOverall Page 49 of 218

1
January 2018
Data as at 31st December 2017
Prepared by: Quality & Business Services Team People and Organisational Effectiveness Department Tel no: 01246 253077 (option 3) Email: [email protected]
DCHS Safer Staffing Report
Page 8 of 2816 Quality Report.pdfOverall Page 50 of 218

1
Ash Green - Hillside …………………………………………………………………………………………………………………..3
Ash Green - Valley View …………………………………………………………………………………………………………………..4
Ash Green Site …………………………………………………………………………………………………………………..5
Babington Hospital - Baron …………………………………………………………………………………………………………………..6
Bolsover Hospital - Hudson …………………………………………………………………………………………………………………..7
Cavendish - Fenton …………………………………………………………………………………………………………………..8
Cavendish - Spencer …………………………………………………………………………………………………………………..9
Cavendish Hospital Site …………………………………………………………………………………………………………………..10
Clay Cross - Alton …………………………………………………………………………………………………………………..11
Ilkeston - Heanor …………………………………………………………………………………………………………………..12
Ilkeston - Hopewell …………………………………………………………………………………………………………………..13
Ilkeston Hospital Site …………………………………………………………………………………………………………………..14
Newholme - Riverside …………………………………………………………………………………………………………………..15
Newholme - Rowsley …………………………………………………………………………………………………………………..16
Newholme Hospital Site …………………………………………………………………………………………………………………..17
Ripley - Butterley …………………………………………………………………………………………………………………..18
St Oswald's - Okeover …………………………………………………………………………………………………………………..19
Walton - Linacre …………………………………………………………………………………………………………………..20
Walton - Melbourne …………………………………………………………………………………………………………………..21
Walton Hospital Site …………………………………………………………………………………………………………………..22
Whitworth - Oker …………………………………………………………………………………………………………………..23
Contents
Page 9 of 2816 Quality Report.pdfOverall Page 51 of 218

1
Late Night
Safe Staffing Minimum Numbers (based on funded establishment)
Ash Green - Hillside Ward Safer Staffing as at December 2017
2 2 1
Actual Staffing Number (reported above)
Early Late Night Early
4 3 2
RN 4 4 1 RN
HCA 5 5 3 HCA
83% 79%
113%
85% 85%
96%
84% 82%
100%
0%
20%
40%
60%
80%
100%
120%
E L N
Hillside Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
7
5
0
1
2
3
4
5
6
7
8
Hillside
Hillside Ward Bed Occupancy December 2017 - 73%
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 0% 0% 0% 0% 0%
Bank 0% 0% 0% 0% 0% 0%
Substantive 100% 100% 100% 100% 100% 100%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Hillside Ward - Bank and Agency Use December 2017
Substantive Bank Agency
0 0 0 0
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Hillside Bank and Agency use
Page 10 of 2816 Quality Report.pdfOverall Page 52 of 218

1
1 1 0
HCA 2 2 2 HCA 3 3 2
RN 0.5 0.5 0 RN
Ash Green - Valley View Safer Staffing as at December 2017
Actual Staffing Number (reported above) Safe Staffing Minimum Numbers (based on funded establishment)
Early Late Night Early Late Night
45% 45%
0%
60% 63%
66%
57% 59%
66%
0%
20%
40%
60%
80%
E L N
Valley View Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
5
0
0
1
2
3
4
5
6
Valley View
Valley View Ward Bed Occupancy December 2017 - 05%
0 0 0 0
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Valley View Bank and Agency use
Page 11 of 2816 Quality Report.pdfOverall Page 53 of 218

1
Hillside + Valley View
Ash Green Site Safer Staffing as at December 2017
79% 75%
113%
78% 78%
84%
78% 77%
89%
0%
20%
40%
60%
80%
100%
120%
E L N
Ash Green Site - 1st to 31st December 2017 % staffing against agreed staffing levels
Registered Staff % Non-registered % Overall %
12
5
0
2
4
6
8
10
12
14
Ash Green
Ash Green Site Bed Occupancy December 2017 - 45%
Page 12 of 2816 Quality Report.pdfOverall Page 54 of 218

1Babington Baron Ward Safer Staffing as at December 2017
Safe Staffing Minimum Numbers (based on funded establishment)
2 2HCA 3 2 2 HCA 3
RN RN
Actual Staffing Number (reported above)
Early Late Night Early Late Night
2 2 2 22 2
18 17
0
2
4
6
8
10
12
14
16
18
20
Available Max Avg. Bed No. for Month
Baron Ward Bed Occupancy December 2017 - 93%
13
82
2 2
0
10
20
30
40
50
60
70
80
90
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Baron Bank and Agency use
103% 103% 103% 105%
156%
105% 105%
130%
104%
0%
20%
40%
60%
80%
100%
120%
140%
160%
180%
E L N
Baron Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 2% 0% 2% 1% 0% 2%
Bank 2% 33% 3% 45% 16% 9%
Substantive 97% 67% 95% 54% 84% 89%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Baron Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 13 of 2816 Quality Report.pdfOverall Page 55 of 218

1
Late Night
Cavendish Hospital - Fenton Ward Safer Staffing as at December 2017
Safe Staffing Minimum Numbers (based on funded establishment)
2 2
Actual Staffing Number (reported above)
Early Late Night Early
3 2 1
RN 2 2 2 RN 2
HCA 3 2 1 HCA
102% 97%
102% 100%
113%
103% 101%
105% 102%
0%
20%
40%
60%
80%
100%
120%
E L N
Fenton Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
16
11
0
5
10
15
20
Fenton
Fenton Ward Bed Occupancy December 2017 - 65%
45
20
0 0
0
5
10
15
20
25
30
35
40
45
50
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Fenton Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 0% 0% 0% 0% 0%
Bank 24% 12% 30% 11% 19% 3%
Substantive 76% 88% 70% 89% 81% 97%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Fenton Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 14 of 2816 Quality Report.pdfOverall Page 56 of 218

1
2 2 2
HCA 2 2 2 HCA 2 2 1
RN 2 2 1 RN
Cavendish Hospital - Spencer Ward Safer Staffing as at December 2017
Actual Staffing Number (reported above) Safe Staffing Minimum Numbers (based on funded establishment)
Early Late Night Early Late Night
71% 68%
103%
79% 84%
97%
75% 76%
99%
0%
20%
40%
60%
80%
100%
120%
E L N
Spencer Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
10
2
0
2
4
6
8
10
12
Spencer
Spencer Ward Bed Occupancy December 2017 - 21%
13
19
0 0
0
2
4
6
8
10
12
14
16
18
20
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Spencer Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 0% 0% 0% 0% 0%
Bank 5% 18% 17% 17% 13% 2%
Substantive 95% 82% 83% 83% 88% 98%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Spencer Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 15 of 2816 Quality Report.pdfOverall Page 57 of 218

1
Spencer + Fenton
Cavendish Hospital Site Safer Staffing as at December 2017
86% 82%
102%
92%
98% 99%
89% 90%
101%
0%
20%
40%
60%
80%
100%
120%
E L N
Cavendish Hospital - 1st to 31st December 2017 % staffing against agreed staffing levels
Registered Staff % Non-registered % Overall %
26
13
0
5
10
15
20
25
30
Cavendish
Cavendish Hospital Bed Occupancy December 2017 - 48%
Page 16 of 2816 Quality Report.pdfOverall Page 58 of 218

1Clay Cross Hospital - Alton Ward Safer Staffing as at December 2017
2
2
2
2
HCA
RN
3
2
HCA
RN
Late Night
Safe Staffing Min Numbers (based on funded est)
2
2
2
2
3
2
Actual Staffing Number (reported above)
Early NightLate Early
103% 106% 100%
135%
158%
147%
123%
132% 123%
0%
20%
40%
60%
80%
100%
120%
140%
160%
180%
E L N
Alton Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
16 15
0
5
10
15
20
Available Max Avg. Bed No. for Month
Alton Ward Bed Occupancy December 2017 - 92%
5
18
1 1 0
5
10
15
20
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Alton Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 0% 2% 1% 0% 0%
Bank 2% 3% 3% 1% 3% 14%
Substantive 98% 97% 95% 98% 97% 86%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Alton Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 17 of 2816 Quality Report.pdfOverall Page 59 of 218

1Ilkeston Hospital - Heanor Ward Safer Staffing as at December 2017
Actual Staffing Number (reported above) Safe Staffing Minimum Numbers (based on funded establishment)
Early Late Night Early Late Night
2 2 2
HCA 3 3 2 HCA 3 2 1
RN 1.5 1.5 1 RN
151% 146%
158%
108% 99%
110%
122% 115%
126%
0%
20%
40%
60%
80%
100%
120%
140%
160%
180%
E L N
Heanor Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
18 17
0
5
10
15
20
Heanor
Heanor Ward Bed Occupancy December 2017 - 95%
0
10
0
3
0
2
4
6
8
10
12
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Heanor Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 0% 0% 0% 0% 4%
Bank 0% 5% 0% 0% 0% 7%
Substantive 100% 95% 100% 100% 100% 88%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Heanor Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 18 of 2816 Quality Report.pdfOverall Page 60 of 218

1
Actual Staffing Number (reported above)
Early Late Night Early Late Night
Safe Staffing Minimum Numbers (based on funded establishment)
Ilkeston Hospital - Hopewell Ward Safer Staffing as at December 2017
2 2 2
HCA 3 3 2 HCA 3 2 1
RN 1.5 1.5 1 RN
133% 135% 142%
102% 96%
105% 113%
109%
117%
0%
20%
40%
60%
80%
100%
120%
140%
160%
E L N
Hopewell Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
17
14
0
5
10
15
20
Hopewell
Hopewell Ward Bed Occupancy December 2017 - 84%
5
15
0
4
0
2
4
6
8
10
12
14
16
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Hopewell Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 0% 0% 4% 0% 0%
Bank 0% 5% 0% 7% 11% 6%
Substantive 100% 95% 100% 89% 89% 94%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Hopewell Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 19 of 2816 Quality Report.pdfOverall Page 61 of 218

1
Hopewell + Heanor
Ilkeston Hospital Site Safer Staffing as at December 2017
142% 141%
150%
105%
97%
107%
117% 112%
122%
0%
20%
40%
60%
80%
100%
120%
140%
160%
E L N
Ilkeston Hospital - 1st to 31st December 2017 % staffing against agreed staffing levels
Registered Staff % Non-registered % Overall %
35
31
0
5
10
15
20
25
30
35
40
Ilkeston
Ilkeston Hospital Bed Occupancy December 2017 - 90%
Page 20 of 2816 Quality Report.pdfOverall Page 62 of 218

1
2 2
HCA 2 2 1 HCA 3 2 1
RN 2 2 2 RN 2
Newholme Hospital - Rowsley Ward Safer Staffing as at December 2017
Actual Staffing Number (reported above) Safe Staffing Minimum Numbers (based on funded establishment)
Early Late Night Early Late Night
103% 103% 103%
166%
124%
206%
135%
114%
138%
0%
20%
40%
60%
80%
100%
120%
140%
160%
180%
200%
220%
E L N
Rowsley Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
16
14
0
5
10
15
20
Rowsley
Rowsley Ward Bed Occupancy December 2017 - 85%
48
24
0 0
0
10
20
30
40
50
60
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Rowsley Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 0% 0% 0% 0% 0%
Bank 17% 9% 30% 10% 28% 11%
Substantive 83% 91% 70% 90% 72% 89%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Rowsley Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 21 of 2816 Quality Report.pdfOverall Page 63 of 218

1
Rowsley + Riverside
Newholme Hospital Site Safer Staffing as at December 2017
52% 52%
69%
83%
62%
69% 67%
57%
69%
0%
20%
40%
60%
80%
100%
E L N
Newholme Hospital - 1st to 31st December 2017 % staffing against agreed staffing levels
Registered Staff % Non-registered % Overall %
16
14
0
2
4
6
8
10
12
14
16
18
Newholme
Newholme Hospital Bed Occupancy December 2017 - 85%
Page 22 of 2816 Quality Report.pdfOverall Page 64 of 218

1
Late Night
Ripley Hospital - Butterley Ward Safer Staffing as at December 2017
Safe Staffing Minimum Numbers (based on funded establishment)
2 2
Actual Staffing Number (reported above)
Early Late Night Early
3 2 2
RN 2 2 2 RN 2
HCA 3 3 2 HCA
102% 102% 103%
117%
109% 103%
111% 106% 103%
0%
20%
40%
60%
80%
100%
120%
140%
E L N
Butterley Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
18 17
0
5
10
15
20
Butterley
Butterley Ward Bed Occupancy December 2017 - 91%
8
2
0
1
0
1
2
3
4
5
6
7
8
9
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Butterley Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 0% 0% 1% 0% 0%
Bank 0% 1% 2% 0% 11% 2%
Substantive 100% 99% 98% 99% 89% 98%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Butterley Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 23 of 2816 Quality Report.pdfOverall Page 65 of 218

1
HCA 3 2 2
Night
RN 2 2 2
St Oswald's Hospital - Okeover Ward Safer Staffing as at December 2017
HCA 3 2 2
RN 2 2 2
Actual Staffing Number (reported above) Safe Staffing Minimum Numbers (based on funded establishment)
Early Late Night Early Late
103% 102% 103% 108%
150%
105% 106%
126%
104%
0%
20%
40%
60%
80%
100%
120%
140%
160%
E L N
Okeover Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
19
16
0
5
10
15
20
Okeover
Okeover Ward Bed Occupancy December 2017 - 86%
22
51
12 7
0
10
20
30
40
50
60
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Okeover Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 6% 1% 8% 3% 5% 5%
Bank 13% 19% 10% 30% 13% 6%
Substantive 81% 80% 83% 67% 83% 89%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Okeover Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 24 of 2816 Quality Report.pdfOverall Page 66 of 218

1
RN Nights 1.5 on both Linacre & Melbourne. 3 across site alternating 2, 1 ward, 1 other
RN 3 3 2
Late Night Early Late Night
Walton Hospital - Linacre Ward Safer Staffing as at December 2017
HCA 4 4 3
RN 2 2 1.5
HCA 5 5 4
Actual Staffing Number (reported above) Safe Staffing Minimum Numbers (based on funded establishment)
Early
103% 98% 101%
127% 131% 128%
119% 120% 119%
0%
20%
40%
60%
80%
100%
120%
140%
E L N
Linacre Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
16
13
0
5
10
15
20
Linacre
Linacre Ward Bed Occupancy December 2017 - 80%
14
72
0
9
0
10
20
30
40
50
60
70
80
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Linacre Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 3% 0% 2% 0% 0%
Bank 6% 15% 0% 11% 21% 26%
Substantive 94% 82% 100% 86% 79% 74%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Linacre Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 25 of 2816 Quality Report.pdfOverall Page 67 of 218

1
Night
RN Nights 1.5 on both Linacre and Melbourne. 3 across site alternating 2, 1 ward, 1 other
RN 3 2 2
HCA 4 4 3
Walton Hospital - Melbourne Ward Safer Staffing as at December 2017
HCA 4 4 3
RN 2 2 1.5
Actual Staffing Number (reported above) Safe Staffing Minimum Numbers (based on funded establishment)
Early Late Night Early Late
110% 103%
86%
123%
130% 131%
118% 121% 116%
0%
20%
40%
60%
80%
100%
120%
140%
E L N
Melbourne Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
16 15
0
5
10
15
20
Melbourne
Melbourne Ward Bed Occupancy December 2017 - 91%
6
53
0 2
0
10
20
30
40
50
60
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Melbourne Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 1% 0% 0% 0% 0%
Bank 1% 8% 2% 14% 10% 16%
Substantive 99% 91% 98% 86% 90% 84%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Melbourne Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 26 of 2816 Quality Report.pdfOverall Page 68 of 218

1
Linacre + Melbourne
Walton Hospital Site Safer Staffing as at December 2017
106%
101%
94%
125%
130% 130%
119% 120% 118%
0%
20%
40%
60%
80%
100%
120%
140%
E L N
Walton Hospital - 1st to 31st December 2017 % staffing against agreed staffing levels
Registered Staff % Non-registered % Overall %
32
27
0
5
10
15
20
25
30
35
Walton
Walton Hospital Bed Occupancy December 2017 - 86%
Page 27 of 2816 Quality Report.pdfOverall Page 69 of 218

1
HCA 3 2 2
Night
RN 2 2 2
Whitworth Hospital - Oker Ward Safer Staffing as at December 2017
Early Late Night
HCA 3 2 2
RN 2 2 2
Actual Staffing Number (reported above) Safe Staffing Minimum Numbers (based on funded establishment)
Early Late
103% 105% 103%
141% 148%
152%
126% 127% 127%
0%
20%
40%
60%
80%
100%
120%
140%
160%
E L N
Oker Ward - 1st to 31st December 2017 % staffing against agreed staffing levels Registered Staff % Non-registered % Overall %
19
16
0
5
10
15
20
25
Oker
Oker Ward Bed Occupancy December 2017 - 84%
10
49
0
13
0
10
20
30
40
50
60
RN HCA RN HCA
Shifts Filled by Bank Shifts filled by Agency
Oker Bank and Agency use
RN Early HCA Early RN Late HCA Late RN Night HCA Night
Agency 0% 2% 0% 5% 0% 6%
Bank 0% 5% 3% 17% 13% 29%
Substantive 100% 94% 97% 77% 88% 65%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oker Ward - Bank and Agency Use December 2017
Substantive Bank Agency
Page 28 of 2816 Quality Report.pdfOverall Page 70 of 218

TRUST BOARDDocument Title: Raising Concerns
Presenter/Title: Kirsteen Farrar, Associate Director of Corporate Governance/Trust Secretary
Contents of Paper were previously discussed by:
Author/Title:Kirsteen Farrar, Associate Director of Corporate Governance/Trust SecretaryNicola Erin Walker, Governance and Membership Officer
Contact Email and Telephone Number: [email protected]
Date of Meeting: 25 January 2018 AgendaItem No: 17/18
No of pagesinc. this one: 9
Has an Equality Impact Assessment been undertaken Yes No
Document is for:(more than one box can be ticked) Information Decision Assurance
Purpose of Paper
The purpose of this paper is to provide information regarding Raising Concerns, known nationally as Freedom to Speak Up (FTSU) and the progress made within DCHS in ensuring we have mechanisms in place to enable staff to feel confident to raise any issues as they arise.
Additionally the National Guardians Office (NGO) who are responsible for supporting organisations and individuals regarding FTSU have recently published the findings from their second survey and their Annual Report. A summary of the findings are detailed below.
Recommendations
The Board is asked to note the progress made and take assurance that activities are in place to develop a culture which enables staff to ‘speak up’.
Board Assurance Framework Risk Reference
2.2 There is a risk to patients, service-users and employees due to staff performance and behaviours not being monitored and improved resulting in an adverse impact on the provision of high quality care and organisational reputation
2.5 There is a risk to service users, staff and DCHS’ reputation due to staff not adhering to the principles of an equal, diverse and inclusive culture, resulting in discriminatory and non-inclusive behaviours, non-compliance with Equality Act and potential legal costs
4.1 There is a risk to the organisation due to not having strong corporate governance systems in place resulting in Trust vision not being delivered
Page 1 of 917 Raising Concerns.docxOverall Page 71 of 218

Financial Impact
There is no direct financial impact linked to this report.
Further Information and Appendices
Background: The role of National Guardian was established following the Francis Freedom to Speak Up Review in 2015, which looked into how NHS workers should be better supported to raise concerns.
The National Guardian Office (NGO) provides leadership and advice for Freedom to Speak Up Guardians (also known as Local Guardians) based in NHS trusts and NHS foundation trusts on best practice to enable staff to speak up safely.
The NGO has produced a 2017 Annual report which can be viewed at http://www.cqc.org.uk/sites/default/files/20171115_ngo_annualreport201617.pdf
In September 2017, the National Guardian, Dr Henrietta Hughes, published a set of recommendations for trust leaders based on the findings of a survey of guardians, champions and ambassadors.
The recommendations for the role include: Ring-fenced time to enable guardians properly to meet the needs of workers All workers, particularly the most vulnerable, should have effective routes to enable them to
speak up Boards need to hear regularly from their guardian, in person
DCHS already meet these recommendations, however it is acknowledged that a continued communications campaign is essential to ensure staff throughout DCHS are aware of the different channels that are available to enable them to raise concerns.
The NGO have released a case review process for NHS Trusts and Foundation Trusts following the review at Southport and Ormskirk Hospital NHS Trust which can be viewed at http://www.cqc.org.uk/sites/default/files/20170612_ngo_case_review_summary.pdf
Local Action and issues:
In addition to the existing resources and support that are in place we are looking at how we can further embed Raising concerns within DCHS by implementing the following:
Staff e-learning package Development of training for managers on how to respond to concerns Production of a series of animated awareness videos Awareness sessions at relevant meetings and groups such as Frontline Care Council and
Myriad Voices Attending Patient Safety Roadshows and Production of promotional items for staff which
will include ‘credit cards’ providing easy access to key information.
Within DCHS there are many mechanisms through which concerns can be raised in addition to
Page 2 of 917 Raising Concerns.docxOverall Page 72 of 218

the more formal ‘Raising a Concern ‘ process. We are currently collating some examples and case studies which it is hoped by sharing may encourage staff to feel confident to raise any concerns they have.
Summary of FTSU concernsDCHS have received 7 concerns during quarter two and three of 2017-18. See Appendix 1 for further details.
Monitoring Information Brief Summary
What are the Governor Involvement implications?
Staff Governors are encouraged to support staff in raising any concerns they may have.
What are the Equality, Diversity and Inclusion implications?
EDI implications are considered within the individual aspects of the report and adjustments made where appropriate
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
The initiatives detailed in this paper relate to all DCHS staff
Risk Register
Is the issue on the current Risk Register? No If yes, what is the Risk Number?
Does this update recommend a change in the current risk score? (If so, please provide your rationale below)
N/A
Page 3 of 917 Raising Concerns.docxOverall Page 73 of 218

Appendix 1Summary of Freedom to Speak Up (FTSU) Concerns
ThresholdTo enable DCHS to gain assurance that staff feel able to report concerns, a key performance indicator is to be agreed on the number of concerns received each quarter. This is proposed at no less than 2 but no more than 8. If we receive numbers outside of these parameters, a review will be undertaken to establish if staff are starting to experience barriers to reporting or whether it indicates there may be specific issues that need further investigation.
Date Period Quarter Number of ConcernsApr - Jun 16 1 2 Jul - Sept 16 2 3Oct - Dec 16 3 4Jan - Mar 17 4 1Apr - Jun 17 1 4Jul – Sept 17 2 5Oct – Dec 17 3 2Total 21
Concerns per division No. of concerns
(%)
No. of staff % of staff allocation
Integrated Community Services
12 (57%) 2342 53%
Health Wellbeing & Inclusion 4 (19% 556 13%Planned Care 3 (14%) 726 16%Quality 0 (0%) 140 3%Corporate 2 (10%) 659 15%Total 21 4423 100%
Page 4 of 917 Raising Concerns.docxOverall Page 74 of 218

Who is speaking up?
Based on the total national responses, this is a breakdown of those who declared a profession.
% recorded cases reportedQ1 Q2
Profession
Nationally Nationally DCHSFTNurses 29% 31% 40%AHPs 15% 15% 20%Administrative/Clerical staff
13% 17% 20%
Healthcare Assistants 9% 6% None reportedDoctors 8% 6% None reportedCorporate service staff 7% 6% None reportedMidwives 8% 2% Not applicableBoard members 0.5% <0.5% None reportedDentists <0.5% <0.5% None reportedCleaning/catering/ maintenance/ancillary staff
Not reported 4% None reported
Other 10% 11% *20%*Anonymous reports
The reason why DCHS comparator in this table is provided as a 6 month period, is because the numbers reported would not provide a contextual comparison if presented in quarters. The table above demonstrates that DCHS Nurses raise more concerns than other professions, proportionally nurses account for 31.18% of DCHS workforce.
Page 5 of 917 Raising Concerns.docxOverall Page 75 of 218

What’s the feedback?It is a requirement for all trusts to gain feedback when asked ‘Given your experience, would you speak up again?’ there has nationally been a positive response. The implementation of our feedback form will assist DCHS in better understanding staff’s experiences.
% recorded 2017/18 In Q1 & Q2Given your experience, would you speak up again? Nationally DCHSFT
Yes 89 2No 2 0Maybe 5 0Don’t know 4 0
Nationally common themes in the feedback that workers gave included: Feeling empowered to escalate issues on their own after speaking to a Guardian Being listened to and supported during a difficult time Appreciation of the independence and confidentiality that a Guardian could offer Being asked to feedback Feeling that they were being taken seriously
Challenging themes to the feedback, including: Investigations taking too long Pessimism that anything would change as a result of speaking up Worries about repercussions
National Learning points connected to the FTSU processes: The importance of responding to issues as soon as possible after they are raised – this gives confidence to workers that they
are being listened to and taken seriously Communication between staff and managers
Page 6 of 917 Raising Concerns.docxOverall Page 76 of 218

Regional and National Context
The following two charts display the regional FTSU Quarter 2 data and also comparative national data from community trusts who are defined as medium as per DCHS
East Midlands region Quarter 2 statistical comparison
Trust Name Type of trust Size of trust
Number of cases raised to FTSU in the Trust
Number of these cases raised anonymously
Number of cases with an element of patient safety/quality
Number of cases with an element of bullying / harassment
Number of cases where people indicate that they are suffering detriment as a result of speaking up
Chesterfield Royal Hospital NHS Foundation Trust
Acute Small 19 1 11 12 3
Derby Teaching Hospitals NHS Foundation Trust
Acute Medium 26 0 1 25 9
Derbyshire Community Health Services NHS Foundation Trust
Community Medium 5 1 0 4 0
Derbyshire Healthcare NHS Foundation Trust
Mental health / learning disability
Small 0 0 0 0 0
East Midlands Ambulance Service NHS Trust
Ambulance Small 11 2 3 4 3
Leicestershire Partnership NHS Trust
Combined mental health / learning disability / community
Medium 14 6 10 3 0
Page 7 of 917 Raising Concerns.docxOverall Page 77 of 218

Trust Name Type of trust Size of trust
Number of cases raised to FTSU in the Trust
Number of these cases raised anonymously
Number of cases with an element of patient safety/quality
Number of cases with an element of bullying / harassment
Number of cases where people indicate that they are suffering detriment as a result of speaking up
Lincolnshire Community Health Services NHS Trust
No data received
Lincolnshire Partnership NHS Foundation Trust
Mental health / learning disability
Small 7 3 3 2 0
Milton Keynes University Hospital NHS Foundation Trust
Acute Small 10 10 4 6 0
Northampton General Hospital NHS Trust
Acute Small 9 4 2 2 1
Northamptonshire Healthcare NHS Foundation Trust
Combined mental health / learning disability / community
Small 14 1 5 0 0
Nottingham University Hospitals Trust
Acute Large 15 3 0 3 1
Nottinghamshire Healthcare NHS Foundation Trust
Combined mental health / learning disability / community
Medium 33 29 4 12 2
Sherwood Forest Hospitals NHS Foundation Trust
No data received
United Lincolnshire Hospitals NHS Trust
Acute Medium 4 1 0 4 2
University Hospitals of Leicester NHS Trust
Acute Large 40 13 13 8 0
Page 8 of 917 Raising Concerns.docxOverall Page 78 of 218

DCHSFT comparison with similar size Community Trusts
Trust Name Size of trust(Small <5k)(Medium 5-10k)
Number of cases raised to FTSU in the Trust
Number of these cases raised anonymously
Number of cases with an element of patient safety/quality
Number of cases with an element of bullying / harassment
Number of cases where people indicate that they are suffering detriment as a result of speaking up
Bridgewater Community Healthcare NHS Foundation Trust
Small 1 1 1 1 0
Cambridgeshire Community Services NHS Trust
Small 3 1 0 1 0
Central London Community Healthcare NHS Trust
Small 25 18 8 21 0
Cumbria Partnership NHS Foundation Trust
Small 0 0 0 0 0
Derbyshire Community Health Services NHS Foundation Trust
Medium 5 1 0 4 0
Gloucestershire Care Services NHS Trust
Small 7 0 5 3 0
Hertfordshire Community NHS Trust Small 2 0 1 1 0Hounslow and Richmond Community Healthcare NHS Trust
Small 8 0 7 0 0
Kent Community Health NHS Foundation Trust
Medium 9 0 5 4 0
Leeds Community Healthcare NHS Trust Small 9 10 11 11 0Sussex Community NHS Foundation Trust
Small 22 1 17 6 0
Wirral Community NHS Foundation Trust Small 14 1 11 1 0
Page 9 of 917 Raising Concerns.docxOverall Page 79 of 218

Overall Page 80 of 218

TRUST BOARD Document Title: Performance Report
Presenter/Title: Chris Sands, Director of Finance, Information and Strategy Contents of Paper were previously discussed by:
Author/Title: David Caddy, Senior Management Accountant - Performance and Costing
Contact Email and Telephone Number: [email protected] 01246 253042
Date of Meeting: 25 January 2018 Agenda Item No: 18/18
No of pages inc. this one: 26
Has an Equality Impact Assessment been undertaken Yes No
Document is for: (more than one box can be ticked) Information x Decision Assurance x
Purpose of Paper
The purpose of this paper is to present the Board Performance Report. The Performance Report sets out a summary of Derbyshire Community Health Services (DCHS) performance against the three DCHS Way focus areas of Quality People, Quality Service and Quality Business. The Balanced Scorecard has been reviewed to incorporate the contractual and other performance regime changes in 2017/18. There are 19 green, 7 amber, 4 red, and 1 unrated indicators this month.
Recommendations
Note and comment.
Board Assurance Framework Risk Reference
References 1.1 , 1.4 , 1.6 , 1.7 , 2.1 , 2.2 , 2.3 , 2.4 , 3.6 , 3.1 , 3.2 , 3.4 , 3.5 , 3.6 , 3.7 , 3.8 , 3.9 , 3.10 , 4.1 , 4.5 , 4.6 , 4.7
Financial Impact
The report contains a number of issues and risks that have a financial impact on the organisation.
Further Information and Appendices
Report attached
Page 1 of 2618 Performance Report.pdfOverall Page 81 of 218

Monitoring Information Brief Summary
What are the Governor Involvement implications? The Council of Governors receive performance reports
What are the Equality, Diversity and Inclusion implications?
Equality, Diversity and Inclusion measurements are recorded in the report
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
The report includes measurements of service experienced by patients
Risk Register
Is the issue on the current Risk Register? No If yes, what is the Risk Number?
Does this update recommend a change in the current risk score? (If so, please provide your rationale below) No
Page 2 of 2618 Performance Report.pdfOverall Page 82 of 218

Board Performance Report – December 2017 Background The Board Performance Report sets out a summary of Derbyshire Community Health (DCHS) performance against the three DCHS Way focus areas of Quality People, Quality Service and Quality Business. Section Index Document Page Number 1.1 - Executive Summary 2-6 2.1 - Performance Dashboard 7-8 3.1 - Quality Service Narrative 9 4.1 - Quality People Narrative 10 5.1 - Quality Business Narrative 12 6.1 - Appendix 1 - Exception Reports 13-22 7.1 - Appendix 2 - CQUIN 23 8.1 - Appendix 3 – NHSI Quality Dashboard 24
Page 3 of 2618 Performance Report.pdfOverall Page 83 of 218

1.1 - EXECUTIVE SUMMARY Key Issues The key issues for the Board to discuss are: Data quality kitemark scores are now shown. Scores will be reviewed and revised in future months.
Quality Service • The Commissioning for Quality and Innovation (CQUIN) report is presented at
page 23. There was one red area on the CQUIN indicators shedule. This was against the improvement of our staff survey score. An exception report is enclosed at page 13.
• Inpatient Length of stay for December was 17.3 days and 18.1 days for the
rolling 3 month figure. This is green rated against an aspirational target of 20 days for the month.
• There were no falls reported on Strategic Executive Information System
(STEIS) in December. For the year to date we have had 4 falls. This measure has been green rated against our year to date improvement target of 7 falls.
• There were 7 avoidable grade 2, 3 & 4 pressure ulcers ulcers were there have been lapses in care were recorded for the month. The year to date improvement target is 23 against a year to date actual of 50. This has been red rated. 7 of the monthly cases are in a community setting & none are in an inpatient setting. An improvement target of 34 has been developed for the year.
Page 4 of 2618 Performance Report.pdfOverall Page 84 of 218

The actual month of occurrence is shown below:
An exception report is enclosed at a page 14. The improvement trajectory for 2018/19 will be reviewed with the Chief Nurse as part of the review of the metrics for the new financial year
• The overall occupancy rate for Inpatient wards in December was 83.1% against a target of 85%.
• The Big 9 measure, for the identification of carers on TPP who access our services, is currently red rated. In December we identified 1,420 carers against a revised year to date target of 2,000 carers. An exception report is presented at page 15.
• The Big 9 measure, for nurses who have completed insulin training, is currently red rated. In December we identified 433 nurses against a re-profiled year to date target of 546 nurses. The total target of 715 nurses for the year has now been re-profiled over the full year rather than from April to December. An exception report is presented at page 16.
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 TotalsOccurrence
Feb-17 1 1 3 5Mar-17 1 2 3Apr-17 5 1 1 1 8May-17 1 2 1 1 2 7Jun-17 2 6 1 9Jul-17 1 2 1 4
Aug-17 1 1 1 3Sep-17 2 2Oct-17 2 4 6Nov-17 1 2 3Dec-17 0
Totals 2 3 9 5 9 2 6 7 7 50
Avoidable Grade 2,3, 4 Pressure Ulcers and Suspected Deep Tissue Injuries 2017/18
Reporting Month
Page 5 of 2618 Performance Report.pdfOverall Page 85 of 218

Quality People • Staff Attendance was 94.58% (95%) against a target of 97% and 95.01%
(95%) for the average of the past 12 months.
• There was 1 Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR) Zero Harm event in December. The year to date position is 16 occurrences against an improvement target of 13. This has been amber rated.
• Agency costs were at £0.59m for the year to date. The year to date target is
£1.04m. This has been green rated.
• The Essential Learning rate for December was 89.74% (90%) against a target of 96%. This has been red rated. An exception report is enclosed at page 17. This metric now includes all 7 Essential Learning topics, rather than excluding Fire Safety and Information Governance training, which has been the case previously.
• The Appraisals rate for December was 90.31% (90%) against a target of 96%. This has been red rated. An exception report is enclosed at page 18.
• The New Starters Attending Induction rate for December was 97.06% (97%)
against a target of 96%. This has been Green rated.
• December’s year to date Big 9 figure of 102 Health and Safety near misses has been green rated against our year to date target of at least 101 near misses recorded.
• Safeguarding & Resuscitation measures for December were:
•92.38% (92%) of clinical staff have completed Resuscitation Training. •89.67% (90%) have completed Safeguarding Children Level 2 •75.29% (75%) have completed level 3, where this is required for their role. •90.82% (91%) have completed Safeguarding Adults level 2. •88.88% (89%) have completed WRAP training. •66.70% (67%) have completed Prevent training. An exception report is enclosed at page 19.
Quality Business
• The Sustainable Quality Improvement Plan (SQIP) stood at 5,280k (73.3%) for December against at target of £5,278k (73.3%). This has been green rated. Details have been discussed in the Finance Report.
Page 6 of 2618 Performance Report.pdfOverall Page 86 of 218

• The overall Delayed Transfer of Care (DToC) score for December was
5.6% against a revised NHS England target of target of 3.5%.This has been red rated.
This is made up of: (i) An OPMH Delayed Transfer of Care element in December of 4.1%
against an NHS England target of 3.5% which is red rated. (ii) An inpatients Delayed Transfer of Care element for December of
5.9% against an NHS England target of 3.5% for December which is red rated.
The overall December score of 5.6% can also be summarised as: (i) 3.8% for delays under DCHS control against an internal
improvement target of 3.2%.
(ii) 1.6% delays under social care control against an internal improvement target of 4.9%.
(iii) 0.2% delays under both organisations
An exception report is enclosed at page 20.
• Information Management & Technology (IM&T) measures have been amended to show Electronic Records Coverage Across DCHS & Electronic Point of Care Recording. Electronic Records Coverage Across DCHS is at 76.8% (77%) against a target of 70%. This has been green rated. Electronic Point of Care Recording is at 65.3% (65%) against a target of 66%. This has been amber rated.
• The month 9 contract activity information from SLAM is being reviewed with the services. Exception reports for Physiotherapy & Non AQP Community Podiatry are enclosed at pages 21 & 22.
Quality Governance
• Our Governance rating is green rated. We are currently meeting all our Risk Assurance Framework targets and are forecasting to maintain our green rating for the year.
Page 7 of 2618 Performance Report.pdfOverall Page 87 of 218

• Page 24 sets out benchmarking from NHS Improvement (NHSI) of the Trust’s
performance against a number of metrics used against the CQC Well Led Framework. The Board will note that the Trust benchmarks well across most of these metrics.
Page 8 of 2618 Performance Report.pdfOverall Page 88 of 218

DCHS Board Performance Report 2017/18Kitemark
ScoreMonth
Month December Current Current Trend Plan for Month Outturn PlanOutturn Forecast
Benchmark Notes
QUALITY SERVICE
Friends and Family Score 16 98.1% 98.1% 98% 98% 97% 96%
Length of Stay 18 17.3 18.1 20 20 20 Inpatients
Occupancy 18 83.1% 83.1% 85% 85% 83% 75%-85%
Information Sharing - 89.2% 89.2% 90% 90% 89%
RTT Admitted 16 93% 93% For
InformationFor
Information93% For information - no longer reported
nationally
RTT Non Admitted 16 95% 95% 92% 92% 95%
A&E 4 Hr Wait 16 99.9% 99.9% >95% >95% 100% >95% National target
Harm Free Care 11 92.7% 92.1% 94% 94% 93%
Pressure Ulcers 12 7 50 26 34 75 Community = 7. Inpatients = 0
% of Qualified Shifts Covered 13 85% 85% 80% 80% 84%
Falls Resulting in Severe Injury 16 0 4 7 9 9
Never Events 16 0 0 0 0 0
Outturn
CARING
EFFECTIVE
RESPONSIVE
SAFE
Year to Date
Page 9 of 2618 Performance Report.pdfOverall Page 89 of 218

DCHS Board Performance Report 2017/18Kitemark
ScoreMonth
Month December Current Current Trend Plan for Month Outturn PlanOutturn Forecast
Benchmark Notes
OutturnYear to Date
QUALITY PEOPLE
Appraisal Rate 13 90.3% 90.3% 96% 96% 95.1% 90%
Attendance Rate 13 94.6% 95.0% 97% 97% 95.4%
Engagement Index - 78 78 75 75 78
RIDDOR Reported Injuries - 1 16 13 17 17
Mandatory Training Compliance 13 90% 90% 96% 96% 90% 90% Now 7 facets not 5
Agency Costs as percentage of Paybill (£m) 13/15 0.05 0.59 1.04 1.46 0.67 3% calculation - £1.46m for 17/18
QUALITY BUSINESS
I&E Surplus 15 -5,961 -5,961 -5,834 -4,923 -4,489
Cash 15 23,599 24,801 20,098 21,418 23,528
Sustainable Quality Improvement Plan 15 5,280 5,280 5,278 7,200 7,256
Delayed Transfer of Care 18 5.6% 7.8% 3.5% 3.5% 5.5% 6.0% NHS England target. Monthly NHS 3.3%. Social 0.3%. Both 0.2%
NHSI Single Oversight Framework (SOF) - Green Green Green Green Green
Information Sharing - 89% 89% 90% 90% 89%
Electronic Records Across DCHS - 76.8% 76.8% 70% 70% 77% TPP used
Electronic Point of Care Recording - 65% 65% 66% 66% 65% TPP used
Estate Utilisation 14 7% 7% 6% 6% 7% 6% Proportion of space unoccupied (%). Plan = ERIC 16/17 (Community)
QUALITY GOVERNANCE
NHS England Quality Surveillance Rating - Green Green Green Green Green
Governance Rating - Green Green Green Green Green
AMHAM Audits - 0 4 4 8 8 Associate Mental Health Act Manager
AMHAM Audit Results - Significant Assurance - 100% 100% 100% 100% 100%
Page 10 of 2618 Performance Report.pdfOverall Page 90 of 218

3.1 – QUALITY SERVICE NARRATIVE During month 9 good progress continues on the majority of quality metrics, especially bed occupancy and lengths of stay which have not been impacted upon as a result of winter pressures. • Achievement of CQUIN targets remains challenging. • Analysis of the staff survey is currently being undertaken regarding the staff welfare questions. Good progress has been made against the flu vaccination campaign with 60% of staff (our highest total ever) having been achieved. • Proactive discharge is still at risk of achievement due to its cross organisational nature and failure to agree definition with CCGs. • Personalised care evaluation presents a challenging proposition due the high numbers of patients that have to be contacted and interviewed. Quarterly performance review with NHSI did not raise any specific issues related to quality, assurance was provided regarding focus on flu vaccinations and activity management. Routine quality surveillance meeting was held with the CQC in month with no specific concerns raised by the CQC.
Page 11 of 2618 Performance Report.pdfOverall Page 91 of 218

4.1 – QUALITY PEOPLE NARRATIVE Agency spend for the year to date is currently £0.45m below NHSI year to date target of £1.04m. The biggest area of spend is within registered nursing. This is in line with the national picture. Community Nursing agency costs are increasing. Agency for General Practitioners has reduced throughout the year due to successful vacancy recruitment and the development of a bank staff solution. There is a nat ional focus on Winter Pressures as we now enter the most difficult period of the year. Essential Learning continues a four month positive trend, rising again in December to 89.74% (90%) but remains nearly 6.3% below December's target of 96%. Appraisals show a 2.4% increase from last month (87.95% to 90.31%) but remains below December's 96% target. The continued focussed work on “Better Care Closer to Home” has resulted in lower vacancies going out to external advert. Vacancies are reviewed for employees requiring re-deployment before being advertised externally. The absence rate has dropped slightly this month to 5.42% (Attendance Rate 94.58%). Work continues with our Flu and Well Being Programmes and there is continued focus on MSK injuries. The Trust’s Headcount and FTE have dropped this month by 154 an d 123 respectively. TUPE transfers out to other organisations included Health Promotion, Dental & Health Wellbeing & Inclusion Management. We continue to review the Health and Safety arrangements in place across DCHS. Injury and ne ar miss reporting continues to identify a nu mber of topics with significant incident numbers, including violence and aggression, lifting and handling, slips, trips and falls, needlestick injuries and contact with hazards. All RIDDOR incidents are investigated by the Health and Safety team. We will look at assisting managers with their investigating process for minor injuries and near misses. We are able to confirm that DCHS has registered for Gender Pay Gap reporting via the Government Equalities Office in preparation for 30th March 2018 deadline. Further updates will follow.
Page 12 of 2618 Performance Report.pdfOverall Page 92 of 218

We have vaccinated 2,127 of 3,514 staff, which equates to 60.5% (61%) of frontline staff as at 12th January 2018. More clinics are planned for the middle of January & we would expect the vaccination figure to rise, which would place us nearer to meeting our CQUIN target. We continue to promote the flu vaccination message with our clinical colleagues.
Page 13 of 2618 Performance Report.pdfOverall Page 93 of 218

5.1 – QUALITY BUSINESS NARRATIVE The financial position at month 9 is showing a surplus of £5.96m, which represents a favourable variance to plan of £0.13m. The SQIP is on plan at month 9. The cash balance was £23.6m, which is £2.7m ahead of plan. The month 9 financial position includes the contract agreement reached with commissioners. This fixes the year end contract value, and therefore removes any risk around CQUIN and cost per case income. The forecast outturn position is a surplus of £4.92m which means we are planning to achieve our control total set by NHS Improvement. Our Finance and Resources Rating remains at 1 (low risk). Capital spend is £5.87m against a plan of £5.48m an overspend of £0.39m. The land at Buxton has now been purchased which has led to the increase in expenditure. We expect to spend the full £6.4m plan by the end of the financial year. The Delayed Transfers of Care performance in December was 5.6%. After 3 months of improvement, the position has deteriorated in December by 1.8%. The new systems introduced are having an impact on reducing delays, and we will monitor the position closely to ensure this improvement is sustained.
Page 14 of 2618 Performance Report.pdfOverall Page 94 of 218

Measure2017/18 Full Year Target
YTD Target Oct-17 Nov-17 Dec-17 YTD
CQUIN (rating)
Exception Report Analysis
1. Health and Wellbeing CQUIN - Improvement of 5% points required on staff survey questions related to reduction in work related stress and Trust taking positive action on health and wellbeing. BCCTH impact may result in non-achievement of 3% increase in staff survey, resulting in no payment. Risk currently reflects likelihood of not meeting 3% improvement.
2. Flu CQUIN - Target for frontline clinicians to be vaccinated by Q4 set nationally at 70% - DCHS unlikely to meet this target based on 2016-17 performance of 52.5%. New national requirement released in October 2017 which involves contacting all members of staff with communication about flu immunisation and capturing those staff who decline; this information is required to support payment for the CQUIN. Current performance stands at 60.5% (12/01/2018)
3. Proactive and Safe Discharge CQUIN - Risk highlighted regarding inability of DCHS to sign off Q2 milestones in relation to joint plans and trajectories to improve % of non-elective acute admissions discharged to usual place of residence within 7 days as not confirmed by the CCG.
4. Personalised Care and Support planning CQUIN- scale of patient contact required within limited resources to undertake patient activation survey presents increased risk for DCHS in terms of meeting Q4 milestones.
Based on non-achievement of CQUIN targets there would be a predicted financial risk equating to approximately £700k loss of baseline income. However for 2017/18 financial year this has been mitigated through an agreed settlement with Derbyshire Commissioners. The Trust however continues to focus on CQUIN targets and within-quarter milestones to support the delivery of high quality care. Work has commenced internally to review any risks to 2018/19 as all CQUINS are National and across 2 years.
All actions remain on-going throughout Q4, performance against the milestones is measured monthly and escalated appropriately.
1. Communications continued up until the end of the period of the survey which has now closed. The results of the National staff survey recently received but awaiting national benchmarks. Early comparison suggests DCHS will not meet the target but are awaiting formal publication of the data and will then review.
2. Previous discussions with commissioners regarding local agreement of target - not agreed therefore this remains a risk. Staff campaign is ongoing with a further focus as a result of local outbreaks and information received from Public Health England. Further communications including one recently from the Trust Medical Director have been disseminated and wards have all been restocked to encourage uptake. Awaiting final performance.
3. Formal request made to SDCCG Deputy Director of Quality to extend milestones to Q3 in recognition of delays outside of DCHS' control, correspondence has now being received to decline this request from NHSI. DCHS Continues to work very closely with identified acute providers in regard to achieving across community milestones to support patient flow and D2A workstreams. Data has recently been received from both CTHFT and CRHFT, which needs further analysis . Discussion in regard to this and trajectories for this CQUIN scheduled for January QAG with commissioners.
4. Work now complete to identify the required specialist services and the number of patients who are required to be contacted in Q4. This is approximately 1500 patients. Work has commenced contacting patients and will enable the resource required in order to achieve contacting all of the patients during Q4. Clarity is required in regard to exceptions for these patients if and when contact is unsuccessful or inappropriate
1-Summary of Issues:
2. Action Plan
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
Page 15 of 2618 Performance Report.pdfOverall Page 95 of 218

Measure Frequency2017/18
Full Year Target
YTD Target Q2 Oct-17 Nov-17 Dec-17 YTD
Avoidable Grade 2, 3 & 4 Pressure Ulcers developed or deteriorated in DCHS care (no.) Monthly 34 26 30 6 7 7 50
DCHS will see a reduction in avoidable pressure ulcers.
Exception Report Analysis
Pressure ulcer improvement groups meet monthly to review action plans and issues.Training in health coaching will continue through 2018/19 dependant on resources.
1-Summary of Issues:
2-Action Plan: (actions taken, including assignment of responsibility for this plan)
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
The Matron for Tissue Viability has been working on practice and caseload age profile data from incidents recorded on Datix and TPP as part of the work with Southern Derbyshire CCG to challenge equipment provision under the City ICES contract. Equitable provision of equipment continues to be a cause for concern in the Derby City area.Pressure Ulcer Improvements Groups (PUIGs)have been established in all localities and had all submitted their action plans by the extended deadline of the 12th December. The TV team is supporting Erewash to more effectively support this PUIG. Common themes within action plans relate to risk assessment, completion of SSKIN bundle and education of care home staff. Progress is monitored via the Chronic Wound Management Group monthly.Training in health coaching continues to be rolled out and is being evaluated very favourably with clinical teams and having a positive impact in case management.Chronic Wound Management: a ‘Deep Dive’ will be presented to QSC in February 2017 to bring the Committee up to speed with progress and future plans and to agree the chronic wound management strategy.
There continues to be occurrences of avoidable pressure ulcers within community settings most prevalent within Derby City and NE Derbyshire areas.
2
3
9
5
9
2
6
7 7
0
1
2
3
4
5
6
7
8
9
10
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
No
Month
Avoidable Grade 2, 3 & 4 Pressure Ulcers developed or deteriorated in DCHS care (no.) - December
Avoidable (2, 3, 4) PUs
Page 16 of 2618 Performance Report.pdfOverall Page 96 of 218

Measure Type Frequency 2017/18 Full Year Target
YTD Target Q2 Oct-17 Nov-17 Dec-17 YTD
Identification Of Carers On TPP (Big 9) - Carers Identified (no) External Monthly 2,890 2,000 1,040 1,194 1,329 1,420 1,420
Exception Report Analysis
January 2018 - March 2018.
Increased publicity may improve the year end forecast position.
1-Summary of Issues:
2-Action Plan: (actions taken, including assignment of responsibility for this plan)
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
We are currently behind schedule on the target for reporting carers on TPP and as it stands we are forecasting an end of year deficit of 1,197.
To help us address this deficit we have planned a targeted communications campaign starting on 10 January 2018 for three months. Our key messages will be to all DCHS team members regarding the importance of identifying and registering all patients who have caring responsibilities, offering signposting and support.
1. Key messages will be shared with teams in the weekly communication bulletin, leaders e-mail, poster, and across our social media platforms including following the Ask – Record – Engage procedure with every patient we come into contact with
• Ask – every patient, do you have caring responsibilities?• Record – every answer onto the correct area of the equalities template on sytsmOne or other system, we need to know when a patient has caring responsibilities so we can offer assistance and signposting• Engage – give out the wallet cards to signpost to local support
2. Targeted information and resources will be distributed to teams through senior managers, communication champions and the Quality Always champion platform
3. Educational Tutorial will be shared with DCHS teams and on MyDCHS showing where the information is recorded on the SytsmOne equality and diversity form
4. We will re-distribute the ‘caring for carers’ poster across sites through our communications champions to continue to re-affirm DCHS commitment to carers
5. We would like to ask all board members to take every opportunity to raise awareness across DCHS teams the importance to ask- record-engage all patients with caring responsibilities.
377 524
678 791 909 1,040
1,194 1,329 1,420
200 500
1,000
1,500
2,000
2,500
1,500 1,750
2,000 2,250
2,500
2,890
0
500
1,000
1,500
2,000
2,500
3,000
3,500
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
Activ
ity (
no)
Month
Activity Actual(no)
Activity Target(no)
Activity Forecast(no)
Big 9 - Identification of Carers on TPP - December
Page 17 of 2618 Performance Report.pdfOverall Page 97 of 218

Measure Type Frequency 2017/18 Full Year Target
YTD Target Q2 Oct-17 Nov-17 Dec-17 YTD
Insulin Safe Administration - Right Dose, Right Time - (Big 9) - Nurses Trained (no) External Monthly 715 546 286 379 422 433 433
Exception Report Analysis
It is anticipated that the plan will achieve the revised end of year target.
To continue with current plan of contacting each GM to ensure that remaining staff are informed that the elearning package requires to be completed. This is sent each month.
Continuation of the importance of completion is communicated at all levels.
1-Summary of Issues:
2-Action Plan: (actions taken, including assignment of responsibility for this plan)
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
There continues to be a steady increase of staff completing the eLearning package, however over the last month there have been great demands on clinical staff due to winter pressures to deliver services and this may have impacted on staffs availability to complete the elearning package. The completion data continues to be sent to each General Manager and informs which staff have not yet completed the elearning package with supporting documents on how to access the elearning package. There have been no further reports of any technical issues with the package. The Workforce Development Team who upload the completion of elearning package onto individuals learning records on OLM continue to do this as a priority. Recently there has been a validation of staff who require this skill and this has reduced the number of staff who are required to complete the programme, this number is 620, however, this may change monthly due to staff turnover of staff.
6 22 72 101 138
286
379 422 433
95 151
208 264
320 377
433 490
546 602
659 715
0
100
200
300
400
500
600
700
800
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
Activ
ity (
no)
Month
ActivityActual (no)
ActivityTarget (no)
ActivityForecast(no)
Big 9 - Insulin Safe Administration -December
Page 18 of 2618 Performance Report.pdfOverall Page 98 of 218

Measure2017/18 Full Year Target
YTD Target Oct-17 Nov-17 Dec-17 YTD
Essential Learning completed (% compliance) 96% 96% 87.97% 86.60% 89.74% 89.74%
Exception Report Analysis
Compliance has improved by 3% this month. There have been 10 DNA's on Essential on the face to face course offered this month along with 22 withdrawals which have had a impact on compliance. Although ESR (e-learning) was unavailable due to a system upgrade over the holiday period this does not seem to have impacted training compliance.
It is anticipated that the above outlined action plan will ensure the year end target is achieved.
The action plan commenced January 18 and will continue to year end.
It is anticipated that the following actions will ensure a steady increase in compliance rates thereby meeting the 96% target by the end of March 2018: 1. The Workforce Planning and Development Team (WPD) will work with service managers by attending ops meetings to report on and monitor compliance on a monthly basis. 2. WPD and QBS will undertake a deep dive exercise to review service areas compliance and devise an appropriate supportive plan to increase compliance as required. 3. Staff whom do not attend essential training will continue to be sent DNA's emails which will also be sent to their managers, staff are advised to rebook onto the next available session and the reason for non- attendance is recorded and monitored and discussed with service mangers. 4. WP&D will continue to attend the HR Fix IT sessions across DCHS sites to promote e-learning and support staff to complete training via this method. 5. WPD provides support for staff via telephone, face to face and user guides on how to complete e- learning. 6. Fire officers are now returning registers within 24 hours to ensure timely and accurate compliance data. 7. WPDT have developed a task and finish group so as to collate e- learning issues/ staff difficulties so as increase E- learning use which will in-turn improve compliance rates. 8. All new starters completing essential learning on day 3 of induction will now entered onto the system within first week of employment, this prevents delays in updating learner records and enhances data accuracy. 9. WPD has reviewed available training spaces to ensure supply meets demand with an additional option to complete via e-learning.
1-Summary of Issues:
2. Action Plan
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
87% 88% 89% 89%
88%
86%
88% 87%
90% 92%
94%
96%
80%
82%
84%
86%
88%
90%
92%
94%
96%
98%
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
%ag
e Co
mpl
ianc
e
Month
Essential LearningCompleted (%)
Forecast (%)
Target Profile (%)
Essential Learning (% Compliance) - December
Page 19 of 2618 Performance Report.pdfOverall Page 99 of 218

Measure2017/18 Full Year Target
YTD Target Oct-17 Nov-17 Dec-17 YTD
Staff with Appraisals Completed (% compliance) 96% 96% 90.9% 88.0% 90.3% 90.3%
It is expected that the action plan outlined above will enable the year end target to be achieved.
Exception Report Analysis
There has been a 2% increase in the completion and recording of ESR this month which during the pressures of winter is an achievement.
The supportive plan will commence during January 2018 and continue until year end.
It is anticipated that the following actions will ensure a steady increase in compliance rates thereby meeting the 96% target by the end of March 2018: 1. The Workforce Planning and Development Team (WPD) will work with service managers by attending ops meetings to report on and monitor compliance on a monthly basis. 2. WPD and QBS will undertake a deep dive exercise to review service areas compliance and devise an appropriate supportive plan to increase compliance as required. 3. WPD and QBS will facilitate drop in sessions for staff so as to gain support for accessing/ recording of ESR data such as appraisals. 4. WPD will continue to offer one-one support for staff so as to assist staff in uploading appraisal data as required via a telephone, face to face and user guides.
1-Summary of Issues:
2. Action Plan
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
93% 93% 92% 93%
91% 90%
91%
88%
90% 92%
94%
96%
82%
84%
86%
88%
90%
92%
94%
96%
98%
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
%ag
e Co
mpl
ianc
e
Month
Appraisals (%)
Forecast (%)
Target Profile(%)
Staff With Appraisals Completed (% Compliance) - December
Page 20 of 2618 Performance Report.pdfOverall Page 100 of 218

Measure Type Frequency 2017/18 Full Year Target
YTD Target Q2 Oct-17 Nov-17 Dec-17 YTD
Training Children L2 (%) External Monthly 96% 96% 89.9% 88.8% 87.7% 89.7% 89.7%
Training Children L3 (%) External Monthly 96% 96% 61.4% 64.3% 72.5% 75.3% 75.3%
Training Adults L2 (%) External Monthly 96% 96% 90.5% 89.8% 90.0% 90.8% 90.8%
Prevent (%) External Monthly 85% 59% 42.5% 73.1% 66.7% 66.7%
WRAP (%) External Monthly 85% 82% 76.9% 76.9% 88.9% 88.9%
Exception Report Analysis
The compliance rate for Adult and children safeguarding level 2 has remained consistent and has slightly increased. Both the full day think family and the half day updates that have been planned have been well attended. An extra update session was also provided on the 18.12.17, the room capacity was 20 and 13 attended. A further 21 update Think family sessions are planned for the remainder of this financial year and 7 of these still have places available for staff to book. Wrap has shown a significant compliance improvement and is currently above the 85% that the home office and NHS England have requested. It is however imperative that this continues to increase or is maintained. Staff requiring Basic Prevent Awareness Training (PREVENT) compliance however decreased, this may be related to ESR being unavailable for a short period in December however again 85% compliance is required and must be achieved. On ESR staff have been be recorded as either requiring WRAP or BPAT depending on their role. A level 2 full day training session was cancelled in December due to the trainer getting stuck on route due to the inclement weather. Level 3 safeguarding children training compliance has increased by 9% in December; this update is an annual requirement. The Safeguarding Service has trained 184 of the 265 staff that require level 3a training and 109 are booked onto the remaining sessions which will make a total of 293 staff trained by the end of the financial year and staff that require level 3 training; 353 of the 413 identified staff have already been trained and 80 are booked onto the remaining sessions which will make a total of 433 by the end of the financial year. For DCHS this reflects that the staff that require level 3 (and 3a) are attending their training and by the end of the financial year, except for those on maternity leave or long term sickness the Safeguarding Service is confident that level 3 staff are compliant, although it is not clear why compliance is below 80% when the number of staff trained is on target for the financial year.
The Safeguarding Service continues to work with Workforce Development and QBS to support staff in attending the correct level of safeguarding training to meet their safeguarding adult . Failure to meet the target by year end will impact on our ability to provide assurance on staffs competence regarding safeguarding and prevent/WRAP competencies. It is anticipated that the actions described will support improved performance.
DCHS has until 31.3.18 to ensure that staff are WRAP and BPAT compliant and to reach the targets of 85%.
Managers must continue to ensure that staff complete the 2 ESR PREVENT E-Learning packages to ensure that their team members remain compliant for either WRAP and BPAT. We would request the support of the board to encourage this approach and stress the importance of training completion as per the Home Office and NHS England request. Some professionals have raised that despite attending induction where WRAP is included they are still showing red on ESR for the 2 E learning packages the safeguarding team have requested that workforce planning look into this and make the necessary changes on ESR to ensure that records for staff are update to date. To prevent cancellation due to inclement weather we have developed a buddy system, especially for the full days training, taking into account where the trainer lives and where the session is being held. In order to gain a better understanding of the training compliance figures and to also ascertain that staff are receiving the correct level of training the Safeguarding Service will continue to work with Workforce Development and QBS.
1-Summary of Issues:
2. Action Plan
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
91.0
%
91.4
%
91.0
%
88.5
%
89.9
%
89.9
%
88.9
%
87.7
%
89.7
%
80.5
%
79.9
%
78.1
%
82.2
%
83.1
%
61.4
%
64.3
%
72.5
%
75.3
%
92.7
%
90.9
%
90.5
%
88.7
%
90.6
%
90.5
%
89.8
%
90.0
%
90.8
%
42.5
% 73
.1%
66.7
%
76.9
%
76.9
%
88.9
%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
%ag
e Co
mpl
ianc
e
Month
Training Children L2 (%)
Training Children L3 (%)
Training Adults L2 (%)
Prevent (%)
WRAP (%)
Target Profile (%)
Prevent Target%
WRAP Target%
Safeguarding (% Compliance) - December
Page 21 of 2618 Performance Report.pdfOverall Page 101 of 218

Measure2017/18
Full Year Target
YTD Target Q2 Oct-17 Nov-17 Dec-17 YTD
Delayed Transfer of Care (%) - Inpatients & OPMH 3.5% 3.5% 4.8% 4.9% 3.8% 5.6% 7.8%
In line with the improvements noted up until November it is likely that the overall DTOC figure will improve during January. Some of the delays experienced during December can be linked to the holiday period, particularly where new care packages were slightly limited in availability.
Exception Report Analysis
1. Weekly DTOC calls continue between health and social care to resolve ongoing issues with discharge2. Meeting between Stepping Hill and DCHS to improve transfers of care into DCHS, particularly to community hospital beds. Follow up meeting planned for January. Increased presence of DCHS clinical navigators at Stepping Hill.3. Monthly DTOC meetings of Health and Social Care managers to address delays and identify solutions to specific issues. 4. Plans for workshops with care home managers to initiate Trusted Assessor model.
1-Summary of Issues:
2-Action Plan: (actions taken, including assignment of responsibility for this plan)
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
1. Weekly2. 18th January 20183. Monthly4. 11th January
The Delayed Transfers of Care (DTOC) rate for DCHS in December 2017 was 5.6% which is an increase of 1.8% on November 2017. This was split between OPMH at 4.1% and Rehab and Urgent Care (RUC) at 5.9% and totalled 289 days in delay. The year to date is now 7.8%.The delays were divided between NHS and Social Care as follows;194 days attributable to NHS• 125 days waiting for Nursing home placement• 56 days related to patient and/or family choice• 7 days waiting foe care package• 6 days waiting for residential care placement81 days were attributable to Social Care• 77 days waiting for care packages• 4 days waiting for assessment14 were attributable to both NHS and Social Care• 8 days waiting for care package• 6 days waiting for Nursing Home placementIn terms of costRehab & Urgent Care = £123KOPMH = £21KThe figures for the wards are below (Linacre and Hopewell had no DTOC during December)Okeover – 34; Fenton – 15; Alton – 34; Rowsley – 49; Butterley – 13; Baron – 41; Heanor- 4; Oker – 28; Melbourne – 26; Spencer – 12
Many of the delays recorded as patient/family choice relate to relatives finding appropriate care homes, difficult social circumstances or engagement of relatives in supporting discharge. Wherever patients were delayed waiting for care packages at home every effort was made in conjunction with social care to locate interim care beds rather than wait in hospital. It has been identified that some of the delays are due to wards waiting for care homes to visit the ward to assess patients before accepting them. Work is underway to establish a Trusted Assessor model between DCSH, Adult Care and care providers.
7.6%
12.4%
10.1% 11.3%
8.8%
4.8% 4.9% 3.8%
5.6%
0%
2%
4%
6%
8%
10%
12%
14%
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
% o
f D
elay
s
Month
Delayed Transfer of Care (% ) - December
Actual %
Forecast %
NHSI Target %
Page 22 of 2618 Performance Report.pdfOverall Page 102 of 218

Measure Type Frequency 2017/18 Full Year Target
YTD Target Q2 Oct-17 Nov-17 Dec-17 YTD
Community Podiatry Non AQP Activity (no) External Monthly 148,415 110,933 65,217 76,249 88,551 97,102 97,102
Exception Report Analysis
It is anticipated that new staffing will be in place by the end of February / March 2018. However, the current recruitment process may in turn, lead to further vacancies as a result of internal candidates becoming successful in their application
Recruitment process has started in January 2018 to appoint to all vacancies
The community podiatry service had experienced a significant number of vacancies as a result of staff leaving the organisation, staff retirement and reduction of staff hours going into new financial year. Following a previous recruitment process, there has been a retraction of 1 wte posts offered and one staff member has recently gave notice of employment with the Trust. There has also been a delay in the recruitment process following on-going discussions with commissioners around waiting times for non urgent referrals. The service has been unable to recruit to the full amount of vacancies in November 2017. Recruitment is underway in January 2018.
The forecast has been amended to reflect the current vacancies
1-Summary of Issues:
2-Action Plan: (actions taken, including assignment of responsibility for this plan)
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
9,020 20,848 32,711 43,438 54,498 65,217 76,249 88,551 97,102
12,488 24,689
37,890 50,305
61,889 73,882
86,245 100,350
110,933 123,358
135,524 148,415
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
Activ
ity (
no)
Month
ActivityActual (no)
ActivityTarget (no)
ActivityForecast(no)
Community Podiatry Activity Non AQP (no) Cumulative -December
Page 23 of 2618 Performance Report.pdfOverall Page 103 of 218

Measure Type Frequency 2017/18 Full Year Target
YTD Target Q2 Oct-17 Nov-17 Dec-17 YTD
Physiotherapy Activity (no.) External Monthly 126,000 93,766 57,509 67,490 78,943 87,416 87,416
Exception Report Analysis
The service will not reach the activity target for this financial year (120,693), this is partly due to a focus on 2018/19 and development work with commissioners which should result in increased activity and income for DCHS.
Job planning approach ongoing in service to maximise productivity . The service have also completed detailed demand and capacity work to support the absorption of extra work into the DCHS MSK service as requested by Commissioners. Although extra staff have been recruited there will still be a shortfall in terms of meeting the current and new demand for services. There is still ongoing discussion with commissioners around funding of the extra staff, which is showing as an overspend. A paper has been presented to the Executive Committee detailing the issues related to the MSK pathway work which is impacting on activity and expenditure in this financial year. As a result of this there will be an Executive to Executive meeting to discuss the opportunities and risks involved in progressing with this project during the latter part of this financial year and into next year.
The baseline for Physiotherapy activity for 2017/18 was set at a level of 5,427 contacts higher than the baseline in 2016/17. This was partially due to the fact that the baseline was set using data from month 6 forecasts which were not realised due to staffing issues at the latter end of 16/17. There was also some over establishment built into the baseline setting which was then not funded into the service budget. Due to the work on MSK pathways there has been some recruitment into Advanced Clinical Practitioner posts both internally and externally which has impacted on the ability of the service to balance the position in terms of expenditure. There has also been some need to invest in training for internal staff linked to increasing the capacity for Advanced Clinical Practice which has meant lost activity this year but which will put DCHS in a position to play a significant role in the MSK work and potentially increase income in the next financial year.
The target for 2016/17 will not be achieved , however active discussions are taking place with commissioners on potential extra funding to support increased activity levels in 2018/19.
1-Summary of Issues:
2-Action Plan: (actions taken, including assignment of responsibility for this plan)
3-Timescales
4-Effect of this Exception on the Forecast Plan (how we get to our final forecast position from here)
8,041 18,282 28,399 38,169 48,202 57,509 76,490 78,943 87,416
10,253 19,834
30,438 40,670
51,253 61,816
72,452 83,323
93,766 104,736
114,971 126,000
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
Activ
ity (
no)
Month
ActivityActual (no)
ActivityTarget (no)
ActivityForecast(no)
Physiotherapy Activity (no) Cumulative - December
Page 24 of 2618 Performance Report.pdfOverall Page 104 of 218

MeasureFrequency of
Reporting2016/17 Full Year Target Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Narrative
Health and Wellbeing - Staff
survey improvementAnnual
5% point improvement over two years in two annual staff survey questions on health and wellbeing, MSK and stress
Improvement of 5% points required on staff survey questions related to reduction in work related stress and Trust taking
positive action on health and wellbeing. Weighted payment, 50% if 3% improvement achieved. BCCTH expected to affect
this and risk reflects likelihood of not meeting 3% improvement.
Health and Wellbeing - Healthy
food and drink
AnnualEnd of Q4
70% of drink lines stocked must be sugar free
60% of confectionary and sweets do not exceed 250kcal
60% of pre-packed sandwiches contain 400kcal or less and do not exceed 5g
sat fat
Vending machine options now available at most sites and plans made for Ripley to receive decommissioned one from Ilkeston. Discussions with external supplier to ensure pre-
packed sandwiches are CQUIN compliant by end of Quarter 4.
Health and Wellbeing - Flu
vaccination
Monthly from start of flu campaign
70% uptake of flu vaccination by frontline clinical staff by 28th February
2018
Risk highlighted in meeting 70% target based on 2016-17 performance of 52.5%. Predicted achievement of 50%
payment based on performance in 2017-18 being equal or better to that of 2016-17. New national requirement released
in October 2017 which involves contacting all members of staff with communication about flu jab and capturing staff
who decline; this information is required to support payment for the CQUIN. To be discussed during January QAG.
Q2
Map and streamline existing discharge pathways
Roll out protocols in partnership with local whole system
Q42.5% improvement in non-elective
acute admissions discharged to usual place of residence within 7 days
Risk highlighted as data associated with targets is acute-held and achievement of target is influenced by acute and social
care. Target associated with discharge to 'usual place of residence' within 7 days of admission. CCG have now agreed to review data sets if target is missed to determine impact of other community providers. Data received from DTHFT and
awaiting most recent data including Dec 17 from CRHFT
Q1Training of inpatient ANP staff in
alcohol and tobacco brief intervention
Training in smoking and alcohol brief advice and intervention completed by inpatient ANPs, including self-assessment.
Payment for Q1 achieved.
QuarterlyAudit of tobacco and alcohol screening, brief intervention and onward referral
for inpatient services
Q3 data being compiled re. smoking and alcohol use, brief advice and intervention and onward referral to treatment
services. Further clarification required from commissioners regarding quarterly targets as DCHS exceeding Q4 targets for
some elements.
Improving the assessment of
woundsQuarterly
Audit and improvement of the completion of full wound assessments
for chronic wounds
Audit undertaken in September 2017 - baseline position confirmed and action plan developed which has been being implemented during Q3. Improvement target of 15% agreed
with commissioners during Q2.
End of Q3Identification of patient cohort with
multiple long term conditions with low activation levels
Scale of patient contact required to establish patient activation level represents a significant challenge for DCHS
(~2000). Long term Condition services now identified across the county and planning commenced to establish scope of patient survey. The resource needed to deliver the patient
contact exercise is being assessed.
End of Q4 Training of identified staff cohort in personalised care and support planning
Pending confirmation of number of staff required to undertake training. E-learning training package identified on
ESR which will minimise impact on staff.
NHS DERBYSHIRE COUNTY CCGs AND ASSOCIATES CONTRACT
Focus Area
CQUIN INDICATORS 2017-18
Supporting Proactive and Safe Discharge
Preventing Ill Health - alcohol and tobacco
Personalised Care and Support
Planning
QU
ALIT
Y SE
RVIC
E
PATI
ENT
EXPE
RIEN
CE, S
AFET
Y IN
OVA
TIO
N &
CLI
NIC
AL E
FFEC
TIVE
NES
S
Page 25 of 2618 Performance Report.pdfOverall Page 105 of 218

Trust DERBYSHIRE COMMUNITY HEALTH SERVICES NHS TRUSTPeer Group Community
Focus Area
Domain Indicator RelevanceNHSI Reported
PeriodValue
Peer Group
AverageNHSI Rank Apr-17 May-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 -
Referral To Treatment (RTT) waiting time compliance (%):
Incomplete Trust Level June 2017 96.7 96.7 96.9% 97.0% 95.8% 93.9% 95.3% 94.7% 93.2% 95.0%
Accident and Emergency (% discharged, admitted or transferred within 2 hours of arrival at MIU/walk-in centre) (%)
A&E Depts March 2017 88.7 76.9 84.5% 87.8% 85.7% 90.2% 89.8% 91.0% 91.5% 91.5%
Outpatients (% DNA):
Adults (%) Clinics in community March 2017 5.2 9.0 5.4% 6.3% 5.5% 5.6% 5.8% 5.6% 5.3% 6.0%
Community Children and Young persons contacts (%DNA) Trust Level April 2017 14.4 11.6 8.3% 11.6% 9.8% 9.2% 9.7% 8.7% 9.6% 10.4%
Average Length of Stay (days):
Emergency (Urgent Care) Community beds March 2017 13.7 9.5 17.2 21.9 12.0 11.7 14.7 18.8 17.2 15.9
Other (Rehabilitation) Community beds March 2017 21.4 24.5 19.8 21.3 20.7 18.7 19.1 19.3 18.2 17.5
Return to usual place of residence after discharge (%) Community beds March 2017 64.1 67.8 69.2% 68.6% 65.5% 65.8% 66.7% 66.0% 63.8% 63.2%
Harm free care for patients surveyed for new pressure ulcers:
Community (%) Community services June 2017 99.0 98.7 98.9% 99.4% 98.9% 99.3% 98.9% 99.3% 99.3% 98.9%
Community Hospital Ward (%) Community wards June 2017 100.0 99.5 99.5% 100.0% 99.3% 100.0% 93.8% 100.0% 100.0% 99.4%
Other Safety Measures
The rate of reported Serious Incidents Requiring Investigation (SIRIs) Trust Level October 2016 1.9 6.8 2.4 3.1 3.6 6.6 0.0 3.9 2.7 1.0
Total number of reported falls per 1,000 occupied bed days (OBDs) Trust Level September 2016 10.8 9.4 7.5 9.3 14.6 11.8 11.6 11.8 4.8 8.6Total number of reported falls resulting in injury per 1,000 occupied bed days
(OBDs)Trust Level September 2016 4.3 2.8 1.92 4.57 5.74 5.33 5.58 4.56 1.66 3.84
Community Friends and Family (from Jan 2015)
Response Rate (%) Community services June 2017 4.5 4.1 4.7% 5.0% 5.0% 5.2% 4.6% 4.8% 3.6% 3.4%
Recommended (%) Community services June 2017 97.6 95.8 98.0% 98.0% 97.3% 97.9% 97.9% 98.2% 97.0% 98.1%
Staff Friends and Family:
Response Rate (%) Trust Level Q4 2016/17 36.8 20.4 39% 39% 37% 37% 37% 37% 37% 37%
Recommend as Place to Work (%) Trust Level Q4 2016/17 72.4 58.1 72% 72% 73% 73% 73% 73% 73% 73%
Recommend as Caring Place (%) Trust Level Q4 2016/17 91.1 81.6 91% 91% 92% 92% 92% 92% 92% 92%
Not Recommend as Place to Work (%) Trust Level Q4 2016/17 10.7 22.0 12.2% 12.2% 12.2% 12.2% 12.2% 12.2% 12.2% 12.2%
Not Recommend as Caring Place (%) Trust Level Q4 2016/17 1.7 5.2 1.7% 1.7% 1.7% 1.7% 1.7% 1.7% 1.7% 1.7%
Safe Staffing
Percentage of staff turnover (Monthly) Trust Level June 2017 0.7 1.2 0.8% 0.8% 0.7% 0.7% 0.7% 0.8% 0.7% 0.8%
Percentage of staff turnover (Rolling 12 Months) Trust Level June 2017 10.7 19.5 9.0% 9.1% 8.3% 8.3% 8.2% 9.2% 8.0% 9.6%
Percentage of unplanned sickness absence (%) Trust Level April 2017 4.1 4.3 4.42% 4.52% 4.95% 4.94% 4.76% 5.25% 5.50% 5.42%
Qua
klity
Ser
vice
Qua
lity
Peop
le
Measures as at August 2017
NHS Improvement Community Indicators Scorecard 2017-18
Safe
Caring
Well Led
Responsive
Effective
Page 26 of 2618 Performance Report.pdfOverall Page 106 of 218

TRUST BOARD Document Title: Financial Performance Report
Presenter/Title: Chris Sands, Director of Finance, Information and Strategy Contents of Paper were previously discussed by: QBC held on Wednesday 17 January 2018
Author/Title: David Gray, Head of Financial Management Contact Email and Telephone Number: [email protected] 01246 253046
Date of Meeting: 25 January 2018 Agenda Item No: 19/18
No of pages inc. this one: 12
Has an Equality Impact Assessment been undertaken Yes No x
Document is for: (more than one box can be ticked) Information Decision Assurance x
Purpose of Paper
The paper sets out the financial performance of the Trust as at 31st December 2017. The report details performance against statutory and internal targets. The Trust is reporting a surplus position of £5.96m at month 9, which represents a surplus variance of £0.13m against the planned surplus of £5.83m. The cash position is £2.65 m ahead of plan. A year end surplus of £4.92m is forecast. The cash position is forecast to be £23.5 million at the end of March 2018. The Trust is forecasting that it will meet all its statutory financial duties for the year.
Recommendations
Board Members are asked to discuss the report and note the actions being taken.
Board Assurance Framework Risk Reference
3.7 There is a risk to the financial stability of the organisation of not meeting future Sustainable Quality Improvement Programme over the next two years. 3.8 There is a risk to the organisation due to the inability to meet contractual activity targets, resulting in financial risk.
Financial Impact
The report contains a number of issues and risks that have a financial impact on the organisation.
Page 1 of 1219 Financial Performance Report.pdfOverall Page 107 of 218

Further Information and Appendices
Report attached
Monitoring Information Brief Summary
What are the Governor Involvement implications?
Governors will hold the Board to account around its financial position
What are the Equality, Diversity and Inclusion implications? None
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
None
Risk Register
Is the issue on the current Risk Register? No If yes, what is the Risk Number?
Does this update recommend a change in the current risk score? (If so, please provide your rationale below) No
Page 2 of 1219 Financial Performance Report.pdfOverall Page 108 of 218

WORKING CAPITAL23.56 G 23.53 G4.46 G 1.67 G
£m % £m % % £m % £m % £m % (5.55) G (1.13) GEBITDA (10.51) (7.14) (10.88) (7.35) 3.52 (11.15) (5.75) (11.50) (5.89) (0.34) 3.08
Net (surplus)/deficit (5.83) (3.96) (5.96) (4.03) 2.18 (4.92) (2.54) (4.91) (2.52) 0.01 (0.20) SINGLE OVERSIGHT FRAMEWORKSingle oversight framework capital service capacity (x) 5.94 G 4.71 G
I&E SURPLUS (excl. IMPAIRMENT) I&E SUMMARY AS AT 31 DECEMBER 2017 Single oversight framework capital service capacity 1 G 1 GSingle oversight framework liquidity (days) 29.76 G 34.39 GSingle oversight framework liquidity 1 G 1 GSingle oversight framework I&E margin (%) 4.03 G 2.52 GSingle oversight framework I&E margin 1 G 1 G
£m £m £m £m £m £m Single oversight framework distance from plan (%) 0.06 G 0.00 G(147.16) (148.01) (0.85) (194.12) (195.19) (1.08) Single oversight framework distance from plan 1 G 1 G
PAY 98.61 98.22 (0.39) 131.02 130.73 (0.29) Single oversight framework agency spend - Dist. from Cap (%) -43.4 G -43.4 GNON-PAY 38.04 38.91 0.86 51.94 52.97 1.03 Single oversight framework agency spend - Dist. from Cap 1 G 1 GOTHER 4.68 4.92 0.24 6.23 6.58 0.34 Overall rating 1 G 1 G
(5.83) (5.96) (0.13) (4.92) (4.92) (0.00)
PERFORMANCE AND SQIP YTD FOTCAPITAL PROGRAMME MONTH END CASH BALANCE Contract over/(under) performance (£m) 0.77 G 1.00 G
Over/(under)achievement of SQIP target (£m) 0.00 G 0.06 G(Over)/underspend against investments (£m) 0.00 G 0.00 GNet impact Performance and SQIP (£m) 0.77 G 1.06 G
ADDITIONAL TRIGGERS YTD FOTReceivables aged over 90 days (%) 5.0 17.3 R 5.0 GPayables aged over 90 days (%) 5.0 31.8 R 5.0 GChange in Finance Director in last year 2 0 G 0 GInterim Finance Director in place over QE 2 0 G 0 GDays expenditure covered by QE cash 10 47.0 G 46.7 GCapital Expenditure % of plan (%) 85.0 107.2 R 100.0 G
DERBYSHIRE COMMUNITY HEALTH SERVICES NHS FOUNDATION TRUST FINANCIAL PERFORMANCE REPORT
PLAN ACTUAL VARIANCE PLAN FOT VARIANCE
DECEMBER 2017 KEY FINANCIAL INDICATORS
EBITDA AND SURPLUS AS AT 31 DECEMBER 2017YTD 2017/18 FULL YEAR
DECEMBER 2017
FOTYTD
Current Assets Variance (£m)Cash at bank as per the ledger (£m)
Current Liabilities Variance (£m)£m
VAR
FOT
PLAN
FULL YEAR
(0.13)
(0.37)
INCOME
TOTAL
DEC 2017
YTD
FOTYTD
VAR
ACTU
AL
PLAN
0.01.02.03.04.05.06.07.0
Cum
ulat
ive
surp
lus
(£m
)
Plan Actual Forecast
0.0
5.0
10.0
15.0
20.0
25.0
30.0
Cas
h at
mon
th e
nd (£
m)
Plan Actual Forecast
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
Cum
ulat
ive
capi
tal s
pend
(£m
)
Plan Actual Forecast
Page 3 of 1219 Financial Performance Report.pdfOverall Page 109 of 218

DERBYSHIRE COMMUNITY HEALTH SERVICES NHS FOUNDATION TRUST
MONTHLY FINANCIAL PERFORMANCE REPORT FOR TRUST BOARD AS AT 31ST DECEMBER 2017
1. Introduction The purpose of this report is to update and inform the Committee on performance against key financial criteria for month 9 of the current financial year, 2017/18. The Trust is reporting a surplus position of £5.96m at month 9, which represents a surplus variance of £0.13m against the planned surplus of £5.83m. The cash position is £2.65m ahead of plan. We are forecasting a year end surplus of £4.92m, which is consistent with our control total set by NHS Improvement. 2. Summary Financial Position NHS Improvement has changed the way that they assess the financial sustainability of all providers. The Single Oversight Framework became effective from 1st October 2016 and replaced the previous Risk Assessment Framework. The new framework uses five metrics, each with an equal weighting to derive an overall rating score for the organisation. A rating of a 1 represents the lowest financial risk, with a score of a 4 being the highest risk. The Trust is forecasting a surplus of £4.92m. Table One – Finance Metrics The Trust’s Performance against the new Finance Metrics ratings is detailed in the table below. The Trust achieved a rating of 1 at year-end. This reflects the strong balance sheet of the Trust.
Area Metric Weight Year to Date Year End Outturn
Value Score Wtd Score
Value Score Wtd Score
Financial Sustainability
Capital Service Capacity
20% 5.94 1 0.2 4.71
1 0.2
Financial Sustainability
Liquidity (Days)
20% 29.76
1 0.2 34.39 1 0.2
Financial Efficiency
I&E Margin 20% 4.03% 1 0.2 2.52% 1 0.2
Page 4 of 1219 Financial Performance Report.pdfOverall Page 110 of 218

Financial Controls
Distance from Control Total
20% 0.06% 1 0.2 0.00 1 0.2
Financial Controls
Agency Spend 20% -43.4% 1 0.2 -43.4% 1 0.2
Overall Rating 1 1
To move to a forecast outturn rating of 2, there would need to be deterioration in the income and expenditure position of £3.0m. A further reduction to the position of £1.2m or a total of £4.2m would move the overall rating to a 3. The Trust’s performance against the Agency Spend metric continues to show our spend is still significantly below the submitted planned run rate due to a combination of the work that went in since the metric was introduced and improved rostering across services. 3. Income & Expenditure Appendix 1 details the Income and Expenditure Statement as at Month 9. More detail on the income and expenditure position is provided below.
3.1 Clinical Income At month 9 the clinical income position is showing an over performance of £759k, against plan with a year end forecast over performance of £994k. This financial position reflects a fixed year end contract settlement figure which has now been agreed with Derbyshire CCG’s which removes a lot of the risk associated with clinical income for 2017/18. The reflection of this contract settlement in the month 9 positon is the main driver for the changes to the year to date and forecast outturn position reported in previous months. The contracting team continue to work with services to closely monitor contract activity against plans to help inform 2018/19 planning and any associated financial risk for next financial year.
3.2 Non-Clinical and Other Income
Across the majority of Services Non-Clinical Other Income is ahead of plan resulting in an overall recovery against plan of £0.08m, however there are a couple of areas where due to loss of rental income through various organisations leaving DCHS premises (£0.08m), reductions in Catering Income (£0.05m) reduction in external maintenance rechargeable work (£0.01m) and Training Income (£0.03m) are under achieving.
3.3 Expenditure Overall, the Trust is reporting an overspend position against the expenditure plan at month 9 of £0.48m. Pay costs are underspent compared to plan by £0.39m. The main contributors to the under-spend are Health and Wellbeing, Integrated Care Services and Planned Care.
Page 5 of 1219 Financial Performance Report.pdfOverall Page 111 of 218

Agency Spend continues to be significantly lower than plan at the end of December (£0.45m) with actual spend for the month of £0.05m. The measures introduced to address agency spend are having a positive impact on the pay position, due to Winter Pressures and shortages in Substantive Staff Agency Spend is expected to rise over the next quarter. Agency and Flexible Workforce continue to remain at 2.6% of the Total Pay Spend to date. Detailed analysis of Workforce Spend by Staff Category can be found in Appendix 6. Non-pay Costs are over-spent against plan (£0.86m), due mostly to the under achievement in planned SQIP Schemes (£0.45m), provision for some property related expenses and increased activity performance within Planned Care and Outpatient services (£0.26m). Travel Costs across Integrated Community Services, Health and Wellbeing and Corporate Divisions remains a cost pressure with a year to date overspend of £0.14m. Health and Wellbeing Division continues to underspend (£0.37m) due to activity related payments to accredited providers being much lower than plan based on the activity under-performance within Integrated Sexual Health and Wellbeing Services. Depreciation charges and Cost of Capital are over-spent due to slippage against the planned SQIP target. 3.4 Sustainable Quality Improvement Plan The Trust has a SQIP target of £7.2m for 2017/18. As at month 9 there is a slight over achievement against the planned schemes of £0.002m. There has been slippage against the Seasonal Bed Flexing, Capital and Apprenticeship Levy Schemes. This slippage is being offset by Non recurrent schemes over achieving their year to date target. The Trust is forecasting an over achievement of £0.06m against the SQIP target by year end.. Further detail of the SQIP position can be found in Appendix 2. 4. Statement of Financial Position Appendix 3 sets out the Statement of Financial Position. 4.1 Cash At the end of December the cash balance was £2.65m ahead of plan (actual £23.56m against a plan of £20.91m). The capital programme has caught up to plan so this variance is caused by significant positive working capital variations, principally in payables. The Trust continues to actively manage working capital in line with the Working Capital Framework. In particular, the Treasury team continues to chase outstanding debt and promote prompt invoicing of income. A detailed Treasury Management Report was discussed at the January Quality Business Committee Further detail can be found in Appendix 4 attached.
Page 6 of 1219 Financial Performance Report.pdfOverall Page 112 of 218

5. Capital Plans and Expenditure
The Trust’s capital plan for 2017-18 totals £6,400k. Year-to-date spend is £5,870.2k against a plan of £5,477.2k, an overspend of £393.0k. The principle variance is the land at Buxton, which we have now purchased. Underspend against other schemes mean the forecast outturn remains at £6,400k. The Walton land sale is progressing, and solicitors are engaged in finalising the transaction. We expect the sale to be completed in late January / early February 2018. Further detail can be found in Appendix 5 attached. 6. Risks The Trust has reviewed its reporting of financial risk. A detailed table was reported through Quality Business Committee which set out the key financial risks, their estimated value, and the mitigations being put in place. The key risks are:
• Restructure costs associated with commissioner decommissioning and the implications of the Better Care Closer to Home transformation programme
• Restructure costs associated with changes to support the SQIP plan • Charging arrangements for Derbyshire LIFT and NHSPS properties. • Winter pressures
The estimated financial implications of these risks are included in our forecast outturn position. Progress in addressing these risks will be reported through QBC. Under planning guidance, the Trust is holding a 0.5% risk reserve for CQUIN. We are in discussions with NHS Improvement as to how this reserve will be allocated in 2017/18.
7. Summary
Board Members are asked to note the month 9 position against the financial targets. Chris Sands Director of Finance, Information and Strategy
Page 7 of 1219 Financial Performance Report.pdfOverall Page 113 of 218

1 2 3 4 5 6 7 8 9 10 11 12
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Annual Annual
Actual Plan Variance Actual Actual Actual Actual Actual Actual Actual Actual Actual Forecast Forecast Forecast Outturn Plan
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
OPERATINGIncome
Clinical Income -137,992 -137,225 -767 -14,963 -15,048 -15,755 -15,496 -14,820 -15,329 -15,259 -16,603 -14,719 -14,689 -14,659 -14,791 -182,131 -181,130
Other NHS Income -7,074 -6,997 -77 -740 -745 -803 -710 -759 -828 -810 -830 -849 -736 -728 -728 -9,266 -9,201
Education and Training -582 -642 60 -58 -63 -72 -67 -68 -65 -71 -61 -57 -80 -68 -68 -798 -854
Other Income -2,357 -2,294 -63 -212 -469 -223 -223 -244 -267 -276 -235 -208 -212 -204 -225 -2,998 -2,932
INCOME TOTAL -148,005 -147,158 -847 -15,973 -16,325 -16,853 -16,496 -15,891 -16,489 -16,416 -17,729 -15,833 -15,717 -15,659 -15,812 -195,193 -194,117
Operating ExpensesEmployee Benefit Expenses 98,219 98,605 -386 10,745 11,156 10,867 10,987 10,847 10,833 11,131 10,946 10,707 10,764 10,861 10,883 130,727 131,021
Drugs 1,410 1,377 33 181 111 157 169 156 135 163 173 165 153 153 153 1,869 1,814
Clinical Supplies and Services 8,772 8,686 86 921 916 1,035 880 936 898 1,051 1,011 1,124 945 943 947 11,607 11,515
Other Costs 28,725 27,981 744 2,822 3,121 3,316 3,150 3,183 3,247 2,971 3,707 3,208 3,759 3,451 3,557 39,492 38,613
OPERATING EXPENSES TOTAL 137,126 136,649 477 14,669 15,304 15,375 15,186 15,122 15,113 15,316 15,837 15,204 15,621 15,408 15,540 183,695 182,963
OPERATING (PROFIT) / LOSS EBITDA -10,879 -10,509 -370 -1,304 -1,021 -1,478 -1,310 -769 -1,376 -1,100 -1,892 -629 -96 -251 -272 -11,498 -11,154
NON OPERATINGLoss / (Profit) on Asset Disposal 54 0 34 0 0 0 0 0 0 0 0 54 0 0 0 54 0
Impairment of non-current assets 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Depreciation / Amortisation 3,076 2,934 162 335 336 336 336 344 345 345 350 349 354 355 360 4,145 3,911
Interest (Receivable) / Payable -37 -52 15 -3 -3 -3 -3 -3 -4 -4 -4 -10 -7 -7 -7 -58 -70
Public Dividend Capital 1,825 1,793 32 205 205 205 221 233 194 148 204 210 203 203 203 2,434 2,390
NON OPERATING TOTAL 4,918 4,675 243 537 538 538 554 574 535 489 550 603 550 551 556 6,575 6,231
RETAINED (SURPLUS) / DEFICIT -5,961 -5,834 -127 -767 -483 -940 -756 -195 -841 -611 -1,342 -26 454 300 284 -4,923 -4,923
ADJUSTMENTS TO RETAINED SURPLUSDonated Asset Income -30 0 -30 -22 0 0 0 0 0 0 0 -8 0 0 0 -30 0
Donated Asset Depreciation 103 0 103 11 11 11 11 11 11 11 11 11 12 12 13 140 120
Impairment of non-current assets 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
TOTAL ADJUSTMENTS 73 0 73 -11 11 11 11 11 11 11 11 4 12 12 13 110 120
ADJUSTED RETAINED (SURPLUS) / DEFICIT -5,888 -5,834 -54 -778 -472 -929 -745 -184 -830 -600 -1,331 -22 466 312 297 -4,813 -4,803
STATEMENT OF INCOME & EXPENDITUREDECEMBER 2017
Category
Year to Date Monthly Actual / Forecast
As at 31 December 2017
Page 8 of 1219 Financial Performance Report.pdfOverall Page 114 of 218

Appendix 2
SQIP Monitoring 2017/18 - December 2017
Summary of Overall SQIP Monitoring 2017/18
Year to Date Annual
R/NR Plan Plan % of Annual
Actual Actual % of Annual
Variance Risk Rating Plan Out-turn Actual Variance Risk Rating
FYE Forecast
£'s % £'s %
Total SQIP 17/18 £5,278,300 73.3% £5,280,134 73.3% £1,834 0.0% £7,200,000 £7,256,487 £56,487 0.8% £5,303,000Recurrent SQIP R £3,760,500 £3,421,122 -£339,378 -9.0% £5,185,500 £4,886,700 -£298,800 -5.8% £5,303,000Non Recurrent SQIP NR £1,517,800 £1,859,012 £341,212 22.5% £2,014,500 £2,369,787 £355,287 17.6% £0
SQIP Schemes 2017/18
Year to Date Annual
Scheme R/NR Plan Plan % of Annual
Actual Actual % of Annual
Variance Risk Rating Plan Out-turn Actual Variance Risk Rating
FYE Forecast
£'s % £'s %
Integrated Community Based Services Babington 16/17 Scheme (South) R £42,300 100.0% £42,300 100.0% £0 0% £42,300 £42,300 £0 0% £42,300Babington seasonal bed flex (South) NR £21,200 100.0% £21,200 100.0% £0 0% £21,200 £21,200 £0 0% £0St Oswalds seasonal bed flex (South) NR £20,000 100.0% £2,287 11.4% -£17,713 -89% £20,000 £2,287 -£17,713 -89% £0Newholme (Rowsley Ward) seasonal bed flex (North) NR £36,000 100.0% £15,000 41.7% -£21,000 -58% £36,000 £15,000 -£21,000 -58% £0Clay Cross (Alton Ward) seasonal bed flex (North) NR £36,000 100.0% £22,900 63.6% -£13,100 -36% £36,000 £22,900 -£13,100 -36% £0Outstanding Way - Revised Staffing Levels (Joint) R £333,300 66.7% £333,300 66.7% £0 0% £500,000 £500,000 £0 0% £500,000DHU Activity Reduction (South) R £3,800 76.0% £3,800 76.0% £0 0% £5,000 £5,000 £0 0% £5,000DHU Activity Reduction (North) R £9,800 75.4% £9,800 75.4% £0 0% £13,000 £13,000 £0 0% £13,000DHU Clerking (Joint) R £15,000 50.0% £3,500 11.7% -£11,500 -77% £30,000 £3,500 -£26,500 -88% £0Vacancy Review (South) R £112,500 75.0% £112,500 75.0% £0 0% £150,000 £150,000 £0 0% £150,000Vacancy Review (North) R £112,500 75.0% £112,500 75.0% £0 0% £150,000 £150,000 £0 0% £150,000Health, Wellbeing and InclusionStaff Efficiencies Skill Mix R £136,500 75.0% £136,500 75.0% £0 0% £182,000 £182,000 £0 0% £182,000Staffing Levels Review - Childrens NR £225,000 75.0% £372,000 124.0% £147,000 65% £300,000 £447,000 £147,000 49% £0Reduction of Discretionary Non Pay Spend R £127,500 75.0% £127,500 75.0% £0 0% £170,000 £170,000 £0 0% £170,000Underspends NR £52,500 75.0% £70,500 100.7% £18,000 34% £70,000 £88,000 £18,000 26% £0Work in Progress at Contract End NR £0 0.0% £0 0.0% £0 0% £40,000 £36,000 -£4,000 -10% £0Primary Care - additional QOF / Increased Income R £11,300 75.3% £0 0.0% -£11,300 -100% £15,000 £0 -£15,000 -100% £0Primary Care - Mitigations R £0 - £11,300 - £11,300 0% £0 £15,000 £15,000 £15,000Vacancy Review R £112,500 75.0% £80,925 54.0% -£31,575 -28% £150,000 £107,900 -£42,100 -28% £150,000Vacancy Review NR £0 - £31,575 - £31,575 0% £0 £42,100 £42,100 0% £0Planned Care and Outpatient ServicesStaffing Review R £82,500 75.0% £87,397 79.5% £4,897 6% £110,000 £110,000 £0 0% £110,000Orthotics/Seating Wheelchairs R £30,000 50.0% £0 0.0% -£30,000 -100% £60,000 £15,000 -£45,000 -75% £76,000Sterile Services & Decontamination R £0 0.0% £0 0.0% £0 0% £10,000 £3,300 -£6,700 -67% £10,000General Appliances R £26,300 75.1% £26,300 75.1% £0 0% £35,000 £35,000 £0 0% £35,000Trust Admin - Digital Dictation R £13,500 75.0% £13,500 75.0% £0 0% £18,000 £18,000 £0 0% £18,000Integrated Facilities ManagementWaste Management Reduction (Trust & Service Wide) R £22,500 75.0% £0 0.0% -£22,500 -100% £30,000 £0 -£30,000 -100% £30,000Procurement Scheme - Energy Utility R £187,500 75.0% £187,500 75.0% £0 0% £250,000 £250,000 £0 0% £250,000IFM Workforce Optimisation R £397,500 75.0% £397,500 75.0% £0 0% £530,000 £530,000 £0 0% £530,000Printers / Copiers (Trust & Service Wide) R £15,000 75.0% £0 0.0% -£15,000 -100% £20,000 £0 -£20,000 -100% £0EstatesEstates 16/17 Schemes - FYE R £29,800 75.1% £29,800 75.1% 0 0% £39,700 £39,700 £0 0% £39,700CorporateCorporate Non Pay Efficiencies R £75,000 75.0% £75,000 75.0% £0 0% £100,000 £100,000 £0 0% £100,000SBS Contract Review R £67,500 75.0% £67,500 75.0% £0 0% £90,000 £90,000 £0 0% £90,000Back Office Functions R £506,300 75.0% £530,300 78.6% £24,000 5% £675,000 £683,000 £8,000 1% £675,000Corporate Vacancy Freeze NR £375,000 75.0% £372,500 74.5% -£2,500 -1% £500,000 £482,000 -£18,000 -4% £0VOIP Implementation R £62,500 50.0% £20,100 16.1% -£42,400 -68% £125,000 £75,000 -£50,000 -40% £150,000ALPS (annual leave purchase scheme) R £71,300 75.1% £71,300 75.1% £0 0% £95,000 £95,000 £0 0% £95,000Records Management R £45,000 75.0% £45,000 75.0% £0 0% £60,000 £60,000 £0 0% £60,000Library Services - SLA Review R £4,800 50.5% £0 0.0% -£4,800 -100% £9,500 £0 -£9,500 -100% £0OtherNon Pay Inflation Reserve - Zero Inflation Purchases R £225,000 75.0% £225,000 75.0% £0 0% £300,000 £300,000 £0 0% £300,000Reserves Review R £273,000 75.0% £273,000 75.0% £0 0% £364,000 £364,000 £0 0% £364,000Capital charge review 16/17 R £67,500 75.0% £0 0.0% -£67,500 -100% £90,000 £90,000 £0 0% £90,000Capital charge review 17/18 R £75,000 75.0% £0 0.0% -£75,000 -100% £100,000 £100,000 £0 0% £100,000Income Target NR £375,000 75.0% £375,000 75.0% £0 0% £500,000 £500,000 £0 0% £0Rates Rebates NR £161,000 75.0% £161,000 75.0% £0 0% £214,600 £214,600 £0 0% £0Apprenticeship Levy - Maximise Utilisation R £75,000 75.0% £17,000 17.0% -£58,000 -77% £100,000 £23,000 -£77,000 -77% £100,000Walton Land - Capital Revaluation R £10,000 66.7% £0 0.0% -£10,000 -100% £15,000 £15,000 £0 0% £20,000Over-achievement 2016/17 R £172,500 75.0% £172,500 75.0% £0 0% £230,000 £230,000 £0 0% £230,000Non Recurrent Benefits NR £150,000 75.0% £150,000 75.0% £0 0% £200,000 £200,000 £0 0% £0
Total £5,003,700 £4,806,584 -£197,116 £6,801,300 £6,635,787 -£165,513 £4,850,000MITIGATIONS
Scheme R/NR
Depreciation Charge Rebase NR £5,800 £5,800 75.3% £0 0% £7,700 £7,700 £0 £0ALPS (annual leave purchase scheme) additional 17/18 NR £26,300 75.1% £28,500 81.4% £2,200 8% £35,000 £38,000 £3,000 9% £0Void space - rent reduction Newholme R £0 0.0% £0 0.0% £0 0% £44,000 £44,000 £0 0% £175,0002 * 11 bedded wards at Ilkeston (July to Oct) NR £34,000 100.0% £34,000 100.0% £0 0% £34,000 £34,000 £0 0% £0In Year Reserves Review R £208,500 75.0% £208,500 75.0% £0 0% £278,000 £278,000 £0 0% £278,000HWI - Derby City Sexual Health - reduction in contract NR £0 - £66,750 - £66,750 £0 £89,000 £89,000 £0HWI - LLBD - NR benefit to loss of contract NR £0 - £130,000 - £130,000 £0 £130,000 £130,000 £0
Total £274,600 £473,550 £198,950 £398,700 £620,700 £222,000 £453,000
£5,278,300 £5,280,134 £1,834 £7,200,000 £7,256,487 £56,487 £5,303,000
Page 9 of 1219 Financial Performance Report.pdfOverall Page 115 of 218

Appendix 3
1 2 3 4 5 6 7 8 9 10 11 122016-17 Annual Annual
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Outturn PlanEnd Actual Plan Variance Actual Actual Actual Actual Actual Actual Actual Actual Actual Forecast Forecast Forecast Outturn
£'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s
ASSETSNon Current
Tangible Assets 83,612 86,413 85,426 987 83,564 83,570 83,501 83,593 83,939 83,982 84,206 84,555 86,413 86,089 85,914 85,739 85,450
Intangible Assets 2,535 2,401 1,788 613 2,483 2,497 2,456 2,488 2,459 2,435 2,384 2,332 2,401 2,401 2,401 2,501 1,767
Total Non Current Assets 86,147 88,814 87,214 1,600 86,047 86,067 85,957 86,081 86,398 86,417 86,590 86,887 88,814 88,490 88,315 88,240 87,217
CurrentInventories 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
NHS Trade Receivabes 112 1,246 1,416 (170) 921 2,290 3,034 2,167 2,097 1,775 2,667 1,694 1,246 906 981 1,056 1,616
Non NHS Trade Receivabes 1,077 2,235 910 1,325 2,224 2,230 2,099 882 1,048 813 1,173 2,383 2,235 1,035 1,185 1,335 910
PDC Dividend Receivable 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Bad Debt Provision (218) (279) (200) (79) (224) (227) (245) (255) (258) (267) (276) (277) (279) (250) (250) (250) (200)
Capital Receivables 44 80 0 80 22 22 0 0 0 0 0 35 80 45 45 0 0
Accrued Income 3,411 3,128 2,712 416 3,189 3,552 4,185 2,718 2,159 2,146 2,097 3,538 3,128 3,228 2,028 2,128 2,712
Prepayments 808 1,062 800 262 1,135 1,681 1,604 1,747 1,546 1,369 1,510 1,233 1,062 1,092 1,102 1,102 800
Other Receivables 838 817 838 (21) 691 774 796 955 688 814 840 807 817 820 820 820 838
Land Held For Sale 3,100 3,100 3,100 0 3,100 3,100 3,100 3,100 3,100 3,100 3,100 3,100 3,100 0 0 0 0
Cash and Cash Equivalents 21,402 23,559 20,908 2,651 19,338 18,904 18,371 23,745 25,922 25,877 26,564 24,801 23,559 27,524 26,619 23,528 21,374
Total Current Assets 30,574 34,948 30,484 4,464 30,396 32,326 32,944 35,059 36,302 35,627 37,675 37,314 34,948 34,400 32,530 29,719 28,050
TOTAL ASSETS 116,721 123,762 117,698 6,064 116,443 118,393 118,901 121,140 122,700 122,044 124,265 124,201 123,762 122,890 120,845 117,959 115,267
LIABILITIESCurrent
Trade Payables (4,606) (5,405) (3,669) (1,736) (2,851) (2,898) (2,011) (3,860) (5,085) (4,748) (7,169) (6,005) (5,405) (6,349) (4,549) (3,605) (3,975)
Other Payables (5,071) (4,064) (4,100) 36 (4,378) (4,218) (4,128) (4,162) (4,126) (4,094) (4,136) (4,142) (4,064) (4,161) (4,161) (4,161) (4,100)
Public Dividend Capital Payable (1) (595) (615) 20 (205) (410) (615) (837) (1,070) (33) (181) (385) (595) (798) (1,001) 0 0
Capital Payables (850) (893) (153) (740) (402) (567) (190) (439) (400) (457) (599) (662) (893) (563) (593) (153) (153)
Accrued Expenditure (3,847) (4,486) (1,948) (2,538) (5,431) (6,402) (6,555) (5,905) (5,670) (5,943) (4,046) (4,404) (4,486) (3,542) (3,542) (3,542) (1,988)
Annual Leave Accrual (474) (474) (474) 0 (474) (474) (474) (474) (474) (474) (474) (474) (474) (474) (474) (434) (434)
Deferred Income, Current (307) (510) (189) (321) (356) (605) (1,188) (1,003) (1,322) (936) (1,690) (818) (510) (330) (164) 0 (389)
Provisions, Current (637) (514) (244) (270) (617) (617) (635) (611) (517) (493) (503) (513) (514) (514) (514) (514) (244)
Other Liabilities 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Total Current Liabilities (15,793) (16,941) (11,392) (5,549) (14,714) (16,191) (15,796) (17,291) (18,664) (17,178) (18,798) (17,403) (16,941) (16,731) (14,998) (12,409) (11,283)
Non CurrentDeferred Income, Non Current 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Provisions, Non Current (30) (30) (60) 30 (30) (30) (30) (30) (30) (30) (30) (30) (30) (30) (30) (30) (60)
Total Non Current Liabilities (30) (30) (60) 30 (30) (30) (30) (30) (30) (30) (30) (30) (30) (30) (30) (30) (60)
TOTAL LIABILITIES (15,823) (16,971) (11,452) (5,519) (14,744) (16,221) (15,826) (17,321) (18,694) (17,208) (18,828) (17,433) (16,971) (16,761) (15,028) (12,439) (11,343)
TOTAL ASSET EMPLOYED 100,898 106,791 106,246 545 101,699 102,172 103,075 103,819 104,006 104,836 105,437 106,768 106,791 106,129 105,817 105,520 103,924
TAXPAYERS' EQUITYPublic Dividend Capital 243 243 243 0 243 243 243 243 243 243 243 243 243 243 243 243 243
Retained Earnings 75,493 81,388 81,327 61 76,296 76,769 77,672 78,416 78,603 79,433 80,034 81,365 81,388 80,922 80,610 80,313 79,005
Revaluation Reserve 25,162 25,160 24,676 484 25,160 25,160 25,160 25,160 25,160 25,160 25,160 25,160 25,160 24,964 24,964 24,964 24,676
TOTAL TAXPAYERS EQUITY 100,898 106,791 106,246 545 101,699 102,172 103,075 103,819 104,006 104,836 105,437 106,768 106,791 106,129 105,817 105,520 103,924
Year to DateAs at 31 December 2017
Monthly Actual / Forecast
STATEMENT OF FINANCIAL POSITION 2017-1831 DECEMBER 2017
Page 10 of 1219 Financial Performance Report.pdfOverall Page 116 of 218

Appendix 41 2 3 4 5 6 7 8 9 10 11 12
Annual Annual Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Outturn Plan
Actual Plan Variance Actual Actual Actual Actual Actual Actual Actual Actual Actual Forecast Forecast Forecast Forecast Outturn£'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s
SURPLUS / (DEFICIT) 5,893 5,834 59 779 473 929 745 184 830 600 1,331 22 (466) (312) (297) 4,818 4,444
Less Non Operating Income / ExpenditureFinance Income / Charges (37) (45) 8 (3) (3) (3) (3) (3) (4) (4) (4) (10) (7) (7) (7) (58) (70)
Depreciation and Amortisation 3,196 2,889 307 346 347 347 347 356 356 356 361 380 366 367 373 4,302 3,911
Donated Asset Income (8) 0 (8) 0 0 0 0 0 0 0 0 (8) 0 0 0 (8) 0
PDC Dividend Expense 1,825 1,845 (20) 205 205 205 221 233 194 148 204 210 203 203 203 2,434 2,390
Impairment Losses and Losses on Disposal of PPE 34 0 34 0 0 0 0 0 0 0 0 34 0 0 0 34 0
Other non-cash adjustments (944) 0 (944) 0 (944) 0 0 0 0 0 0 0 (196) 0 0 (1,140) 0
OPERATING CASHFLOWS BEFORE MOVEMENTS IN WORKING CAPITAL 9,959 10,523 (564) 1,327 78 1,478 1,310 770 1,376 1,100 1,892 628 (100) 251 272 10,382 10,675
Inventories 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
NHS Trade Receivabes (1,129) (1,304) 175 (809) (1,369) (744) 867 73 322 (891) 973 449 338 (75) (77) (943) (1,504)
Non NHS Trade Receivabes (1,095) 149 (1,244) (1,141) (3) 149 1,227 (163) 244 (351) (1,207) 150 1,171 (150) (150) (224) 149
Accrued Income 258 699 (441) 222 (363) (658) 1,467 559 13 49 (1,441) 410 (100) 1,200 (100) 1,258 699
Prepayments (254) 8 (262) (327) (546) 77 (143) 201 177 (141) 277 171 (30) (10) 0 (294) 8
Other Receivables 21 0 21 147 (83) (22) (159) 267 (126) (26) 33 (10) (3) 0 0 18 0
Trade Payables 799 (847) 1,646 (1,755) 47 (887) 1,849 1,225 (337) 2,421 (1,164) (600) 944 (1,800) (944) (1,001) (631)
Other Payables (63) (971) 908 251 (160) (90) 34 (36) (32) 42 6 (78) 97 0 0 34 (971)
Accrued Expenditure 639 (955) 1,594 640 1,915 153 (650) (235) 273 (1,897) 358 82 (944) 0 0 (305) (1,859)
Annual Leave Accrual 0 0 0 0 0 0 0 0 0 0 0 0 0 0 (40) (40) (40)
Deferred Income, Current & Non Current 203 (118) 321 49 249 583 (185) 319 (386) 754 (872) (308) (180) (166) (164) (307) 82
Provisions, Current & Non Current (123) (363) 240 (20) 0 18 (24) (94) (24) 10 10 1 0 0 0 (123) (363)
Increase / (Decrease) in working capital (744) (3,702) 2,958 (2,743) (313) (1,421) 4,283 2,116 124 (30) (3,027) 267 1,293 (1,001) (1,475) (1,927) (4,430)
NET CASHFLOW FROM OPERATIONS 9,215 6,821 2,394 (1,416) (235) 57 5,593 2,886 1,500 1,070 (1,135) 895 1,193 (750) (1,203) 8,455 6,245
Property, Plant & Equipment Expenditure (5,870) (5,477) (393) (225) (367) (238) (470) (673) (375) (529) (660) (2,333) (40) (192) (298) (6,400) (6,400)
Proceeds on Disposal of Property, Plant & Equipment 0 0 0 0 0 0 0 0 0 0 0 0 3,100 0 0 3,100 3,100
(Increase) / Decrease in Capital Receivables (36) 44 (80) 22 0 22 0 0 0 0 (35) (45) 35 0 45 44 44
Increase / (Decrease) in Capital Payables 42 (697) 739 (448) 165 (377) 248 (39) 57 142 63 231 (330) 30 (440) (698) (697)
NET CASHFLOW FROM INVESTING ACTIVITIES (5,864) (6,130) 266 (651) (202) (593) (222) (712) (318) (387) (632) (2,147) 2,765 (162) (693) (3,954) (3,953)
PDC Dividends Paid (1,231) (1,230) (1) 0 0 0 0 0 (1,231) 0 0 0 0 0 (1,202) (2,433) (2,390)
PDC Received 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Interest Received on Cash and Cash Equivalents 37 45 (8) 3 3 3 3 3 4 4 4 10 7 7 7 58 70
NET CASHFLOW FROM FINANCING ACTIVITIES (1,194) (1,185) (9) 3 3 3 3 3 (1,227) 4 4 10 7 7 (1,195) (2,375) (2,320)
NET CASH INFLOW / (OUTFLOW) 2,157 (494) 2,651 (2,064) (434) (533) 5,374 2,177 (45) 687 (1,763) (1,242) 3,965 (905) (3,091) 2,126 (28)
Opening Cash Balance 21,402 21,402 0 21,402 19,338 18,904 18,371 23,745 25,922 25,877 26,564 24,801 23,559 27,524 26,619 21,402 21,402
Net Cash Inflow / (Outflow) 2,157 (494) 2,651 (2,064) (434) (533) 5,374 2,177 (45) 687 (1,763) (1,242) 3,965 (905) (3,091) 2,126 (28)
CLOSING CASH BALANCE 23,559 20,908 2,651 19,338 18,904 18,371 23,745 25,922 25,877 26,564 24,801 23,559 27,524 26,619 23,528 23,528 21,374
OPERATING ACTIVITIES
INVESTING ACTIVITES
FINANCING ACTIVITES
CASHFLOW STATEMENT 2015/1631 DECEMBER 2017
As at 31 December 2017Monthly Actual / ForecastYear to Date
Page 11 of 1219 Financial Performance Report.pdfOverall Page 117 of 218

Appendix 5
1 2 3 4 5 6 7 8 9 10 11 12Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Actual Actual Actual Actual Actual Actual Actual Actual Actual Forecast Forecast Forecast£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
SAFETY AND STATUTORYA5106 Theatre Air Handling Unit/Upgrade to Ventilation Plant Ilkeston Hospital Backlog 190.0 6.2 228.7 0.4 1.0 18.6 20.0 274.9 (84.9)A5133 Upgrade Castle Street Backlog 50.0 50.0A5134 Upgrade Ripley MC Backlog 50.0 50.0A5140 Spencer Ward Service Riser Cavendish Hospital BacklogA5141 Replacement Boiler Rockley Core Unit Backlog 7.8 (1.3) 6.5 (6.5)A5146 Replacement Boiler Walton Hospital Backlog 6.6 6.6 (6.6)A5135 Defibrillators Various Equipment 28.0 26.9 0.4 27.3 0.7A5136 Theatre Monitoring Kit Ilkeston Hospital Equipment 25.0 25.3 25.3 (0.3)A5137 Podiatry Power Kit x 3 TBA Equipment 28.5 28.9 0.3 29.2 (0.7)A5144 UTC Kit Various Equipment 85.8 70.2 70.2 15.6Various Replace service critical equipment Various Equipment 27.7 43.0 43.0 (15.3)
STAY IN BUSINESSA5432 Desktop renewal and local infrastructure Various IM&T 300.0 15.7 11.9 22.9 20.7 52.3 12.0 46.2 20.0 24.5 20.0 20.0 20.0 286.2 13.8A5434 LAN/WAN Infrastructure Various IM&T 290.0 3.7 76.9 (0.1) 2.9 19.8 50.0 153.2 136.8A5116 Fire Stopping Ilkeston Hospital Estates 18.4 (3.6) 0.9 2.6 0.3 (0.1) 18.5 (18.5)A5138 Replace floor in ward areas Ilkeston Hospital Estates 15.9 17.0 (3.3) 0.2 29.8 (29.8)A5132 VOIP project Various IM&T 19.2 17.2 (4.6) 73.5 (19.8) 0.8 16.1 26.6 129.0 (129.0)Various Staff costs Pro rata Estates 200.0 17.5 18.4 18.3 18.3 17.4 18.4 18.1 18.1 18.0 18.1 18.1 18.1 216.8 (16.8)
SYSTEM TRANSFORMATIONA5050 Site Development - Stage 2 Heanor Hospital Estates 2,500.0 181.9 199.6 194.8 268.4 250.0 183.0 339.8 584.6 48.8 2,250.9 249.1A5057 Site Development - enabling and fees Belper Estates 400.0 14.2 6.0 (2.8) 2.8 110.9 226.1 357.2 42.8N/A Purchase of Land Buxton Estates 1,400.0 1,780.0 1,780.0 (380.0)A5105 Site Development - enabling and fees Buxton Estates 50.0 (4.3) 1.5 4.2 3.0 0.2 0.6 10.7 2.0 4.0 5.0 26.9 23.1A5123 Site Development - Stage 3 Walton Hospital Estates 7.5 7.5 (7.5)
SUSTAINABLE QUALITY IMPROVEMENT PLAN (SQIP)A5473 IM&T - Mobile working Various IM&T 325.0 95.0 12.3 88.7 130.0 326.0 (1.0)A5435 IM&T - PAS Replacement Various IM&T 100.0 55.9 22.5 24.5 102.9 (2.9)A5139 Brookdale Refurbishment Ash Green Estates 7.0 53.6 10.2 7.8 (0.1) 78.5 (78.5)
EXPANSIONARY
OTHERCONT Contingency Various Contingency 350.0 161.5 161.5 188.5PREV Expenditure relating to 2016-17 schemes Various Prior year 14.6 24.0 (22.3) (11.4) 0.2 1.5 (2.3) 0.1 (12.3) (7.9) 7.9
Capital Programme Expenditure 6,400.0 225.4 366.8 237.5 470.6 673.0 375.1 528.9 659.2 2,333.7 40.1 192.1 297.6 6,400.0 (0.0)
DONATEDDON Phlebotomy Suite Ripley Hospital Donated 34.5 45.4 45.0 45.0 45.1 215.0 (215.0)
Capital Programme Expenditure 34.5 45.4 45.0 45.0 45.1 215.0 (215.0)
CAPITAL PROGRAMME 2017-1831 DECEMBER 2017
Scheme Number Scheme Description Category 2017-18
PlanPlan v
ForecastFull Year ForecastLocation
Page 12 of 1219 Financial Performance Report.pdfOverall Page 118 of 218

TRUST BOARD Document Title: Board Assurance Framework (BAF) Quarter 3
Presenter/Title: Kirsteen Farrar, Associate Director of Corporate Governance/ Trust Secretary
Contents of Paper were previously discussed by:
Quality Service, Quality People and Quality Business Committees in September 2017 and Audit and Assurance Committee in January 2018
Author/Title: Melanie Curd, Deputy Trust Secretary Contact Email and Telephone Number: [email protected]
Date of Meeting: 25 January 2018 Agenda Item No: 20/18
No of pages inc. this one: 36
Has an Equality Impact Assessment been undertaken Yes No x
Document is for: (more than one box can be ticked) Information x Decision x Assurance x
Purpose of Paper
The purpose of the paper is to present the Board Assurance Framework (BAF) to the Board for approval.
Recommendations
The Board is asked to approve the Board Assurance Framework for Quarter 3.
Board Assurance Framework Risk Reference
4.3 - There is a risk to the organisation due to not having strong risk management controls in place resulting in failure to put effective mitigation plans in place promptly
Financial Impact
There is no direct financial impact linked to this report.
Further Information and Appendices
There are currently 33 strategic risks on the BAF. Each individual section of the BAF has been reviewed by the appropriate Quality Committee in January and the following amendments made; Quality Service Committee (QSC) 1.5 – the risk score has been reduced to L1 x C4 1.6 – The risk score has been reduced to L1 x C5 1.9 – The risk score has been reduced to L3 x C4 These amendments will be reflected in the Quarter 4 BAF. In addition, QSC requested an update for the March meeting on the position regarding tenders and assurances from acquired services
Page 1 of 3620 BAF Q3.pdfOverall Page 119 of 218

(GP, Derby City, Children’s and Sexual Health Services) to ensure they are meeting quality metrics which will help inform the level of BAF risk for 1.1 and 1.2. Quality Business Committee 3.13 - the target risk score has been amended to L2xC4 This will be reflected in the Quarter 4 BAF. Quality People Committee (QPC) There were no amendments when the Quality People section of the BAF was reviewed at QPC. The Audit and Assurance Committee (AAC) reviewed the BAF in its entirety at the meeting held on 19 January 2018 an update will be provided to Board via the AAC Summary Report. Attached is the Summary View of the BAF which details all areas of limited assurance. Assurance is formally recorded on the BAF using the colour scheme below:
• Green – Significant Assurance • Amber – Limited Assurance with clear action to resolve, • Red – Negative Assurance
Further to the Board Development Session held in October 2017, a new BAF will be in place from the 1 April 2018 which members of the Quality Committees have been involved in the discussion and development of. The revised BAF will reflect the changing landscape and will be further reviewed by the Executive Team on 5 February 2018; with the entire Board after the private Board meeting on 22 February 2018 and with the Quality Committees in March 2018.
Monitoring Information Brief Summary
What are the Governor involvement implications?
The Governors receive the BAF on a quarterly basis as part of the Board papers.
What are the Equality, Diversity and Inclusion implications?
There are specific risks on the BAF in relation to Equality, Diversity and Inclusion.
What are the Patient, Public, Staff, Member and Stakeholder involvement implications?
The BAF is a public document and in the public domain.
Risk Register
Is the issue on the current Risk Register? N/A If yes, what is the Risk Number?
Does this update recommend a change in the current risk score? (If so, please provide your rationale below)
All operational risks are aligned to the BAF risks. This allows an operational profile to be established. These have been updated on the BAF as of 8 January 2018.
Page 2 of 3620 BAF Q3.pdfOverall Page 120 of 218

DCHS NHS Foundation Trust Board Assurance Framework
QUALITY SERVICE - 2017-18 - Quarter 3 Risk Score Summaries
BAF No Risk Description
Target Risk
Score
Timeframe to achieve
Target Risk Score
Movement 2016/17
Q4 Risk
Score
2017/18 Q1
Risk Score
2017/18 Q2
Risk Score
2017/18 Q3
Risk Score
1.1 There is a risk to management capacity and overall service continuity from the process of bidding for and acquiring new services and/or the requirement to retender for existing services
8 L2xC4 April 2018 12
L3xC4 12
L3xC4 12
L3xC4 12
L3xC4
1.2
There is a risk to comprehensive patient information due to discontinuity between systems employed NB: Following discussion at Quality Service Committee in September 2017 the timeframe was extended to April 2018
8 L2xC4 April 2018 12
L3xC4 12
L3xC4 12
L3xC4 12
L3xC4
1.3 There is a risk to the provision of safe, effective care due to a lack of consistent clinical leadership and expertise
5 L1xC5 April 2018 10
L2xC5 10
L2xC5 10
L2xC5 10
L2xC5
1.4 There is a risk that DCHS does not provide patient centred care due to a lack of engagement and involvement of service users and stakeholders
8 L2xC4 N/A 8
L2xC4 8
L2xC4 8
L2xC4 8
L2xC4
1.5 There is a risk that our Clinical Governance initiatives do not deliver the outcomes necessary to support our strategy for high quality care
4 L1xC4 April 2018 8
L2xC4 8
L2xC4 8
L2xC4 8
L2xC4
1.6 There is a risk to the provision of safe, effective care due to a lack of consistent employment of the trust’s quality improvement and assurance framework
5 L1xC5 April 2018 10
L2xC5 10
L2xC5 10
L2xC5 10
L2xC5
1.7 There is a risk to the provision of effective care due to a failure to learn and share lessons and implement change resulting from audit and feedback
4 L1xC4 April 2018 8
L2xC4 8
L2xC4 8
L2xC4 8
L2xC4 Page 3 of 3620 BAF Q3.pdf
Overall Page 121 of 218

BAF No Risk Description
Target Risk
Score
Timeframe to achieve
Target Risk Score
Movement 2016/17
Q4 Risk
Score
2017/18 Q1
Risk Score
2017/18 Q2
Risk Score
2017/18 Q3
Risk Score
1.8 There is an overarching risk to patient quality and safety during periods of major system change and employment of new governance systems and processes related to place based care.
8 L2xC4 April 2018 12
L3xC4 12
L3xC4 12
L3xC4 12
L3xC4
1.9 There is a risk to population health through the failure to fully embed public health principles within DCHS service delivery impacting on the ability to reduce inequalities in access and outcomes for our populations
8 L2xC4 April 2018 16
L4xC4 16
L4xC4 16
L4xC4 16
L4xC4
Page 4 of 3620 BAF Q3.pdfOverall Page 122 of 218

QUALITY SERVICE - Quarter 3 2017-18
Objective: To deliver high quality and sustainable services that echo the values and aspirations of the communities that we serve
Lead Committee: Quality Service Committee, chaired by Chris Bentley, Non-Executive Director Lead Executive Director: Carolyn White, Director of Quality/ Chief Nurse Strategic Priorities 2017/18 1. Ensure delivery of safe and clinically effective services 2. Ensuring a positive patient experience and meaningful engagement 3. Develop comprehensive and effective systems of quality improvement and assurance Summary of Quality Service BAF Risks by Lead Executive Director: During Quarter 3 we have continued to be rated Green in the quarterly quality surveillance meeting by NHS England. Positive assurance has been received in relation to the majority of risk areas within the quality section of the BAF. Staff within the Health, Wellbeing and Inclusion division are once again working hard with regard to the tendering of services and it will be important to monitor performance in this area to ensure that this additional work does not have a detrimental impact on service delivery. The People and Organisational Effectiveness Team are working with operational and quality managers to develop the Organisational Leadership Strategy. This will be integral in improving our risk management in relationship to consistent quality outcomes and patient care. During this reporting period Quality Always has been formally reviewed and has met all its key performance indicators for the year, this provides valuable assurance against the BAF risk related to clinical governance initiatives supporting the Trust’s strategy for high quality care. Progress is starting to be made in identifying assurance against the BAF risk in relation to population health. This is important to note and we will need to continue to drive improvements in this area as we develop our strategies for the coming year.
Page 5 of 3620 BAF Q3.pdfOverall Page 123 of 218

Areas for improvement Risk areas continue to be in relation to chronic wound care in particular the management of pressure ulcers. A Tissue Viability Strategy will be presented to QSC in January which will identify the specific actions we will be taking in relation to pressure ulcers, leg ulcers, diabetic foot ulcers and complex wound healing requiring vacuum therapy. The areas of work identified for improvement at the Equality, Diversity and Inclusion Deep Dive /Sessions in Autumn 2017 are being developed and progressed. Good progress has been made with establishing mortality reviews with the policy and terms of reference for the Mortality Review Group being developed and associated reporting to the Board. As the reporting process develops, the more positive assurance will be received. The Board has supported investment to support this process.
Page 6 of 3620 BAF Q3.pdfOverall Page 124 of 218

Board Assurance Framework Risk 1.1 Risk Register ID 2990 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to management capacity and overall service continuity from the process of bidding for and acquiring new services and/or the requirement to retender for existing services. Lead Committee/Group:
Q3 - L3 x C4=12 Q4 - L3 x C4=12 Q1 - L3 x C4=12 Q2 - L3 x C4=12
L3 x C4=12 Medium
High Medium Low
0 1 0
Controls Identified 1. Comprehensive due diligence checks including quality
assessment and staffing profile 2. Risk Strategy and Register 3. Central corporate team to
coordinate processes 4. Commercial Strategy
All papers presented for Assurance in Quarter 3 were received positively with the exception of: Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Pressure Ulcer Ambition 1 Report – patient outcome (CSG) Oct: Grade 3 pressure ulcer reporting above upper limits for 3rd
month running (a) Oct: Ongoing monitoring and deep dives into the issues leading up to removal of the potential grade 3 category
Infection Prevention and Control Summary Report – Continence/E coli bacteraemia Update(CSG)
Oct: Target of reducing bacteraemia by 50% not yet reached (a)
Oct: Action plan to be monitored/updated at IP&C and shared with CSG via summary report
Infection Prevention and Control Summary Report – Ventilation Risk and Management (CSG)
Oct: Current non-compliant areas are sexual health, Coleman Street, Revive Leg Ulcer Clinics and DTC, Ilkeston (a)
Oct: All sites are currently being reviewed, updates to be reported to future IP&C Group
Board Assurance Framework Risk 1.2 Risk Register ID 2991 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to comprehensive patient information due to discontinuity between systems employed Lead Committee/Group:
Q3 - L3 x C4=12 Q4 - L3 x C4=12 Q1 - L3 x C4=12 Q2 - L3 x C4=12
L3 x C4 = 12 Medium
High Medium Low
0 6 2
Controls Identified 1. IMT strategy and provision of TPP SystmOne across all services 2. Records audits 3. Information Governance group 4. Caldicott Guardian All papers presented for Assurance in Quarter 3 were received positively with the exception of: Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Pressure Ulcer Ambition 1 Report – patient outcome (CSG) Oct: Grade 3 pressure ulcer reporting above upper limits for 3rd
month running (a) Oct: Ongoing monitoring and deep dives into the issues leading up to removal of the potential grade 3 category
Page 7 of 3620 BAF Q3.pdfOverall Page 125 of 218

Board Assurance Framework Risk 1.3 Risk Register ID 2992 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the provision of safe, effective care due to a lack of consistent clinical leadership and expertise Lead Committee/Group:
Q3 - L2 x C5 = 10 Q4 - L2 x C5 = 10 Q1 - L2 x C5 = 10 Q2 - L2 x C5 = 10
L2 x C5 = 10 Medium
High Medium Low
1 0 0
Controls Identified 1. NICE standards and review group 2. Rotating clinicians from acute services 3. Policies and procedure 4. Quality Always Process All papers presented for Assurance in Quarter 3 were received positively with the exception of: Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Pressure Ulcer Ambition 1 Report – patient outcome (CSG) Oct: Grade 3 pressure ulcer reporting above upper limits for 3rd
month running (a) Oct: Ongoing monitoring and deep dives into the issues leading up to removal of the potential grade 3 category
Board Assurance Framework Risk 1.4 Risk Register ID 2993 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk that DCHS does not provide patient centred care due to a lack of engagement and involvement of service users and stakeholders Lead Committee/Group:
Q3 - L2 x C4 = 8 Q4 - L2 x C4 = 8 Q1 - L2 x C4 = 8 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 0 0
Controls Identified 1. Patient and engagement and experience group 2. EDILF 3. Stakeholder focus and engagement groups 4. Council of Governors 5. Policies related to Duty of candour 6. Insight visits 7. Consultation and engagement Processes All papers presented for Assurance in Quarter 3 were received positively with the exception of Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Health, Wellbeing and Inclusion Quarterly Report (PEEG) Oct: Waiting times in Sexual Health (c)
Oct: Lack of Health Psychology and Health Promotion feedback (c)
Oct: Plan is in place to improve waiting times Oct: Missing elements to be reported going forward
Commissioning for Quality and Innovation (CQUIN) Update Report
Nov: Financial risk of not meeting CQUIN targets which were formulated for the acute setting and not for the community environment (a)
Nov: The risk score to be reviewed and the risk to be referred to QBC for oversight
Dignity in Care Report (PEEG) Oct: 27 services have expired Dignity Awards (a) Oct: TME has approved work towards Derbyshire Dignity Award linking with Quality Always accreditation, a plan was agreed to address the issues
Page 8 of 3620 BAF Q3.pdf
Overall Page 126 of 218

Board Assurance Framework Risk 1.5 Risk Register ID 2994 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk that our Clinical Governance initiatives do not deliver the outcomes necessary to support our strategy for high quality care Lead Committee/Group:
Q3 - L2 x C4 = 8 Q4 - L2 x C4 = 8 Q1 - L2 x C4 = 8 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 1 0
Controls Identified 1. Quality Improvement and Assurance Framework 2. Quality Always Process 3. Clinical policies and procedures 4. Datix Risk Management System 5. Learning Lessons Panel All papers presented for Assurance in Quarter 3 were received positively Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Research Champions Update (RIG) Oct: Loss of Integrated Community Services Research
Champion (a) Oct: Vacancy has been filled, new champion commences in November 2017
Update Report from Clinical Studies Development Officer (RIG) Oct: The loss of the role of Principal Investigator means all primary care research studies are being withdrawn (a)
Oct: Meeting to take place on 24/11/17 with senior representatives of the Clinical Research Network to discuss current situation. An action plan formulated to provide assurance that all primary care study closure requirements have been completed
Learning Disability Forensic Service Activity Nov: Risk raised to 16 in respect of patients in the north of the county (a)
Nov: Medical Director to write to the National Leadership for Policy at NHS England to highlight the change in risk
Research and Innovation Group Summary Report Nov: Recent resignation of the Clinical Director will result in a loss of research income for the trust (a)
Nov: Medical Director to prepare a paper for the next QSC on moving forward and next steps more generally
Update Report Research Officer (RIG) Oct: Ongoing capacity challenges due to long term absence in the team (a)
Oct: New research officer in post
Board Assurance Framework Risk 1.6 Risk Register ID 3056 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the provision of safe, effective care due to a lack of consistent employment of the trust’s quality improvement and assurance framework Lead Committee/Group:
Q3 - L2 x C5 = 10 Q4 - L2 x C5 = 10 Q1 - L2 x C5 = 10 Q2 - L2 x C5 = 10
L2 x C5 = 10 Medium
High Medium Low
1 12 1
Controls Identified 1. Quality Improvement and Assurance Framework 2. Quality Always Process 3. Clinical policies and procedures 4. Datix Risk Management System 5. Insight and Back to the floor visits 6. Triangulation Visits All papers presented for Assurance in Quarter 3 were received positively
Page 9 of 3620 BAF Q3.pdfOverall Page 127 of 218

Board Assurance Framework Risk 1.7 Risk Register ID 3057 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the provision of effective care due to a failure to learn and share lessons and implement change resulting from audit and feedback Lead Committee/Group:
Q3 - L2 x C4 = 8 Q4 - L2 x C4 = 8 Q1 - L2 x C4 = 8 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 0 0
Controls Identified 1. Lessons Learned Panel 2. Datix Risk Management System 3. Clinical Audit Programme All papers presented for Assurance in Quarter 3 were received positively Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Infection Prevention and Control Summary Report – Continence/E coli bacteraemia Update(CSG)
Oct: Target of reducing bacteraemia by 50% not yet reached (a)
Oct: Action plan to be monitored/updated at IP&C and shared with CSG via summary report
Infection Prevention and Control Summary Report – Ventilation Risk and Management (CSG)
Oct: Current non-compliant areas are sexual health, Coleman Street, Revive Leg Ulcer Clinics and DTC, Ilkeston (a)
Oct: All sites are currently being reviewed, updates to be reported to future IP&C Group
Review of end of life questions on DATIX (CSG) Oct: Changes to DATIX not yet implemented yet (c) Oct: Changes to be implemented on 10 October 2017
Board Assurance Framework Risk 1.8 Risk Register ID 3058 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is an overarching risk to patient quality and safety during periods of major system change and employment of new governance systems and processes related to place based care Lead Committee/Group:
Q3 - L3 x C4 = 12 Q4 - L3 x C4 = 12 Q1 - L3 x C4 = 12 Q2 - L3 x C4 = 12
L3 x C4 = 12 Medium
High Medium Low
0 0 0
Controls Identified 1. Sustainability and Transformation Plan
All papers presented for Assurance in Quarter 3 were received positively
Page 10 of 3620 BAF Q3.pdfOverall Page 128 of 218

Board Assurance Framework Risk 1.9 Risk Register ID 3081 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to population health through the failure to fully embed public health principles within DCHS service delivery impacting on the ability to reduce inequalities in access and outcomes for our populations Lead Committee/Group:
Q3 - L4 x C4 = 16 Q4 - L4 x C4 = 16 Q1 - L4 x C4 = 16 Q2 - L4 x C4 = 16
L4 x C4 = 16 High
High Medium Low
0 0 0
Controls Identified 1. Operational Plan 2. Clinical Strategy
All papers presented for Assurance in Quarter 3 were received positively
Page 11 of 3620 BAF Q3.pdfOverall Page 129 of 218

DCHS NHS Foundation Trust Board Assurance Framework QUALITY PEOPLE - 2017-18 - Quarter 3 Risk Score Summaries
BAF No Risk Description
Target Risk
Score
Timeframe to achieve
Target Risk Score
Movement 2016/17
Q4 Risk
Score
2017/18 Q1
Risk Score
2017/18 Q2
Risk Score
2016/17 Q3
Risk Score
2.1
There is a risk of our staff not being able to provide high quality care due to national and local workforce supply shortages and the challenges of developing the workforce to have the appropriate skills and competencies to provide the future model of care resulting in poor patient outcomes
8 L2xC4 April 2018 15
L3xC5 15
L3xC5 15
L3xC5 15
L3xC5
2.2
There is a risk to patients, service-users and employees due to staff performance and behaviours not being monitored and improved resulting in an adverse impact on the provision of high quality care and organisational reputation
6 L2xC3 N/A 6
L2xC3 6
L2xC3 6
L2xC3 6
L2xC3
2.3
There is a risk that the Trust fails to develop a proactive Health and Safety culture across the organisation, resulting in the trust not achieving zero harm to staff, visitors, contractors and members of the public. NB: Following Quality People Committee in January 2017 the consequence was increased to 4; the committee agreed that if DCHS was to seriously breach health and safety legislation, leading to serious harm to a patient, visitor, or member of staff, the consequence would be high from both a financial and reputational basis. NB: A new Health & Safety Lead has been appointed with a potential start date in October 2017; therefore following discussion at Quality People Committee in September 2017 the likelihood was decreased to 2.
8 L2xC4
December 2017
12 L3xC4
12 L3xC4
8 L2xC4
8 L2xC4
Page 12 of 3620 BAF Q3.pdfOverall Page 130 of 218

BAF No Risk Description
Target Risk
Score
Timeframe to achieve
Target Risk Score
Movement 2016/17
Q4 Risk
Score
2017/18 Q1
Risk Score
2017/18 Q2
Risk Score
2016/17 Q3
Risk Score
2.4
There is a risk to organisational performance due to the high volume of organisational and health system change, which is likely to continue to be a feature of our health economy for several years NB: Following discussion at Quality People Committee in September 2017 the consequence was increased to 4, due to organisational changes currently taking place.
12 L4xC3 April 2018 12
L4xC3 12
L4xC3 16
L4xC4 16
L4xC4
2.5
There is a risk to service users, staff and DCHS’ reputation due to staff not adhering to the principles of an equal, diverse and inclusive culture, resulting in discriminatory and non-inclusive behaviours, non-compliance with Equality Act and potential legal costs
6 L2xC3 April 2018 9
L3xC3 9
L3xC3 9
L3xC3 9
L3xC3
2.6
There is a risk to the personal engagement, morale, and health and wellbeing of our staff due to the uncertain operating environment DCHS is working in NB: Following discussion at Quality People Committee in September 2017 the consequence was increased to 4, due to organisational changes currently taking place.
9 L3xL3 April 2018 12
L4xC3 12
L4xC3 16
L4xC4 16
L4xC4
Page 13 of 3620 BAF Q3.pdfOverall Page 131 of 218

QUALITY PEOPLE - Quarter 3 2017/18
Objective: To build a high performance work environment that engages, involves and supports staff to reach their full potential
Lead Committee: Quality People Committee, chaired by Barbara-Anne Walker, Non-Executive Director Lead Executive Director: Amanda Rawlings, Director of People and Organisational Effectiveness Strategic Priorities 2017/18 1. Effectiveness workforce planning and development to meet our current and future patient needs. 2. Ensuring DCHS maintains its excellent staff engagement and grows this further. 3. To build cultural competence and awareness across DCHS to ensure we deliver equity of access and outcomes for staff and service users. 4. To ensure DCHS is compliant with health and safety legislation and builds a zero harm environment. Summary of Quality People BAF Risks by Lead Executive Director: The BAF risks associated with workforce supply and retention remain the most challenging for the Trust during Quarter 3 and are the ones that are proving the most complex in terms of mitigation; these include BAF risk 2.1 - workforce supply and 2.4 - change within the healthcare system. The impact of service transformation, including the scale of the Better Care Closer to Home proposals, coupled with the staff shortages which have previously been reported, are affecting retention, particularly within nursing staff . The scale of the transformation including analysis of staff future work preferences has been mapped out and work continues at system level to manage the change and mitigate the risk. In relation to BAF risk 2.3, the new Health and Safety Manager is now in post and we have seen an improvement in reporting, which is an indicator that we are moving in the right direction in terms of health and safety culture.
Page 14 of 3620 BAF Q3.pdfOverall Page 132 of 218

All papers presented for Assurance in Quarter 3 were received positively Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales):
Board Assurance Framework Risk 2.1 Risk Register ID 2995 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk of our staff not being able to provide high quality care due to national and local workforce supply shortages and the challenges of developing the workforce to have the appropriate skills and competencies to provide the future model of care resulting in poor patient outcomes Lead Committee/Group: Workforce Planning and Development
Q3 - L3 x C5 = 15 Q4 - L3 x C5 = 15 Q1 - L3 x C5 = 15 Q2 - L3 x C5 = 15
L3 x C5 = 15 High
High Medium Low
1 11 0
Controls Identified 1. Regular reporting of training compliance to Ops Management, SWDE&EG and
QPC 2. Revised Training needs analysis aligned to Service and strategic
workforce plans 3. Attainment of required nurse staffing numbers guidance with regular reporting of
workforce requirements to SWD&EG and OWG with actions addressed by POE, as well as publication of data online as per NHS England requirements.
4. Workforce development strategy which outlines costed workforce development, aligned to the STP and reported to SWIG/LWAB, sharing our position and working collaboratively to address hard to fill posts
5. Ongoing provision of training for the future NHS workforce and engagement in national/ local initiatives to increase the supply of the future health & care workforce (e.g. RtP, nurse associate, Talent Academy)
6. Re-registration policy
7. DATIX Incidents 8. Clinical Audits (e.g. Quality Always Assessment) 9. Staff Survey 10. Triannual deep dive into profile of our workforce to understand trends
in relation to hard to recruit groups
Page 15 of 3620 BAF Q3.pdfOverall Page 133 of 218

Board Assurance Framework Risk 2.2 Risk Register ID 2996 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to patients, service-users and employees due to staff performance and behaviours not being monitored and improved resulting in an adverse impact on the provision of high quality care and organisational reputation Lead Committee/Group: Staff Partnership Committee
Q3 - L2 x C3 = 6 Q4 - L2 x C3 = 6 Q1 - L2 x C3 = 6 Q2 - L2 x C3 = 6
L2 x C3 = 6 Medium
High Medium Low
0 2 0
Controls Identified 1. Robust People Policies (e.g. Disciplinary, Performance
Attendance) 2. Outcomes and actions from result of Staff Survey and
Pulse checks 3. Resolve Staff Support service
4. Feedback and action from “Raising Concerns” app 5. Friends and Family test 6. Revalidation / Registration and monitoring process 7. Quality Always development centre 8. DATIX incidents
All papers presented for Assurance in Quarter 3 were received positively with the exception of Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Infection Prevention and Control Summary Report – Ventilation Risk and Management (CSG)
Oct: Current non-compliant areas are sexual health, Coleman Street, Revive Leg Ulcer Clinics and DTC, Ilkeston (a)
Oct: All sites are currently being reviewed, updates to be reported to future IP&C Group
Infection Prevention and Control Summary Report – Continence/Ecoli Bacteraemia Update(CSG)
Oct: Target of reducing bacteraemia by 50% not yet reached (a) Oct: Action plan to be monitored/updated at IP&C and shared with CSG via summary report
Page 16 of 3620 BAF Q3.pdfOverall Page 134 of 218

Board Assurance Framework Risk 2.3 Risk Register ID 2997 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk that the Trust fails to develop a proactive Health and Safety culture across the organisation, resulting in the trust not achieving zero harm to staff, visitors, contractors and members of the public. Lead Committee/Group: Staff Health Safety and Wellbeing Group
Q3 - L3 x C4 = 12 Q4 - L3 x C4 = 12 Q1 - L3 x C4 = 12 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 0 0
Controls Identified 1. Health and Safety Strategy
(September 2016) 2. Manager Training for Health and
Safety (April 2016) 3. Health and Safety Training for all
staff 4. Annual Health and Safety Self
Audits 5. Regular reports from Occupational
Health and Resolve on activity 6. Policies and Operating Standards
for health and safety activities. 7. Banksmen Training
All papers presented for Assurance in Quarter 3 were received positively with the exception of: Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Learning Disability Forensic Service Activity (QSC) Nov: The Transforming Care agenda will lead to a number of
highly complex individuals who present with a significant forensic history and risk profile returning to North Derbyshire (a)
Nov: Medical Director to write to the National Leadership for Policy at NHS England to highlight the change in risk
Infection Prevention and Control Summary Report – Ventilation Risk and Management (CSG)
Oct: Current non-compliant areas are sexual health, Coleman Street, Revive Leg Ulcer Clinics and DTC, Ilkeston (a)
Oct: All sites are currently being reviewed, updates to be reported to future IP&C Group
Infection Prevention and Control Summary Report – Continence/Ecoli Bacteraemia Update(CSG)
Oct: Target of reducing bacteraemia by 50% not yet reached (a)
Oct: Action plan to be monitored/updated at IP&C and shared with CSG via summary report
Page 17 of 3620 BAF Q3.pdfOverall Page 135 of 218

Board Assurance Framework Risk 2.4 Risk Register ID 2998 Risk Description Previous Quarters Risk Score Operational Risk Profile There is a risk to organisational performance due to the high volume of organisational and health system change, which is likely to continue to be a feature of our health economy for several years. Lead Committee/Group: Staff Partnership Committee
Q3 - L4 x C3 = 12 Q4 - L3 x C4 = 12 Q1 - L4 x C3 = 12 Q2 - L4 x C4 = 16
L4 x C4 = 16 High
High Medium Low
0 2 0
Controls Identified 1. Organisational Change Policy 2. Dedicated POEM support to each
organisational change 3. Check and challenge of each organisational change proposal
through the Management of Change section of SPC 4. Derbyshire-wide HR Policy Sub-Group agreement on cross –
organisational support during organisational change 5. Resolve staff support service 6. Clinical Vision Events
7. Resolve staff support service
All papers presented for Assurance in Quarter 3 were received positively with the exception of: Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Working Together Through Change – supporting managers and staff during periods of workforce change and transformation
Nov: Work in this area is still being progressed (a) Nov: Paper to be brought to a future meeting
Proposed Voluntary Redeployment Scheme (SPC) Nov: To be further developed to include a voluntary transfer request scheme to aid retention (c)
Nov: To be re-presented to the next Committee
Page 18 of 3620 BAF Q3.pdfOverall Page 136 of 218

Board Assurance Framework Risk 2.5 Risk Register ID 2999 Risk Description Previous Quarters Risk Score Operational Risk Profile There is a risk to service users, staff and DCHS’ reputation due to staff not adhering to the principles of an equal, diverse and inclusive culture, resulting in discriminatory and non-inclusive behaviours, non-compliance with Equality Act and potential legal costs Lead Committee/Group: Equality, Diversity & Inclusion Leadership Forum
Q3 - L3 x C3 = 9 Q4 - L3 x C3 = 9 Q1 - L3 x C3 = 9 Q2 - L3 x C3 = 9
L3 x C3 = 9 Medium
High Medium Low
0 1 0
Controls Identified 1. Equality and Diversity Training for staff 2. Board Equalities Action Plan 3. Corporate Equalities Action Plan 4. Directorate / Service-level Equalities Action Plans 5. Workforce Equality Data Analysis 6. Service User Equality Data Analysis 7. People Policies 8. People Strategy
All papers presented for Assurance in Quarter 3 were received positively Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales):
Page 19 of 3620 BAF Q3.pdfOverall Page 137 of 218

Board Assurance Framework Risk 2.6 Risk Register ID 3045 Risk Description Previous Quarters Risk Score Operational Risk Profile There is a risk to the personal engagement, morale, and health and wellbeing of our staff due to the uncertain operating environment DCHS is working in Lead Committee/Group:
Q3 - L4 x C3 = 12 Q4 - L4 x C3 = 12 Q1 - L4 x C3 = 12 Q2 - L4 x C4 = 16
16 L4xC4
High Medium Low
0 0 0
Controls Identified 1. Health Needs Assessment and associated Action Plan 2. Supporting and Maintaining Attendance Policy 3. Occupational Health Service 4. Resolve Staff Support Service 5. Organisational Change Policy and Guidance 6. Positive Staff Partnership relationship
All papers presented for Assurance in Quarter 2 were received positively with the exception of Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Infection Prevention and Control Summary Report – Continence/Ecoli Bacteraemia Update(CSG)
Oct: Target of reducing bacteraemia by 50% not yet reached (a)
Oct: Action plan to be monitored/updated at IP&C and shared with CSG via summary report
Working Together Through Change – supporting managers and staff during periods of workforce change and transformation
Nov: Work in this area is still being progressed (a) Nov: Paper to be brought to a future meeting
Proposed Voluntary Redeployment Scheme(SPC) Nov: To be further developed to include a voluntary transfer request scheme to aid retention (c)
Nov: To be re-presented to the next Committee
Infection Prevention and Control Summary Report – Ventilation Risk and Management (CSG)
Oct: Current non-compliant areas are sexual health, Coleman Street, Revive Leg Ulcer Clinics and DTC, Ilkeston (a)
Oct: All sites are currently being reviewed, updates to be reported to future IP&C Group
Page 20 of 3620 BAF Q3.pdfOverall Page 138 of 218

DCHS NHS Foundation Trust Board Assurance Framework QUALITY BUSINESS – 2017/18 – Quarter 3
Risk Score Summaries BAF No Risk Description
Target Risk
Score
Timeframe to achieve
Target Risk Score
Movement 2016/17
Q4 Risk
Score
2017/18 Q1
Risk Score
2017/18 Q2
Risk Score
2017/18 Q3
Risk Score
3.1
There is a risk to the organisation achieving strategic objectives due to inconsistent implementation / organisational support of the Sustainability and Transformation Plan resulting in poor outcomes for patients and poor use of resources
10 L2xC5 April 2018 15
L3xC5 15
L3xC5 15
L3xC5 15
L3xC5
3.2
There is a risk to the organisation of delivering public health contracts due to local authority price cuts resulting in poor outcomes for patients and poor use of resources NB: July 17 – Likelihood reduced to 2 as no evidence of further local authority price cuts in their commissioned contracts.
8 L2xC4 N/A 12
L3xC4 12
L3xC4 8
L2xC4 8
L2xC4
3.3 There is a risk to future sustainability due to change in national policy for out of hospital care and commissioner priorities
10 L2xC5 April 2018 15
L3xC5 15
L3xC5 15
L3xC5 15
L3xC5
3.4
There is a risk to the effective and efficient provision of DCHS services due to the impact of funding cuts within Local Authorities resulting in greater activity being directed towards health services, and flow of patients being disrupted NB: July 17 – Likelihood reduced to 2 as additional funding for social care identified through specific Council Tax rises. Derbyshire County Council have raised an additional resources from this source, and plan to invest this in 2017/18
8 L2xC4 N/A 12
L3xC4 12
L3xC4 8
L2xC4 8
L2xC4
Page 21 of 3620 BAF Q3.pdfOverall Page 139 of 218

BAF No Risk Description
Target Risk
Score
Timeframe to achieve
Target Risk Score
Movement 2016/17
Q4 Risk
Score
2017/18 Q1
Risk Score
2017/18 Q2
Risk Score
2017/18 Q3
Risk Score
3.5
There is a risk to the organisation due to capital controls leading to poor estate impacting upon patient care resulting in poor outcomes NB: Following Quality Business Committee in May 2017 the likelihood was reduced to 2 to take into consideration the increasing assurance being given to the committee.
8 L2xC4 N/A 12
L3xC4 8
L2xC4 8
L2xC4 8
L2xC4
3.6 There is a risk to the organisation regarding the efficient use of resources constrained by Health Economy Plans
9 L3xC3 April 2018 12
L3xC4 12
L3xC4 12
L3xC4 12
L3xC4
3.7 There is a risk to the financial stability of the organisation of not meeting future Sustainable Quality Improvement Programme over the next two years (2017/18 and 2018/19)
10 L2xC5 April 2018 15
L3xC5 15
L3xC5 15
L3xC5 15
L3xC5
3.8 There is a risk to the organisation that activity levels will exceed contractual activity and capacity plans, resulting in financial risk and / or increased waiting times
8 L2xC4 April 2018 12
L3xC4 12
L3xC4 12
L3xC4 12
L3xC4
3.9
There is a risk to the organisation due to non-delivery of elements of the IM&T strategy, resulting in financial risk benefits not being realised and impact on patient care NB: Following Quality Business Committee in January 2017 the likelihood was reduced to 3 to take into consideration the increasing assurance being given to the committee.
8 L2xC4 April 2018 12
L3xC4 12
L3xC4 12
L3xC4 12
L3xC4
3.10 There is a risk to the organisation due to lack of comprehensive financial data quality systems resulting in poor decisions that could affect outcomes and financial loss
8 L2xC4 N/A 8
L2xC4 8
L2xC4 8
L2xC4 8
L2xC4
3.11 There is a risk to the Trust’s resilience, due to an emergency or severe disruption, resulting in an impact on patient care, inability to meet targets, loss of revenue
10 L2xC5 N/A 10
L2xC5 10
L2xC5 10
L2xC5 10
L2xC5
Page 22 of 3620 BAF Q3.pdfOverall Page 140 of 218

BAF No Risk Description
Target Risk
Score
Timeframe to achieve
Target Risk Score
Movement 2016/17
Q4 Risk
Score
2017/18 Q1
Risk Score
2017/18 Q2
Risk Score
2017/18 Q3
Risk Score
3.12 There is a risk to the organisation, due to failure to align and influence stakeholders resulting in poor relationships that impact on patient care
8 L2xC4 April 2018 12
L3xC4 12
L3xC4 12
L3xC4 12
L3xC4
3.13 There is a risk of stranded costs through the loss of service contracts, impacting upon the financial stability of the organisation
9 L3 x C3 April 2019 New in Q2 12
L3xC4
Page 23 of 3620 BAF Q3.pdfOverall Page 141 of 218

QUALITY BUSINESS - Quarter 3 2017/18
Objective: To ensure an effective, efficient and economical organisation which promotes productive working and which offers good value to its community and commissioners
Lead Committee: Quality Business Committee, chaired by Ian Lichfield, Non-Executive Director Lead Executive Director: Chris Sands, Director of Finance, Information and Strategy Strategic Priorities 2017/18 1. To deliver a resilient current and future financial position, and be able to demonstrate value for money in the use of resources 2. To develop the Trust’s estate and infrastructure to support patient care ensuring benefits are identified, tracked and delivered 3. To explore, implement and monitor technical innovative approaches to providing care in a better way whilst demonstrating value for money 4. To develop the Trust in line with the commercial strategy to support the health economy in delivering the 5 year forward view Summary of Quality Business BAF Risks by Lead Executive Director: The Trust has 3 red risks on the Quality Business Section of the BAF. There is a risk to the organisation achieving strategic objectives due to inconsistent implementation / organisational support of the Sustainability and Transformation Plan resulting in poor outcomes for patients and poor use of resources. The Sustainability and Transformation Plan was submitted in October 2016 with the support of all health and social care partner organisations. It was planned that this would form the basis for the commissioning intentions and would be translated into contracts with providers for 2017/18 and 2018/19. This has not happened. The national guidance is that Sustainability and Transformation Partnerships will continue to be the vehicle for local strategic planning. We are working with our partners to refresh our plans and identify the priority areas for transformation. This will require both commissioners and providers to work in a different way. There are still limited tangible outputs coming out of the STP. Until we start to see a credible plan being developed, this will need to remain as a high risk on the BAF. The next quarter is crucial as system priorities are finalised, and these are converted into commissioning intentions and
Page 24 of 3620 BAF Q3.pdfOverall Page 142 of 218

contracts. A Programme Director has been appointed to start from January 2018. This will give the programme leadership over this crucial period. There is a risk to future sustainability due to change in national policy for out of hospital care and commissioner priorities. The STP has developed a plan for out of hospital care which is based upon the delivery of services at a PLACE level. Business cases have been developed to support community proactive and reactive care to reduce the reliance on traditional acute inpatient beds. However, the 2017/18 contract negotiations have not resulted in the new out of hospital teams being commissioned. The 5 Year Forward View Next Steps has been issued. This continues to promote a shift in activity from acute to out of hospital care. So the national strategy and local strategy are aligned. However, the implementation of the strategy is not progressing as fast as we would want it to and there is a lack of resources to fund the double running costs required to enact such significant service transformation. The Trust is continuing to work as part of the local Sustainability and Transformation Partnership to try and influence these changes. In the north of the county, we are starting to implement the changes around Better Care Closer to Home. One of the commitments throughout the consultation was that as the beds were reduced, community resources and “beds with care” resources would be bolstered. This is now starting to happen as the new services are introduced. In the absence in seeing consistent plans being implemented to demonstrate the shift in resources to Out of Hospital care across the county, and the improvement in outcomes for patients, this will need to remain a red risk on the BAF. The deterioration in the system finances will make this change even more difficult to implement consistently. There is a risk to the financial stability of the organisation of not meeting future Sustainable Quality Improvement Programme over the next two years (2017/18 and 2018/19). A plan for the full £7.2 million has now been identified in 2017/18. This has proven to be challenging, but a full plan is now in place. Whilst the full plan has been achieved, some of the savings will be delivered on a non-recurrent basis, and therefore we need to ensure the underlying financial position is addressed. Initial plans discussed through QBC identified an efficiency requirement of £7m for 2018/19. This is before any decommissioning plans agreed with commissioners. The efficiency requirement is challenging. Updates have been provided through QBC, and a further update is planned in January 2018. The work in developing the 2018/19 plan is being overseen through the Programme Delivery Group (PDG). Given the level of risk around the 2018/19 efficiency plan, and the general level of financial risk across the system, the risk will need to remain red on the BAF.
Page 25 of 3620 BAF Q3.pdfOverall Page 143 of 218

All papers presented for Assurance in Quarter 3 were received positively
Board Assurance Framework Risk 3.2 Risk Register ID 3005 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation of delivering public health contracts due to local authority price cuts resulting in poor outcomes for patients and poor use of resources Lead Committee/Group: Board
Q3 - L3 x C4 = 12 Q4 - L3 x C4 = 12 Q1 - L2 x C4 = 8 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 1 0
Controls Identified 1. Business Development Reporting 2. Commercial Strategy 3. Business development framework (eg investment policy / decision making tool) 4. Competitor and market analysis 5. Tender oversight and analysis All papers presented for Assurance in Quarter 3 were received positively
Board Assurance Framework Risk 3.1 Risk Register ID 3004 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation achieving strategic objectives due to inconsistent implementation / organisational support of the Sustainability and Transformation Plan resulting in poor outcomes for patients and poor use of resources Lead Committee/Group: Quality Business Committee
Q3 - L3 x C5 = 15 Q4 - L3 x C5 = 15 Q1 - L3 x C5 = 15 Q2 - L3 x C5 = 15
L3 x C5 = 15 High
High Medium Low
0 0 0
Controls Identified 1. IBP 2. LTFM 3. Annual Plan 4. Operational Plan Updates 5. Performance Reports 6. Chief Executives Report 7. Policies and Procedures 8. Transformation Update
Page 26 of 3620 BAF Q3.pdfOverall Page 144 of 218

Board Assurance Framework Risk 3.3 Risk Register ID 3006 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to future sustainability due to change in national policy for out of hospital care and commissioner priorities Lead Committee/Group: Quality Business Committee
Q3 - L3 x C5 = 15 Q4 - L3 x C5 = 15 Q1 - L3 x C5 = 15 Q2 - L3 x C5 = 15
L3 x C5 = 15 High
High Medium Low
0 1 0
Controls Identified 1. Contract management and negotiation process 2. Board and Executive colleagues meetings with
Commissioner Chief Officers /team /other contacts 3. Analysis of commissioning intentions as part of planning process
4. SQIP indicate level of commissioner support 5. Tender oversight and analysis 6. Board and Executive colleagues attendance at National Meetings/ National Groups
All papers presented for Assurance in Quarter 3 were received positively with the exception of Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Learning Disability Forensic Service Activity (QSC)
Nov: The Transforming Care agenda will lead to a number of highly complex individuals who present with a significant forensic history and risk profile returning to North Derbyshire (a)
Nov: Medical Director to write to the National Leadership for Policy at NHS England to highlight the change in risk
Risk Description Previous Quarters Risk Score Operational Risk Profile
There is a risk to the effective and efficient provision of DCHS services due to the impact of funding cuts within Local Authorities resulting in greater activity being directed towards health services, and flow of patients being disrupted Lead Committee/Group: Quality Business Committee
Q3 - L3 x C4 = 12 Q4 - L3 x C4 = 12 Q1 - L3 x C4 = 12 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 0 0
Controls Identified 1. Health and Wellbeing Board 2. Contract Management Board 3. Transformation groups 4. Better Care Fund All papers presented for Assurance in Quarter 3 were received positively
Page 27 of 3620 BAF Q3.pdfOverall Page 145 of 218

Board Assurance Framework Risk 3.5 Risk Register ID 3008 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation due to capital controls leading to poor estate impacting upon patient care resulting in poor outcomes Lead Committee/Group: Capital and Estate Programme Group
Q3 - L3 x C4 = 12 Q4 - L2 x C4 = 12 Q1 - L2 x C4 = 8 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 6 0
Controls Identified 1. Estates Planning System 2. Capital Planning System 3. Progress Reports against Estates Strategy 4. Planned Preventative Maintenance System 5. Policies and procedures 6. Facet Survey All papers presented for Assurance in Quarter 3 were received positively with the exception of Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): NHSPS/Mitie (Capital and Estate Programme Group)
Oct: There continues to be minor issues relating to planned and reactive maintenance (a)
Oct: Mitie will continue to be monitored through site audits and reviews to ensure that compliance is being met
Board Assurance Framework Risk 3.6 Risk Register ID 3009 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation regarding the efficient use of resources constrained by Health Economy Plans Lead Committee/Group: Capital and Estate Programme Group
Q3 - L3 x C4 = 12 Q4 - L3 x C4 = 12 Q1 - L3 x C4 = 12 Q2 - L3 x C4 = 12
L3 x C4 = 12 Medium
High Medium Low
0 1 0
Controls Identified 1. Capital Planning System 2. Progress Reports against Estates Strategy All papers presented for Assurance in Quarter 3 were received positively
Page 28 of 3620 BAF Q3.pdfOverall Page 146 of 218

Board Assurance Framework Risk 3.7 Risk Register ID 3010 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the financial stability of the organisation of not meeting future Sustainable Quality Improvement Programme over the next two years (2017/18 and 2018/19) Lead Committee/Group: Quality Business Committee
Q3 - L3 x C5 = 15 Q4 - L3 x C5 = 15 Q1 - L3 x C5 = 15 Q2 - L3 x C5 = 15
L3 x C5 = 15 High
High Medium Low
0 2 0
Controls Identified 1. Finance Reports 2. SQIP Reports 3. Performance Management System 4. PMO Office 5. Policies and procedures All papers presented for Assurance in Quarter 3 were received positively with the exception of Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): SQIP 2018/19 (PDG) Oct: PDG members to undertake further work with their services to
progress SQIP planning (a) Nov: Work ongoing with services regarding plan (a)
Oct: To feedback to Nov meeting Nov: Programme for 2018/19 to be drafted and brought to next PDG meeting
Board Assurance Framework Risk 3.8 Risk Register ID 3011 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation that activity levels will exceed contractual activity and capacity plans, resulting in financial risk and / or increased waiting times Lead Committee/Group: Quality Business Committee
Q3 - L3 x C4 = 12 Q4 - L3 x C4 = 12 Q1 - L3 x C4 = 12 Q2 - L3 x C4 = 12
L3 x C4 = 12 Medium
High Medium Low
0 2 0
Controls Identified 1. Finance Reports 2. Performance Reports 3. Performance Management System 4. Policies and Procedures 5. Planning Process 6. Contract Management meetings with Commissioners All papers presented for Assurance in Quarter 3 were received positively
Page 29 of 3620 BAF Q3.pdfOverall Page 147 of 218

Board Assurance Framework Risk 3.9 Risk Register ID 3012 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation due to non-delivery of elements of the IM&T strategy, resulting in financial risk benefits not being realised and impact on patient care Lead Committee/Group: Information Management & Technology Group
Q3 - L4 x C4 = 16 Q4 - L3 x C4 = 12 Q1 - L3 x C4 = 12 Q2 - L3 x C4 = 12
L3 x C4 = 12 Medium
High Medium Low
0 2 0
Controls Identified 1. IM&T Reporting 2. IM&T Strategy 3. IMT Group 4. Policies and Procedures All papers presented for Assurance in Quarter 3 were received positively with the exception of Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Apria Developments for Children’s Services (Informatics Strategy Group)
Oct: Number of issues still outstanding (a) Oct: Remedial work being undertaken, a further report to be presented to the February meeting
Board Assurance Framework Risk 3.10 Risk Register ID 3013 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation due to lack of comprehensive financial data quality systems resulting in poor decisions that could affect outcomes and financial loss Lead Committee/Group: Information Management & Technology Group
Q3 - L2 x C4 = 8 Q4 - L2 x C4 = 8 Q1 - L2 x C4 = 8 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 0 0
Controls Identified To be confirmed All papers presented for Assurance in Quarter 3 were received positively
Page 30 of 3620 BAF Q3.pdfOverall Page 148 of 218

Board Assurance Framework Risk 3.11 Risk Register ID 3014 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the Trust’s resilience, due to an emergency or severe disruption, resulting in an impact on patient care, inability to meet targets, loss of revenue Lead Committee/Group: Quality Business Committee
Q3 - L2 x C5 = 10 Q4 - L2 x C5 = 10 Q1 - L2 x C5 = 10 Q2 - L2 x C5 = 10
L2 x C5 = 10 Medium
High Medium Low
0 2 1
Controls Identified 1. Accountable Emergency Officer appointed 2. Member of the multi-agency Local Health
Resilience Partnership 3. Member of the multi-agency Local Resilience Forum
4. Framework for Responding to Industrial Action in-place
5. Quarterly reporting to the board via QBC 6. Major Incident Plan/Business Continuity Plan
7. Site Contingency Plan in-place 8. Pandemic Influenza Contingency Plan in-place 9. Internal assessment against NHS England's Core Standards for EPRR undertaken
All papers presented for Assurance in Quarter 3 were received positively
Board Assurance Framework Risk 3.12 Risk Register ID 3015 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation, due to failure to align and influence stakeholders resulting in poor relationships that impact upon patient care Lead Committee/Group: Trust Board
Q2 - L3 x C4 = 12 Q3 - L3 x C4 = 12 Q4 - L3 x C4 = 12 Q1 - L3 x C4 = 12
L3 x C4 = 12 Medium
High Medium Low
0 0 0
Controls Identified 1. Communications and marketing strategy 2. Board level lead for communications and marketing 3. Staff survey 5. Partnership strategy and governance 6. Tender oversight includes review of necessary partnership arrangements All papers presented for Assurance in Quarter 3 were received positively
Board Assurance Framework Risk 3.13 Risk Register ID Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk of stranded costs through the loss of service contracts, impacting upon the financial stability of the organisation
Lead Committee/Group:
New in Q2 Q2 - L3 x C4 = 12
L3 x C4 = 12 Medium
High Medium Low
0 0 0 Controls Identified
There were no papers presented for Assurance in Quarter 3
Page 31 of 3620 BAF Q3.pdfOverall Page 149 of 218

DCHS NHS Foundation Trust Board Assurance Framework QUALITY GOVERNANCE – 2017/18 – Quarter 3
Risk Score Summaries BAF No Risk Description
Target Risk
Score
Timeframe to achieve
Target Risk Score
Movement 2016/17
Q4 Risk
Score
2017/18 Q1
Risk Score
2017/18 Q2
Risk Score
2017/18 Q3
Risk Score
4.1 There is a risk to the organisation due to not having strong corporate governance systems in place resulting in Trust vision not being delivered
10 L2xC5 N/A 10
L2xC5 10
L2xC5 10
L2xC5 10
L2xC5
4.2 There is a risk to the organisation due to not meeting regulatory, contractual or legal obligations resulting in sanctions
10 L2xC5 N/A 10
L2xC5 10
L2xC5 10
L2xC5 10
L2xC5
4.3 There is a risk to the organisation due to not having strong risk management controls in place resulting in failure to put effective mitigation plans in place promptly
8 L2xC4 N/A 8
L2xC4 8
L2xC4 8
L2xC4 8
L2xC4
4.5 There is a risk to the organisation due to lack of comprehensive data quality systems resulting in poor decisions that could affect outcomes and financial loss
8 L2xC4 April 2018 12
L3xC4 12
L3xC4 12
L3xC4 12
L3xC4
4.6 There is a risk to the organisation of ineffective Derbyshire system wide governance arrangements which may impact on the quality of our services, workforce and business arrangements.
12 L3xC4
December 2017
16 L4xC4
16 L4xC4
16 L4xC4
16 L4xC4
Page 32 of 3620 BAF Q3.pdfOverall Page 150 of 218

QUALITY GOVERNANCE - Quarter 3 2017/18
Objective: To manage and develop a successful organisation Lead Committee: Audit and Assurance Committee, chaired by Nigel Smith, Non-Executive Director Lead Executive Director: Kirsteen Farrar, Trust Secretary Strategic Priorities 2017/18 1. To ensure control systems to manage strategic risks are operating effectively 2. To ensure the Board Assurance Framework remains a live document which fully reflects the risks and opportunities facing the Trust to deliver
our vision 3. To understand the implications of new models of care and to advise the Board as to the emerging governance issues arising and the Trust’s
response Summary of Quality Governance BAF Risks by Lead Executive Director: There are five risks on the Quality governance section of the BAF; one high risk and four medium rated risks. The high risk is in relation to system-wide governance. The Trust has been working with the main providers and commissioners of health and social care to develop the Derbyshire Sustainability and Transformation Partnership (STP). The latest version of the plan was submitted in October 2016. The STP Board is now meeting monthly, and the new Provider Alliance Group is also meeting monthly. The STP has recently appointed a new Programme Director, Vikki Taylor, and her appointed should provide some impetus to discussions. Whilst there continues to be good intentions from all parties to take forward measures to address the STP priorities, this has not yet been converted into tangible actions. With regard to Better Care Closer to Home; the Implementation Board have accepted a governance structure and recommended it for approval at the two CCG Governing Bodies. Additionally a Senior Responsible Officer, Helen Dillistone, has been appointed for the programme by the CCGs. DCHS has been leading on the financial analysis of the programme and this work has demonstrated that to date the changes are within the predicted financial envelope of the business case.
Page 33 of 3620 BAF Q3.pdfOverall Page 151 of 218

All papers presented for Assurance in Quarter 3 were received positively
Board Assurance Framework Risk 4.2 Risk Register ID 3001 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation due to not meeting regulatory, contractual or legal obligations resulting in sanctions Lead Committee/Group: Audit & Assurance Committee
Q3 - L2 x C5 = 10 Q4 - L2 x C5 = 10 Q1 - L2 x C5 = 10 Q2 - L2 x C5 = 10
L2 x C5 = 10 Medium
High Medium Low
0 2 0
Controls Identified
1. CQC Compliance Reporting 2. NHS Improvement Self-Certification 3. Performance Reporting All papers presented for Assurance in Quarter 3 were received positively with the exception of: Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Information Governance (IG) Group Summary Report (QSC) Nov: Limited assurance was taken on issue of
preparedness in respect of General Data Protection Regulations (c)
Nov: A report from the IGG on the issue of GDPR to be submitted to the next QSC and AAC
Records Management Group Summary Report (QSC) Nov: Ability to sustain progress which has been made by the group (a)
Nov: An options paper to be presented to Exec Team early in 2018
Infection Prevention and Control Summary Report – Continence/E coli bacteraemia Update(CSG)
Oct: Target of reducing bacteraemia by 50% not yet reached (a)
Oct: Action plan to be monitored/updated at IP&C and shared with CSG via summary report
Learning Disability Forensic Service Activity Nov: Risk raised to 16 in respect of patients in the north of the county (a)
Nov: Medical Director to write to the National Leadership for Policy at NHS England to highlight the change in risk
Infection Prevention and Control Summary Report – Ventilation Risk and Management (CSG)
Oct: Current non-compliant areas are sexual health, Coleman Street, Revive Leg Ulcer Clinics and DTC, Ilkeston (a)
Oct: All sites are currently being reviewed, updates to be reported to future IP&C Group
Board Assurance Framework Risk 4.1 Risk Register ID 3000 Risk Description Previous
Quarters Risk Score Operational Risk Profile
There is a risk to the organisation due to not having strong corporate governance systems in place resulting in Trust vision not being delivered Lead Committee/Group: Audit & Assurance Committee
Q3 - L2 x C5 = 10 Q4 - L2 x C5 = 10 Q1 - L2 x C5 = 10 Q2 - L2 x C5 = 10
L2 x C5 = 10 Medium
High Medium Low
0 1 0
Controls Identified 1. Constitution and Procedures 2. Board Committee Reporting 3. Quality Governance reporting 4. Internal Audit Reports 5. Counter Fraud Reports 6. External Audit Reports 7. Scheme of Delegation 8. Self-Certification Reporting 9. Board Assurance Framework 10. Clinical Audit Programme 11. Annual Governance Statement
Page 34 of 3620 BAF Q3.pdfOverall Page 152 of 218

Board Assurance Framework Risk 4.3 Risk Register ID 3002 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation due to not having strong risk management controls in place resulting in failure to put effective mitigation plans in place promptly Lead Committee/Group: Quality Service Committee Risk Register Review Meeting
Q3 - L2 x C4 = 8 Q4 - L2 x C4 = 8 Q1 - L2 x C4 = 8 Q2 - L2 x C4 = 8
L2 x C4 = 8 Medium
High Medium Low
0 0 0
Controls Identified 1. Risk Management Strategy 2. Board Assurance Framework 3. Risk Register 4. Risk Management Policy
5. DATIX Risk Management System 6. Annual Governance Statement All papers presented for Assurance in Quarter 3 were received positively with the exception of: Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Infection Prevention and Control Summary Report – Continence/E coli bacteraemia Update(CSG)
Oct: Target of reducing bacteraemia by 50% not yet reached (a)
Oct: Action plan to be monitored/updated at IP&C and shared with CSG via summary report
Infection Prevention and Control Summary Report – Ventilation Risk and Management (CSG)
Oct: Current non-compliant areas are sexual health, Coleman Street, Revive Leg Ulcer Clinics and DTC, Ilkeston (a)
Oct: All sites are currently being reviewed, updates to be reported to future IP&C Group
Board Assurance Framework Risk 4.5 (previously 3.10) Risk Register ID 3059 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation due to lack of comprehensive data quality systems resulting in poor decisions that could affect outcomes and financial loss Lead Committee/Group: Information Management & Technology Group
Q3 - L3 x C4 = 12 Q4 - L3 x C4 = 12 Q1 - L3 x C4 = 12 Q2 - L3 x C4 = 12
L3 x C4 = 12 Medium
High Medium Low
3 0 4
Controls Identified 1. Performance Reporting - Data Quality issues 2. Data Quality Kitemark 3. Policies and procedures 4. IM&T Strategy 5. IMT Group All papers presented for Assurance in Quarter 3 were received positively
Page 35 of 3620 BAF Q3.pdfOverall Page 153 of 218

Board Assurance Framework Risk 4.6 Risk Register ID 3080 Risk Description Previous Quarters Risk Score Operational Risk
Profile There is a risk to the organisation of ineffective Derbyshire system wide governance arrangements which may impact on the quality of our services, workforce and business arrangements. Lead Committee/Group:
Q3 - L4 x C4 = 16 Q4 - L4 x C4 = 16 Q1 - L4 x C4 = 16 Q2 - L4 x C4 = 16
L4 x C4 = 16 High
High Medium Low
0 0 0
Controls Identified 1. STP Chiefs Meeting 2. STP Multi-agency working (engine room) All papers presented for Assurance in Quarter 3 were received positively with the exception of: Name of Paper Identified Gaps in Control (c) /Assurance (a): Action planned to address (and timescales): Infection Prevention and Control Summary Report – Continence/E coli bacteraemia Update(CSG)
Oct: Target of reducing bacteraemia by 50% not yet reached (a)
Oct: Action plan to be monitored/updated at IP&C and shared with CSG via summary report
Infection Prevention and Control Summary Report – Ventilation Risk and Management (CSG)
Oct: Current non-compliant areas are sexual health, Coleman Street, Revive Leg Ulcer Clinics and DTC, Ilkeston (a)
Oct: All sites are currently being reviewed, updates to be reported to future IP&C Group
Page 36 of 3620 BAF Q3.pdfOverall Page 154 of 218

Summary Report from Quality Service Committee Report To: Board
Date: Thursday 25th January 2018
Name of Reporting Committee / Group: Quality Service Committee
Date of Meeting: Tuesday 16th January 2018
Presenter: James Reilly, Non-Executive Director
Author: Andrea Graham, Corporate Governance Manager
This paper is for Assurance
Key Issues discussed at meeting:
Board Assurance Framework Reference and Level of Assurance Agreed
3/18 Patient Story The Story discussed the Dental Treatment of a 22 year old male with obsessive compulsive disorder, body dysmorphia, agoraphobia and an extremely low BMI which resulted in him being housebound. On examination he had multiple broken teeth and decay in several others which would require multiple extractions. The story showed a good example of patient centered care and close working with other health professionals in challenging circumstances. The Committee agreed it was a g ood example of the complexity of Patients being treated in the Community The story was powerful and a good example of the 6Cs and suggested the story be s hared with Commissioners to illustrate the challenges faced in the Community The Committee congratulated the team on their hard work in managing the patient
Paper for Information
8/18 Board Assurance Framework Quarterly Review The Commtitee discussed 1.5 (Clinical Governance Initiatives) The Committee agreed this is an area where most papers receive significant assurance and there is some external validation of the levels of assurance. The Committee agreed the score should be reduced from L2xC4 to L1xC4 based on the levels of assurance given over the year.
Significant Assurance 4.3
Page 1 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 155 of 218

1.6 (Quality Improvement and Assurance Framework) The Committee agreed the framework is consistently employed and controls have been consistently applied. The Committee agreed there is good evidence that staff understand the framework. The Committee agreed the score should be reduced from L2xC5 to L1xC5 1.9 (Public Health Principles) The Committee agreed the Health Coaching Initiative was a goo d example of work particularly in deprived areas. With a good spread of actions which are making a pos itive impact,he Committee agreed the score should be reduced from L4xC4 to L3xC4 9/18 Quality Performance Report/Dashboard JH presented highlights against the range of quality indicators across DCHS including
• Age profile of Patients with a Pressure Ulcer which showed an increasingly elderly population particularly in Derby City
• Pressure Ulcer Improvement plans are in place and updates on their progress by locality
• Pressure Ulcers continued to fall in November. December data was not available at the time of the report. There were no avoidable Pressure Ulcers in November 2017.
• 10 Patients and 12 staff presented with Diarrhoea and/or vomiting on H opewell Ward during December. Novovirus was not confirmed
Signficant Assurance 1.1, 1.2, 1.3, 1.4, 1.5, 1.9
12/18 CQUIN Quarterly Report The Committee discussed the CQUINS which were unlikely to be achieved which were in respect of:
• Flu vaccine uptake (currently at 60%), • Safe and proactive discharge of patients, which is dependent on
whole system performance • Staff health and wellbeing including staff survey results which
have not progressed in some areas
Limited Assurance in respect of the areas which were not likely to be achieved Significant Assurance from the process 1.4, 1.9
15/18 Preparedness for the implementation of General Data Protection Regulations The Committee received an update on the Trust’s preparedness for the introduction of the new General Data Protection Regulations (GDPR) in May 2018 The Commtitee were assured the trust is likely to be compliant with the new regulations.
Significant Assurance 4.2
Page 2 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 156 of 218

10/18 Corporate Risk Management Report The Committee reviewed and asked for adjustments where appropriate on the Corporate risks with a risk rating of 10 and above. The Committee noted there have been no overdue risks on the register in the last 12 months which the Committee agreed was exceptional
Significant Assurance 4.3
11/18 Quality Assurance and Compliance Report The Commtitee discussed; • Actions to close the CQC action plan which are progressing • Ratings and t hemes from unannounced triangulation visit in
December 2017 • Governors’ development sessions • Re-energising of the Communication campaign
Significant Assurance 1.5, 2.5
29/18 Mortality Review Group The Committee received
• Summary Report • Mortality Report • Terms of Reference • Learning from Deaths Policy
The Committee discussed the Mortality Report, the format for which is still developing and suggested modifications to help its evolution into a more user friendly and transparent document. It was noted that actioning the process fully has been delayed by capacity constraints, now resolved by recruitment of extra staff..The latest Mortality Report is attached
Significant Assurance 1.3, 1.4, 1.5, 1.7, 3.12, 4.2
22/18 Patient Outcomes and Clinical Effectiveness The Committee discussed
• The Clinical outcomes Pilot taking place in the Chapel and Ripley Community Therapy Teams
• The development of a central clinical outcomes database • Some examples of reporting including the Derby Outcome
Measure – 95% of patients on the rehab wards, showed an improvement in their score.
The Committee agreed it was good to see a focus around outcomes rather than processes and that it was important to link to the patient expectations. The Committee were assured that the Big 9 target will be met.
Significant Assurance 1.7
Page 3 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 157 of 218

24/18 Moving forward with Research and Innovation and the next steps The Committee reviewed the updated Research and Innovation Strategy. The Committee discussed
• Strengthening collaborative partnerships with universities • Developing clinical leadership and broadening participation
across the workforce: embedding research awareness, skills and confidence across disciplines and roles.
• Raising the profile of research to commissioners as part of DCHS’ Quality Governance. Building closer links between research and audit, outcomes and evidence based practice under the umbrella of Clinical Effectiveness
Significant Assurance 1.5, 2.1, 3.2
23/18 Clinical Effectiveness Group Summary Report The Committee noted the request for formal approval from the Board via QSC to implement the ReSPECT form within DCHS and t he request for SLT Staff story to be tabled at a future Board with support from the Medical Director
Significant Assurance 1.2.1.3 1.4.1.5 1.6 1.7 2.2
33/18 QSC Annual Review The Committee received the Annual Report of the work of the Committee for the period November 2016 to December 2017. The Commtitee agreed the Annual Report could be presented to the Board
Significant Assurance 1.1 – 1.9
13/18 Divisional Operational Quality Report
Significant Assurance 1.5, 4.1
14/18 Quarterly Legal Issues Report
Signficant Assurance 1.6, 4.1, 4.2
17/18 Quality Always Group – Summary Report
Significant Assurance 1.3, 1,5, 2.2, 1.7, 3.9, 3.10
16/18 Information Governance Group Summary Report including Terms of Reference
Significant Assurance 4.2
19/18 Patient Experience and Engagement Group Summary Report
Signficant Assurance 1.4
20/18 Equality Diversity Inclusion and Leadership Group Annual Review
Significant Assurance 1.4 But Limited Assurance as no reporting on Healthcare for All
Page 4 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 158 of 218

25/18 Research and Innovation Group Summary Report
Significant Assurance 1.5
27/18 Clinical Safety Group Summary Report
Significant Assurance 1.1, 1.2, 1.3, 1.4, 1.5, 1.6, 2.2, 4.3, 4.6
28/18 Safeguarding Governance Group Summary Report
Significant Assurance 1.3, 1.5, 1.7, 2.5, 3.4, 3.12, 4.3
34/18 Forward Agenda
Paper for Decision
31/18 Board Assurance Framework Paper for Decision
Policies Approved Learning from Deaths Policy Complaints and Concerns Policy Policy Development Framework Issues to be escalated to Board or a Committee
Page 5 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 159 of 218

QUALITY SERVICE COMMITTEE Document Title: Quality Service Annual Report
Presenter/Title: Chris Bentley, QSC Chair and Non-Executive Director Contents of Paper were previously discussed by:
The QSC Terms of Reference were last reviewed, and approved, at the May 2017 QSC meeting
Author/Title: Carolyn White, Director of Quality and Chief Nurse Andrea Graham, Corporate Governance Manager
Contact Email and Telephone Number: Andrea Graham 01773 525022
Date of Meeting: 16th January 2018 Agenda Item No:
No of pages inc. this one:
Has an Equality Impact Assessment been undertaken Yes No x
Document is for: (more than one box can be ticked) Information Decision x Assurance x
Purpose of Paper
This is the Annual Report of the Quality Service Committee and covers the work from November 2016 to December 2017 The report demonstrates that the Committee has fulfilled its terms of reference and significantly contributed to shaping, influencing and producing overall assurance in relation to the quality of our services QSC monitored the controls and provided assurance to the Board regarding the strategic risks and controls in the Board Assurance Framework (BAF) with respect to Quality Service
Recommendations
The Committee is asked to Approve the Annual Report. Once approved, the Annual Report will be presented to the Board
Board Assurance Framework Risk Reference
All references in the Quality Service section of the Board Assurance Framework; 1.1 to 1.9
Financial Impact
There are costs incurred for running the Committee. These are the costs of attendance, cost of producing and circulating the papers and cost of ensuring Committee members are up to date with the latest developments in Governance. The Committee has its functions set out in its terms of reference and its officers have endeavored to manage the Committee in an effective and efficient manner
Page 6 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 160 of 218

Further Information and Appendices
Quality Service Committee Annual Report 2016/2017
• SCOPE The Annual Report of the Quality Service Committee (QSC) covers the work of the Committee for the period November 2016 to December 2017
• INTRODUCTION The Board remain committed to the continued development of good governance principles that reflect the changing needs of the NHS, recognise the developments in broader corporate governance and ensure that the organisation remains relevant and responsive in this changing environment
• ROLE OF THE QUALITY SERVICE COMMITTEE As one of DCHS’ key Board sub-committees, the role of the Quality Service Committee is central to the good governance of the Trust. During the reporting period the Committee met on a Bi-monthly basis and reported directly to the Board. The Membership of the Committee consists of two Non-Executive Directors appointed by the Board, including the Chair of the Committee and;
• Chief Nurse /Director of Quality • Chief Operating Officer • Medical Director • Deputy Director of People and Organisational Effectiveness • Chair – Safeguarding Governance Group (Deputy Chief Nurse) • Chair of Clinical Safety Group • Chair – Patient Experience and Engagement Group (Assistant Director of Quality and
Professional Lead for Allied Health Professions) • Chair – Clinical Effectiveness Group (Head of Quality Governance) • Chair – Equality, Diversity and Inclusion Group (Deputy Director of People and
Organisational Effectiveness) • Associate Director of Corporate Governance/Trust Secretary • Head of Operational Quality
Page 7 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 161 of 218

Membership (Period November 2016 to December 2017): Chris Bentley Chair – Non Executive Director November 2016 –
December 2017 John Coyne Non-Executive Director Until November 2016
James Reilly Non-Executive Director From March 2017
Sarah Banks Head of Quality Governance November 2016 – December 2017
Kirsteen Farrar Associate Director of Corporate Governance/ Trust Secretary
November 2016 – December 2017
Mary Heritage Assistant Director of Quality and Professional Lead for AHPs
November 2016 – December 2017
Jo Hunter Deputy Chief Nurse November 2016 – December 2017
William Jones Chief Operating Officer
November 2016 – December 2017
Rick Meredith Medical Director
November 2016 – December 2017
Amanda Rawlings
Director of People and Organisational Effectiveness
November 2016 – December 2017
Jen Guiver Deputy Director of People and Organisational Effectiveness
November 2016 –August 2017
Beverley Smith Deputy Director of People and Organisational Effectiveness
September 2017 – December 2017
Carolyn White
Chief Nurse/Director of Quality
November 2016 – December 2017
Julie Wheeldon Interim Assistant Director ICBS South July 2017 – December 2017
The Chief Executive, representatives from the Frontline Care Council and the Staff Partnership Forum also attended the meetings on a regular basis. Other individuals were invited to attend as named deputies or to offer specific assurance on agenda items QSC delegated responsibility for specific aspects of performance and management to a number of subgroups. These included;
• Clinical Safety Group • Clinical Effectiveness Group • Patient Experience and Engagement Group • Equality, Diversity and Inclusion Leadership Forum • Information Governance Group • Safeguarding Governance Group • Records Management Group • Research and Innovation Group
Page 8 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 162 of 218

• ATTENDANCE
For QSC, a quorum is a minimum of one Non-Executive Director, one Executive Director and two other Committee members, one of whom shall have a c linical background. All meetings were quorate. Attendees at the meeting are listed below
QSC Attendance record Key
Not a Member
√ Attended
Apologies
Nov 16
Jan 17
Mar 17
May 17
Jul 17
Sep 17
Nov 17
Chris Bentley
Chair – Non Executive Director
√ √ √ √ √ √
John Coyne Non Executive Director √
James Reilly
Non Executive Director
√ √ √ √
Sarah Banks
Head of Quality Governance
√ √ √ √ √ √ √
Kirsteen Farrar
Associate Director of Corporate Governance/ Trust Secretary
√ √ √ √ √ √ √
Mary Heritage
Assistant Director of Quality and Prof Lead for AHPs
√ √ √ √ √ √
Jo Hunter Deputy Chief Nurse, Chair of Safeguarding Gov Group
√ √ √ √ √ √ √
William Jones
Chief Operating Officer √ √ √ √
Carolyn White
Chief Nurse, Director of Quality
√ √ √ √ √ √
Page 9 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 163 of 218

Rick Meredith
Medical Director √ √ √ √ √
Julie Wheeldon
Head of Operational Quality
√ √
Jen Guiver Deputy Director of People and Organisational Effectiveness
√ √
Beverley Smith
Deputy Director of People and Organisational Effectiveness
√
Nigel Smith Non-Executive Director
√
Prem Singh DCHS Chair
√
Attendance at Risk Review meetings:
QSC Risk Review Meetings – Attendance record
Key
Not a Member
√ Attended Apologies
Nov-16 Feb-17 Aug-17 Nov 17 Chris Bentley
Chair – Non Executive Director √ √ √ √
Sarah Banks Head of Quality Governance √ √ √
Kirsteen Farrar
Associate Director of Corporate Governance/ Trust Secretary
√ √ √
Jo Hunter Deputy Chief Nurse √
√ √
Mary Heritage
Assistant Director of Quality and Professional Lead for AHPs
√
William Jones
Chief Operating Officer √ √
√
Rick Meredith
Medical Director √ √ √ √
Carolyn White
Chief Nurse/Director of Quality
√ √
√
Page 10 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 164 of 218

Julie Wheeldon
Head of Operational Quality
√
• REVIEW OF BUSINESS 2016/2017
o DCHS Quality Assurance and Improvement Framework During 2016/17 the Quality Service Committee has Overseen the review of Quality assurance and improvement framework and further developed quality governance processes to provide assurance to the board that DCHS has a high quality and sustainable service which echo’s the values and aspirations of the community. This has been supported by designated sub groups and has encompassed the three domains of quality service delivery; Safety, Clinical Effectiveness and Patient Experience The established quality priorities are;
• Keeping Patients safe in our care • To get the basis right • Put our patient at the centre of care delivery
The work of the Committee has included receiving assurance of progress against work supporting quality improvement and assurance QSC regularly considers its work in the context of whole system working across the County, including models of integrated care and also the expanding DCHS portfolio of services including primary care and services won through Tender; Examples of where QSC monitored the delivery of services during change are;
• Rollout of SystemOne • Integrated sexual health updates • Introduction of new interpreter services • Patient stories • Strategic shift updates
The Committee has continued to review the work of the supporting IT systems including the DCHS quality dashboard. The Committee has monitored the important challenge of ensuring IT properly reflects clinical need. The Committee has driven forward the Equality, Diversity and Inclusion Strategy and is working jointly with QPC to review the Equalities agenda and ensure our services meet the needs of all service users. 5.2 Compliance against regulatory requirements and external scrutiny QSC has overseen the Trust Quality Performance as part of its regulatory requirements. DCHS is currently rated GOOD overall with elements of OUTSTANDING following the CQC inspection in September 2016. In year all three DCHS GP services were rated as GOOD In line with the trusts commitment to continue to strengthen its clinical governance arrangements QSC has;
Page 11 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 165 of 218

• Regularly reviewed the Trusts arrangements for assessing compliance with the Care Quality Commissions (CQC) standards and where the Trust is failing to meet these essential standards has improved and overseen the action plans for remedial action
• Scrutinised CQC reports CQC reports following inspection and ensured development of robust action plans following CQC inspection
• Received updates on the progress of action plans In place following CQC Inspections to ensure timely progress
• Received regular Quality Assurance and Compliance Reports which provided updates on insight visits, Quality Always and other forms of triangulation
• Acted upon and implemented learning from cases referred to the Coroner • Ensured Compliance with Health Acts, Infection Prevention and Control, Deprivation of
Liberty Safeguards, End of Life, Safeguarding, public/patient engagement. During the year we have received assurance where any actions are required to strengthen compliance.
• The Committee reviewed the Independent Assurance provided from reports including 360 Assurance Integrated Sexual Health Service 360 Assurance OPMH falls and Improvement plan
5.3 Performance Framework A comprehensive framework has been developed to ensure that reporting to QSC incorporates key quality performance areas. This incorporates the quality assurance requirements of our commissioners and regulators QSC have provided assurance to the board incorporating areas of patient safety, experience and effectiveness of care. During the year QSC has commissioned additional “Deep Dive” reports into areas including;
• Leg Ulcers • Learning from death including end of life strategy • Derby City Services Update – embedding new governance procedures and operational
arrangements • Equality, Diversity and inclusion Strategy
QSC also sought assurance in relation to areas performing below expectations which have included;
• Community falls • Pressure Ulcers • Integrated community service waiting times • Learning Disability Forensic Service • Ligature Management • Non-Medical Prescribing
Performance reports in year have also been provided for a range of issues including;
• Harm free care • Safety Thermometer Performance
We have also overseen the development of the Annual Quality Report for 2016/2017
Page 12 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 166 of 218

5.4 Controls and Assurance During the year QSC has overseen the quality service controls and assurance processes. We have identified areas where there have been gaps and any subsequent improvements required Oversight has been maintained at each meeting in relation to risk management and assurance provided to the Board. A QSC Risk Review meeting was held five times in the reporting period and these meetings focused on the whole risk register and areas where further information, assurance, or action have been identified. The risk review meetings have supported the development of a robust system to manage and challenge risks In addition the Committee receives a Divisional Governance Report at every meeting that provided assurance and identified any areas for review The Board Assurance Framework was reviewed on a quarterly basis and assurance provided to the Board. The Committee reviewed new risks, challenged the existing risks and scores and identified any gaps in controls or assurance. At each meeting consideration has been given to the assurance provided by papers against the Board Assurance Framework QSC oversees the work of all the sub groups, receiving regular reports, assurance and annual reports. Over the year the committee has seen a high number of Significant Assurances received from sub group. QSC noted any areas from the sub groups where Limited Assurance has been given and ensures they are monitored and progressed 5.5 Effectiveness of care QSC monitors clinical effectiveness through the work of the clinical effectiveness group. During the year QSC monitored delivery of the clinical audit plan. The Committee monitors the work of the clinical effectiveness group and in particular clinical audit. Importantly during the year QSC has monitored remedial action plans for any services deemed to be failing to meet acceptable care standards. Detailed reports on progress have provided assurance that adequate actions have been taken to ensure provision of good quality care to patients at all times In year the research strategy was considered by the Committee and following recent changes to staffing will be further reviewed to investigate other avenues of research and possibilities for collaboration with other Trusts/Universities 5.6 Safety QSC monitors patient safety through the work of the Clinical Safety Group which provides assurance on the systems and processes in place. The group reports to QSC at every meeting and has provided QSC with overall assurance on the safety management systems and processes in place, to meet statutory, mandatory, legislative and best practice requirements for patient safety. The Clinical Safety Group is chaired by the Deputy Chief Nurse and is accountable to QSC.
Page 13 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 167 of 218

The Clinical Safety Group oversees and delegates responsibility for specific areas of safety performance and assurance to the operational sub groups, statutory reporting committees and across service delivery. An Annual Review of the work of this Committee was undertaken and presented to the Committee in July 2017 QSC has a regular performance report that has included assurance reports regarding in respect of harm free care including;
• Safety Thermometer performance • Falls • Catheter Associated Urinary Tract Infections • Medication incidents • Infection, Prevention and control • Never Events
QSC held detailed discussion at every meeting regarding the progress of the Pressure Ulcer Improvement plan and considered strategies including
• Reinstatement of Pressure Ulcer Improvement Groups • The development of a deprivation and wound prevalence map • The use of Smart Phones by community teams to photograph wounds and enable triage • Chronic wound support visits
5.7 Risk Management During the year QSC has continued to drive improvements in risk reporting. The risk report provides information regarding Strategic Executive Information System Incidents (STEIS), Central Alerting System (CAS alerts) and the risk register. The risk register has been reviewed and dynamically managed during the reporting period with continued improvements in reporting time and a reduction in overall risks. QSC review all low and medium risks on the risk register on a tri-annual basis to identify any key themes and check on how risks are moderated 5.8 Information Governance During the year QSC monitored compliance with Information Governance requirements and performance against the Information Governance Toolkit. DCHS submitted its IG Toolkit on 31st March 2017 with all requirements scoring at least level 2 and therefore achieving a ‘satisfactory’ rating overall. QSC delegated responsibilities to the Information Governance (IG) Group which is chaired by the Head of IM&T and attended by the medical director and Caldicott Guardian (Rick Meredith). The IG Group has responsibility for developing and leading on DCHS’ Information Governance Strategy, Management Framework and work programme. This includes ensuring that DCHS meets its annual compliance on the information governance toolkit, has required policies and procedures in place, and that all staff are trained in information governance every year. Where there have been omissions in information governance action has been taken to investigate and protect against future risks
Page 14 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 168 of 218

The Records Management Group provides assurance to QSC that DCHS complies with national guidance, Trust policy and legislation on records management. QSC has delegated responsibility for the development, implementation and monitoring of standard for records management to the record management group 5.9 Patient Experience QSC delegated responsibility for specific aspects of performance and management to the Patient Experience and Engagement Group (PEEG) which leads and monitors the development of patient experiences across DCHS to ensure that there is a consistent, positive approach that is patient centered. The group provides assurance to QSC that DCHS Services put patients ‘in the heart of everything we do’ and that patient and public engagement and involvement are inherent parts of service design, delivery and improvement. QSC received reports at every meeting on the national Friends and Family test. This has provided regular assurance that the majority of patients asked this question would recommend DCHS services to Friends and Family Patient stories were a regular feature at QSC meetings and brought the patients voice into the meeting room. The Committee received patient stories in the following areas;
• Breastfeeding support • Enhanced Community Service • Community based physiotherapy • The Impact on a family of increasing frailty of older relatives • Rehabilitation • Pressure Ulcer Management • Blood transfusions
The stories provided proved to be an important source of learning for Committee members and the wider organisation. In the year QSC reviewed a number of Patient Experience Reports;
• Patient Experience Annual Report • PEEG Summary reports and Annual review • Summary reports from lessons learnt panel • Complaints Annual Report • General Practice; Patient Experience Improvement plan
The Committee also reviewed regular reports regarding claims and Coroners inquests The Committee also reviewed Summary Reports from the Equality Diversity and Inclusion Leadership Forum 5.10 Policy Approval During the year the Committee considered and approved the following policies;
• Claims Handling Policy • Advanced Decisions Policy • Mental Health Act Policy
Page 15 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 169 of 218

• Records Management Policy • Mental Health Act Policy
5.11 Forward Planning The Committee will continue to ensure strong governance arrangements are maintained, and enhanced in 2018/19. In addition to the routine work the Committee undertakes each year, the focus for the next 12 month period will be in the following areas:
• Chronic wound management • Well led preparation for CQC inspection • Medicines management • Management of medical equipment
5.12 Other matters
• Terms of reference The Committee reviewed its Terms of Reference in November 2016 and May 2017
• Annual Report to the Committee This Annual Report summarises the work of the Committee for the period November 2016 to December 2017 6. THE COMMITTEE QSC reported formally to DCHS Board and provided assurance to both the Board and the Audit and Assurance Committee. The Chair of QSC prepared a Summary Report after each meeting that provided an overview of the meeting and identified any issues or areas of risk that the DCHS Board or other Committee needed to action/note. Through the Annual Report, it can be demonstrated the added value that the Committee brings to the governance of the organisation. It is the Committees view that this added value is delivered in an efficient manner. QSC reflects on its own performance by ensuring that members self-assess their performance at the end of each meeting. In addition continuity of events and cross referencing of important issues to and from other key Committees are also considered at each meeting. The Committee made and received referrals from the Board, Mental Health Act Committee, Quality People and Quality Business Committees. 7. CONCLUSION In summary, the Trust continues to develop and improve systems and processes for assurance. QSC has an important wide ranging set of responsibilities. To fulfil these responsibilities, the Committee is constantly reviewing how it undertakes its work, and its forward agenda. It has worked closely with the Quality Business and Quality People Committees along with the Audit and Assurance Committee to ensure comprehensive execution of respective responsibilities and to ensure that all Committees fulfil their roles effectively and efficiently
Page 16 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 170 of 218

This report demonstrates that the Committee has fulfilled its Terms of Reference and significantly contributed to improving internal control and assurance processes within the Trust.
Monitoring Information Brief Summary
What are the Governor Involvement implications?
At each meeting the Committee assesses the need for our governors to be briefed on issues discussed. Actions are then allocated to an appropriate member to brief or involve Governors
What are the Equality and Diversity implications?
Each paper is scrutinised in terms of its equality, diversity and inclusion implications when it is presented to the Committee. There are no direct Equality, diversity and I nclusion implications to this report
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
There are no direct Patient, Public or Stakeholder Involvement Implications to this report
Risk Register
Is the issue on the current Risk Register?
No If yes, what is the Risk Number?
Does this update recommend a change in the current risk score? (If so, please provide your rationale below)
N/A
Page 17 of 1721 QSC Summary Report inc Annual Report.pdfOverall Page 171 of 218

Overall Page 172 of 218

1
Quality Service Committee Document Title: Mortality Review Update
Presenter/Title: Bola Owolabi - Deputy Medical DirectorContents of Paper were previously discussed by: Mortality Review Group
Author/Title: Bola Owolabi - Deputy Medical Director
Contact Email and Telephone Number: [email protected]/07886499135
Date of Meeting: 16 January 2018 AgendaItem No: 29/18
No of pagesinc. this one: 32
Has an Equality Impact Assessment been undertaken Yes N/A NoDocument is for:(more than one box can be ticked) Information x Decision x Assurance x
Purpose of Paper
To provide QSC with an update on progress with respect to implementation of the of the newly established Mortality Review process in DCHS
Present the revised Terms of Reference of the Mortality Review Group (MRG) and the updated Learning from Deaths policy.
Recommendations
That QSC reviews the revised Terms of Reference of the Mortality Review Group and determine whether these can be approved.
That QSC reviews the updated DCHS Learning from Deaths policy and determine whether this can be approved.
That QSC decides whether the proposed reporting schedule meets the requirements of the Committee.
QSC to note the approval of additional funding requested from the Executive Team in support of the DCHS Mortality Review Group as well as the new mortality review process and learning from deaths policy.
Board Assurance Framework Risk Reference
1.3 There is a risk to the provision of safe, effective care due to a lack of consistent clinical leadership and expertise
1.4 There is a risk that DCHS does not provide patient centered care due to a lack of engagement and involvement of service users and stakeholders
1.5 There is a risk that our Clinical Governance initiatives do not deliver the outcomes necessary to support our strategy for high quality care
1.7 There is a risk to the provision of effective care due to a failure to learn and share lessons and implement change resulting from audit and feedback
3.12 There is a risk to the organisation, due to failure to align and influence stakeholders resulting in poor relationships that impact on patient care
Page 1 of 3221 Mortality Review Update.docxOverall Page 173 of 218

2
4.2 There is a risk to the organisation due to not meeting regulatory, contractual or legal obligations resulting in sanctions.
Financial Impact
The recruitment of additional case note reviewer capacity and administrative support for the mortality review process/Mortality Review Group represents additional investment.
DCHS Contract now includes the following clauses:
“With effect from 1 January 2018, Service Condition 3 is varied to include the additional provision below:
3.4The Provider must:
3.4.1 implement policies and procedures for reviewing deaths of Service Users whilst under the Provider’s care and for engaging with bereaved families and Carers; and
3.4.2 Where it is an NHS Trust or an NHS Foundation Trust, comply with National Guidance on Learning from Deaths where applicable.
and the definitions in the General Conditions are varied to include the following additional definition:
National Guidance on Learning from Deaths guidance published by the National Quality Board to help standardise and improve the way acute, mental health and community NHS Trusts and Foundation Trusts identify, report, review, investigate and learn from deaths, and engage with bereaved families and carers, available at https://www.england.nhs.uk/publication/national-guidance-on-learning-from-deaths/”
Further Information and Appendices
Learning from Deaths policy and MRG Terms of Reference (ToR)
The Learning from Deaths policy and revised Terms of Reference of the Mortality Review Group were presented at the September QSC. In response to feedback received at the meeting, the policy has been extensively reviewed and updated with significant contributions from the Quality Directorate and members of the Mortality Review Group. Particular acknowledgment of the Deputy Chief Nurse’s contributions to the updated policy and Terms of Reference of the MRG.
The revised ToR is at appendix 1 and the update learning from deaths policy at appendix 2
Additional Investment
At the September meeting of the Quality Service Committee, a referral was made to the Executives to discuss the requirements with respect to building capacity for case note reviewers and administrative support. In response to this, a mortality resource paper was presented to the DCHS Executive Team on 08/11/2017 setting out the additional investment required. The funding
Page 2 of 3221 Mortality Review Update.docxOverall Page 174 of 218

3
has been approved. A mortality review facilitator has been appointed and is currently undergoing induction. Recruitment of administrative support is to commence.
Reporting Schedule
The National Guidance on Learning from Deaths stipulates that quarterly mortality reports are provided to the Boards of NHS Trusts. In DCHS the mortality report is reported via the Summary Report of the Quality Service Committee (QSC).The Terms of Reference of the DCHS Mortality Review Group requires that group to provide bi-monthly Summary Reports to the Quality Service Committee. In order to comply with these performance indicators, the following reporting schedule is proposed:
Mortality Review Group Meeting
Quality Services Committee Meeting
Report due
August 2017 September 2017 Mortality ReportOctober 2017 November 2017 Summary ReportDecember 2017 January 2018 Summary Report & Mortality
ReportFebruary 2018 March 2018 Summary ReportApril 2018 May 2018 Summary Report & Mortality
ReportJune 2018 July 2018 Summary ReportAugust 2018 September 2018 Summary Report & Mortality
Report
Monitoring Information Brief Summary
What are there Governor Involvement implications?
DCHS Governors will want to be assured that the Trust is providing a robust response to the requirements within the National Guidance on Learning from Deaths; A Framework for NHS Trusts and NHS Foundation Trusts on Identifying, Reporting, Investigating and Learning from Deaths in Care
What are the Equality and Diversity implications?
The emphasis given to Learning Disability and Mental Health within the DCHS Mortality Review Policy is an indication of the Trust’s commitment to safeguarding the rights of all our patients including those with vulnerabilities.
What are the Patient, Public, Staff, Member and Stakeholder Involvement implications?
Our Public, Patients, Staff, Members and Stakeholders will be seeking assurance that DCHS has comprehensive, robust and responsive mortality review policy and process which are executed to the highest standards thus ensuring a culture of continuous quality improvement in learning from deaths across
Page 3 of 3221 Mortality Review Update.docxOverall Page 175 of 218

4
the organisation.
Risk Register
Is the issue on the current Risk Register?
Yes/No(Delete as appropriate)
If yes, what is the Risk Number? 3150
Does this update recommend a change in the current risk score? (If so, please provide your rationale below)The risk score has been amended to 8.This reflects the approval of the additional investment requested, the appointment of a mortality review facilitator/case note reviewer and the fact that administrative support recruitment is to commence.
Yes/No(Delete as appropriate)
Page 4 of 3221 Mortality Review Update.docxOverall Page 176 of 218

5
APPENDIX 1- Mortality Review GroupTerms of Reference
Page 5 of 3221 Mortality Review Update.docxOverall Page 177 of 218

Mortality Review GroupTerms of Reference
December 2017
IntroductionThe Mortality Review Group is a sub group of the Quality Services Committee. It is the strategic mortality overview group of DCHS with senior leadership and support to ensure the alignment of all DCHS teams for the purpose of reducing all avoidable deaths.
What
The purpose of the Group is to ensure that effective mechanisms are in place to review all relevant deaths and work towards the elimination of all avoidable mortality with a particular focus on:
(i) Case record review: The application of a systematic case record/note review to determine whether there were any problems in the care provided to the patient who died, in order to learn from what happened, for example Global Trigger Tool to determine if appropriate care occurred within the right timeframe.
(ii) Death due to lapses in care: A death that has been clinically assessed using a recognised methodology of case record/note review and determined more likely than not to have resulted from lapses in healthcare and therefore to have been potentially avoidable.
(iii) Capturing and responding to external and internal mortality outcomes and trends
enable/facilitate Trust-wide learning from mortality reviews through established mechanisms eg. Lessons Learnt Panel, Divisional Governance meetings
(iv) The Patient Experience Team will retain reponsibility for engaging with bereaved families and carers as per existing processes within the Trust.
Who
Core Membership: Deputy Medical Director- Chair Clinical Lead for Advanced Practice Mortality Review Facilitator/Case Note Reviewer Head of Patient Safety & Risk Management DCHS Public Governor Head of Patient & Family Centred Care Information Analytics Team Representative
Page 6 of 3221 Mortality Review Update.docxOverall Page 178 of 218

7
Clinical Lead for Operational Quality Strategic and Clinical Lead OPMH Physiotherapy Manager
In attendance:
Group admin support.
Senior Matron – Clinical Quality and Professional Standards Advanced Clinical Practitioner representative Integrated Community Matron Matron Expert Clinical Representative - To be determined( Will vary depending
on case under review)-
Quoracy Chair or Deputy ( Clinical Lead for Advanced Practice) plus three members
When The Mortality Review Group will meet bi-monthly
Where Meetings will be held on DCHS Premises or via Webex
Why The Group provides the DCHS response to the ‘National Guidance on Learning from Deaths’ produced by the National Quality Board (March 2017) and the ‘Implementing the Learning from Deaths framework: key requirements for Trust Boards’ produced by NHS Improvement (July 2017).
How
Receive & Review the Case Note (s) Review Reports Bimonthly Oversee the development of data collection systems to ensure the Trust’s
mortality data is timely, robust and in line with best practice Determine the avoidability of deaths within the Case Note Review
Reports. Refer all avoidable deaths for appropriate further investigation Review 3 ‘no concerns’ deaths at 6 monthly intervals The Group will provide the Quality Service Committee with an annual
report to demonstrate compliance with its Terms of Reference and that it has discharged its responsibilities appropriately and recommends any changes it considers necessary for approval.
A quarterly Mortality Report including any data regarding number of deaths and classification assigned to them will be sent to Quality Services Committee (QSC).
Identifying themes and areas of concern and recommend corrective actions or preventative measures
Escalate learning and action points to the Lessons Learned Panel and
Page 7 of 3221 Mortality Review Update.docxOverall Page 179 of 218

8
teams involved in the case through the Divisional Governance Meetings. To receive reports from the End of Life Care group of deaths warranting
case note review following review of complaints, incidents and audit reports received by the End of Life Care Group.
To provide feedback to the End of Life Care Group following case note review of deaths notified to the MRG by that group.
Recommend action plans and methodologies that are designed to reduce mortality across the Trust to QSC for approval.
Receive regular assurance that particular attention is paid to mortality reviews relating to patients with a learning disability or mental health condition.
Provide responses to mortality related enquiries from Regulatory bodies To report on Mortality performance to the Board via the Quality Services
Committee
Sub Committees /
Groups
The Mortality Review Group has no formal sub-group but will convene task & finish groups as required.
Communication Links
Quality Services CommitteePatient Safety TeamLessons Learned PanelDCHS Teams ( In-patients & communities)End of Life Care GroupCritically Ill People Prevention Group( CIPP)Clinical Safety GroupClinical Effectiveness GroupPatient Experience Team
Reporting To Quality Services Committee via bimonthly Summary report
Key Performance
Indicators/Key Deliverables
Receive & review the Case Note (s) Review Reports - Bimonthly Oversee the development of data collection systems to ensure the Trust’s
mortality data is timely, robust and in line with l best practice-by March 2018
Refer 100% of all avoidable deaths for further investigation Review 3 ‘no concerns’ deaths at 6 monthly intervals Quarterly Mortality Reports to QSC Annual Report to QSC demonstrating compliance with the Terms of
Reference. Biennial review of trends emerging from mortality reports and commission
in-depth review where concerning trends noted.
Review Date December 2018
Page 8 of 3221 Mortality Review Update.docxOverall Page 180 of 218

9
APPENDIX 2 – DCHS Learning from Deaths Policy
Page 9 of 3221 Mortality Review Update.docxOverall Page 181 of 218

10
DCHS Learning from Deaths PolicyDocument HistoryModified Date: 29/09/2017
Version Number: 2 Reference Number: P72
Next Revision Due: 6 Months29/06/2018
Review Status Actively under Review
Author: Owolabi Bola (RY8) Derbyshire Community Health Services
Policy Sponsor: Meredith Rick (RY8) Derbyshire Community Health Services
Team: Clinical
Approved by: Quality Service Committee Date:29/09/2017
Category: Clinical
Sub Section: Clinical Services
Type of Document: PoliciesHave you assessed the Equality Impact of this policy?
(please see section 12)
Contact Name for Policy Queries Owolabi Bola (RY8) Derbyshire Community Health Services
Contact Name for SharePoint document upload [email protected]
Key Words mortality, end of life, case note review, duty of candour, investigation
Comments
Corporate Leads: Dr Rick Meredith – Executive Medical DirectorProfessor Chris Bentley - Lead Non-Executive Director for Mortality Reviews as per National Guidance
Please indicate which groups have discussed this policy:
[Governance Group]Quality
Date(s) discussed: 03/07/2017
Has this Policy previously been known under another title? If so, please state previous title.
Mortality Review Policy
Date changed: December 2017
Revision HistoryVersion Revision
dateSummary of Changes
Page 10 of 3221 Mortality Review Update.docxOverall Page 182 of 218

11
1 June 2017 Development of new policy
2 November 2017
Title Changed to Learning from Deaths Policy
To help ensure that this policy is as accessible as possible, it has been left-aligned and is available in alternative formats and languages. To obtain a copy of the policy in large print, audio, Braille (or other format) or in a different language, please contact The Communications Team, by Tel: 01246 515224 or email [email protected]
TABLE OF CONTENTS
1 Aim/Purpose.......................................................................................................................4
2 Intended Users...................................................................................................................5
3 Disclaimer Statement ........................................................................................................5
4 Definitions and An Explanation of Terms Used..............................................................6
5 Full Details of The Policy ..................................................................................................75.1 Reporting and Initial Review of Deaths..........................................................................75.2 Central Recording of Deaths..........................................................................................85.3 Initial Death Review .......................................................................................................8
5.3.1 Initial Death Review Outcome Criteria Investigation Requirements........................85.4 Responding to Deaths .................................................................................................10
5.4.1 Multi Agency Response.........................................................................................105.4.2 Specified Categories of Deaths.............................................................................105.4.3 Referred Deaths....................................................................................................105.4.4 Expected Deaths...................................................................................................11
5.5 Support and Engagement with The Bereaved.............................................................115.5.1 Signposting and Guidance ....................................................................................11
5.6 Case Note Review .......................................................................................................115.6.1 Investigation and Case Note Review Timescales .................................................13
5.7 Consent........................................................................................................................135.8 Minimum Standards For Mortality Review Process .....................................................13
6 Education And Training ..................................................................................................13
7 Support and Additional Contacts...................................................................................14
8 Supporting Documents or Relevant References ..........................................................14
9 Consultation and Approval .............................................................................................15
10 Monitoring/Audit ...........................................................................................................1610.1 Monitoring Compliance with The Document.............................................................16
11 Governance ...................................................................................................................16
12 Equality Impact..............................................................................................................17
Page 11 of 3221 Mortality Review Update.docxOverall Page 183 of 218

12
12.1 Equality Analysis Summary ......................................................................................17
13 Dissemination And Implementation ............................................................................17
14 Appendices....................................................................................................................1814.1 Appendix 1 – Monitoring/Audit Tool..........................................................................1914.2 Appendix 2 - Flow Chart For The Mortality Review Process ....................................2014.3 Table 1: Avoidability Of Death Scale .......................................................................2114.4 Appendix 3 - “In Depth Review” Mortality Summary Sheet ......................................22APPENDIX 6 – END OF LIFE STRATEGY………………………………………………… 14APPENDIX 7 – INVESTIGATION OF INCIDENTS, COMPLAINTS AND CLAIMS…… 14
Page 12 of 3221 Mortality Review Update.docxOverall Page 184 of 218

13
1 Aim/Purpose
This policy confirms the process to ensure a multi-disciplinary, consistent and coordinated approach for the review of deaths that occur in all DCHS in-patient and community team case loads.
The aim of the learning from deaths process is to identify any areas of practice both specific to the individual case and beyond that could potentially be improved, based upon peer group review. Areas of good practice are also identified and supported.
To describe in detail the three-stage mortality review process within the Trust, detailing how reviews should be completed, by whom and when to ensure that learning from deaths is made a Trust priority and leads to developments and improvements in patient care.
The purpose of these reviews is to highlight lapses in care that may have contributed to a death and to learn from the death to prevent, where possible, recurrence. The outputs from mortality reviews are; shared learning and corrective actions undertaken.
The learning from death process will ensure that there are clear auditable reporting mechanisms in place, to escalate any areas of concern identified: to the clinicians concerned; and the appropriate Committees through to DCHS Trust Board so that they are aware and can take appropriate action.
This policy outlines how DCHS responds to, and learns from, deaths of patients who die under its management and care, whether or not they meet the definition of a serious incident (SI) in accordance with the National Quality Board’s National Guidance on Reporting and Learning from Deaths.
The Learning from death policy does not replace existing policies relating to the review of deaths e.g. LeDER. However, it provides an overview of the current processes, policies and approaches to reviewing death in DCHS.
The policy also clarifies:
i) How our processes respond to the death of an individual with a learning disability, or mental health needs, an infant or child death and a stillbirth or maternal death
ii) The Trust’s approach in undertaking case record reviews
iii) Categories and selection of deaths in scope for case record review
iv) Categories and selection of deaths out of scope for case record review and our rationale for exclusion.
v) DCHS’ approach to meaningful involvement and engagement of bereaved families and carers in the investigation of deaths deemed as more likely than not to be avoidable following case note review.
vi) Our data collection and reporting approach: The data will include
a) The total number of deaths (In-patients (including OPMH) & Community Team caseloads)
b) Deaths subjected to case record review. c) Deaths deemed avoidable following case note review
Page 13 of 3221 Mortality Review Update.docxOverall Page 185 of 218

14
vii) Quality Account: The data published by DCHS in our Public Board papers will be summarised in the Quality Account from June 2018 including evidence of learning and action as a result of this information and an assessment of the impact of actions taken by the Trust.
Our Guiding Principles: Improved speed of response to concerns. An open and transparent learning culture. Continuous quality improvement through lessons gained from the mortality review
process.
NHS staff work tirelessly under increasing pressures to deliver safe, high-quality healthcare. When mistakes happen, Providers working with their partners need to do more to understand the causes. The purpose of reviews and investigations of deaths, which lapses in care might have contributed to, is to learn in order to prevent recurrence. Reviews and investigations are only useful for learning purposes if their findings are shared and acted upon. DCHS intend to share learning both within and outside our organisation to facilitate wider improvements across the health and social care system. This will be achieved by sharing learning and recommendations from mortality reviews with the team to whom the case reviewed relates, Lessons Learned Panel and by secure email communication with organisations external to DCHS where this is relevant and appropriate.
2 Intended UsersDCHS
Chief Executive’s Department YESFinance Performance and Information YES
Quality YESStrategy YES
Operations YESPeople & Organisational Effectiveness YES
General Practices (GP) YES
Where this policy where states “all employees”, please note that it relates to all the employees who are highlighted in the table above
3 Disclaimer StatementIt is a requirement that the reader follows this policy and accepts professional accountability and maintains the standards of professional practice as set by the appropriate regulatory body applicable to their professional role and to act in accordance with the express and implied terms of your contract of employment, in accordance with the legal duties outlined in the NHS Staff Constitution (section 3b). If there are any concerns with this document, then the reader should initially discuss the specific issue with their line manager or raise it through appropriate “raising concerns” channels. The line manager should agree a course of action that is appropriate and reflect this in the patients notes and with the policy sponsor.
Page 14 of 3221 Mortality Review Update.docxOverall Page 186 of 218

15
4 Definitions and Explanation of Terms Used
Terms ExplanationAvoidable/Preventable
Something that is avoidable can be prevented from happening. These terms are used interchangeably in the NHS and for the purpose of this policy ‘avoidable’ or ‘unavoidable’ will be used with reference to whether anything could have been done to change the outcome.
Case Record Review
Is a process aimed at obtaining retrospective information to determine if care was delivered within expected standards. The application of a case record/note review to determine whether there were any problems in the care provided to the patient who died in order to learn from what happened.
Complication An additional problem that arises following a procedure, treatment or illness and is secondary to it/complicates the situation.
Death due to a problem in care
Death that has been clinically assessed using a recognised methodology of case record/note review and determined more likely than not to have resulted from problems in healthcare and therefore to have been potentially avoidable.
Investigation The act or process of investigating; a systematic analysis of what happened, how it happened and why. This draws on evidence, including physical evidence, witness accounts, policies, procedures, guidance, good practice and observation - in order to identify the problems in care or service delivery that preceded an incident to understand how and why it occurred. The process aims to identify what may need to change in service provision in order to reduce the risk of future occurrence of similar events.
Mortality For the purpose of the Mortality Report, mortality relates to:i) All deaths classified as avoidable by the Mortality Review Group
following case note review and using the avoidability of death scale (See Table 1)
ii) Cases where concerns have been raised in relation to the care of deceased patients – these are expected to be identified by incident reporting
iii) All cases subject to Serious Incidents investigations(SI))/Cases reported to the Coroner
iv) Deaths where complaints, concerns or incidents have been reported in relation to the end of life care provided to the deceased requiring further case review
v) Deaths of patients with known mental health diagnosis (In-Patients Only)vi) Deaths of patients with learning disabilityvii) Infant deaths, still births, maternal deathsviii) A proportion of deaths that are classified as expected and for which no
concerns were raised (3 every 6 months)Mortality Review Group (MRG)
A multi-disciplinary group that reviews and discusses clinical cases, outcome data (clinician and patient reported) and related information (e.g. SI, complaints, other benchmarking data).
Policy A statement of the Board’s agreed position and governing principles in relation to particular issues or situations. In the context of this policy the subject is relating to Mortality Review Process.
Lead Non-Executive
The Trust nominated Lead Non-Executive Director for Mortality oversees the Trust’s approach to learning from patient deaths and guidance on this role
Page 15 of 3221 Mortality Review Update.docxOverall Page 187 of 218

16
Director for Learning from deaths
can be found within Appendix B of the National Guidance on Learning from Deaths produced by the National Quality Board. The role of the nominated Non-Executive Director for learning from deaths is to ensure that there are mortality review processes in place that are ‘robust, focus on learning and can withstand external scrutiny, by providing challenge and support’ with quality improvement as the purpose of the exercise’.
NRLS The National Reporting and Learning System (NRLS) is the central database of all patient safety incident reports. The Trust regularly submits data to this national database which is analysed nationally to identify hazards, risks and opportunities to continuously improve the safety of patient care on a national basis. Reports are produced every six months by NHS Improvement. The NRLS also shares information on incidents to the Care Quality Commission.
Regulation 28 The Coroner has a legal power and duty to write a report following an inquest if it appears there is a risk of other deaths occurring in similar circumstances. This is known as a 'report under regulation 28' or a Preventing Future Deaths Report (PFD) because the power comes from regulation 28 of the Coroners (Inquests) Regulations 2013. The Executive Medical Director is responsible for liaison with the Coroner and the Trust must reply within 56 days to say what action we plan to take or have taken already.
STEIS The Strategic Executive Information System is an electronic database through which the Providers communicate serious incidents to the Commissioners. This detail is accessible by the CQC and helps to inform Provider inspections. The Patient Safety team are responsible for recording serious incidents onto STEIS.
Serious Incident (SI)
An accident occurring on NHS premises that resulted in serious injury, and or permanent harm, unexpected or avoidable death (ref SI details).
Never Event Never Event Incidents are serious, preventable patient safety incidents that should not occur if the available preventative measures have been implemented by the healthcare provider. These are reviewed on an annual basis and are available on the Department of Health website. https://www.england.nhs.uk/patientsafety/never-events/
5 Full Details of the Policy
5.1 Reporting and Initial Review of Deaths
Compliance with this section of the policy will ensure the Trust follows the National Quality Board’s Guidance on Learning from Deaths.
Page 16 of 3221 Mortality Review Update.docxOverall Page 188 of 218

17
5.2 Central Recording of Deaths
There are existing mechanisms for recording deaths in DCHS.As part of implementing the learning from deaths policy; these are being developed further through the creation of a central mortality reporting system whereby data on deaths are drawn from the Electronic Patient Records (EPR). These will be cross-referenced with other review processes e.g. deaths subject to coroner’s inquest, safeguarding reviews, etc. The cross-referenced data will be held on the Quality Drive pending further development of a bespoke mortality IT platform.
5.3 Initial Death Review
The mortality review facilitator will work with appropriate clinical lead for ensuring the completion of the Initial Death Review within three working days of the Trust becoming aware of a death. The data will be pulled from the Quality Drive as described above. The initial death review should:
Identify and provide assurance that any necessary immediate action to ensure the safety of patients, staff, and the public is in place
Assess the death according to the criteria below and determine whether Outcome 1, 2 or 3 apply and propose the level of investigation or case note review required
Provide details of communication with the family and any information regarding the application of the Duty of Candour
The Initial Death Review Report should be uploaded to the Quality Drive.
This review also acts as a triage to determine whether the death should be reported on STEIS as a serious incident and the level of investigation required. The outcome of the Initial Death Review will be either:
Outcome 1 - With the facts known it meets the definition of an SI – if not already recorded, this would require reporting on Datix & STEIS.
Or
Outcome 2 - The death does not appear to meet the definition of an SI but does need to be looked at in more detail and a case note review is warranted.
Or
Outcome 3 - There are no apparent issues that need to be explored.
NB: If following the Initial Death Review in 3 working days, any of the Outcome 1 or 2 criteria are found to have been met, the process will start from that date.Recording the outcome of decision whether or not to review or investigate a death: Following initial death review (IDR) as detailed above, if the outcome is Outcome 3, the rationale for this decision will be recorded and updated on the Quality Drive.
Page 17 of 3221 Mortality Review Update.docxOverall Page 189 of 218

18
5.3.1 Initial Death Review Outcome Criteria Investigation Requirements
Outcome 1 - The definition of an SI is met (see Section 4), as a minimum this relates to the following deaths:
Apparent suicide/ self-inflicted death/ accidental overdose
Apparent homicide – perpetrator or victim – These will normally be received via safeguarding processes
Deaths where abuse or neglect is known - These will normally be received via safeguarding processes
Deaths following a Never Event
Deaths of patients detained under the MHA/CTO or subject to recall
Deprivation of Liberty applied (including care home)
The Initial Death Review will propose a comprehensive investigation is conducted as per NHS England SI Framework or a case note review and provide rationale for this.
Outcome 2 – The definition of an SI has not been met, however the following apply: All deaths where bereaved families and carers, or staff, have raised a significant
concern about the quality of care provision;
All deaths in a service specialty, particular diagnosis or treatment group where an ‘alarm’ has been raised with DCHS through whatever means (for example raised by audit work, concerns raised by the CQC or another regulator);
All deaths in areas where people are not expected to die, for example death occurring within 30 days of day case surgery/elective procedure
Deaths where learning will inform DCHS’ existing or planned improvement work, for example if a death is reported via DCHS End of Life Care audit as being due to sepsis, such a death will be reviewed.
All unexpected in-patient deaths (including OPMH)
Deaths within the Integrated Community Services (ICS) division where complaints/ concerns/incidents have been reported in relation to the patient’s end of life care.
All deaths subjected to Coroner’s inquest (and the death has not already been investigated or reviewed by the Trust)
A proportion of expected deaths e.g. of patients receiving end of life care
Cases flagged through the Trust’s Bereavement Survey
If the above apply, a Case Notes Review should be conducted.
Outcome 3 – The criteria for Outcome 1 and 2 have not been met, therefore no further investigation is required. Rationale for this will be provided. In these cases, the final stage will be updating the Quality Drive. However, Case Notes Review will be
Page 18 of 3221 Mortality Review Update.docxOverall Page 190 of 218

19
conducted in a sample of “no-concern” deaths. Three “no-concern” deaths will be reviewed by the Mortality Review Group on a six-monthly basis.
The template for Initial Management and Death Review Reports are available in the Quality Drive. All Initial Death Review Reports which meet outcome 1 will be reviewed via the process outlined in the existing Serious Incident/Issues Review policy. Outcomes from the Serious Incident Investigation will be included in the Mortality Report to QSC. Additionally, all case note review findings for deaths which meet Outcome 2 criteria will also be included in the mortality report. .
5.4 Responding to Deaths
5.4.1 Multi Agency Response
Reporting death within DCHS and to other organisations that may have an interest (including the deceased person’s GP). The mortality review process is shown in Appendix 2 (Flow Chart). On receipt and review of the Case Note Reviewer(s) reports, the MRG will assess the avoidability of the death. Where a death is deemed to have been more than likely to be avoidable, the MRG will escalate this to the Service General Manager for further investigation. The General Manager is required to instigate Duty of Candour processes to undertake a root cause analysis investigation and to determine learning. Other organisations that may have interest (including the patient’s GP) will be notified as part of the investigation process. The MRG will also report all deaths subjected to case note review to the QSC.
5.4.2 Specified Categories of Deaths
Responding to the death of an individual with a learning disability, or mental health needs, an infant or child death and a stillbirth or maternal death. The following categories of deaths (except severe mental illness) are excluded from our case note review process because they are reviewed via independent processes to DCHS. However, learning from these deaths will be captured and communicated across DCHS through various governance groups in the Trust including Mortality Review Group, Clinical Safety Group, Lessons Learned Panel, Safeguarding Governance Group and external organisations such as Derby Safeguarding Children Board sub-group, the Serious Case Review Group, the Derbyshire Safeguarding Adults Board, Domestic Homicide Review Group and Fatal Fire Review Panel.
The death of an individual with a learning disability will be reviewed via the regional LeDER programme
Deaths of patients within the OPMH service (severe mental health needs) will be subjected to case note review through the DCHS mortality review process. The case note review report will be discussed by the Mortality Review Group with a view to identifying any lapses in care and learning from these. The findings will be communicated via the communication links of the MRG and the Mortality Report to QSC
Infant or child death are reviewed via the Derbyshire Safeguarding Children Board Child Death Overview Panel
Stillbirth or maternal deaths are reviewed via the Confidential Enquiries into Maternal and Infant Deaths.
Page 19 of 3221 Mortality Review Update.docxOverall Page 191 of 218

20
5.4.3 Referred DeathsReviewing the care provided to patients not under the care of DCHS at the time of death but where another organisation suggests that the Trust should review the care provided to the patient in the past; In instances where DCHS is notified by Partner organisations of the need to review the care provided to patients not under the Trust’s care at the time of death, the Trust will respond in a timely manner. Review of the death will be carried out through the Mortality Review Process outlined in Appendix 2 Flow Chart. There may be instances where it is more appropriate for the review to be carried out by other groups within the Trust. Learning from such reviews will be communicated via a range of channels including the Mortality Report and the Lessons Learned Panel.
5.4.4 Expected DeathsReviewing the care provided to patients whose death may have been expected, for example those receiving end of life care; DCHS has an established end of life care audit programme. This is the mechanism by which the Trust reviews the care provided to patients whose death may be expected for example end of life care. The end of life audit programme assesses the quality of care delivered against the standards within the One Chance to Get It Right document in line with the Five Priorities of Care.
5.5 Support and Engagement with the BereavedEngaging meaningfully and compassionately with bereaved families and carers is a key priority for DCHS. The existing DCHS Complaints and Concerns Policy is geared towards meaningful and compassionate involvement with bereaved families and carers. Contact is coordinated by the Patient Experience Team. All bereaved families and carers are offered a meeting at the outset as this often strengthens their confidence in the process. The Patient Experience Team will provide support within the complaints processes to ensure concerns are investigated and responded to in a timely manner. Bereaved families and carers are offered a meeting at the end of the complaint investigation process to share the findings.
5.5.1 Signposting and Guidance.Everyone who has concerns investigated under the complaints procedure, including bereaved families and carers are advised on what to do should they remain dissatisfied with the outcome of the complaint investigation and response to their concerns. Information on how to contact the Parliamentary and Health Service Ombudsman (PHSO) is provided in every complaint response letter. The PHSO will review the complaint and the way in which it has been handled by the Trust. The Complaints and Concerns Policy provides further information and guidance on complaints handling within the organisation.
5.6 Case Note Review Case note reviews will be completed for deaths that do not meet the definition of an SI but would benefit from a further review. This will be implemented through a phased approach prioritising in-patients, where bereaved families or staff have raised concerns. Until this is fully rolled out, a Level 1 concise investigation will be always be conducted for these deaths to ensure they are subject to a review.
Individual case note reviewers will apply the following tools for conducting the case note review objectively:
There is currently no consensus on the best case note review tool to use in Community and Mental Health settings. DCHS will adapt existing tools and methodologies including:
Page 20 of 3221 Mortality Review Update.docxOverall Page 192 of 218

21
Global Trigger Tool (Community element)Structured Judgment Review (SJR) methodologyPRISM methodologySuicide Review ToolExisting modified DCHS RCA Tool
This will mean that at this point in the Learning from death process our case note review tool will be a hybrid of the above (This process is currently being developed)The case note reviewer will employ whichever tool is most suitable and appropriate to the case under review
Page 21 of 3221 Mortality Review Update.docxOverall Page 193 of 218

22
5.6.1 Investigation and Case Note Review Timescales
Investigations into STEIS reported serious incidents are required by commissioners to be completed within 60 working days. In exceptional circumstances an extension to this time frame can be applied for to the Commissioners by the Divisions on request from Division Governance Teams.
Internal SIs and case note reviews should also be completed with 60 working days.
There may be occasions where an internal investigation cannot start until an external agency has given the go-ahead i.e. Police, Coroner, Fire Service, Health and Safety Executive, etc. In such cases it may also be possible to coordinate or combine the investigation with the external body.
The Mortality Review Facilitator will be responsible for monitoring and ensuring that required timescales are being met and escalating via appropriate mechanisms where there may be potential breaches. They will also ensure that case note reviews are carried out accordingly and in a timely manner using objective case note review tools and techniques.
5.7 Consent
The Consent Policy must be adhered to. In the case of deceased patients this must be raised with the Responsible Clinician with reference to the Mental Capacity Act Policy and Procedure
5.8 Minimum Standards for Mortality Review Process For meetings to take place regularly and all associated processes to be completed in line
with DCHS Trust policies. To provide Mortality Report to QSC for onward publication in Public Board papers to
include o total number of deathso deaths reviewed by Mortality Review Groupo deaths deemed avoidable by Mortality Review Groupo Log of deaths subject to investigation/review processes by external bodies e.g.
Coroners or other groups within DCHS e.g. as part of SUIs process..o deaths flagged to DCHS for review by partner organisations (Health and Social Care)o learning from deaths subjected to case note reviewo learning from other mortality review processes – Learning Disabilities Mortality Review
(LeDER) Programme, Child Death Overview Panel, The Confidential Enquiry into Maternal Deaths (CEMD)
6 Education and Training Training is a key element to the successful implementation of this policy. There is currently no nationally defined training programme for case note reviewers in Community Trusts. Pending the availability of this, DCHS Case Note Reviewers and members of the MRG will receive formal RCA training. This will be mandatory and conducted at 3 yearly intervals. A learning pathway will be created on ESR for members of staff involved in this process in order to ensure robust training compliance monitoring. Once a national case note review training
Page 22 of 3221 Mortality Review Update.docxOverall Page 194 of 218

23
programme is available for Community Providers, DCHS case note reviewers will engage and comply fully with the training requirements.
STAFF TRAINING
Training regarding the incident reporting and investigation procedures will be delivered in various forms for all staff and will be covered in:
Staff Induction (local)
Training Needs Analysis
Essential Skills and Training
Guidance (to be made available on myDCHS)
Training for undertaking case note reviews will be developed. The Case Note Reviewers require training on the use of the various case note review tools/methodologies. Members of the MRG require formal RCA training and updates at regular intervalsIn the Community Hospitals, Outpatients and Community based teams, all staff who provide patient care should have an awareness of this policy. This will better aid their understanding of the policy aims in demonstrating effective and safe patient care and provide a clear vision on the importance of their role in this process.
Where managers identify the need for some specific training in this policy and procedure they should contact the Training & Workforce Development Team.
7 Support and Additional ContactsThe individuals responsible for developing the document and from whom additional support and advice can be obtained in order to implement the document.
Deputy Medical Director [email protected] Tel: 07886 499135
Clinical Lead for Advanced Practice [email protected] Tel: 07765 863054
Head of Patient Safety & Risk Management [email protected] Tel: 07824 624452
Head of Patient & Family Centred Care [email protected] Tel:07979653837Mortality Review Facilitator [email protected]
Quality Triage Office 01246515870
8 Supporting Documents or Relevant References
National Guidance on Learning from Deaths: A Framework for NHS Trusts and NHS Foundation Trusts on Identifying, Reporting, Investigating and Learning from Deaths in Care’ and the earlier CQC Learning, Candour and Accountability report.
Page 23 of 3221 Mortality Review Update.docxOverall Page 195 of 218

24
The Learning Disability Mortality Review Programme (LeDeR) http://www.hqip.org.uk/national-programmes/a-z-of-clinical-outcome-review-programmes/learning-disability-mortality-review-programme/
Transforming Care for People with Learning Disability- Next Steps https://www.england.nhs.uk/learningdisabilities/care/
LeDER Process Flowchart Confidential Inquiry into premature deaths of people with learning disabilities (CIPOLD)
http://www.bristol.ac.uk/cipold/ Learning, candour and accountability - A review of the way NHS trusts review and
investigate the deaths of patients in England https://www.cqc.org.uk/sites/default/files/20161213-learning-candour-accountability-full-report.pdf
Learning from deaths in the NHS https://improvement.nhs.uk/resources/learning-deaths-nhs/
The Mid Staffordshire NHS Foundation Trust Inquiry; Independent Inquiry into care provided by Mid Staffordshire NHS Foundation Trust; January 2005 to March 2009; Volume 1. Chaired by Robert Francis QC, Published 24 February 2010. https://www.gov.uk/government/publications/independent-inquiry-into-care-provided-by-mid-staffordshire-nhs-foundation-trust-january-2001-to-march-2009
DCHS’ Incident & Serious Incident (SI) Policy DCHS’ Bereavement Survey Using the structured judgement review method A guide for reviewers
9 Consultation and Approval Consultation The Deputy Medical Director has delegated responsibility for the review of the Mortality
Review Policy. The document has been written with advice from Medical Directorate Clinicians and Mortality Review Group members. This policy has been developed based on requirements outlined in the ‘National Guidance on Learning from Deaths - A Framework for NHS Trusts and NHS Foundation Trusts on Identifying, Reporting, Investigating and Learning from Deaths in Care’.The draft policy has been circulated to the Quality Services Committee (Deep Dive session), Clinical Lead for Advanced Practice, Head of Patient Safety & Risk Management, Safe Care Officer, Deputy Chief Nurse, Clinical Effectiveness Facilitator and the Patient Safety Team for comments and amendments made where necessary.
An equality impact assessment has been conducted on this policy to ensure its consideration to the impact on local vulnerable people and those from the protected equality groups.
Page 24 of 3221 Mortality Review Update.docxOverall Page 196 of 218

25
Trust Board The Trust Board is responsible for setting the strategic context in which the organisational procedural documents are developed. The Board will approve strategies for implementation. Depending upon the nature of the procedural document, the Board may also be asked to ratify procedural documents making them valid by formally confirming approval.
Committees The Deputy Medical Director will present a final copy of the policy to the Mortality Review Group (MRG) for comment and Quality Services Committee (QSC) for approval.
10 Monitoring/Audit It is necessary to routinely check whether or not a policy is being followed. Appendix 1 should be completed for all clinical policies and can be used to determine compliance for all policies. This section should also be used to make reference to any other monitoring of this policy (e.g. planned audits).
10.1 Monitoring Compliance with the Document This policy will be monitored and reviewed by the MRG, for key indications.
The data collected from the monitoring process will be available for inspection by the NHS Litigation Authority and other appropriate external bodies. The outcome of the monitoring will be reported to the Mortality Review Group (MRG) and Quality Services Committee (QSC).
11 Governance Key Performance Indicators
The MRG will hold bi-monthly meetings and have agreed Terms of Reference. A quarterly assurance report including any data regarding number of deaths and
classification assigned to them, and the summary of the meetings, will be provided to QSC.
The Deputy Medical Director, Chair of the Mortality Review Group will provide an Annual Report to QSC.
Information Governance The minutes of the MRG will summarise the discussion taking place at the meeting,
including outcomes of individual reviews. The reports concerning individual cases and discussion relation to them are confidential
and shall be exempt from requests under the Freedom of Information Act.
Duty of Candour and Raising Concerns Where issues or incidents not previously identified or raised are found during a review of the patient care the MRG will report the incident according to the usual Trust process.
Page 25 of 3221 Mortality Review Update.docxOverall Page 197 of 218

26
12 Equality Impact
12.1 Equality Analysis SummaryAll public bodies have a statutory duty under The Equality Act 2010 (Statutory Duties) Regulations 2011 to provide, “evidence of the analysis it undertook to establish whether its policies and practices would further, or had furthered, the aims set out in section 149(1) of the [Equality Act 2010]”, in effect to undertake a written record of equality analysis and due regard on all procedural documents and practices.
Derbyshire Community Health Services, NHS FT considers how the decision it makes affects people who share different protected characteristics (race, disability, sex, gender re-assignment, religion/belief, sexual orientation and age). DCHS also recognises that there are groups/communities that are recognised at a local level within society as excluded or disadvantaged in addition to those listed as protected groups above and this document is inclusive to these groups also for example, young teenage parents, homeless people etc.
The policy applies to all groups and there will be no discrimination based on age, race, disability, sex, gender re-assignment, religion/belief or sexual orientation. Where discrimination is noted this will be addressed through the Human Resources Framework and may result in disciplinary actions. A completed Equality Analysis is presented at appendices 2a and 2b of this document.
13 Dissemination and Implementation
Dissemination The document will be published electronically on the DCHS Trust intranet.
What effect or impact will the new/changed policy have on each of the Protected Characteristics (age, gender, disability, gender reassignment, marriage or civil partnership, pregnancy or maternity, race, religion or belief, sexual orientation)?
This policy will ensure that equal focus is given to the review of deaths of patients with learning disability, maternity deaths, patients with mental health diagnosis and patients with other/no protected characteristics
Stage_1_-_Equality_relevance Mortality Review Policy.doc
Stage_2_-_Equality_Impact_Assessment_or_Analysis Mortality Review Policy.doc
If this effect or impact is negative or disadvantages one or more of the Protected Characteristics, what changes are going to be made to either remove entirely or minimise this effect or impact? (Note: if the policy could be discriminatory, seek immediate advice from the Head of Equality, Diversity and Inclusion)
N/A
Page 26 of 3221 Mortality Review Update.docxOverall Page 198 of 218

27
ImplementationThis policy has some significant changes to previous policy, particularly the introduction of Initial Death/Management Reviews, Case Note Reviews and the central recording and monitoring of deaths. Full implementation of this policy will not be immediate and therefore implementation will be incremental and subject to evaluation. The policy will be announced to all relevant staff via the communications e-bulletin (Safe Care Newsletter) with the support of the Patient Safety and Communication Teams
The policy will be disseminated via leadership and teams briefings and the MRG.
The Mortality Administrator will be a key role in ensuring the successful implementation of this policy. They will co-ordinate the processes covered by this policy and will ensure that all those involved in the process are aware of their responsibilities and the requirements of the policy.
14 Appendices
Appendix 1 – Monitoring & Audit ToolAppendix 2 – Flow Chart for the Mortality Review ProcessAppendix 3 – “In Depth Review” Mortality Summary SheetAppendix 4 – Being Open and Duty of CandourAppendix 5 – Terms of Reference for Mortality Review Group
Mortality Review Group Terms of Reference Dec 2017 v3.3.docx
Appendix 6 – End of Life Strategy
EOL strategy.docx
Appendix 7 – Investigation of Incidents Complaints and Claims
Page 27 of 3221 Mortality Review Update.docxOverall Page 199 of 218

28
14.1 Appendix 1 – Monitoring/Audit Tool
CORE STANDARDS (relevant to this policy)
Indic. No
Description of the Core Standard Standard (%)
Exception’s Definitions and Instructions
1 Mortality Review Group to meet bimonthly 100%2 Mortality Review Group to provide Quarterly Report to QSC 100%
3 Annual Mortality Report to be published in public Board papers 100%
4 In-depth Case Note Review Report to be presented to MRG bi-monthly by the Case Note Reviewer 100%
5 In-depth Case Note Review of All eligible categories to be conducted monthly by the Case Note Reviewer 100%
Page 28 of 3221 Mortality Review Update.docxOverall Page 200 of 218

29
14.2 Appendix 2 - Flow Chart for the Mortality Review ProcessMortality data
drawn from Electronic Patient
Records(TPP) monthly
Mortality review facilitator cross references with other mortality review data e.g.
safeguarding review
Conduct initial Death Review (IDR)
within 3 working days*
Outcome 2Death is not an SI but further review
needed Undertake a Case Note Review (CNR)
within 60 days and update Mortality database on Quality Drive
Submit CNR report to Mortality Review Group
If the Case Note Review identifies that definition of an SI is met – follow Outcome 1 process
Outcome 1Death meets the definition of an SI Complete SI1 Report on STEIS Update DATIX if not already
done Recommend Comprehensive
Level 2 investigation if not already commenced.
Submit IDR form to the Patient Safety Team
Update Mortality database on Quality Drive
Outcome 3No CNR or Investigation Required
Record rationale on IDR Update Mortality data base
on Quality Drive
Patient Safety Team to: Determine Investigation
procedure and teams to involve e.g. Patient Experience Team.
Ensure Duty of Candour policy is adhered to
Mortality Review Group Meet bi-monthly Review Case Note Review reports Determine degree of avoidability using Structured
Judgment Review(SJR) Avoidability Scale Mortality Review Facilitator to upload individual
“In-depth Review Mortality Summary Sheet” on to Mortality Database on Quality Drive
Submit report and learning to relevant Divisional Governance Group and Lessons Learned Panel
Communicate learning to external agencies via secure nhs.net email where relevant
Refer cases warranting further investigation to relevant Clinical LeadLevel 2 –
Comprehensive Investigation
60 working days
Submit completed investigation to Division Governance Team
Initial Death Review Outcome
Outcome 1 Apparent suicide/self inflicted death/
accidental overdose Apparent homicide – perpetrator or
victim Deaths where abuse or neglect is
known Deaths following a Never Event Deaths of patients detained under
the MHA/CTO Deprivation of Liberty applied
(including care home)
Outcome 2 Where bereaved families and carers, or staff have
raised a significant concern about the quality of care provision
Deaths in areas where an ‘alarm’ has been raised with DCHS through whatever means(for example raised by audit work, concerns raised by CQC or another regulator)
Deaths where people are not expected to die, for example occurring within 30 days of day case surgery/elective procedure
Deaths where learning will inform DCHS’ existing or planned Quality Improvement work .g. deaths due to sepsis
All unexpected in-patient deaths(including OPMH) Deaths subjected to Coroner’s Inquest(and the
death has not already been investigated or reviewed by the Trust)
Deaths flagged through the Trust’s Bereavement Survey
A proportion of expected deaths e.g. of patients receiving end of life care
Outcome 3No further investigation or Case Note Reviews is required.
Page 29 of 3221 Mortality Review Update.docxOverall Page 201 of 218

30
14.3 Table 1: Avoidability of Death Scale
Avoidability of Death ScaleScore 1 Definitely avoidable
Score 2 Strong evidence of avoidability
Score 3 Probably avoidable (more than 50:50)
Score 4 Possibly avoidable, but not very likely (less than 50:50)
Score 5 Slight evidence of avoidability
Score 6 Definitely not avoidable
Example structured judgement commentary Non-invasive ventilation management was sub-optimal, but ultimately it was the patient’s wish not to continue treatment. There may have been an alternative cause of breathlessness that was not fully explored or treated, which is why there may have been some avoidability
Using the structured judgement review method a guide for reviewers
Page 30 of 3221 Mortality Review Update.docxOverall Page 202 of 218

31
14.4 Appendix 3 - “In Depth Review” Mortality Summary Sheet
Date of IN DEPTH Review:
Group members in attendance at this review (list names and roles)
Patient NHS Number: Hospital/Ward/Community team: Date of Admission (to in-patient hospital or Community Team caseload):
Date of Death
‘Avoidability of Death’ scale (trigger tool) (circle your response)
Score 1 Definitely avoidableScore 2 Strong evidence of avoidabilityScore 3 Probably avoidable (more than 50:50)Score 4 Possibly avoidable, but not very likely (less than 50:50)Score 5 Slight evidence of avoidabilityScore 6 Definitely not avoidable
Timeline of patient history prior to death:
What were the Triggers for this review (please tick all that apply)
Serious Incidents relating to the care of deceased patientComplaint or concerns relating to the care of deceased patientCase subject to an Inquest/Cases reported to the CoronerMental Health DeathDeath in which Duty of Candour process was in place (where the subject matter is related to the patient’s death)
Actions Taken(identify person responsible for action and date action to be completed (SMART))
Action Required Action by date Person responsible Action status
Page 31 of 3221 Mortality Review Update.docxOverall Page 203 of 218

32Page 32 of 3221 Mortality Review Update.docx
Overall Page 204 of 218

Summary Report from Quality People CommitteeReport To: BoardDate: Thursday 25 January 2018Name of Reporting Committee / Group: Quality People CommitteeDate of Meeting: Monday 15 January 2018Presenter: Kaye Burnett, Non-Executive DirectorAuthor: Deborah Brennan, Legal Services Manager
This paper is for Assurance
Key Issues discussed at meeting: Board Assurance Framework Reference and Level of Assurance Agreed
16/18 Staffing for Quality and Agency Spend Report - an update was provided on the inpatient staffing levels and the Committee were advised that additional beds had been opened in response to seasonal pressures. Further updates were provided on other staffing within the Trust; performance against agency spend and the Carter 90 day rapid improvement programme.
The Committee recognised the good performance against agency spend and the improved position on GP spend on Locums.
7/18 Staff Story – the staff member who had previously worked as a Housekeeper at Bolsover Hospital attended to present her story and share her experience of moving into a new role within the Finance Team, which she is enjoying and feels supported by her new Team.
She advised that when the ward closed, she and her colleagues were moved to the ward at Clay Cross Hospital whilst other job opportunities could be offered. She advised the Committee that she did not feel supported throughout the period from the ward closing to finding alternative employment; she found the interview process very difficult; staff were not consulted appropriately after the move and training to try and gain new skills was not available in a timely manner. She also advised that within an administration role, which is Monday to Friday, she doesn’t get the weekend and bank holiday enhancements and so now has to work more hours to earn the same pay as she did previously.
Significant Assurance2.1, 3.3
Limited Assurance2.1, 2.6
Page 1 of 422 QPC Summary Report.docxOverall Page 205 of 218

A detailed discussion took place about what the Trust could learn from this.
20/18 Strategic Workforce Development and Education Group Summary Report – the Committee were informed that membership of the group had been changed, the format had been reviewed and Terms of Reference revised. The Committee questioned the rationale for items which had been given Significant Assurance by the Group when QPC were documenting the same issues as Limited Assurance.
9/18 BAF Quarterly Review – an update was presented on the BAF for Quarter 3, 2017/18.
The Committee considered the risks, discussed the scoring and gaps and delegated authority back to the People and Organisational Effectiveness Team to review.
10/18 Strategic Workforce ReportNational and Regional
1. The NHS Workforce Strategy - Facing the Facts, Shaping the Future.
2. Nursing Associates – Next Steps. DCHS has been one of the pilot sites and we have eight trainees and plan to increase this to a further ten in March 2018.
Local3. People and Organisational Effectiveness – Joint working
with DHCT4. Better Care Closer to Home (BCCTH) – 381 staff will be
impacted.
The Committee discussed the report and were advised that the contract for the Discharge Support Service in the South of the County was coming to an end.
11/18 Addressing Workforce Supply Challenges – an update was provided on the following:
1. A daily ‘Agency watch’2. Re-introduction of the responsive bank3. Bank incentives – these were put in place again for
winter 17/18, however, five complaints have been received from substantive staff who worked over the Christmas period but did not get the additional enhancements. This will be discussed further at the January Staff Forum.
4. Other options aimed at increasing retention.
12/18 Staff Engagement and Culture - the Committee were updated on staff engagement, culture and supporting our
Limited Assurance
Significant Assurance 4.3
Significant Assurance2.1 – 2.6
Significant Assurance1.3, 2.1, 2.5, 4.2
Significant Assurance2.3 – 2.6
Page 2 of 422 QPC Summary Report.docxOverall Page 206 of 218

workforce through change and discussed the following:Bullying and Harassment – a deep dive has been carried out to analyse the data in order for plans to be put in place to eradicate this within DCHS.
NHS Staff Survey – from the results released to date it shows that some scores where improvement was made last year have now gone back down to 2015 figures.
Working Together through Change – a new guide has been introduced for staff and managers who are going through or leading changes at work. This is split into the pre, during and post stages of change.
14/18 People Performance Report – the Committee discussed the report and expressed concern regarding the Health Wellbeing and Inclusion indicators and in particular their high sickness figure. The issue of low training and appraisal compliance was also debated.
15/18 Health and Safety Update - the Committee were advised that near miss reporting continues to increase, which is a positive sign. In addition, the topics with significant incident numbers continue to be violence/aggression, lifting/handling, slips/trips/falls, needlestick injuries and contact with hazard.
In response to the needlestick injuries a working group has been set up, with operational representation, to review the incidents and produce an action plan.
18/18 Equality, Diversity and Inclusion Leadership Forum - the Annual Review was presented. Concern was expressed regarding the high number of people who hadn’t attended the Forum and the Committee were advised that the meeting structure has been reviewed and changes implemented.
Healthcare for All is to be included in the Annual Review.
19/18 Staff Partnership Committee Summary Report - the Committee took Significant Assurance from the report.
21/18 Staff Health Wellbeing and Safety Group Summary Report - the Committee were provided with an update on the Occupational Health Report section. A physiotherapy room is not now going to be provided at Walton Hospital, physiotherapy suites across the Trust will be utilised instead.
Concern was expressed regarding the high number of people who had not attended the Group. Membership is to be reviewed.
Significant Assurance2.1 – 2.5
Significant Assurance2.3
Significant Assurance1.4, 2.5, 4.2
Significant Assurance
Significant Assurance
Page 3 of 422 QPC Summary Report.docxOverall Page 207 of 218

Policies Approved
The Committee approved: HRP19 Organisational Change Policy
The Committee agreed to extend the renewal date until May 2018 for:HRP36 Equality Diversity and Inclusion PolicyGD28 Agenda for Change Collective Agreement of Local Arrangements Handbook
Issues to be escalated to Board or a CommitteeNone.
Page 4 of 422 QPC Summary Report.docxOverall Page 208 of 218

Summary Report from Quality Business CommitteeReport To: Trust BoardDate: Thursday 25 January 2018Name of Reporting Committee / Group: Quality Business CommitteeDate of Meeting: Wednesday 17th January 2018Presenter: Ian Lichfield, Non-Executive Director
Author: Andrea Graham, Corporate Governance Manager
This paper is for Assurance
Key Issues discussed at meeting: Board Assurance Framework Reference and Level of Assurance Agreed
8/18 - Board Assurance Framework Quarterly Review
The Committee discussed:
3.13 (Stranded costs)CS explained the risk relates to costs going forward mostly as a result of the Tender position in a number of services which is not yet known. The Committee will be updated in May 2018 as to the position of the Tenders which will then help inform the risk.
The Q3 risk score should be L3 X C4 with a target score of L2xC4
Significant Assurance 4.3
28/18 Fire Safety Compliance The Committee received the 360 Internal Audit Report of
fire safety commissioned after the Grenfell fire incident which provided Significant Assurance to the Trust. The Commtitee note that report covered fire safety proceses more generally
The Committee agreed the actions identified as part of that report would be monitored by the Audit and Assurance Committee
The Commtitee agreed it was a good opportunity to look at all of DCHS estates and to identify what fire risks have been identified, if any, and what the status of those risk assessments is.
Limited Assurance 3.5, 3.6
Page 1 of 423 QBC Summary Report.docxOverall Page 209 of 218

12/18 STP Financial Update 2018/19 The Committee noted QIPP/CIP requirement for 2018/19
to provide the financial context in which the Trust will operate in 2018/19.
The Committee agreed that there will be a lot of challenge to the system next year to be able to balance
Paper for Information
13/18 Operational Plan 2018/19 Including the Financial plan
The report highlighted The need to refresh the operational plan in light of the
changing financial landscape The National context The next steps including Governor Involvement
The Committee also received an update on the progress being made in developing a robust and realistic financial plan. Plans would be further refined in the next few weeks, taking into account planning guidance once this was issued.
Both the Operational Plan and Financial Plan would be presented to the Board in March 2018.
Significant Assurance3.1, 3.2, 3.3, 3.6, 3.7, 3.8, 3.12
17/18 SQIP Plan 2018/19
The Committee discussed the SQIP Plan for 2018/19 which included
Forecast requirements Approach to Efficiencies Opportunities list with indicative figures Commissioner QIPP Next steps
The Committee noted the challenge in the plan and the work that was required over the next few weeks to develop a fully costed plan
The Committee discussed the change in approach required to deliver efficiencies in future years through transformation and commercial opportunities. It was agreed that this would be discussed in more detail at the Board Development session in February 2018
Signficant Assurance 3.1, 3.7
19/18 - Transformation Update
The Committee discussed Delayed Transfers of Care (DToC) and the current number of delays in the system together with the reasons for those delays.
Significant Assurance 3.7, 3.9
Page 2 of 423 QBC Summary Report.docxOverall Page 210 of 218

The Committee noted the reduction of delays but acknowledged there is more work to do
The Committee discussed an update on the Outstanding Way work, and noted the progress being made
22/18 Procurement Transformation Plan including use of future operating model
The Committee received an update on the Future Operating Model for procurement, and how the Trust was preparing for these changes
The Trust reviewed current performance against the Procurement Transformation Plan, and noted that most KPIs were on track. It was noted that the procurement savings target for the year would not deliver against plan, but would deliver recurrently on a full year basis.
The Committee discussed the difficulty in determining the level of saving for services which go out to Tender
Signficant Assurance 3.7
27/18 - Reference Costs 2016/17 The Commtitee received the final reference cost results for
2016/17 which showed The Trusts’ Reference Costs Index (RCI) for 2016/17 was 101, a decrease from the 2015/16 RCI of 111.
The Committee agreed the reference costs provide useful information to start a discussion with services around variation
Paper for Information
24 /18 - Finance Report M9
The Committee noted the Financial Position at Month 9. The Trust is forecasting that it will meet all its statutory
financial duties for the year.
Significant Assurance 3.7, 3.8
25/18 - Treasury Management Report M9 Significant Assurance 3.7
9/18 - Performance Report Paper received for Information
10/ 18 Estates and Facilities Performance Indicators 2017/18 Paper received for Information
15/18 Estates Strategy 2018 – 2020 Paper for Information
16/18 Draft Capital Programme 2018/19 Paper for Information
30/18 - Plan Delivery Group Summary Report Signficant Assurance 3.7
Page 3 of 423 QBC Summary Report.docxOverall Page 211 of 218

31/18 - Capital & Estates Programme Group Signficant Assurance 3.5, 3.6, 3.7, 3.8, 3.9, 3.10
32/18 - Informatics Summary Report Significant Assurance 3.9, 4.5
34/18 Forward Agenda Paper for Decision 23/18 Informatics Strategy Bi-Monthly Update Signficant Assurance
3.9, 4.5
Policies Approved
Issues to be escalated to Board or a Committee
Page 4 of 423 QBC Summary Report.docxOverall Page 212 of 218

Summary Report from Council of GovernorsReport To: Board
Date: 10 January 2018
Name of Reporting Committee / Group: Council of Governors
Date of Meeting: 25 January 2018
Presenter: Prem Singh, Chair
Author: Nicola Erin Walker, Governance and Membership Officer
Key Issues discussed at meeting: Board Assurance Framework Reference and Level of Assurance Agreed
07/18 Patient Story – the story represents the benefits of Fenton Ward in Buxton providing a Blood Transfusion Service to the local community, resulting in better patient experiences
The Council of Governors discussed: The risk of not having a Service Level Agreement in place for the
IV service The impact on resources if service needs increased Positive story illustrating how we respond to patient needs and
requests resulting in better patient experience.
Paper for Information
09/18 Patient Experience 2017/18 Quarter 2 Report – highlights included: Improved response rate to complaints within 40 working days
timeframe Successful annual takeover day in school nursing Continued promotion of Caring for Carers 98% of People would recommend our services Improvements in Integrated Sexual Health Services
Paper for Information
Page 1 of 425 CoG Summary Report Board.docxOverall Page 213 of 218

10/18 Quality and Performance Report – highlights included: DCHS continue to meet the key performance indicators and remain
green rated by NHSI as part of their quarterly Quality monitoring and surveillance
No red ratings as part of the Single Oversight Framework and fully compliant with regulators
Big 9 – Red ratings Insulin Safety e-learning which is due in part to difficulties with the e-
learning module, however will achieve target by year end. Continued work undertaken to support the identification of carers
within operational services Delayed Transfer of Care (DTOC) has significantly reduced. A
discussion was held in relation to the inheritance of patients already in delay due to winter pressures.
Paper for Information
15/18 Chief Executive’s Report – highlights included: Additional funding for NHS Trusts following the November 2017
Chancellor’s budget NHS Improvement Quarter 2 Performance and Finance – continuing
operational pressures within provider sectors and overall financial position
Reached agreement with commissioners on the fixing of the 2017/18 contract value
Excellent Delayed Transfer of Care work ongoing across Derbyshire with collaborative work with Derbyshire County Council to ensure people are being discharged and to the right place with appropriate package of care
Current vaccination uptake of DCHS staff marginally higher than 2016/17
Paper for Information
18/18 Associate Director of Corporate Governance/TrustSecretary’s Report Confirmation that the 2018 AMM will take place on the 12/09/18. Community Week scheduled for July 2018 to coincide with
Celebrating 70 years of the NHS DCHS has commissioned Deliotte to commence a Well-Led Review
in January 2018, this will include a focus group with which are to be scheduled
Announcement of the nominations stage for the Deputy Lead Governor role.
Paper for Information
11/18 Quality Business Committee Annual Report
The Council reviewed the annual report of the Quality Business
For Information
Page 2 of 425 CoG Summary Report Board.docxOverall Page 214 of 218

Committee as part of their role in holding the Non-Executive Directors to account.
The Council noted this is the first time they have received full annual reports from the Quality Committees which provided detail of the work undertaken by the Committees in the past 12 months.
The report covers 3 keys elements; strategy, performance and delivery and performance and governance
Governors asked a number of probing questions of the report including how the public know they are getting value for money, How the Trust deals with Winder Pressures and how the Quality Committees work together to achieve the big 9.
The Council noted the area of focus for the next 12 months including financial planning, driving efficiencies and overseeing the performance of the Trust
12/18 Strategy Group Annual Review The Council heard about the work of the Strategy sub group over
the last 12 months The group’s role is to oversee future service plans and how they
affect patients and staff. The Council noted the work of the sub group over the past 12
months has included; overseeing the development of the 2017-2019 Operational plan, receiving updates in respect of the progress of the Better Care Closer to Home programme and ensuring that staff were well supported, contributing to the development of strategies’ including the End of Life Care Strategy
The Council agreed that the sub group should continue in its current form as this will continue to add value to the strategic development of the organisation
For Information
13/18 Updates from Governor Groups
The Following updates were provided from Governor Groups Engagement:
Training has been provided to Council members on engagement and membership
The next meeting is due to take place on 25th January 2018
Quality: The Group received and reviewed the Patient Engagement
Quarterly Report Received an update from the Quality Service Committee by the
Non-Executive Director
Governance: Received an update from Pricewaterhouse Cooper on the
progress of external audit work Discussed Governors attending Quality Committees to observe
Verbal Updates
Page 3 of 425 CoG Summary Report Board.docxOverall Page 215 of 218

the performance of Non-Executive Directors Discussed Governor Support at Insight Visits
16/18 Operational Plan 2017/19 Planning Process and Guidance – Update
The Council noted the context in which the operational plans are being refreshed and that the PDG group will continue to oversee the development of the plans
Good progress is noted against the ten point efficiency plan
The Council noted the DCHS next steps
For Information
19/18 Governor Involvement
A Map of Governor Involvement was presented to the group to ensuring the correct balance of staff and public involvement on all activities
Report showed how the activities attended by Governors supported and informed the work of the Governor Groups and the Council of Governors
Report showed the breadth of activities which Governors were involved in over the last 12 months.
For Information
Policies Approved
None.
Issues to be escalated to Board or a Committee
None.
Page 4 of 425 CoG Summary Report Board.docxOverall Page 216 of 218

Summary Report from Mental Health Act CommitteeReport To: BoardDate: 25 January 2018Name of Reporting Committee / Group: Mental Health Act CommitteeDate of Meeting: 29 November 2017Presenter: James Reilly, Non-Executive DirectorAuthor: Suzanne Pancisi, Corporate Governance Officer
This paper is for Assurance
Key Issues discussed at meeting: Board Assurance Framework Reference and Level of Assurance Agreed
89/17 Use of Restrictive Interventions (incl Seclusion) & Update on 360 Assurance work on Terms of Reference The Committee received the report following the recent work undertaken by 360 Assurance; it was highlighted that the report includes:
Suggestions for changes to DCHS policies and guidance Confirmation that controls are in place to support staff Suggestions on how to help staff understand the definition of
restraint Recommendation that the DATIX system is used to record all
unplanned interventions
The following work is now underway: The report is being reviewed in detail A working group is being arranged to carry out
recommendations An action plan will be created and be monitored at every
meeting of this committee going forward
The Committee took significant assurance from process but limited assurance relating to outcomes due to the work still to be carried out
Significant assurance from process but limited assurance to outcomes due to the work still to be carried out4.2
88/17 Update on Mental Health Act Patients in DCHS Care including updated Associate Mental Health Act Manager Audit ChecklistThe Committee took Significant Assurance from the report and approved the updated AMHAM Audit Checklist.
Significant assurance4.2
92/17 Quarter 2 2017/18 Legal Issues ReportThe Committee took Significant Assurance from the report.
Significant assurance4.2
Page 1 of 226 MHAC Summary Report Nov 2017.docxOverall Page 217 of 218

Key Issues discussed at meeting: Board Assurance Framework Reference and Level of Assurance Agreed
86/17 Patient StoryThe Committee received the story of a young man in his mid-20s who was referred via Hardwick CCG and, following discussion with staff in the south of the county where he was known, admitted to Hillside; the following points were highlighted
Full details of the patient were not shared with Hillside prior to admission however it soon became clear that they were able to meet the complex needs of the patient. Had full details been known he would not have been accepted.
The patient assaulted staff and caused environmental damage to the ward; the door to the seclusion room was breached due to continued body barging, leading to the patient being restrained and tranquilised throughout the rest of the period he was in the unit (approximately 14 hours)
An urgent call was made to Commissioners requesting a more appropriate setting be found; the patient was eventually found an emergency bed in a psychiatric intensive care unit by staff at Hillside. The patient was in the unit for approximately 26 hours.
The police initially attended however, following the breach of the door five further 999 calls were made but the police refused to attend again. Upon transfer out of Hillside a police escort was requested by East Midlands Ambulance and was refused.
A route cause analysis (RCA) has been undertaken to be reported to the Clinical Safety Group.
The Committee noted that the details will be reported to QSC in the normal way and as a serious incident notified to the whole Board.
Paper for Information
Policies ApprovedNone
Issues to be escalated to Board or a Committee
Page 2 of 226 MHAC Summary Report Nov 2017.docxOverall Page 218 of 218