Embed Size (px)
Citation preview

Michigan Depression Outreach and Collaborative Care (M-DOCC):
Using phone-based primary care augmentation to promote recovery.
Niki Feller, MSW LifeWays Community Mental Health Mike Klinkman, MD University of Michigan/Jackson Health Network Marcia Valenstein, MD University of Michigan
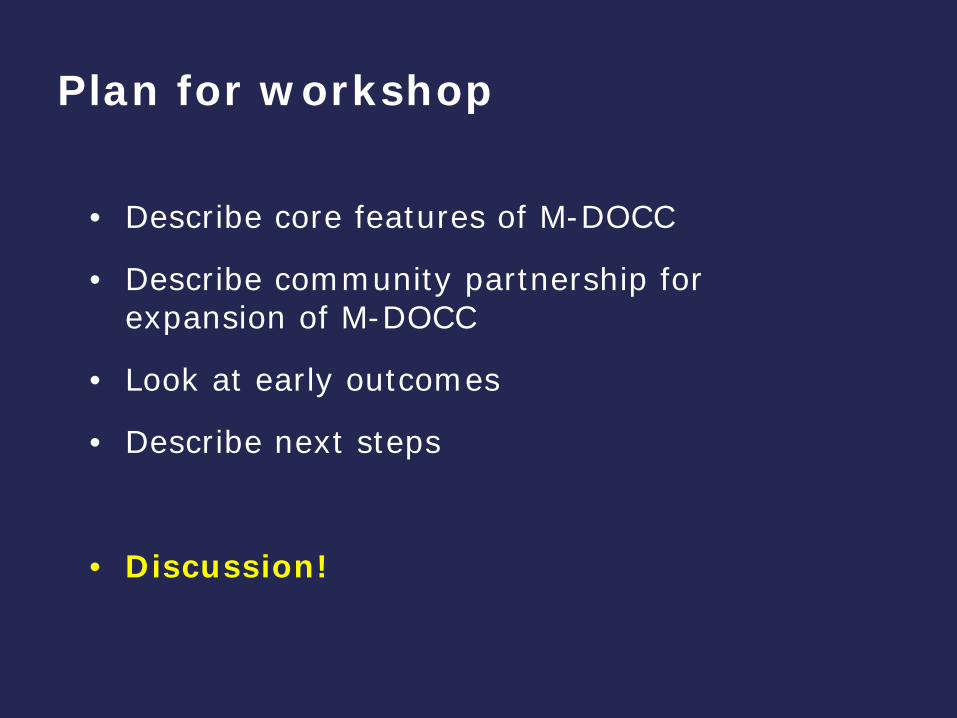
Plan for workshop
• Describe core features of M-DOCC
• Describe community partnership for expansion of M-DOCC
• Look at early outcomes
• Describe next steps
• Discussion!
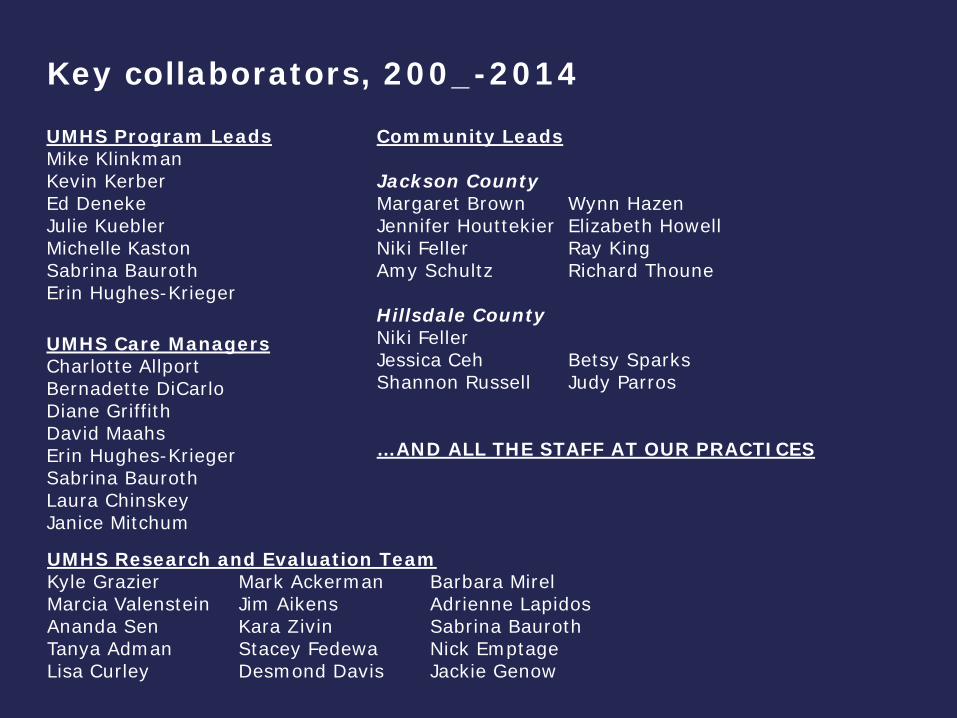
Key collaborators, 200_-2014
UMHS Program Leads Mike Klinkman Kevin Kerber Ed Deneke Julie Kuebler Michelle Kaston Sabrina Bauroth Erin Hughes-Krieger
UMHS Research and Evaluation Team Kyle Grazier Mark Ackerman Barbara Mirel Marcia Valenstein Jim Aikens Adrienne Lapidos Ananda Sen Kara Zivin Sabrina Bauroth Tanya Adman Stacey Fedewa Nick Emptage Lisa Curley Desmond Davis Jackie Genow
UMHS Care Managers Charlotte Allport Bernadette DiCarlo Diane Griffith David Maahs Erin Hughes-Krieger Sabrina Bauroth Laura Chinskey Janice Mitchum
Community Leads Jackson County Margaret Brown Wynn Hazen Jennifer Houttekier Elizabeth Howell Niki Feller Ray King Amy Schultz Richard Thoune Hillsdale County Niki Feller Jessica Ceh Betsy Sparks Shannon Russell Judy Parros …AND ALL THE STAFF AT OUR PRACTICES
Core beliefs guiding M-DOCC design
• Problems are chronic and episodic
• Comorbidity is the rule
– medical and mental health
• Complexity is the rule (biopsychosocial)
• ‘Conspiracy of silence’ in practice
– High stigma, high-effort, low payoff
• Goal – integrate behavioral health into PCMH by supporting primary care treatment

Low severity / low complexity
Moderate severity, MH or medical comorbidity
High severity / low to moderate complexity
High severity / high complexity
Tiers in the behavioral health population (proportions vary across care settings)

M-DOCC features
Hybrid of disease management / case management
Care Managers as agents of practice/physician to help keep patients in treatment and coordinate care
Links to local mental health and social services resources
Patient “activation” and self-management training
Flexible and long-term monitoring, by phone or Web
Decision support: options/resources for practices to improve screening, case-finding, treatment (“toolbox”)
CIS support: M-DOCC software application, Outcome Summary Reports (PHQ-9 plus..) posted to EMR
Tailored to fit workflow of each participating practice

What the M-DOCC care manager does:
• Assesses severity and complexity
• Provides basic education
• Works on patient self-management (goals, priorities)
• Monitors progress
• Feeds back information on clinical progress to referring clinician
• When needed, provides links to specialty mental health
• Connects patients to needed resources
• Continues monitoring after “recovery”
Differences between M-DOCC and other collaborative care programs
• Designed to support chronic problems
• We take everyone
• Less expensive per enrollee ($240/first year)
• Flexible and ongoing support
– intensity, duration, method (phone, Web)
• Secondary screening and clinician feedback built in
• Principles of support (self-management, goals, tracking) apply to medical and mental health problems

Low severity / low complexity
Moderate severity, MH or medical comorbidity
High severity / low to moderate complexity
High severity / high complexity
Referrals to M-DOCC to date (n=3500)
M-DOCC @ UMHS: population reach

% positive Level 1 screen
% “case” - Level 2 screen
Threshold for positive screen
Bipolar disorder 45% 28% 2 of 7
GAD 72% 66% 3 of 8
Panic disorder 50% 43% 3 of 9
PTSD 32% 26% 2 of 4
Substance abuse 27% 27% 1 of 2
Sleep problems 71% n/a none
% positive screens for primary care M-DOCC patients. [n=222]
21% screened positive for at least 3 comorbid MH conditions.

43.5%
52.0%49.2%
33.3% 33.9%
27.3%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
6 months 12 months 18 months
Time
Perc
enta
ge
% in remissionIntervention
% in remissionusual care
“Remission” rates: M-DOCC patients vs usual care patients
* *
*
* p<.05

Summary of core clinical outcomes • Mean PHQ scores were lower for M-DOCC patients than for
patients receiving usual care at 6, 12, and 18 months
• The proportion of M-DOCC patients in remission was significantly higher than for usual care patients at 6, 12, and 18 months
• The number-needed-to-treat (NNT) to achieve remission, compared to usual care, was 5.
• In multivariate AUC analyses, M-DOCC patients had significantly more reduction in their depressive symptom burden over the full 18 months than usual care patients after controlling for age, gender, ethnicity, baseline severity, and comorbid medical illness [p=.013].
• Enrollees had an average 35% increase in work productivity (self-reported) during their time in the program
• Net cost of the program was $0.17 PMPM Zivin et al. Int J Psychiatry Med, 39(1):1-13. 2009 Klinkman et al. Ann Fam Med ;8 :387-96. 2010

Health IT platform: M-DOCC Clinical Record
M-DOCC Clinical Record features
• Workflow management –registry, notifications, call lists, outreach
• Clinical documentation – structured clinical intake and assessment, structured clinical data, free-text care notes
• Patient education/self-management curriculum -incorporating patient-specific goals and progress tracking
• Clinical outcome assessment and tracking
• Standardized feedback to referring clinician and patient
• Secure Web interface for on-line outcome assessments
• ‘Shadow billing’ function can expand to support CM codes
• Data analytics functionality –standard or custom-designed population reports
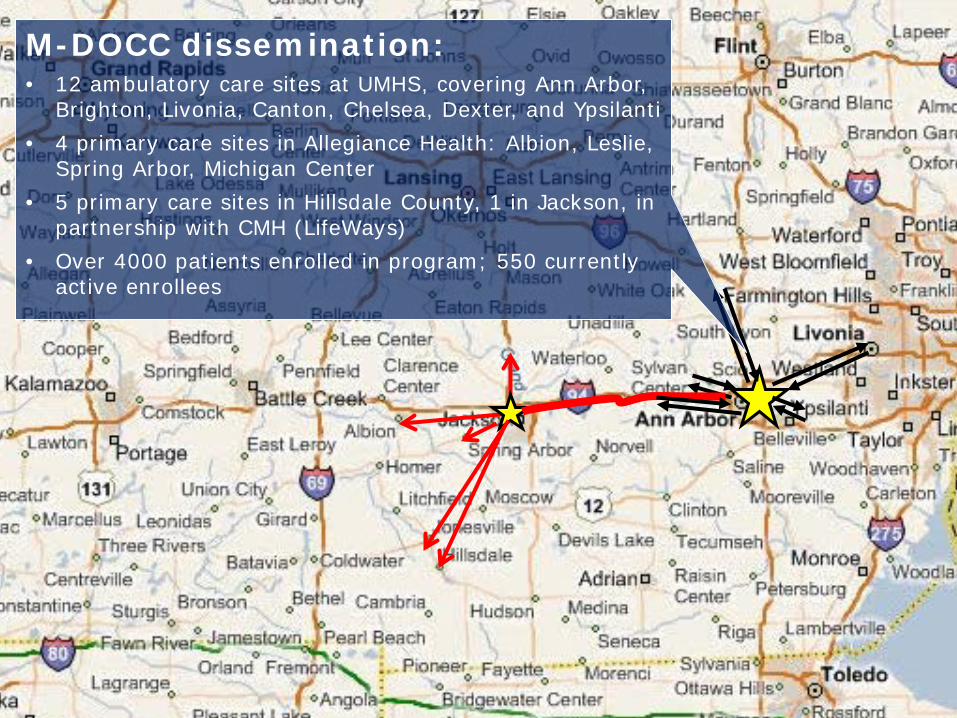
M-DOCC dissemination: • 12 ambulatory care sites at UMHS, covering Ann Arbor,
Brighton, Livonia, Canton, Chelsea, Dexter, and Ypsilanti • 4 primary care sites in Allegiance Health: Albion, Leslie,
Spring Arbor, Michigan Center • 5 primary care sites in Hillsdale County, 1 in Jackson, in
partnership with CMH (LifeWays) • Over 4000 patients enrolled in program; 550 currently
active enrollees

Community experience: Jackson and Hillsdale
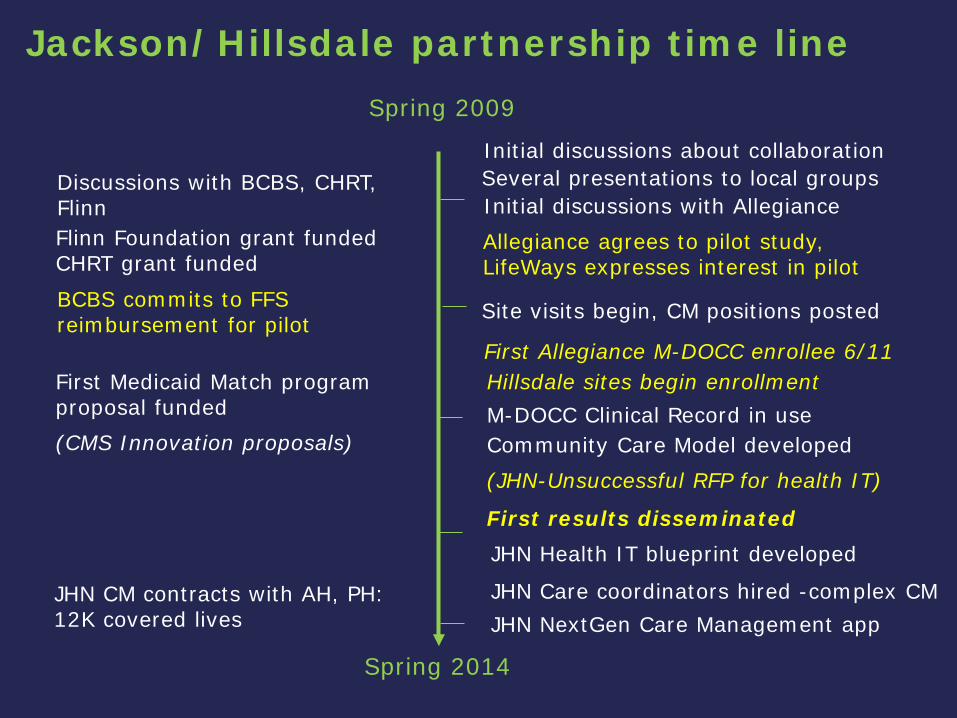
Jackson/Hillsdale partnership time line Spring 2009
Spring 2014
Initial discussions about collaboration Several presentations to local groups Initial discussions with Allegiance
Community Care Model developed
Allegiance agrees to pilot study, LifeWays expresses interest in pilot
Site visits begin, CM positions posted
Flinn Foundation grant funded CHRT grant funded
Hillsdale sites begin enrollment
(CMS Innovation proposals)
Discussions with BCBS, CHRT, Flinn
First Medicaid Match program proposal funded
First Allegiance M-DOCC enrollee 6/11
BCBS commits to FFS reimbursement for pilot
(JHN-Unsuccessful RFP for health IT)
M-DOCC Clinical Record in use
JHN Care coordinators hired -complex CM
JHN Health IT blueprint developed First results disseminated
JHN CM contracts with AH, PH: 12K covered lives JHN NextGen Care Management app

Jackson and Hillsdale expansion
• Implement Allegiance Depression Management Program in 2 sites – Spring Arbor and Leslie (later 2 more sites)
– Allegiance “Health Coach” shared between sites
• Implement LifeWays LINC program in 2 private practices in Hillsdale County (later 4 more sites)
– LifeWays Access staff member as care manager
– Focus on Medicaid, uninsured population
• Assess feasibility of implementation
• Measure clinical and economic outcomes over 6 months
• Compare to clinical outcomes from 2 Allegiance control sites
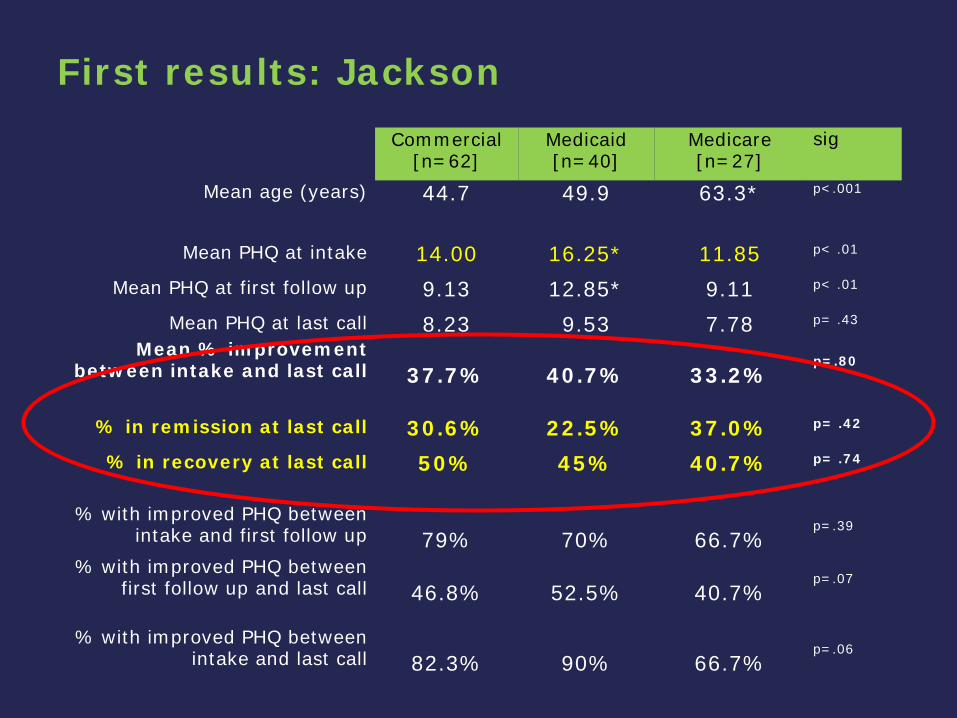
First results: Jackson Commercial
[n=62] Medicaid [n=40]
Medicare [n=27]
sig
Mean age (years) 44.7 49.9 63.3* p<.001
Mean PHQ at intake 14.00 16.25* 11.85 p< .01
Mean PHQ at first follow up 9.13 12.85* 9.11 p< .01
Mean PHQ at last call 8.23 9.53 7.78 p= .43
Mean % improvement between intake and last call
37.7%
40.7%
33.2%
p=.80
% in remission at last call 30.6% 22.5% 37.0% p= .42
% in recovery at last call 50% 45% 40.7% p= .74
% with improved PHQ between intake and first follow up
79%
70%
66.7%
p=.39
% with improved PHQ between first follow up and last call
46.8%
52.5%
40.7%
p=.07
% with improved PHQ between intake and last call
82.3%
90%
66.7%
p=.06

St Peter’s Free Clinic, Hillsdale, MI

First results: Hillsdale (short duration)
Private sites [n=27]
St Peters [n=22]
sig
Mean age (years) 50 43.1 P=.08
Mean PHQ at intake 15.15 12.45 P=.08 Mean PHQ at first follow up 12.04 10.82 ns
Mean PHQ at last call 9.37 10.00 ns Mean % improvement between
intake and last call
33.4%
18.7% ns
% in remission at last call 18.5% 18.2% ns % in recovery at last call 44.4% 31.8% ns
% with improved PHQ between
intake and first follow up
74.1%
59.1% ns
% with improved PHQ between first follow up and last call
51.9%
40.9%
ns
% with improved PHQ between intake and last call
81.5%
63.6%
ns

Low severity / low complexity
Moderate severity, MH or medical comorbidity
High severity / low to moderate complexity
High severity / high complexity
Referrals to Jackson and Hillsdale programs to date
Community program reach
NEEDED: Expanded social support Full spectrum MH backup Child and adolescent support
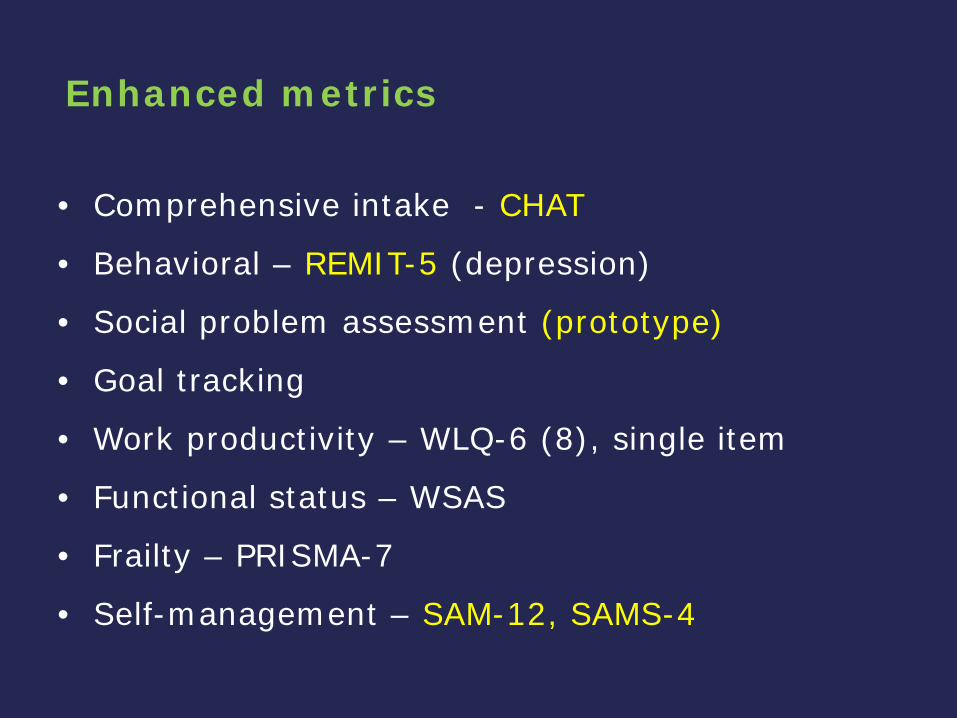
Enhanced metrics
• Comprehensive intake - CHAT
• Behavioral – REMIT-5 (depression)
• Social problem assessment (prototype)
• Goal tracking
• Work productivity – WLQ-6 (8), single item
• Functional status – WSAS
• Frailty – PRISMA-7
• Self-management – SAM-12, SAMS-4

LifeWays experience

About Jackson and Hillsdale Counties
Jackson County: Population – 160,369
Hillsdale County:
Population – 46,101
CMH serves approximately 8500
individuals in these two counties.
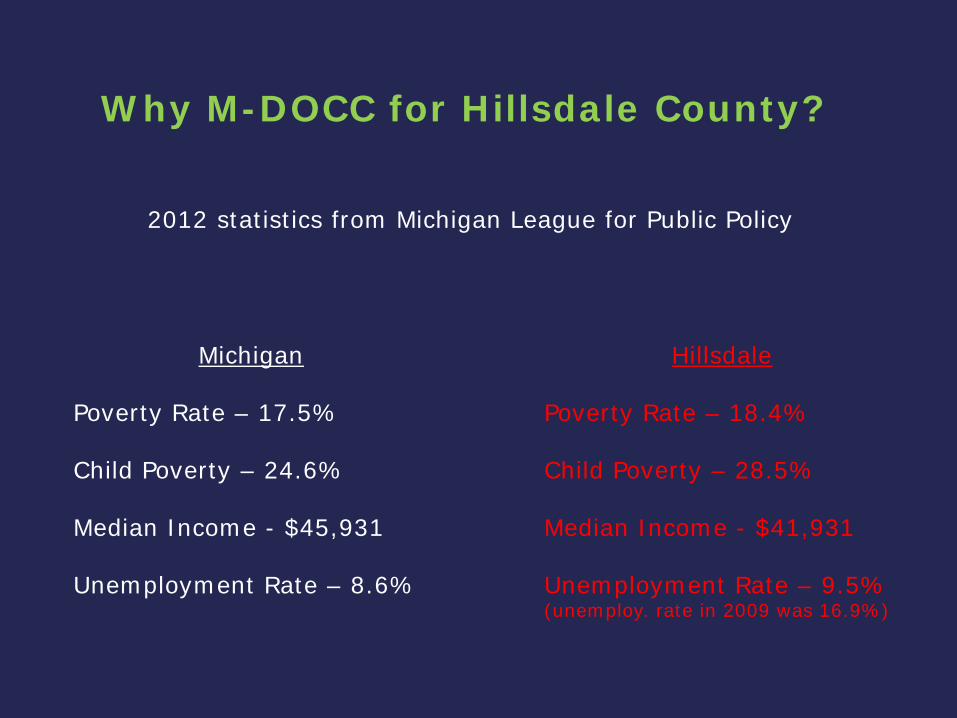
Why M-DOCC for Hillsdale County?
2012 statistics from Michigan League for Public Policy
Michigan
Poverty Rate – 17.5% Child Poverty – 24.6% Median Income - $45,931 Unemployment Rate – 8.6%
Hillsdale
Poverty Rate – 18.4% Child Poverty – 28.5% Median Income - $41,931 Unemployment Rate – 9.5% (unemploy. rate in 2009 was 16.9%)

Government Assistance in Hillsdale County
Children receiving free or reduced school lunches
56.1%
25.9 % Of the population
received some type of
government assistance in
2012
Medicaid Eligible – 9,784
Uninsured: Age 0-17: 6.0% Ages 18-64: 19.6%

Or lack thereof …
• No Federally Qualified Health Center or Rural Health Clinic • One free clinic on Tuesday nights at St Peters Church • 1 FTE Psychiatric at CMH - .2 FTE Child Psychiatrist • No community Psychiatry

It’s All About Relationships

And Education
• CMH Funding
• CMH Priority Populations
• Support Services and Resources
• Screening for Specialty Services
Future Planning
• “Reverse” Referrals
• Stable People Back to PCP
• Ongoing Monitoring
• Psychiatric Consultation
• Fluid Movement between specialty and primary care

Panel Review: What is it? Why do it?
Panel Review
• Psychiatrist review and role
– Review panel once a week with CM
– Focus on patients not responding to treatment, complications, comorbidities
– Communication with PCP
• In-person preferred, phone okay if relationship
– Treatment suggestions
• Another diagnosis? Treatment adherence? Substance use?
Panel Review
• Patients with PHQ scores >15; >10 on multiple occasions
• Patients that concern CM – Suicidal thoughts
• 161 patients in Lifeways panel – 99 active
– 59 reviewed at some point by psych
• Indirect communication with PCP

Issues with Patients Reviewed
• Difficult psychosocial situations
– No propane/housing
– Poor adherence due to inability to pay for meds
• Alcohol use disorder
– Limited use of alcohol pharmacotherapy
• Limited psychotherapy resources
• Pts moving between Lifeways and PCPs

Potential Next Steps
• Lifeways psychiatrist takes on role
• Maintaining weekly review despite multiple roles
• Increase in-person and phone interaction with PCPs
• Lower cost psychotherapy—
– internet options

Discussion.

Macro: The implementation chasm
SUCCESS!
SUSTAINABLE PRACTICE CHANGE
Reality.
Individual clinics Atypical systems Research/dissemination Pieces of model
Diverse settings Cross-platform scaling Tailored implementation Comprehensive IT and workflow integration
Venture capital ($ and human) Visionary leadership Compelling case for change Comprehensive plan /model

Our contact information:
Niki Feller [email protected] Mike Klinkman [email protected] Marcia Valenstein [email protected]