-
7/28/2019 Depression in Neurological Disorders
1/46
Dr pavan kumar kadiyala
Depression in Neurological
disorders
-
7/28/2019 Depression in Neurological Disorders
2/46
Introduction
Depression is a relatively common psychiatriccomorbidity of most
neurological disorders, with
prevalence rates ranging between 20 and 50%
among patients with stroke, multiple sclerosis,
epilepsy, Parkinsons disease and dementia.
Depression is an independent predictor of poor
quality of life in these patients and
has a negative impact on the response totreatment, course and
recovery of neurological
deficits.
-
7/28/2019 Depression in Neurological Disorders
3/46
-
7/28/2019 Depression in Neurological Disorders
4/46
Comorbid depressive disorders in neurologicpatients can be
indistinguishable to the primary
mood disorders.
The great overlap of medical and psychiatric
symptoms in depression and neurologic disorders
may lead to both false-positive and false-negative
diagnoses of depression.
Patient with comorbid condition have lower
response rate and /or a longer time to response,
greater reports of side effect early in treatment
and greater likely hood of dropping out.
-
7/28/2019 Depression in Neurological Disorders
5/46
Neurobiology
-
7/28/2019 Depression in Neurological Disorders
6/46
-
7/28/2019 Depression in Neurological Disorders
7/46
depression since long have been suggested asdysfunction of basic
CNS processes.
With respect to cortical function, depressioninvolves multiple
disturbances of information
processing.
Clinical phenomenology
-
7/28/2019 Depression in Neurological Disorders
8/46
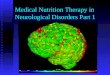
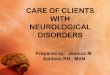
Four brain regions in the regulation of normalemotions:
The PFC,
The anterior cingulate, The hippocampus, and
The amygdala
Emotional Processing and the Brain
-
7/28/2019 Depression in Neurological Disorders
9/46
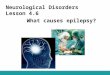
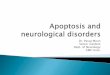
neurocognitivechanges (poor
concentration and
abstraction)
Anhedonia anddecreased
consummatorybehavior (appetite
and libido)
dysfunction involving thehippocampus, prefrontal
cortex (PFC), and other
limbic structures
neural circuits involved in the
anticipation and
consummation of rewards,
which involve the thalamus,
hypothalamus, nucleus
accumbens, and PFC.
-
7/28/2019 Depression in Neurological Disorders
10/46
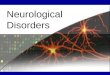
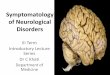
psychomotordisturbances (retardation,pacing and frequent
posturalshifts, stereotypical behaviors
of furrowed brow, hair pulling,biting at the lips or nail
beds,and compulsive scratching
circadian rhythms(insomnia, hypersomnolence,diurnal mood
variation)
dysfunction ofsubcortical circuitsconnecting the thalamus,basal
ganglia, andstriatum
dysregulation of thalamicnuclei and the brainstem
-
7/28/2019 Depression in Neurological Disorders
11/46
Neuroimaging
most consistent abnormality - increasedfrequency of abnormal
hyperintensities in
subcortical regions, such as periventricular
regions, the basal ganglia, and the thalamus
Structural brain changes:
reduced hippocampal and caudate volumes
suggesting more focal defects in relevant
neurobehavioral systems
Functional changes:
hypoperfusion in frontal (left), temporal and
parietal areas
Reduced blood flow and metabolism in
-
7/28/2019 Depression in Neurological Disorders
12/46
Neurotransmitters:
Monoamine theory - reduced monoamine function
ie, 5HT, NE, DA
Endocrine factors:
Stress - Increased HPA activity, hypercortisolemia
Decreased brain-derived neurotrophic growth factor
Thyroid dysfunction in 5-10%
Blunted GH and prolactin response to serotonin
agonists
-
7/28/2019 Depression in Neurological Disorders
13/46
Medical causes of depression
Neurological: CVA, epilepsy, PD, dementia, MS,tumor,
Huntingtons, head injury
Infectious: HIV, EBV, Brucellosis
Endocrine and Metabolic: hypothyroidism,
Cushings, Addisons, parathyroid disease,
porphyria, Vit B12 and folate deficiency
Cardiac disease: MI, CCF
-
7/28/2019 Depression in Neurological Disorders
14/46
Connective tissue disorders: SLE,RA
Cancers
Medications: analgesics, antihypertensives, l-
dopa, steroids, OCP, cytotoxins, cimetidine,
salbutamol
Drugs and toxins: alcohol, benzodiazepines,
cannabis, cocaine, opioids
-
7/28/2019 Depression in Neurological Disorders
15/46
Depression and headache
Major depression is present in nearly 18% ofmigraineurs compared
to 7.4% of the general
population.
Headache, depression, and other
neuropsychological comorbidities, are
fundamentally neurophysiological disorders.
Patients with depression are more vulnerable to
general pain and traumatic pain sequelae,
particularly head and neck pain, than the general
public (OReardon 2007).
-
7/28/2019 Depression in Neurological Disorders
16/46
both depression and headache share certainneurophysiological
commonalities, including
anatomical relationships, possibly in the
prefrontal cortex.
So failure to effectively treat depression may
prevent the successful control of headache
Some medications used to treat headache
patients may paradoxically worsen or contribute
significantly to depression, and vice versa.
-
7/28/2019 Depression in Neurological Disorders
17/46
preventive agents topiramate, valproic acid, betablockers,
depression may be a side effect of these
medications.
There may be a secondary improvement,
however, in mood, by reducing the headache
itself.
For severe intractable cases, lithium and MAOinhibitors, such as
phenelzine, may have an
important role.
Recent reports suggest that transcranial magnetic
stimulation (TMS) may provide treatment for
-
7/28/2019 Depression in Neurological Disorders
18/46
Targeted mechanisms involve the suprachiasmicnucleus of the
hypothalamus and the
neurohormone melatonin, an anti-inflammatory
neuromodulating substance.
These may be key factors in both the sleep andheadache phenomena
and perhaps depression
as well.
TCAs were recognized as useful for both chronic
pain (including headache) and depression.
Amitriptyline, nortriptyline, doxepin.
weight gain and anticholinergic effects.
efficacy of fluoxetine and venlafaxine for migraine
-
7/28/2019 Depression in Neurological Disorders
19/46
DEPRESSION IN PARKINSONS
DISEASE
Diagnosis and management of depression inParkinsons disease (PD)
is important for two
main reasons:
firstly, depression is common in PD and
secondly depression causes significant morbidity
in terms of quality of life, disability (measured by
ADL), and carer stress. This effect is independent
from the effect of motor disability.
-
7/28/2019 Depression in Neurological Disorders
20/46
Epidemiology
prevalence of depression in PD is probably
between 2045%
male=female
prevalence of depression relative to the course of
PD is biphasic, with
a peak early in the illness (possibly related to
increased life events) and another gradual increase as the
illness reaches
its latter stages
Depressive illness also appears to be more
common in those people with more rapidly
-
7/28/2019 Depression in Neurological Disorders
21/46
Studies - psychiatric symptoms (particularlydepression and
anxiety) may precede motor
symptoms of PD by a number of years (as often
they do in Huntingtons disease).
The average time between onset of depressivesymptoms and motor
symptoms was around 6
years, correlates well with PET studies
suggesting that the
onset of the disease process may predate motor
symptoms by the same time period
-
7/28/2019 Depression in Neurological Disorders
22/46
Diagnosis of depression in
Parkinsons disease
difficult because of the clinical overlap between thetwo
syndromes.
Symptoms that are common to both depression andidiopathic
Parkinsons disease include motor slowing,bradyphrenia, sleep and
appetite disturbance, weightloss, loss of interest and
concentration, and reducedlibido.
The body language of depression looks similar tothat of PD at
first glance.
The patient often appears hunched with a lack of anobvious
affective response and spontaneity (thepatient with PD may well
have an intact affectiveresponse but may not be able effectively to
translatethis into motor phenomena).
-
7/28/2019 Depression in Neurological Disorders
23/46
Symptoms that may help in the diagnosis ofdepression in people
with PD include;
pervasive low mood with diurnal variation (for at
least two weeks)
early morning wakening
pessimistic thoughts about the world, themselves,
and the future (out of context with their level of
disability or their previous attribution style) suicidal
ideation.
-
7/28/2019 Depression in Neurological Disorders
24/46
Low mood can also occur as a consequence ofmedications used to
treat Parkinsons disease or
other conditions (such as hypertension).
There is transient dysphoria during surgery for PD
following pallidotomy and DBS(esp stimulation aroundsubthalamic
N).
Beck depression inventory is not a useful rating scale
in PD. The Montgomery and Asberg depression rating
scale (MADRS) and the Hamilton depression scale(HAM-D) have
performed better.
TCAs and SSRIs as Rx
ECT- motor symptoms of PD may be temporarily
alleviated by a but that does not change the overallro nosis of
the illness.
-
7/28/2019 Depression in Neurological Disorders
25/46
DEPRESSION IN MULTIPLE
SCLEROSIS
Depressed mood also contributes significantly toreductions in
quality of life for people with MS.
depressogenic MS lesion - right temporallesions.
prevalence - 25%. Rates of depression are higher in nursing
home
settings and younger people with MS were morelikely to be
depressed than their older
counterparts with similar levels of physicaldisability.
Like Parkinsons disease, vegetative or somaticsymptoms do not
tend to be good diagnosticdiscriminators for depression in MS.
-
7/28/2019 Depression in Neurological Disorders
26/46
disinterest in sex was uniquely related todepression in MS
(rather than fatigue or physical
disability).
Pervasive mood change Diurnal variation in
mood Becks cognitive triad Mood congruentpsychotic symptoms
Suicidal ideation A change
in function not related to physical disability
All the anti-spasticity drugs associated with low
mood (including baclofen, dantrolene, and
tizanidine) and following the abrupt
discontinuation of baclofen and other anti-
spasticity drugs
-
7/28/2019 Depression in Neurological Disorders
27/46
Suicidal behaviour in MS
15% of the deaths were recorded as suicide.
being male, young age of onset, previous history
of depression, social isolation, and substance
abuse
controversy over whether interferon treatment is a
risk factor for depression in MS.
-
7/28/2019 Depression in Neurological Disorders
28/46
Treatment
SSRIs (sertraline and fluoxetine).
Mild to moderate forms of depression - CBT.
ECT- MS symptoms worsened in around 20%
cases.
-
7/28/2019 Depression in Neurological Disorders
29/46
DEPRESSION AND STROKE Pathophysiology sudden, multiple loss
events (loss of physical
function, employment, change in social or marital
status)
lose the neurological capacity to process these lossevents
Affect areas of the brain directly involved in control of
mood.
Peak incidence of depression is between six monthsand two years
post-stroke and
point prevalence for depression varies between 10
34% according to studies.
younger, more often white and less likely to be alive
-
7/28/2019 Depression in Neurological Disorders
30/46
clear relation between proximity of the lesion tothe left
frontal pole and depression, especially in
the first few months after stroke.
a brain infarct affecting the pallidum was a strong
predictive factor for post-stroke depression
-
7/28/2019 Depression in Neurological Disorders
31/46
Diagnosis Communication difficulties, impairments of facial
and
emotional expression, and disturbance in vegetativefunctions
make difficult.
A deterioration in function over a few days or weeksfollowing a
period of improvement is one clinical clue for the
development of depression. Pathological emotionalism is
relatively common after stroke,
affecting up to 20% of patients in 1st 6 months post-strokebut
tending to improve over next year. treated withantidepressant
medication and levodopa
Extreme abulia can sometimes be mistaken for depressionand can
be related to either frontal (especially left frontal)and
diencephalic lesions.
The patient may appear to be extremely retarded but mayfunction
at a high level within a structured environment.
Dopamine agonists, such as bromocriptine treat abulia.
-
7/28/2019 Depression in Neurological Disorders
32/46
Rating scales for depression post-
stroke
On acute hospital wards, the signs ofdepression scale
In rehabilitation settings, the best validated scales
were the hospital anxiety and depression scale
(HADS) and the general health questionnaire-12(GHQ-12).
In the community, HADS and GHQ-12 are
recommended
-
7/28/2019 Depression in Neurological Disorders
33/46
psychotherapy better than medications inpreventing of depression
post-stroke
Treatment trials have indicated that SSRI
treatments (citalopram, sertraline) and other
antidepressants (reboxetine) are superior toplacebo
TMS
-
7/28/2019 Depression in Neurological Disorders
34/46
Depression and Dementia
depression can be an early sign of dementia
-
7/28/2019 Depression in Neurological Disorders
35/46
Some depressive patients show cognitive abnormalities. These
can
be
due to personal predisposition, activation of hysterical
mechanisms, cerebral metabolic abnormalities, changes in level
of
arousal and as a part of the general of psychomotor
retardation.
-
7/28/2019 Depression in Neurological Disorders
36/46
The ageing process affecting the brain such as the neuronal
loss
may combine with the neurochemical changes in depression and
lead to cognitive failure.
It is these chemical and physiological alternationswhich are
responsible for both depression and the cognitive
changes. Therefore, this syndrome should be considered to be
organic in origin and should be labeled as dementia of
depression
rather than
pseudodementia
-
7/28/2019 Depression in Neurological Disorders
37/46
Dothiepin is an effective antidepressant withanxiolytic action
and has lesser anticholinergic
side-effects.
Hypnotics and tranquilizers can be used on an
SOS basis, but antidepressants should beadministered daily for
several weeks or months
-
7/28/2019 Depression in Neurological Disorders
38/46
Epilepsy and Depression
depression is a frequent complication of epilepsy. can be
related ictally or post ictally
Ictal depression occurs with temporal lobe seizures,during
status epilepticus, petit mal status and partialseizure status.
Fears and depression are the
commonest ictal experiences. Interictal depressions are common
in patients with
late onset epilepsy, in children, and in complex
partialseizures.
The longer the duration of epilepsy the more sever
the depression Depression is more closely related totemporal
lobe epilepsy than to other types of epilepsy
Laterality of lesion responsible for depressionreported is
controversial as both dominanthemispheric as well as non-dominant
hemispheric
lesions have been involved.
-
7/28/2019 Depression in Neurological Disorders
39/46
The onset and subsidence of depression tends to besudden and the
mood disorder fluctuates markedly.
Paranoid features frequently accompany thedepression as well as
depresonalisation, anxiety andhostility.
There may be family history of depression in morethan 50% of
cases.
The suicidal rate is higher among epileptics than inthe general
population. Temporal lobe epileptics carry
the greatest risk. The implicated biochemical abnormalities
are,
disorders of noradrenaline, dopamine, serotonin,
andgamma-aminobutyric acid metabolism andmalfunctioning of the
hypothalamic, pituitary axis and
disturbances in folic acid metabolism
-
7/28/2019 Depression in Neurological Disorders
40/46
Patients receiving carbamazepine are the leastdepressed while
patients receiving phenobarbitoneare the most depressed.
The level of psychopathology correlates positivelywith
phenobarbitone and negatively with
carbamazepine Low foliate levels in serum, RBCs and CSF have
been demonstrated in epileptics with mentalsymptoms including
depression.
Folic acid supplements do not influence the onset of
prognosis of the depressive state. However S-adenosylmethionine
which is involved in
folate metabolism seems to have antidepressantproperties.
The folic acid metabolism is least affected by
carbamazepine and sodium valproate.
-
7/28/2019 Depression in Neurological Disorders
41/46
Treatment
need a higher dose of antidepressants All non-MAOI and some MAOI
antidepressants lower
the sedation threshold and can potentially aggravate
clinical seizures
Therapeutic doses of antidepressants can do this inpredisposed
individuals who have a family history of
epilepsy, existing brain damage or previous history of
ECT.
Patients receiving anticonvulsants demonstrate
lowerantidepressant level than patients who are not
receiving anticonvulsants.
Electroconvulsive therapy is not contraindicated in
epilepsy and can be life-saving in suicidal epileptics
-
7/28/2019 Depression in Neurological Disorders
42/46
Cerebral Tumors and Depression
Frontal and temporal locations of tumour areassociated with the
greatest frequency of both
depression and personality disturbances.
The frontal location is characterized by irritability,
depression or euphoria, and apathy. Irritability is afrequent
presenting symptom
Parietal lobe tumours are less likely to produce
mental changes
-
7/28/2019 Depression in Neurological Disorders
43/46
Headtrauma and Depression
Depression is the most common emotionalreaction to head
injury
"reactive" depression- symptoms may last for
many months after the injury.
Chances of death by suicide is considerably
increased after head injury, accounting for 14% of
all deaths.
Significantly, a change in the character of the
person, after the injury has been observed in 40%
of patients who committed suicide.
-
7/28/2019 Depression in Neurological Disorders
44/46
Huntington's Chorea and Depression
Psychiatric changes may be present for sometime before the onset
of involuntary movements
or intellectual impairment
The depression can be severe in the early stages
when the patient still retains insight. Later on themood becomes
apathetic, self neglect and
euphoria replace the depression.
The depression responds to antidepressant drugs
and electroconvulsive therapy.
S t i L E th t d
-
7/28/2019 Depression in Neurological Disorders
45/46
Systemic Lupus Erythematosus and
Depression
The functional psychoses in SLE can bedepressive, schizophrenia
like, or rarely, manic.
Steroids which are the mainstay of treatment in
SLE can precipitate or aggravate the mental
symptoms. These may respond to a reduction indose of the
steroids.
Immunosuppresive drugs like cylcophosphamide
and azathioprine can be tried instead of steroids.
Antidepressants and E.C.T. can be used for
treating the depression.
-
7/28/2019 Depression in Neurological Disorders
46/46
Thank u