Embed Size (px)
Citation preview

Depressed heart rate response to vasodilator stress for myocardial SPECTpredicts mortality in patients after myocardial infarction
Young Hwan Kim1, Kyung-Han Lee1,2, Hong Joo Chang1, Eun Jeong Lee1,Hyun Woo Chung1, Joon Young Choi1, Yong Choi1, Yearn Seong Choe1,Sang Hoon Lee2 & Byung-Tae Kim1
1Departments of Nuclear medicine, and 2Cardiovascular Institute, Sungkyunkwan University School ofMedicine, Samsung Medical Center, 135-710, Seoul, Republic of Korea
Received 3 May 2005; accepted in revised form 2 December 2005
Key words: dipyridamole, heart rate response, myocardial infarction, mortality
Abstract
Background: As heart rate (HR) response during vasodilator stress myocardial perfusion studies can be amarker of HR variability, we investigated its prognostic value in patients after myocardial infarction (MI).Methods: Subjects were 147 survivors of MI who underwent vasodilator stress thallium-201 scintigraphy.HR response was measured as peak to basal (P/B) ratios during vasodilator infusion. End points forsurvival analysis were all-cause deaths, non-fatal recurrent MI, and soft events. Results: HR response wassignificantly depressed in the post-MI patients compared to controls (p<0.0005). HR response correlatedto LVEF (r=0.37, p<0.0001) and summed stress scores (r=)0.18, p<0.05), but not with antianginalmedication. During 58±30 mo of follow-up, there were 15 deaths, 7 recurrent MI, and 11 soft events. LowHR response, old age, low LVEF, and high difference score were significant univariate risk factors fordeath. Multivariate analysis identified low HR response (p=0.03), high stress score (p=0.02), and lowLVEF (p=0.05) as independent predictors of mortality. The predictive value of HR response was incre-mental to that offered by other variables (p=0.02). Conclusions: HR response, readily attained duringvasodilator stress myocardial perfusion studies, may provide useful additional prognostic information inpost-MI patients.
Abbreviations: P/B ratio – peak to basal heart rate ratio; SDS – summed difference score SPECT; SPECT –single photon emission computed tomography; SSS – summed stress score
Introduction
There is a clear need to identify survivors of acutemyocardial infarction (MI) who have an increasedrisk of dying. Although several predictors ofmortality have been documented, simple nonin-
vasive tests that provide additional informationmay help identify high-risk subjects.Myocardial single photon emission computed
tomography (SPECT) with vasodilator stress offersimportant prognostic information in patients withcoronary artery disease and after MI [1, 2]. During
The International Journal of Cardiovascular Imaging (2006) 22: 663–670 � Springer 2006DOI 10.1007/s10554-005-9066-3

stress with dipyridamole or adenosine, subjectsshow an increase in heart rate (HR) [3, 4], but thisresponse is depressed with ischemic myocardialdisease [5, 6]. Dipyridamole-induced HR responseis also suggested to be an indicator of autonomicimbalance and a marker of HR variability [7–9], apowerful predictor of cardiovascular death amongpatients surviving acute MI [10–13]. Thus, the aimof this study was to determine whether HRresponse to vasodilator infusion for myocardialSPECT in post-MI patients can provide prognosticinformation additional to that obtained from theperfusion images.
Methods
Study population
Entry criteria were consecutive first acute MIsurvivors who underwent vasodilator stress myo-cardial SPECT and coronary angiography within3 months of the MI. SPECT was performed at anaverage of 25.4±24.3 days after the MI. In orderto compare HR responses according to infarctterritories and avoid confounding effects fromremote zone ischemia, only patients demonstratingsingle vessel disease on coronary angiography wereincluded. Exclusion criteria included the presenceof atrial fibrillation, frequent supraventricularectopic beats, resting HR of <60 or >100 beats/min, history of old MI, and revascularization priorto the SPECT study. A total of 147 patients werefinally included in the study (58±11 years; 117males and 30 females). Controls were 28 subjectswith low probability of coronary artery diseasewho underwent vasodilator stress myocardialSPECT to screen for noncardiac chest discomfort(61±10 years; 13 males and 15 females). The fol-lowing variables were recorded for each patient:age, gender, height, weight, infarct territory,diabetes mellitus, hypertension, hyperlipidemia,and smoking habit. The infarct territory wasclassified according to the location of myocardialperfusion defects and the location of ST changeson admission electrocardiogram. Two-dimen-sional echocardiography was performed at9±29 days of the SPECT study in 119 (81.0%) of
the patients, from which left ventricular ejectionfraction (LVEF) was measured.
Vasodilator stress and myocardial perfusionimaging
Patient preparation included overnight fasting,and 24 h abstinence from caffeine products, anti-cholinergics, and smoking. In order to avoid theeffect of medication on measured HR response,beta-blockers, calcium channel blockers, andnitrates were withheld from all patients for at least24 h before the test. Tests were performed in thesupine position in the morning, without precedingexertion. No patient had an acute illness duringthe 48 h preceding the study.Dipyridamole was infused into an antecubital
vein with an automated infusion pump at 0.14 mg/kg/min for 4 min. Adenosine infusion at an iden-tical rate for 6 min was used in 39 patients. Thal-lium-201 (111 MBq) was injected 4 min afterstarting adenosine infusion, or 8 min after dipyri-damole infusion. HR and blood pressure weremeasured at baseline and periodically for a mini-mum of 8 and 10 min for patients infused withadenosine and dipyridamole, respectively. The P/Bratio was calculated as the ratio of the highest HRmeasured over the basal HR and was used as anindex of HR response.Five minutes stress and 4 h redistribution
SPECT images were acquired on a triple-headgamma camera with a low-energy, high-resolution,all-purpose parallel-hole collimator (Triad XLT,Trionix Research Laboratory). Forty-five projec-tion images were acquired over a 180� semicircularorbit with a 20% energy window centered on the68–80 keV peak and were stored on a 128�64matrix. Transaxial tomographs reconstructedthrough filtered backprojection were reorientedinto short-axis oblique, sagittal, and coronal viewsthat were visually assessed by 2 independentobservers. Summed stress and rest scores weremeasured from polar maps of the tomographicimages using a 13-segment, standard 5-pointscoring method, and summed difference scoreswere calculated as the difference between stressand rest scores as previously described [14, 15].
664

Follow up and statistical analysis
Follow up of patients was done retrospectively bychart reviews and telephone interviews in the sametime period (in a month). Information on eventswas obtained by the patient, relatives, or by clini-cal records. The end points of hard events were all-cause mortality and nonfatal recurrent MI. Softevents were defined as hospitalization for unstableangina or heart failure.Continuous variables were expressed as
mean±SD, and compared by Student’s t-tests.Comparison of P/B ratios between patientsgrouped according to infarct territory or antian-ginal drugs was done by one-way ANOVA withBonferroni’s post-hoc test. Linear regression anal-ysis was used to evaluate correlation betweenHR response and summed stress scores or LVEF.P-values < 0.05 were considered significant. Sur-vival curves were constructed by the Kaplan–Meiermethod and were compared by log-rank tests.Variables of interest included sex, age, diabetes,hypertension, infarct territories, HR response,LVEF and perfusion defect scores. Cox propor-tional hazards regression models were used toidentify independent predictors of adverse events.A significant increase in the global v2 of a modelafter addition of a variable indicated incrementalprognostic significance. Analysis was performedusing SPSS statistical software (SPSS, Chicago)and GraphPad Prism version 3.00 for Windows(GraphPad Software, San Diego, CA).
Results
Clinical characteristics and myocardial perfusionimaging
The 147 study subjects had a mean age of57.5±11.2 years, andmean LVEFof 51.6±10.1%.(Table 1). Infarctions were predominantly in theleft anterior descending artery (LAD) territory(57.1%), while the remaining was located in the leftcircumflex (LCx) and right coronary artery (RCA)territories at similar rates. Myocardial SPECTidentified significant perfusion defects in 137/147
(93.2%) of the patients (Table 2). The perfusiondefects were persistent in 77 and reversible in 60patients. Segmental scoring of the defects resultedin a mean summed stress score of 14.2±8.6 andsummed difference score of 1.5±3.1.
Heart rate response to vasodilator stress
During vasodilator stress, the patient group dem-onstrated a P/B ratio of 1.22±0.13, which wassignificantly lower than that for the control group(1.32±0.12, p< 0.0005). The P/B ratios showedno evidence of dependence on interval between MIonset and vasodilator stress (data not shown).When patients were grouped according to infarctterritory, the P/B ratios for the LAD (1.21±0.13;p<0.001), LCx (1.22±0.12; p<0.05), and RCA(1.23±0.13; p<0.05) groups were all lower thanthat of controls, but not significantly differentbetween groups.
Table 1. Clinical characteristics of the 147 study subjects.
Age (years) 57.5±11.2
Male/Female 117/30
Diabetes Mellitus 32 (21.8%)
Hypertension 59 (40.1%)
Hyperlipidemia 69 (46.9%)
Current Smokers 93 (63.3%)
LVEF (%) 51.6±10.1
Infarct territory
LAD 84 (57.1%)
LCx 28 (19.0%)
RCA 32 (21.8%)
Undetermined 3 (2.0%)
Data are number of subjects or mean±SD.
Table 2. Findings of myocardial perfusion images.
Visual Assessment
Reversible defect present 60 (40.8%)
Fixed defects only 77 (52.4%)
No defect 10 (6.8%)
Segmental Analysis
Summed stress score 14.2±8.6
Summed difference score 1.5±3.1
Data are number of subjects or mean±SD.
665

Relation of heart rate responseto clinical variables
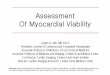
Comparison of HR response to clinical variablesdemonstrated greater depression of P/B ratios forpatients over 60 years (p<0.005), and those withdiabetes mellitus (p<0.0005). On the other hand,P/B ratios were not affected by patient gen-der, presence of hypertension, hyperlipidemia, orsmoking habits. Comparison of HR response to LVfunction and perfusion defects revealed thatP/B ratios had a high correlation with LVEF(p<0.0001, r=0.37) and a modest correlation withsummed stress scores (p<0.05; r=)0.18, Figure 1).Even though all subjects were withheld from
antianginal medication for more than 24 h, weevaluated whether there was any difference in HRresponse according to the antianginal drugs theyhad been using. As a result, there was no signifi-cant difference in HR response between patientswho had been using b blockers, calcium channelblockers, both, or none. Moreover, subjects withand without a low HR response showed no dif-
ference in the frequency of any particular antian-ginal drug being used.
Prognostic value of heart rate response tovasodilator stress
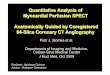
During a mean follow-up period of 58.0±29.6months, there were a total of 15 deaths, 7 nonfatalrecurrent MIs, and 11 soft events (8 unstableanginas and 3 heart failures). Also, there were15 patients who underwent revascularization,which were the same patients who had nonfatalrecurrent MIs (7 patients) and unstable angina(8 patients). Kaplan–Meier analysis revealed thatold age (>60 years; p=0.004; hazard ratio 4.58; CI1.62–13.2), low HR response (P/B<1.19; p=0.02;hazard ratio 3.57; CI 1.21–9.35; Figure 2), lowLVEF (£35; p=0.03; hazard ratio 4.49; CI 1.24–328.4), and high summed difference scores (>1.0;p=0.04; hazard ratio 2.74; CI 1.05–9.66) to be sig-nificant univariate predictors for mortality(Table 3). None of the variables tested were signif-icant predictors of nonfatal recurrent MI or soft
Figure 1. Scattergram showing correlation between heart rate response versus (a) LVEF and (b) summed stress scores. LVEF, left
ventricular ejection fraction; P/B, peak to basal.
Table 3. Prognostic value of heart rate response to vasodilator stress.
Variables p-value hazard ratio CI
Univariate predictors of death old age (>60 years) 0.004 4.58 1.62–13.2
low HR response (P/B<1.19) 0.02 3.57 1.21–9.35
low LVEF (£35) 0.03 4.49 1.24–328.4
high summed difference scores (>1.0) 0.04 2.74 1.05–9.66
Multivariate predictors of death low HR response 0.03
high summed stress scores 0.02
borderline for low LVEF 0.05
666

events. Stepwise Cox regression analysis showedthat multivariate predictors of death were lowHR response (p=0.03), high summed stress scores(p=0.02), and showed a borderline significance forlow LVEF (p=0.05). The global v2 of the multi-variable Cox proportional hazards model for pre-diction of death significantly increased from 8.01 to13.10 (p=0.02) after addition ofHR response to thevariables of summed stress score and LVEF.
Discussion
The purpose of this retrospective study was tocharacterize HR response to vasodilator inpatients after MI and determine the prognosticvalue of this factor. As a result, we found thatpost-MI patients have a depressed HR response tovasodilator infusion and that low HR response hassignificant prognostic value for predicting futuremortality.Dipyridamole and adenosine are routinely used
as a mode of pharmacological stress for myocardialperfusion SPECT. During infusion of these vaso-dilators, healthy subjects consistently show an in-crease in HR, explained in part by a reduction inbaroreceptor afferent nerve discharge after periph-eral vasodilation [4]. On the other hand, patientswith myocardial ischemia have a depressed HR
response [5, 6], which has been attributed to ablunted hypotensive response and alterations inmyocardial G protein levels [5]. Our results showthat vasodilator-induced HR response is alsodepressed in post-MI patients, most likely due tomechanisms similar to that for patients withmyocardial ischemia.Since b-blockers and calcium channel blockers
may blunt HR variability in patients with MI [16,17], such drugs have the potential to influence HRresponse during vasodilator stress. However, wewithheld these drugs before the SPECT test in allpatients for a minimum of 24 h and more often for48 h. Moreover, we were able to confirm that theHR response was not different according to whe-ther b-blockers and/or calcium channel blockershad been used, and that no particular drug wasused in higher frequency in subjects with comparedto those without low HR response. It is thusunlikely that antianginal medication significantlyaffected the results of our study.Depression in HR response was observed irre-
spective of the infarct site, with subjects of differ-ent infarct territories showing comparable levelsof depression. Analogous comparisons betweendecreased HR variability and infarct site haveshown a complex relationship. Whereas Lotzeet al. and Doulalas et al. observed a more evidentdepression of HR variability in the early phase ofanterior compared to inferior wall infarction[18, 19], other investigators did not find a signifi-cant difference based on infarct location [11, 20].The relation has also been reported to be timedependent, with more depressed HR variabilitywith anterior infarction only in the very earlyphase [21]. Since in our study, vasodilator stresstests were performed up to 3 months after infarc-tion, we cannot exclude the possibility that HRresponse between patients with anterior and infe-rior MI may be somewhat different in a more acutephase of MI.Among clinical characteristics, HR response was
more severely depressed in patients who had dia-betes mellitus. This is consistent with a previousobservation where vasodilator-induced HR in-crease was diminished in the presence of diabeticcardiac autonomic neuropathy [9]. HR responsewas also more severely depressed for those over
Figure 2. Kaplan–Meier survival curves for all-cause deaths
according to the presence or absence of low HR response to
vasodilator stress. Low HR response (P/B<1.19) was a signif-
icant predictor for mortality (p=0.02; hazard ratio 3.57; CI
1.21–9.35). P/B ratio, peak to basal heart rate ratio.
667

60 years of age. Although it is well known that HRvariability decreases with aging [21], it is not clearwhether this is also true for vasodilator-inducedHR response [22]. Because, in our study, otherassociated factors may have contributed to themore depressed HR response for the older sub-jects, further investigations may be necessary toclarify this issue.Comparison of HR response to LV function and
perfusion defects revealed a direct correlation toLVEF levels and an inverse correlation to stressdefect scores. These findings are consistent withthe known association of low HR variability withlarger sized infarction [18, 20, 23], that is creditedto a heightened sympathetic drive and reducedcardiac parasympathetic outflow [18].Prognosis after MI depends on many risk vari-
ables that are inter-related in that they reflect theextent of myocardial damage or activity of theautonomic nervous system. As such, the value ofinfarct size in predicting mortality following acuteMI is well recognized [24, 25], and the size ofperfusion defects on myocardial SPECT have beenshown to be a powerful prognostic factor in pa-tients after MI [1, 2]. But in our results, summedrest score which refers infarct size, was not anindependent predictor of mortality in post-MIpatients. On the other hand, multivariate analysisdemonstrated high summed stress scores, whichrefers to inducible perfusion abnormality, to be anindependent predictor of mortality in our study.This finding concurs to previous reports that ob-served significant prognostic value of summedstress scores [26].The probability of death after MI is also sub-
stantially influenced by the remnant left ventricu-lar systolic function, and LVEF has long beenrecognized as a powerful predictor of subsequentmortality [24, 25]. In our study, low LVEF was asignificant univariate risk factor for mortality andhad borderline significance on multivariate analy-sis. The somewhat less than expected predictivepower of LVEF most likely results from its asso-ciation with perfusion defect size as previouslynoted [27, 28]. This is supported by a significantinverse correlation observed between LVEF andsummed stress score (Pearson correlation coeffi-cient=)0.342, p< 0.0001). Because LVEF levels
were available in only 81% of the study subjects(n=119), the relatively smaller sample size is likelyto have contributed to the apparent stronger pre-dictive power of defect scores. Similarly, due to thesmall number of nonfatal recurrent MI (n=7), wewere not able to detect previously recognizedprognostic values of perfusion defect size or LVEFfor its prediction [29, 30].In our study, low HR response to dypiridamole
had a significant independent and incrementalprognostic value for predicting all-cause death.Although subjects with a low HR response had asomewhat older age, multivariate analysis showedthat low HR response was a predictor of mortalityindependent of patient age. Rather, the ability ofdepressed HR response to predict future mortalityappears to arise from its association with signifi-cant myocardial dysfunction [5]. Alternatively, itmay reflect a substantial derangement in HR var-iability, which is a known powerful predictor ofarrhythmic cardiac death [23].The findings of our study have important clini-
cal implication because pharmacological stressmyocardial SPECT procedures routinely includeHR measurements during vasodilator infusion,which in turn provides the HR response index.Therefore, in post-MI patients, recognition of thisreadily accessible index may provide clinicallyuseful prognostic information that may be used incombination with the patient’s myocardial perfu-sion status for risk stratification.
Study limitations
The major limitation of this study is its retrospec-tive design. Another important limitation is therelatively small number of patients included, whichmay have underpowered the ability to detect thepredictive value of certain variables. The subjects inour study were not evaluated at an identical timepoint after MI, which may have influenced the HRresponse. However, the interval was within3 months for all subjects, and we were not able tofind any evidence that HR response was dependenton the interval. In addition, the prognostic value ofHR variability for predicting mortality has beenshown to be valid in a broad range of times afterMI. These facts indicate that a difference in interval
668

after MI would not have significantly affected theresults of our study.
Conclusion
Our results demonstrate that HR response tovasodilator infusion is depressed after MI and thatlow HR response has significant independent andincremental value for predicting mortality. Since itis routinely obtained during vasodilator stressmyocardial SPECT, recognition of vasodilator-induced HR response as a prognostic factor afterMI may allow its use in combination with myo-cardial perfusion status for risk stratification insuch patients.
Acknowledgments
The investigators thank Ms. So Mi Park, BS, forsecretarial assistance and Mr. Sung-Wook Choi,BS, for technical assistance. This work was sup-ported in part by the National Mid- and Long-termNuclear R&D Program Grant #M20243010001-04A0701-00110 of the Korean Ministry of Scienceand Technology
References
1. Chiamvimonvat V, Goodman SG, Langer A, Barr A,
Freeman MR. Prognostic value of dipyridamole SPECT
imaging in low-risk patients after myocardial infarction.
J Nucl Cardiol 2001; 8: 136–143.
2. Brown KA, Heller GV, Landin RS, et al. Early dipyrida-
mole (99 m)Tc-sestamibi single photon emission computed
tomographic imaging 2 to 4 days after acute myocardial
infarction predicts in-hospital and postdischarge cardiac
events: comparison with submaximal exercise imaging.
Circulation 1999; 100: 2060–2066.
3. Gupta NC, Esterbrooks DJ, Hilleman DE, Mohiuddin SM.
Comparison of adenosine and exercise thallium-201 single-
photon emission computed tomography (SPECT) myo-
cardial perfusion imaging. The GE SPECT Multicenter
Adenosine Study Group. J Am Coll Cardiol 1992; 19:
248–257.
4. Clarke B, Conradson TB, Dixon CM, Barnes PJ. Repro-
ducibility of heart rate changes following adenosine infu-
sion in man. Eur J Clin Parmacol 1988; 35: 309–311.
5. Vashist A, Heller EN, Blum S, Brown EJ, Bhalodkar NC.
Association of heart rate response with scan and left ven-
tricular function on adenosine myocardial perfusion imag-
ing. Am J Cardiol 2002; 89: 174–177.
6. Zahedi A, Floras JS, Burns RJ. Absence of heart rate
increase during inferoposterior left ventricular hypoperfu-
sion caused by dipyridamole infusion. Can J Cardiol 1999;
15: 1345–1349.
7. Petrucci E, Mainardi LT, Balian V, et al. Assessment of
heart rate variability changes during dipyridamole infusion
and dipyridamole-induced myocardial ischemia: a time
variant spectral approach. J Am Coll Cardiol 1996; 28:
924–934.
8. Petretta M, Spinelli L, Marciano F, et al. Wavelet trans-
form analysis of heart rate variability during dipyridamole-
induced myocardial ischemia: relation to angiographic
severity and echocardiographic dyssynergy. Clin Cardiol
1999; 22: 201–206.
9. Lee KH, Yoon JK, Lee MG, Lee SH, Lee WR, Kim BT.
Dipyridamole myocardial SPECT with low heart rate re-
sponse indicates cardiac autonomic dysfunction in patients
with diabetes. J Nucl Cardiol 2001; 8: 129–135.
10. La Rovere MT, Bigger JT Jr, Marcus FI, Mortara A,
Schwartz PJ. Baroreflex sensitivity and heart-rate variabil-
ity in prediction of total cardiac mortality after myocardial
infarction. ATRAMI (Autonomic Tone and Reflexes After
Myocardial Infarction) Investigators. Lancet 1998; 351:
478–484.
11. Zuanetti G, Neilson J, Latini R, Santoro E, Maggioni A,
Ewing D. Prognostic significance of heart rate variability in
post-myocardial infarction patients in the fibrinolytic era.
Circulation 1996; 94: 432–436.
12. Copie X, Hnatkova K, Staunton A, Fei L, Camm AJ,
Malik M. Predictive power of increased heart rate versus
depressed left ventricular ejection fraction and heart rate
variability for risk stratification after myocardial infarction.
Results of a two-year follow-up study. J Am Coll Cardiol
1996; 27: 270–276.
13. Liu PY, Tsai WC, Lin LJ, et al. Time domain heart rate
variability as a predictor of long-term prognosis after acute
myocardial infarction. J Formos Med Assoc 2003; 102:
474–479.
14. Elhendy A, Schinkel AF, van Domburg RT, Bax JJ, Pol-
dermans D. Prognostic significance of fixed perfusion
abnormalities on stress technetium-99 m sestamibi single-
photon emission computed tomography in patients without
known coronary artery disease. Am J Cardiol 2003; 92:
1165–1170.
15. Berman DS, Kang X, Van Train KF, et al. Comparative
prognostic value of automatic quantitative analysis versus
semiquantitative visual analysis of exercise myocardial
perfusion single-photon emission computed tomography.
J Am Coll Cardiol 1998; 32: 1987–1995.
16. Lampert R, Ickovics JR, Viscoli CJ, Horwitz RI, Lee FA.
Effects of propranolol on recovery of heart rate variability
following acute myocardial infarction and relation to
669

outcome in the Beta-Blocker Heart Attack Trial. Am
J Cardiol 2003; 91: 137–142.
17. Pinar E, Garcia-Alberola A, Llamas C, et al. Effects of
verapamil on indexes of heart rate variability after acute
myocardial infarction. Am J Cardiol 1998; 81: 1085–1089.
18. Lotze U, Ozbek C, Gerk U, et al. Early time course of heart
rate variability after thrombolytic and delayed interven-
tional therapy for acute myocardial infarction. Cardiology
1999; 92: 256–263.
19. Doulalas AD, Flather MD, Pipilis A, et al. Evolutionary
pattern and prognostic importance of heart rate variability
during the early phase of acute myocardial infarction. Int
J Cardiol 2001; 77: 169–179.
20. Casolo G, Torder P, Signorimi C, et al. Heart rate vari-
ability during the acute phase of myocardial infarction.
Circulation 1992; 85: 2073–2079.
21. Pitzalis MV, Mastropasqua F, Massari F, et al. Different
trends of changes in heart rate variability in patients with
anterior and inferior acute myocardial infarction. Pacing
Clin Electrophysiol 1998; 21: 1230–1238.
22. Watt AH, Bayer A, Routledge PA, Swift CG. Adenosine-
induced respiratory and heart rate changes in young and
elderly adults. Br J Clin Pharmacol 1989; 27: 265–267.
23. Hartikainen JE, Malik M, Staunton A, Poloniecki J, Camm
AJ. Distiction between arrhythmic and nonarrhythmic
death after acute myocardial infarction based on heart rate
variability, signal-averaged electrocardiogram, ventricular
arrhythmias and left ventricular ejection fraction. J Am
Coll Cardiol 1996; 28: 296–304.
24. Multicenter Postinfarction Research Group. Risk stratifi-
cation and survival after myocardial infarction. N Engl
J Med 1983; 309: 331–336.
25. Burns RJ, Gibbons RJ, Yi Q, et al. The relationships of left
ventricular ejection fraction, end-systolic volume index and
infarct size to six-month mortality after hospital discharge
following myocardial infarction treated by thrombolysis.
J Am Coll Cardiol 2002; 39: 30–36.
26. Petix NR, Sestini S, Coppola A, et al. Prognostic value of
combined perfusion and function by stress technetium-
99 m sestamibi gated SPECT myocardial perfusion imaging
in patients with suspected or known coronary artery dis-
ease. Am J Cardiol 2005; 95: 1351–1357.
27. Kroll D, Farah W, McKendall GR, Reinert SE, Johnson
LL. Prognostic value of stress-gated Tc-99 m sestamibi
SPECT after acute myocardial infarction. Am J Cardiol
2001; 87: 381–386.
28. Gursurer M, Emre A, Gercekoglu H, Uslubus H, Aksoy
M, Ersek B. Long-term prognostic value of stress-redis-
tribution-reinjection Tl-201 imagingn in patients with
severe left ventricular dysfunction and coronary artery
bypass surgery. Int J Cardiovasc Imaging 2002; 18:
125–133.
29. Hachamovitch R, Berman DS, Shaw LJ, et al. Incremental
prognostic value of myocardial perfusion single photon
emission computed tomography for the prediction of car-
diac death: differential stratification for risk of cardiac
death and myocardial infarction. Circulation 1998; 97: 535–
543.
30. Mahmarian JJ, Mahmarian AC, Marks GF, Pratt CM,
Verani MS. Role of adenosine thallium-201 tomography
for defining long-term risk in patients after acute myocar-
dial infarction. J Am Coll Cardiol 1995; 25: 1333–1340.
Address for correspondence: Kyung-Han Lee, Departments of
Nuclear medicine, and cardiovascular institute, Sungkyunkwan
University School of Medicine, Samsung Medical Center, 135-
710, Seoul, Republic of Korea
Tel.: +82-2-3410-2630; Fax: +82-2-3410-2639
E-mail: [email protected]
670