Embed Size (px)
Citation preview

Surgical Infections
Pisake Boontham M.D., Ph.D.Department of Surgery
Phramongkutklao Hospital
Pathogenesis of Infection
•Host defences•Bacterial factors•Bacterial-host interaction•Immune response to infection

Host Defences
FEATURES OF INNATE AND ADAPTIVE IMMUNITY
Innate Immunity Adaptive Immunity
BarriersSkinMucosal epitheliumSecretions (skin surface, gut lumen)
IgA in gut lumen
Humoral components
LysozymeComplement components(C3a, C5a and C3b, C5b)Cytokines
Antibodies (IgG and IgM)Cytokines (Th1, Th2)*
CellsPhagocytic cells (mononuclear cells, polymorphonuclear cells)Natural killer cellsDendritic cells
Dendritic cellsT cells (helper*, cytotoxic, memory)B cells
*Th1: T helper (type 1) cells; Th2: T helper (type 2) cells

Humoral
Acute Phase proteins
Complement
Antibodies
Interferon
Cellular
Neutrophils
Macrophages
Nkcells
B – lymphocytes
T - lymphocytes
Physical Barriers
Skin
Mucus Membranes
Cilia
Gastric Acid
Tears
Urine
HOST DEFENCE SYSTEMS
Host Defences
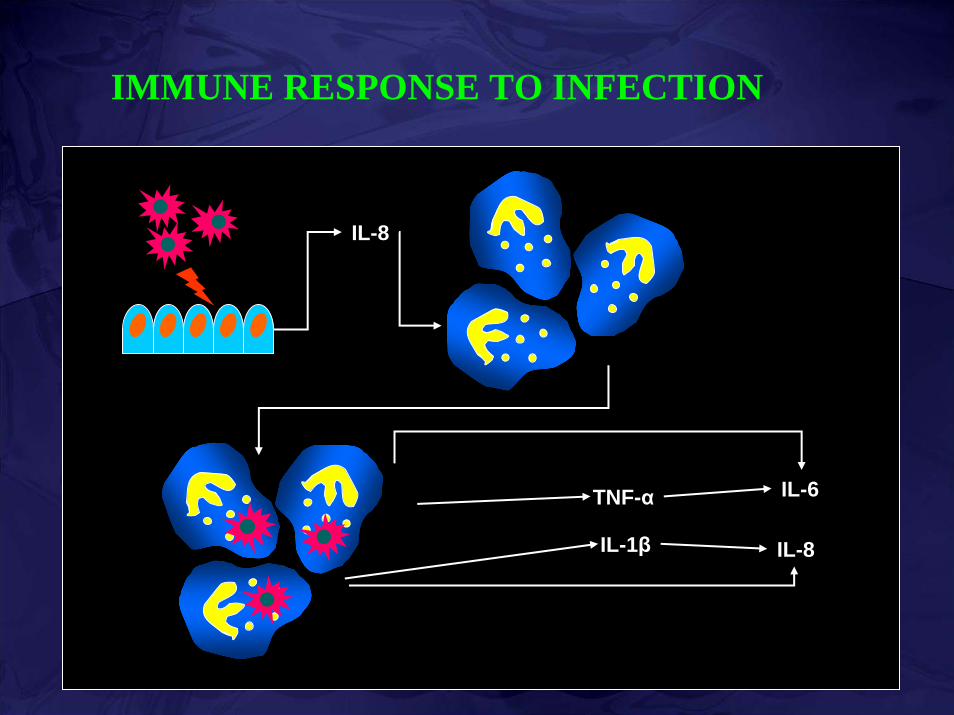
IMMUNE RESPONSE TO INFECTION
IL-8
TNF-α
IL-1β IL-8
IL-6


The cells and mediators involved in a local acute inflammatory response

Bacterial Factors
• Virulence Factors–Cell Wall Antigens–Serum Resistance–Hemolytic Capability–Growth Dynamics–Iron Scavenging
• Adherence Factors–P Fimbriae–Type 1 Fimbriae–DR Fimbriae
Bacterial Factors
• Microorganisms show Pathogen-Associated Molecular Patterns (PAMPs), which can be recognized, by so-called ‘Pattern-Recognition Receptors’ (PRRs) by the host: example of PAMPs –LPS of Gram-negative bacteria –Glycolipids of mycobacteria –Peptidoglycans (PGs) and Lipoteichoic acids (LTAs) of
Gram-positive bacteria, –Mannans of yeast or fungi–Double-stranded RNAs of viruses –Unmethylated CpG motifs of bacterial DNA

Bacterial-Host Interaction
• Bacterial components activate host immune responses via PRRs, which called Toll-like receptors (TLRs)
• There are ten TLRs (1-10) had been studied.–TLR-1 TLR-2–TLR-3 TLR-4–TLR-5 TLR-6–TLR-7 TLR-8–TLR-9 TLR-10
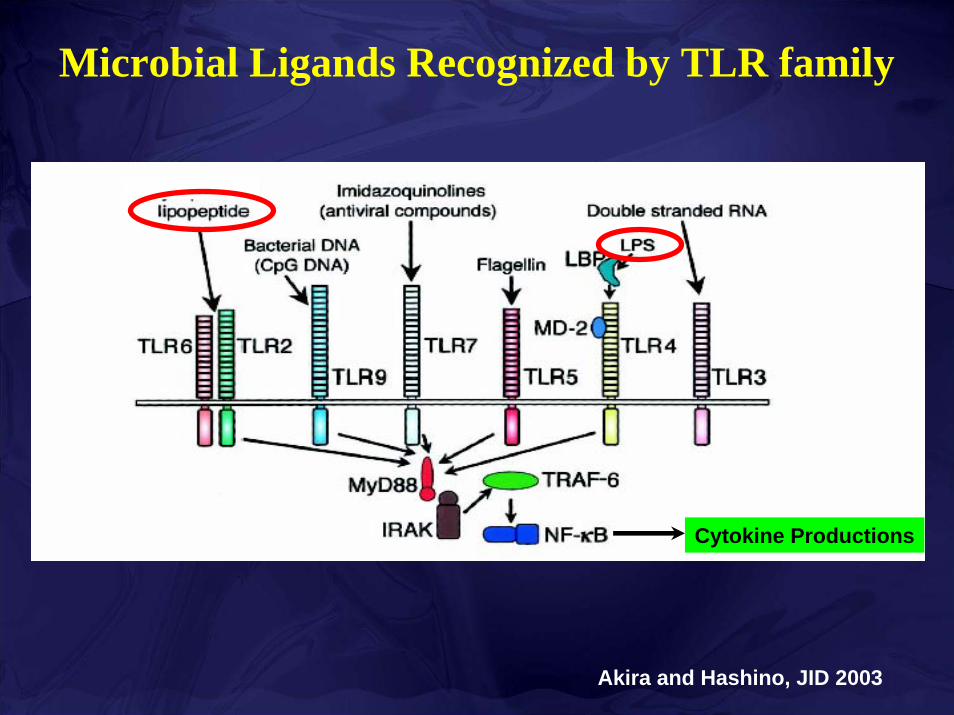
Akira and Hashino, JID 2003
Microbial Ligands Recognized by TLR family
Cytokine Productions


Sequence of Immune Response
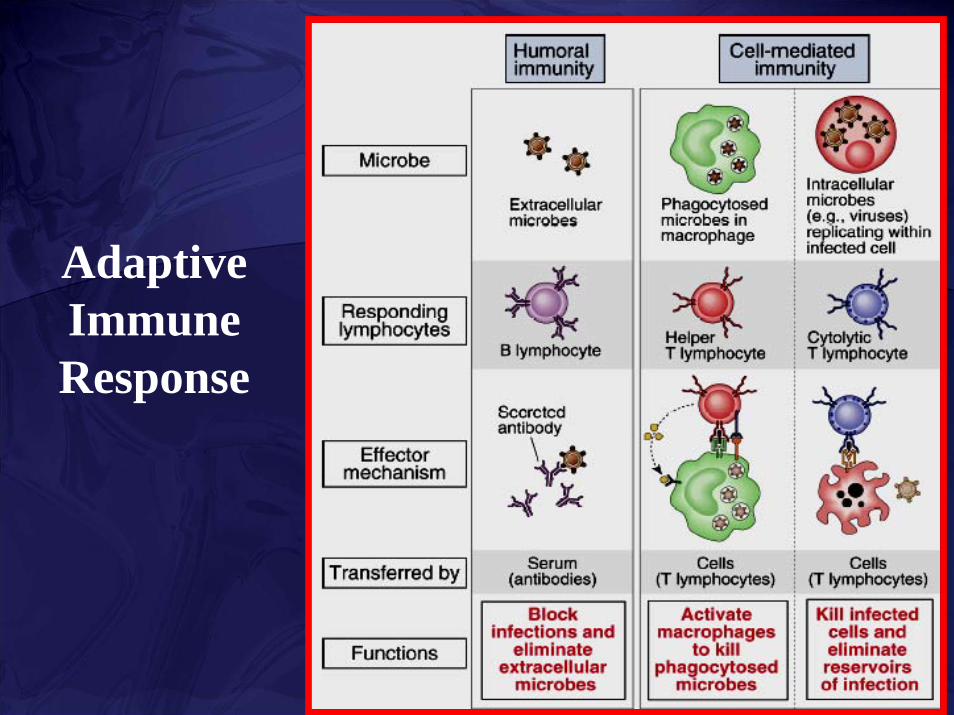
Adaptive Immune Response

SIRS
TRAUMA
BURNS
PANCREATITIS
INFECTION SEPSIS
BACTEREMIA
SEVERE SEPSIS
DEFINITIONS

• Systemic Inflammatory Response Syndrome (SIRS) ≥ 2 of the following:
•Temp > 38°C or < 36°C •Heart rate > 90 bpm•Respiratory rate > 20 bpm•WBC > 12,000, < 4,000 or bands > 10%
• SepsisSIRS + documented infection
Bone, et al. 1992. Chest 101:1644-1655

• Severe sepsis–Sepsis with organ dysfunction, hypoperfusion
or hypotension• Septic Shock
–Sepsis with hypotension and perfusion abnormalities despite adequate volume replacement
• MODS–Presence of altered organ function that need
intervention
Bone, et al. 1992. Chest 101:1644-1655

PATHOGENESIS OF SEPSIS
• Bacterial components (Cell wall)• Host immune responses; 3 major entities
–Cytokine cascade •Proinflammatory cytokines [T helper 1 (Th1)]•Antiinflammatory cytokines [T helper 2 (Th2)]–Mediators: NO, O2
-
–Apoptosis of immune and non-immune cells

ROLE OF CYTOKINES
• Sepsis is associated with the production of many cytokines including:
–Pro-inflammatory cytokines (early phase; SIRS)
: IFN-γ, TNF-α, IL-1β, IL-6, IL-8, IL-12
–Anti-inflammatory cytokines (late phase; CARS)
: IL-4, IL-10, IL-13

• Proinflammatory cytokines activate:–Biochemical systems
•Complement, coagulation, kinin, etc.–Endothelial cells–PMN / platelets–Release of secondary mediators
•NO, prostaglandins, vasoactive agents, endorphins, free-O2 radicals, etc.
ROLE OF CYTOKINES

Arya et al, AJS183 (2002); 268-273

CYTOKINE PROFILE IN SEPSIS
IL-8

• Stage 1. In response to injury / infection, the local environment produces cytokines
• Stage 2. Small amounts of cytokines are released into the circulation:• Recruitment of inflammatory cells• Acute Phase Response• Normally kept in check by endogenous anti-
inflammatory mediators (IL-10, PGE2, Antibodies, Cytokine receptor antagonists)
Bone, et al. 1996
Sequential Stages in Sepsis

Sequential Stages in Sepsis• Stage 3. Failure to control inflammatory cascade:
• Loss of capillary integrity• Stimulation of Nitric Oxide Production• Maldistribution of microvascular blood flow• Organ injury and dysfunction
• Stage 4. Compensatory anti-inflammatory response syndrome [CARS]:• Inappropriate and excessive anti-inflammatory responses• Immunosuppression• Multiple organs injuries• Significant morbidity and mortality
Bone, et al. 1996


Appropriate cytokineresponse
Inappropriate cytokineresponse
Low bacterial loadBalanced cytokine
Minimal SIRS
High bacterial loadExcessive cytokine
SIRS or CARS
ROLE OF CYTOKINES

CYTOKINES AND COAGULATION PATHWAY
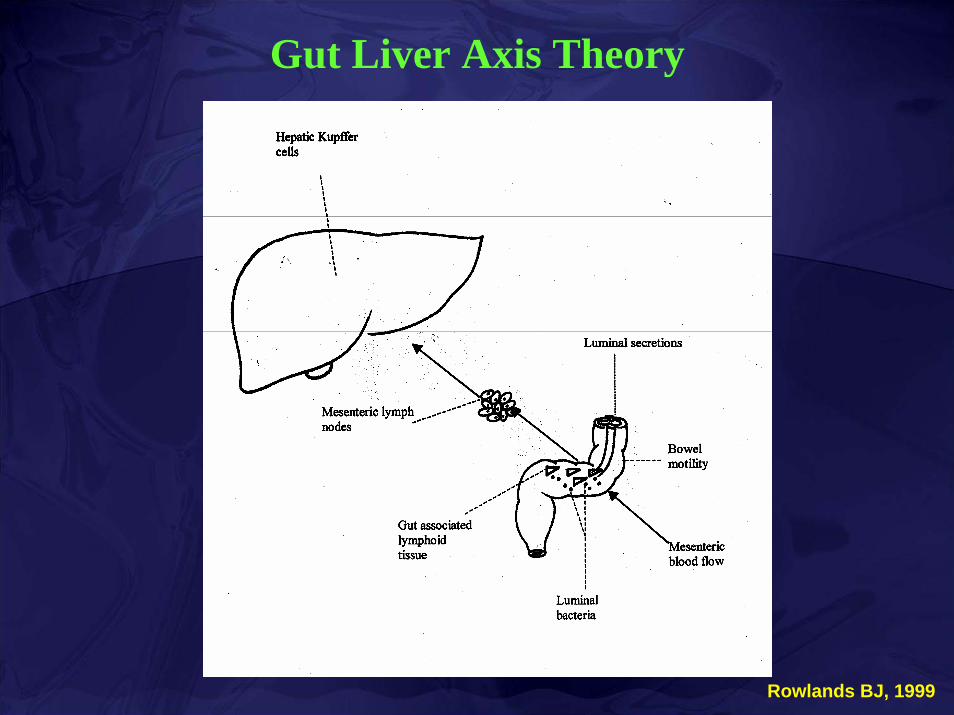
Gut Liver Axis Theory
Rowlands BJ, 1999

Gut Liver Axis Theory
Rowlands BJ, 1999

Severe sepsis
Clinical hypoperfusion
Gut barrier dysfunction
Influx of bacterial products (e.g. QSSMs) into systemic circulation
Bacterial products inhibit host immunity
Dysfunction of host immunity
MODS

Tissue injuryApoptosis
Septic shock

Apoptosis
MODS

Bacteria Host immune cells
Bacterial products+Cytokines Apoptosis

Bacteria Host immune cells
Antibiotics
Anti-apoptosis
CytokinesApoptosis
Neutralization

Surgical Infection
• Infections that require operative treatment or result from operative treatment
Definition

Specific Surgical Infections
•Surgical Site Infections•Skin and Soft Tissue Infections •Intra-abdominal Infections•Sepsis•Organ specific Infections•Catheter Related Infections•Post-operative Nosocomial Infections

Surgical Site Infection (SSI)
DefinitionAn infection that occurs at the incision site within 30
days after surgery or within 1 year if a prosthetic implant is in place.

Nosocomial PathogensNNIS, Jan. 1990 - Mar. 1996
0
5000
10000
15000
20000
25000
30000
35000
40000
Urinary TractInfection
Surgical SiteInfection
BloodstreamInfection
Pneumonia Other Sites
Num
ber o
f Iso
late
s
Burke JP. N Engl J Med. 2003;348:651-656.

Systematic review of economic analyses of health care-associated infections: AJIC 2005;33:501 – 9.
Attributable costs of HAI

ระยะเวลาที่อยูโรงพยาบาลนานขึ้นเฉลี่ย 12.5 วัน
คายาตานจุลชีพ 4,544 บาท
Impacts of SSIs
Prevalence and Impacts of Nosocomial Infection in Thailand 2001J Med Assoc Thai 2005 Vol. 88 Suppl.10

CLASSIFICATION OF SURGICAL WOUNDS
CLEAN
Uninfected operative wounds in which no inflammation is encountered and the respiratory, alimentary, genital and uninfectedurinary tractare not entered.
CLEAN-CONTAMINATED
Operative wounds in which the respiratory, alimentary, genital or urinary tract is entered under controlled conditions and without unusual contamination.
CONTAMINATED
Includes open, fresh accidental wounds, operations with major breaks in sterile technique or gross spillage from the GI tract and incisions in which acute, non-purulent inflammation is encountered.
DIRTY
Old traumatic wounds with retained devitalised tissue and those that involve existing clinical infection or perforated viscera.

Deep soft tissue (fascia & muscle) Deep incisional
SSI
Superficial incisional SSI
Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20:250-278.
Subcutaneous tissue
Skin
Organ/space SSIOrgan/space

SSI rate in Thailand
Surgical Wound Classification
Risk พ.ศ.2531 (1)
พ.ศ.2535 (2)
พ.ศ.2544 (3)
Clean
Clean-ContaminatedContaminated
Dirty-Infected
1- 5 %
3-11 %
10-17 %> 27%
15.3 %
18.6 %
24.7 %
30.1 %
1.3 %
1.5 %
5.1 %
9.7 %
1.5 %
3.4 %
6.3 %
7.7 %
(3) Prevalence and Impacts of Nosocomial Infection in Thailand 2001J Med Assoc Thai 2005 Vol. 88 Suppl.10
(1) A National Prevalence Study on Nosocomial Infections 1988J Med Assoc Thai July 1989 Vol. 72 Suppl.2 :1-6.
(2) A National Study on Surgical Wound Infections 1992J Med Assoc Thai July 1995 Vol. 78 Suppl.2 :73-77.

NNIS risk index categoryKnight R, et al. Am J Surgery 182 (2001) 682–686

SSI rates of different types of procedures and risk index category
Procedures 75th percentile operation time (min)
NNIS risk index 0
NNIS risk index 1
NNIS risk index 2,3
Craniotomy 130 0.90 1.67 NA
Thyroid surgery 120 0.47 NA NA
Cardiac surgery 250 0.70 1.71 2.21
Other thoracic surgery 150 0.65 1.17 3.07
Vascular surgery 140 0.89 1.74 4.51
Mastectomy 140 1.80 2.48 NA
Inquinal hernia repair 60 0.77 1.90 3.77
Laparotomy 90 1.71 3.29 5.16
Cholecystectomy 60 0.68 1.93 3.33
Appendectomy 60 1.20 2.55 4.85
Gastric surgery 140 2.79 5.02 10.36
Small bowel surgery 140 5.20 7.33 9.38
Colon surgery 140 4.02 5.76 8.73,11.62
Nephrectomy 180 1.13 1.13 1.13
Open reduction of fracture 90 0.73 1.25 3.51
NNIS. CDC. Am J Infect Control. 2001;29:404-421.

American Society of Anesthesiologists(ASA)physical status
1 Normal2 Mild systemic disease3 Severe systemic disease4 Incapacitating systemic disease that
is a constant threaten to life5 Moribund, not expected to survive
for 24 hours with/without operation

SSI – Wound Class vs NNIS Class
Wound Class All NNIS 0 NNIS 1 NNIS 2 NNIS 3
Clean 2.1% 1.0% 2.3% 5.4% N/A Clean contaminated 3.3% 2.1% 4.0% 9.5% N/AContaminated 6.4% N/A 3.4% 6.8% 13.2%Dirty infected 7.1% N/A 3.1% 8.1% 12.8%
All 2.8% 1.5% 2.9% 6.8% 13.0%
NNIS. CDC. Am J Infect Control. 2001;29:404-421.

Risk Factors for Surgical Site Infections
Surgical/ Environmental
Factors
Microbial Factors
AgeProlonged preoperativestayInfection at distal siteMorbid ObesityMalnutritionCancerDiabetesASA classDisease severityImmunosuppression
Nasal/skin carriageVirulenceAdherenceInoculum
Abdominal siteWound classificationDuration of surgeryType of procedureHair removalIntraoperative contaminationProphylactic antibioticsSurgical techniqueSurgical volumeMultiple operationsPoor hemostasisDrain/foreign body Dead spaceUrgency of surgeryHypothermiaOxygenation
Host Factors
Roy MC, et al. Infect Control Hosp Epidemiol 1997;18:659-68.

Possible Risk Factors for Postoperative Wound Infections
Host Factors
• Age• Gender• Severity of disease• ASA physical status
classification• Immunocompromising
disease
• Diabetes mellitus• Estimated prognosis• Nutritional status• Serum albumin• Weight• Presence of other
infections• Duration of preoperative
stay

Effect of Aging on Surgical Site Infection
10-year, prospective, cohort studyN = 144,485 patients undergoing surgical proceduresAge ranged from 17 to 108 years
Age was a strong predictor of infection between 17 and 65 years, the rate of infection increased (~ 1%) per decade peaking at 65 years
At 65, the risk of SSI actually decreased in a linear manner for each additional year;
candidate for less risky selected surgical procedures – low risk procedureshardy survivor effectless likely to detect an infection in this patient population
Kaye KS. J Infect Dis 2005;191:1056-1062

Hyperglycemia: Diminished Phagocytic Cell Function
Rayfield et al, Am J Med 1982; 72: 439-450
Hyperglycemia: Impaired Wound Healing - Collagenase
Hennessey et al, J Pediatr Surg 1990; 25: 75-78

Link Between High Blood Glucose and Poor Outcomes: Potential Mechanisms
Copyright 2004 American Diabetes Association. From Clement S, et al. Diabetes Care.2004;27:553–591. Reprinted with permission.
Immune dysfunction Reactive O2 species
Secondary mediators
Transcription factors
Metabolic stress response↑ Stress hormones and peptides
GlucoseInsulin
Infection dissemination
FFAKetonesLactate
Cellular injury/apoptosisInflammationTissue damageAltered tissue/wound repairAcidosisInfarction/ischemia
Prolonged hospital stayDisabilityDeath

Perioperative Glucose Control
0
5
10
15
20
<200 200-249 250-299 >300
% In
fect
ions
Latham R. Infect Control Hosp Epidemiol. 2001;22:607-12
*1,000 cardiothoracic surgery patients

SSIs Reduced By Tight Peri-op Glucose Control
Type of SurgeryType of Surgery PrePre--Tight Tight glycemic controlglycemic control
Post_Tight Post_Tight Glycemic ControlGlycemic Control
CardiothoracicCardiothoracic 4.6%4.6% 2.5%2.5%
VascularVascular 1.9%1.9% 0.83%0.83%
Hip replacementHip replacement 1.0%1.0% 0.7%0.7%
Knee Knee replacementreplacement
1.1%1.1% 1.0%1.0%
BariatricBariatric 17.9%17.9% 5.3%5.3%
Morris Brown MD, Henri Ford Hospital,Morris Brown MD, Henri Ford Hospital,International Anesthesia Research SocietyInternational Anesthesia Research Society

Possible Risk Factors for Postoperative Wound Infections
Surgery Factors
• Emergency vs elective procedure
• Hair removal technique• Hand washing• Surgical skin prep• Perioperative
antibiotics• Site of surgery• Operating room
environment
• Increased O2 tension• Normothermia• Surgeon• Duration of surgery• Drains• Packs & Drapes• Glove puncture• Primary or secondary
closure• Iatrogenic

Hair Removal and SSI
• Presence of hair does not does not increase SSI• Razor blades increase SSI• Hair removal with clippers was found to be safer
and result in a lower incidence of SSI• Hair removal closer to incision time decrease SSI
compared to hair removal the night before surgery.
Alexander et al, Arch surg 1983, 118(3): 347

Shaving, Clipping & SSI
0
0.5
1
1.5
2
2.5
Shave Clip Neither
% Infected
Cruse. Arch Surg 1973; 107:206

Ability of Hand Hygiene Agents to Reduce Bacteria on Hands
99.9 3.0
99.0 2.0
90.0 1.0
0.0 0.0
Baseline
Bac
teria
l Red
uctio
n% log 0 60 180 minutes
Plain soap
Antimicrobial soap(4% Chlorhexidine)
Alcohol-based handrub(70% Isopropanol)
Hosp Epidemiol Infect Control, 2nd Edition, 1999
Time after disinfection

Agent Action Gram + Gram - Tbc Fungi Virus Rapidity Residual
activity
toxicity
Alcohol Denature
protein
E E G G G Most rapid None Drying,
Volatile
Chlorhexidine Disrupt cell
membrane
E G P F G Intermediate Excellent Ototoxic,
Keratitis
Iodine /
Iodophore
Oxidation /
substitution
by free
iodine
E G G G G Intermediate Minimal Absroption
from skin,
Irritation
Chlorhexidine
/ Alcohol
Denature
protein
E E G G G Most rapid Excellent Ototoxic,
Keratitis
E-excellent; F-fair; G-good

200000
180000
160000
140000
120000
100000
80000
60000
40000
20000
0
Hallux
Tota
l num
ber o
f bac
teria
l col
onie
s
Toes Controls
Ostrander RV. J. Bone Joint Surg. Am. 2005;87:980-985
Effects of Skin Preparative Agents in Foot and Ankle Surgery
Chlorhexidine /alcohol
Iodophor /alcohol
Chloroxylenol

Antibiotic Prophylaxis

Goals of Surgical ProphylaxisPrevent postoperative infection of the surgical sitePrevent postoperative infectious morbidity and mortalityReduce duration and cost of health careProduce no adverse effectsHave no adverse consequences for the microbial flora of patient or hospital

Probability of Wound Infection
Houang ET, et al. J Hosp Infect 1991;19:181-9.

Guidelines of prophylactic antibiotics
Recommended in:
Some Clean wound*Clean-contaminated woundContaminated woundDirty wound
Documented beneficialin clean wounds
Prosthesis is insertedVascular surgeryNeurosurgeryBone is incised (craniotomy,
sternotomy)High risk patients e.g. old,
DM, co-morbidityControversy on cases of clean surgery of soft tissues (eg,
breast, hernia)
Barie PR, et al. Surg Clin N Am 2005;85:1115–35.
Mangram AJ, et al. Infect Control Hosp Epidemiol 1999;20:247–80.

Which Antibiotics?1st-gen cephalosporin is the preferred agent Clindamycin and vancomycin preferred for patients with a history of anaphylaxis to penicillin*No evidence of routine use of vancomycin for prophylaxisVancomycin prophylaxis is appropriate only in institutions where the incidence of MRSA infection is high (>20% of all SSIs caused by MRSA)Vancomycin should be considered for prophylaxisin patients with known MRSA colonization
Barie PR, et al. Surg Clin N Am 2005;85:1115–35.
*Bratzler DW, et al. Am J Surg 2005;189:395–404.

Procedure-Specific Recommendations for Prophylaxis Procedure Likely organisms Recommended antibiotic Adult dose Cutaneous S. aureus, S. epidermidis No uniform recommendation Head and neck S. aureus, streptococci Cefazolin 1 to 2 g IV Neurosurgery S. aureus, S. epidermidis Cefazolin 1 to 2 g IV Thoracic S. aureus, S. epidermidis Cefazolin 1 to 2 g IV Cardiac S. aureus, S. epidermidis Cefazolin 1 to 2 g IV Gastro-intestinal-Appendectomy
Gram-positive cocci, enteric gram-negative bacilli
High risk: cefoxitin or cefminox Alternative: ampicillin/sulbactam
amoxicillin/clavulanic acid
1 to 2 g IV 3 g IV1.2 g IV
Colorectal Enteric gram-negative bacilli, anaerobes
Oral: neomycin + erythromycin Parenteral: cefoxitin or cefminox Alternative: ampicillin/sulbactam
amoxicillin/clavulanic acid
1 g oral x 3 1 to 2 g IV3 g IV
1.2 g IV
Biliary tract Enteric gram-negative bacilli High risk: cefoxitin or cefminox Alternative: ampicillin/sulbactam
amoxicillin/clavulanic acid
1 to 2 g IV 3 g IV1.2 g IV
Ob-Gynecologic Enteric gram-neg bacilli, anaerobes Cefazolin, cefoxitin or cefminox 1 to 2 g IV
Urologic S. aureus, enteric gram-neg bacilli High risk: ciprofloxacin 400 mg IV
Orthopedic S. aureus, S. epidermidis Cefazolin 1 to 2 g IV
Vascular surgery S. aureus, S. epidermidis Cefazolin 1 to 2 g IV
Breast and hernia S. aureus, S. epidermidis High risk: cefazolin 1 to 2 g IV


The Medical Letter; Dec 2006:83-88

The Medical Letter; Dec 2006:83-88

SSI Rates by Time of Antibiotic Administrations
0
1
2
3
4
5
6
>2 2 1 1 2 3 4 6 7 8 9 >10
SSI R
ate
Classen DC, NEJM 1992; 326:281-6

Single vs Multiple Dose Surgical Prophylaxis: Systematic Review
McDonald. Aust NZ J Surg 1998;68:388
0.01
0.1
1
10
100
All
stud
ies,
fixe
dA
ll st
udie
s, ra
ndom
Mul
ti >
24h
Mul
ti <
24h
Favo
rs m
ultip
le d
ose
Favo
rs s
ingl
e do
se
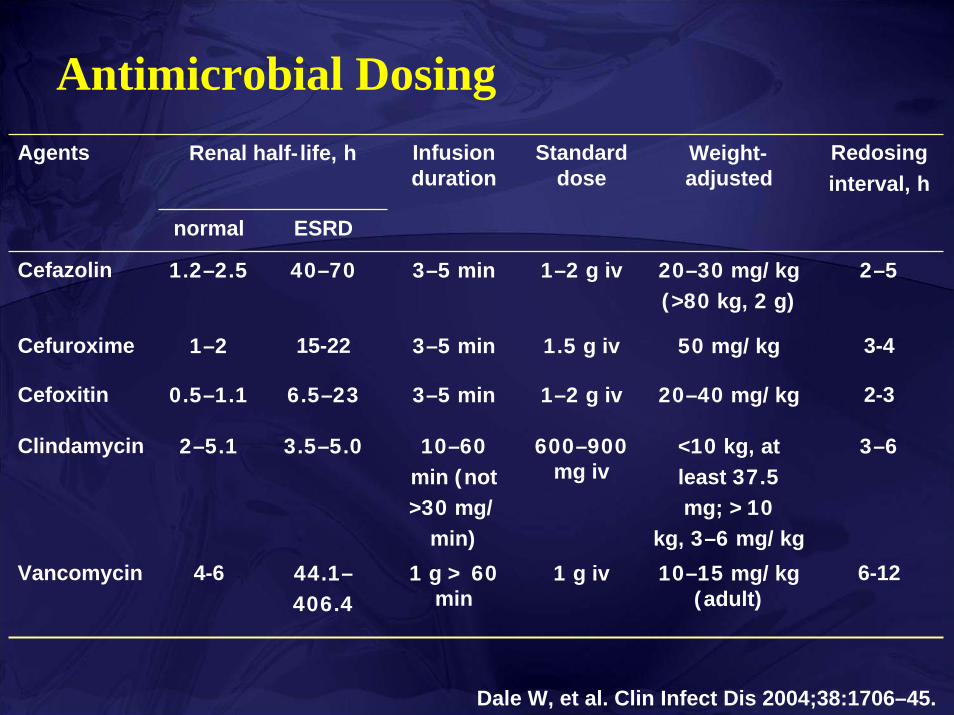
Antimicrobial DosingAgents Renal half-life, h Infusion
durationStandard
doseWeight-adjusted
Redosinginterval, h
normal ESRD
Cefazolin 1.2–2.5 40–70 3–5 min 1–2 g iv 20–30 mg/kg (>80 kg, 2 g)
2–5
Cefuroxime 1–2 15-22 3–5 min 1.5 g iv 50 mg/kg 3-4
Cefoxitin 0.5–1.1 6.5–23 3–5 min 1–2 g iv 20–40 mg/kg 2-3
Clindamycin 2–5.1 3.5–5.0 10–60min (not>30 mg/
min)
600–900mg iv
<10 kg, at least 37.5mg; >10
kg, 3–6 mg/kg
3–6
Vancomycin 4-6 44.1–406.4
1 g > 60min
1 g iv 10–15 mg/kg (adult)
6-12
Dale W, et al. Clin Infect Dis 2004;38:1706–45.

Principles of Antibiotic Prophylaxis
Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20:250-278.
Preop administration, serum levels adequate throughout procedure with a drug active
against expected microorganisms.
High Serum Levels1. Pre-op timing2. IV route3. Highest dose
of drug4. Long half-life
Re-doses when:1. Operation time
more than 2 half-life of drug
2. Long procedure3. Large blood loss
Duration1. None after wound
closed2. 24 hours maximum

Prolongation of Antibiotic Prophylaxis
Harmful and no benefitClostridium difficile-associated diseaseIncreases ris k of later nosocomial infections unrelated to surgical site
Pneumonia and catheter-related infection
Emergence of multi-drug resistant pathogensMRSA, ESBL

StaphylococcusStreptococcusStaphylococcusStaphylococcusStreptococcusStreptococcus
Gram-negative
bacilli
Gram-negative
bacilliAnaerobesAnaerobes
Distribution of Bacteria from Superficial to Deep Infection
Superficial infection
Deep infection
Microorganism of SSI

Major Pathogen in SSI%
of i
nfec
tions
NNIS 2003

Microbiology of SSI in Ramathibodi Hospital (47 isolates)
MRSAEnterococci
A. baumanniiP. aeruginosa K. pneumoniae (inc. ESBL)E. coli (inc. ESBL)Proteus spp. Stenotrophomonas spp.Enterobacter spp. (ESBL)

Treatment of SSI
Incision and drainage and evacuate infected material of the SSITissue specimens or pus collected aseptically (no routine swabs of fluid)Antibiotics is not required for uncomplicated SSI
Minimal surrounding evidence of invasive infection and minimal systemic signs of infectionObservation-dressing changes-opening the incision site
Antibiotics may be indicated in SSI with the presence of systemic toxicity
Barie PR, et al. Surg Clin N Am 2005;85:1115–35.
Stevens DL, et al. Clin Infect Dis 2005;41:1373-405.

Empiric Antibiotic Therapy
Findings of Gram stain and results of culture of the wound contentsType and site of surgeryResident flora of surgical environmentColonization flora of specific hospitalStatus of patients’ immune system
Barie PR, et al. Surg Clin N Am 2005;85:1115–35.
Coverage against gram-positive cocci is indicated in most circumstances

Antibiotic Treatment Regimens
Type of infection Common infecting bacteria Antibiotic therapy
Superficial wound and surgical incisioninfections
Strep, staph Not used routinely; if needed, 1st
gen ceph or oxacillin
Deep wound infections other than GI, female genital tract, or oropharyngealsurgery
Strep, staph, Gram- negative enteric bacteria
1st-gen ceph or cloxacillin; if mixed infections are suspected, 2nd or 3rd
gen ceph or amoxicillin/clavulanate, ampicillin/sulbactam, or piperacillin/tazobactam (imipenem or meropenem)
GI, female genital tract, or oropharyngeal surgery
Same as for other deep wound infections, with addition of Bacteroides species, other anaerobes,enterococci
Same as for mixed infection, above
Nichols RL, et al. Clin Infect Dis 2001;33:S84-93.

SSI organism Antibiotic susceptibilityStaphylococcus aureus •90% remain susceptible to cloxacillin,
macrolides and clindamycin Skin wound at any site
Beta-haemolytic streptococci
•90% remain susceptible to penicillins, macrolides and clindamycin
Head and neck surgery
Oral anaerobes •95% remain susceptible to metronidazole and amoxi/clav. •Penicillin can no longer be relied upon.
Anaerobes •95% remain susceptible to metronidazole and amoxi/clav.
Abdominal surgery
E. coli and other enterobacteriaceae
•Complex resistance problems. However, 90% of E. coli remain susceptible to 2nd generation cephalosporins or BL/BIs, or gentamicin
Insertion of a prosthesis, graft or shunt
Coagulase negative Staphylococci (CNS)Staphylococcus aureus
•90% of S. aureus remain susceptible to cloxacillin, macrolides or clindamycin. Although 2/3 of CNS are methicillin-resistant, prophylaxis with beta-lactam antibiotics is still appropriate.
►

Environmental controlsOperating room environment
Maintain > 15 air changes per hour Maintain positive-pressure ventilation with laminar flowFilter all air, recirculated and fresh, through the appropriate filters Keep operating room doors closed
►

• Double-blind, randomized, controlled trial• 3 hospitals (2 in Austria, 1 in Germany)• N=500, colorectal resection (cancer, IBD)• July 1996-October 1998• FiO2 0.8 vs 0.3 during and 2 hours postop• SSI during 14 days postop
Greif R et al. Greif R et al. N Engl J MedN Engl J Med. 2000;342:161. 2000;342:161--167.167.

Greif R et al. Greif R et al. N Engl J MedN Engl J Med. 2000;342:161. 2000;342:161--167.167.

Supplemental Perioperative Oxygen and the Risk of Surgical Wound Infection
A Randomized Controlled Trial
• Double-blind, randomized, controlled trial• 14 Spanish Hospitals• N=300,Colorectal surgery, general anesthesia• March 2003- October 2004• FiO2 0.8 vs 0.30 during and 6 hours postop• SSI : 35 (24.4%) vs 22 (14.9%), p=0.04
Belda et al, JAMA, 2005; 194: 2035

Hypothermia
Low Oxygen TensionVasoconstriction
↓Oxidative Killing by neutrophils
↓Collagen deposition
Impaired immune function
Effects of Hypothermia and Hypoxia on Wound Healing

Perioperative normothermia
Normothermic Hypothermic Temperature 36.6+0.5 34.7+0.6 Infections (%) 6 19 Hospitalization (Days)
12.1+4.4 14.7+6.5
Melling et al., Lancet 2001;358:876
*200 colorectal surgical patients
Clinical Wound Infections
Blood transfusion–Avoid blood transfusion
–Prospective cohort study 2003: transfusion of more than 4 units of packed red blood cells was associated with a 9.28-fold increased risk of infection
Hill GE, et al. J Trauma 2003;54:908–14.

SurgeonHand washingGloves: double gloves
20% of surgical gloves fail during operationOther barriers
CapsMasksGowns

0
10
20
30
40
50
60
cfu/
m3
90 minutesTest Interval
180 minutes
No Mask - HealthySurgical Mask - HealthyNo Mask - RhinorrheaSurgical Mask - Rhinorrhea
Impact of Surgical Masks on Prevention of Microbial Nasopharyngeal Shedding in Healthy Individuals (N = 22)
and Subjects with Symptoms of Rhinorrhea (N = 8)
NS
NS
p<0.05
p<0.05
Edmiston et al, Surgery 2005; 138:572-583

Surgical techniquesGentle tissue handlingRemoval of devitalized tissue or blood or other substancesUsing drain appropriatelyAvoid extensive cauterizationAvoid anastomosis of intestine under tension

Postoperative wound care
• Sterile dressing for 24-48 hrs postoperatively
• Wash hands before and after dressing changes
• Changed with sterile technique
• Educate patient and family regarding proper incision care, symptoms of SSI, and need to report

PreoperativeIntraoperativePostoperative Surveillance
Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20:250-278.
AimsReduce the inoculums of bacteriaImprove the host defences

Infection surveillance
Good surveillance program lowered wound infection rate from 4.9 to 1.9 %
Mangram AJ, et al. Infect Control Hosp Epidemiol 1999;20:247–80.

Thank you


![[XLS] · Web viewJIVAN JYOT CHARITABLE TRUST, PATAN JANTA HOSPITAL-PATAN SAL HOSPITAL (2) CARDIOLOGY (4) CARDIOVASCULAR SURGERY (5) GENITOURINARY SURGERY AARNA SUPERSPECIALITY HOSPITAL](https://img.pdfslide.us/doc/110x75/5ad68f887f8b9a32618b4569/xls-viewjivan-jyot-charitable-trust-patan-janta-hospital-patan-sal-hospital-2.jpg)