Embed Size (px)
Citation preview
Department of Origin: Integrated Healthcare Services
Effective Date: 06/09/21
Approved by: Medical Policy Quality Management Subcommittee
Date Approved: 06/08/21
Clinical Policy Document: Anesthesia Services for Routine Screening and Diagnostic Gastrointestinal Endoscopic Procedures
Replaces Effective Clinical Policy Dated: 06/24/20
Reference #: MC/G013
Page: 1 of 4
PURPOSE: The intent of this clinical policy is to ensure monitored anesthesia (deep sedation) or general anesthesia services in conjunction with routine screening and diagnostic esophagogastroduodenoscopy (EGD) or colonoscopy procedures are medically necessary. Please refer to the member’s benefit document for specific information. To the extent there is any inconsistency between this policy and the terms of the member’s benefit plan or certificate of coverage, the terms of the member’s benefit plan document will govern. POLICY: Benefits must be available for health care services. Health care services must be ordered by a provider. Health care services must be medically necessary, applicable conservative treatments must have been tried, and the most cost-effective alternative must be requested for coverage consideration. GUIDELINES: Medical Necessity Criteria - Must satisfy any of the following: I - VI
I. The member’s physical status is classified as ASA III – VI per the American Society of
Anesthesiologists Physical Status Classification System (see Attachment A); or
II. The member is less than or equal to 17 years of age; or
III. The member requires prolonged or therapeutic endoscopy; or
IV. The member has a documented neurologic, psychological, or developmental disorder requiring the need for deeper sedation to achieve procedure compliance; or
V. The member has a history any of the following: A - C
A. Prescribed or illicit benzodiazepine or opioid use; or
B. Other illicit drug use; or
C. Heavy alcohol use.
VI. The member has failed previous moderate (conscious) sedation for routine endoscopic procedure(s). EXCLUSIONS (not limited to): Refer to member’s Certificate of Coverage or Summary Plan Description. DEFINITIONS: Minimal sedation (anxiolysis): Is an induced state of altered cognition whereby cognitive function and coordination may be impaired, but airways remain patent (ie, open/unobstructed) and protective airway reflexes remain intact. The patient is
Department of Origin: Integrated Healthcare Services
Effective Date: 06/09/21
Approved by: Medical Policy Quality Management Subcommittee
Date Approved: 06/08/21
Clinical Policy Document: Anesthesia Services for Routine Screening and Diagnostic Gastrointestinal Endoscopic Procedures
Replaces Effective Clinical Policy Dated: 06/24/20
Reference #: MC/G013
Page: 2 of 4
also able to maintain a normal response to verbal commands and physical stimulation. Sedatives that induce minimal sedation include, but are not limited to, benzodiazepines (eg, diazepam [Valium]; lorazepam [Ativan]), GABA agonists (zolpidem [Ambien®]; zopiclone [Imovane®]. Moderate (conscious) sedation: Is an induced state of sedation characterized by a minimally depressed consciousness such that the patient is able to continuously and independently maintain a patent airway, retain protective reflexes, and remain responsive to verbal commands and physical stimulation. Drugs that induce moderate sedation include, but are not limited to, combination benzodiazepine (eg, midazolam [Versed®]) and an opioid (eg, Fentanyl). Monitored anesthesia care (MAC): May include varying levels of sedation, anxiolysis, and analgesia. Based on the American Society of Anesthesiologists' (ASA) standard for monitoring, MAC is to be provided by qualified anesthesia personnel who provide or medically direct a number of specific services such as administration of sedatives, analgesics, hypnotics, anesthetic agents or other medications as necessary. Anesthesia care becomes general anesthesia if the patient loses consciousness and the ability to respond purposefully. Monitored anesthesia (deep sedation): Is an induced state of sedation characterized by depressed consciousness such that spontaneous ventilation may be inadequate. The patient is unable to continuously and independently maintain a patent airway and experiences a partial loss of protective reflexes and ability to respond to verbal commands or physical stimulation. Drugs that induce deep sedation include, but are not limited to, propofol (Diprivan®) or dexmedetomidine (Precedex™). General anesthesia: Is a drug-induced loss of consciousness whereby patients are not arousable even with painful stimulation. The ability to independently maintain ventilatory function is often impaired. Patients often require assistance in maintaining a patent airway and ventilation may be required. Cardiovascular function may also be impaired. Drug administration can be either via intravenous injection (IV) or inhalation induction. Commonly used IV agents include etomidate, ketamine, sodium thiopental, and propofol. A commonly-used agent for inhalation induction is sevoflurane.
Department of Origin: Integrated Healthcare Services
Effective Date: 06/09/21
Approved by: Medical Policy Quality Management Subcommittee
Date Approved: 06/08/21
Clinical Policy Document: Anesthesia Services for Routine Screening and Diagnostic Gastrointestinal Endoscopic Procedures
Replaces Effective Clinical Policy Dated: 06/24/20
Reference #: MC/G013
Page: 3 of 4
Prior Authorization: No REFERENCES: 1. Integrated Healthcare Services Process Manual: UR015 Use of Medical Policy and Criteria 2. Clinical Policy: MP/C009 Coverage Determination Guidelines 3. American Society of Anesthesiologists (ASA). ASA Physical Status Classification System. Last
Amended: 12/13/20. Retrieved from http://www.asahq.org/quality-and-practice-management/standards-guidelines-and-related-resources/asa-physical-status-classification-system. Accessed 04-02-21.
4. Calderwood AH, et al. American Society for Gastrointestinal Endoscopy (ASGE). Guidelines for safety in the gastrointestinal endoscopy unit. Gastrointest Endosc 2014;79:363-372. Retrieved from https://www.asge.org/home/resources/key-resources/guidelines. Accessed 04-02-21.
5. Cohen J. Gastrointestinal endoscopy in adults: procedural sedation administered by endoscopists. (Topic 2567, Version 24.0; last updated: 05/08/20). In: Robson KM, ed. UpToDate. Waltham, Mass.: UpToDate; 2020. 2018. www.uptodate.com. Accessed 04-02-21.
6. Goudra B. Anesthesia for gastrointestinal endoscopy in adults. (Topic 105511, Version 18.0; last updated: 12/15/20) In: Crowley M, ed. UpToDate. Waltham, Mass.: UpToDate; 2020. www.uptodate.com. Accessed 04-02-21.
DOCUMENT HISTORY: Created Date: (previously MP/A007) 04/22/20 Reviewed Date: 04/02/21 Revised Date:
Department of Origin: Integrated Healthcare Services
Effective Date: 06/09/21
Approved by: Medical Policy Quality Management Subcommittee
Date Approved: 06/08/21
Clinical Policy Document: Anesthesia Services for Routine Screening and Diagnostic Gastrointestinal Endoscopic Procedures
Replaces Effective Clinical Policy Dated: 06/24/20
Reference #: MC/G013
Page: 4 of 4
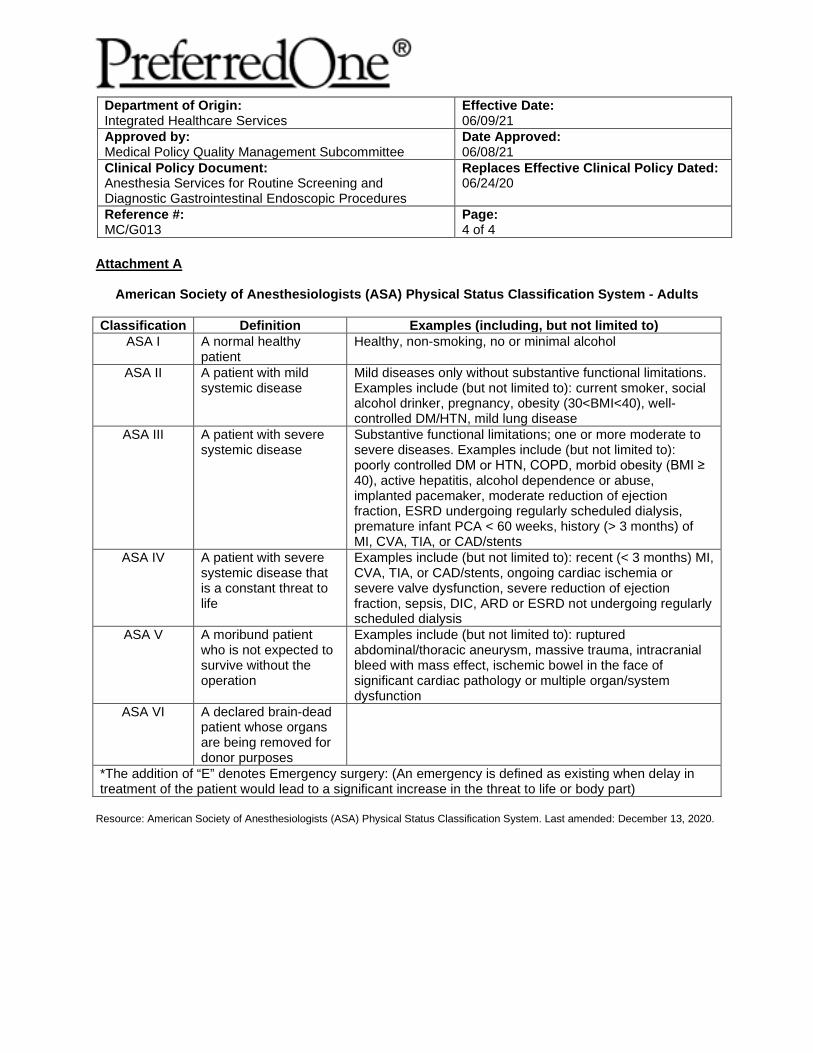
Attachment A
American Society of Anesthesiologists (ASA) Physical Status Classification System - Adults
Classification Definition Examples (including, but not limited to)
ASA I A normal healthy patient
Healthy, non-smoking, no or minimal alcohol
ASA II A patient with mild systemic disease
Mild diseases only without substantive functional limitations. Examples include (but not limited to): current smoker, social alcohol drinker, pregnancy, obesity (30<BMI<40), well-controlled DM/HTN, mild lung disease
ASA III A patient with severe systemic disease
Substantive functional limitations; one or more moderate to severe diseases. Examples include (but not limited to): poorly controlled DM or HTN, COPD, morbid obesity (BMI ≥ 40), active hepatitis, alcohol dependence or abuse, implanted pacemaker, moderate reduction of ejection fraction, ESRD undergoing regularly scheduled dialysis, premature infant PCA < 60 weeks, history (> 3 months) of MI, CVA, TIA, or CAD/stents
ASA IV A patient with severe systemic disease that is a constant threat to life
Examples include (but not limited to): recent (< 3 months) MI, CVA, TIA, or CAD/stents, ongoing cardiac ischemia or severe valve dysfunction, severe reduction of ejection fraction, sepsis, DIC, ARD or ESRD not undergoing regularly scheduled dialysis
ASA V A moribund patient who is not expected to survive without the operation
Examples include (but not limited to): ruptured abdominal/thoracic aneurysm, massive trauma, intracranial bleed with mass effect, ischemic bowel in the face of significant cardiac pathology or multiple organ/system dysfunction
ASA VI A declared brain-dead patient whose organs are being removed for donor purposes
*The addition of “E” denotes Emergency surgery: (An emergency is defined as existing when delay in treatment of the patient would lead to a significant increase in the threat to life or body part)
Resource: American Society of Anesthesiologists (ASA) Physical Status Classification System. Last amended: December 13, 2020.
PreferredOne Community Health Plan (“PCHP”) complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. PCHP does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
PCHP:Provides free aids and services to people with disabilities to communicate effectively with us, such as:
• Qualified sign language interpreters• Written information in other formats (large print, audio, accessible electronic formats, other formats)
Provides free language services to people whose primary language is not English, such as:• Qualified interpreters• Information written in other languages
If you need these services, contact a Grievance Specialist.
If you believe that PCHP has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with:
Grievance SpecialistPreferredOne Community Health PlanPO Box 59052Minneapolis, MN 55459-0052Phone: 1.800.940.5049 (TTY: 763.847.4013)Fax: [email protected]
You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, a Grievance Specialist is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services200 Independence Avenue, SWRoom 509F, HHH BuildingWashington, D.C. 202011-800-368-1019, 800-537-7697 (TDD)
Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
PreferredOne Community Health Plan Nondiscrimination Notice
Language Assistance Services
NDR PCHP LV (10/16)
PreferredOne Insurance Company (“PIC”) complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. PIC does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
PIC:Provides free aids and services to people with disabilities to communicate effectively with us, such as:
• Qualified sign language interpreters• Written information in other formats (large print, audio, accessible electronic formats, other formats)
Provides free language services to people whose primary language is not English, such as:• Qualified interpreters• Information written in other languages
If you need these services, contact a Grievance Specialist.
If you believe that PIC has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with:
Grievance SpecialistPreferredOne Insurance CompanyPO Box 59212Minneapolis, MN 55459-0212Phone: 1.800.940.5049 (TTY: 763.847.4013)Fax: [email protected]
You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, a Grievance Specialist is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services200 Independence Avenue, SWRoom 509F, HHH BuildingWashington, D.C. 202011-800-368-1019, 800-537-7697 (TDD)
Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
PreferredOne Insurance Company Nondiscrimination Notice
Language Assistance Services
NDR PIC LV (10/16)





























