Embed Size (px)
Citation preview

Therapeutic drug monitoring
Department of Clinical Pharmacology,
Wrocław Medical University

Therapeutic index
concentration range characterized by a
high efficacy of action and low risk of
upper toxic symptoms
The essence of therapeutic drug
monitoring with drug
concentration
relationship between the pharmacological
activity and drug concentration in blood
or in other available biological material

Therapeutic Drug Monitoring – TDM
action leading to achieve such a dosage of
the drug in a patient that the obtained
levels of concentration remain within the
therapeutic range
Factors conditioning the
efficacy of therapeutic drug
monitoring
the use of pharmacokinetic rules
combined analysis of obtained results and
clinical status of the patient
verification of pharmacological activity of
administered drugs by means of other
methods

Criteria for the selection of drugs
for monitoring
low therapeutic index
dangerous toxic effects of the drug and
unnoticeable clinical effect
close interrelationship between the drug
concentration and its activity
administration in a long-term therapy

Criteria for the selection of drugs
for monitoring – continuation
the use in life-threatening diseases
significant individual differences in the
range of pharmacokinetics
non – linear pharmacokinetics
high distribution coefficient
Basic clinical indications
for the use of therapeutic drug
monitoring
lack of the expected result of therapy or
occurrence of unexpected toxic symptoms
in spite of the administered dosage scheme
Basic clinical indications for
the use of therapeutic drug
monitoring - continuation
lack of the possibility of adequate clinical
or laboratorial control of the efficacy and
power of the pharmacological effect of a
drug, especially in long – lasting therapy
and in the prophylactic use

Basic clinical indications for
the use of therapeutic drug
monitoring – continuation
pathological conditions in which
symptoms associated with unsuccessfully
treated disease are the same as toxic
symptoms of the drug’s effect

Basic clinical indications for
the use of therapeutic drug
monitoring – continuation
individual pharmacokinetic differences
depend on the age and genotype of the
patient
Basic clinical indications
for the use of therapeutic drug
monitoring – continuation
coincidence of diseases in organs
responsible for the drugs in the organism
(renal failure, severe liver diseases,
gastrointestinal diseases, pathological states
in hypo or dysproteinemia, disturbances in
water and electrolyte balance and acid-base
balance)

Basic clinical indications for
the use of therapeutic drug
monitoring – continuation
concomitant administration of other
drugs, especially if there is a possibility of
interaction between them

Basic clinical indications for
the use of therapeutic drug
monitoring – continuation
protection against toxic effects of some
drugs especially administered at high
doses to achieve better therapeutic action
of drug (calcium folinate + methotrexate)

Basic clinical indications for the
use of therapeutic drug
monitoring – continuation
estimation of the therapeutic value of new drugs
Rules for rational
pharmacotherapy based on
measurements of blood serum
drug concentration
development of such a dosage scheme of the
drug that in a study state its concentration
remains between the minimal active and the
minimal toxic concentrations

Factors changing drug kinetics
concomitant diseases – specially renal and
liver diseases, alimentary tract disease,
thyroid disease, disturbances in protein
binding
receptors’ reactivity
concomitant administration of other drugs
and interaction of drugs
Factors changing drug kinetics
- continuation
genetic – genotype, sex and age determine
the individual variability
improper dosage administration
poor bioavailability of drugs
environmental factors, especially tobacco
smoking

Factors changing drug kinetics
– continuation
tbe use of drugs by patients incompatible
with doctor’s prescription
analytical disturbances, e.g.: the presence of
Digoxin – Like Immunoreactive Substance –
DLIS in serum
Genetically directed
therapeutic monitoring
concomitant use of pharmacogenetics and
traditional therapeutic monitoring of drugs
concentrations in the organism to increase
the efficacy and safety of pharmacotherapy

Genetically directed therapeutic
monitoring - continuation
patient’s genotype and phenotype estimation
before initiation of treatment allows a priori
dose modification of such drugs as:
mercaptopurine, tioguanine, fluorouracil,
azathioprine, trastusumab, irinotecan,
tricyclic antidepressants, antiarrhythmic

Timing of blood sampling for the
estimation of drug concentration
after achieving the steady state
before administration of another dose of the
drug, especially in the morning (minimal drug
concentration, Cmin – through concentration)

Timing of blood sampling for the
estimation of drug concentration
– continuation
in rare cases during administration of toxic
drugs, e.g. aminoglycoside antibiotics –the
estimation of maximal concentration (Cmax –
peak concentration) is recommended

Recommendations for the
estimation of free level of drug
concentration
diseases of the liver and kidney with
associated hypoalbuminemia
concomitant use of therapeutic substances
with concurrent displacement of the other
drugs from serum protein bindings

Recommendations for the
estimation of free level of drug
concentration – continuation
non – linear serum protein binding (salicylates, prednisolon, phenylobutazone, theophylline, disopyrimide)
increase of acid – α–1–glycoprotein level in some pathological conditions, e.g. myocardial infarction

Calculation of changed dose or
changed dose interval for drugs
undergoing linear pharmacokinetics
indicated drug concentration Changed = Former x
________________________________________
dose dose estimated drug concentration
Changed Former estimated dose interval dose = dose x _________________________
interval interval indicated dose interval
Drugs whose administration is based
on therapeutic drug monitoring:
cardiac glycosides (digoxin, digitoxin)
antiarrhythmic drugs (amiodarone,
disopyramide, flecainide, lidocaine,
procainamide, propafenone, propranolol)
antiepileptic drugs (phenytoine,
phenobarbital, carbamazepine,
primidone, ethosuximide, valproic acid)

Drugs whose administration
is based on therapeutic drug
monitoring – continuation:
tricyclic antidepressant drugs (amitriptyline,
desipramine, imipramine, norptriptyline)
lithium
aminoglycosides antibiotics (gentamycin,
tobramycin, netilmycin, amikacin, dibecacin,
streptomycin, kanamycin)
Drugs whose administration
is based on therapeutic drug
monitoring – continuation:
theophylline
methotrexate
cyclosporine
tacrolimus

Therapeutic concentration
range of cardiac glycosides
digoxin 0,8 – 2,0 μg/l
digitoxin 10 – 25 μg/l
Indications for therapeutic
monitoring of cardiac glycosides
divergence between expected, based on rational premises, and obtained effect of therapy
patient’s clinical condition restricting correct evaluation of complications after administration of cardiac glycosides
pregnancy
lactation
Indications for therapeutic
monitoring of cardiac glycosides
– continuation
diseases of the liver, kidneys, hypo and
hyperthyroidaemia, hypoalbuminaemia
concomitant administration of drugs
increasing the digoxine concentration in
plasma by about 60 – 300% (amiodarone,
diltiazem, quinidine, verapamil, nifedipine,
indomethacin, spironolactone, gentamycin,
tetracyclines, cefradine, erythromycin)

Therapeutic concentration range of
quinidine 2 – 5 mg/l

Indications for therapeutic
monitoring of antiarrhythmic drugs –
quinidine
cirrhosis, hypoproteinemia, circulatory insufficiency, renal insufficiency
age (infants)
concomitant administration of other drugs increasing quinidine concentration (cimetidine, itraconazole, katoconazole, ciprofloxacin, metronidazole, erythromycin, clarythromycin, fluvoxamine)

Therapeutic concentration range of
procainamide 4 – 10 mg/l
Indications for therapeutic
monitoring of antiarrhythmic drugs –
procainamide
genetically determined acetylation
polymorphism to active pharmacological
metabolite
N – acetylo – procainamide
kidney insufficiency
high individual variability of processes:
adsorption, distribution, metabolism

Therapeutic concentration range of
lidocaine 1,5 – 5 mg/l
Indications for therapeutic
monitoring of antiarrhythmic drugs
– lidocaine
Pathological conditions, in which liver blood
supply decreases (congestive heart failure,
cardiac shock)
concomitant use of drugs increasing the
lidocaine concentration (propanolol,
mexiletine, cimetidine)
drug infusion lasting longer than 24h

Therapeutic concentration range of
propafenone 42 – 1679 μg/l
Indications for therapeutic
monitoring of antiarrhythmic
drugs – propafenone
genetically determined oxidation
polymorphism
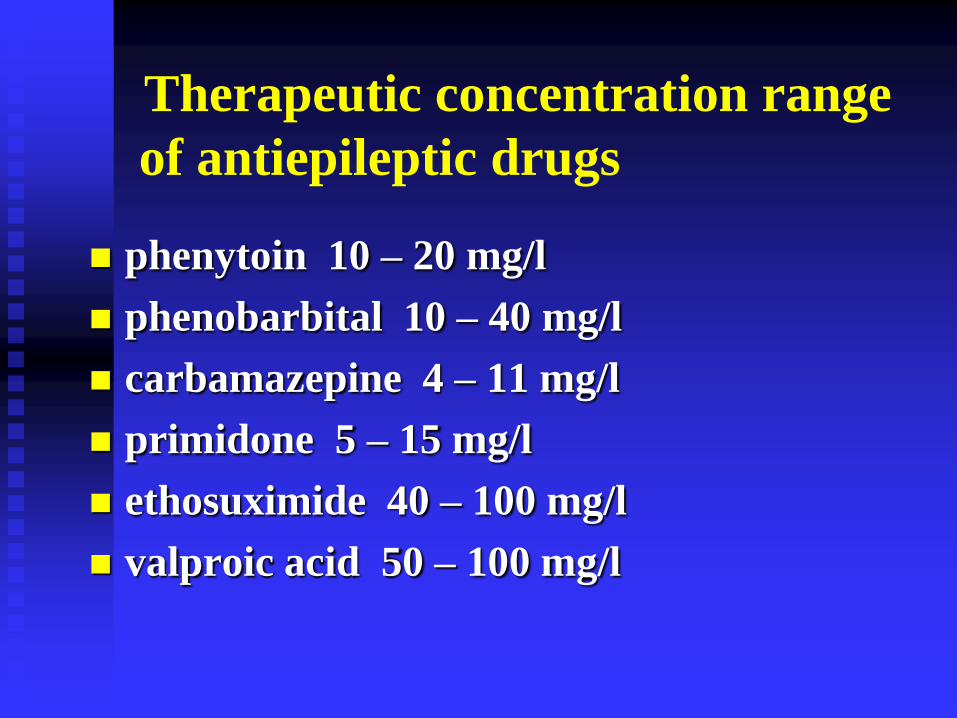
Therapeutic concentration range
of antiepileptic drugs
phenytoin 10 – 20 mg/l
phenobarbital 10 – 40 mg/l
carbamazepine 4 – 11 mg/l
primidone 5 – 15 mg/l
ethosuximide 40 – 100 mg/l
valproic acid 50 – 100 mg/l

Indications for therapeutic drug
monitoring of antiepileptic drugs
narrow therapeutic index of antiepileptic
drugs

Indications for therapeutic drug
monitoring of antiepileptic drugs –
continuation
failure of monotherapy because of too
low concentration of drug as an effect of:
non – compliance of patient to doctor’s
recommendations
adsorption disturbances
pharmacokinetic changes caused by
external and internal factors
Indications for therapeutic drug
monitoring of antiepileptic drugs –
continuation
Occurrence of undesired drug effects
during antiepileptic therapy associated
with:
concomitant liver, renal diseases and other
pathological conditions which are
associated with the loss of protein,
especially albumins

Indications for therapeutic drug
monitoring of antiepileptic drugs
– continuation
Occurrence of undesired drug effects during
antiepileptic therapy associated with:
concomitant administration of other drugs
decreasing the antiepileptic drugs
concentration (erythromycin, klarythromycin
+ carbamazepine)

Indications for therapeutic drug
monitoring of antiepileptic drugs
– continuation
Occurrence of undesired drug effects during
antiepileptic therapy associated with:
concomitant administration of some
antiepileptics increasing their concentration
(valproic acid + phenytoine)
Indications for therapeutic drug
monitoring of antiepileptic drugs –
continuation
early age (premature infants, infants)
pregnant women with epilepsy
(concentration of free fraction of phenytoine,
karbamazepine, valproic acid increases in
the third trimester )
non – linear kinetics (phenytoine)

Therapeutic concentration range
of tricyclic antidepressants:
amitriptyline 120 – 250 μg/l
desipramine 125 – 300 μg/l
imipramine 150 – 250 μg/l
nortriptyline 50 – 150 μg/l
fluoxetine 100 – 800 μg/l

Indications for therapeutic drug
monitoring of tricyclic
antidepressants
narrow therapeutic index, lack of satisfactory clinical effect and increase of depression
genetically determined oxidation polymorphism
occurrence of undesired drugs effects
administration of high doses of antidepressants

Indications for therapeutic drug
monitoring of tricyclic
antidepressants – continuation
suspicion of lack of cooperation between
patient and doctor
diseases of the heart, liver and kidneys
advanced age
overdosage or suspicion of drug poisoning

Indications for therapeutic drug
monitoring of tricyclic
antidepressants – continuation
Possibility of interactions
(drugs and other substances increasing
the tricyclic antidepressant drugs –
cimetidine, haloperidol, phenothiazines –
cosegregates, chloramphenicol,
fluconazole, verapamil, diltiazem,
propafenone, quinidine, ritonavir, oral
contraceptives)

Therapeutic concentration range of
Lithium 0,3 – 1,3 mmol/l

Indications for therapeutic drug
monitoring of lithium
high nephro – and neurotoxicity
concomitant administration of other drugs increasing the cardiotoxicity of lithium preparations (thiazide diuretics, monosteroidal anti-inflammatory drugs, general anaesthetics)
coexistence of other diseases
pregnancy

Therapeutic concentration range
of aminoglycosides
amikacin 20 – 30 mg/l
gentamycin 5 – 12 mg/l
dibekacin 5 – 12 mg/l
netylmycin 5 – 12 mg/l
tobramycine 5 – 12 mg/l
streptomycin 15 – 40 mg/l
vankomycin 20 – 40 mg/l

Indications for therapeutic drug
monitoring of aminoglycosides
narrow therapeutic index
high oto- and nephrotoxicity
administration of other oto- and
nephrotoxic drugs
age-dependent differences in toxicity
Indications for therapeutic drug
monitoring of aminoglicosides –
continuation kidney insufficiency
therapy with high doses
hypovolemia
insufficiency of kidneys and hearing in the history
repeated therapy of aminoglycosides
the use in peritoneal dialysis, hemodialysis patients and patients with kidney’s transplantation

Therapeutic concentration range of
theophylline 8 – 20 mg/l

Indications for therapeutic drug
monitoring of theophylline
difficult to anticipate relationship between
standard daily dose of the drug and its
serum concentration in some patients
narrow therapeutic index
high individual variations in drug
elimination, especially in biotransformation
of the drug even in patients with efficient
liver
Indications for therapeutic drug
monitoring of theophylline –
continuation
pathological conditions (diseases of the liver
and kidneys)
patient’s age (infants, elderly people)
tobacco smoking
diet
consumption of high amounts of fat
high – protein and low – carbohydrate diet

Indications for therapeutic drug
monitoring of theophylline –
continuation
concomitant administration of other drugs and
substances increasing the theophylline
concentration (macrolides antibiotics,
fluoroquinolones, cimetidine, zileuton, oral
contraceptives)
concomitant administration of other drugs and
substances decreasing the theophylline
concentration (barbiturates, rifampicin,
phenytoin, preparations of Hypericum perforatum
Indications for therapeutic drug
monitoring of methotrexate
administration of methotrexate in high doses with
calcium folinate
coexistence of kidneys and liver failure, the
presence of exudation in body cavities
concomitant administration of other drugs
increasing the toxicity of methotrexate (salicylates,
sulphonamides, probenecid, non – steroidal anti –
inflammatory drugs, cefalothin, penicillin,
aminoglycosides antibiotics, cisplatin,
cyclosporine)

Therapeutic concentration range of
cyclosporine
inductive therapy: 150 – 350 ng/l
sustaining therapy: 100 – 250 ng/l

Therapeutic concentration range of
tacrolimus
0,2 – 2,0 μg/l (serum)
4 – 40 μg/l (whole blood)

Indications for therapeutic drug
monitoring of immunosuppressive
drugs cyclosporine, tacrolimus
low therapeutic index
high pharmacokinetic variability in– and
intra individually
frequent administration of drugs in
severely ill patients

Indications for therapeutic drug
monitoring of immunosuppressive
drugs cyclosporine, tacrolimus –
continuation
the possibility of determination of the risk
of transplant rejection or nephrotoxic
action of the drug
interaction between concomitantly used
drugs
verification of cooperation of the patient
and the doctor
Benefits associated with therapeutic
concentration drug monitoring
increasing the efficacy and safety of
administered drugs
possibility of tailoring individual patient’s
dosage
possibility of quick doctor’s intervention in
case of changing clinical condition of the
patient
Benefits associated with therapeutic
concentration drug monitoring –
continuation
decrease in the incidence of undesired drug
reactions
possibility of drug administration in high
doses
possibility of detection of imminent risk of
undesired reactions before their clinical
appearance

Benefits associated with therapeutic
concentration drug monitoring –
continuation
possibility of checking patient’s
compliance with the doctor’s
recommendations
shortening of therapy time
decrease of the cost of therapy





























