Embed Size (px)
Citation preview

SMI857A 22/6/2000 14:08 Page 233
Dental students in NorthernIre land in 1992 and 1995:changing trends inpsychological stress
Ruth Freeman1,*,{, PhD MSc MMedSc[psych] BDS DDPH.RCS, Ryan L. Lindner1,2,BA DDS, James Rooney1, BDS and Sena Narendran2, MSc BDS DDPH.RCS
1Dental Public Health Research Group, Queen's University of Belfast, Belfast,Northern Ireland, UK2Department of Health Promotion, University of Texas Health Science Center at Houston,Houston, TX, USA
SummaryThe political violence which took place in Northern Ireland was hypothesised (Fraser, Brit. J. Psychiat.1971; 118: 257±264; Lyons, Brit. J. Psychiat. 1971; 118: 265±273; Lyons, J. Psychosomat. Res. 1979;23: 373±393) to increase psychological stress in its population. This assumption led to the validity ofwork conducted in 1992 to assess Belfast dental students' stress to be questioned by researchers. Anidentical survey of clinical students was conducted in 1995, during the 1994±96 cease-®re in order tocompare this additional cohort with the original cohort of clinical students' ( from 1992) psychologicalstress. One hundred and seventy-nine students, in total, completed the occupational stress indicator.The results showed that there was no effect of year or the interaction of gender by year for sources ofstress, type A behaviour, social support, health behaviours or stress outcomes. The main effect ofgender explained differences in social support, alcohol consumption and the outcomes of stress (iephysical and mental ill-health). The ®ndings suggest that social support, cohesiveness and groupidentity may act to contain the psychological stress associated with the political violence in NorthernIreland. Copyright # 2000 John Wiley & Sons, Ltd.
Key Words
psychological stress; dental students; politicalviolence; Northern Ireland
Introduction
The political violence, vernacularly known as`troubles', started in Northern Ireland in 1969. Atthat time rioting in the streets, shootings andbombs were commonplace. Concerns about howthe people living in the most affected areas wouldcope with the real dangers led to a series ofpapers1±3 on the effects of political violence uponmental health. Little differences in the pre-valence of mental illness were shown,2,3 withincreases in the prescription of tranquillisers and
S t r e s s M e d i c i n eStress Med. 16: 233±238 (2000)
Copyright # 2000 John Wiley & Sons, Ltd. Received 14 September 1999Accepted 3 November 1999
*Correspondents to: Dr R Freeman, Dental PublicHealth Research Group, Division of Paediatric, Pre-ventive and Public Health Dentistry, School of ClinicalDentistry, Queen's University of Belfast, GrosvenorRoad, Belfast BT12 6BP, Northern Ireland, UK. Tel:�44-1232-240503, ext. 3827. Fax: �44-1232-438861.{E-mail: [email protected]

SMI857A 22/6/2000 14:08 Page 234
antidepressants being linked to the increase in thepopularity of these medications throughout theUK in the 1970s.1
More recent research4,5 has supported theseearly ®ndings. For instance, adolescents residentin Northern Ireland with greater social supportdiffered little in their mood when compared tothose in the rest of the UK. Similarly, people fromcommunities within Northern Ireland, which hadhigh social cohesiveness, tended to have bettermental health compared with people who weresocially isolated.
The relationship between political violence andpsychological stress does not appear to be asimple one. Although political violence acted as acontributing factor, for those with a propensityfor depressed mood or high anxiety states, theextent to which political violence affected thepsychological health of the Northern Irelandpopulation, as a whole, remained unclear. Infact, it seemed that social cohesiveness in terms ofgroup identity6 assisted in the containment of thepsychological stress associated with the politicalviolence of Northern Ireland.
The idea that social cohesiveness within thehome/family environment buffered the effects ofwork stress has also been investigated in under-graduate dental and medical students.7,8 Studentswith greater social support experienced lowerlevels of psychological stress. Furthermore, whenthese students were exposed to urban violencethose with less social and home/family supportexperienced greater psychological stress.7
While research has studied the in¯uence ofviolent crime7 upon the lives of dental students,the constant threat of political violence upondental students' psychological stress has not beenstudied. In this respect Northern Ireland is in aunique situation. A group of young people, whogrew up under the threat of constant urban unrestand political violence, is comprised of thestudents who attend the School of ClinicalDentistry at the Queen's University of Belfast(QUB). Ninety-six per cent of dental students atQUB come from homes across Northern Ireland.Ninety-three per cent of clinical students eitherlive in accommodation which is in the vicinity ofthe dental school or live with their families inBelfast. The remaining 7 per cent live outside thecity boundaries and travel daily to the dentalschool.
In an attempt to examine the psychologicalstress in clinical dental undergraduates at QUB asurvey was conducted in 1992. At this time, thepeace process had not yet begun and concernswere raised that the data collection simplyre¯ected a collective, generalised anxiety associ-ated with the political violence. Despite the®nding that the 1992 survey suggested that maleand female dental students coped with andreacted to stress in different ways,9 the fact thatthe research took place in Northern Irelandnulli®ed the hypothesis that gender differencesexisted. An identical survey in 1995, during the1994±96 cease-®re, was planned to investigatethis area further. It was hypothesised that the1995 cohort of clinical students would have lowerlevels of stress and have better physical andpsychological health compared with the 1992clinical students. The aim of this work, therefore,was to examine the role of political violence uponclinical dental students' psychological stress. Theobjectives were to compare the 1992 and 1995cohort of clinical students for their stated sourcesof stress, coping strategies, stress outcomes andhealth behaviours.
Materials and Methods
The sample
In 1992 and 1995 all the dental students from thethree clinical years were invited to participate.The reason for targeting clinical students asopposed to pre-clinical students was related tothe fact that the School of Clinical Dentistry isgeographically located in an area which has seenthe worst ravages of the political violence. Thepre-clinical students have their classes at the mainuniversity campus and would not have experi-enced the daily threat of political violencecompared with their clinical colleagues. Thetwo cohorts of clinical students contained differ-ent people. The ®rst year clinical students in 1992had quali®ed by 1994 prior to the second datacollection in 1995. The clinical students wereassured that their responses would be treated incomplete con®dence.
The questionnaires
The ®rst questionnaire administered was theOccupational Stress Indicator (OSI).10 This
R. Freeman et al.
234 Copyright # 2000 John Wiley & Sons, Ltd. Stress Med. 16: 233±238 (2000)

SMI857A 22/6/2000 14:08 Page 235
inventory was developed from a theoreticalmodel to explain stress and has been shown tohave high content, construct and empiricalvalidity, as well as high internal consistency ofsub-scales and test±retest reliabilities (see OSImanual, pp. 55±59).10 The OSI was chosenbecause it contains elements which examinesources of stress, both intrinsic (work-related)and extrinsic (home/family-related) to the work-ing environment. The OSI assesses social contactas a coping strategy and physical and mental ill-health as indicators of psychological stress.Physical ill-health is measured on a six-pointscale: questions include `inability to get to sleepor stay asleep', `decrease in appetite', `ingestionor sickness', etc. Mental ill-health is also assessedon a six-point scale. Questions in this part of theinventory relate to changes in mood, ability torelax, inappropriate anxieties and worries, etc.
The OSI assesses stress within the 3-monthperiod prior to completion of the inventory10,11
and assesses sources of stresses associated withthe home environment. Both of these propertiesof the OSI allowed the stresses of living andstudying in Belfast to be realised. Four speci®cgroups of questions were used in the study. Thesewere sources of stress related to the `job of being adental student' (work environment) and thehome/family environment, the personality traitType A behaviour, the copying strategy socialsupport and current physical and mental ill-health. All questions were presented as six-pointLikert scales and scored in accordance with theOSI scoring frame.
Additional questions assessing the students'demography and health behaviours wereincluded.12 Students were asked about theirsmoking habits and alcohol consumption. Ofthose students who reported that they drankalcohol (af®rmed by all students in both cohorts)the frequency of alcohol consumption wasassessed using a four-point scale. The scoresranged from `drink only on special occasions'(scoring 1) to `drink at least daily' (scoring 4).
Administration of the questionnaires
The questionnaires were administered to the1992 and 1995 cohorts during the second halfof the winter semester. This time was chosen as it
is a quiet time with regard to the dental studentssitting professional examinations or class tests.An identical protocol was used for the adminis-tration of the questionnaires in both 1992 and1995. The dental students were invited tocomplete the questionnaires during a lunch-timebreak in the lecture hall under `examinationconditions'. They were instructed to place theircompleted questionnaires in the sealed envelopeprovided. The sealed envelopes were collectedafter the last student had ®nished.
Coding of the questionnaire and statisticalanalysis
After all the questionnaires had been scored,10 per cent were randomly chosen to verify thedata. A 3 per cent error was found, and so all ofthe data were recalculated and errors corrected.Once completed, the data were entered onto amicrocomputer.
The data were analysed using analysis of vari-ance to investigate differences between the samplepopulations in 1992 and 1995. In additionchi-squared, Mann±Whitney U and correlationanalyses were undertaken to investigate relation-ships between gender, Type A behaviour, healthbehaviours and social support with stress out-comes. The alpha level was set to the conven-tional 5 per cent level.
Results
The sample
In 1992, 84 questionnaires were administered tothe dental students, of which 80 were returned(response rate of 95 per cent). In 1995, 100questionnaires were administered to the dentalstudents of which 99 were returned (response rateof 99 per cent). Fifty per cent of men and womentook part in the study of both 1992 and 1995(w2 � 0.00: p � 1.00). There was no signi®cantdifference in the mean age of the students in 1992(22.00+1.92) compared with that in 1995(21.75+1.94), (t � 0.86 : p4 0.05). Three percent of students both in 1992 and 1995 weremarried.
Dental students in Northern Ireland in 1992 and 1995
Copyright # 2000 John Wiley & Sons, Ltd. Stress Med. 16: 233±238 (2000) 235
SMI857A 22/6/2000 14:08 Page 236
Comparisons of personality, sources of stress,coping strategies and stress outcomes byyear and gender
The mean score for Type A behaviour for the1992 cohort was 48.16 (+5.94) compared with48.67 (+6.20) for the 1995 students. Thenormative value for Type A behaviour is 51.15(+7.63).13 Analysis of variance was employedwhich showed that there were no main effects foryear, gender or the interaction of year by gender.The mean scores for the source of stress, workenvironment, for the 1992 cohort was 33.12(+6.73) compared with 33.25 (+5.92) for the1995 students. The mean scores for the source ofstress, home/family environment, for the 1992cohort was 36.71 (+10.89) compared with38.87 (+12.02) for the 1995 students. Therewere no main effects for either source of stress byyear, gender or the interaction of year by gender.
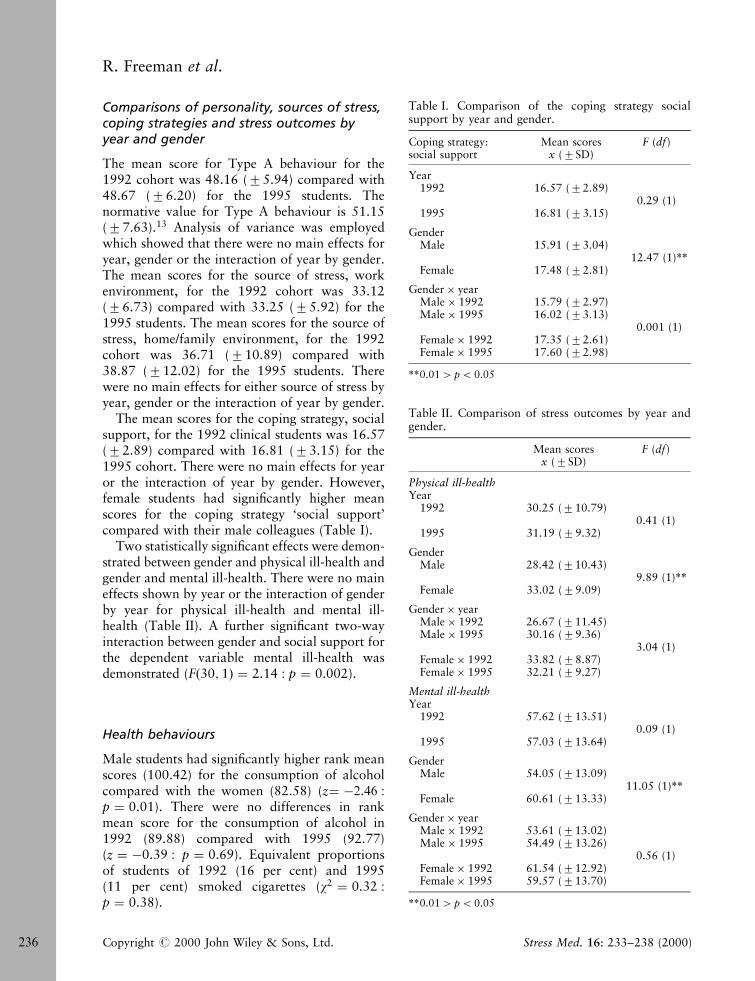
The mean scores for the coping strategy, socialsupport, for the 1992 clinical students was 16.57(+2.89) compared with 16.81 (+3.15) for the1995 cohort. There were no main effects for yearor the interaction of year by gender. However,female students had signi®cantly higher meanscores for the coping strategy `social support'compared with their male colleagues (Table I).
Two statistically signi®cant effects were demon-strated between gender and physical ill-health andgender and mental ill-health. There were no maineffects shown by year or the interaction of genderby year for physical ill-health and mental ill-health (Table II). A further signi®cant two-wayinteraction between gender and social support forthe dependent variable mental ill-health wasdemonstrated (F�30; 1� � 2.14 : p � 0.002).
Health behaviours
Male students had signi®cantly higher rank meanscores (100.42) for the consumption of alcoholcompared with the women (82.58) (z� ÿ2.46 :p � 0.01). There were no differences in rankmean score for the consumption of alcohol in1992 (89.88) compared with 1995 (92.77)(z � ÿ0.39 : p � 0.69). Equivalent proportionsof students of 1992 (16 per cent) and 1995(11 per cent) smoked cigarettes (w2 � 0.32 :p � 0.38).
Table I. Comparison of the coping strategy socialsupport by year and gender.
Coping strategy:social support
Mean scoresx (+SD)
F (df)
Year1992 16.57 (+2.89)
0.29 (1)1995 16.81 (+3.15)
GenderMale 15.91 (+3.04)
12.47 (1)**Female 17.48 (+2.81)
Gender� yearMale� 1992 15.79 (+2.97)Male� 1995 16.02 (+3.13)
0.001 (1)Female� 1992 17.35 (+2.61)Female� 1995 17.60 (+2.98)
**0.014 p5 0.05
Table II. Comparison of stress outcomes by year andgender.
Mean scoresx (+SD)
F (df)
Physical ill-healthYear
1992 30.25 (+10.79)0.41 (1)
1995 31.19 (+9.32)
GenderMale 28.42 (+10.43)
9.89 (1)**Female 33.02 (+9.09)
Gender� yearMale� 1992 26.67 (+11.45)Male� 1995 30.16 (+9.36)
3.04 (1)Female� 1992 33.82 (+8.87)Female� 1995 32.21 (+9.27)
Mental ill-healthYear
1992 57.62 (+13.51)0.09 (1)
1995 57.03 (+13.64)
GenderMale 54.05 (+13.09)
11.05 (1)**Female 60.61 (+13.33)
Gender� yearMale� 1992 53.61 (+13.02)Male� 1995 54.49 (+13.26)
0.56 (1)Female� 1992 61.54 (+12.92)Female� 1995 59.57 (+13.70)
**0.014 p5 0.05
R. Freeman et al.
236 Copyright # 2000 John Wiley & Sons, Ltd. Stress Med. 16: 233±238 (2000)
SMI857A 22/6/2000 14:08 Page 237
Correlation analysis (Pearson product moment)demonstrated that there were signi®cant butnegative relationships between social supportand mental ill-health (r � ÿ0.15 : p5 0.05) andbetween social support and stress, work environ-ment (r � ÿ0.19 : p5 0.05). A signi®cant nega-tive relationship between social support andmental ill-health was shown for female students(r � ÿ0.26 : p5 0.01). The relationship betweensocial support and mental ill-health wasapproaching signi®cance for the male under-graduates (r � ÿ0.21 : p � 0.05). There weresigni®cant relationships between mental ill-healthand the sources of stress, work environment(r � 0.28 : p5 0.01) and home/family environ-ment (r � 0.22 : p5 0.01). No signi®cantrelationship was shown between Type A beha-viour and mental ill-health (r � 0.24 : p � 0.74).
Correlation analyses (Spearman's rho) demon-strated a signi®cant relationship between socialsupport and alcohol consumption (rs � 0.23 :p5 0.01) existed. For women students no signi®-cant association was shown between socialsupport and alcohol consumption (rs � 0.12 :p4 0.05), whereas for the men a signi®cantrelationship was demonstrated (rs � 0.21 :p5 0.05).
Discussion
Since 1969 the population in Northern Irelandhas contended with the political violence andsocial unrest known as `the troubles'. Despite theconcerns that the political violence would resultin increased psychological stress and the increaseduse of psychotrophic medication, research has notsupported these fears. Rather, it has demon-strated that in communities with high socialcohesiveness and group identity6 the effect ofviolence, in terms of psychological stress has beenlower than predicted.4
The dental students in Northern Ireland in1992 grew up and trained in a constant atmos-phere of social unrest and political violence. Itwas to be expected that their experience ofpsychological stress would be higher than thestudents who experienced 18 months of living inpeace.4,14 The aim of the work presented here wasto examine psychological stress in two cohorts ofclinical dental students in 1992 (during the
troubles) and 1995 (during the cease-®re of1994±96).
Similar, to the ®ndings of Fraser1, Lyons2,3 andDonnelly5 no differences could be shown betweenthe 1992 and 1995 clinical students' sources ofstress, Type A behaviour, coping strategies, healthbehaviours or physical and mental ill-health.Furthermore, since no relationship was shownbetween Type A behaviour and mental ill-health,the link between Type A behaviour as anunderlying cause of mental ill-health and psycho-logical stress was not supported. The main effectupon changing trends in psychological stress wasgender. Differences between male and femalestudents were shown for social support, alcoholconsumption, physical and mental ill-health.These results support the ®ndings of the 1992study.9
It may have been simplistic, on the part of theauthors, to assume that political violence wouldhave resulted in different experiences of psycho-logical stress in the two cohorts of students. Theresults showed that irrespective of the year (1992or 1995) the students' psychological stress wassimilar, therefore, alternative explanations neededto be considered. The ®rst was related to thestudents' life time experiences of growing up withpolitical violence Ð no differences between thegroups should have been expected. The studentsin 1995 were as stressed as those in 1992. In otherwords the questionnaire ®ndings simply, re¯ecteda generalised trait anxiety of people living inNorthern Ireland. However, the value of the OSIis that it assessed stress in the 3-month periodprior to completion and so other explanationshad to be sought.10
A second explanation was linked to earlierresearch ®ndings.1±5 It would seem reasonable toassume that dental students in Northern Irelandmay have developed the group characteristicsnecessary to meliorate against psychologicalstress. They used social support as a copingstrategy and would seem to have high groupidentity. Evidence for this suggestion comes fromthe correlation analyses. While acknowledgingthat the correlation analyses accounted for asmall proportion of the explained variance, theanalyses demonstrated that a relationship existedbetween social support and mental ill-health. Itwould seem that those students with good socialcontacts and support were less affected by
Dental students in Northern Ireland in 1992 and 1995
Copyright # 2000 John Wiley & Sons, Ltd. Stress Med. 16: 233±238 (2000) 237

SMI857A 22/6/2000 14:08 Page 238
intrinsic or extrinsic sources of stress. For womenstudents8 social support appeared to be an impor-tant strategy in containing psychological stressand maintaining their mental health and socialwell-being. For the men, alcohol in combinationwith social support, seemed to have an equivalenteffect in raising social cohesiveness and groupidentity, while keeping psychological stress inabeyance.
This second explanation would supportBenbow's7 view of the effects of violence uponthe experience of psychological stress in dentalstudents. He showed that those with good socialsupport coped better compared with others. In agroup of dental students, such as those in Belfast,who have good social support and high groupidentity, it would seem that they were bufferedagainst the psychological stress associated withpolitical violence. It seemed that, once more inNorthern Ireland, social support and groupidentity5,6 were central with regard to containingthe effects of psychological stress.
A third explanation must, nevertheless, beconsidered. Is it possible that the students inNorthern Ireland were able to withstand the stressof violence because people in general are moreresilient than commonly thought? This suggestionquestions the relationship between life event stressand mental ill-health by proposing that peoplemay not be so vulnerable to external stresses.Such ideas as these are supported by Andrews andTennant.15 They proposed the need to `look atfactors which may mediate between life eventstress and illness'15 and in particular the moder-ating effects of social support in the interactionbetween life event stress and mental ill-health.16
The ®ndings of this study are supported byresearch in the medical and dental literature. Itwould seem that social cohesiveness, support andgroup identity act as mediators in the stress±illness equation. The study highlights the need forfurther research not only into the role of life eventstress in the causation of mental ill-health, but
also the moderating effect of social support in thestress±illness equation.
References
1. Fraser RM. The cost of commotion: an analysis of thepsychiatric sequelae of the 1969 Belfast riots. Brit. J.Psychiat. 1971; 118: 257±264.
2. Lyons HA. Psychiatric sequelae of the Belfast riots. Brit. J.Psychiat. 1971; 118: 265±273.
3. Lyons HA. Civil violence Ð the psychological aspects.J. Psychosom. Res. 1979; 23: 373±393.
4. Cairns E, Lewis CA. Collective memories, politicalviolence and mental health in Northern Ireland. Brit. J.Psychol. 1999; 90: 25±33.
5. Donnelly M. Factors associated with depressed moodamongst adolescents in Northern Ireland. J. Commun.Appl. Psychol. 1999; 9: 47±59.
6. McKeever CF, Joseph S, McCormack J. Memory ofNorthern Irish Catholics and Protestants for violentincidents and their explanation for the 1981 hunger strike.Psychol. Rep. 1993; 73: 463±466.
7. Benbow EW. Some effects of urban violence on the lives ofdental students. J. Dent. Educ. 1994; 58: 221±224.
8. Rospenda KM, Halpert J, Richman JA. Effects of socialsupport on medical students' performances. Acad. Med.1994; 69: 496±500.
9. Lindner R, Narendran S, Freeman R. Occupational stressamong dental students: behavioural strategies. J. Dent.Res. 1993; 72: 1679.
10. Cooper CL, Sloan SJ, Williams S. Occupational StressIndicator Management Guide. NFER-Nelson: Windsor,1988.
11. Cooper CL, Clarke S, Rowbottom AM. Occupationalstress, job satisfaction and well-being in anaesthetists.Stress Med. 1999; 15: 115±126.
12. Hale R, Hudson L. The Tavistock study of young doctors:report of the pilot phase. Br. J. Hosp. Med. 1992; 47:452±464.
13. Sutherland VJ, Cooper CL. Identifying distress amonggeneral practitioners: predictors of psychological ill-healthand job dissatisfaction. Soc. Sci. Med. 1993; 37: 575±581.
14. McLernon F, Ferguson N, Cairns E. Comparison ofNorthern Irish children's attitudes to war and peace beforeand after the paramilitary cease®res. Int. J. of Behav. Dev.1997; 4: 715±730.
15. Andrews JG, Tennant C. Life events and psychiatricillness. Psychol. Med. 1978; 8: 545±549.
16. Andrews JG, Tennant C, Hewson DM, Vaillant GE. Lifeevent stress, social support, coping style and risk ofpsychological impairment. J. Nerv. Ment. Dis. 1978; 166:307±316.
R. Freeman et al.
238 Copyright # 2000 John Wiley & Sons, Ltd. Stress Med. 16: 233±238 (2000)








![SHORTSEA’96 Bergenmartrans.org/documents/2001/sssca/pfrvol2.doc · Web viewProject sponsored by the Statistical & Social Inquiry Society of Ireland. [COL92H] Coleman, M., (1992),](https://img.pdfslide.us/doc/110x75/5f229c3b2595b96bcf6c16ef/shortseaa96-web-view-project-sponsored-by-the-statistical-social-inquiry.jpg)