Embed Size (px)
Citation preview

Dental Dental Management of Management of
Patients withPatients withRheumatology Rheumatology
DisordersDisorders22

Systemic Lupus Systemic Lupus ErythematosusErythematosus
A chronic multisystem disease of A chronic multisystem disease of unknown origin that exhibits wide unknown origin that exhibits wide
variations in its clinical expression and variations in its clinical expression and disease coursedisease course
Females are affected 8-10 times more than Females are affected 8-10 times more than menmen
Average age is 31 yearsAverage age is 31 years

Signs and SymptomsSigns and Symptoms
Fever, weight loss, Fever, weight loss, arthritis, fatigue, arthritis, fatigue, and general and general malaisemalaise
Butterfly rash on Butterfly rash on the malar area and the malar area and nosenose
40-50% of patients 40-50% of patients have affected have affected kidneyskidneys
Cardiac Cardiac involvementinvolvement-Libman-sacks endocarditis -Libman-sacks endocarditis found in 50% of patients upon found in 50% of patients upon autopsyautopsy
-pericarditis, myocarditis, -pericarditis, myocarditis, endocarditis, CADendocarditis, CAD
Oral lesionsOral lesions-5-25% of patients have -5-25% of patients have affected palate, buccal affected palate, buccal mucosa, and gingivamucosa, and gingiva

SLE : Classification CriteriaSLE : Classification Criteria
1. 1. SSerositis: erositis: (a) pleuritis, or (a) pleuritis, or (b) pericarditis(b) pericarditis
2. 2. OOral ulcersral ulcers3. 3. AArthritisrthritis4. 4. PPhotosensitivityhotosensitivity
10. 10. MMalar rashalar rash11. 11. DDiscoid rashiscoid rash
5.5. B Blood/Hematologic disorder: lood/Hematologic disorder: (a) hemolytic anemia or(a) hemolytic anemia or(b) leukopenia of < 4.0 x 10(b) leukopenia of < 4.0 x 1099 (c) lymphopenia of < 1.5 x (c) lymphopenia of < 1.5 x
101099 (d) thrombocytopenia < 100 (d) thrombocytopenia < 100
X 10X 1099
6. 6. RRenal disorder: enal disorder: (a) proteinuria > 0.5 gm/24 h (a) proteinuria > 0.5 gm/24 h
or or 3+ dipstick or3+ dipstick or(b) cellular casts(b) cellular casts
7. 7. AAntinuclear antibody (positive ANA) ntinuclear antibody (positive ANA) 8. 8. IImmunologic disorders: mmunologic disorders:
(a) raised anti-native DNA (a) raised anti-native DNA antibody binding orantibody binding or(b) anti-Sm antibody or (b) anti-Sm antibody or (c) positive anti-phospholipid (c) positive anti-phospholipid antibody work-upantibody work-up
9. 9. NNeurological disorder: eurological disorder: (a) seizures or (a) seizures or (b) psychosis(b) psychosis
". ..A person shall be said to have SLE if four or more of the 11 criteria are present, serially or simultaneously, during any interval of observation."
Systemic Lupus ErythematosusSystemic Lupus Erythematosus Head and Neck ManifestationsHead and Neck Manifestations
Malar rash first sign in 50%Malar rash first sign in 50% Erythematous maculopapular eruption after sun Erythematous maculopapular eruption after sun
exposureexposure Oral ulcerationOral ulceration 3-5% nasal septum perforation3-5% nasal septum perforation Acute parotid enlargement 10%Acute parotid enlargement 10% Xerostomia 15%Xerostomia 15% Larynx and trachea involvement uncommonLarynx and trachea involvement uncommon
-Vocal Cords thickening and paralysis, -Vocal Cords thickening and paralysis, cricoarytenoid arthritis, subglottic stenosiscricoarytenoid arthritis, subglottic stenosis
Laboratory ValuesLaboratory Values
95% of patients have elevated ANA95% of patients have elevated ANA 70% of patient have antibodies 70% of patient have antibodies
directed against double-stranded directed against double-stranded DNA DNA

Medical & Dental Medical & Dental ManagementManagement
Medical ManagementMedical Management Avoid excessive exposure to sunlightAvoid excessive exposure to sunlight NSAIDS for mild active disease with NSAIDS for mild active disease with
antimalarial drugs antimalarial drugs Topical corticosteroidsTopical corticosteroids Dental ManagementDental Management Assess adrenal function for possible suppressionAssess adrenal function for possible suppression Consult with physician regarding systemic Consult with physician regarding systemic
manifestationmanifestation Assess if NSAIDS are affecting platelet functionAssess if NSAIDS are affecting platelet function

Sjogren SyndromeSjogren Syndrome
Chronic disorder characterized by immune-mediated Chronic disorder characterized by immune-mediated destruction of exocrine glandsdestruction of exocrine glands
A slowly progressive inflammatory disease affecting A slowly progressive inflammatory disease affecting primarily the exocrine glandsprimarily the exocrine glands
1% of the population and in 10-15% of RA patients1% of the population and in 10-15% of RA patients 9:1 Female :Male preponderance9:1 Female :Male preponderance Age of onset 40-60 yearsAge of onset 40-60 years Dry mouth, skin, eyes, nose and vaginaDry mouth, skin, eyes, nose and vagina Tongue becomes fissured and exhibits atrophy of the Tongue becomes fissured and exhibits atrophy of the
papillaepapillae Oral mucosa red and tenderOral mucosa red and tender Parotid enlargementParotid enlargement

Sjogren SyndromeSjogren Syndrome Primary vs Secondary:Primary vs Secondary: Primary is diagnosis of exclusionPrimary is diagnosis of exclusion Secondary refers to the sicca complex Secondary refers to the sicca complex
accompanying any of the connective tissue accompanying any of the connective tissue diseases (xerophthalmia, keratoconjuntivitis, diseases (xerophthalmia, keratoconjuntivitis, xerostomia with/without salivary gland xerostomia with/without salivary gland enlargement)enlargement)
Lymphocytic infiltratesLymphocytic infiltrates Associated with a 33-44 times increased risk Associated with a 33-44 times increased risk
of lymphoma.of lymphoma. Characteristic autoantibodies - Ro, La Characteristic autoantibodies - Ro, La

Extra-glandular Signs and Extra-glandular Signs and SymptomsSymptoms
Raynaud’s phenomenonRaynaud’s phenomenon Peripheral Neuropathies Peripheral Neuropathies LymphadenopathyLymphadenopathy VasculitisVasculitis Interstitial nephritisInterstitial nephritis Interstitial lung fibrosisInterstitial lung fibrosis Primary Biliary CirrhosisPrimary Biliary Cirrhosis

Sjogren SyndromeSjogren Syndrome

Laboratory ValuesLaboratory Values
High ESR & serum immunoglobulin High ESR & serum immunoglobulin levels (IgG)levels (IgG)
75% of patients have RF regardless of 75% of patients have RF regardless of rheumatoid arthritisrheumatoid arthritis
Antinuclear antibodies (ANA) also Antinuclear antibodies (ANA) also presentpresent

Sjogren Syndrome Diagnostic Sjogren Syndrome Diagnostic CriteriaCriteria
1. Dry eyes (>3mos), sensation of sand or gravel in 1. Dry eyes (>3mos), sensation of sand or gravel in eyes, or use of tear substitutes>3x per dayeyes, or use of tear substitutes>3x per day
2. Dry mouth (>3mos), recurrent or persistent 2. Dry mouth (>3mos), recurrent or persistent swollen salivary glands, or frequent drinking of swollen salivary glands, or frequent drinking of liquids to aid in swallowing dry foods.liquids to aid in swallowing dry foods.
3. Schirmer-I test (<5mm in 5 min) or Rose Bengal 3. Schirmer-I test (<5mm in 5 min) or Rose Bengal score >4.score >4.
4. >50 mononuclear cells/4mm4. >50 mononuclear cells/4mm2 2 glandular tissueglandular tissue
5. Abnormal salivary scintigraphy or parotid 5. Abnormal salivary scintigraphy or parotid sialography or unstimulated salivary flow sialography or unstimulated salivary flow <1.5ml in 15 min<1.5ml in 15 min
6. Presence of anti-Ro/SS-A, anti-La/SS-b, 6. Presence of anti-Ro/SS-A, anti-La/SS-b, antinuclear antibodies, or rheumatoid factor.antinuclear antibodies, or rheumatoid factor.
Medical ManagementMedical Management Local manifestations can be treated Local manifestations can be treated
symptomaticallysymptomatically Symptomatic: saliva substitutes, Symptomatic: saliva substitutes,
artificial tears, increased oral fluid artificial tears, increased oral fluid intakeintake
Avoid decongestants, antihistamines, Avoid decongestants, antihistamines, anticholinergics, diureticsanticholinergics, diuretics
Pilocarpine, antifungals, close dental Pilocarpine, antifungals, close dental follow-up, surveillance for malignancyfollow-up, surveillance for malignancy

Dental ManagementDental Management
Prevention of cariesPrevention of cariesdaily use of fluoride, frequent recallsdaily use of fluoride, frequent recalls
Enhance salivary outputEnhance salivary outputsugarless gum/candy, saliva substitutes (salivart, biotene, sugarless gum/candy, saliva substitutes (salivart, biotene,
oral oral balance, mouth kote, glandosane, prescription medication balance, mouth kote, glandosane, prescription medication (salagen, `(salagen, ` evoxac)evoxac)
Treatment of oral candidiasisTreatment of oral candidiasisantifungalsantifungals
Pain control for enlarged salivary Pain control for enlarged salivary glandsglands

SclerodermaScleroderma Generalised disorder of CT affecting skin Generalised disorder of CT affecting skin
(scleroderma)(scleroderma) and internal organs and internal organs Associated with specific auto-antibodiesAssociated with specific auto-antibodies Localised (CREST) or Systemic ( Variants Localised (CREST) or Systemic ( Variants
SSc)SSc) May be benign cutaneous involvement or May be benign cutaneous involvement or
aggressive systemic disease.aggressive systemic disease. 4-12 new cases per million per year4-12 new cases per million per year 3-4:1 Female preponderance3-4:1 Female preponderance Average age of onset between 3Average age of onset between 3rdrd and 5 and 5thth
decadedecade

Scleroderma : PresentationScleroderma : Presentation Raynaud’s phenomenonRaynaud’s phenomenon Inflammatory, indurative then atrophic Inflammatory, indurative then atrophic
phasephase Oedema, tightening, thickening, waxy feelOedema, tightening, thickening, waxy feel edema fingers and hands & Loss of function of edema fingers and hands & Loss of function of
handhand skin thickeningskin thickening Arms, legs, chest involvedArms, legs, chest involved
Visceral manifestationsVisceral manifestations GI tract, lung, heart, kidneys, thyroid , arthralgias GI tract, lung, heart, kidneys, thyroid , arthralgias
and muscle weakness oftenand muscle weakness often

Musculoskeletal: Arthralgia, Musculoskeletal: Arthralgia, MyalgiaMyalgia
Small mouth, tightening of skin around mouthVitiligo or hyperpigmentation, telangectasia,

Skin changes in systemic Skin changes in systemic sclerosissclerosis

Raynaud’s Raynaud’s phenomenonphenomenon
Calcinosis Ulceration

Systemic Systemic involvementinvolvement
Gut Gut involvementinvolvement OropharynxOropharynx Esophagus Esophagus Small bowel Small bowel Large bowelLarge bowel

PulmonaryPulmonary
Interstitial Interstitial fibrosisfibrosis
Pulmonary HTNPulmonary HTN
CardiacCardiac
CCF, ArrythmiasCCF, Arrythmias
RenalRenal
Accelerated HTN Accelerated HTN
Renal CrisisRenal Crisis

Head and Neck ManifestationsHead and Neck Manifestations Dysphagia most common initial complaint:Dysphagia most common initial complaint:
80% exhibit pathology in distal 2/3 of esophagus 80% exhibit pathology in distal 2/3 of esophagus Decreased or absent peristalsis, hiatal hernia, Decreased or absent peristalsis, hiatal hernia,
refluxreflux Tight, thin lips with vertical perioral furrowsTight, thin lips with vertical perioral furrows Trismus 2Trismus 2ndnd to tight skin, not TMJ path to tight skin, not TMJ path Xerostomia, xerophthalmia, Xerostomia, xerophthalmia, Laryngeal involvement with hoarsenessLaryngeal involvement with hoarseness Transition zone around dental rootsTransition zone around dental roots
Considered pathognomonic by someConsidered pathognomonic by some

Scleroderma Diagnostic Scleroderma Diagnostic CriteriaCriteria
One major criterion: scleromatous skin One major criterion: scleromatous skin changes proximal to the metacarpal-changes proximal to the metacarpal-phalangeal jointsphalangeal joints
Two of three minor criteria: Two of three minor criteria: sclerodactyly, digital pitting scars, bi-sclerodactyly, digital pitting scars, bi-basilar pulmonary fibrosis on CXRbasilar pulmonary fibrosis on CXR

InvestigationInvestigation BP - monitor closely for hypertensionBP - monitor closely for hypertension Renal function - Creatinine clearance Renal function - Creatinine clearance ANA, anti- ENA, anti-centromereANA, anti- ENA, anti-centromere
Pulmonary function testsPulmonary function tests ECG ECG Radiology Radiology
CXR, CT scan chest, barium swallowCXR, CT scan chest, barium swallow

ManagementManagement Raynaud’sRaynaud’s
Simple measuresSimple measures vasodilators - topical (nitrate), oral vasodilators - topical (nitrate), oral
(calcium channel blockers) (calcium channel blockers) Skin diseaseSkin disease
Simple measures, Immunosuppressive Simple measures, Immunosuppressive Systemic involvementSystemic involvement
Specific therapy aimed at organ involvedSpecific therapy aimed at organ involved Prevent renal crisis with ACE InhibitionPrevent renal crisis with ACE Inhibition

Prognosis: systemic Prognosis: systemic sclerosissclerosis
5 yr survival5 yr survival 70-90%70-90% 10 yr survival10 yr survival 50-70%50-70%
Causes of deathCauses of death:: Renal CrisisRenal Crisis
PulmonaryPulmonary HHypertensionypertension
Myocardial IschaemiaMyocardial Ischaemia

Polymyositis and Polymyositis and DermatomyositisDermatomyositis
Chronic inflammation in striated muscleChronic inflammation in striated muscle Proximal muscle weakness Proximal muscle weakness 2 main subgroups recognised2 main subgroups recognised
Myositis Myositis Dermatomyositis (with skin involvement)Dermatomyositis (with skin involvement)
5 cases per million per year5 cases per million per year 2:1 Female: Male2:1 Female: Male Age 40-60, but a pediatric variant of 5-15 year Age 40-60, but a pediatric variant of 5-15 year
oldold Autoantibody associationAutoantibody association
anti-Jo-1, anti-Mi-2anti-Jo-1, anti-Mi-2

Head and Neck ManifestationsHead and Neck Manifestations Difficulty phonating and deglutition 2Difficulty phonating and deglutition 2ndnd to to
affected tongue musculatureaffected tongue musculature Nasal regurgitation 2Nasal regurgitation 2ndnd to affected to affected
pharyngeal and palatal musculaturepharyngeal and palatal musculature 30% with dysphagia 230% with dysphagia 2ndnd to involvement of to involvement of
upper esophagus, cricopharyngeus, pharynx upper esophagus, cricopharyngeus, pharynx Aspiration pneumoniaAspiration pneumonia
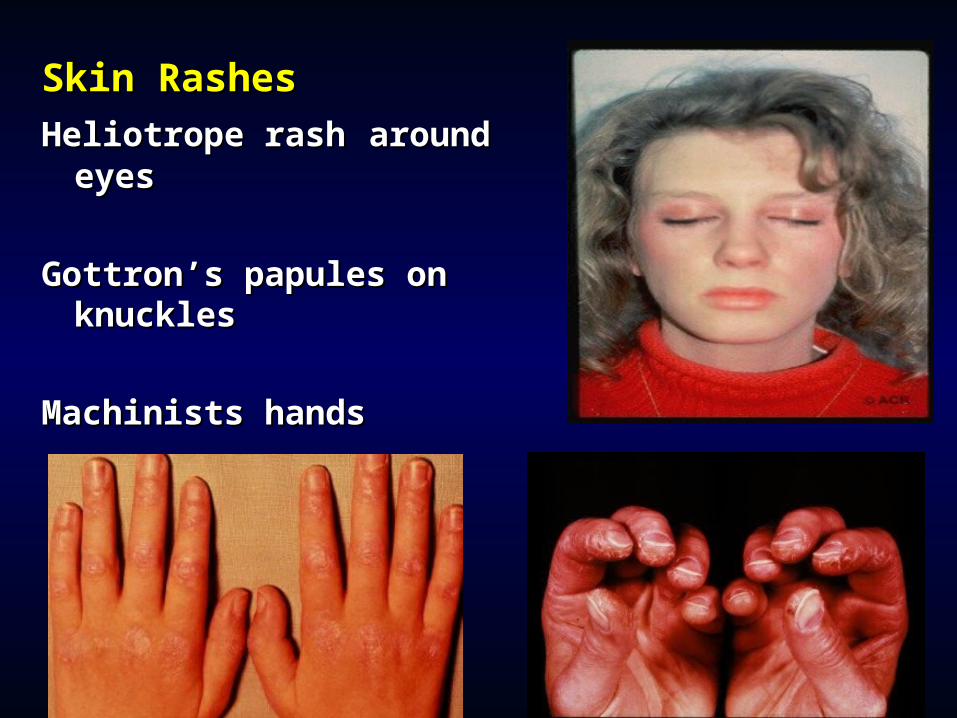
Skin RashesSkin RashesHeliotrope rashHeliotrope rash around around
eyeseyes
Gottron’s papules on Gottron’s papules on knucklesknuckles
Machinists handsMachinists hands
Investigations - MyositisInvestigations - Myositis
Blood testsBlood tests CPK, AST, ALT, LDH, ESRCPK, AST, ALT, LDH, ESR ANA (80%), anti-synthetase antibodies - ANA (80%), anti-synthetase antibodies -
anti-Jo-1 (lung), PM-Scl (SSc), RNP (SLE) anti-Jo-1 (lung), PM-Scl (SSc), RNP (SLE) ECG ECG Radiology - CXR, MRI of thigh muscleRadiology - CXR, MRI of thigh muscle EMGEMG Biopsy Biopsy - muscle, skin- muscle, skin Investigation for malignancy in older age Investigation for malignancy in older age
groupgroup

DiagnosisDiagnosis Proximal muscle weaknessProximal muscle weakness Elevated serum creatinine kinaseElevated serum creatinine kinase Myopathic changes on Myopathic changes on
electromyographyelectromyography Muscle biopsy with evidence of Muscle biopsy with evidence of
lymphocytic inflammationlymphocytic inflammationDiagnosis Diagnosis is :is : Definitive with all fourDefinitive with all four Probable with threeProbable with three Possible with two.Possible with two.
Rash accompanies these in Rash accompanies these in dermatomyositisdermatomyositis

Therapy - MyositisTherapy - Myositis
CorticosteroidsCorticosteroids oral, IV pulseoral, IV pulse
ImmunosuppressantsImmunosuppressants methotrexate, azathioprine, cyclosporin methotrexate, azathioprine, cyclosporin
AA Immunoglobulin (IV IG)Immunoglobulin (IV IG) Monitor disease progressMonitor disease progress
CPK, muscle strengthCPK, muscle strength

Giant Cell Arteritis (Temporal Giant Cell Arteritis (Temporal Arteritis)Arteritis)
Most common vasculitisMost common vasculitis Prevalence:850/100000Prevalence:850/100000 Age 80+Age 80+ Only extracranial vessels involvedOnly extracranial vessels involved Most common initial complaint: Headache-boring and Most common initial complaint: Headache-boring and
constant (47%), up to 90% will develop headacheconstant (47%), up to 90% will develop headache Tender and erythematous temporal artery 50%Tender and erythematous temporal artery 50% Blindness: 1/3 untreated patientsBlindness: 1/3 untreated patients Tender scalpTender scalp Jaw ischemia 50%Jaw ischemia 50% Lingual ischemia 25%Lingual ischemia 25% ESR >50mm/hrESR >50mm/hr Confirmed by temporal artery biopsy of affected sideConfirmed by temporal artery biopsy of affected side Treatment with prednisone and normalizaton of ESRTreatment with prednisone and normalizaton of ESR

Polymyalgia RheumaticaPolymyalgia Rheumatica
Seen in 50% of patients with giant Seen in 50% of patients with giant cell arteritiscell arteritis
Muscular pain, morning stiffness of Muscular pain, morning stiffness of proximal muscles, elevated ESR proximal muscles, elevated ESR without inflammatory joint or muscle without inflammatory joint or muscle diseasedisease
Low grade fever, wt loss, malaiseLow grade fever, wt loss, malaise Low dose prednisoneLow dose prednisone

Relapsing PolychondritisRelapsing Polychondritis GeneralGeneral
Recurring inflammation cartilaginous structuresRecurring inflammation cartilaginous structures Eventual fibrosisEventual fibrosis PrevalencePrevalence
F>MF>M 25-4525-45
Can affect any cartilaginous structureCan affect any cartilaginous structure Including heart valves and large arteriesIncluding heart valves and large arteries
Diagnostic criteriaDiagnostic criteria Recurrent chondritis of the auriclesRecurrent chondritis of the auricles Nonerosive inflammatory polyarthritisNonerosive inflammatory polyarthritis Chondritis of the nasal cartilagesChondritis of the nasal cartilages Inflammation of ocular structuresInflammation of ocular structures Chondritis of laryngeal or tracheal cartilages, Chondritis of laryngeal or tracheal cartilages, Cochlear (SNHL, tinnitus) Vestibular (vertigo) Cochlear (SNHL, tinnitus) Vestibular (vertigo)
damagedamage

PolychondritisPolychondritis Laboratory Laboratory
ESR, leukocytosis, anemiaESR, leukocytosis, anemia HistologyHistology
Loss of basophilic staining of cartilageLoss of basophilic staining of cartilage Perichondral inflammationPerichondral inflammation Destruction fibrotic replacementDestruction fibrotic replacement
TreatmentTreatment Salicylates, ibuprofen-symptomatic reliefSalicylates, ibuprofen-symptomatic relief Steroids for life threateningSteroids for life threatening Dapsone (anti-leprosy) reduces Dapsone (anti-leprosy) reduces
lysozymeslysozymes

Mixed Connective Tissue Mixed Connective Tissue DiseaseDisease
Coexisting features of SLE, Coexisting features of SLE, scleroderma, and polymyositisscleroderma, and polymyositis
High titers of Anti-U1RNPHigh titers of Anti-U1RNP 80% female, 30-60 years80% female, 30-60 years Head and neck: combination of Head and neck: combination of
manifestations of the above. manifestations of the above. Treat with steroidsTreat with steroids

Polyarteritis NodosaPolyarteritis Nodosa Prototype of vasculitisPrototype of vasculitis Less than 1/100000 per yearLess than 1/100000 per year Males = FemalesMales = Females 50-60 years of age50-60 years of age Involves small and medium arteriesInvolves small and medium arteries May result from Hep B infection (30%)May result from Hep B infection (30%) GI, hepatobiliary, renal, pancreas and skeletal GI, hepatobiliary, renal, pancreas and skeletal
musclesmusclesHead and neck symptoms primarily involve the ear Head and neck symptoms primarily involve the ear
and include SNHL and vestibular disturbance.and include SNHL and vestibular disturbance.Proposed mechanism is thromboembolic occlusion Proposed mechanism is thromboembolic occlusion
of inner ear arteriesof inner ear arteriesMay also see CN palsiesMay also see CN palsies

Wegener’s Granulomatosis?Wegener’s Granulomatosis? Young or middle age; M> F Young or middle age; M> F Triad Triad of Necrotizing vasculitis of Upper resp of Necrotizing vasculitis of Upper resp
tract, Lower resp tract, Focal segmental tract, Lower resp tract, Focal segmental glomerulonephritisglomerulonephritis
NonspecificNonspecific
Wegener’s GranulomatosisWegener’s Granulomatosis Upper Respiratory TractUpper Respiratory Tract
Chronic sinusitis with/without hematochezia – 90 %Chronic sinusitis with/without hematochezia – 90 % Oral/nasal ulcers 75 %Oral/nasal ulcers 75 % Otitis media/hearing lossOtitis media/hearing loss Hoarseness of the voiceHoarseness of the voice
Lower Respiratory TractLower Respiratory Tract Cough, Shortness of BreathCough, Shortness of Breath Pulmonary Infiltrates 95 % or Nodules that may Pulmonary Infiltrates 95 % or Nodules that may
cavitatecavitate Renal Renal 80 %80 %
Glomerulonephritis (Rapidly Progressive)Glomerulonephritis (Rapidly Progressive) JointsJoints
ArthritisArthritis

Head and Neck ManifestationsHead and Neck Manifestations Nasal symptomsNasal symptoms
crusting, epistaxis, rhinnorrhea, erosion crusting, epistaxis, rhinnorrhea, erosion of septal cartilage, saddle deformity, of septal cartilage, saddle deformity, recurrent sinusitisrecurrent sinusitis
Oral cavityOral cavity hyperplasia of gingiva, gingivitishyperplasia of gingiva, gingivitis

Wegener’s GranulomatosisWegener’s Granulomatosis Antineutrophil cytoplasmic antibody (c-Antineutrophil cytoplasmic antibody (c-
ANCA)ANCA) sensitivity 65-90%sensitivity 65-90% high specificityhigh specificity
Need to confirm diagnosisNeed to confirm diagnosis often 3-4 biopsies necessaryoften 3-4 biopsies necessary nasopharynx commonly involved good sitenasopharynx commonly involved good site open pulmonary biopsy occasionally open pulmonary biopsy occasionally
neededneeded untreated mortality of 90% at two yearsuntreated mortality of 90% at two years

TreatmentTreatment Meticulous dental and nasal careMeticulous dental and nasal care Middle ear drainageMiddle ear drainage Isolated sinonasal diseaseIsolated sinonasal disease
low dose steroids, saline irrigation, antibiotics as low dose steroids, saline irrigation, antibiotics as neededneeded
Subglottic stenosisSubglottic stenosis may warrant tracheotomymay warrant tracheotomy
Cyclophosphamide 2 mg/kg plus prednisone 1 Cyclophosphamide 2 mg/kg plus prednisone 1 mg/kgmg/kg Remission 93% Remission 93%
Azathioprine or methotrexate alternative to Azathioprine or methotrexate alternative to cyclophosphamidecyclophosphamide

Henoch Schonlein PurpuraHenoch Schonlein Purpura
Purpura on extensor surfaces of arms, legs, buttocks
GI disturbances
Renal involvement
Fever
Previous URI
Hypersensitivity VasculitisHypersensitivity Vasculitis Head and Neck ManifestationsHead and Neck Manifestations
Petechiae, Purpura of oral and nasal Petechiae, Purpura of oral and nasal mucosamucosa
AngioedemaAngioedema Serous otitis mediaSerous otitis media
TreatmentTreatment Usually self limitedUsually self limited
especially when only skin involvedespecially when only skin involved Systemic involvement- more aggressive Systemic involvement- more aggressive

Churg-Strauss SyndromeChurg-Strauss Syndrome
Also called angiitis granulomatosisAlso called angiitis granulomatosis Consists of small vessel vasculitis, Consists of small vessel vasculitis,
extra vascular granulomas, and extra vascular granulomas, and hypereosinophilia.hypereosinophilia.
In patients with preexisting asthma In patients with preexisting asthma and allergic rhinitisand allergic rhinitis
Behcet’s DiseaseBehcet’s Disease
Vasculitis with triad of oral and genital Vasculitis with triad of oral and genital ulcers and uveitis or iritisulcers and uveitis or iritis
Aphthous like ulcers, covered in pale Aphthous like ulcers, covered in pale pseudomembranepseudomembrane
Painful, on lips, gingiva, buccal Painful, on lips, gingiva, buccal mucosa, tongue, palate and mucosa, tongue, palate and oropharynxoropharynx
Genital ulcers similar in appearanceGenital ulcers similar in appearance Heal in days to weeks with scarringHeal in days to weeks with scarring

Behcet’s DiseaseBehcet’s Disease

Behcets and Churg StraussBehcets and Churg Strauss
CSS has been divided into 3 distinct phases, which may or may not be sequential.
The prodromal phase is characterized by asthma with or without allergic rhinitis.
The second phase is marked by a peripheral blood eosinophilia and eosinophilic tissue infiltration producing a picture similar to Loeffler syndrome, chronic eosinophilic pneumonia, or eosinophilic gastroenteritis.
The third, vasculitic phase may involve any organ. The most frequent site of involvement is the heart. Other organs that may be involved with a vasculitis include the lung, central nervous system, kidney, lymph nodes, muscle, and skin. Skin involvement occurs in more than two-thirds of patients