Embed Size (px)
Citation preview

Dental ManagementDental Management of of
Patients with Heart FailurePatients with Heart Failure

What is Heart Failure?What is Heart Failure?A symptom complex due A symptom complex due to the inability of the to the inability of the heart to function heart to function efficiently as a pump - efficiently as a pump - there is a disproportion there is a disproportion between the between the hemodynamic demand hemodynamic demand and the capacity of the and the capacity of the heart to handle the heart to handle the demand demand
( Supply ( Supply ≠ ≠ Demand)Demand)

What is Heart Failure?What is Heart Failure? HF occurs when the heart is unable to pump enough blood to meet the oxygen requirements of the body
Nearly 10% of populations > 70 years of age will have HF
Overall mortality close to 20%
HF risk factors: CAD and its sequelae HTN - Myocarditis, Cardiomyopathy - Valvular heart diseasesPericardial disease - Pulmonary embolism
Types and Classifications of H.FTypes and Classifications of H.F (measured by ejection fraction [EF])(measured by ejection fraction [EF])
Systolic or diastolicSystolic or diastolic
High output or low outputHigh output or low output
Left or right sidedLeft or right sided
Acute or chronicAcute or chronic

Systolic HFSystolic HF
Inability of heart to Inability of heart to contract stronglycontract strongly enough to provide enough to provide adequate blood adequate blood flow to peripheryflow to periphery
Diastolic Diastolic HFHF
Abnormal Abnormal relaxationrelaxation of of myocardium myocardium resulting in resulting in reduced fillingreduced filling of of ventricleventricleSystolic dysfunction:Systolic dysfunction:
- - EF < 50%; results from EF < 50%; results from reduced left ventricular reduced left ventricular functionfunction - Increased preload- Increased preload - Most cases of CHF- Most cases of CHF

If Heart does not contract well If Heart does not contract well (systolic HF) traffic (blood) piles (systolic HF) traffic (blood) piles up before the heart (lungs and up before the heart (lungs and
periphery).periphery).

Common Causes of HFCommon Causes of HF
Coronary Heart Disease/MICoronary Heart Disease/MI
HypertensionHypertension
Valvular Heart DiseaseValvular Heart Disease
ArrhythmiasArrhythmias
MyocarditisMyocarditis
CardiomyopathyCardiomyopathy
Infective EndocarditisInfective Endocarditis
Congenital Heart DiseaseCongenital Heart Disease
Pulmonary HypertensionPulmonary Hypertension
Endocrine Disorders (thyroid Endocrine Disorders (thyroid disease)disease)
MI is a leading cause

Sequelae of Heart FailureSequelae of Heart Failure Right Heart Right Heart
FailureFailure Systemic Systemic
venous venous congestion congestion (distended (distended neck veins, neck veins, enlarged liver, enlarged liver, peripheral peripheral edema, edema, ascites)ascites)
Left Heart Left Heart FailureFailure Pulmonary Pulmonary
edema edema (Dyspnea)(Dyspnea)

Symptoms of Heart FailureSymptoms of Heart Failure
Compensated (Asymptomatic)Compensated (Asymptomatic)
Uncompensated (Symptomatic)Uncompensated (Symptomatic) FatigueFatigue DyspneaDyspnea OrthopneaOrthopnea Paroxysmal Nocturnal DyspneaParoxysmal Nocturnal Dyspnea Ankle EdemaAnkle Edema Weight GainWeight Gain
Note: patients with a very low EF may have no symptoms

Laboratory Findings of Laboratory Findings of CHFCHF
BPBP: elevated: elevated Chest x-rayChest x-ray: heart enlarged: heart enlarged ECGECG:: arrhythmia arrhythmia Serum chemistries:Serum chemistries:
electrolytes: elevatedelectrolytes: elevated liver function tests (AST, ALT, bilirubin): elevatedliver function tests (AST, ALT, bilirubin): elevated Renal function tests (BUN, creatinine): elevatedRenal function tests (BUN, creatinine): elevated C-reactive protein: if > 3 mg/L increased risk for MIC-reactive protein: if > 3 mg/L increased risk for MI Cardiac natriuretic peptides (BNP): adjunctive test to rule Cardiac natriuretic peptides (BNP): adjunctive test to rule
out HF in acute setting (increased risk of HF if > 100 out HF in acute setting (increased risk of HF if > 100 pg/mL) pg/mL)
Stress testStress test: diminished capacity: diminished capacity Arterial blood gas levels:Arterial blood gas levels: hypoxia (< 95%) and acid-base hypoxia (< 95%) and acid-base
imbalanceimbalance

Functional Classification of Heart Functional Classification of Heart Failure (NYHA)Failure (NYHA)
Class IClass I:: No limitation of physical activity. No No limitation of physical activity. No dyspnea, fatigue, or palpitations with ordinary dyspnea, fatigue, or palpitations with ordinary physical activityphysical activity
Class IIClass II:: Slight limitation of physical activity. Slight limitation of physical activity. Fatigue, palpitations and dyspnea with Fatigue, palpitations and dyspnea with ordinary physical activity but comfortable at ordinary physical activity but comfortable at rest.rest.
Class IIIClass III:: Marked limitation of activity. Less Marked limitation of activity. Less than ordinary physical activity results in than ordinary physical activity results in symptoms but comfortable at rest.symptoms but comfortable at rest.
Class IVClass IV:: Symptoms present at rest and any Symptoms present at rest and any physical activity exacerbates the symptomsphysical activity exacerbates the symptoms

To Prevent Heart FailureTo Prevent Heart Failure lower high blood pressurelower high blood pressure;; lose extra weightlose extra weight;; quit smoking, alcohol use, illegal drug usequit smoking, alcohol use, illegal drug use control irregular or too-fast heart rhythmscontrol irregular or too-fast heart rhythms;; correct too-low or too-high thryoid functioncorrect too-low or too-high thryoid function;; lower bad cholesterol and raise good cholesterollower bad cholesterol and raise good cholesterol;; if diabetic, control blood sugarif diabetic, control blood sugar;; if had a heart attack, restore lost blood flow with if had a heart attack, restore lost blood flow with bypassbypass surgery surgery
or angioplasty if possibleor angioplasty if possible;; if had a heart attack (even if long ago), take an ACE inhibitor or if had a heart attack (even if long ago), take an ACE inhibitor or
ARB, ARB, and alsoand also take a beta-blocker to reduce risk of heart failure take a beta-blocker to reduce risk of heart failure down the road, even if you have no symptoms and even if your EF down the road, even if you have no symptoms and even if your EF is normalis normal;;
if have reduced EF, take a beta-blocker if have reduced EF, take a beta-blocker andand an ACE inhibitor an ACE inhibitor even if you have no symptomseven if you have no symptoms;;
if have significant heart valve dysfunction, get surgical repairif have significant heart valve dysfunction, get surgical repair;; perform regular perform regular echocardiogramsechocardiograms in people who have had in people who have had
chemotherapychemotherapy;;

Medical Management of Heart Medical Management of Heart FailureFailure
1.1.Decreased cardiac output CODecreased cardiac output CO
2.2.Decreased ejection fractionDecreased ejection fraction - repair of diseased valves- repair of diseased valves
3.3.Fluid overloadFluid overload
4.4.OverweightOverweight
5.5.HTNHTN
Main Problems Main Problems requiring requiring treatmenttreatment

Medical Management of Medical Management of Heart FailureHeart Failure
Treatment of underlying diseaseTreatment of underlying disease Life-style modificationsLife-style modifications Drug therapyDrug therapy
ACE inhibitorsACE inhibitors- Or angiotensin receptor blockers- Or angiotensin receptor blockers
Beta Blockers Beta Blockers (Coreg, Toprol-XL, or bisoprolol)(Coreg, Toprol-XL, or bisoprolol) DiureticsDiuretics
- Or direct-acting vasodilators- Or direct-acting vasodilators NitratesNitrates Digitalis GlycosidesDigitalis Glycosides
Heart transplantHeart transplant
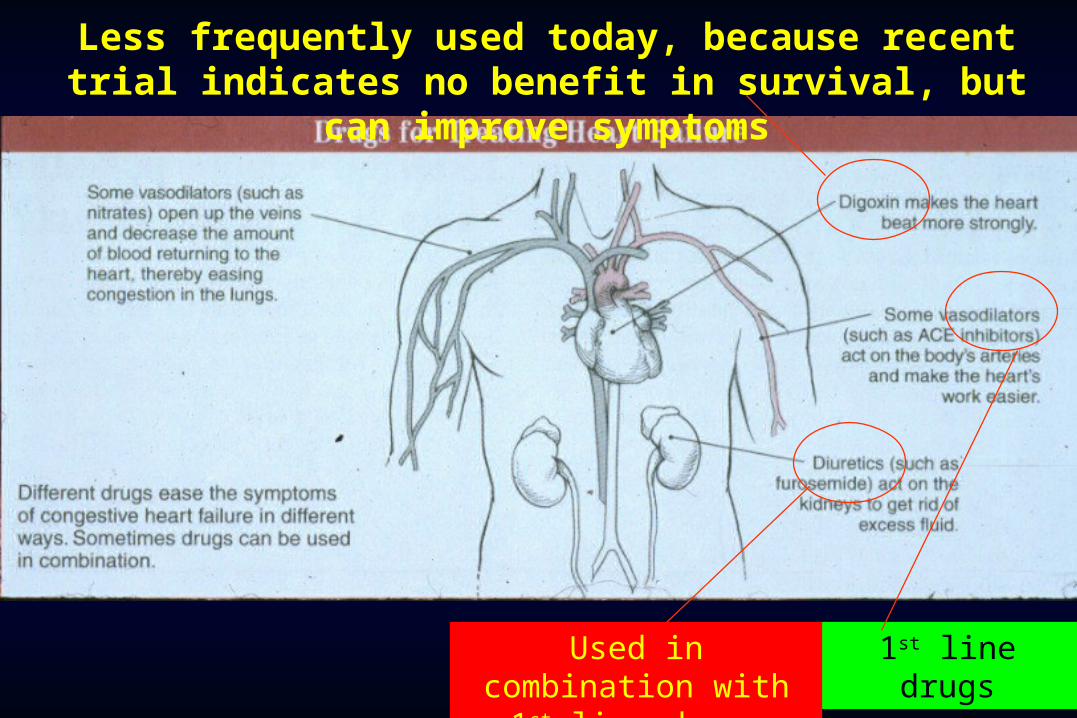
Less frequently used today, because recent trial indicates no benefit in survival, but can
improve symptoms
1st line drugsUsed in combination with 1st line drugs
ACE inhibitors (ACEI) - ACE inhibitors (ACEI) - (Oral (Oral
Meds)Meds) Benazepril - Lotensin Benazepril - Lotensin
Captopril - Capoten Captopril - Capoten
Enalapril - Vasotec Enalapril - Vasotec
Fosinopril - Monopril Fosinopril - Monopril
Lisinopril - Prinivil Lisinopril - Prinivil
Moexipril - Univasc Moexipril - Univasc
Quinapril - Accupril Quinapril - Accupril
Perindopril erbumine - Perindopril erbumine - Aceon Aceon
Ramipril - Altace Ramipril - Altace
ACEI block an ACEI block an enzyme that is enzyme that is necessary to necessary to produce renin that produce renin that causes blood causes blood vessels to tighten. vessels to tighten. As a result, they As a result, they relax blood vessels relax blood vessels and lower BP.and lower BP.
Adv effects: cough, Adv effects: cough, angioedema, oral angioedema, oral burningburning

DiureticsDiuretics Common thiazide diureticsCommon thiazide diuretics
Chlorothiazide (Diuril) Chlorothiazide (Diuril) Indapamide (Lozol) Indapamide (Lozol) Metolazone (Zaroxolyn) Metolazone (Zaroxolyn)
Common loop diureticsCommon loop diuretics Bumetanide (Bumex) Bumetanide (Bumex) Ethacrynic acid (Edecrin) Ethacrynic acid (Edecrin) Furosemide (Lasix) Furosemide (Lasix)
Common potassium-sparing diureticsCommon potassium-sparing diuretics Amiloride (Midamor) Amiloride (Midamor) Eplerenone (Inspra) Eplerenone (Inspra) Spironolactone (AldactoneSpironolactone (Aldactone

Drug Therapy - Digitalis Drug Therapy - Digitalis GlycosidesGlycosides
Action: Increases the Action: Increases the force and velocity force and velocity of myocardial of myocardial contractioncontraction
Digoxin (Lanoxin)Digoxin (Lanoxin)
Digitoxin Digitoxin (Crystodigin)(Crystodigin)
Purple foxglove - digitalis

Drug Considerations – Drug Considerations – Digitalis GlycosidesDigitalis Glycosides
Vasoconstrictor Interaction: concurrent use may Vasoconstrictor Interaction: concurrent use may increase the risk of cardiac arrhythmias – avoid if increase the risk of cardiac arrhythmias – avoid if possible possible
Oral Manifestations: increased gag reflex, Oral Manifestations: increased gag reflex, nausea/vomitingnausea/vomiting
Other Considerations: Other Considerations: macrolide antibiotics (erythromycin) can increase macrolide antibiotics (erythromycin) can increase
bioavailability of DG resulting inbioavailability of DG resulting in toxicity; avoid these toxicity; avoid these drugs drugs
watch for DG toxicity (tachycardia, N/V, hypersalivation, watch for DG toxicity (tachycardia, N/V, hypersalivation, vision changes, fatigue, HA)vision changes, fatigue, HA)
ACC/AHA Guidelines for ACC/AHA Guidelines for perioperative cardiovascular perioperative cardiovascular
evaluation for noncardiac surgeryevaluation for noncardiac surgery Clinical predictors of increased Clinical predictors of increased
perioperative cardiovascular risk perioperative cardiovascular risk (major, intermediate, minor)(major, intermediate, minor) Major riskMajor risk: Decompensated CHF: Decompensated CHF Intermediate riskIntermediate risk: Compensated or prior : Compensated or prior
CHFCHF Minor riskMinor risk: Inability to climb 1 flight of : Inability to climb 1 flight of
stairs with a bag of groceriesstairs with a bag of groceries

Dental Management Dental Management Considerations (Heart Failure)Considerations (Heart Failure)
For undiagnosed pt with symptoms of HF: For undiagnosed pt with symptoms of HF: avoid elective care; refer to physicianavoid elective care; refer to physician
For patients with diagnosed HF:For patients with diagnosed HF: Class IClass I (asymptomatic): routine care (asymptomatic): routine care Class IIClass II (mild symptoms with exertion): elective care (mild symptoms with exertion): elective care
OK and recommend consultation with physician OK and recommend consultation with physician Class III or IVClass III or IV (symptoms with minimal activity or at (symptoms with minimal activity or at
rest): rest): avoid elective careavoid elective care; if treatment necessary, ; if treatment necessary, manage in consultation with physician; consider manage in consultation with physician; consider referral to a special patient care setting; avoid use referral to a special patient care setting; avoid use of vasoconstrictorsof vasoconstrictors

Stress management protocolStress management protocol
ID underlying disease (CHD, HBP, RHD) and ID underlying disease (CHD, HBP, RHD) and manage appropriatelymanage appropriately
Semisupine or upright chair positionSemisupine or upright chair position
Take BP, monitor with pulse oximeter, watch Take BP, monitor with pulse oximeter, watch for orthostatic hypotensionfor orthostatic hypotension
Drug ConsiderationsDrug Considerations If taking digitalis, avoid vasoconstrictors if possible If taking digitalis, avoid vasoconstrictors if possible
If taking nonselective If taking nonselective ββ-blocker, use -blocker, use vasoconstrictor cautiouslyvasoconstrictor cautiously
Watch for digitalis toxicity Watch for digitalis toxicity

Other Drug ConsiderationsOther Drug Considerations
Patients on spironolactone should have Patients on spironolactone should have potassium levels checked more often and potassium levels checked more often and every time a drug dose is changed. every time a drug dose is changed.
Patients on digoxin need dig level testing. Patients on digoxin need dig level testing. Patients on Coumadin (warfarin) need INR Patients on Coumadin (warfarin) need INR
testing. testing. Patients on amiodarone need thyroid and Patients on amiodarone need thyroid and
lung function testing. lung function testing.





















![Dental Implant Failure [Compatibility Mode].pdf](https://img.pdfslide.us/doc/110x75/5695cf451a28ab9b028d579b/dental-implant-failure-compatibility-modepdf.jpg)






