Embed Size (px)
Citation preview

12/2/2014
1
Bethesda, MD
Dental Implant Replacement of
Central IncisorKey Surgical Considerations and
Site Development for a Successful
Restorative Outcome
H. Ryan Kazemi, DMD
Oral & Maxillofacial Surgery
Bethesda, MD

12/2/2014
2
Site Characteristics
Site
Development
Implant
Placement
Tissue
Management
Unique
Requirements for
Central Incisors
Site
Characteristics
•Type and degree of bone deficiency
•Soft tissue biotype
•Tissue health
•Tooth missing / to be extracted?
•Location and size nasopalatine nerve
•Gingival harmony
•Smile line
Site
Development
Extraction site graft
GBR
Inlay bone graft
Onlay bone graft
Mesh / rhBMP2
SonicWeld
Distraction
Soft tissue graft
PDGF

12/2/2014
3
Implant
Placement
Implant diameter
Platform switch
Bucco-palatal placement
Position of the platform
Immediate implant / graft / provisional
CT-Guided planning and placement
Midline / symmetry / smile line
Tissue
Management
Connective tissue graft
Customized healing abutments
Implant uncovering designs
Immediate implant provisional
Delayed implant provisional
classification- cologneorientation
H: horizontal
V: vertical
C: combination
S / +S: sinus
graft needs
1: low < 4 mm
2: medium 4-8 mm
3: high > 8 mm
relation graft to defect
i: internal, inside the
contour
e: external, outside the
ridge
h.2.e
C.2.e.S.1combined defect of 4-8 mm, outside the
envelope, with sinus defect < 4 mm
V.2.i.+S.2vertical defect 4-8 mm, inside the contour
with sinus defect 4-8 mm

12/2/2014
4
Defect-Specific Treatment Options
Central Incisor: #8

12/2/2014
5

12/2/2014
6

12/2/2014
7
classification- cologneorientation
H: horizontal
V: vertical
C: combination
S / +S: sinus
graft needs
1: low < 4 mm
2: medium 4-8 mm
3: high > 8 mm
relation graft to defect
i: internal, inside the
contour
e: external, outside the
ridge
c.2.e
Horizontal deficiency of 6 mm
Vertical deficiency of 3 mm
Thick tissue biotype

12/2/2014
8
🚩 🚩Aesthetic zone
Vertical deficiency
Thick tissue biotype
Good interseptal bone
Low smile line
Vertical def. 3mm
Mostly horizontal def.
What is the best bone augmentation technique?
“No single technique or biomaterial is
optimum for every clinical application.
Instead, surgeons should consider the
advantages an disadvantages of
each alternative in a given clinical
situation, and select the approach with
lowest overall cost and morbidity, and
the highest likelihood of success”
Rogers, Greene 2012
What is the best bone augmentation technique?
Bone Augmentation Axiom #1“The morphology of a bone defect should influence
our choice of material or technique for repair”
Bone Augmentation Axiom #2“Sites with less bone (fewer walls, > atrophy) are
more demanding and require materials and/or
techniques that offer greater biologic activity and
regenerative capacity.”
Craig Misch

12/2/2014
9
GBR
Bone Blocks
Ridge Split
Mesh
+ Growth factors
Horizontal Bone Augmentation
Gain (Avg.)
Ridge Split 2.9 mm
GBR 3.1 mm
Block Autograft 4.3 mm
Milinkovic, I, Cordaro L, Int J Oral Maxillofac Surg 2014
Gain (Avg.)
GBR: Non-resorb memb 2.5 - 3.5 mm
GBR: Resorb memb 3.2 - 4.6 mm
Block Autograft 4.0 - 5.7 mm
Jensen SS, Terheyden H, Int J Oral Maxillofac Surg 2009
GBR
Bone Blocks
Ridge Split
Mesh
+ Growth factors
Horizontal Bone Augmentation
Minimal: < 2.0 mm
GBR, Split
Moderate: 2.0 - 4.0 mm
GBR, Split, Block, Mesh
Maximum: > 4.0 mm
Block, Mesh
Gain
Craig Misch
GBR
Bone Blocks
Ridge Split
Mesh
+ Growth factors
Horizontal Bone Augmentation
Minimal: < 2.0 mm
GBR, Split
Moderate: 2.0 - 4.0 mm
GBR, Split, Block, Mesh
Maximum: > 4.0 mm
Block, Mesh
Gain

12/2/2014
10
GBR
Bone Blocks
Distraction
Mesh
Interpositional
Tent pole
+ Growth factors
Vertical Bone Augmentation
< / = 5 mm•GBR (resorb/PTFE + autograft or bone substitute)
•Intraoral bone blocks
•Ti mesh + oral autograft or bone substitute
•Inlay graft
•Distraction
5 - 10 mm•GBR (resorb/PTFE + autograft)
•Extraoral bone blocks
•Ti mesh + oral autograft
•Inlay graft
•Tent pole
•Distraction osteogenesis
> 10 mm• Iliac block bone grafts
• Ti mesh + extraoral autograft
• Distraction osteogeneis
GBR
Bone Blocks
Distraction
Mesh
Inlay graft
Tent pole
Combination Bone Augmentation
< / = 5 mm•GBR (resorb/PTFE + autograft)
•Intraoral bone blocks
•Ti mesh + oral autograft or bone substitute
•Inlay graft
•Distraction
5 - 10 mm•GBR (resorb/PTFE + autograft)
•Extraoral bone blocks
•Ti mesh + oral autograft
•Inlay graft
•Tent pole
•Distraction osteogenesis
> 10 mm• Iliac block bone grafts
• Ti mesh + extraoral autograft
• Distraction osteogeneis
Consider
Staged
Bone
Grafting
Horizontal deficiency of 6 mm
Vertical deficiency of 3 mm

12/2/2014
11
Horizontal: Onlay graft
Vertical: GBR- autogenous
Space maintenance is
critical in GBR techniques

12/2/2014
12
Membrane selection
for space maintenance
Implant
Placement
• Implant diameter based on bucco-palatal
dimension
•Allow 3 mm between implant and outer surface of
buccal bone wall - José Carlos Martins da ROSA Dental Pres Implantol. 2014
Apr-June;8(2):80-9
•Palatal implant placement
Maintain proper buccal tissue
thickness and stability
•Position of the platform- 3 mm apical to CEJ

12/2/2014
13
6 months
Inadequate
Space
Maintenance??
?
Modified block
Extended resorb memb
Non-resorb reinforced memb
Ti-mesh
SonicWeld
6 months

12/2/2014
14
Maxillary Anterior: #6 - #9

12/2/2014
15
#6 #7-8 #8-9 #10
Non-restorable 6 & 8
Horizontal defect 7
Combination defect 9
classification- cologneorientation
H: horizontal
V: vertical
C: combination
S / +S: sinus
graft needs
1: low < 4 mm
2: medium 4-8 mm
3: high > 8 mm
relation graft to defect
i: internal, inside the
contour
e: external, outside the
ridge
c.2.e
Staged Treatment
1. Ext 6
2. Bone graft 9
3. Fixed provisional
1. Implant 6 & 9
2. Tissue graft
1. Provisional 6-9
2. Ext 8 / site graft
Implant-supported
bridge 6-9

12/2/2014
16

12/2/2014
17

12/2/2014
18
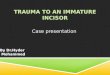
Central Incisor: #8

12/2/2014
19
classification- cologneorientation
H: horizontal
V: vertical
C: combination
S / +S: sinus
graft needs
1: low < 4 mm
2: medium 4-8 mm
3: high > 8 mm
relation graft to defect
i: internal, inside the
contour
e: external, outside the
ridge
v.1.i

12/2/2014
20
Central Incisor: #8

12/2/2014
21

12/2/2014
22

12/2/2014
23

12/2/2014
24
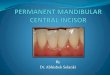
Central Incisor: #8

12/2/2014
25
classification- cologneorientation
H: horizontal
V: vertical
C: combination
S / +S: sinus
graft needs
1: low < 4 mm
2: medium 4-8 mm
3: high > 8 mm
relation graft to defect
i: internal, inside the
contour
e: external, outside the
ridge
h.2.e

12/2/2014
26
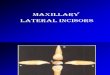
Maxillary Incisors: #7 - #9

12/2/2014
27
#6 #7-8 #8-9 #10
Missing 7
Horizontal defect #7
Perio #9

12/2/2014
28

12/2/2014
29

12/2/2014
30

12/2/2014
31
Maxillary Incisors: #9 - #10

12/2/2014
32
classification- cologneorientation
H: horizontal
V: vertical
C: combination
S / +S: sinus
graft needs
1: low < 4 mm
2: medium 4-8 mm
3: high > 8 mm
relation graft to defect
i: internal, inside the
contour
e: external, outside the
ridge
c.1.e

12/2/2014
33

12/2/2014
34

12/2/2014
1
Dr. Ben Watkins has a financial relationship with BIOMET 3i LLC, resulting from speaking engagements, consulting
engagements and other retained services.
Ben Watkins, DDS, FICDProsthodontist
www.drbenwatkins.com
Planning for Implant Restorations
Ben Watkins, DDS, FICDProsthodontist
www.drbenwatkins.com

12/2/2014
2
Keys To Successful Implant Esthetics
1. A Diagnosis That Reflects Endpoint Thinking.
2. Precise Surgical and Prosthetic Execution.
Gingival Health
Interdental Closure
Gingival Zenith Gingival Level Equilibrium
Interdental Contact Levels
Patient Evaluation and Implant Site Assessment
1. Biologically Acceptable
2. Functionally Enduring & 3. Esthetically Pleasing

12/2/2014
3
Running room
Space for components
Emergence profile
In the Facial Plane
Langer and Sullivan I.J.P.R.D. Vol. 9 no. 3, 1989
How can we control the position and direction of tissue?
Think Water Balloons

12/2/2014
4
Thick Biotype
Moves tissue apically.
FACIALTISSUE
Thin Biotype
Moves tissue incisally.
FACIALTISSUE
Interproximal Shaping
Moves papillae incisally

12/2/2014
5
Interproximal Shaping
Moves papillae apically
Cylindrical vs. AnatomicEmergence
7 wks healing
“Maintenance of the (tissue) depth range allows clinicians to establish an esthetic, natural-appearing emergence profile .”
--William Becker, DDS, MSD
J Esthet Restor Dent 24:395-401, 2012
Creation of Emergence Profile

12/2/2014
6
Custom Provisional Technique
Creation of Emergence Profile
Creation of Emergence Profile

12/2/2014
7
Once the soft tissue has been shaped to our satisfaction, how do we
communicate this to our laboratory for customized abutment fabrication ?
Custom Impression Coping
TechniqueMark Buccal

12/2/2014
8
Custom Healing Abutment Technique
Technique by Joseph Kan, DDS, MSLoma Linda University
Custom lmpression Coping for an Exact Registration of the Healed Tissue in the Esthetic lmplant Restoration
lnt J Periodont Rest Dent. 1997;17:585-591Kenneth F. Hinds, DDS

12/2/2014
9
Encode®
Zirconia Abutments

12/2/2014
10
Zirconia Copingsveneered with
Noritake CZR Porcelain
Ceramics—Rick Bishop, CDTDiplomate Dental Lab
Washington, DC
tissue response13 wks post
implant placement
day of delivery

12/2/2014
11
CEMENT DELIVERY JIG
Salama H,Salama MA,Garber D,Adar P. The Interproximal Height of Bone: A Guidepost to Esthetic Strategies and Soft Tissue Contours in Anterior Tooth Replacement
Prac Periodontics Aesthet Dent 1998;10:1131-1141
Class Restorative
Environment
Proximity
Limitations
Vertical Soft
Tissue
Limitations
1 Tooth-Tooth
2 Tooth-Pontic
3 Pontic-Pontic
4 Tooth-Implant 1.5 mm 4.5 mm
5 Implant-Pontic N/A 5.5 mm
6 Implant-Implant 3 mm 3.5 mm

12/2/2014
12
13 mos post delivery1-14-13

12/2/2014
13

12/2/2014
14
Take-home PointCustom Healing Abutment
+ Custom Impression Coping
+ Custom Abutment (CAD/CAM)
+ World-class Lab Support
+ Application of the Literature
= Best Chance For Superior Esthetic Results