Embed Size (px)
Citation preview

Earn1 CE creditThis course was
written for dentists, dental hygienists,
and assistants.
Dental Electronic Health Records: Meaningful and UsefulA Peer-Reviewed Publication Written by Patti DiGangi, RDH, BS
AbstractInteroperable electronic health records (EHRs) are promising tools to improve quality and efficiency in health care. This course will look at the tides of change and how dentistry became part of the interoperable EHR process. It will assess the impact of standards, coding, and systems being developed by the American Dental Association for EHR. The reader is given five simple steps that can be taken to help with navigating the choppy waters of adoption.
Educational Objectives:The learner will be able to:1. Identify new communication and technol-
ogy trends affecting health care2. Discuss historic decisions bringing dentistry
into interoperable electronic health records3. Determine the American Dental Association
directions in creating standards and codes4. Take five simple action steps from an
individual’s current position to prepare for interoperable electronic health records
Author ProfilePatti DiGangi, RDH, BS, is a vision-driven practicing clinician. She is an American Dental Association Evidence Based Champion and Current Dental Terminology licensee, currently writing a series of mini-books on insurance coding for hygienists. She is a member of the National Speakers Association and a Certified Speaking Professional candidate. She is a key opinion leader for multiple manufacturers and well known author. Patti is a certified Health Information Technology trainer and a member of the American Health Information Management Association, taking an active role in our shaping the changes in our electronic world.
Author DisclosurePatti DiGangi, RDH, BS has no commercial ties with the sponsors or providers of the unrestricted educational grant for this course.
Publication date: Dec. 2012 Expiration date: Nov. 2015
This educational activity was developed by PennWell’s Dental Group with no commercial support.This course was written for dentists, dental hygienists and assistants, from novice to skilled. Educational Methods: This course is a self-instructional journal and web activity. Provider Disclosure: PennWell does not have a leadership position or a commercial interest in any products or services discussed or shared in this educational activity nor with the commercial supporter. No manufacturer or third party has had any input into the development of course content.Requirements for Successful Completion: To obtain 1 CE credit for this educational activity you must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%.CE Planner Disclosure: Heather Hodges, CE Coordinator does not have a leadership or commercial interest with products or services discussed in this educational activity. Heather can be reached at [email protected] Disclaimer: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.Registration: The cost of this CE course is $20.00 for 1 CE credit. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
Supplement to PennWell Publications
PennWell designates this activity for 1 Continuing Educational Credit
Dental Board of California: Provider 4527, course registration number 01-4527-12076“This course meets the Dental Board of California’s requirements for 1 unit of continuing education.”
The PennWell Corporation is designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing dental education programs of this program provider are accepted by the AGD for Fellowship, Mastership and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from (11/1/2011) to (10/31/2015) Provider ID# 320452.
Go Green, Go Online to take your course

94 03.2013 | www.dentaleconomics.com
Educational Objectives:The learner will be able to:1. Identify new communication and technology trends affect-
ing health care2. Discuss historic decisions bringing dentistry into interoper-
able electronic health records3. Determine the American Dental Association directions in
creating standards and codes4. Take five simple action steps from an individual’s current
position to prepare for interoperable electronic health records
AbstractInteroperable electronic health records (EHRs) are promis-ing tools to improve quality and efficiency in health care. This course will look at the tides of change and how dentistry became part of the interoperable EHR process. It will assess the impact of standards, coding, and systems being developed by the American Dental Association for EHR. The reader is given five simple steps that can be taken to help with navigat-ing the choppy waters of adoption.
Sweeping changes have come to health care. Will dentistry be ready? When will dentistry be required to use interopera-ble electronic health records (EHR) in 2013? 2014? 2015? There is no fixed date for the vast majority of practices. The current exceptions are those dental practices billing Medi-care/Medicaid; according to the ADA, these practices must demonstrate meaningful use of EHR by 2015. Whether paper or electronic, all records should be both meaningful and useful. Records are the most important tools for verifying the delivery of predictable wellness-centered care based on up-to-date evidence-based decision-making that patients want and expect.
Tides of Change1
It can feel as if technology drives barriers between people, particularly when learning to integrate new tools. Our heads are looking down at the screen more often than looking at the patient. This is nothing more than a learning cycle. While in the learning stages, there can be some disconnect. For many, personal computers, iPads, and smartphones were game changers and have created a world in which we have become competent. We are now looking for increased engagement and human-to-human interaction.
A white paper from futurist Dr. Graeme Codrington di-scusses four growing trends in communication. They are:• User-generatedcontent—thedesireforpeopletoengage
and contribute• Socialmedia—thedesiretointeractandconnect• Augmentedreality—thedesiretomakesenseoftheworld
by tapping into data and information• Mobilityinthecloud—thedesiretodoallofthesethings
anywhere on any devices using any platform at any time.1
We have already experienced patients bringing in in-formation they have found online. The questions they are asking are more complex than ever before. They visit web-sites such as www.patientslikeme.com. This site was created in 2004 based on the belief that “... when patients share real-world data, collaboration on a global scale becomes possible. New treatments become possible. Most importantly, change becomes possible.”2 This website is just one of many exam-ples fulfilling Dr. Codrington’s prophetic future. Dental professionals can’t sit this one out, playing ostrich, thinking they will retire before EHR become reality. If that is your plan, you should have retired a few years ago. There is no “maybe,” there is only “when” to be determined.
Evolution of EHREHR is not a new initiative; it has been an ongoing effort for decades. Dentistry became specifically involved when, on April 27, 2004, then-President Bush called for the major-ity of Americans to have EHR within 10 years and signed an Executive Order.3-4 This order included dentistry based on the information provided by David Satcher, MD, PhD, then surgeon general, in the first-ever Surgeon General’s Report on Oral Health5 in May 2000. The American Recovery and Reinvestment Act (ARRA) was signed into law by President Obama on February 17, 2009. Part of that law included the Health Information Technology for Economic and Clinical Health (HITECH) Act6 to further promote the adoption and meaningful use of health information technology. There are multiple benefits projected when all of this comes to fruition.
HIMSS (Healthcare Information Management Systems Society) defines EHR as “a longitudinal electronic record
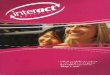
Figure 1. Percent distribution of electronic health record satisfaction among office-based physicians: United States, 201118
Very dissatis�ed
Somewhatdissatis�ed
47Somewhat satis�ed
38Very satis�ed
5
10
Notes: Data represent o�ce-based physicians who reported having adopted electronic health record systems (55% of sample). The sample includes nonfederal,o�ce-based physicians and excludes radiologists, anesthesiologist, and pathologists. Missing values are excluded. Source: CDC/NCHS, Physician Work�ow study, 2011.

95www.dentaleconomics.com | 03.2013
of patient health information generated by one or more en-counters in any care delivery setting. Included in this infor-mation are patient demographics, progress notes, problems, medications, vital signs, past medical history, immuniza-tions, laboratory data and radiology reports.”7 EHR is not an automated version of the paper record. By having access to a clearer picture of the patient’s complete health, not just the patient’s oral condition, dental practitioners can improve and enhance care. There is no reason to invest the time, energy and finances unless there is a return on investment (ROI). Enhanced care is what ever-growing knowledge-driven pa-tients want and expect.
An analogy can be made to smartphones. They are very different than lower-end phones and almost completely unlike old-style home phones. Smartphones bring together combined functions of digital cameras, digital video, recor-ding devices, player devices, web browsers, touchscreens, GPS navigation, gaming, and a huge variety of applications. Smartphones give us more possibilities; so will interopera-ble EHR. Smartphones are interoperable, meaning there is an electronic architecture behind the scenes that allows a Samsung on the Verizon system to be able to communicate with an iPhone on AT&T. It doesn’t mean that the phone numbers listed in the Samsung or iPhone directory will go into the other phone or a central data base. All or parts of information from primary health care, pharmacies, hospitals, individual practitioners, and diagnostic labs will be accessible to other practitioners based on the permission of that indivi-dual patient.
StandardsDental standards are to help keep everyone on the same page and ensure the highest level of patient safety. There are a va-riety of architectures developed for electronic transference. Some readers are familiar with the DICOM (Digital Imaging and Communication in Medicine) standard used for transfer-ring digital radiographs. In September 2009, the American Dental Association (ADA) signed an agreement with Health Level Seven International (HL7), a leading global authority on health-care information interoperability and standards, to develop consistent dental IT standards in order to enhance coordination between medical and dental offices.8
The ADA Standards Committee on Dental Informatics (SCDI) helps dentists streamline and empower their practi-ces through the use of information technology.9 Jean Narcissi, ADA Director of Dental Informatics, presented a program on September 13, 2011, updating ADA’s current work on the X12/5010 updates, WEDI, SCDI, SCDP, ISO TC 215, ISO TC 106, IHE, and IHTSDO.10 There is no reason for the purpose of this article to attempt to describe these standards. It is sufficient to say, this is not a simple process. It has been the absence of standards for EHR that has created major ob-stacles in the past.
CodesPhysicians, medical examiners, and coroners have used a di-agnosis coding system called the International Classification of Diseases (ICD) since the early 1900s. It was developed collaboratively between the World Health Organization (WHO) and 10 international centers so that the medical terms reported on death certificates can be grouped together for statistical purposes.11 Medicine was moving toward a 2013 goal date for implementation of ICD-10. The Depart-ment of Health and Human Services announced on April 9, 2012,adelay forrequiredcompliancebyoneyear—fromOct.1,2013,toOct.1,2014—foruseofICD-10coding.12
How does this affect dentistry? The key portion of Ms. Narcissi’s report is the work being done on SNODENT (Sy-stemized Nomenclature of Dentistry), a diagnostic coding system for dentistry. In order for dental records to interface with other health-care records, there needs to be coding sy-stems. SNODENT is a 6,000+ term dental diagnostic voca-bulary designed as a diagnostic companion13 to the Current Dental Terminology (CDT) treatment codes. Ms. Narcissi’s report states SNODENT will help with:• Decisionsupport/patientsafety—Forexample,isthepatient
allergic to penicillin?• Statistical/populationdata—Forexample,howmany
patients have root caries?• Financialdata-mappingtoICDtoidentifypatientsrequiring
additional oral treatment for related systemic conditions and administrative reporting
• Developmentofdecisionsupportsystems• Developmentofevidence-basedpracticeresearch10
An updated ADA Dental Claim Form 2012 became available in spring 2012 to incorporate key HIPAA (Health Insurance Portability and Accountability Act) changes and includes a new section for diagnostic coding (Figure 2). This area for diagnostic codes is when the specific diagnosis may minimize the risks associated with the connection between the patient’s oral and systemic health conditions.14 At this time, these are the ICD-9 codes. Offices do not have to wait until SNODENT is completed. ADA created the CDT Companion: The ADA Guide to Dental Coding (www.ada.org). Chapter 10 covers dental/medical procedure cross coding. Other consultants have also created cross-coding guides.
Clinical Decision Support Systems (CDSS) provide clini-cians, staff, and patients with knowledge and person-specific information, presented at appropriate times, to enhance he-alth and health care.15 They do not provide generic medical advice, rather are considered patient-specific data to assist clinicians at the point of care. CDSS are designed to be used for a wide range of decisions including those for prevention, screening, diagnosis, treatment, drug dosing, test ordering, and/or chronic disease management.

96 03.2013 | www.dentaleconomics.com
Figure 2. ADA Dental Claim form 201214
SAMPLE

97www.dentaleconomics.com | 03.2013
ADA has created the Center for Evidence-Based Den-tistry (http://ebd.ada.org/) to connect the latest research findings with the daily practice of dentistry.16 The reciprocal of this concept can also be helpful in the future. Clinical prac-tice statistics and evidence can and should also feed the EBD system. This can only be accomplished through EHR.
Navigating the Choppy WatersYou may be thinking this is NOT going to happen in my prac-tice because the dentist will retire first. The window for retiring before EHR is already closed. A practice without any kind of EHR integration won’t be worth much to a potential buyer.
If your practice is at the beginning of this process, you can get your feet wet with a 2010 book EHR for Dummies by Dr. Trenor Williams and Anita Samarth (Wiley Publishing, Inc., Hoboken, N.J.) It is divided into five sections from the basics, planning, buying a system, optimizing, and improving, with the final section called The Part of Tens that gives the top ten websites, pitfalls to avoid, and questions to ask while making the move.
Some offices have fully integrated a paperless practice. That’s wonderful and gives you a step up. Yet your software probably has capabilities that you are not using. Even if you are paperless with your current system, there are still steps to take. Integration of EHR is an ongoing process.
Action StepsThe first section of this article gave you some background that at first glance can seem overwhelming. No matter where your office is in the transition process, you can handle it when fol-lowing these how-to action steps.
Action Step #1 CommunicationIt is important to include patients in the ground floor of EHR implementation. You may be surprised at the support you get. Many have gone through it with their own work. They have been experiencing it happening at most hospitals and many physicians’ offices. The National Center for Health Statistics reported in 2011 that 55% of physicians have adopted an EHR system and a majority (85%) are somewhat to very satisfied.17 Sending a note to let patients know of the benefits they will get from EHR will help smooth the way. Most patients will not be surprised; rather they are more likely accepting as they have been with their physicians. Many may even think that it’s about time as discussed earlier; they will want to know when the app will be ready.
Action Step: Design, with your team, a note to let pa-tients know you are implementing EHR.
Action Step #2 Dental RecordsIn 2010, ADA updated their Dental Records18 guidelines that can readily be accessed on the ADA website. These guidelines
are not meant for EHR only. The ADA guidelines list the specific information that should be contained in a dental record no matter the medium. The ADA document contains helpful information including page 6 links to specific documentation guidelines and requirements from individual states.
For offices already using digital recordkeeping, the softwa-re is most likely capable of managing these basics; yet there is no guarantee the guidelines are being followed. Page 13 of the guideline has a list of common errors or inaccuracies from the insurance carrier’s point of view. Box 1 shows a partial list. An important section is Ownership of the Record; using this guideline is a small step toward HIPAA compliance.
Action Step: Download ADA Dental Records18 guidelines and have a review exercise at a staff meeting to make sure eve-ry person in the practice is consistent in their recordkeeping.
Action Step #3 AbbreviationsProfessions, businesses, and particularly government use ab-breviations and acronyms that can seem like alphabet soup and make little sense to a newcomer or have a completely different meaning in a different arena. Historically, in dentistry, each practice used whatever abbreviations and acronyms that made sense to them. The only requirement was if there was litigation, a key was needed; this too is changing. With EHR, consistent use of well-defined abbreviations and acronyms will facilitate improved communication. ADA has again stepped up to the plate with their 2008 abbreviations19 guidelines that can readily be downloaded from the ADA website. Adopting these abbre-viations is a step toward diagnostic coding.
Action Step: Download ADA abbreviations guide.19 Have a team meeting to use the template in the book to create a list of abbreviations, acronyms, and symbols your practice will consistently utilize.
Action Step #4 HIPAASecurity is a hot button for most of us, as it should be. Vast amounts of electronic data come with many new opportuni-ties for a new kind of theft and security breaches orchestrated from continents away. (How many of us have gotten emails
Box 1 Partial List from ADA Dental Records16

98 03.2013 | www.dentaleconomics.com
fromNigeria?)Uneasiness over theprivacy and security ofelectronic health information falls into two general categories: (1) concerns about inappropriate releases of information from individual organizations and 2) concerns about the systemic flows of information throughout the health-care and related industries. These concerns are real and appropriate.
HIPAA is about privacy and security. Many dental profession-als only know HIPAA as the form patients had to sign a couple years ago. After 14 years of HIPAA regulation, some dental pro-fessionals still using paper records assume their practice is unaf-fected by HIPAA rules. In 2011, ADA created an EHR Primer20 that clearly states,
“Regardless of your decision on adoption of EHRs, you must still comply with: HIPAA Privacy and Security Standards and HITECH Breach Notification Rule.”20
A lesser known part of the HITECH Act affecting practitioners significantly expands the reach of HIPAA and gives it more teeth. The HITECH Act increases the civil monetary penalties for HIPAA noncompliance to as much as $50,000 per violation.4 ADA has created a Complete HIPAA Compliance Kit21 that features updated HIPAA privacy and security information and incorporates HITECH changes; it includes a three-year update service assuring a resource that covers pending changes.
Action Step: Buy the ADA Complete HIPAA Com-pliance Kit21 and decide who will be your HIPAA privacy officer. Give that person the time and support needed to learn what is necessary, including taking courses. Develop with the entire team how you will protect and safeguard as well as share patients’ private information
Action Step #5 Meaningful UseRecording information electronically will not mean that it is meaningful. With EHR, meaningful use can seem confusing at first. There are numerous complex definitions and govern-mental criteria that currently have little meaning for dentistry with the exception mentioned earlier of those dental practices billing Medicare/Medicaid. So why should dental profes-sionals care about EHR meaningful use? Two personal stories can best illustrate the reasons.• Patient 1 was referred to a specialist. She is a proactive patient
who wants to engage, interact, and contribute to decisions by tapping into her personal information. She has her many tests and information saved on her cell phone so she can access it when needed. (She sounds like Dr. Codrington’s description.) When making the appointment with the specialist, she states she has a recent CT scan. She was asked to fax the report in advance and to arrive at the office 30 minutes before the ap-pointment to fill out paperwork. She complies to the request, also bringing copies of previous tests and her medication
history. She has to fill out three forms, repeating some of the same data several times. There is not enough space for her history or medication list. She is brought into the treatment room and asked the same questions over again. The person records something in the computer but doesn’t ask the patient to check for accuracy. When the physician arrives, he asks many of the same questions again. He doesn’t read anything the patient filled out, none of the history she brought, has not read the report faxed in advance, and only briefly looks over what the previous person entered. Based on his questions, much was missing.
• Patient 2 has small cell lung cancer and has been hospital-ized for 12 days. During this 12 day period, it is spring break and the hospital team of nurses, techs, oncologists, and everyone involved with care is different nearly every day. It is obvious to the patient and his wife that every person see-ing the patient knows the case. They are clear on the details; they know what has already happened and the care plan.
Why the difference? The culture of the hospital for Pa-tient 2 dictates that every person must read and familiarize themselves with the chart BEFORE entering the patient’s room. This was not the case for Patient 1.
Action Step: Create a practice culture where records truly become tools for delivering predictable wellness-centered care based on up-to-date evidence-based decision-making. (For further details, go to www.aurorahealthcare.org/misc/temp/home-page/beeson.aspx.)
EHR bottom line Transitioning to EHR won’t be worth the effort if there is no improvement, enhancement, or value gained by all stakehold-ers, particularly the patients. EHR will not make inadequate recordkeeping magically become useful, and it can’t be useful if it is not read. There is no reason to wait until dentistry has to comply. Rules and laws dictate only the lowest end; what is required. By the time a patient sits in our chair, we have their trust; we don’t have to create it. Dental professionals reading and familiarizing themselves with useful, meaningful records —whetherpaperorelectronic—before seeing patients build trust and help patients get what they want and expect.
References:1. Codrington G. The TIDES of Change White Paper. May 2010. http://
www.tomorrowtoday.uk.com/articles/pdf/TomorrowToday_TIDES_of_Change_article.pdf. Accessed 7/25/12.
2. PatientsLikeMe. http://www.patientslikeme.com/about/openness Accessed 7/25/12.
3. Brailer D. The Decade of Health Information Technology: Delivering Consumer-centric and Information-rich Health Care Framework for Strategic Action. Department Health and Human Services. July 21, 2004. http://www.providersedge.com/ehdocs/ehr_articles/The_Decade_of_HIT-Delivering_Customer-centric_and_Info-rich_HC.pdf Accessed 7/25/12.
4. The Health Information Technology for Economic and Clinical Health (HITECH) Act, enacted as part of the American Recovery and Reinvestment Act of 2009. Department of Health and Human Services. 2009. http://www.

99www.dentaleconomics.com | 03.2013
hhs.gov/ocr/privacy/hipaa/understanding/coveredentities/guidance_breachnotice.html Accessed 7/25/12.
5. US Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General — Executive Summary. Rockville, MD: US Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2000. http://www.nidcr.nih.gov/datastatistics/surgeongeneral/report/executivesummary.htm Accessed 7/25/12.
6. HITECH Act Enforcement Interim Final Rule. Department Health and Human Services. February 17, 2009 http://www.hhs.gov/ocr/privacy/hipaa/administrative/enforcementrule/hitechenforcementifr.html Accessed 7/26/12.
7. EHR Electronic Health Record. HIMSS. 2012. http://www.himss.org/asp/topics_ehr.asp Accessed 7/27/12.
8. Health Level Seven and the American Dental Association Sign Agreement to Develop Joint Healthcare IT Standard Initiatives. September 2, 2009. Available at: http://www.hl7.org/documentcenter/public/pressreleases/HL7_PRESS_20090902.pdf Accessed 7/25/12.
9. Standards. American Dental Association. http://www.ada.org/275.aspx Accessed 7/25/12.
10. Narcisi J. Update from ADA. American Dental Association. September 13, 2011. http://www.nadp.org/Libraries/CONVERGE/SNODENT-Dental_Diagnostic_Coding_Narcisi_9_13_11.sflb.ashx Accessed 5/1/12.
11. International Classification of Diseases. World Health Organization. http://www.who.int/classifications/icd/en/ Accessed 7/25/12.
12. New health care law provisions cut red tape, save up to $4.6 billion. Department of Health and Human Services. April 12, 2012. http://www.hhs.gov/news/press/2012pres/04/20120409a.html Accessed 7/24/12.
13. SNODENT goes global. American Dental Assocation. June 18, 2012. http://www.ada.org/news/7187.aspx Accessed 7/25/12.
14. 2012 ADA Dental Claim Form available. American Dental Assocation. April 9, 2012. http://www.ada.org/news/6959.aspx Accessed 7/26/12.
15. Clinical Decision Support Systems: State of the Art. Agency for Healthcare Research and Quality. June 2009. http://healthit.ahrq.gov/images/jun09cdsreview/09_0069_ef.html Accessed 5/2/12.
16. Evidence Based Dentistry. American Dental Association. http://www.ada.org/276.aspx Accessed 9/1/10.
17. Jamoom E, Beatty P, Bercovitz A, and Woodwell D. Physician Adoption of Electronic Health Record Systems: United States, 2011. NCHS Data Brief No. 98 July 2012. http://www.cdc.gov/nchs/data/databriefs/db98.pdf Accessed 7/27/12.
18. Dental Records. American Dental Assocation. 2010. http://www.ada.org/sections/professionalResources/pdfs/dentalpractice_dental_records.pdf Accessed 7/5/11.
19. Dental Abbreviations, Symbols and Acronyms. American Dental Association. 2nd Edition, 2008. http://www.ada.org/sections/professionalResources/pdfs/dentalpractice_abbreviations.pdf Accessed 7/5/11.
20. EHR Primer. American Dental Assocation. 2011. https://www.ada.org/sections/dentalPracticeHub/members/ehr_primer.pdf Accessed 5/3/12.
21. HIPAA compliance kit helps dentists protect patients’ privacy. American Dental Association. April 21, 2011. http://www.ada.org/news/5410.aspx Accessed 7/5/11.
Author profilePatti DiGangi, RDH, BS, is a vision-driven practicing clinician. She is an American Dental Association Evidence Based Champion and Current Dental Terminology licensee, currently writing a series of mini-books on insurance coding for hygienists. She is a member of the National Speakers Association and a Certified Speaking Profes-sional candidate. She is a key opinion leader for multiple manufac-turers and well known author. Patti is a certified Health Information Technology trainer and a member of the American Health Informa-tion Management Association, taking an active role in our shaping the changes in our electronic world.
Author DisclosurePatti DiGangi, RDH, BS has no commercial ties with the sponsors or providers of the unrestricted educational grant for this course.
Reader FeedbackWe encourage your comments on this or any PennWell course. For your convenience, an online feedback form is available at www.ineedce.com.
Online CompletionUse this page to review the questions and answers. Return to www.ineedce.com and sign in. If you have not previously purchased the program select it from the “Online Courses” listing and complete the online purchase. Once purchased the exam will be added to your Archives page where a Take Exam link will be provided. Click on the “Take Exam” link, complete all the program questions and submit your answers. An immediate grade report will be provided and upon receiving a passing grade your “Verification Form” will be provided immediately for viewing and/or printing. Verification Forms can be viewed and/or printed anytime in the future by returning to the site, sign in and return to your Archives Page.
Questions
1. Trends in communication:a. Decreasing the desire for increased engagement and
human-to-human interactionb. Driving greater barriers between peoplec. Mobility in the cloudd. Create less complex patient questions
2. Electronic health records are defined as: a. Paperless dental recordsb. Longitudinal electronic record from any care delivery
settingc. Chartless hospital and physician recordsd. Automated paper record
3. Interoperable meansa. Any health-care provider can access without reservationb. Government controls informationc. Loss of privacyd. Accessible only by permission of patient
4. All statements about SNODENT are true except:a. Dentistry needs diagnostic coding to be interoperableb. Available through ADA websitec. 6,000+ term dental diagnostic vocabularyd. Mapping to ICD system to identify patients
requiring additional oral care for related systemic conditions
5. ADA Center for Evidence Based Dentistry provides:a. Help connecting research to daily practiceb. Patient-specific datac. New insurance formd. Cross-coding information
6. The percentage of physicians adopting EHR by 2011a. 25%b. 55%c. 85%d. 45%
7. ADA Dental Records guidelines contain:a. Abbreviation, acronyms, and symbolsb. Are only for EHRc. Automatic for already paperless officesd. Lists of what should be contained in a record
8. Abbreviationsa. Are usually obvious to any observerb. Make little difference to future EHRc. Are a step toward diagnostic codingd. Need no key due to familiarity
9. HIPAAa. Has minimal penalties for non-complianceb. Is about the real and appropriate concerns about
privacy and securityc. Has no compliance required if not using EHRd. Is already accomplished in most practices
10. Meaningful use in dentistry is:a. Not needed yetb. Fully definedc. An alphabet soup of lettersd. An opportunity to enhance care when practice culture
supports it
11. Dentistry became specifically involved in electronic health records process through
a. President George Bush 2004 Executive Orderb. 2009 American Recovery and Reinvestment Actc. Surgeon General David Satcher 2000 Surgeon
General’s Report on Oral Healthd. All of the above
12. EHRa. Began in 2004 under the Bush administrationb. Is not a new initiativec. Can be accomplished in a few steps by buying the
right equipmentd. Has been adopted by 25% of physicians
13. Clinical Decision Support Systems providea. Generic informationb. Medical advicec. Person‐specific informationd. Data from single portal
14. A dental practice with little or no integra-tion of EHR bea. May not be worth much to a potential buyerb. Easy to sellc. Equal to a completely paperless officed. No big deal because there is no date EHR is required
15. If a practice choose not to adopt EHR’s, they still musta. Follow ADA/FDA Guidelines for Radiologyb. Comply with HIPAA Privacy and Security Standards
and HITECH Breach Notification Rulec. Obey rules for CDSSd. Purchase ADA HIPAA Compliance Kit

Customer Service 216.398.7822
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
ELECT312DE
COURSE EVALUATION and PARTICIPANT FEEDBACKWe encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected].
INSTRUCTIONSAll questions should have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification of Participation forms will be mailed within two weeks after taking an examination.
PROVIDER INFORMATIONPennWell is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, not does it imply acceptance of credit hours by boards of dentistry.
Concerns or complaints about a CE Provider may be directed to the provider or to ADA CERP ar www.ada.org/cotocerp/
COURSE CREDITS/COSTAll participants scoring at least 70% on the examination will receive a verification form verifying 1 CE credit. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact PennWell for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California Provider. The California Provider number is 4527. The cost for courses ranges from $20.00 to $110.00.
RECORD KEEPINGPennWell maintains records of your successful completion of any exam for a minimum of six years. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
CANCELLATION/REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
© 2012 by the Academy of Dental Therapeutics and Stomatology, a division of PennWell
ANSWER SHEET
Dental Electronic Health Records: Meaningful and Useful
Name: Title: Specialty:
Address: E-mail:
City: State: ZIP: Country:
Telephone: Home ( ) Office ( )
Lic. Renewal Date: AGD Member ID:
Requirements for successful completion of the course and to obtain dental continuing education credits: 1) Read the entire course. 2) Complete all information above. 3) Complete answer sheets in either pen or pencil. 4) Mark only one answer for each question. 5) A score of 70% on this test will earn you 1 CE credit. 6) Complete the Course Evaluation below. 7) Make check payable to PennWell Corp. For Questions Call 216.398.7822
Educational Objectives1. Identify new communication and technology trends affecting health care
2. Discuss historic decisions bringing dentistry into interoperable electronic health records
3. Determine the American Dental Association directions in creating standards and codes
4. Take five simple action steps from an individual’s current position to prepare for interoperable electronic health records
Course Evaluation1. Were the individual course objectives met? Objective #1: Yes No Objective #3: Yes No
Objective #2: Yes No Objective #4: Yes No
Please evaluate this course by responding to the following statements, using a scale of Excellent = 5 to Poor = 0.
2. To what extent were the course objectives accomplished overall? 5 4 3 2 1 0
3. Please rate your personal mastery of the course objectives. 5 4 3 2 1 0
4. How would you rate the objectives and educational methods? 5 4 3 2 1 0
5. How do you rate the author’s grasp of the topic? 5 4 3 2 1 0
6. Please rate the instructor’s effectiveness. 5 4 3 2 1 0
7. Was the overall administration of the course effective? 5 4 3 2 1 0
8. Please rate the usefulness and clinical applicability of this course. 5 4 3 2 1 0
9. Please rate the usefulness of the supplemental webliography. 5 4 3 2 1 0
10. Do you feel that the references were adequate? Yes No
11. Would you participate in a similar program on a different topic? Yes No
12. If any of the continuing education questions were unclear or ambiguous, please list them.
___________________________________________________________________
13. Was there any subject matter you found confusing? Please describe.
___________________________________________________________________
___________________________________________________________________
14. How long did it take you to complete this course?
___________________________________________________________________
___________________________________________________________________
15. What additional continuing dental education topics would you like to see?
___________________________________________________________________
___________________________________________________________________
For iMMEDiATE results, go to www.ineedce.com to take tests online.
Answer sheets can be faxed with credit card payment to (440) 845-3447, (216) 398-7922, or (216) 255-6619.
Payment of $20.00 is enclosed. (Checks and credit cards are accepted.)
If paying by credit card, please complete the following: MC Visa AmEx Discover
Acct. Number: ______________________________
Exp. Date: _____________________
Charges on your statement will show up as PennWell
If not taking online, mail completed answer sheet to
Academy of Dental Therapeutics and Stomatology,A Division of PennWell Corp.
P.O. Box 116, Chesterland, OH 44026 or fax to: (440) 845-3447
AGD Code 561