Embed Size (px)
Citation preview
D E N T I S T R Y / O R A L S U R G E R Y / O R I G I N A L R E S E A R C H
Charlotte Lewis, MD, MPHHeather Lynch, MDBrian Johnston, MD, MPH
From the Child Health Institute(Lewis), Department ofPediatrics (Lewis, Lynch,Johnston), and Robert WoodJohnson Clinical ScholarsProgram (Lynch), University ofWashington, and the Harbor-view Injury Prevention andResearch Center (Johnston),Seattle, WA.
Copyright © 2003 by the AmericanCollege of Emergency Physicians.
0196-0644/2003/$30.00 + 0doi:10.1067/mem.2003.234
Dental Complaints in Emergency Departments:
A National Perspective
J U L Y 2 0 0 3 4 2 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 3
Study objective: Using nationally representative data, we sought to describe theincidence of emergency department (ED) visits for dental-related complaints for chil-dren and adults in the United States. We hypothesized that dental-related ED visitswere more likely than other ED visits to have Medicaid or no insurance as the payer.
Methods: We used data from the 1997 to 2000 National Hospital Ambulatory MedicalCare Survey, a national probability sample survey of hospital ED visits that is con-ducted by the National Center for Health Statistics. From these data, all ED visits inwhich one of the reasons for the visit was toothache or tooth injury were compiledand used to determine national estimates of counts and rates of ED visits for dental-related complaints. Logistic regression analysis on the outcome variable, presenta-tion to the ED with a dental complaint (versus other problem), was performed todetermine the association with payer and other covariates.
Results: During the 4-year period from 1997 to 2000, there were an estimated 2.95million ED visits in the United States for complaints of tooth pain or tooth injury, for anaverage of 738,000 visits annually. Population-based rates and proportion of all EDvisits for dental complaints were highest in the 19- to 35-year-old group, accountingfor 1.3% of all ED visits and 5.6 ED visits per 1,000 people in this age category. “Dentalproblem, not otherwise specified” was the most commonly assigned InternationalClassification of Diseases, Ninth Revision, Clinical Modification diagnosis. Multi-variate logistic regression results indicated that the adjusted odds of presentation tothe ED for a dental complaint compared with other problems were significantly ele-vated for visits in which Medicaid or self-pay was listed as the payer relative to thosewith private insurance.
Conclusion: EDs are an important point of care for dental-related complaints, par-ticularly for individuals who lack private insurance. ED providers should be equippedto triage, diagnose, provide basic treatment, and ensure appropriate follow-up carefor dental problems, which may require enhancement of dental training for emer-gency medicine providers and improved dental care during and after ED visits.[Ann Emerg Med. 2003;42:93-99.]

D E N T A L C O M P L A I N T S I N E M E R G E N C Y D E P A R T M E N T SLewis, Lynch & Johnston
I N T R O D U C T I O N
Medicine and dentistry have largely existed as indepen-dent entities, with distinct training, care systems, andsettings where care is provided. However, patients mayseek dental care from medical providers because theyare unaware of this distinction, because the dentalproblem exists in the context of an injury or other medi-cal problem, or because they lack access to traditionaldental care. Emergency departments (EDs) are a well-known point of entry into the health care system, par-ticularly for persons with difficulty accessing routine,preventive services; 44% of Americans lack dental in-surance and, therefore, may experience these difficul-ties in accessing nonemergency dental services.1 How-ever, to date, knowledge of the nature of dental concernsamong patients presenting to EDs has been limited toinformation obtained from single institutions.2-11 Toour knowledge, no previous study has addressed thenature of ED use for dental complaints from a nationalperspective. Using nationally representative data, wesought to describe the incidence of dental-related com-plaints most commonly reported among children andadults visiting EDs. In addition, we hypothesized thatdental-related ED visits were more likely than other EDvisits to have Medicaid or no insurance as the payer.
M A T E R I A L S A N D M E T H O D S
We used 1997 to 2000 National Hospital AmbulatoryMedical Care Survey data, which are publicly availablefrom the US Centers for Disease Control and PreventionWeb site.12
The National Hospital Ambulatory Medical CareSurvey is a national probability sample survey of hospi-tal ED visits that is conducted by the National Centerfor Health Statistics. EDs were located in noninstitu-tional general and short-stay hospitals, exclusive of fed-eral, military, and Veterans Affairs hospitals, in the 50states and the District of Columbia.12
The basic sampling unit for the National HospitalAmbulatory Medical Care Survey is the patient visit.Within an ED, patient visits were systematically selected
9 4 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 2 : 1 J U L Y 2 0 0 3
throughout a randomly assigned 4-week reportingperiod.12 Trained hospital staff collected data for theNational Hospital Ambulatory Medical Care Survey. Apatient record form was completed for each visit andincluded information on patient demographic charac-teristics; patient’s complaint; time, day of week, andmode of arrival; whether the visit was injury related andcause of injury; categories of diagnostic tests and proce-dures performed; discharge diagnoses; medicationsprescribed; and disposition. Up to 3 reasons for visitcodes and 3 discharge diagnoses were possible for eachvisit. Diagnoses were coded according to the Inter-national Classification of Diseases, Ninth Revision, Clini-cal Modification (ICD-9-CM).13 Additional detail on theNational Hospital Ambulatory Medical Care Surveymethodology can be obtained from the Centers forDisease Control and Prevention.12
We extracted all ED visits from the 1997 to 2000National Hospital Ambulatory Medical Care Surveydata sets in which one of the patient’s complaints or rea-son for the visit was toothache or tooth injury (reason-for-visit codes 1500.0 and 1500.1). We selected ourstudy population according to the patient’s reason forthe visit because we were particularly interested in thephenomenon of patients using the ED for a perceiveddental problem. In addition, we tabulated patients’ICD-9-CM diagnoses assigned at discharge for patientswho presented with a dental complaint and those whowere discharged with any dental ICD-9-CM diagnosis.
Statistical analyses were performed with Stata soft-ware (version 7.0, Stata Corporation, College Station,TX). Counts were weighted by using National HospitalAmbulatory Medical Care Survey–provided weights toderive national estimates of numbers of ED visits fordental-related complaints. All estimates were based onobservations with relative standard errors of less than30%, a criterion of reliability established by the NationalCenter for Health Statistics.12 With 2 exceptions, notedin the tables, estimates were based on observations ofmore than 30 occurrences, an additional reliability cri-terion.12 We generated population-based incidencerates of ED visits for dental complaints by using US cen-sus population estimates for 1997 to 2000.14 The sur-

D E N T A L C O M P L A I N T S I N E M E R G E N C Y D E P A R T M E N T SLewis, Lynch & Johnston
middle-aged adults; 19- to 50-year-olds accounted for77% of these visits but for only 47% of other ED visits.The payer distribution was also significantly differentfor ED dental-complaint visits relative to other ED vis-its; self-pay was the most common payer for dental-complaint visits, whereas private insurance was themost common payer for other ED visits (Table 2).
Relative to other ED visits, visits for dental com-plaints were more likely to occur on the weekend.However, there was no significant difference betweendental complaint and other ED visits in the proportionof visits that occurred after hours during weekdays.Approximately 10% of visits with a dental-related com-plaint had any procedure performed compared with42% of ED visits for other reasons. Procedures wereclassified into general categories; the most commonduring dental-complaint visits were wound care (2.4%),intravenous-tube placement (2.0%), and ear, nose, andthroat and eye care (2.0%). “Another procedure” wasdocumented in 3.7% of ED visits for dental complaints;however, the data set provided limited detail on specificprocedures performed. More than 80% of visits re-sulted in the prescription of at least 1 medication, mostcommonly antibiotics and pain medications. Dental-complaint visits were significantly more likely to resultin the prescription of a medication (most commonlypain medication, narcotic, or antibiotic) relative tonon–dental complaint visits. Dental-complaint visits
vey commands in Stata were used with NationalHospital Ambulatory Medical Care Survey variables toaccount for the 4-stage probability sampling design,generate weighted proportions and mean estimates,and perform χ2 and logistic regression analysis.
We assessed the independent association betweenpresentation to the ED with a dental complaint (com-pared with ED presentation for other problems) andeach variable hypothesized a priori to be associatedwith the outcome variables by using logistic regressionmultivariate analysis. Independent variables includedin the regression equation were modeled categoricallyand included primary payer (private as reference), agecategory (0 to 6 years as reference), race (white as refer-ence), whether visit was injury related, US geographicregion (northeast as reference), hospital ownership(proprietary as reference), and metropolitan statisticalarea (in metropolitan statistical area as reference).
R E S U L T S
During the 4-year period from 1997 to 2000, there were693 observed ED visits for complaints of tooth pain ortooth injury, for an estimated 2.95 million ED visitsnationally and an average of 738,000 visits yearly. Therewere no significant time trends in the incidence of EDvisits for dental complaints. Dental complaints accountedfor 0.7% of all ED visits (Table 1). As a point of reference,dental complaints were approximately as common aspresentation to the ED with “painful urination,” forwhich there were an estimated 2.86 million ED visitsduring this same period.
Population-based rates and proportion of all ED visitsfor dental complaints were highest in the 19- to 35-year-old group, accounting for 1.3% of all ED visits and 5.6ED visits per 1,000 people in this age category (Table 1).Children younger than 7 years comprised the smallestportion of ED visits; only 5% of dental-complaint visitsto the ED were in this age group. However, young chil-dren had the greatest proportion of dental-related visitsbecause of injury; 46% of their ED visits for dental com-plaint were associated with an injury. The majority ofED visits for dental complaints were made by young and
J U L Y 2 0 0 3 4 2 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 5
Table 1.Weighted population-based rates, proportion of all of ED vis-its, and dental-complaint visits by age category.
Percentage ofRate/1,000 Dental Complaints
People Among All ED VisitsAge Category, y (95% CI) (95% CI)
0–6 1.4 (0.9–1.9) 0.27 (0.18–0.36)7–18 1.6 (1.0–2.1) 0.54 (0.36–0.73)19–35 5.6 (4.5–6.6) 1.31 (1.13–1.49)36–50 3.2 (2.7–3.8) 1.01 (0.84–1.18)>50 0.8 (0.5–1.1) 0.22 (0.15–0.29)All ages 2.7 (2.3–3.1) 0.73 (0.64–0.81)
CI, Confidence interval.
D E N T A L C O M P L A I N T S I N E M E R G E N C Y D E P A R T M E N T SLewis, Lynch & Johnston
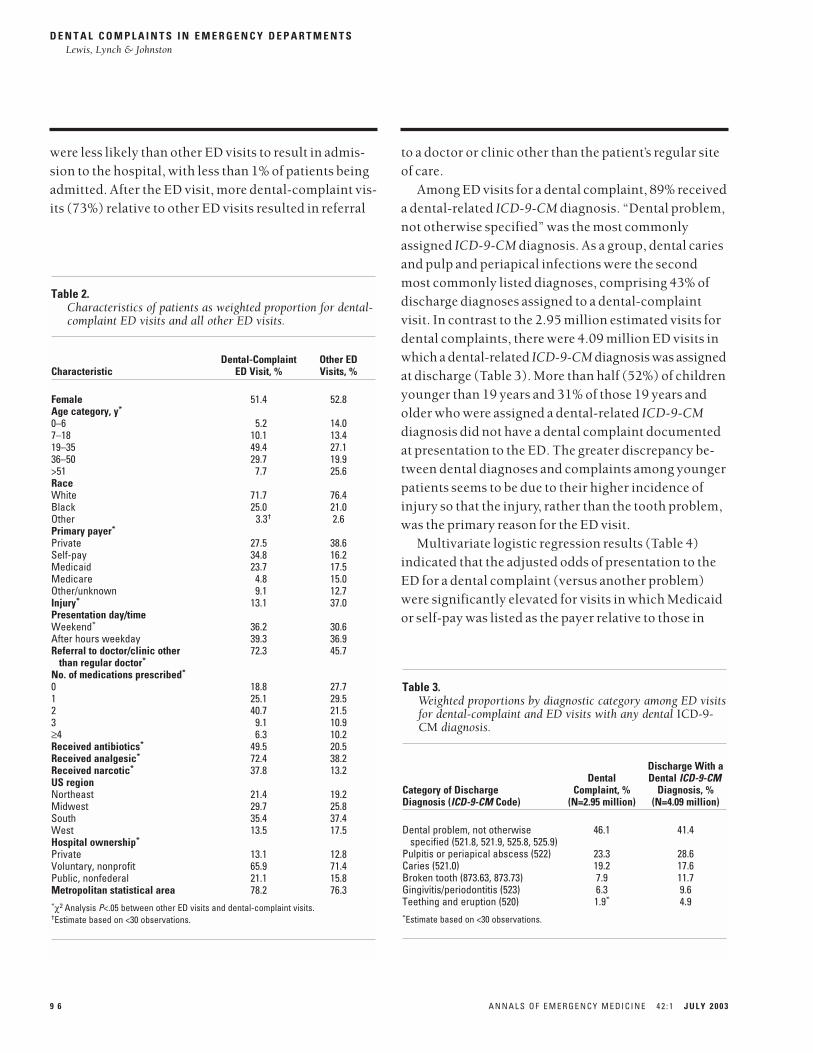
were less likely than other ED visits to result in admis-sion to the hospital, with less than 1% of patients beingadmitted. After the ED visit, more dental-complaint vis-its (73%) relative to other ED visits resulted in referral
9 6 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 2 : 1 J U L Y 2 0 0 3
to a doctor or clinic other than the patient’s regular siteof care.
Among ED visits for a dental complaint, 89% receiveda dental-related ICD-9-CM diagnosis. “Dental problem,not otherwise specified” was the most commonlyassigned ICD-9-CM diagnosis. As a group, dental cariesand pulp and periapical infections were the secondmost commonly listed diagnoses, comprising 43% ofdischarge diagnoses assigned to a dental-complaintvisit. In contrast to the 2.95 million estimated visits fordental complaints, there were 4.09 million ED visits inwhich a dental-related ICD-9-CM diagnosis was assignedat discharge (Table 3). More than half (52%) of childrenyounger than 19 years and 31% of those 19 years andolder who were assigned a dental-related ICD-9-CMdiagnosis did not have a dental complaint documentedat presentation to the ED. The greater discrepancy be-tween dental diagnoses and complaints among youngerpatients seems to be due to their higher incidence ofinjury so that the injury, rather than the tooth problem,was the primary reason for the ED visit.
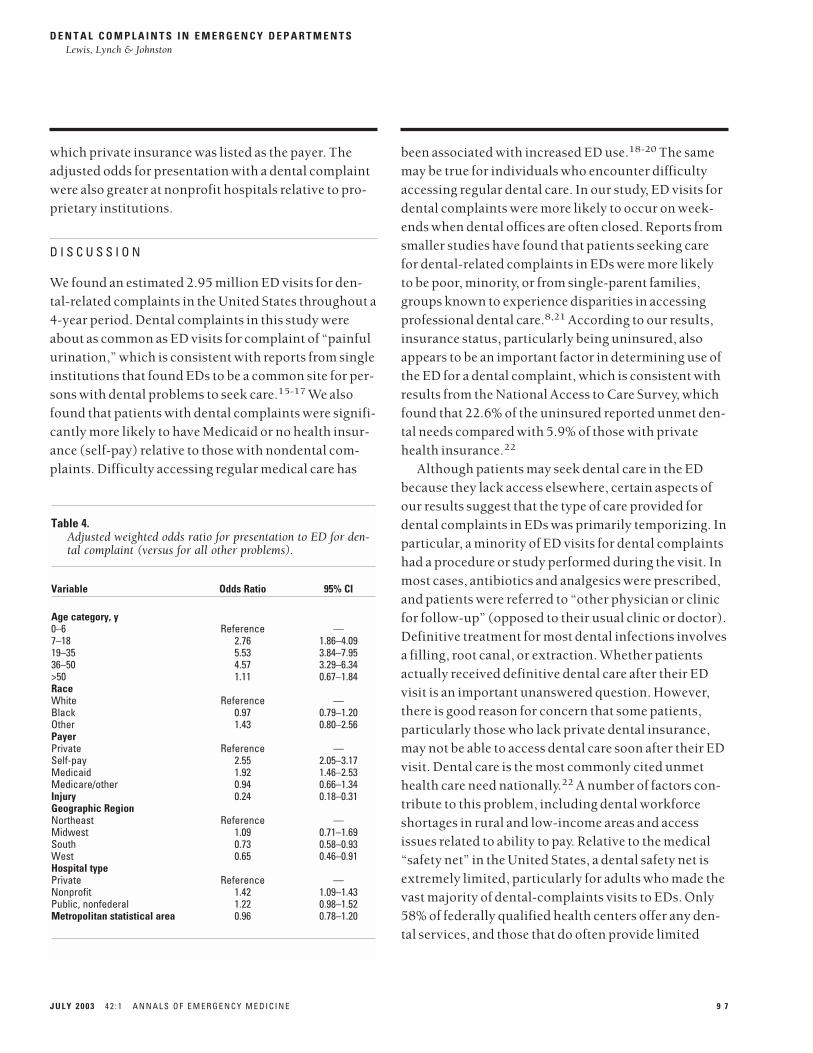
Multivariate logistic regression results (Table 4)indicated that the adjusted odds of presentation to theED for a dental complaint (versus another problem)were significantly elevated for visits in which Medicaidor self-pay was listed as the payer relative to those in
Table 2.Characteristics of patients as weighted proportion for dental-complaint ED visits and all other ED visits.
Dental-Complaint Other EDCharacteristic ED Visit, % Visits, %
Female 51.4 52.8Age category, y*
0–6 5.2 14.07–18 10.1 13.419–35 49.4 27.136–50 29.7 19.9>51 7.7 25.6RaceWhite 71.7 76.4Black 25.0 21.0Other 3.3† 2.6Primary payer*
Private 27.5 38.6Self-pay 34.8 16.2Medicaid 23.7 17.5Medicare 4.8 15.0Other/unknown 9.1 12.7Injury* 13.1 37.0Presentation day/timeWeekend* 36.2 30.6After hours weekday 39.3 36.9Referral to doctor/clinic other 72.3 45.7
than regular doctor*
No. of medications prescribed*
0 18.8 27.71 25.1 29.52 40.7 21.53 9.1 10.9≥4 6.3 10.2Received antibiotics* 49.5 20.5Received analgesic* 72.4 38.2Received narcotic* 37.8 13.2US regionNortheast 21.4 19.2Midwest 29.7 25.8South 35.4 37.4West 13.5 17.5Hospital ownership*
Private 13.1 12.8Voluntary, nonprofit 65.9 71.4Public, nonfederal 21.1 15.8Metropolitan statistical area 78.2 76.3*χ2 Analysis P<.05 between other ED visits and dental-complaint visits.†Estimate based on <30 observations.
Table 3.Weighted proportions by diagnostic category among ED visitsfor dental-complaint and ED visits with any dental ICD-9-CM diagnosis.
Discharge With aDental Dental ICD-9-CM
Category of Discharge Complaint, % Diagnosis, %Diagnosis (ICD-9-CM Code) (N=2.95 million) (N=4.09 million)
Dental problem, not otherwise 46.1 41.4specified (521.8, 521.9, 525.8, 525.9)
Pulpitis or periapical abscess (522) 23.3 28.6Caries (521.0) 19.2 17.6Broken tooth (873.63, 873.73) 7.9 11.7Gingivitis/periodontitis (523) 6.3 9.6Teething and eruption (520) 1.9* 4.9*Estimate based on <30 observations.
D E N T A L C O M P L A I N T S I N E M E R G E N C Y D E P A R T M E N T SLewis, Lynch & Johnston
been associated with increased ED use.18-20 The samemay be true for individuals who encounter difficultyaccessing regular dental care. In our study, ED visits fordental complaints were more likely to occur on week-ends when dental offices are often closed. Reports fromsmaller studies have found that patients seeking carefor dental-related complaints in EDs were more likelyto be poor, minority, or from single-parent families,groups known to experience disparities in accessingprofessional dental care.8,21 According to our results,insurance status, particularly being uninsured, alsoappears to be an important factor in determining use ofthe ED for a dental complaint, which is consistent withresults from the National Access to Care Survey, whichfound that 22.6% of the uninsured reported unmet den-tal needs compared with 5.9% of those with privatehealth insurance.22
Although patients may seek dental care in the EDbecause they lack access elsewhere, certain aspects ofour results suggest that the type of care provided fordental complaints in EDs was primarily temporizing. Inparticular, a minority of ED visits for dental complaintshad a procedure or study performed during the visit. Inmost cases, antibiotics and analgesics were prescribed,and patients were referred to “other physician or clinicfor follow-up” (opposed to their usual clinic or doctor).Definitive treatment for most dental infections involvesa filling, root canal, or extraction. Whether patientsactually received definitive dental care after their EDvisit is an important unanswered question. However,there is good reason for concern that some patients,particularly those who lack private dental insurance,may not be able to access dental care soon after their EDvisit. Dental care is the most commonly cited unmethealth care need nationally.22 A number of factors con-tribute to this problem, including dental workforceshortages in rural and low-income areas and accessissues related to ability to pay. Relative to the medical“safety net” in the United States, a dental safety net isextremely limited, particularly for adults who made thevast majority of dental-complaints visits to EDs. Only58% of federally qualified health centers offer any den-tal services, and those that do often provide limited
which private insurance was listed as the payer. Theadjusted odds for presentation with a dental complaintwere also greater at nonprofit hospitals relative to pro-prietary institutions.
D I S C U S S I O N
We found an estimated 2.95 million ED visits for den-tal-related complaints in the United States throughout a4-year period. Dental complaints in this study wereabout as common as ED visits for complaint of “painfulurination,” which is consistent with reports from singleinstitutions that found EDs to be a common site for per-sons with dental problems to seek care.15-17 We alsofound that patients with dental complaints were signifi-cantly more likely to have Medicaid or no health insur-ance (self-pay) relative to those with nondental com-plaints. Difficulty accessing regular medical care has
J U L Y 2 0 0 3 4 2 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 7
Table 4.Adjusted weighted odds ratio for presentation to ED for den-tal complaint (versus for all other problems).
Variable Odds Ratio 95% CI
Age category, y0–6 Reference —7–18 2.76 1.86–4.0919–35 5.53 3.84–7.9536–50 4.57 3.29–6.34>50 1.11 0.67–1.84RaceWhite Reference —Black 0.97 0.79–1.20Other 1.43 0.80–2.56PayerPrivate Reference —Self-pay 2.55 2.05–3.17Medicaid 1.92 1.46–2.53Medicare/other 0.94 0.66–1.34Injury 0.24 0.18–0.31Geographic RegionNortheast Reference —Midwest 1.09 0.71–1.69South 0.73 0.58–0.93West 0.65 0.46–0.91Hospital typePrivate Reference —Nonprofit 1.42 1.09–1.43Public, nonfederal 1.22 0.98–1.52Metropolitan statistical area 0.96 0.78–1.20

D E N T A L C O M P L A I N T S I N E M E R G E N C Y D E P A R T M E N T SLewis, Lynch & Johnston
adult dental care.23 Dental care is not a mandated bene-fit for adult Medicaid beneficiaries, and already limitedadult dental services for low-income individuals haverecently been reduced or eliminated in a number ofstates with budget crises.24
Although there has been recent focus on improvingchildren’s oral health, children from low-income fami-lies continue to have difficulty accessing dental care.Although pediatric dental care coverage is mandatedunder Medicaid, only 10% of dentists nationallyparticipate in Medicaid.25 In 1998, only 19% of chil-dren with Medicaid had a dental visit.26 Dental school–and hospital-based dental training programs are oftenperceived as safety net providers; however, a 2001 sur-vey indicated that even children with dental pain waiton average 1 month and in some cases up to 3 months toreceive care at these sites.27 This information raisesimportant questions about whether patients who aretold to see a dentist after an ED visit for a dental com-plaint are actually able to access definitive dental caresoon.
Our results also indicate that the majority of dental-complaint ED visits occurred in public and nonprofithospitals and in metropolitan areas. Although we didnot have teaching hospital status available in our data-base, many of these public or nonprofit metropolitanfacilities are training sites for residents, which hasimportant implications for the educational missions ofthese hospitals and their training of medical residents.ED providers and physicians-in-training need to beknowledgeable about dental problems and have train-ing in the diagnosis and management of these condi-tions, which will require further enhancement of medi-cal curricula with oral health topics.
Our study has several strengths compared with pre-vious studies of ED use for dental complaints. Specifi-cally, use of the National Hospital Ambulatory MedicalCare Survey provides a national perspective on dental-related visits to EDs throughout a 4-year period. Inaddition, we used multivariate regression to bettercharacterize the association between ED use for a den-tal complaint and payer status and ED characteristics.However, our study also has limitations. Specifically, we
9 8 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 2 : 1 J U L Y 2 0 0 3
were lacking information about reasons for seeking carein an ED (opposed to another site) and about any fol-low-up care obtained after the ED visit. We did not havedental insurance status; however, we considered thatpatients classified as Medicaid or self-pay would beunlikely to have private dental insurance. Individualswith private medical insurance may or may not havedental insurance. Patient-specific identifiers were notprovided, prohibiting our ability to determine whetheran individual had more than 1 visit for a dental-relatedcomplaint during the data collection period. Finally,although data are compiled uniformly by the NationalHospital Ambulatory Medical Care Survey, they are col-lected by ED staff who may not have collected or codedall information correctly or completely. Despite theselimitations, we believe this study offers an importantnational perspective on the use of the ED for dentalcomplaints and raises questions about the type andquality of care provided during and after a dental-related ED visit.
In conclusion, EDs are an important point of care fordental-related complaints, particularly for individualswho are publicly insured or uninsured. EDs and theirproviders should be prepared and equipped to triage,diagnose, provide basic treatment, and, ideally, ensureappropriate follow-up care for dental problems.Although improving access to preventive and restora-tive dental services would lessen reliance on the ED andmay decrease the costs associated with this pattern ofuse, this improvement is unlikely to occur soon, giventhe increasing strain on the public health safety net.EDs may even face increasing numbers of patients withdental complaints if the number of uninsured patientsincreases and the barriers to accessing dental care arenot addressed. The need for dental training for emer-gency medicine providers, as well as for improving den-tal care during and after ED visits, should be assessed.
Author contributions: CL conceived of the idea for this project andobtained and formatted the data. CL, HL, and BJ worked together tofurther develop the project concept and analyze the data. BJ pro-vided statistical consultation and expertise. CL and HL drafted themanuscript. BJ made a substantial contribution to its review andrevision. CL takes responsibility for the paper as a whole.
D E N T A L C O M P L A I N T S I N E M E R G E N C Y D E P A R T M E N T SLewis, Lynch & Johnston
20. Baker DW, Stevens CD, Brook RH. Determinants of emergency department use:are race and ethnicity important? Ann Emerg Med. 1996;28:677-682.
21. Cohen LA, Manski RJ, Hooper FJ. Does the elimination of medicaid reimbursementaffect the frequency of emergency department dental visits? J Am Dent Assoc.1996;127:605-609.
22. Mueller CD, Schur CL, Paramore LC. Access to dental care in the United States.J Am Dent Assoc. 1998;129:429-437.
23. Edelstein BL. Public and clinical policy considerations in maximizing children’s oralhealth. Pediatr Clin North Am. 2000;47:1177-1189.
24. Ku L, Ross DC, Nathanson M. State Medicaid cutbacks and the federal role in pro-viding fiscal relief to states. Center on Budget and Policy Priorities Web site. August 2,2002. Available at: http://www.cbpp.org/7-12-02health.htm. Accessed May 7, 2003.
25. US Inspector General. Children’s Dental Services Under Medicaid: Access andUtilization. Washington, DC: US Department of Health and Human Services; 1996.
26. Health Care Financing Administration. Annual EPSDT participation report: 1998.Available at: http://cms.hhs.gov/medicaid/epsdt/ep1998n.pdf. Accessed January 23,2003.
27. Lewis CW, Nowak AJ. Stretching the safety net too far: waiting times for dentaltreatment. Pediatr Dent. 2002;24:6-10.
Received for publication October 18, 2002. Revision receivedJanuary 31, 2003. Accepted for publication March 7, 2003.
Supported by grants (K23 DE14062-01 [Dr. Lewis] and T32 DE07132[Dr. Lynch]) from the National Institute of Dental and CraniofacialResearch.
Reprints not available from the authors.
Address for correspondence: Charlotte Lewis, MD, MPH, ChildHealth Institute, University of Washington, 6200 NE 74th Street,Building 29, Seattle, WA, 98115; 206-616-1205, fax 206-616-4623;E-mail [email protected].
R E F E R E N C E S1. Dental service use and dental insurance coverage: United States, Behavioral RiskFactor Surveillance System, 1995. MMWR Morb Mortal Wkly Rep. 1997;46:1199-1203.
2. Hill CM, Burford K, Martin A, et al. A one-year review of maxillofacial sportsinjuries treated at an accident and emergency department. Br J Oral Maxillofac Surg.1998;36:44-47.
3. Wilson S, Smith GA, Preisch J, et al. Nontraumatic dental emergencies in a pedi-atric emergency department. Clin Pediatr. 1997;36:333-337.
4. Wilson S, Smith GA, Preisch J, et al. Epidemiology of dental trauma treated in anurban pediatric emergency department. Pediatr Emerg Care. 1997;13:12-15.
5. Sae-Lim V, Tan HH, Yuen KW. Traumatic dental injuries at the accident and emer-gency department of Singapore General Hospital. Endod Dent Traumatol. 1995;11:32-36.
6. Fleming P, Gregg TA, Saunders IDF. Analysis of an emergency department serviceprovided at a children’s hospital. Int J Pediatr Dentistry. 1991;1:25-30.
7. Crouch R, Patel A, Williams S, et al. An analysis of telephone calls to an inner-cityaccident and emergency department. J R Soc Med. 1996;89:324-328.
8. Von Kaenel D, Vitangeli D, Casamassimo PS, et al. Social factors associated withpediatric emergency department visits for caries-related dental pain. Pediatr Dent.2001;23:56-60.
9. Whyman RA, Treasure ET, Ayers KMS. Dental disease levels and reasons foremergency clinic attendance in patients seeking relief of pain in Auckland. N Z Dent J.1996;92:114-117.
10. Dorfman DH, Kastner B, Vinci RJ. Dental concerns unrelated to trauma in the pedi-atric emergency department. Arch Pediatr Adolesc Med. 2001;155:699-703.
11. Sheller B, Williams BJ, Lombardi SM. Diagnosis and treatment of dental caries-related emergencies in a children’s hospital. Pediatr Dent. 1997;19:470-475.
12. Centers for Disease Control and Prevention. 1997-2000 NHAMCS micro-data filedocumentation: National Center for Health Statistics. Available at:http://www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm. Accessed January 23, 2003.
13. International Classification of Diseases, Ninth Revision, Clinical Modification.Chicago, IL: American Medical Association; 2001.
14. US Census Bureau Web site. Available at: http://www.census.gov/population/estimates/state/stats/. Accessed May 21, 2003.
15. Bringhurst C, Herr RD, Aldous JA. Oral trauma in the emergency department. Am JEmerg Med. 1993;11:486-490.
16. Gibson DE, Verono AA. Dentistry in the emergency department. J Emerg Med.1987;5:35-44.
17. Klokkevold P. Common dental emergencies. Emerg Med Clin North Am. 1989;7:29-63.
18. Christakis DA, Mell L, Koepsell TD, et al. Association of lower continuity of carewith greater risk of emergency department use and hospitalization in children.Pediatrics. 2001;107:524-529.
19. Lambrew JM, DeFriese GH, Carey TS, et al. The effects of having a regular doctoron access to primary care. Med Care. 1996;34:138-151.
J U L Y 2 0 0 3 4 2 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 9