Embed Size (px)
Citation preview

Denosumab Compared With Zoledronic Acid for the Treatment of Bone Metastasesin Patients With Castration-Resistant
Prostate Cancer
Karim Fizazi,1 Michael Carducci,2 Matthew Smith,3 Ronaldo Damião,4 Janet Brown,5 Lawrence Karsh,6
Piotr Milecki,7 Michael Rader,8 Neal Shore,9
Sylvia Tadros,10 Huei Wang,10 Qi Jiang,10 Roger Dansey,10 Carsten Goessl10
1Institut Gustave Roussy, University of Paris, Villejuif, France2Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, MD, USA
3Massachusetts General Hospital Cancer Center, Boston, MA, USA4Hospital Universitario Pedro Ernesto, Rio de Janeiro, Brazil
5Cancer Research UK Clinical Centre, Leeds, UK6The Urology Center of Colorado, Denver, CO, USA7Wielkopolskie Centrum Onkologii, Poznan, Poland
8Union State Bank Cancer Center, Nyack Hospital, Nyack, NY, USA9Carolina Urological Research Center, Myrtle Beach, SC, USA
10Amgen Inc., Thousand Oaks, CA, USA

Disclosures
• This study was supported by Amgen Inc.• K Fizazi has been a consultant for and received honoraria from Amgen
and Novartis. • M Carducci has been a consultant for and received research funding
from Amgen. • M Smith has been a consultant for Amgen and Novartis and received
honoraria and research funding from Amgen.• R Damião and Piotr Milecki have received research funding from
Amgen.• J Brown has been a consultant for Amgen and received honoraria from
Amgen and Novartis.• L Karsh has been a consultant for Amgen and received honoraria and
received research funding from Amgen.• M Rader has been a consultant for and received honoraria and
research funding from Amgen.• N Shore has been a consultant for and received honoraria from
Amgen.• H Wang, S Tadros, R Dansey, Q Jiang, and C Goessl are employed by
and have received stocks/stock options from Amgen.

Background
• Up to 75% of advanced prostate cancer patients develop bone metastasis1
• Bone metastases lead to osteoclast-mediated bone destruction
• Clinical consequences include skeletal-related events (SREs)2
• IV zoledronic acid (ZA) is the only bisphosphonate approved to delay or prevent SREs in castration-resistant prostate cancer3
1Coleman R. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res. 2006; 12(20 Suppl):6243s-6249s. 2Coleman RE. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev. 2001;27:165-76. 3Saad F, Gleason DM, Murray R. J Natl Cancer Inst. 2002;94:1458-1468.
Pathologic Fracture
Radiation to Bone
Surgery to Bone
Spinal Cord Compression

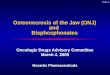
RANKL Is a Central Mediator of the “Vicious Cycle” of Bone Destruction in Metastatic Cancer
PTHrP, BMP,TGF-β, IGF, FGF,VEGF, ET1, WNT
Osteoblasts
Activated Osteoclast
PDGF, BMPsTGF-β, IGFs
FGFs
Adapted from Roodman D. N Engl J Med. 2004;350:1655.
RANKL
RANKTumor
Cell

Denosumab May Interrupt the “Vicious Cycle” of Cancer-Induced Bone Destruction
PDGF, BMPsTGF-β, IGFs
FGFs
Osteoblasts
RANKL
RANK
DenosumabTumor Cell
FormationInhibited
Apoptotic Osteoclast
PTHrP, BMP,TGF-β, IGF, FGF,VEGF, ET1, WNT
Adapted from Roodman D. N Engl J Med. 2004;350:1655.

RANKL and OPG Expression in Osteoblasts When Co-cultured With Prostate Cancer Cells
OPG
RANKL
CTR CTROSB+ 2b
OSB+ 2a
OSB + LNCaP
OSB+ PC3
Fizazi et al. Clin Cancer Res 2003;9:2587–2597

Denosumab: Properties and Clinical Program
To date, approximately 11,000 patients have been exposed to denosumab in clinical trials of patients with cancer or bone loss
1Fizazi K et al. J Clin Oncol. 2009;27:1564-1571 2Ellis et al. J Clin Oncol. 2008;26:4875-48823Stopeck A et al. Eur J Cancer Suppl. 2009;7:2(Abs 2LBA) 4Henry D, et al. Eur J Cancer Suppl. 2009;7:11(Abs 20LBA)
Properties of Denosumab• Fully human monoclonal
antibody with high affinity and specificity for human RANKL
• Advanced cancer dose:subcutaneous 120 mg monthly
• In clinical trials
– No requirement for renal monitoring or dose adjustment1
– No acute phase reactions attributed to denosumab1,2
Pivotal Studies in Patients With Bone Metastases
• Denosumab superior to ZA for preventing/delaying SREs in breast cancer (N=2046; HR=0.82; P<0.0001, non-inferiority endpoint; adjusted P=0.01, superiority endpoint)3
• Denosumab non-inferior (trend to superior) to ZA for preventing/delaying SREs in solid tumors and multiple myeloma (N=1776; HR= 0.84; P=0.0007, non-inferiority endpoint; adjusted P=0.06, superiority endpoint)4

Study Design: International, Randomized, Double-Blind, Active-Controlled Study
Zoledronic acid 4 mg IV* and Placebo SC every 4 weeks (N = 951)
Denosumab 120 mg SC and Placebo IV* every 4 weeks (N = 950)
Key Inclusion• Hormone-refractory (castration resistant) prostate cancer and bone metastases
Key Exclusion• Current or prior IV bisphosphonate treatment
*Per protocol and Zometa® label, IV product dose adjusted for baseline creatinine clearance and subsequent dose intervals determined by serum creatinine.
No SC dose adjustments made due to increased serum creatinine.
• Calcium and Vitamin D supplemented in both treatment groups• Accrual period from May 2006 to December 2008• Analysis cut-off date October 2009

Sequential Testing of Primary and Secondary Endpoints
Primary Efficacy Endpoint (Non-inferiority)
Time to first on-study SRE
Only if P<0.05
Hochberg adjustment for multiplicity between the two secondary endpointsHochberg adjustment for multiplicity between the two secondary endpoints
Secondary Efficacy Endpoints (Superiority)
Time to first on-study SRE Time to first-and-subsequent on-study SRE (multiple events)
Hochberg Y. A sharper Bonferroni procedure for multiple tests of significance. Biometrika. 1998;75:800-802.

Baseline Characteristics
Characteristic, n (%) or medianZoledronic Acid
(N = 951)Denosumab
(N = 950)
Age (years) 71.0 71.0
ECOG performance status of 0 or 1 886 (93) 882 (93)
Stratification factors:
Proportion of subjects with PSA ≥ 10 ng/mL
806 (85) 805 (85)
Chemotherapy (≤ 6 weeks before randomization)
132 (14) 132 (14)
Previous SRE 231 (24) 232 (24)
Time from first bone metastasis to randomization (months): median (Q1, Q3)
5.2 (1.3, 16.1) 3.9 (1.2, 15.7)

Drug Exposure and Adjustments for Renal Function
Overall Exposure IV Zoledronic Acid (N = 946)
SC Denosumab(N = 942)
Median number of doses (Q1, Q3) 10.5 (5.0, 17.0) 13.0 (6.0, 19.0)
Cumulative exposure (patient-years) 913.6 991.3
Adjustments for Renal FunctionSubjects with dose adjustments for creatinine clearance at baseline, n (%)
213 (22.5) NA
Subjects with doses withheld for serum creatinine increases on study, n (%)
143 (15.1) NA
Total number of doses withheld due to serum creatinine increases on study
592 NA
NA = Not applicable per protocol

Patient Disposition
Denosumab Subjects: 950Zoledronic Acid Subjects: 951
Randomized Subjects: 1901*
Reasons for Discontinuation Death 269
(28.3%) Consent Withdrawn 164
(17.2%) Disease Progression 113 (11.9%)
Adverse Event 43 (4.5%)
Other 154 (16.2%)
Reasons for Discontinuation Death 294
(30.9%) Consent Withdrawn 147
(15.5%) Disease Progression 117 (12.3%)
Adverse Event 56 (5.9%)
Other 108 (11.4%)
*Does not include three subjects with insufficient IRB oversight
Discontinued: 743 (78.1%) Discontinued: 722 (76.0%)

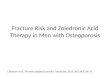
Time to First On-Study SRE
Zoledronic Acid 951 733 544 407 299 207 140 93 64 47
Denosumab 950 758 582 472 361 259 168 115 70 39
Subjects at risk:
0
1.00
Pro
po
rtio
n o
f S
ub
ject
s W
ith
ou
t S
RE
0 3 6 9 12 15 18 21 24 27
0.25
0.50
0.75
KM Estimate ofMedian Months
DenosumabZoledronic acid
20.717.1
HR 0.82 (95% CI: 0.71, 0.95)P = 0.0002 (Non-inferiority)P = 0.008 (Superiority)
Study Month
18%18%Risk
Reduction

Time to First and Subsequent On-Study SRE* (Multiple Event Analysis)
*Events occurring at least 21 days apart
Rate Ratio = 0.82 (95% CI: 0.71, 0.94)
Study Month
0.0
2.0
0 3 6 9 12 15 18 21 24 27
Cu
mu
lati
ve
Mea
n N
um
ber
of
SR
Es
per
Pat
ien
t
30 33 36
0.2
0.6
1.0
1.4
1.8
0.4
0.8
1.2
1.6
18%18%Risk
Reduction
Denosumab Zoledronic acid 584584
494494
Events
P = 0.008

Per
cen
t o
f S
ub
ject
s W
ith
Fir
st S
RE
Radiationto Bone
FractureSurgeryto Bone
Spinal CordCompression
20.0
14.7
3.3
0.3
First On-study SRE by Type
All subjects
0
5
10
15
20
25
30

Prostate-Specific Antigen (PSA)M
edia
n (
Q1,
Q3)
PS
A (
ng
/mL
)
Study Month
0
100
200
300
400
500
600
0 3 6 9 12 15 18 21 24 27 30 33
Zoledronic acid (N = 951)
Denosumab (N = 950)

Overall Disease Progression
Zoledronic Acid 951 708 507 356 246 168 108 74 50 33
Denosumab 950 715 518 370 273 180 111 71 51 32
0
Pro
po
rtio
n o
f S
ub
ject
sW
ith
ou
t D
isea
se P
rog
ress
ion
0 3 6 9 12 15 18 21 24 27
Study MonthSubjects at risk:
1.00
0.25
0.50
0.75
DenosumabZoledronic acid
HR = 1.06 (95% CI: 0.95, 1.18)P = 0.30

Overall Survival
Zoledronic Acid 951 864 745 635 519 401 297 207 143 98 55
Denosumab 950 872 746 645 552 427 310 233 156 99 54
0
Pro
po
rtio
n o
f S
ub
ject
s S
urv
ived
0 3 6 9 12 15 18 21 24 27 30
Subjects at risk:
1.00
0.25
0.50
0.75
HR = 1.03 (95% CI: 0.91, 1.17)
DenosumabZoledronic acid
Study Month
P = 0.65

Summary of Adverse Events
Subject incidence, n (%)
Zoledronic Acid(N = 945)
n (%)
Denosumab(N = 943)
n (%)
Adverse events (AEs) 918 (97) 916 (97)
Most common AEs in either arm
Anemia 341 (36) 337 (36)
Back Pain 287 (30) 304 (32)
Decreased appetite 274 (29) 267 (28)
Nausea 245 (26) 272 (29)
Fatigue 222 (24) 257 (27)
CTC Grade 3, 4, or 5 AEs 672 (71) 718 (76)
Serious AEs 568 (60) 594 (63)
AEs leading to treatment discontinuation 138 (15) 164 (17)

Forest Plot of Adverse Events With Unadjusted P < 0.05
Risk greater with Zoledronic Acid Risk greater with Denosumab
Risk Difference (% in Denosumab - % in Zoledronic Acid)
Zoledronic Acid Denosumab(N = 945) (N = 943)n (%) n (%)
133 (14.1) 100 (10.6)33 (3.5) 11 (1.2)57 (6.0) 37 (3.9)28 (3.0) 11 (1.2)10 (1.1) 0 (0.0)11 (1.2) 1 (0.1)15 (1.6) 5 (0.5) 1 (0.1) 7 (0.7) 1 (0.1) 7 (0.7) 2 (0.2) 9 (1.0) 1 (0.1) 9 (1.0) 1 (0.1) 10 (1.1) 2 (0.2) 11 (1.2) 5 (0.5) 15 (1.6) 5 (0.5) 16 (1.7)10 (1.1) 21 (2.2)12 (1.3) 26 (2.8)13 (1.4) 28 (3.0)24 (2.5) 40 (4.2)19 (2.0) 36 (3.8)30 (3.2) 47 (5.0)11 (1.2) 31 (3.3)27 (2.9) 51 (5.4)51 (5.4) 116 (12.3)Hypocalcemia
Muscle spasmsHyperhidrosis
Thoracic vertebral fractureProstatic specific antigen increased
InfluenzaHypophosphatemia
ToothacheOsteonecrosis
SinusitisCerebrovascular accident
Tooth abscessOral herpes
Blood alkaline phosphataseHypercalcemia
Ilium fractureDrug hypersensitivity
Blood glucose increasedCognitive disorder
CholelithiasisChills
MyalgiaInfluenza like illness
Pyrexia
-15 -10 -5 0 5 10 15

Adverse Events of Interest
Subject incidence, n (%)Zoledronic Acid
(N = 945)Denosumab
(N = 943)
Infectious AEs 375 (39.7) 402 (42.6)
Infectious serious AEs 108 (11.4) 130 (13.8)
Acute phase reactions (first 3 days) 168 (17.8) 79 (8.4)
Renal AEs* 153 (16.2) 139 (14.7)
Cumulative rate of osteonecrosis of the jaw (ONJ)† 12 (1.3) 22 (2.3)
Year 1 5 (0.5) 10 (1.1)
Year 2 8 (0.8) 22 (2.3)
Hypocalcemia 55 (5.8) 121 (12.8)
New primary malignancy 10 (1.1) 18 (1.9)
*Includes renal failure, increased blood creatinine, acute renal failure, renal impairment, increased blood urea, chronic renal failure, oliguria, hypercreatininemia, anuria, azotemia, decreased creatinine renal clearance, decreased urine output, abnormal blood creatinine, proteinuria, decreased glomerular filtration rate, and nephritis.†P = 0.09

Subjects with positively adjudicated ONJ, n (%)
Zoledronic AcidN = 12 (1.3%)
DenosumabN = 22 (2.3%)
Risk factors
Tooth extraction, dental appliance, or poor oral hygiene 10 (83) 17 (77)
Chemotherapy 9 (75) 14 (64)
Treatment*
Limited surgery (eg, debridement) 3 (25) 10 (45)
Bone resection 1 (8) 2 (9)
Outcome*
Resolution (mucosal coverage) 1 (8) 4 (18)
ONJ
*As of April 2010

Summary
• Denosumab was superior to zoledronic acid in preventing/delaying:
– First SREs
– Multiple SREs
• Notable adverse events occurring in both treatment groups included hypocalcemia and ONJ
• Denosumab continues to be studied as a potential treatment option for bone metastases– Administered as a monthly SC injection
– No need for renal monitoring or dose adjustment
– No need to manage acute phase reactions

Acknowledgements
• We thank all patients, their families, investigators, and study site staff who participated in the 20050103 study for their contributions.