Embed Size (px)
Citation preview

Den Krebs verstehen. Highlights der CIO-Forschung
Understanding Cancer.Key approaches of CIO research

CIO Köln Bonn as „Center for Integrated Oncology“ is a joint cancer center of the University Hospitals
Cologne and Bonn. Both hospitals belong to the largest institutions of their kind in Germany with a
catchment area of more than seven million people. Since 2007 all clinics and institutes of both sites are
acting jointly as CIO in the fields of tumor research, diagnosis and coherent treatment. Since 2008 the
CIO Köln Bonn was repeatedly awarded as Comprehensive Cancer Center by the Germany Cancer Aid
(Deutsche Krebshilfe).
Das „Centrum für Integrierte Onkologie Köln Bonn“ ist das gemeinsame Krebszentrum der Unikliniken
Köln und Bonn – zwei der größten universitären Kliniken in Deutschland mit einem Einzugsgebiet von
über sieben Millionen Menschen. Unter dem Dach des CIO arbeiten seit 2007 alle Kliniken und Institute
beider Häuser zusammen, die sich mit der Erforschung, Diagnose und Behandlung von Tumorerkrankun-
gen befassen. Das CIO Köln Bonn wurde seit 2008 wiederholt als „Onkologisches Spitzenzentrum“ von
der Deutschen Krebshilfe ausgezeichnet.
Welcome to CIO Köln BonnWillkommen im CIO Köln Bonn
Prof. Dr. Michael Hallek Vorstandsvorsitzender CIO KölnChairman of the Board of Directors CIO Köln
Prof. Dr. Walther KuhnVorstandsvorsitzender CIO BonnChairman of the Board of Directors CIO Bonn
Prof. Dr. Jürgen Wolf Ärztlicher Leiter CIO KölnMedical Director CIO Köln
Prof. Dr. Ingo Schmidt-Wolf Ärztlicher Leiter CIO BonnMedical Director CIO Bonn
3

Vor gut zehn Jahren haben wir in Köln
beschlossen, durch mehr gelebte In-
terdisziplinarität die Versorgung der
Krebspatienten in der Region deutlich
zu verbessern. Dieser Gedanke führte
konsequenterweise schnell zu einer
Kooperation mit der Uniklinik Bonn
und heute arbeiten beide Standorte
insbesondere beim Thema Forschung
und Leitlinienentwicklung (SOPs) eng
zusammen.
Ich möchte mich deshalb an dieser
Stelle bei allen bedanken, die diesen
Erfolg möglich gemacht haben, expli-
zit auch bei der Deutschen Krebshil-
fe, die durch die finanzielle Förderung
des CIO Köln Bonn als onkologisches
Spitzenzentrum den Aufbau der not-
wendigen Strukturen und Abläufe
grundlegend unterstützt hat.
Exzellenz initiieren
It is now ten years that we decided
to improve the medical care of cancer
patients in our region significantly. To
achieve this goal we focused on the
availability of interdisciplinary cancer
services of the highest quality. Hence
this idea quickly led us to a coopera-
tion with the University Hospital of
Bonn and today Cologne and Bonn
are closely interlinked particularly in
the fields of research and the devel-
opment of Standard Operating Pro-
cedures (SOPs).
Therefore I’d like to take this opportu-
nity and express my sincere gratitude
to all who made this idea become
a great success story. Especially the
financial support of the “Deutsche
Krebshilfe” for the CIO Köln Bonn as
Comprehensive Cancer Center has
promoted the implementation of
necessary structures and procedures
fundamentally.
With this booklet we’d like to provide
a short insight into our main current
research activities. We address them
in terms of:
Advanced fields of research
research activities that can be
claimed as outstanding – also on
international level
Emerging fields of research
research activities that may take
some more time but are very prom-
ising for the future
Mit dieser Broschüre möchten wir Ih-
nen einen kurzen Einblick in unsere
wichtigsten aktuellen Forschungsakti-
vitäten geben. Wir haben diese unter
zwei Aspekten zusammengefasst:
Forschungsschwerpunkte
Darunter verstehen wir Forschungs-
aktivitäten, die – auch im internatio-
nalen Maßstab – als wissenschaftlich
herausragend bezeichnet werden
können.
Neue Forschungsfelder
Hierunter stellen wir Ihnen einige
Aktivitäten vor, die vielleicht noch
etwas Zeit brauchen, von denen wir
uns in Zukunft aber wichtige neue
Impulse erwarten.
Initiating excellence
Viele unserer Forschungsprojekte sind
eng mit dem Ansatz der „personali-
sierten Medizin“ verknüpft. Aufgrund
der spektakulären Ergebnisse zum Bei-
spiel in der Therapie des Bronchialkar-
zinoms, haben wir uns das Ziel gesetzt,
bis 2015 alle Krebspatienten im CIO
routinemäßig auf therapeutisch rele-
vante genomische Veränderungen zu
untersuchen.
Viel Spaß bei der Lektüre.
Prof. Dr. Michael HallekDirektor / Director CIO Köln Bonn
Many of our research projects are
closely connected to the approach of
“personalized medicine”. Due to the
exciting results e.g. in the therapy of
lung cancer we set ourselves the target
to establish standard testing of all our
cancer patients on therapeutically rel-
evant genomic modifications by 2015.
Enjoy reading.
4 5
Prof. Dr.Michael Hallek

Inhalt Contents
Forschungsschwerpunkte im CIO Köln Bonn Advanced fields of research
Entwicklung zielgerichteter Therapien für die CLL
Development of targeted CLL therapies
Prof. Dr. Michael HallekDirektor der Klinik I für Innere Medizin, CIO KölnDirector of the Dept. I of Internal Medicine
Prof. Dr. Christian Reinhardt Leiter der KFO-286, CIO KölnScientific coordinator of the CRU-286
12
Neue zielgerichtete Ansätze für die Therapie des Hodgkin Lymphoms
Novel targeted strategies for the treatment of Hodgkin Lymphoma
Prof. Dr. Andreas Engert Leiter der GHSG, CIO KölnGHSG chairman
Dr. Bastian von TresckowStudienarzt der GHSG, CIO KölnGHSG trial physician
14
Personalisierte Therapie beim Lungenkrebs: Erfolg durch translationale Vernetzung
Personalized therapy of lung cancer: Success by translational crosslinking
Prof. Dr. Reinhard Büttner Direktor des Instituts für Pathologie, CIO KölnChair Department of Pathology
Prof. Dr. Roman Thomas Leiter der Abteilung Translationale Genomik an der Universität zu Köln, CIO KölnHead Department of Translational Genomics, University of Cologne
Prof. Dr. Jürgen Wolf Ärztlicher Leiter CIO Köln, Leiter Lungenkrebs-Studiengruppe Köln Medical Director CIO Köln, Chair Lung Cancer Group Cologne
16
6 7

Inhalt Contents
Zielgerichtete Immunintervention beim Melanom
Directing innate immunity against melanoma
Prof. Dr. Gunther Hartmann Direktor des Instituts für Klinische Chemie und Klinische Pharmakologie, CIO Bonn Director Institute of Clinical Chemistry and Clinical Pharmacology
Prof. Dr. Dr. Cornelia MauchLeiterin der Arbeitsgruppe Dermato-Onkologie der Klinik für Dermatologie, CIO Köln Group leader Dermatooncology, Department of Dermatology
Prof. Dr. Thomas Tüting Leiter der Arbeitsgruppe Dermato-Onkologie der Klinik für Dermatologie, CIO Bonn Group leader Dermatooncology, Department of Dermatology
18
Familiärer Brust- und Eierstockkrebs: Forschung für die personalisierte Prävention
Hereditary breast- and ovarian cancer: Research for a personalized prevention
Prof. Dr. Rita K. Schmutzler Direktorin des Zentrums Familiärer Brust- und Eierstockkrebs, CIO Köln Director of the Center of Familial Breast and Ovarian Cancer
20
Molekulare und multimodale Bildgebung
Molecular and multimodal Imaging
Prof. Dr. Alexander DrzezgaDirektor der Klinik und Poliklinik für Nuklearmedizin, CIO KölnDirector Department of Nuclear Medicine
Prof. Dr. Markus EsslerDirektor der Klinik und Poliklinik für Nuklearmedizin, CIO BonnDirector Department of Nuclear Medicine
22
24
Translationale Therapieforschung beim Pankreaskarzinom
Pancreatic cancer translational research
PD Dr. Georg FeldmannMedizinische Klinik 3, CIO BonnMedical Department 3
26
Translationale Prostatapathologie
Translational prostate Pathology
Prof. Dr. Glen Kristiansen Direktor des Instituts für Pathologie, CIO BonnChairman Institute for Pathology
28
Neue Therapieansätze beim Ovarialkarzinom
New therapeutic approaches in ovarian cancer
Prof. Dr. Walther Kuhn Geschäftsführender Direktor der Universitätsfrauenklinik, CIO BonnChairman of the Center of Obstetrics and Gynecology
30
Neue Forschungsfelder im CIO Köln BonnEmerging fields of research
8 9
Prof. Dr. Reinhard Büttner Direktor des Instituts für Pathologie, Chair Department of Pathology CIO Köln
Hoffnungsträger „Personalisierte Medizin“ – unser AnsatzChallenge „personalized medicine“ – our approach
Prof. Dr. Michael HallekDirektor der Klinik I für Innere Medizin, Director of the Dept. I of Internal MedicineCIO Köln
Prof. Dr. Jürgen Wolf Ärztlicher Leiter CIO Köln, Leiter Lungenkrebs-Studiengruppe Köln Medical Director CIO Köln, Chair Lung Cancer Group Cologne

Inhalt Contents
Prof. Dr. Peter MallmannDirektor der Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe, CIO KölnChairman of the Department of Gynaecology and Obstetrics
Co-Autoren / Co-Authors:Dr. Mignon-Denise Keyver-Paik, CIO BonnDr. Kirsten Kübler, CIO BonnDr. Michael Mallmann, CIO Bonn
30
Maligne Hirntumoren: Schritte in Richtung personalisierter Therapie
Malignant brain tumors: Steps to personalized therapy
Prof. Dr. Roland GoldbrunnerDirektor Zentrum für Neurochirurgie, CIO KölnDirector Center for Neurosurgery
Prof. Dr. Ulrich HerrlingerLeiter Klinische Neuroonkologie, CIO BonnHead Division of Clinical Neurooncology
Prof. Dr. Matthias SimonKlinik für Neurochirurgie, CIO BonnDepartment for Neurosurgery
Co-Autoren / Co-Authors:PD Dr. Norbert Galldiks, CIO KölnPD Dr. Martin Glas, CIO BonnPD Dr. Maximilian Ruge, CIO Köln Dr. Pantelis Stavrinou, CIO Köln
32
Anti-(lymph)angiogene Therapie bei malignen Tumoren des Auges
Anti-(lymph)angiogenic therapies for malignant tumors of the eye
Prof. Dr. Claus Cursiefen Geschäftsführender DirektorZentrum für Augenheilkunde, CIO KölnChairman Department of Ophthalmology
PD Dr. Ludwig M. HeindlOberarzt am Zentrum für Augenheilkunde, CIO KölnSenior Physician Department of Ophthalmology
34
Moderne quantitative und funktionelle Bildgebung
Modern quantitative and functional imaging
Prof. Dr. David Maintz Direktor Institut und Poliklinik für Radiologische Diagnostik, CIO KölnDirector radiologic diagnostics
Dr. Thorsten PersigehlInstitut und Poliklinik für Radiologische Diagnostik, CIO KölnRadiologic diagnostics
36
Radionuklidtherapie der Tumorerkrankungen
Cancer Radionuclide Therapy
PD Dr. Samer EzziddinKlinik und Poliklinik für Nuklearmedizin, CIO BonnDepartment of Nuclear Medicine
Prof. Dr. Matthias Schmidt Klinik und Poliklinik für Nuklearmedizin, CIO KölnDepartment of Nuclear Medicine
Co-Autor / Co-Author:Prof. Dr. Alexander Drzezga, CIO Köln
38
Palliativmedizin Luftnot und Schmerzen lindern
Palliative Care Relieving pain and dyspnoea
Prof. Lukas RadbruchLehrstuhl für Palliativmedizin, CIO Bonnchair of palliative medicine
Prof. Raymond VoltzLehrstuhl für Palliativmedizin, CIO Kölnchair of palliative medicine
40
Wissenschaftlicher BeiratScientific Advisory Board
42
CIO Köln Bonn in ZahlenCIO Köln Bonn – facts and figures
44
ImpressumImprint
46
10 11

Die chronisch lymphatische Leukämie
(CLL) ist die häufigste Leukämie des
Erwachsenenalters. Die CLL ist durch
heterogene klinische Verlaufsformen
gekennzeichnet. Obwohl sich die Be-
handlungsmöglichkeiten für die CLL
in den letzten Jahren ständig verbes-
sert haben, so bleibt die CLL letztlich
doch eine weitestgehend unheilbare
Erkrankung.
Unser translationaler Ansatz
Eine zentrale Eigenschaft der CLL ist
ihre enorme genomische Instabilität,
die das Resultat von Mutationen in
zwei gut charakterisierten Genen ist,
nämlich ATM und TP53. CLL Patien-
ten mit ATM oder TP53 Mutationen
sind resistent gegen Chemotherapie.
Überdies zeigt die CLL eine charakte-
ristische Abhängigkeit vom Tumormik-
romilieu. Mit unserem Team aus mehr
als 40 Wissenschaftlern identifizieren
wir molekulare Abhängigkeiten von
CLL Zellen, um diese in zielgerichte-
Entwicklung zielgerichteter Therapien für die CLL
Chronic lymphocytic leukemia (CLL) is
the most common leukemia of adults
in the Western world and is extraor-
dinarily heterogeneous in its clinical
course. Although treatment of CLL
could be significantly improved by the
introduction of modern immunochem-
otherapies, therapeutic challenges re-
main as the disease is still not acces-
sible for feasible curative approaches.
Our translational approach
One of the hallmark features of CLL is
its extraordinary genomic instability,
which is the result of well-character-
ized mutations in two genes: ATM and
TP53. Intriguingly, CLLs with mutant
ATM or TP53 display resistance against
frontline chemotherapeutic drugs. Fur-
thermore, disease progression as mini-
mal residual disease greatly depends
on the tumor microenvironment. With
our team of more than 40 scientists,
we analyze specific dependencies of
CLL cells and aim to transfer these
essential factors of pathogenesis into
novel therapeutic approaches. Our
innovative therapeutic concepts will
target both DNA-damage pathways
and the tumor microenvironment. Our
te Therapien zu übertragen. Unsere
neuen Therapieansätze werden so-
wohl dysregulierte Mechanismen der
genomischen Stabilität, als auch das
Tumormikromilieu zum Ziel haben. Un-
sere translationalen Aktivitäten sind
durch verschiedene klinische Studien
widergespiegelt, in die wir CLL Patien-
ten basiert auf den individuellen Muta-
tionen in ihren CLL Zellen einschließen.
Development of targeted CLL therapies
translational activities are mirrored by
numerous clinical trials, into which we
include patients based on the genetic
makeup of their CLL.
12 13
Prof. Dr. Christian Reinhardt
Prof. Dr. Michael Hallek
Publications
1. N Engl J Med, 2014 Jan 8: Obinutuzumab plus Chlorambucil in Patients with CLL and Coexisting Conditions
2. N Engl J Med, 2014 Jan 22: Idelalisib and Rituximab in Relapsed Chronic Lymphocytic Leukemia
3. Cell, 2014 Jan 30; 156(3): 590-602: Sensitizing protective tumor microenvironments to antibody-mediated therapy
The Kinase DNA-PK has been identified recently by the team of Prof. Reinhardt as target molecule for the perso-nalized therapy of ATM mutated CLL.
Die Kinase DNA-PK wurde kürzlich von dem Team um Prof. Reinhardt als Zielmolekül für die personalisierte Therapie von ATM-mutierter CLL identifiziert.

Neue zielgerichtete Ansätze für die Therapie des Hodgkin Lymphoms
Novel targeted strategies for the treatment of Hodgkin Lymphoma
Hodgkin Lymphoma (HL) is one of the
most frequent cancers in young adults.
Most patients with HL can be cured
with modern combined chemo- and
radiotherapy. However, patients suf-
fer from the acute and long-term side
effects of these systemic therapies.
Therefore, more targeted therapies
and a treatment intensity tailored ac-
cording to the risk profile of the indi-
vidual patient are needed.
Our therapeutic approach
To allow for a more individualized
treatment, current German Hodgkin
Study Group (GHSG) trials for early
stages evaluate positron emission
tomography (PET) as predictive tool
for the regulation of treatment in-
tensity. In randomized phase III trials,
PET is performed after chemotherapy
and in PET negative patients radio-
therapy is omitted to reduce unnec-
essary toxicity. In advanced stages of
the disease, a novel combination of
chemotherapy and the first targeted
substance in HL – brentuximab vedo-
tin – is currently evaluated in a phase II
clinical trial: “Targeted BEACOPP”. The
most toxic substances of the current
standard chemotherapy for advanced
HL are replaced by this highly active
substance to maintain the high cure
rates while reducing the toxicities.
Das Hodgkin Lymphom (HL) ist eine
der häufigsten Krebserkrankungen
junger Erwachsener. Die meisten HL-
Patienten können durch kombinierte
Chemo- und Strahlentherapie geheilt
werden. Patienten leiden allerdings an
den Akut- und Langzeitnebenwirkun-
gen dieser Therapien. Es werden daher
gezieltere Therapien und eine Thera-
pieintensität, die an das individuelle
Risikoprofil des Patienten angepasst
ist, benötigt.
Unser therapeutischer Ansatz
Um die Therapie besser zu individu-
alisieren, setzen die Studien der Ger-
man Hodgkin Study Group (GHSG)
die Positronen-Emissions-Tomogra-
phie (PET) als prädiktives Werkzeug
zur Steuerung der Therapieintensität
ein. In randomisierten Phase III-Studien
wird das PET nach der Chemotherapie
durchgeführt, um bei PET negativen
Patienten mittels Verzicht auf Bestrah-
lung unnötige Toxizität zu vermeiden.
In fortgeschrittenen Stadien wird eine
neue Kombination aus Chemothera-
pie und der ersten gezielten Substanz
für das HL – Brentuximab vedotin – in
einer Phase II-Studie evaluiert: „Tar-
geted BEACOPP“. Die schädlichsten
Substanzen aus der aktuellen Stan-
dardtherapie werden durch diese
Substanz ersetzt, um die Heilungsra-
ten beizubehalten, aber die Toxizität
zu reduzieren.
14 15
Prof. Dr. Andreas Engert
Dr. Bastian von Tresckow
Publications
1. Lancet, 2012 May 12;379(9828):1791-9: Reduced-intensity chemotherapy and PET-guided radiotherapy in patients with advanced stage Hodgkin’s lymphoma (HD15 trial): a randomised, open-label, phase 3 non-inferiority trial
2. J Clin Oncol, 2012 Mar 20;30(9):907-13: Dose-intensification in early unfavorable Hodgkin’s lym-phoma: final analysis of the German hodgkin study group HD14 trial
3. Lancet Oncol, 2013 Sep 14;10:943-52: Effect of initial treatment strategy on survival of patients with advanced-stage Hodgkin’s lymphoma: a systematic review and network meta-analysis
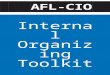
Brentuximab vedotin ADCMonomethyl auristatin E (MMAE), potent antimicrotubule agentProtease-cleavable linkerAnti-CD30 monoclonal antibody
Apoptosis
G2/M cell cycle arrest
ADC binds to CD30
MMAE disruptsmicrotubule network
ADC–CD30 complex traffics to lysosome
MMAE is released
Brentuximab-Vedotin (SGN-35)
Brentuximab vedotin selectively binds to CD30 and is internalized by the malignant cell. This leads to targeted release of the antimicrotubule agent.
Brentuximab vedotin bindet selektiv an CD30 und wird von der Krebszelle internalisiert. Dies führt zur gezielten Freisetzung des Mikrotubuli-Giftes.

Lungenkrebs ist die häufigste Krebsto-
desursache weltweit. Der unselektio-
nierte Einsatz von Chemotherapie und
neueren zielgerichteten Medikamen-
ten ist wenig effektiv. Erst die gezielte
Behandlung von molekular definierten
Subgruppen ermöglicht eine länger
anhaltende Tumorkontrolle.
Unser translationaler Ansatz
Durch eine enge Vernetzung von
Grundlagenforschung, molekularer
Diagnostik und klinischer Studien-
plattform entwickeln wir neue perso-
nalisierte Therapiestrategien. Aktuel-
le Erfolge beinhalten die Entdeckung
therapeutisch angehbarer genetischer
Veränderungen, so genannter Treiber-
mutationen, beim Plattenepithelkar-
zinom, die genomische Kartierung
des kleinzelligen Bronchialkarzinoms
sowie die Entwicklung neuer Verfah-
ren zur simultanen Diagnose mehrerer
Treibermutationen. Das Studienpro-
gramm der Lung Cancer Group Co-
logne ermöglicht es, jedem Patienten
mit einer Treibermutation einen per-
sonalisierten Therapieansatz anzubie-
Personalisierte Therapie beim Lungenkrebs: Erfolg durch translationale Vernetzung
Lung cancer is the most frequent cause
of cancer death worldwide. Chemo-
therapy as well as targeted drugs are
of limited efficacy in unselected pa-
tients. Only the targeted treatment of
molecularly defined subgroups ena-
bles efficient tumor control.
Our translational approach
A close interaction of basic science,
molecular diagnostics and clinical trial
platform allows us to develop new
personalized treatment approaches.
Current achievements include the
discovery of therapeutically amend-
able driver mutations in squamous
cell cancer, the genomic analysis of
small cell lung cancer and the devel-
opment of new methods for simulta-
neous diagnostics of numerous driver
mutations. The clinical trial program
of the Lung Cancer Group Cologne
enables us, to offer each patient with
a driver mutation at least one person-
alized treatment approach. With the
Network Genomic Medicine we have
established one of the world´s larg-
est lung cancer genotyping platforms
ten. Mit dem Netzwerk Genomische
Medizin haben wir in einer engen Zu-
sammenarbeit mit Krankenhäusern
und niedergelassenen Fachärzten in
Nordrhein-Westfalen eine der weltweit
größten Genotypisierungsplattformen
für Lungenkrebs aufgebaut und füh-
ren aktuell bei über 3.500 Patienten
jährlich eine umfassende molekulare
Diagnostik durch.
Personalized therapy of lung cancer: Success by translational crosslinking
in a tight collaboration with hospitals
and private practices in North-Rhine
Westphalia and offer comprehensive
molecular diagnostics to more than
3,500 patients yearly.
16 17
Prof. Dr. Jürgen Wolf
Prof. Dr. Reinhard Büttner
Prof. Dr. Roman Thomas
Publications
1. Sci Transl. Med 5, 209ra153 (2013): The Clinical Lung Cancer Genome Project (CLCGP) and Network Genomic Medicine (NGM), A genomics-based clas-sification of human lung tumors
2. Journal of Clinical Oncology, Vol 15, No 15, May 2013, doi:10.1200/jco.2012.45.9867: Lessons Learned From Lung Cancer Genomics: The Emerging Concept of Individualized Diagnostics and Treatment
3. Nature Genetics, Vol 44, No 10, October 2012. doi: 10.1038/ng.2396: Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer
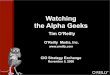
Therapeutically amendable driver mutations in lung cancer and personalized trials of LCGC.
Therapeutisch angehbare Treibermutationen beim Lungen-krebs und personalisiertes Studienprogramm der LCGC.
EGFRmut ph I (FIM) 3rdgen EGFR-TKI (T790M)MET ampl, mut ph I MET-inhibitorALKtransl ph I (FIM) LDK378 (Alk-inhibitor)
KRASmut ph II selumetinib (MEK-inhibitor) + docetaxel
BRAFmut V600 ph II: vemurafenib (BRAF-inhibitor)
BRAFmut inact.ph II: dasatinib
DDR2mut
HER2amp / mut ph II: AUY922 (hsp90-inh.) + trastuzumabROStransl Crizotinib (MET-/ALK-/ROS-inhibitor)FGFR1amp ph I (FIM): BGJ398 (FGFR-TKI)P53wildtype ph I (FIM): CGM097 (p53/HDM2inh)
unknown
KRAS
EGFR
ALK BRAF PIK3CA
HER2 MET RET ROS
EGFRmut ph I (FIM) 3rdgen EGFR-TKI (T790M)
MET ampl, mut ph I MET-inhibitor
ALKtransl ph I (FIM) LDK378 (Alk-inhbitor)
KRASmut ph II selumetinib (MEK-inhibitor) + docetaxel
BRAFmut V600 ph II: vemurafenib (BRAF-inhibitor)
BRAFmut inact. ph II: dasatinib
DDR2mut
HER2amp / mut ph II: AUY922 (hsp90-inh.) + trastuzumab
ROStransl Crizotinib (MET-/ALK-/ROS-inhibitor)
FGFR1amp ph I (FIM): BGJ398 (FGFR-TKI)
P53wildtype ph I (FIM): CGM097 (p53/HDM2inh) unknown
FGFR1amp
PTENmut
PTENloss
PIK3CAmut
KRASmut DDR2mut
Adenocarcinoma
Sqamous cell carcinoma
unknown
KRAS
EGFR
ALK BRAF PIK3CA
HER2 MET RET ROS
EGFRmut ph I (FIM) 3rdgen EGFR-TKI (T790M)
MET ampl, mut ph I MET-inhibitor
ALKtransl ph I (FIM) LDK378 (Alk-inhbitor)
KRASmut ph II selumetinib (MEK-inhibitor) + docetaxel
BRAFmut V600 ph II: vemurafenib (BRAF-inhibitor)
BRAFmut inact. ph II: dasatinib
DDR2mut
HER2amp / mut ph II: AUY922 (hsp90-inh.) + trastuzumab
ROStransl Crizotinib (MET-/ALK-/ROS-inhibitor)
FGFR1amp ph I (FIM): BGJ398 (FGFR-TKI)
P53wildtype ph I (FIM): CGM097 (p53/HDM2inh) unknown
FGFR1amp
PTENmut
PTENloss
PIK3CAmut
KRASmut DDR2mut
Adenocarcinoma
Sqamous cell carcinoma Sqamous cell carcinomaAdenocarcinoma

Das maligne Melanom hat die schlech-
teste Prognose aller Hauttumore. In
Deutschland entwickeln etwa 15.000
Menschen pro Jahr ein Melanom und
2.000 Menschen versterben daran.
Melanome sind besonders gefährlich,
da sie früh metastasieren. In den ver-
gangenen Jahren wurden eine Reihe
von neuen Therapien entwickelt, die
bestimmte Signalwege im Melanom
unterbrechen (z. B. BRAF, NRAS oder
CKIT) oder die Effektivität von immu-
nologischen Abwehrmechanismen
verstärken (z. B. Antikörper gegen
CTLA-4, PD-1) und damit das Fort-
schreiten der Erkrankung verzögern.
Unser translationaler Ansatz
Prof. G. Hartmann, Prof. C. Mauch
and Prof. T. Tüting untersuchen Me-
chanismen der Tumorinvasion und
Tumormetastasierung sowie die Ak-
tivierung der angeborenen und der
erworbenen Immunantwort gegen
Melanomzellen. Prof. Hartmann ent-
wickelt neue therapeutische Ansätze,
bei denen definierte Oligonukleotide
Rezeptoren des angeborenen Immun-
Zielgerichtete Immunintervention beim Melanom
Malignant melanoma is the most fatal
form of skin cancer. In Germany, ap-
proximately 15,000 people develop
melanoma annually and 2,000 people
die of it every year. Its particular malig-
nancy is based on the fact that small
tumours tend to metastasize early via
the lymphatic vessels and the blood
stream. In the last years new therapies
for melanoma have been developed
targeting specific genetic mutations in
tumor cells (e.g. BRAF, NRAS or CKIT)
and mechanisms how tumor-specif-
ic cytotoxic immune responses are
regulated (e.g. CTLA-4, PD-1) which
brought new hope for patients with
progressive disease.
Our translational approach
Prof. G. Hartmann, Prof. C. Mauch and
Prof. T. Tüting investigate mechanisms
involved in tumor invasion and metas-
tasis as well as processes governing
the activation of innate and adaptive
immunity against melanoma cells. Spe-
cifically, Prof. Hartmann targets innate
immune sensing receptors expressed
in melanoma cells, such as RIG-I, and
develops synthetic oligonucleotides
selectively targeting these receptors.
systems nicht nur in Immun- sondern
auch in Tumorzellen selbst aktivieren,
insbesondere den Rezeptor RIG-I. Auf
diese Weise können Tumorzellen in
den Zelltod getrieben werden. Ge-
meinsam planen die Gruppen, diesen
Ansatz in Kombination mit anderen
neuen Therapieverfahren in translatio-
nalen Forschungsansätzen in die Klinik
zu bringen.
Directing innate immunity against melanoma
Besides exploring the biology of ma-
lignant melanoma the groups aim to
experimentally develop novel combi-
nation therapy protocols which can
be translated from basic science into
clinical trials.
18 19
Prof. Dr. Gunther Hartmann
Prof. Dr. Thomas Tüting
Prof. Dr. Cornelia Mauch
Publications
1. Nature, 2014 507: 109-13: Ultraviolet-radiation-induced inflammation promotes angiotropism and metastasis in melanoma
2. Cancer Discov, 2014: Immune-cell poor melanomas benefit from PD-1 blockade after targeted type I IFN activation
3. Nature, 2012 490, 412-6: Melanomas resist T-cell therapy through inflammation-induced reversible dedifferentiation
Activation of RIG-I results in selective tumor cell death and the induction of an anti-tumor response in immune cells.
Die Aktivierung von RIG-I führt in Tumorzellen zum Zelltod, während in Immunzellen eine Immunantwort gegen den Tumor induziert wird.

Das Kölner Zentrum für familiären
Brust- und Eierstockkrebs bietet gene-
tische Beratung und Unterstützung für
Frauen mit einem erhöhten familiären
Risiko für Brust- und Eierstockkrebs,
einschließlich interdisziplinäre Konsul-
tation und präventive Maßnahmen.
Trotz der Fortschritte im Verständnis
der erblichen Grundlagen des fami-
liären Brust- und Eierstockkrebses
können heute bekannte erbliche Fak-
toren wie z. B. Veränderungen in den
BRCA1/2 Genen nur einen Teil aller
familiären Fälle erklären. Neuere Daten
deuten darauf hin, dass zusätzliche ge-
netische und nicht-genetische Kompo-
nenten multifaktoriell zur Erkrankung
beitragen und das Erkrankungsrisi-
ko in Gegenwart einer pathogenen
BRCA1/2 Genmutation modulieren
können.
Unser Ziel ist es, die vielfältige Archi-
tektur des Brust- und Eierstockkrebses
weiter aufzuschlüsseln, neue Risiko-
faktoren und deren Interaktionen zu
identifizieren und dieses Wissen für
Patientinnen durch eine personalisierte
Familiärer Brust- und Eierstockkrebs: Forschung für die personalisierte Prävention
The Cologne Center of Familial Breast
and Ovarian Cancer provides genetic
counselling and support for women
with an increased familial risk for
breast and ovarian cancer, including
interdisciplinary consultation and ad-
equate preventive measures. Despite
the progress achieved in understand-
ing the genetic basis of familial breast
and ovarian cancer, known genetic
risk factors such as alterations in the
BRCA1/2 genes explain only part of
all familial cases. Recent data suggest
that additional genetic and non-genet-
ic risk factors contribute to the mul-
tifactorial disease and also modulate
disease risk in the presence of a clearly
pathogenic BRCA1/2 gene mutation.
Due to the multifaceted architecture
of breast and ovarian cancer, our vi-
sion is to identify and validate novel
genetic and non-genetic risk factors
and their interactions, followed by the
implementation of both into personal-
ised risk prediction and cancer preven-
tion programmes. To reach these goals
we are closely cooperating with inter-
Risiko-Prädiktion und Krebsprävention
nutzbar zu machen. Um diese Ziele zu
erreichen arbeiten wir eng mit inter-
nationalen Studiengruppen zusam-
men und koordinieren das Deutsche
Konsortium für familiären Brust- und
Eierstockkrebs, das durch die Identifi-
zierung neuer Risikogene internatio-
nale Aufmerksamkeit erzielen konnte.
Hereditary breast- and ovarian cancer: Research for a personalized prevention
national study groups and coordinate
the German Consortium for Heredi-
tary Breast- and Ovarian Cancer, which
raised international attention due to
the identification of new disease and
disease-modifying genes.
20 21
PD Dr. Kerstin Rhiem
Prof. Dr. Rita K. Schmutzler
PD Dr. rer. nat. Eric Hahnen
Dr. rer. nat. Barbara Wappenschmidt
Publications
1. Nat. Genet., 2013 Apr; 45(4):371-84: Multiple inde-pendent variants at the TERT locus are associated with telomere length and risks of breast and ovarian cancer
2. Nat. Genet., 2013 Apr; 45(4):353-61: Large-scale genotyping identifies 41 new loci associated with breast cancer risk
3. Nat. Genet., 2013 Apr; 45(4):392-8: Genome-wide association studies identify four ER negative-specific breast cancer risk loci
Interaction partners and function of BRCA1 and BRCA2. Mutations in genes such as ATM, CHK2, NBN also increase breast cancer risk (Meindl et al., 2013).
Interaktionspartner/Funktion von BRCA1 und BRCA2. Neben BRCA1/2 erhöhen auch Mutationen z. B. in ATM, CHK2, NBN das Brustkrebsrisiko (Meindl et al., 2013).

A) VOR Therapie /Before therapy B) NACH Therapie/After therapy
Vitales Tumorgewebe
Vital tumor
Kein vitales Tumorgewebe No vital tumor
Die nicht nicht-invasiven Möglich-
keiten der molekularen Bildgebung
und der sogenannten Hybrid-Bildge-
bung erlauben eine immer präzisere
und individuell maßgeschneiderte
Diagnostik.
Der Begriff der molekularen Bild-
gebung bezieht sich auf die Mög-
lichkeit krankhafte Veränderun-
gen im Körper bereits in kleinster
(molekularer) Form nachweisen
zu können. Dies gelingt mit der
Positronen-Emissions-Tomographie
(PET), die durch entsprechende
Spürsubstanzen („Tracer“) eine
äußerst hohe Empfindlichkeit zum
Nachweis von bösartig veränderten
Zellen aufweist. In den modernen
„Hybrid“ PET/CT-Scannern wird die
PET kombiniert mit der Computer-
tomographie (CT) in einem Gerät
durchgeführt. So wird bei größt-
möglichem Patientenkomfort eine
exakte anatomische Zuordnung (CT)
der empfindlich erfassten Tumor-
suspekten Veränderungen (PET)
möglich.
Molekulare und multimodale Bildgebung
The non-invasive methods of molecu-
lar and „hybrid“-imaging facilitate a
more precise and individually tailored
diagnosis.
Molecular imaging refers to the possi-
bility to measure pathological changes
in the body in smallest (molecular)
magnitude. This became possible with
Positron Emission Tomography (PET),
which has a paramount sensitivity with
regard to the detection of malignant
tissue. In modern hybrid PET/CT-scan-
ners, PET is technically combined with
conventional computer tomography
(CT) in one instrument. This allows an
anatomically exact allocation (CT) of
tumor-suspicious findings (PET) at high
patient comfort.
Within CIO research on PET/CT is per-
formed in manifold ways:
1. Staging of the extent of disease at
the time of first diagnosis.
2. Re-staging to exclude/verify recur-
rence of a tumor.
3. Therapy-monitoring to select an in-
dividually tailored therapy, to meas-
Im CIO findet Forschung zum Thema
PET/CT in vielerlei Hinsicht statt:
1. Bestimmung der Ausdehnung der Er-
krankung bei Erstdiagnose (Staging).
2. Nachweis/Ausschluss von erneut auf-
tretendem Tumorgewebe (Re-Staging).
3. Auswahl einer individualisiert maß-
geschneiderten Tumortherapie und
frühzeitige Kontrolle des Anspre-
chens mit der Möglichkeit das The-
rapieregime anzupassen.
4. Entwicklung neuer PET-Tracer.
Molecular and multimodal Imaging
ure therapy response and to change
the therapy regime, if necessary.
4. Development of novel PET-tracers.
22 23
Prof. Dr. Alexander Drzezga
Prof. Dr. Markus Essler
Publication
1. Lancet, 2012; May; 379(9828):1791-9: Reduced-intensity chemotherapy and PET-guided radiotherapy in patients with advanced stage Hodgkin’s lymphoma (HD15 trial): a randomised, open-label, phase 3 non-inferiority trial
PET/CT in Hodgkin lymphoma, before and after chemo-therapy. Good therapy response is obvious on the basis of the decrease in activity of the mediastinal lymph node packages.
PET/CT beim Hodgkin-Lymphom vor und nach Chemothe-rapie. Das gute Therapieansprechen ist an der Abnahme der Stoffwechselaktivität der mediastinalen Lymphkno-tenpakete ablesbar.
Hodgkin-Lymphom / Lymphoma
B) NACH Therapie / After therapyA) VOR Therapie / Before therapy

Prof. Dr. Michael Hallek
Prof. Dr. Jürgen Wolf
Prof. Dr. Reinhard Büttner
Das zunehmende Verständnis der
molekularen Grundlagen von Krebs
ermöglicht für immer mehr Patienten
eine spezifisch auf die genetischen
Eigenschaften ihres Tumors zuge-
schnittene, sogenannte personalisierte
Therapie. Aktuelle Herausforderungen
beinhalten die Entdeckung neuer mo-
lekularer Zielstrukturen (Treibermutati-
onen), die Entwicklung einer leistungs-
fähigen molekularen Diagnostik, die
schnelle klinische Überprüfung neuer
Ansätze und die Implementierung die-
ser high-tech Medizin in die klinische
Routineversorgung.
Unser Ansatz:
Im CIO arbeiten wissenschaftliche
und klinische Arbeitsgruppen Hand
in Hand. Der Aufbau einer translati-
onalen Plattform für frühe klinische
Studien ermöglicht die schnelle Über-
prüfung neuer Therapieansätze am Pa-
tienten. Der Aufbau einer molekularen
Hoffnungsträger „Personalisierte Medizin“ Unser Ansatz
Our increasing understanding of the
molecular mechanisms underlying
cancer enables new personalized
therapies, specifically tailored to the
genetic characteristics of individual
tumors. Current challenges are the
discovery of new molecular target
structures (driver mutations), the de-
velopment of powerful molecular di-
agnostics, the rapid clinical evaluation
of new therapies and the implementa-
tion of such a high-tech medicine into
clinical routine.
Our approach:
Within CIO basic science and clinical
groups are working closely together.
Challenge „personalized medicine“ Our approach
The development of a translational
platform for early clinical trials ena-
bles rapid evaluation of new thera-
peutic approaches in patients. The
development of molecular multiplex-
diagnostics, based on next generation
sequencing technologies, allows us to
analyse tumor samples of currently
19,000 patients yearly for the pres-
ence of driver mutations. By 2015 we
want to offer these genotyping pro-
gram to all cancer patients within the
CIO Köln Bonn. Moreover, outreach
structures like the Network Genomic
Medicine established initially for lung
cancer will be developed for further
cancers including melanoma, gastro-
Multiplex-Diagnostik auf der Basis der
Next Generation Sequencing Techno-
logie ermöglicht schon jetzt die Unter-
suchung der Tumorproben von über
19.000 Patienten jährlich auf das Vor-
handensein von Treibermutationen.
Bis 2015 soll diese Untersuchung al-
len Krebspatienten im CIO Köln Bonn
angeboten werden. Parallel hierzu
bauen wir das zunächst für Lungen-
krebspatienten entwickelte Netzwerk
Genomische Medizin sukzessive für
weitere Tumorerkrankungen (aktuell
Melanom, gastrointestinale Tumoren)
auf, um auch den Patienten im Ein-
zugsbereich des CIO Köln Bonn den
Zugang zu innovativen Therapien zu
ermöglichen.
intestinal cancer and breast cancer to
give patients in the catchment area of
the CIO Köln Bonn access to innovative
therapies.
24 25
Publication
1. Journal of Clinical Oncology, Vol 15, No 15, May 2013, doi:10.1200/jco.2012.45.9867 Lessons Learned From Lung Cancer Genomics: The Emerging Concept of Individualized Diagnostics and Treatment

PD Dr. Georg Feldmann
Duktale Adenokarzinome des Pankre-
as („Bauchspeicheldrüsenkrebs“) stel-
len die vierthäufigste krebsbedingte
Todesursache in der westlichen Welt
dar. In der überwiegenden Mehrzahl
der Fälle wird die Erkrankung in fort-
geschrittenen Stadien diagnostiziert,
die eine operative Resektion in kurati-
ver Intention nicht mehr zulassen. Die
in diesen Fällen verbleibenden palli-
ativen Therapiemöglichkeiten sind
nur begrenzt wirksam, so dass die
Entwicklung neuer Therapieansätze
wünschenswert ist.
Im Rahmen unserer Arbeiten verwen-
den wir klinisch relevante transgene
sowie Xenograft-Mausmodellsysteme,
welche die wichtigsten Charakteristi-
ka humaner Pankreaskarzinome mög-
lichst realistisch widerspiegeln sollen,
um molekular definierte therapeuti-
Translationale Therapieforschung beim Pankreaskarzinom
Pancreatic cancer is one of the most
dismal of human malignancies and
represents the forth most common
cause of cancer-related mortality in the
Western World. Therapeutic options
for the majority of advanced, non-re-
sectable cases of pancreatic cancer are
limited and hence novel therapeutic
strategies are urgently required.
As part of this project we aim to em-
ploy genetically engineered as well
as personal low-passage xenograft
models that faithfully recapitulate key
clinical features and genetic variety of
human pancreatic cancers in order to
identify novel molecular targets for
therapeutic intervention and perform
preclinical drug testing studies.
This research platform will help to
guide our clinical efforts in picking the
best possible treatment modality for
each individual patient in the future
and hopefully also lead to the initiation
of clinical trials of novel therapeutic
agents.
sche Angriffsziele zu identifizieren und
so neue therapeutisch wirksame Subs-
tanzen zu entwickeln und präklinisch
zu testen.
Auf diese Weise wird eine Forschungs-
plattform aufgebaut, mit deren Hilfe
zukünftig die für individuelle Patienten
jeweils am besten geeignete Thera-
piestrategie gefunden und ihre Wirk-
samkeit im Rahmen klinischer Studien
getestet werden soll.
Pancreatic cancer translational research
26 27
Publications
1. Clin Cancer Res., 2013 Mar 1; 19(5):1139-46: Per-sonalized chemotherapy profiling using cancer cell lines from selectable mice
2. J Biol Chem., 2012 Nov 30; 287(49):40924-37: The NAD+-dependent histone deacetylase SIRT6 promotes cytokine production and migration in pancreatic can-cer cells by regulating Ca2+ responses
3. Neoplasia, 2011 Oct;13(10):923-30: Ectopic over-expression of Sonic Hedgehog (Shh) induces stromal expansion and metaplasia in the adult murine pancreas
Genetically engineered syngenic as well as xenograft mouse models of pancreatic cancer are generated and used for target discovery and preclinical evaluation of novel treatment regimens. (reproduced from Tentler J et al., Nat. Rev. Clin. Oncol. 2012)
Transgene und Xenograft-Mausmodelle humaner Pankre-askarzinome werden generiert und zur Identifikation neuer therapeutischer Angriffsziele verwendet. (modifiziert aus Tentler J et al., Nat. Rev. Clin. Oncol. 2012)

Prof. Dr. Glen Kristiansen
Das Prostatakarzinom ist der häufigs-
te maligne Tumor des Mannes in der
westlichen Welt. Bis heute beruht die
Planung der Therapie auf klinischen
und histologischen Parametern, ins-
besondere dem Gleason Score; die
zugrundeliegende molekulare Biolo-
gie ist noch unverstanden. Die zwei
wesentlichen klinischen Probleme
sind a) die zuverlässige Erkennung
insignifikanter Karzinome in frühen
Erkrankungsstadien (denen eine The-
rapie erspart werden kann) und b) die
erfolgreiche Behandlung hormonre-
fraktärer Karzinome.
Unsere Arbeit konzentriert sich auf die
Entdeckung a) diagnostischer, prog-
nostischer und prädiktiver Biomarker
für frühe Stadien, b) therapeutischer
Ziele für späte Stadien, und c) von
Markern zur Verlaufskontrolle.
Translationale Prostatapathologie
Prostate cancer is the most common
malignant tumor of men in the west-
ern world. Till now, therapy planning
rests mainly on clinical and histological
parameters, particularly the Gleason
score, and the underlying molecular
biology is only insufficienly under-
stood. The two leading clinical prob-
lems are a) the reliable identification of
insignificant carcinoma in early stages
(that might be spared treatment), and,
b) successful treatment of castrate re-
sistant tumors in late stages.
Consequently, our work focuses on
the identification a) of diagnostic,
prognostic and predictive biomarkers
for early stages, b) therapeutic targets
for late stage disease, and c) mark-
ers for monitoring therapy response.
In recent years, we have extensively
profiled prostate cancer on various
biological levels (mRNA, epigenetics/
microRNA, proteome, metabolome)
and have made seminal contributions
in the field. Our expertise in genitou-
rinary histopathology, which is among
the leading in europe, is beneficial to
several large clinical trials including
Wir haben in den letzten Jahren um-
fangreiche Prostatakarzinomprofile
auf verschiedenen Ebenen (mRNA,
Epigenetik/microRNA, Proteom, Me-
tabolom) erstellt und hier ganz we-
sentliche Beiträge geleistet. Unsere Ex-
pertise in Urogenitaler Pathologie, die
zu den führenden in Europa gehört,
leistet wichtige Beiträge zu mehreren
großen klinischen Studien (einschließ-
lich PREFERE und PROBASE) und dient
als verlässliche Basis für die weiterfüh-
rende molekulare Forschung.
Translational prostate pathology
the PREFERE and the PROBASE trial
and serves as a robust basis for further
molecular research.
28 29
Publication
1. Histopathology, 2012 Jan; 60(1):125-41: Diagnos-tic and prognostic molecular biomarkers for prostate cancer
Workflow of reference pathology in the PREFERE trialAblauf der Referenzpathologie in der PREFERE-Studie
1
RANDOMISATION
Überprüft Selektionskriterien und vervollständigt die Diagnostik, veranlasst ggf. Re-Biopsie
Kriterien nicht erfüllt
Teilnahme nicht möglich
Erklärung des Ablaufs,Aushändigung derStudienunterlagen
Stratifikation- Zentrum- Gleason Score < 7 vs. 7a- Alter < 65 vs. 65-70 vs. > 70 J.- PSA < 6 ng/ml vs. > 6 ng/ml
Studientherapie
Prüfzentrum
Aufklärung
Teilnahme nicht möglich
Kriterien erfüllt
Kriterien nicht erfüllt
SchriftlicheEinwilligungserklärung
Präferenzentscheidung
Kriterien erfüllt
Referenzpathologie
! Berlin M. Dietel ! Bonn G. Kris0ansen
(Koordinator) ! Dresden G. Bare5on ! Erlangen A. Hartmann ! Rostock A. Erbersdobler
Ablauf PZ

Das Ovarialkarzinom besitzt unter
Tumoren des weiblichen Genitaltrakts
die höchste Mortalitätsrate und ist das
fünfthäufigste zum Tode führende
Malignom der Frau. Um die Progno-
se zu verbessern, ist die Etablierung
neuer Therapien unabdingbar.
Basierend auf der hohen Immuno-
genität des Ovarialkarzinoms ist eine
Immuntherapie sinnvoll. Wir unter-
suchen ein Konzept, welches eine
Virusinfektion imitiert und somit anti-
virale Mechanismen zur Verstärkung
der Immunantwort nutzt. Wir zeigten,
dass die Stimulation der angeborenen
Immunität über die Induktion einer
immunogenen Tumorzellapoptose
zur Immunverstärkung und Überwin-
dung immunsuppressiver Mechanis-
men führt.
Trotz der hohen Ansprechrate auf
die Primärtherapie kommt es in der
überwiegenden Mehrzahl aller Fälle
zu Rezidiven. Aufgrund fehlender
Daten führten wir eine Phase I-Studie
mit Cisplatin als hypertherme intrape-
Neue Therapieansätze beim Ovarialkarzinom: Von der Immuntherapie zur HIPEC
Ovarian cancer is the most fatal cancer
of the female genital tract, and the fifth
most lethal type of cancer in women.
Since new treatments are needed to
improve survival we evaluate innovative
therapies either based on immunologic
mechanisms or new routes of chemo-
therapeutic application.
Immunotherapy plays an important
role since ovarian cancer has a high
immunogenic potential, which can be
harnessed for therapy. Our approach
is using nucleic acid agonists, which
mimics a viral infection in cancer cells.
We thereby exploit the highly effec-
tive anti-viral mechanisms of innate
immunity, consequently inducing
an immunogenic form of tumor cell
death, enhancing proinflammatory
mechanisms and overcoming anti-
inflammatory effects.
One of the main obstacles in ovar-
ian cancer is the failure of the initial
therapy to prevent relapse. Since a
local administration of chemothera-
py is rational to achieve higher drug
concentrations, and hyperthermia is
known to cause direct cytotoxicity, we
conducted a phase I trial of Cisplatin
ritoneale Chemoperfusion (HIPEC) bei
Patienten mit platinsensiblem Rezidiv
durch. Hintergrund ist, dass eine
lokale Applikation höhere Wirkstoff-
konzentrationen erreicht, während
die Hyperthermie tumorizid wirkt. Wir
zeigten, daß dies sicher und machbar
ist. Basierend auf diesen in Kürze
publizierten Daten ist eine Multicen-
terstudie zum adjuvanten Einsatz in
Vorbereitung.
New therapeutic approaches in ovarian cancer: From immunotherapy to HIPEC
administered as hyperthermic intra-
peritoneal chemoperfusion (HIPEC)
in patients with recurrent cancer,
and showed, the method is safe and
feasible. Based on these soon to be
published results a multicentre study
in the adjuvant setting is underway.
30 31
Prof. Dr. Peter Mallmann
Prof. Dr. Walther Kuhn
Publications
1. Int J Cancer, 2014 (accepted): Hyperthermic intra-peritoneal chemoperfusion for patients with recurrent ovarian cancer
2. BMC Cancer, 2012;12: 600: Mucin-1 and its rela-tion to grade, stage and survival in ovarian carcinoma patients
3. Eur J Immunol, 2011 Oct;41(10):3028-39: Immuno-genic cell death of human ovarian cancer cells induced by cytosolic poly(I:C) leads to myeloid cell maturation and activates NK cells
Characterization of ovarian cancer cells. Expression of epithelial antigen and tumor-associated antigen FRα visualized by immunocytochemistry (600x).
Epithelial antigen FRα
Charakterisierung von Ovarialkarzinomzellen. Expression von epithelial antigen und des Tumorantigens FRα (Im-munzytochemie, 600x).

Eine effektivere Behandlung von
malignen primären Hirntumoren
und Hirnmetastasen ist das große
Ziel des Netzwerk Neuroonkologie
im CIO. Wir sind hier schon sehr
erfolgreich und leiteen die deutsch-
landweit größten molekular (nach
MGMT-Status) definierten Studien
zur Primärtherapie von Patienten
mit Glioblastom (CeTeG- und Glari-
us-Studie). Diese Studien haben das
Potential, die Standardtherapie für
Glioblastompatienten neu zu defi-
nieren. Für Patienten mit Hirnmeta-
stasen werden wir die Rolle lokaler
Therapien wie Chirurgie, Brachythe-
rapie und Cyber Knife-Radiochirurgie
im multimodalen Therapiekonzept
untersuchen.
Alle Studien zu primären Hirntumo-
ren und Hirnmetastasen im Netz-
werk Neuroonkologie umfassen ein
umfangreiches translationales Pro-
gramm, welche vor allem auf mole-
kulare und bildgebende Parameter
wie MRT und PET abzielen.
Maligne Hirntumoren: Schritte in Richtung personalisierter Therapie
The improvement of therapeutic op-
tions for malignant primary brain tu-
mors and CNS metastases is the main
task for the neurooncology network at
the CIO. Our group has already been
successful in this regard by leading
the concurrent key randomized trials
(Glarius and CeTeG) for newly diag-
nosed glioblastoma (GBM) patients
with the potential to redefine the
standard treatment of GBM accord-
ing to the MGMT methylation status.
For patients with brain metastases,
we will address the role of local treat-
ments like surgery, brachytherapy and
cyberknife radiosurgery within a mul-
timodal concept. Future trials for all
kinds of brain malignancies include a
strong translational program focusing
on molecular and imaging parameters
like MRI and PET.
Beyond defining new therapies, these
approaches will also help to better
understand the underlying genetic
processes leading to primary brain
tumors and CMS metastases and to
better define the response of these
tumors to therapy.
Wir wollen mit unserem Programm
nicht nur neue, personalisierte, Be-
handlungsansätze definieren, son-
dern auch die zugrundeliegende
genetischen Prozesse, die zur Entste-
hung von Hirntumoren und Hirnme-
tastasen führen oder das Ansprechen
auf Behandlungen bedingen, besser
verstehen.
Malignant brain tumors: Steps to personalized therapy
32 33
Prof. Dr. Roland Goldbrunner
Prof. Dr. Matthias Simon
Prof. Dr. Ulrich Herrlinger
Publications
1. Nat Genet, 2009; 41: 899-904 Genome-wide associ-ation study identifies five susceptibility loci for glioma
2. Neurosurgery, 2011; 68:1209-18: Stereotactic 125iodine brachytherapy for the treatment of singular brain metastases: closing a gap?
3. J Clin Oncol, 2011; 29:134-41: Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952-26001 study

Uveale Melanome, konjunktivale
Melanome und konjunktivale Karzi-
nome zählen zu den häufigsten und
bösartigsten Tumoren des Auges. Eine
wirksame Therapie zur Prävention oder
Therapie des metastasierten Uvea- und
Bindehautmalignoms ist derzeit nicht
bekannt.
Unser translationaler Ansatz
Die Ausbildung neuer aus bereits
bestehenden Lymph- und Blutgefä-
ßen (Lymph- und Hämangiogenese)
gilt als ein entscheidender Risiko-
faktor für die Metastasierung und
Mortalität nicht-okulärer Neoplasien.
In Vorarbeiten konnten wir erstmals
das Vorhandensein einer tumor-
assoziierten Lymphangiogenese auch
bei malignen Tumoren der Augenober-
fläche zeigen. Diese Tumor-induzierten
Lymphgefäße korrelieren signifikant
mit der lokalen und systemischen
lymphogenen Metastasierung, dem
Rezidivrisiko und der Mortalität.
Anti-(lymph)angiogene Therapie bei malignen Tumoren des Auges
Uveal melanomas, conjunctival
melanomas, and conjunctival carci-
nomas are the most common and
frequently lethal malignancies of the
eye. Currently, there is no effective
therapy for prevention or treatment
of uveal and conjunctival tumor
metastases.
Our translational approach
The outgrowth of new from preex-
isting lymphatic and blood vessels
(lymph- and hemangiogenesis) is
considered as a decisive risk factor
for metastasis and mortality of non-
ocular neoplasms. Recently, we could
demonstrate the presence of tumor-
associated lymphangiogenesis in
ocular surface malignancies, to our
knowledge for the first time. These
tumor-induced lymphatic vessels
were significantly associated with an
increased risk of local and systemic
lymphatic spread, local recurrence
and tumor-related death.
Our vision includes the transla-
tional implementation of novel
non-invasive risk scores as well as
Unser translationales Ziel umfasst
die Etablierung neuer nicht-invasiver
klinischer Risikoscores als auch neu-
er adjuvanter anti(lymph)angiogener
Therapien in der klinischen Versorgung
von malignen Tumoren des Auges,
um Rezidiv-, Metastasierungs- und
Mortalitätsrisiko dieser Patienten zu
verringern.
Anti-(lymph)angiogenic therapies for malignant tumors of the eye
novel adjuvant anti(lymph)angiogen-
ic therapies in the clinical workup of
malignant ocular tumors in order to
reduce the risk of local recurrence,
lymphatic spread, hematogenous
metastasis, and tumor-related death
in these patients.
34 35
PD Dr. Ludwig M. Heindl
Prof. Dr. Claus Cursiefen
Publications
1. Prog Retin Eye Res, 2013 May; 34:89-124: Novel anti(lymph)angiogenic treatment strategies for corneal and ocular surface diseases
2. J Exp Med, 2011 May 9; 208(5): 1083-92: Throm-bospondin 1 inhibits inflammatory lymphangiogenesis by CD36 ligation on monocytes
3. Ophthalmology, 2011 Dec; 118(12): 2351-60: Prog-nostic significance of tumor-associated lymphangi-ogenesis in malignant melanomas of the conjunctiva
Conjunctival melanoma: Clinical (left) and histologic findings (middle) with immunohistochemical detection of tumor-associated lymphatic vessels.
Malignes Melanom der Bindehaut: Klinisches (links) und histologisches Bild (Mitte) mit immunhistochemischer Darstellung tumorassoziierter Lymphgefäße.

Die Computertomographie (CT) und
Magnetresonanz-Tomographie (MRT)
erlauben meist eine hochaufgelöste
Darstellung von Tumoren und eine
Bestimmung des Therapieansprechens
von klassischen Chemotherapien an
Hand der Größenänderung. Neue
zielgerichtete molekulare Therapeuti-
ka führen jedoch oftmals lediglich zu
einer Veränderung in der Tumorphy-
siologie, wie der Tumordurchblutung,
ohne messbare Größenänderung.
Unsere Motivation ist die Entwick-
lung und Erforschung von modernen
quantitativen und funktionellen Bild-
gebungsmethoden, die eine sichere
Bestimmung der Tumorperfusion, der
Tumorgefäßpermeabilität und des
Tumorgefäßdurchmessers ermögli-
chen. Durch die hervorragende Ver-
knüpfung von Forschung und Klinik
im Institut für Radiologie können
diese modernen Techniken direkt in
klinische Untersuchungsprotokolle
transferiert werden und im Patien-
ten zur verbesserten Tumorcharakte-
risierung (Staging) und frühzeitigen
Moderne quantitative und funktionelle Bildgebung
Computed Tomography (CT) and
Magnetic Resonance Imaging (MRI)
are main-stays in oncological imaging
with respect to tumor detection, char-
acterization, and treatment monitor-
ing. Novel target-specific drugs induce
predominantly changes in tumor vas-
culature and physiology which are not
necessarily reflected in conventional
size regression measurements. Hence,
there is a strong need for non-invasive
biomarkers which allow for an assess-
ment of tumor vascular functionality.
Hence, our motivation focuses on the
development and evaluation of mod-
ern quantitative and functional imag-
ing methods for non-invasive determi-
nation of tumor perfusion, microvessel
permeability, and mean vessel size.
Our institutional platform allows for
a direct translation of these modern
imaging techniques into clinical study
protocols. Among others, dynamic
contrast-enhanced MRI (DCE-MRI) is a
very promising, non-ionizing imaging
method which allows early response
monitoring of novel molecular agents
already a few days after treatment
initiation.
Evaluierung des Therapieansprechens
(Response) angewendet werden. Die
dynamische Kontrastmittel-gestützte
MRT (DCE-MRT) stellt hierbei eine sehr
vielversprechende Technik dar, die ide-
alerweise eine Response-Beurteilung
bereits in den ersten Tagen nach The-
rapieinitiierung erlaubt.
Modern Quantitative and Functional Imaging
36 37
Prof. Dr. David Maintz
Dr. Thorsten Persigehl
Publications
1. Mol Imaging, 2013 Oct; 12(7): 1-11: Vessel Size Imaging (VSI) by Robust Magnetic Resonance (MR) Relaxometry: MR-VSI of Solid Tumors in Correlation with Immunohistology and Intravital Microscopy
2. Angiogenesis, 2014 Jan; 17(1): 235-46: Non-invasive monitoring of tumor-vessel infarction by retargeted truncated tissue factor tTF-NGR using multi-modal imaging
DCE-MRI of a lung cancer demonstrating a clear reduction of the tumor perfusion as early as 1 week after novel molecular therapy.
DCE-MRT eines Bronchial-Karzinoms, dass bereits 1 Woche nach zielgerichteter molekularer Therapie eine deutliche Reduktion der Tumorperfusion zeigt.

A) VOR Therapie/Before therapy B) NACH Therapie/After therapy
Vitales Tumorgewebe
Vital tumor tissue
Kein vitales Tumorgewebe No vital tumor
tissue
Radionuklidtherapie [PRRT] beim neuroendokrinen Pankreas-Tumor Radionuclide therapy in a neuroendocrine tumor of the pancreas
Die Radionuklidtherapie erlaubt die
Therapie bösartiger Erkrankungen
mit Hilfe von speziell radioaktiv mar-
kierten Substanzen, die Ihren Weg
gezielt ins Tumorgewebe finden, das
gesunde Gewebe dabei aber weitest-
gehend aussparen. Anders als bei der
Strahlentherapie, erfolgt die Behand-
lung hierbei nicht von außen sondern
direkt im Tumor durch die Anreiche-
rung der Therapeutika. Dadurch sind
die Radionuklidtherapieverfahren sehr
effektiv und zugleich überwiegend gut
verträglich. Der stationäre Aufenthalt
findet im CIO Köln Bonn in komfortab-
len Therapiestationen statt und kann
im Regelfall 48 Stunden nach der The-
rapie wieder beendet werden.
Neben der langjährig etablierten Ra-
dioiodtherapie der Schilddrüsenkrebs-
erkrankungen werden im CIO Köln/
Bonn auch neuere Radionuklidthera-
pieverfahren erforscht, z. B.:
1. Die Peptidrezeptor-Radionuklidthe-
rapie (PRRT) der neuroendokrinen
Tumoren (NET). Bei diesem Ver-
fahren binden die therapeutischen
Radionuklidtherapie der Tumorerkrankungen
Radionuclide therapy is a targeted mo-
lecular therapy used in cancer therapy.
Radioactively labelled substances find
their specific way into malignant cells
while mostly sparing benign tissue. In
contrast to external beam radiation,
radiolabelled substances accumu-
late directly in the tumor. As a con-
sequence radionuclide therapies are
quite efficient and usually well toler-
ated. Radionuclide therapies require a
special ward: comfortable bedrooms
are available within the CIO Cologne /
Bonn. Usually, discharge is possible 48
hours after the intravenous infusion of
the radiolabelled substance.
In addition to established molecular
therapies such as radioiodine therapy
in thyroid cancer, the CIO Köln Bonn
performs research on innovative radio-
nuclide therapy options such as:
1. Peptide receptor radionuclide
therapy of neuroendocrine tumors
(NET). This therapy directly targets
somatostatin receptors expressed at
the cell surface of neuroendocrine
tumors.
2. Selective internal radiotherapy
(SIRT) describes the injection of
Substanzen gezielt an Oberflächen-
Bindungsstellen (Somatostatinre-
zeptoren) auf den NET-Tumorzellen.
2. Die selektive interne Radiothera-
pie (SIRT) basiert auf der Injektion
kleiner radioaktiver Partikel (Mik-
rosphären), die sich selektiv in Le-
bertumorgewebe anreichern. So ist
eine effektive und gut verträgliche
Therapie von Lebertumoren und
Lebermetastasen möglich.
Cancer Radionuclide Therapy
radiolabelled microspheres which
selectively accumulate in malignant
tumor tissue within the liver, aim-
ing for an effective and mostly well
tolerated therapy of primary liver
tumors and liver metastases.
Publication
1. Eur J Nucl Med Mol Imaging, 2014 Feb 7: Out-come of peptide receptor radionuclide therapy with 177Lu-octreotate in advanced grade 1/2 pancreatic neuroendocrine tumours
38 39
PD Dr. Samer Ezziddin
Prof. Dr. Matthias Schmidt
Distinct tumor-regression as a result of PRRT in a patient with a pancreatic NET Physiological uptake in kidneys, bladder and spleen.
Darstellung der deutlichen Tumorregredienz nach einer PRRT bei einem Pankreas-NET-Patienten. Physiologisch ist die kräftige Speicherung in den Nieren und der Blase und der Milz.
Radionuklidtherapie [PRRT] beim neuroendokrinen Pankreas-TumorRadionuclide therapy in a neuroendocrine tumor of the pancreas
B) NACH Therapie / After therapyA) VOR Therapie / Before therapy

PalliativmedizinLuftnot und Schmerzen lindern
Palliative CareRelieving pain and dyspnoea
Pain and dyspnoea are among the
most frequent and burdensome symp-
toms of cancer patients. Treatment is
based on clinical experience, and only
a small percentage of patients is re-
fractory to symptomatic treatment.
However, there is a lack of knowledge
in non-specialist settings.
The palliative medicine departments
in Cologne and Bonn are performing
studies on pain and dyspnea manage-
ment, including a clinical study com-
paring different opioids for the relief
of dyspnoea, clinical surveys on break-
through pain and electromechanical
stimulation in chemotherapy-related
neuropathy.
Evidence produced in surveys, clini-
cal trials and systematic reviews has
been integrated in Standard Opera-
tion Procedures in the hospitals and in
national palliative care guidelines, such
as national guidelines for the German
Cancer Society and the German Medi-
cal Board.
Schmerzen und Luftnot gehören zu
den häufigsten und belastendsten
Symptomen bei Tumorerkrankungen.
Die Behandlung beruht auf klinischer
Erfahrung und nur wenige Patienten
scheinen therapierefraktär zu sein.
Außerhalb der spezialisierten Ein-
richtungen sind die Kenntnisse in der
Symptomkontrolle jedoch oft unzu-
reichend.
Die Kliniken für Palliativmedizin in
Bonn und Köln führen Studien zur
Therapie dieser Symptome durch,
unter anderem eine klinische Studie
zum Vergleich von verschiedenen
Opioiden zur Linderung von Luftnot,
Umfragen zu Durchbruchschmerzen
und die Wirkung von elektromechani-
scher Stimulation bei Chemotherapie-
induzierter Neuropathie.
Die Evidenz aus den Studien, Umfra-
gen und Übersichtsarbeiten wurde
in die klinischen Standards der
Krankenhäuser sowie in nationale
Leitlinien integriert.
Der Wissenstransfer zu den nichtspe-
zialisierten Einrichtungen und Be-
handlern erfordert jedoch nachhaltige
Implementationsmaßnahmen. Hierzu
werden Studien sowohl auf der natio-
nalen Ebene (z. B. als geplante Phase-II
Studie zur frühen Integration der Pal-
liativversorgung bei Glioblastom) wie
auch auf der internationalen Ebene in
mehreren EU-geförderten Kollaborati-
ven durchgeführt.
Transfer of knowledge to the non-
specialist setting requires structured
implementation, and implementation
studies are performed both on nation-
al level (for example with a planned
clinical phase II study on early integra-
tion of palliative care for glioblastoma)
as well as on an international level in
several EU-funded collaboratives.
40 41
Prof. Dr. Lukas Radbruch
Prof. Dr. Raymond Voltz
Publications
1. Palliat Med, 2013;27(6):524-32: Episodes of breathlessness: Types and patterns - a qualitative study exploring experiences of patients with advanced diseases
2. Curr Opin Oncol, 2013;25(4):342-52: Early palliative care for patients with advanced cancer: how to make it work?
3. Journal of Pain and Symptom Management, 2012 (43); 593-605: Validation of the Symptom and Problem Checklist of the German Hospice and Pallia-tive Care Evaluation (HOPE)

The Scientific Advisory Board is a council of highly distinguished experts from several countries. It is counselling the CIO since
its foundation in various strategic and scientific concerns. In 2013 the emphasis was placed on the scientific development of
the center by identifying the most promising research approaches. This booklet provides a quick overview of the outcome.
Der wissenschaftliche Beirat steht dem CIO seit seiner Gründung in allen wichtigen strategischen und wissenschaftlichen
Fragen zur Seite. 2013 lag der Arbeitsschwerpunkt auf der wissenschaftlichen Ausrichtung des Zentrums: Das CIO
beriet sich mit dem hochkarätigen, international besetzten Gremium über die vielversprechendsten Forschungsansätze
und ihre weitere Entwicklung. Einen kurzen Einblick in die Ergebnisse gibt diese Broschüre.
Scientific Advisory Board (SAB)Wissenschaftlicher Beirat
Members / Mitglieder
Participants at the SAB meeting 2013 in Cologne.Teilnehmer am SAB-Meeting 2013 in Köln.
William M. BurnsVerwaltungsrat / Board of AdministrationF. Hoffmann-La Roche LtdSchweiz / Switzerland
Prof. Dr. Nancy E. DavidsonDirektorin / DirectorUniversity of Pittsburgh Cancer InstituteUSA
Prof. Dr. James GriffinDirektor / ChairDana Faber Cancer InstituteUSA
Prof. Dr. Adriaan LammertsmaDirektor / Head Department of Nuclear Medicine & PET Research at VU University Medical Center, AmsterdamNiederlande / Netherlands
Ralf RambachVorstandsvorsitzender / CEO Bundesverband Deutsche Lymphom- und LeukämiehilfeDeutschland / Germany
Prof. Dr. Rafael RosellDirektor / HeadMedical Oncology DepartmentHospital Universitari Quirón Dexeus BarcelonaSpanien / Spain
Prof. Dr. Jean-Charles Soria Medical Oncology Paris University XIFrankreich / France
Dr. Christoph StraubVorstandsvorsitzender / CEOBarmer GEKDeutschland / Germany
Prof. Dr. Herbert WaldmannDirektor / DirectorAbteilung Chemische BiologieMax-Planck-Institut für Molekulare PhysiologieDeutschland / Germany
42 43

Joint study platform with more than 200 oncological clinical trials / year.
29 interdisciplinary oncological project groups (IOPs).
Gemeinsame Studienplattformen mit über 200 onkologischen Studien im Jahr.
29 Interdisziplinäre Onkologische Projektgruppen (IOPs).
CIO Köln Bonn Facts and figures
CIO Köln Bonn in Zahlen
Cologne / Köln Campus university hospitalCampus der Uniklinik
Bonn Campus university hospitalCampus der Uniklinik
CIO Köln
24 Kliniken24 hospitals
13 Institute13 institutes
2012: 16.000 Krebspatienten 16,000 cancer patients
CIO Bonn
24 Kliniken24 hospitals
11 Institute11 institutes
2012: 11.000 Krebspatienten 11,000 cancer patients
44 45

Impressum Imprint
Universitätsklinikum Köln Centrum für Integrierte Onkologie Kerpener Straße 62 50937 Köln www.uk-koeln.de
Universitätsklinikum Bonn Centrum für Integrierte Onkologie Sigmund-Freud-Straße 25 53105 Bonnwww.ukb.uni-bonn.de
www.cio-koeln-bonn.de
Gestaltung, DesignMedizinFotoKöln, Uniklinik Köln
Fotografie, PhotographyMedizinFotoKöln, Uniklinik KölnUniversitätsklinikum Bonn (S. 23, 33, 37, 43)
Druck, PrintDruckerei der Uniklinik Köln
© Februar 2014
46

Impressum Imprint
Universitätsklinikum Köln Centrum für Integrierte Onkologie Kerpener Straße 62 50937 Köln www.uk-koeln.de
Universitätsklinikum Bonn Centrum für Integrierte Onkologie Sigmund-Freud-Straße 25 53105 Bonnwww.ukb.uni-bonn.de
www.cio-koeln-bonn.de
Gestaltung, DesignMedizinFotoKöln, Uniklinik Köln
Fotografie, PhotographyMedizinFotoKöln, Uniklinik KölnUniversitätsklinikum Bonn (S. 23, 33, 37, 43)
Druck, PrintDruckerei der Uniklinik Köln
© Februar 2014