Embed Size (px)
Citation preview
Demystifying Insulin The Science and The Art
Davida F. Kruger, MSN,APN-BC,BC-ADM Certified Nurse Practitioner
Division of Endocrinology, Diabetes, Bone and Mineral Disorders
Henry Ford Health SystemDetroit, Michigan

1. ADA National Diabetes Fact Sheet. Available at: http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2005.pdf. Accessed October 11, 2006.
2. ADA. The dangerous toll of diabetes. Available at: http://www.diabetes.org/diabetes-statistics/dangerous-toll.jsp. Accessed October 11, 2006.
Diabetes Today: An Epidemic• In 2005, 20.8 million Americans
(7% of the population) were diagnosed with diabetes1
• In 2008, 40% of Americans >age 20 have either pre-DM or DM
• Complications of diabetes are a major cause of mortality and morbidity1
– >224,000 deaths – 82,000 lower-limb amputations – 44,000 began treatment for
end-stage kidney disease– 12,000-24,000 new cases of
blindness each year• Total cost in the United States in 2002:
$132 billion1

ADA Glycemic Control Targets
• A1C < 7%• Preprandial plasma glucose 70-130 mg/dl• Postprandial plasma glucose (PPG) <180mg/dl
A1c goal must be customized for the individual patient, with consideration of numerous factors such as comorbid conditions, duration of diabetes, history of hypoglycemia, hypoglycemia unawareness, patient education, motivation, adherence, age, limited life expectancy, and use of other
medications.


1
3
5
7
9
11
13
15
6 7 8 9 10 11 12
Eye disease
Kidney disease
Nerve damage
HbA1c
Relative Risk of
Complications
Skyler, J: Endo Met Cl N Am, vol 25, 2, p.243- 254, June 1996 Adapted from DCCT Research Group: NEJM 1993;329:977-986Minshall M, et al. Clin Ther. 2005;27:940–950.
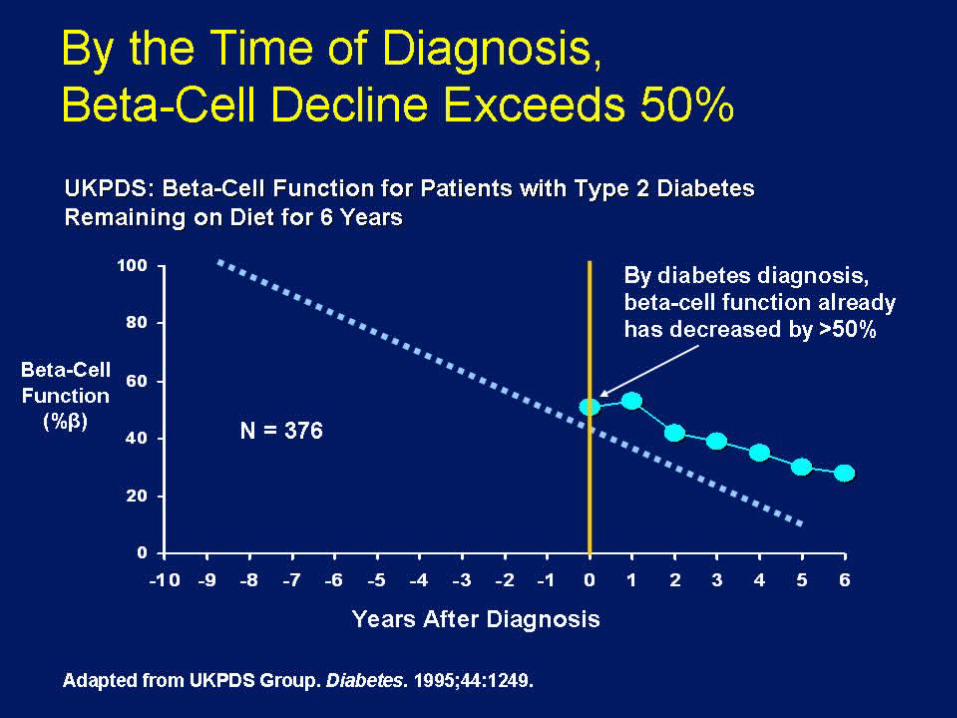
DCCT ResultsHbA1c and Relative Risk of Diabetic Complications
6.5*
Average US HbA1c
Range 7.8-8.6%
Average US HbA1c
Range 7.8-8.6%
AACE recommendatio
n is 6.5%
AACE recommendatio
n is 6.5%
Most patients Most patients with T2DM with T2DM will will
eventually eventually require insulin require insulin
therapytherapy

What are some of the obstaclesWhat are some of the obstacles??• Delayed diagnosis of diabetes Delay in starting Delayed diagnosis of diabetes Delay in starting
insulin in patients failing oral agentsinsulin in patients failing oral agents
• Weight gain with intensification of glycemic Weight gain with intensification of glycemic controlcontrol
• Hypoglycemia with intensification of glycemic Hypoglycemia with intensification of glycemic controlcontrol
• Patient and provider resistance to starting insulin as Patient and provider resistance to starting insulin as well as clinical inertiawell as clinical inertia
• Inappropriate managed care practices Inappropriate managed care practices

DinnerBreakfast Lunch
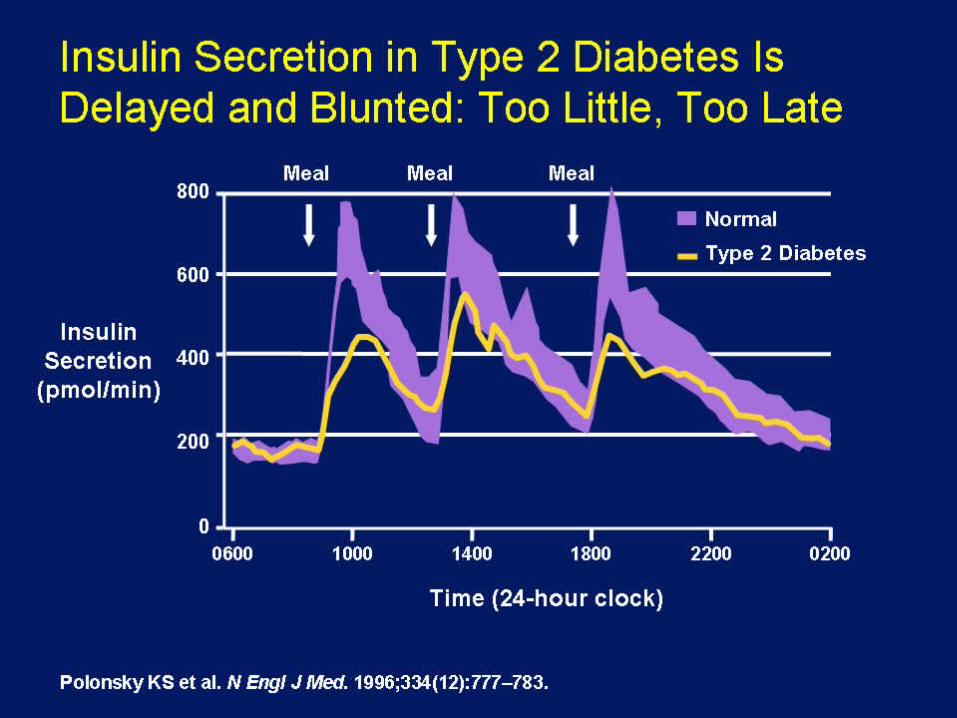
Polonsky. N Engl J Med. 1996;334:777-783.
Time of day
Serum insulin
Insu
lin
(m
U/L
)
70
12:00PM
3:00PM
6:00PM
9:00PM
12:00AM
3:00AM
6:00AM
9:00AM
10
30
50
0
Normal Insulin Secretion

Natural History of Type 2 DiabetesNatural History of Type 2 Diabetes
Insulin ResistanceInsulin Resistance
Hepatic Glucose Hepatic Glucose ProductionProduction
Endogenous InsulinEndogenous Insulin
Postprandial Blood GlucosePostprandial Blood Glucose
Fasting Blood GlucoseFasting Blood Glucose
Typical Diagnosis of DiabetesTypical Diagnosis of Diabetes
Microvascular ComplicationsMicrovascular Complications
Macrovascular ComplicationsMacrovascular Complications
Severity of DiabetesSeverity of Diabetes
Impaired Glucose ToleranceImpaired Glucose Tolerance Frank DiabetesFrank Diabetes
Years Years to to
DecadeDecadess
TimeTime
Ramlo-Halsted and Edelman: Clinics of NA Vol. 26 P771, 1999
AsymptomaticStage
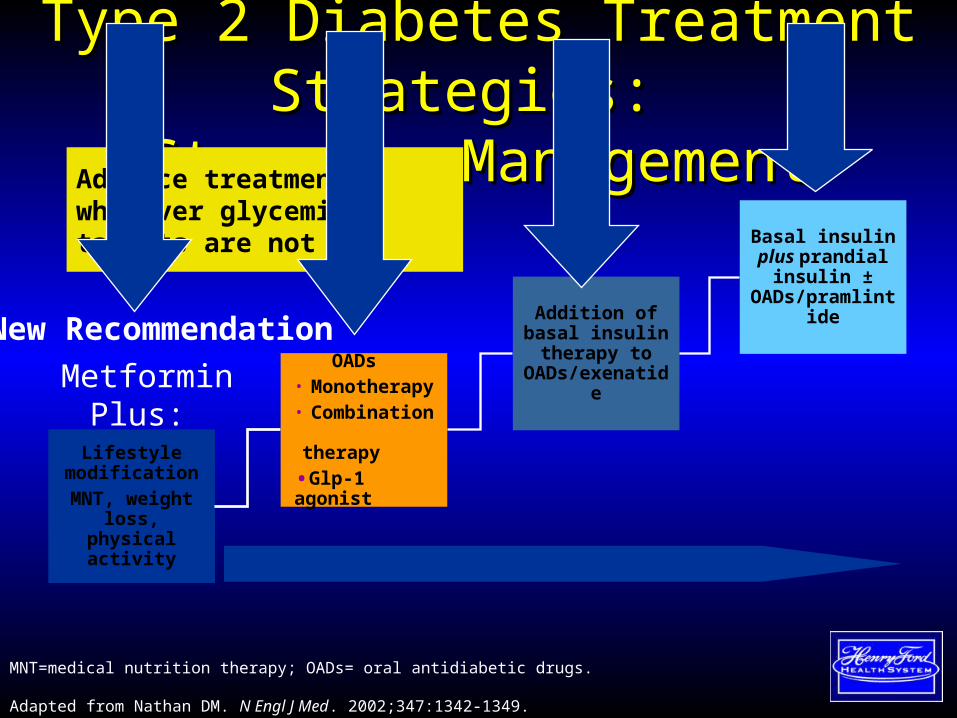
Type 2 Diabetes Treatment Strategies: Type 2 Diabetes Treatment Strategies: Stepwise ManagementStepwise Management
Lifestyle modificationMNT, weight
loss, physical activity
OADs• Monotherapy• Combination therapy
•Glp-1 agonist
Addition of basal insulin
therapy to OADs/exenatide
Basal insulin plus prandial
insulin ±OADs/pramlintid
e
MNT=medical nutrition therapy; OADs= oral antidiabetic drugs.
Adapted from Nathan DM. N Engl J Med. 2002;347:1342-1349.
Advance treatment whenever glycemic targets are not met
MetforminPlus:
New Recommendation
The Case For Insulin

Indications for Insulin in Indications for Insulin in T2DMT2DM
• Symptomatic Hyperglycemia Symptomatic Hyperglycemia
– BG > 250 mg/dL)BG > 250 mg/dL)
• Inadequate glycemic control Inadequate glycemic control ((patient specific (Apatient specific (A1c >7%)1c >7%)
• Oral agents cannot be Oral agents cannot be tolerated/contraindicatedtolerated/contraindicated
• Longstanding Type 2 Diabetes/not Longstanding Type 2 Diabetes/not responding to oral medsresponding to oral meds
• Transient poor controlTransient poor control
– Intercurrent illnessIntercurrent illness
– Glucocorticoid therapyGlucocorticoid therapy

Goals of Insulin TherapyGoals of Insulin Therapy
• HbA1c < 7% (patient specific)HbA1c < 7% (patient specific)– Fasting and pre-prandial: 70 – 130 mg/dLFasting and pre-prandial: 70 – 130 mg/dL– 2 hr after start of meal: < 180 mg/dL2 hr after start of meal: < 180 mg/dL
• Avoid frequent or severe hypoglycemia with Avoid frequent or severe hypoglycemia with physiologicphysiologic insulin replacement therapies insulin replacement therapies
• Minimize weight gainMinimize weight gain
• A1c goal must be customized for the individual patient, with consideration of numerous factors such as comorbid conditions, duration of diabetes, history of hypoglycemia, hypoglycemia unawareness, patient education, motivation, adherence, age, limited life expectancy, and use of other medications.

Mimicking Nature With Insulin Mimicking Nature With Insulin TherapyTherapy
Basal/Bolus ConceptBasal/Bolus ConceptPhysiologic Insulin Secretion
Insu
lin
(
AM PM
Suppresses glucose production between meals and overnight
Nearly constant levels
50% of daily needs
Basal glucose
50
24-hr profile
Basal insulin
Adapted with permission from Bergenstal RM et al. In: DeGroot LJ, Jameson JL, eds. Endocrinology. 4th ed. Philadelphia, Pa: WB Saunders Co.; 2001:821
0
25
Insu
lin
(uU
/mL)
B L D
0
50
100
150
Glu
cose
(mg/d
L)

TYPES OF INSULINTYPES OF INSULIN AND AND
HOW THEY WORKHOW THEY WORK
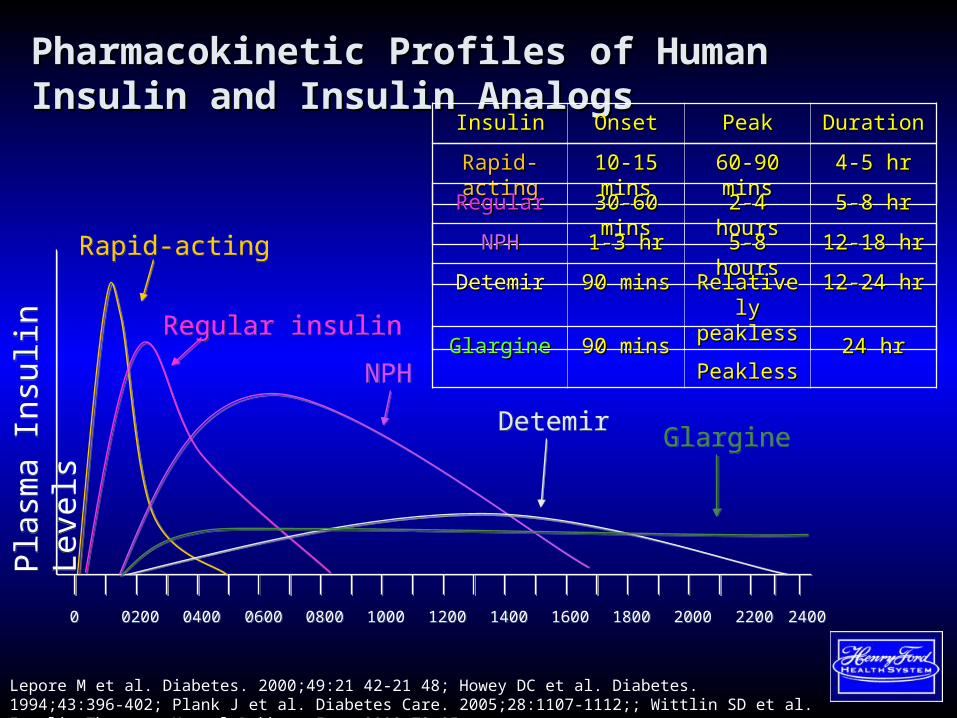
Pharmacokinetic Profiles of Human Insulin and Pharmacokinetic Profiles of Human Insulin and Insulin AnalogsInsulin Analogs
Pla
sma
Insu
lin
Leve
lsP
lasm
a In
sulin
Le
vels
00 02000200 04000400 06000600 08000800 10001000 12001200 14001400 16001600 18001800 20002000 22002200 24002400
Rapid-actingRapid-acting
Regular insulinRegular insulin
NPHNPH
DetemirDetemir
Lepore M et al. Diabetes. 2000;49:21 42-21 48; Howey DC et al. Diabetes. 1994;43:396-402; Plank J et al. Diabetes Care. 2005;28:1107-1112;; Wittlin SD et al. Insulin Therapy. Marcel Dekker, Inc.;2002:73-85.
GlargineGlargine
InsulinInsulin OnsetOnset PeakPeak DurationDuration
Rapid-actingRapid-acting 10-15 mins10-15 mins 60-90 mins60-90 mins 4-5 hr4-5 hr
RegularRegular 30-60 mins30-60 mins 2-4 hours2-4 hours 5-8 hr5-8 hr
NPHNPH 1-3 hr1-3 hr 5-8 hours5-8 hours 12-18 hr12-18 hr
DetemirDetemir 90 mins90 mins Relatively Relatively peaklesspeakless
12-24 hr12-24 hr
GlargineGlargine 90 mins90 mins PeaklessPeakless 24 hr24 hr
BASAL BASAL INSULININSULINIntermediate ActingIntermediate Acting
NPHNPH
Long-Acting AnalogsLong-Acting Analogs
Glargine (Lantus)Glargine (Lantus)
Detemir (Levemir)Detemir (Levemir)
NPH InsulinNPH Insulin
• Human Insulin Isophane Human Insulin Isophane SuspensionSuspension
• PharmacokineticsPharmacokinetics– Onset: 2 - 4 hourOnset: 2 - 4 hour– Peak: 4 - 10 hoursPeak: 4 - 10 hours– Duration: 10 - 16 hoursDuration: 10 - 16 hours– 40% variance!!40% variance!!– Can be mixed with Regular and Rapid Can be mixed with Regular and Rapid
Acting insulinActing insulin

Insulin Glargine (Lantus)Insulin Glargine (Lantus)• Recombinant human insulin analog Recombinant human insulin analog • PharmacokineticsPharmacokinetics
– Onset: 2 - 4 hourOnset: 2 - 4 hour– Peak: PeaklessPeak: Peakless– Duration: 24 hoursDuration: 24 hours
• Administration:Administration:– Once Daily at anytime of dayOnce Daily at anytime of day– When converting from once daily When converting from once daily
NPH, same dose used.NPH, same dose used.– When converting from twice daily When converting from twice daily
NPH, start with 20% lessNPH, start with 20% less

Insulin Detemir (Levemir)Insulin Detemir (Levemir)• Recombinant human insulin analog Recombinant human insulin analog • PharmacokineticsPharmacokinetics
– Onset: 2 - 4 hourOnset: 2 - 4 hour– Peak: PeaklessPeak: Peakless– Duration: 12 hoursDuration: 12 hours
• Administration:Administration:– Once or Twice Daily Once or Twice Daily – Same dose as once daily NPHSame dose as once daily NPH– 20% less than twice daily NPH20% less than twice daily NPH– May actually require more detemir than May actually require more detemir than
glargineglargine
• Shown to be associated with weight Shown to be associated with weight loss/less weight gain than other insulinloss/less weight gain than other insulin

Insulin glargine (Lantus)Insulin glargine (Lantus)Insulin detemir (Levemir)Insulin detemir (Levemir)
• Similar rates of absorption from Similar rates of absorption from abdominal, thigh and deltoid regionabdominal, thigh and deltoid region
• Cannot be mixed with any other form Cannot be mixed with any other form of insulin or IV solutionof insulin or IV solution
• Incidence of nocturnal and severe Incidence of nocturnal and severe hypoglycemia were less frequent hypoglycemia were less frequent compared to once-daily NPH insulincompared to once-daily NPH insulin
• CLEAR solutionCLEAR solution• Available in Pen DeviceAvailable in Pen Device
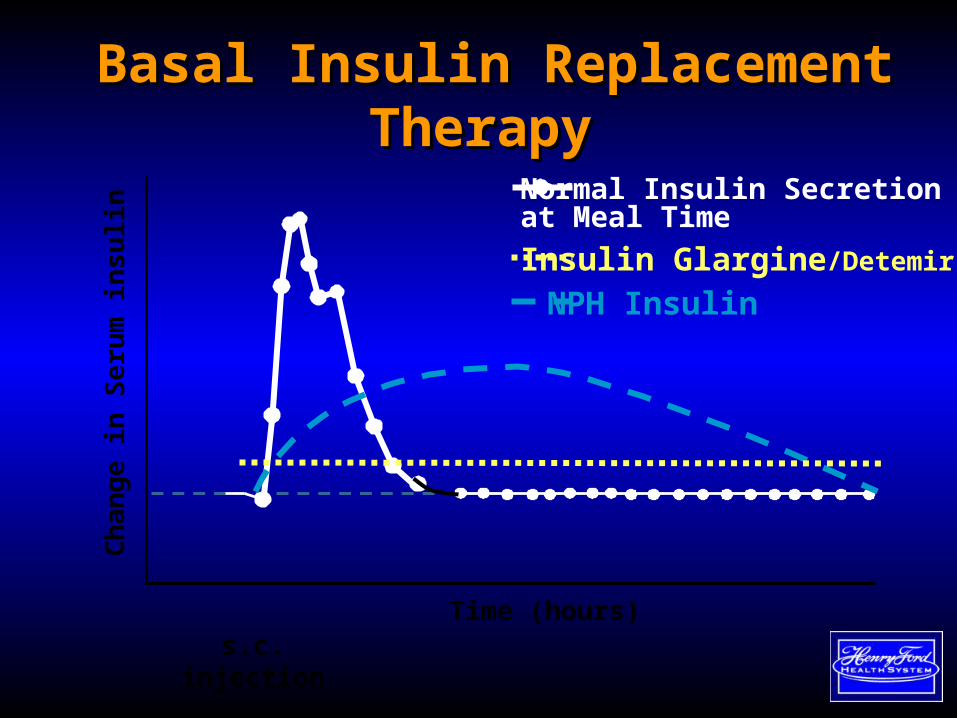
Basal Insulin Replacement Basal Insulin Replacement TherapyTherapy
Time (hours)s.c. injection
Normal Insulin Secretion at Meal Time
Ch
an
ge
in S
eru
m in
su
lin
NPH Insulin
Insulin Glargine/Detemir
25
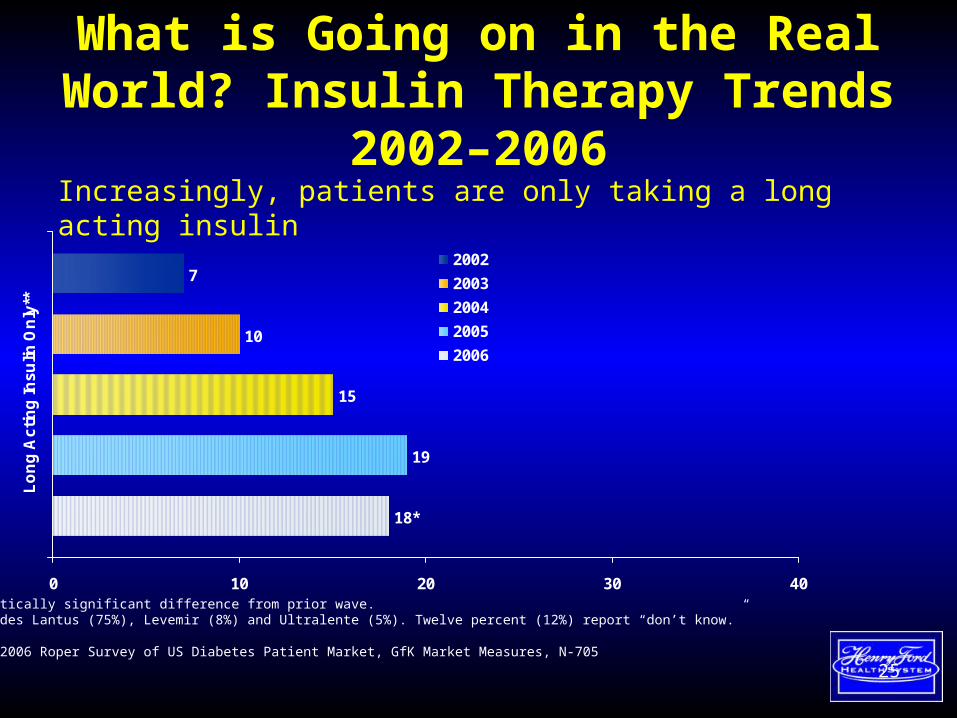
What is Going on in the Real World? Insulin Therapy Trends 2002–2006
Increasingly, patients are only taking a long acting insulin
* Statistically significant difference from prior wave.** Includes Lantus (75%), Levemir (8%) and Ultralente (5%). Twelve percent (12%) report “don’t know.”
Source: 2006 Roper Survey of US Diabetes Patient Market, GfK Market Measures, N-705
19
15
10
7
18*
0 10 20 30 40
Lo
ng
Ac
tin
g In
su
lin O
nly
**
2002
2003
2004
2005
2006
BOLUS BOLUS INSULININSULINShort ActingShort Acting
RegularRegular
Rapid- Acting AnalogsRapid- Acting Analogs
Aspart (Novolog)Aspart (Novolog)
Lispro (Humalog)Lispro (Humalog)
Glulisine (ApidraGlulisine (Apidra))
Regular InsulinRegular Insulin• Human Insulin (soluble)Human Insulin (soluble)• PharmacokineticsPharmacokinetics
– Onset: 0.5 - 1 hourOnset: 0.5 - 1 hour– Peak: 2 - 3 hoursPeak: 2 - 3 hours– Duration: 3 - 6 hours (as long as 8 Duration: 3 - 6 hours (as long as 8
hours)hours)
• Administration:Administration:– 30 - 45 minutes BEFORE meals30 - 45 minutes BEFORE meals– Can be mixed with NPH insulinCan be mixed with NPH insulin– Only insulin that can be given IVOnly insulin that can be given IV
Rapid-Acting Insulin AnalogsRapid-Acting Insulin Analogs
• Equipotent to Regular InsulinEquipotent to Regular Insulin• ProductsProducts
– Lispro (Humalog)Lispro (Humalog)– Aspart (NovoLog)Aspart (NovoLog)– Glulisine (Apidra)Glulisine (Apidra)
• Goal: to mimic physiological prandial Goal: to mimic physiological prandial responseresponse

Rapid-Acting Insulin AnalogsRapid-Acting Insulin Analogs
• PharmacokineticsPharmacokinetics– Onset: < 0.25 – 0.5 hourOnset: < 0.25 – 0.5 hour– Peak: 0.5 – 1 hour (lispro 2.5 hour)Peak: 0.5 – 1 hour (lispro 2.5 hour)– Duration: 1 - 3 hours (lispro 3 - 4 Duration: 1 - 3 hours (lispro 3 - 4
hours)hours)
• Administration:Administration:– Within 15 minutes BEFORE mealsWithin 15 minutes BEFORE meals– Can be mixed with NPH insulinCan be mixed with NPH insulin

Bolus Insulin Replacement Bolus Insulin Replacement Therapy Therapy
Time (hours)s.c. injection
Normal Insulin Secretion at Meal Time
Ch
an
ge
in S
eru
m in
su
lin
Rapid-acting Analogue
Regular insulin
Apidra
Humalog
Novolog

32
Why is Mealtime Control Important?
• 99% of patients with A1Cs ≥7% have 2-hour postprandial glucose (PPG) levels ≥200 mg/dL2
1. Polonsky KS, et al. N Engl J Med. 1988;318(19):1231-1239. 2. Erlinger TP, et al. Diabetes Care. 2001;24(10):1734-1738.
Pla
sma
Glu
cose
(m
g/d
L)2
400
200
100
0
300
Breakfast Lunch Dinner
6 AM 6 AM10 AM 2 PM 6 PM 10 PM 2 AM
Time of Day
Control
Type 2 diabetes
Patients with poorly controlled type 2 diabetes may spend much of their waking day with postprandial hyperglycemia1
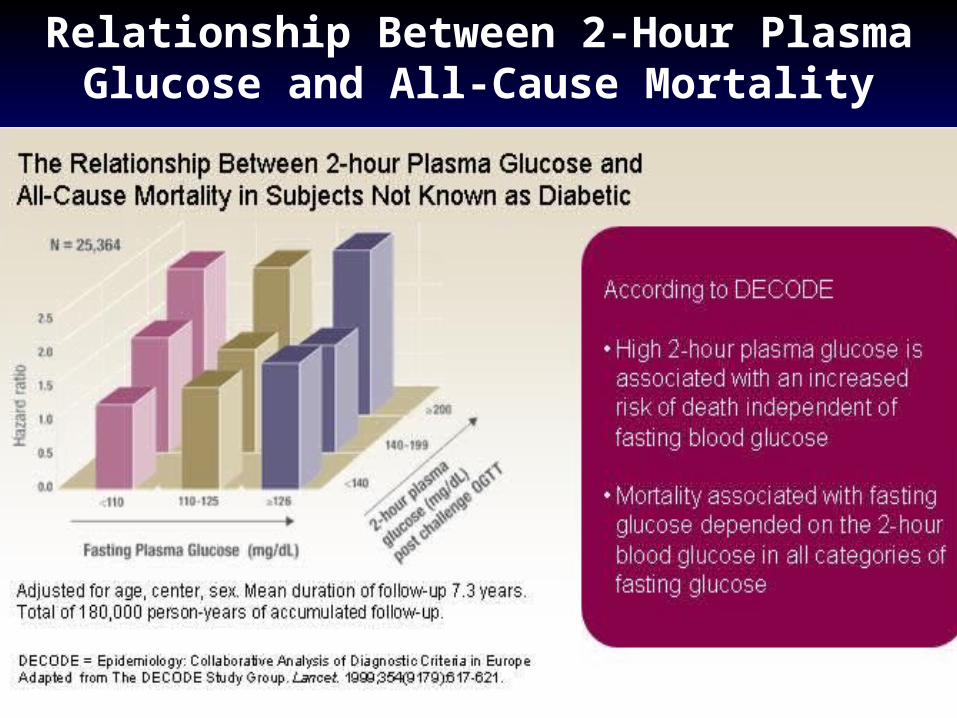
Relationship Between 2-Hour Plasma Glucose and All-Cause Mortality
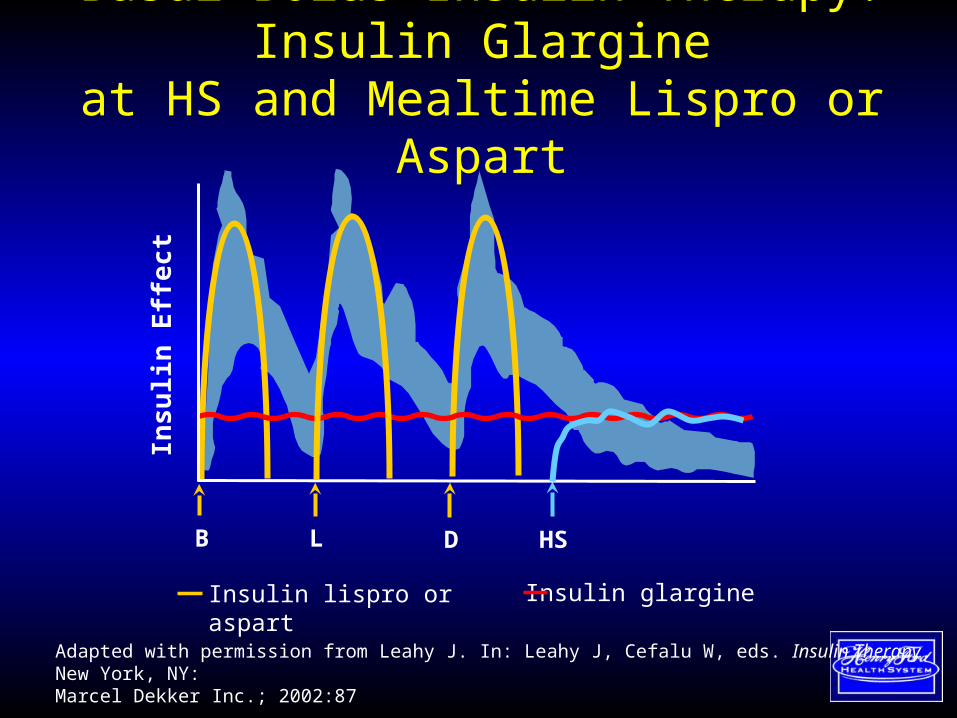
Insulin lispro or aspart Insulin glargine
Basal-Bolus Insulin Therapy: Insulin Glargine
at HS and Mealtime Lispro or Aspart
B DL HS
Insu
lin E
ffe
ct
Adapted with permission from Leahy J. In: Leahy J, Cefalu W, eds. Insulin Therapy. New York, NY: Marcel Dekker Inc.; 2002:87

Premixed InsulinPremixed InsulinHUMAN HUMAN
• 70/30 70/30 – 70% NPH70% NPH– 30% REG 30% REG
• 50/5050/50– 50% NPH50% NPH– 50% REG 50% REG
• Dual Peak Dual Peak
• Administration:Administration:– Must be injected 30 - 45 minutes before a Must be injected 30 - 45 minutes before a
mealmeal– Once or twice daily dosingOnce or twice daily dosing
Premixed InsulinPremixed InsulinHUMAN HUMAN
• Advantages:Advantages:– ConvenienceConvenience– Accuracy Accuracy
• visually impaired visually impaired • Manual dexterity challengesManual dexterity challenges
• Disadvantages:Disadvantages:– Inability to adjust only one componentInability to adjust only one component– Nocturnal Hypoglycemia Nocturnal Hypoglycemia – MUST eat CONSISTENTLY timed mealsMUST eat CONSISTENTLY timed meals

Premixed InsulinPremixed InsulinANALOG ANALOG
• 70/30 MIX (Novolog)70/30 MIX (Novolog)– 70% Aspart protamine70% Aspart protamine– 30% Aspart 30% Aspart
• 75/25 (Humalog)75/25 (Humalog)– 75% Lispro protamine75% Lispro protamine– 25% Lispro25% Lispro
• One Peak followed by "long Tail” (No NPH) One Peak followed by "long Tail” (No NPH)
• Administration:Administration:– Must be injected within 15 minutes before a Must be injected within 15 minutes before a
mealmeal– Once, twice or three times daily dosingOnce, twice or three times daily dosing
Premixed InsulinPremixed InsulinANALOG ANALOG
• Advantages:Advantages:– ConvenienceConvenience– Accuracy Accuracy
• visually impaired visually impaired • Manual dexterity challengesManual dexterity challenges
– Flexibility with mealsFlexibility with meals– Less Nocturnal HypoglycemiaLess Nocturnal Hypoglycemia
• Disadvantages:Disadvantages:– Inability to adjust only one componentInability to adjust only one component
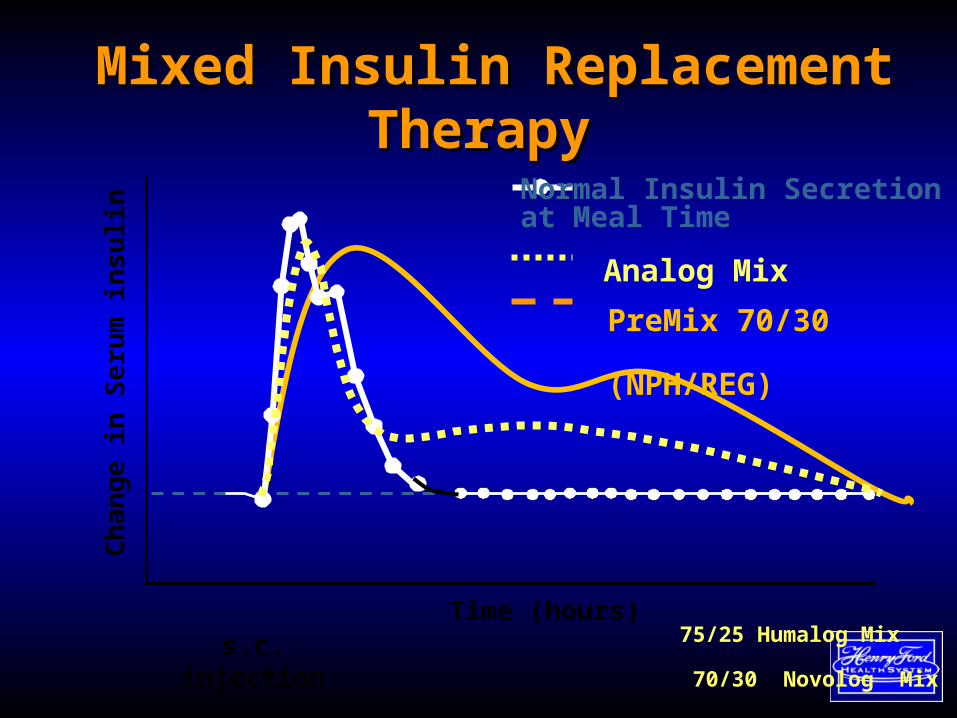
Mixed Insulin Replacement Mixed Insulin Replacement TherapyTherapy
Time (hours)s.c. injection
Normal Insulin Secretion at Meal Time
Ch
an
ge
in S
eru
m in
su
lin
Analog Mix
75/25 Humalog Mix
70/30 Novolog Mix
PreMix 70/30
(NPH/REG)

Now What ?
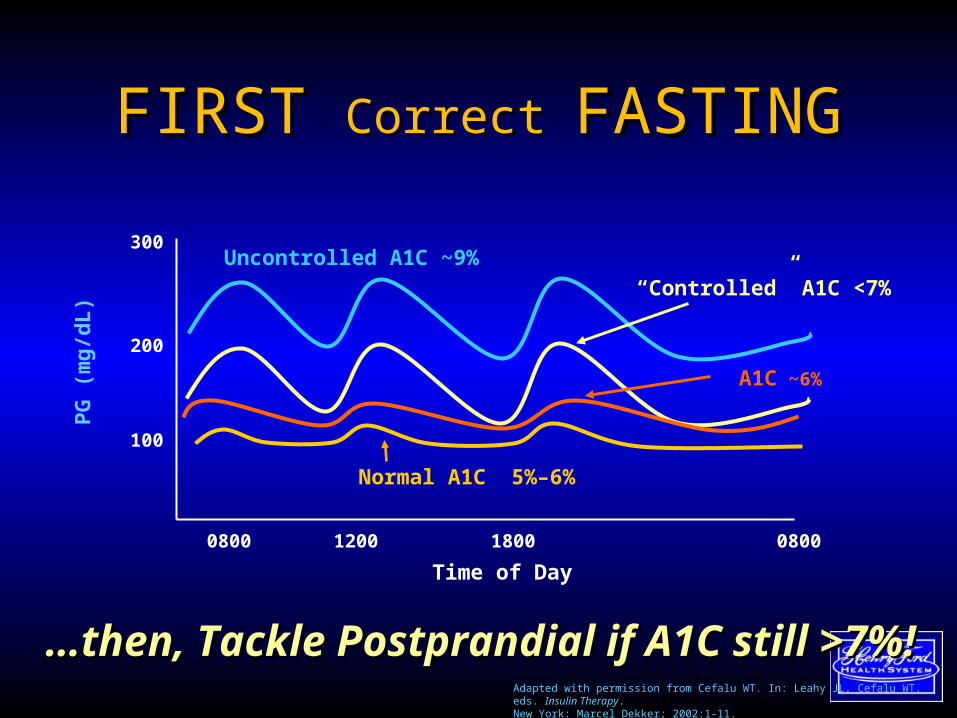
FIRST FIRST Correct Correct FASTINGFASTING
……then, Tackle Postprandial if A1C still >7%!then, Tackle Postprandial if A1C still >7%!
100
200
300
Normal A1C 5%–6%
PG
(m
g/d
L)
0800 1200 1800 0800
Time of Day
Uncontrolled A1C ~9%
A1C ~6%
“Controlled” A1C <7%
Adapted with permission from Cefalu WT. In: Leahy JL, Cefalu WT, eds. Insulin Therapy. New York: Marcel Dekker; 2002:1-11.

Possible Approaches for Adding InsulinPossible Approaches for Adding Insulin
• using a basal insulin with continued oral using a basal insulin with continued oral agentsagents
• using pre-mixed insulin with continued using pre-mixed insulin with continued oral agents oral agents
• stopping oral agents and initiating insulin stopping oral agents and initiating insulin using various regimens:using various regimens:• pre-mixed insulin pre-mixed insulin • prandial insulin with a basal insulin once (or prandial insulin with a basal insulin once (or
twice) dailytwice) daily
Start a Basal Insulin“Treat to Target”
• Continue oral agent(s) at same dosage – Do NOT stop insulin secreting agent
• Add single, evening insulin dose (0.1 - 0.2 U/kg)– 10 - 20 units– Glargine, Detemir or NPH (bedtime)
Increase insulin dose every 3-4 days as needed– Increase 3 - 5 U if FBG >150 mg/dL
– Increase 1 - 2 U if FBG = >110,<150 mg/dL • Treat to target FBG (usually <120 mg/dL)
6-596-59
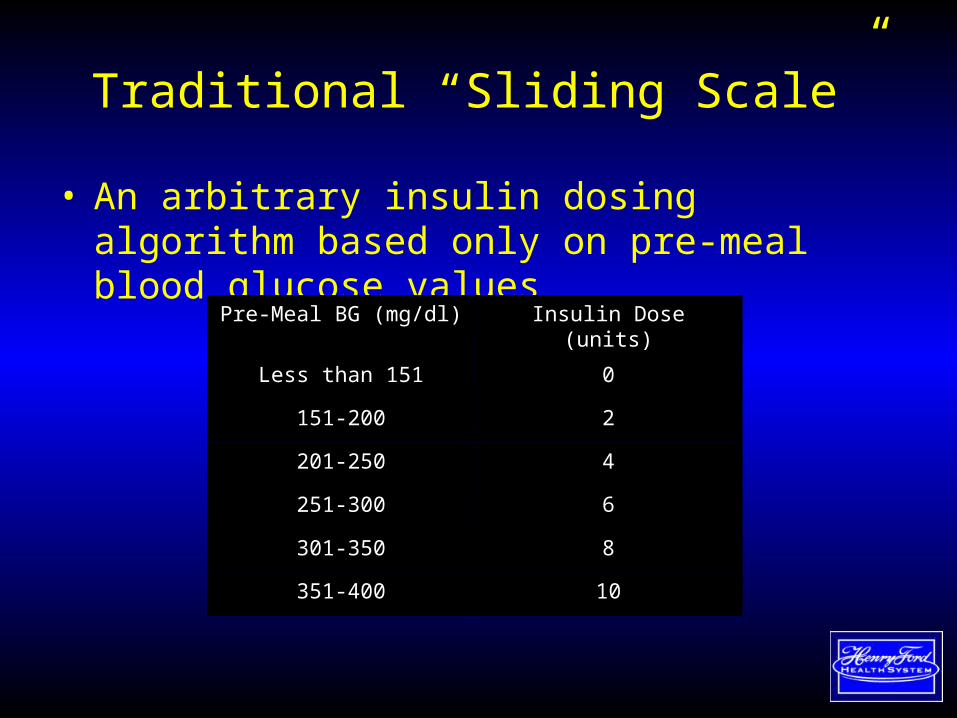
Traditional “Sliding Scale”
• An arbitrary insulin dosing algorithm based only on pre-meal blood glucose values
Pre-Meal BG (mg/dl) Insulin Dose (units)
Less than 151 0
151-200 2
201-250 4
251-300 6
301-350 8
351-400 10

Traditional “Sliding Scale”
Breakfast Lunch Dinner Bedtime
Day 1 BG (mg/dl) 141 335 89 290
Insulin Dose 0 8 0 6
Day 2 BG (mg/dl) 381 76 261 121
Insulin Dose 8 0 6 0
Day 3 BG >600

Adding a meal time bolus:Only Fasting BGs at target
• Stop insulin secreting agent• Add Bolus insulin before meals (REG or analog)• Isocaloric meals
– Add 10 units and redistribute total dose 50/50• Pt taking 30 units Lantus already• Add 10 units to a new total dose of 40 units• 50% will be new basal (20 units)• 50% in divided doses will be the meal time bolus (i.e. 7/6/7)
• Carb counting and correction factors• BG checks a must! “blind leading the
blind”• SAFETY
Total Daily Insulin
• Total daily insulin requirement is calculated by body weight– T1: need about 0.6 units/kg (range 0.4 -
0.8)– T2: need about 1.2 units/kg (range 1 –
1.4)• BGs at goal without hypoglycemia.• 40-50% basal (background)• 50-60% bolus (meal doses)

Calculating “Basal–Bolus” Insulin
• Calculate TDD– T1: need about 0.6 units/kg (range 0.4-
0.8)– T2: need about 1.2 units/kg (range 1 –
1.4)• Basal dose: 40 – 50% of TDD• Bolus dose: 50-60% of TDD:
– Divide equally for three meals OR– Sensitivity Factor = 1700/TDD
• 1 unit will drop BG by XX points
– Carbohydrate Ratio = 500/TDD • 1 unit for every XX gm carbs
• (Pt BG – target) / (SF) = CORRECTION• Now add carb ratio for meal.
For Example
• 250 pound T2DM (114 kg) • Calculated TDD: 114 x 1.2 = 137 u/day• Basal Dose: 68 units a day (50% of TDD)• Bolus Dose: (other 50% of TDD)
– Isocaloric meals: • 68/3 = 23 units before each meal
– Carbohydrate ratio: 500/137 = 3• 1 unit for every 3 grams of carbs
– Insulin Sensitivity: 1700/137 = 12• 1 unit will lower BG 12 mg/dL

For Example:Above Target at Lunch
• Pre meal target: 100• Pt BG before lunch: 160• Will be eating a meal of 65 gm CHO• 160 – 100 = 60 points too HIGH before eating• Sensitivity Factor = 12
– 60/12 = 5 (will need 5 units to correct to target)
• Carb ratio = 1 : 3– 65 gm CHO / 3 = 21 (will need 21 units for the meal)
5 units +21 units = 26 units before lunch
For Another Example:Below Target at Lunch
• Pre meal target: 100• Pt BG before lunch: 80• Will be eating a meal of 65 gm CHO• 80 - 100 = - 20 points too LOW before eating• Sensitivity Factor = 12
– -20/12 = -1.6 >> -2 (will need -2 units to correct to target)
• Carb ratio = 1 : 3– 65 gm CHO / 3 = 21 (will need 21 units for the meal)
21 units – 2 units = 19 units before lunch
Sliding scale: CorrectionSliding scale: Correction
• Correction Scales:Correction Scales:– Helpful for sick days/NPOHelpful for sick days/NPO– Still need to calculate the TDD and the insulin Still need to calculate the TDD and the insulin
sensitivitysensitivity– Example: TDD = 137; SF 1:12Example: TDD = 137; SF 1:12– WILL NOT COVER FOR CARBS, ONLY TO WILL NOT COVER FOR CARBS, ONLY TO
CORRECTCORRECT• <100-125, no insulin<100-125, no insulin• 126 - 150, 2 units 126 - 150, 2 units (102-126)(102-126)• 151 - 175, 4 units 151 - 175, 4 units (103-127)(103-127)• 176 - 200, 6 units 176 - 200, 6 units (104-128)(104-128)• 201 - 225, 8 units 201 - 225, 8 units (105-129)(105-129)• 226-250, 10 units, etc 226-250, 10 units, etc (106-130)(106-130)
Sliding scale: Correction + Sliding scale: Correction + CarbsCarbs• Incorporates BOTH the correction and the Incorporates BOTH the correction and the
meal requirementsmeal requirements– Still need to calculate the TDD, sensitivity factor, and Still need to calculate the TDD, sensitivity factor, and
carbohydrate ratio carbohydrate ratio – Works best for consistent carb intake (may have Works best for consistent carb intake (may have
different scale for each meal)different scale for each meal)
• Example: TDD = 137 unitsExample: TDD = 137 units– SF = 1:12SF = 1:12– CR = 1:3CR = 1:3– Eats approx 65 gm carbs at each mealEats approx 65 gm carbs at each meal
• <70, no insulin<70, no insulin• 71 – 125, 21 units71 – 125, 21 units• 126 - 150, 23 units126 - 150, 23 units• 151 - 175, 25 units151 - 175, 25 units• 176 - 200, 27 units176 - 200, 27 units• 201 - 225, 29 units201 - 225, 29 units• 226 - 250, 31 units226 - 250, 31 units
What’s the dose range?
• Type 2: 0.3 to 1.2 units/kg – “Thin type 2’s” are more insulin deficient
– “Heavy type 2’s” are more insulin resistant
– Most pts with T2DM need insulin doses of
1 to 1.2 units/kg to achieve an A1c <7%
(basal dose of 0.5 to 0.6 units/kg per day)

• Convenient• Discreet• Protect Insulin
from light, heat and
agitation
NovoNordisk: NovoPen 3
Sanofi-Aventis: SoloStar
Lilly Pens: Memoir & KwikpenInsulin PensInsulin Pens

U-500 Insulin

History: Why U-500?
• Main reason in early 1950s was for high insulin requirements in type 1 diabetes due to high levels of insulin antibodies developed from other animal insulins– Also used for severely insulin resistant type 2’s– Only developed as a regular insulin
• Replaced by pork U-500 regular insulin in 1980• Replaced by human U-500 regular insulin in
1997

What About the Need for More CONCENTRATED Insulins?
• For more resistant patients, U-100 insulin both impractical and inconvenient– When over 100 units (1mL) required at one time,
would need more than one injection– Large volume of insulin painful– Large depot of insulin impedes absorption making
it unpredictable (a more concentrated insulin should be more predictable at these doses)
Insulin Resistant Conditions to Consider U-500 Insulin
• Non-Syndromic Insulin Resistance– Obesity with T2DM requiring > 200 u/day– Post-op or post-transplant state– High-dose steroids or pressors– Systemic infection– Pregnancy with underlying T2DM

Most Recent PK/PD U-500 Data
• Duration of action was shown to be prolonged for U-500 vs. U-100; mean late tRmax50 was 3.4 hr longer than at the 100-U dose (p<0.001)
• The longer duration of effect of U-500 compared to U-100 suggests that multiple daily injections of U-500 without use of a basal insulin may be a plausible treatment option for insulin-resistant patients with type 2 diabetes
So Is U-500 Regular Insulin a Basal or a Prandial Insulin?
• It is BOTH!
• Lag times never studied, but it only makes sense that when used as mealtime insulin timing between injection and eating is even more important than with U-100 regular (or analogue)
• Main secret for success with U-500 insulin– FREQUENT SMBG!

Communicating U-500 Dosing
• Two ways: “units” on a U-100 insulin syringe or volume (mL) on a tuberculin syringe
• Ideally, would be nice if everyone used both; most patients will discuss this in units
• My compromise with patients and in charting: always note U-500.
Example
• Patient is taking 10 units of U-500 insulin at breakfast (the equivalent of 50 units of U-100 regular) and it is decided to increase the dose to 14 units U-500– I tell the patient to increase the dose to 14 units U-
500 in his U-100 syringe– I chart the dose was increased to 14 units of U-500
(which is 70 units of U-100 regular)

Example• This can also be done in tuberculin syringes and
only discussed in terms of volume of insulin
• Problem: in the US tuberculin syringes only available in 27G needles
• So 10 units of U-500 insulin would be 0.10 mL of insulin
• An increase to 14 units would be 0.14 mL of insulin
• My observation: patients and nurses prefer “units”

Implementing U-500 Insulin
• 150-300 units/day– U-500 has been shown effective with or without
traditional basal insulin– Without basal insulin, U-500 can be split into ac
breakfast and dinner shots (60/40) or ac TID (40/30/30 or 40/35/20)
– Many continue basal insulin, esp. during transition from U-100
Like most insulin management, what we do with U-500 is
generally anecdotal. The good news: these patients don’t
generally get hypoglycemic!
Injection ProblemsInjection Problems• Lipoatrophy (immune response)Lipoatrophy (immune response)
– Breakdown (pitting) of fat tissueBreakdown (pitting) of fat tissue
– Indentation in the skinIndentation in the skin
• LipohypertrophyLipohypertrophy– Thickening (lumps) of SQ fatThickening (lumps) of SQ fat
– Causes: repeated injections same site, Causes: repeated injections same site, needle reuseneedle reuse
– Delays insulin absorptionDelays insulin absorption
• Bruising at Site: Bruising at Site: technique technique
Insulin Delivery SystemsInsulin Delivery Systems• Insulin syringesInsulin syringes
– Know Needle Gauges (29-32), LengthsKnow Needle Gauges (29-32), Lengths– Short Needle: 8mm, Longer: 12.7mmShort Needle: 8mm, Longer: 12.7mm– Syringe size- 1/4ml, 3/10ml, 1/2ml,1mlSyringe size- 1/4ml, 3/10ml, 1/2ml,1ml
• Insulin pens: Nano ® (4mm), mini Insulin pens: Nano ® (4mm), mini (5mm), short (8mm), long (12.7mm) (5mm), short (8mm), long (12.7mm) needlesneedles
• Continuous insulin infusion pumpContinuous insulin infusion pump– Uses bolus insulin onlyUses bolus insulin only
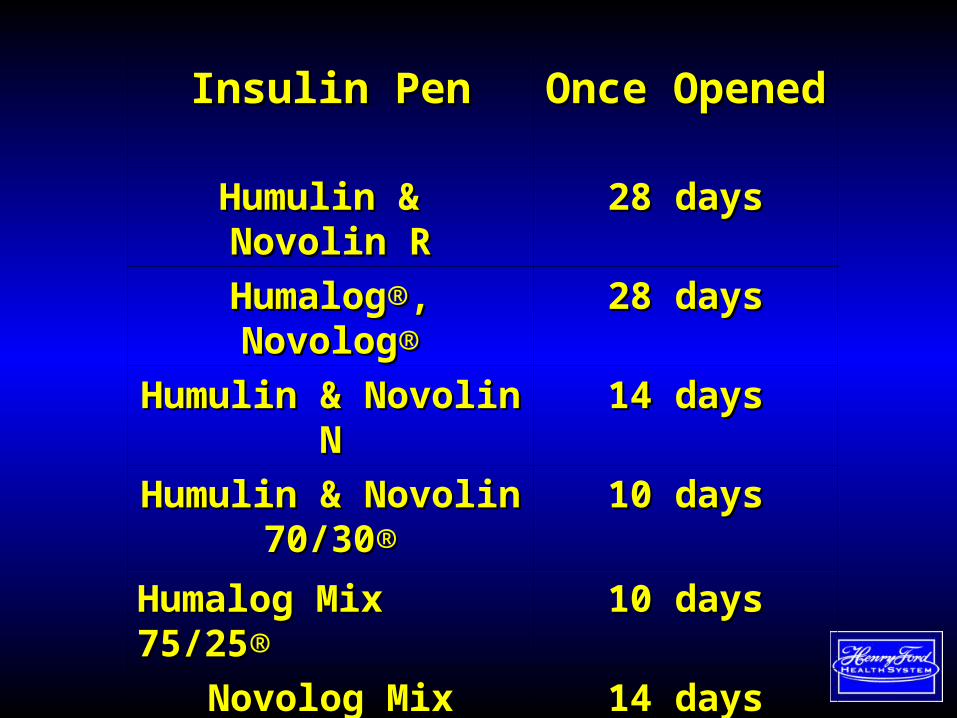
Insulin PenInsulin Pen Once OpenedOnce Opened
Humulin & Novolin RHumulin & Novolin R 28 days28 days
HumalogHumalog®®, Novolog, Novolog®® 28 days28 days
Humulin & Novolin NHumulin & Novolin N 14 days14 days
Humulin & Novolin Humulin & Novolin 70/3070/30®®
10 days10 days
Humalog Mix 75/25Humalog Mix 75/25®® 10 days10 days
Novolog Mix 70/30Novolog Mix 70/30®® 14 days14 days
LevemirLevemir®®LantusLantus®®, Apidra, Apidra®®
42 days42 days28 days28 days

Thank You
• Many individuals freely shared their slides for this presentation:
• Roger Austin• Steve Edleman• Irl Hirsch• Lucia Novak• Jane Seely• Geri Spollet• Virginia Valentine