Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Demographic, clinical, and polysomnographic features in patientswith narcolepsy: an experience of 181 patients with narcolepsyfrom a Turkish sleep center
Murat Erdem • Oguzhan Oz • Adem Balikci •
Mehmet Yucel • Mustafa Alper • Hakan Akgun •
Fuat Ozgen
Received: 1 March 2011 / Accepted: 13 February 2012 / Published online: 2 March 2012
� Belgian Neurological Society 2012
Abstract The present study was designed to describe the
socio-demographic, clinical, and polysomnographic features
of patients diagnosed with narcolepsy in our sleep center. This
retrospective cross-sectional study was conducted on 181
patients diagnosed with narcolepsy based on the results of
clinical evaluation, polysomnography (PSG), and multiple
sleep latency test (MSLT) between 1993 and 2009. Approx-
imately 70% of the patients had cataplexy, whereas 42% had
hallucinations and 55.8% had sleep paralysis. Although
sleep efficiency was higher (91.28 ± 5.89%) in patients
with narcolepsy, they woke frequently during the night, and
their percentages of deep sleep were low (stage 3, 5.12 ±
3.08%, stage 4, 9.60 ± 7.10%). Our study group was divided
into two based on age: individuals aged\30 years (n = 152)
and [30 years (n = 29). REM latency on PSG was shorter
(t = 2.96, p = 0.004) and sleep onset REM (SOREM) on
MSLT was higher (t = 2.56, p = 0.011) in the older group
than in the younger group. Cataplexy is seen in most patients
with narcolepsy. In older patients, REM latency on PSG
is shorter and the number of SOREM on MSLT is higher.
Introduction
Narcolepsy is characterized by irresistible attacks of sleep
under unusual circumstances (for example, while eating,
driving the car, or talking), hypnagogic (vivid) hallucinations
on falling asleep or on waking (hypnopompic hallucinations),
cataplexy (a sudden, usually bilateral loss of muscle tone
provoked by emotional stimuli and which can make the person
fall), sleep paralysis (unpleasant generalized paralysis just
before sleep, while falling asleep, or on waking), and disturbed
nocturnal sleep [1]. The first clinical description of narcolepsy
in the medical literature can be attributed to Sir Thomas
Willis. Yoss and Daly published their criteria for diagnosis of
the narcoleptic syndrome, with a description of the classic
‘‘narcoleptic tetrad’’ comprising the four main symptoms of
narcolepsy: excessive daytime sleepiness, cataplexy, sleep
paralysis, and hypnagogic/hypnopompic hallucinations [2]. In
the next period, biological indicators of narcolepsy were
defined. Vogel has shown the presence of sleep onset rapid eye
movement (SOREM) in these cases, and Honda et al. have
revealed the association of Class II HLA-DR2 antigens with
the disease in 1983 [3]. In studies conducted in the last decade,
cerebrospinal fluid (CSF) hypocretin levels were found to be
lower in more than 90% of the patients with narcolepsy than in
healthy individuals [4–6]. The prevalence of the disease is
around 1/2,000 [7, 8]. The disease is also more common in
men. Typically, narcolepsy starts in the twenties; however,
cases of narcolepsy onset in early childhood or after the age of
60 years have also been reported [6, 9].
In this study, archived patient records from Turkey’s
first sleep disorder center were scanned and examined to
determine socio-demographic, clinical, and polysomno-
graphic features of patients diagnosed with narcolepsy; the
results are discussed in light of the current literature.
Methods
This retrospective study was conducted in the Sleep
Research Center at Gulhane Military Medical Hospital
M. Erdem (&) � A. Balikci � M. Alper � F. Ozgen
Department of Psychiatry, Gulhane Military Medical Academy,
General Tevfik Saglam Street No: 1, 06018 Etlik,
Ankara, Turkey
e-mail: [email protected]
O. Oz � M. Yucel � H. Akgun
Department of Neurology, Gulhane Military Medical Academy,
Etlik, Turkey
123
Acta Neurol Belg (2012) 112:177–181
DOI 10.1007/s13760-012-0053-x

(GMMH), Ankara, Turkey. Most patients admitted to our
center were diagnosed before they enlisted in military
service. To assess whether individuals are fit for military
service, they are evaluated for sleep-related abnormalities.
The results of assessment are then used to determine
qualification for military service. Civilian patients were
also admitted to our center but were present in lower
numbers. Socio-demographic and clinical characteristics
and results of polysomnography (PSG) and multiple sleep
latency test (MSLT) were evaluated at the Sleep Research
Center of the GMMH for 181 patients who were diagnosed
with narcolepsy on the basis of clinical evaluation, PSG,
and MSLT between March 1993 and December 2009.
Patients with abnormal findings in complete blood
count; routine biochemical tests, including kidney and liver
function tests and sedimentation rate; thyroid function
tests; and vitamin B12 levels were excluded from the
study. Patients using sedatives (e.g., benzodiazepines) and
sleep-deprived patients (i.e., sleeping less than 7 h per 24 h
based on sleep diary records) were also excluded. All
patients were evaluated by a psychiatrist to rule out psy-
chiatric disorders. In addition, a neurologist examined the
patients to rule out neurological disorders. Those with
restless legs syndrome (RLS) and obstructive sleep apnea
syndrome (OSAS) were also excluded from the study.
Subjective sleepiness was assessed using the Epsworth
Sleepiness Scale (ESS). The ESS is a specialized, validated
sleep questionnaire containing eight items that ask for self-
reported disclosure of the expectation of dozing in various
situations. The validity and reliability studies of the
Turkish form of the ESS were done by Izci et al. [10].
GRASS Model 78-type analog and Somnostar Alpha Sleep
PSG were used for obtaining sleep records. Consecutive
PSG and MSLT studies were performed on all patients
during diagnosis. Electroencephalogram (EEG), electro-
oculogram (EOG), submental electromyography (EMG),
and electrocardiogram (ECG) data were obtained from
PSG records. With the aim of achieving differential diag-
nosis, during PSG recording, a nasal thermistor was used
for timing respiration, and during EMG recording, leg
electrodes were attached at pre-tibial muscles for assessing
periodic leg movements. Records were scored in 30 second
epochs according to the international criteria [11]. Fol-
lowing PSG, standard MSLTs were performed in accor-
dance with the American Academy of Sleep Medicine
guidelines [12]. Manual analysis of the MSLT data inclu-
ded sleep latency from lights out to first epoch of sleep,
mean latencies to sleep for all naps, and number of
SOREM periods. Four tests (naps) 2 h apart were
performed beginning 2 h after awakening in the morning.
Routine hook-up was carried out after omitting leg EMG
and cardio-respiratory parameters. Sleep was defined as
three consecutive epochs of stage 1 sleep or one epoch of
any other stage of sleep. The test continued for 15 min
after sleep onset to document the presence or absence of
REM sleep. Sleep latency was averaged over all naps and
recorded on the report form. Continuous variables are
given as mean ± standard deviation, and discrete variables
are reported as numbers and percentages in the statistical
analysis.
Results
Men constituted 91.2% of the patients. The high rate of
male patients admitted to our center may be associated
with characteristics of the patient population. The mean
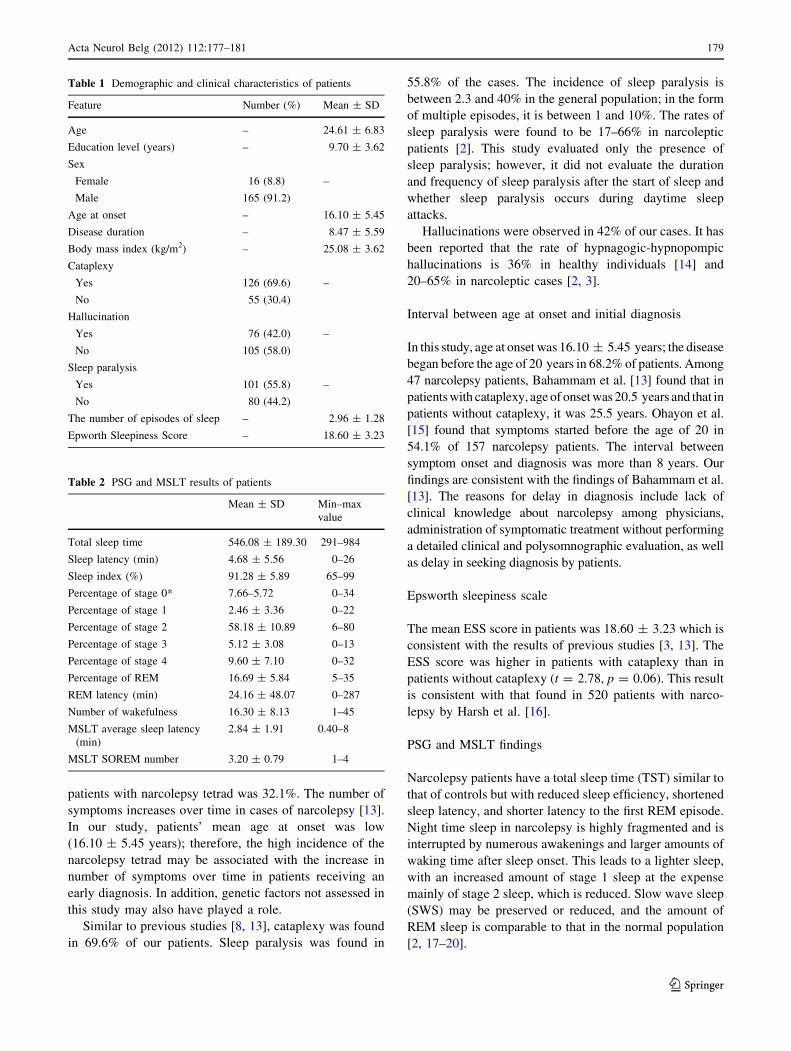
age of patients was 24.61 ± 6.83 years. Of 181 patients,
cataplexy was detected in 126 (69.6%), hallucinations in 76
(42%), and sleep paralysis in 101 patients (55.8%). On an
average, the disease started at the age of 16 years and was
diagnosed approximately 8 years after onset of symptoms.
Socio-demographic and clinical characteristics of all sub-
jects are shown in Table 1.
Polysomnography results showed that the mean sleep
latency and sleep index were 4.68 ± 5.56 min and
91.28 ± 5.89%, respectively. The REM percentage was
16.69 ± 5.84, and REM latency was 24.16 ± 48.07 min.
On MSLT, the SOREM number was detected as
3.20 ± 0.79. PSG and MSLT results of patients are shown
in Table 2.
Our study group was then separated into two groups:
patients aged \30 years (n = 152) and [30 years
(n = 29). REM latency on PSG was shorter (t = 2.96,
p = 0.004) and SOREM on MSLT was higher (t = 2.56,
p = 0.011) in the older group than in the younger group.
Discussion
In this study, socio-demographic, clinical, and polysom-
nographic characteristics were evaluated in patients with
narcolepsy. In summary, the results of the study showed
that 70% of all patients experience cataplexy. Although the
incidence of hallucinations (42%) and sleep paralysis
(56%) was less than that of cataplexy, the incidence of
these two symptoms in the present study is higher than that
reported in the literature [2].
Clinical features
The clinical picture of narcolepsy consists of a tetrad of
symptoms: irresistible attacks of sleep, cataplexy, hypna-
gogic hallucinations, and sleep paralysis. In previous
studies, the proportion of patients with the narcolepsy tet-
rad was 10–27.7% [13]. In our study, the percentage of
178 Acta Neurol Belg (2012) 112:177–181
123
patients with narcolepsy tetrad was 32.1%. The number of
symptoms increases over time in cases of narcolepsy [13].
In our study, patients’ mean age at onset was low
(16.10 ± 5.45 years); therefore, the high incidence of the
narcolepsy tetrad may be associated with the increase in
number of symptoms over time in patients receiving an
early diagnosis. In addition, genetic factors not assessed in
this study may also have played a role.
Similar to previous studies [8, 13], cataplexy was found
in 69.6% of our patients. Sleep paralysis was found in
55.8% of the cases. The incidence of sleep paralysis is
between 2.3 and 40% in the general population; in the form
of multiple episodes, it is between 1 and 10%. The rates of
sleep paralysis were found to be 17–66% in narcoleptic
patients [2]. This study evaluated only the presence of
sleep paralysis; however, it did not evaluate the duration
and frequency of sleep paralysis after the start of sleep and
whether sleep paralysis occurs during daytime sleep
attacks.
Hallucinations were observed in 42% of our cases. It has
been reported that the rate of hypnagogic-hypnopompic
hallucinations is 36% in healthy individuals [14] and
20–65% in narcoleptic cases [2, 3].
Interval between age at onset and initial diagnosis
In this study, age at onset was 16.10 ± 5.45 years; the disease
began before the age of 20 years in 68.2% of patients. Among
47 narcolepsy patients, Bahammam et al. [13] found that in
patients with cataplexy, age of onset was 20.5 years and that in
patients without cataplexy, it was 25.5 years. Ohayon et al.
[15] found that symptoms started before the age of 20 in
54.1% of 157 narcolepsy patients. The interval between
symptom onset and diagnosis was more than 8 years. Our
findings are consistent with the findings of Bahammam et al.
[13]. The reasons for delay in diagnosis include lack of
clinical knowledge about narcolepsy among physicians,
administration of symptomatic treatment without performing
a detailed clinical and polysomnographic evaluation, as well
as delay in seeking diagnosis by patients.
Epsworth sleepiness scale
The mean ESS score in patients was 18.60 ± 3.23 which is
consistent with the results of previous studies [3, 13]. The
ESS score was higher in patients with cataplexy than in
patients without cataplexy (t = 2.78, p = 0.06). This result
is consistent with that found in 520 patients with narco-
lepsy by Harsh et al. [16].
PSG and MSLT findings
Narcolepsy patients have a total sleep time (TST) similar to
that of controls but with reduced sleep efficiency, shortened
sleep latency, and shorter latency to the first REM episode.
Night time sleep in narcolepsy is highly fragmented and is
interrupted by numerous awakenings and larger amounts of
waking time after sleep onset. This leads to a lighter sleep,
with an increased amount of stage 1 sleep at the expense
mainly of stage 2 sleep, which is reduced. Slow wave sleep
(SWS) may be preserved or reduced, and the amount of
REM sleep is comparable to that in the normal population
[2, 17–20].
Table 1 Demographic and clinical characteristics of patients
Feature Number (%) Mean ± SD
Age – 24.61 ± 6.83
Education level (years) – 9.70 ± 3.62
Sex
Female 16 (8.8) –
Male 165 (91.2)
Age at onset – 16.10 ± 5.45
Disease duration – 8.47 ± 5.59
Body mass index (kg/m2) – 25.08 ± 3.62
Cataplexy
Yes 126 (69.6) –
No 55 (30.4)
Hallucination
Yes 76 (42.0) –
No 105 (58.0)
Sleep paralysis
Yes 101 (55.8) –
No 80 (44.2)
The number of episodes of sleep – 2.96 ± 1.28
Epworth Sleepiness Score – 18.60 ± 3.23
Table 2 PSG and MSLT results of patients
Mean ± SD Min–max
value
Total sleep time 546.08 ± 189.30 291–984
Sleep latency (min) 4.68 ± 5.56 0–26
Sleep index (%) 91.28 ± 5.89 65–99
Percentage of stage 0* 7.66–5.72 0–34
Percentage of stage 1 2.46 ± 3.36 0–22
Percentage of stage 2 58.18 ± 10.89 6–80
Percentage of stage 3 5.12 ± 3.08 0–13
Percentage of stage 4 9.60 ± 7.10 0–32
Percentage of REM 16.69 ± 5.84 5–35
REM latency (min) 24.16 ± 48.07 0–287
Number of wakefulness 16.30 ± 8.13 1–45
MSLT average sleep latency
(min)
2.84 ± 1.91 0.40–8
MSLT SOREM number 3.20 ± 0.79 1–4
Acta Neurol Belg (2012) 112:177–181 179
123

Mean sleep latencies in narcoleptic patients are on aver-
age 3.1 ± 2.9 min [21]. In a study by Bahammam et al. [13]
the time required to fall asleep was 5.6 ± 1.1 min for
patients with cataplexy and 10.0 ± 2.6 min for patients
without cataplexy. In our study, the average sleep latency in
patients with narcolepsy was 4.68 ± 5.56 min.
According to the PSG findings in the present study of
patients with narcolepsy, sleep latency is short, sleep effi-
ciency is high, percentage of stage 2 sleep is high, rate of
slow wave sleep is low, REM latency is short, and the
number of bouts of wakefulness is high. Our findings are
consistent with some of the previous studies [16, 22, 23].
The presence of a REM period at the beginning of the
sleep is a significant feature of narcolepsy [24, 25].
SOREM is defined as the appearance of REM sleep within
15 min of the initiation of the recording. This occurs in
nearly 45% of narcolepsy patients [17, 18]. In our study,
the average REM latency was *24 min, and SOREM was
found in 74.6% of the cases. The reason for the higher
SOREM incidence compared with other studies may be the
lower mean age (24.6 years) of patients. In two separate
studies, the incidence of SOREM in young patients was
high and decreased with age [26, 27]. REM latency was
shorter and SOREM number on MSLT was higher in the
older age group than in the younger age group. MSLT is an
important tool in the diagnosis of narcolepsy and was
shown to be useful in distinguishing narcolepsy from idi-
opathic hypersomnolence [28].
Weaknesses of our study are that it is retrospective with
data collected over a long period, i.e. 16 years, and that
there is known inter-reader variability in sleep recording
analyses. With these reservations in mind, we believe that
the data from our cohort of 181 patients contribute to better
define the clinical and polysomnographic characteristics of
narcolepsy and the influence of age on them.
In summary, our findings in a large group of patients
diagnosed with definite narcolepsy according to demo-
graphic, clinical and polysomnographic features are largely
consistent with available data from the literature. The
nature and symptomatology of narcolepsy are insufficiently
known both by patients and physicians, which may delay
the diagnosis. Cataplexy is found in most narcolepsy
patients. In older patients, REM latency on PSG is shorter,
but the number of SOREM on MSLT is higher.
Conflict of interest None.
References
1. Zeman A, Britton T, Douglas N, Hansen A, Hicks J et al (2004)
Narcolepsy and excessive daytime sleepiness. BMJ 329(7468):
724–728
2. Plazzi P, Serra L, Ferri R (2008) Nocturnal aspects of narcolepsy
with cataplexy. Sleep Med Rev 12:109–128
3. Sturzenegger C, Bassetti C (2004) The clinical spectrum of nar-
colepsy with cataplexy: a reappraisal. J Sleep Res 13:395–406
4. Dauvilliers Y, Baumann CR, Maly FE, Billiard M, Bassetti C
(2003) CSF hypocretin-1 levels in narcolepsy, Kleine-Levin
syndrome, other hypersomnias and neurological conditions.
J Neurol Neurosurg Psychiatry 74:1667–1673
5. Mignot E, Lammers GJ, Ripley B, Okun ML, Nevsimalova S et al
(2002) The role of cerebrospinal fluid hypocretin measurement in
the diagnosis of narcolepsy and other hypersomnias. Arch Neurol
59:1553–1562
6. Ripley B, Overeem N, Fujiki N, Nevsimalova S, Uchino M et al
(2001) CSF hypocretin/orexin levels in narcolepsy and other
neurological conditions. Neurology 57:2253–2258
7. Hublin C, Kaprio J, Partinen M, Koskenvuo M, Heikkila K et al
(1994) The prevalence of narcolepsy: an epidemiological study of
the Finnish twin cohort. Ann Neurol 35:709–716
8. Silber MH, Krahn LE, Olson EJ, Pankratz VS (2002) The epi-
demiology of narcolepsy in Olmsted County, Minnesota: a pop-
ulation-based study. Sleep 25(2):197–202
9. Guilleminault C, Anagnos A (2000) Narcolepsy. In: Kryger MH,
Roth T, Dement WC (eds) Principles and practice of sleep
medicine, 3rd edn. W.B. Saunders, Philadelphia, pp 676–687
10. Izci B, Ardic S, Firat H, Sahin A, Altinors M et al (2008) Reli-
ability and validity studies of the Turkish version of the Epworth
Sleepiness Scale. Sleep Breath 12(2):161–168
11. Rechtschaffen A, Kales A (1968) A manual of standardized ter-
minology techniques and scoring system for sleep stages of
human subjects. National Institutes of Health Publication, No.
204
12. Thorpy MJ, Westbrook P, Ferber R, Fredrickson P, Mahowald M
et al (1992) The clinical use of the multiple sleep latency test. An
American Sleep Disorders Association report. Sleep 15:268–276
13. BaHammam AS, Alenezi AM (2006) Narcolepsy in Saudi Arabia
Demographic and clinical perspective of an under-recognized
disorder. Saudi Med J 27(9):1352–1357
14. Dahmen N, Kasten M, Muller MJ et al (2002) Frequency and
dependence on body posture of hallucinations and sleep paralysis
in a community sample. J Sleep Res 11(2):179–180
15. Ohayon MM, Ferini-Strambi L, Plazzi G, Smirne S, Castronovo
V (2005) How age influences the expression of narcolepsy.
J Psychosom Res 59:399–405
16. Harsh J, Peszka J, Hartwig G, Mitler M (2000) Night-time sleep
and daytime sleepiness in narcolepsy. J Sleep Res 9(3):309–316
17. Zorick F, Roehrs T, Wittig R, Lamphere J, Sicklesteel J et al
(1986) Sleep–wake abnormalities in narcolepsy. Sleep 9(1 Pt 2):
189–193
18. Bixler EO, Kales A, Vela-Bueno A, Drozdiak RA, Jacoby JA
et al (1986) Narcolepsy/cataplexy. III: nocturnal sleep and
wakefulness patterns. Int J Neurosci 29(3–4):305–316
19. Tafti M, Villemin E, Carlander B et al (1992) Sleep in human
narcolepsy revisited with special reference to prior wakefulness
duration. Sleep 15(4):344–351
20. Rogers AE, Aldrich MS, Caruso CC (1994) Patterns of sleep and
wakefulness in treated narcoleptic subjects. Sleep 17(7):590–597
21. Standard of Practice Committee of the American Academy of
Sleep Medicine (2005) Practice parameters for clinical use of the
multiple sleep latency test and the maintenance of wakefulness
test. Sleep 28:113–121
22. Besset A, Tafti M, Nobili L, Billiard M (1994) Homeostasis and
narcolepsy. Sleep 17:29–34
23. Guilleminault C, Heinzer R, Mignot E, Black J (1998) Investi-
gations into the neurologic basis of narcolepsy. Neurology 50:
8–15
180 Acta Neurol Belg (2012) 112:177–181
123

24. Mukai J, Uchida S, Miyazaki S, Nishihara K, Honda Y (2003)
Spectral analysis of all-night human sleep EEG in narcoleptic
patients and normal subjects. J Sleep Res 12(1):63–71
25. Nobili L, Beelke M, Besset A, Billiard M, Ferrillo F (2001)
Nocturnal sleep features in narcolepsy: a model-based approach.
Rev Neurol (Paris) 157(11 Pt 2):82–86
26. Gosselin A, Montplaisir J, Lesperance P et al (1997) The effect of
age on the MSLT in 137 patients with narcolepsy. Sleep Res 26:368
27. Dauvilliers Y, Gosselin A, Paquet J, Touchon J, Billiard M et al
(2004) Effect of age on MSLT results in patients with narco-
lepsy–cataplexy. Neurology 62:46–50
28. Boon P, Pevernagie D, Schrans D (2002) Hypersomnolence and
narcolepsy; a pragmatic diagnostic neurophysiological approach.
Acta Neurol Belg 102(1):11–18
Acta Neurol Belg (2012) 112:177–181 181
123





![[Product Monograph Template - Standard]tevacanadainnovation.com/downloads/Alertec_PM_EN.pdfPRODUCT MONOGRAPH . ... adult patients with narcolepsy, obstructive sleep apnea (OSA) and](https://img.pdfslide.us/doc/110x75/5ae5e3e07f8b9acc268c9f47/product-monograph-template-standard-monograph-adult-patients-with-narcolepsy.jpg)







![Narcolepsy treatment: pharmacological and behavioral ... · narcolepsy type 2 (NT2), formerly narcolepsy without cata-plexy and with normal hypocretin levels [1]. Hypocretin isa neurotransmitterinvolvedin](https://img.pdfslide.us/doc/110x75/60a115bf092a2c54425c9eaf/narcolepsy-treatment-pharmacological-and-behavioral-narcolepsy-type-2-nt2.jpg)















