Embed Size (px)
Citation preview

Dementia & Statins: Forget About It?
Cassandra Sanchez, Pharm.D. PGY2 Geriatric Pharmacy Resident
South Texas Veterans Health Care System, San Antonio, Texas Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center The University of Texas Health Science Center at San Antonio
November 14, 2014
Learning Objectives
1. Describe the differences in pathophysiology and presentation of specific dementia subtypes2. Discuss the rationale for the use of HMG-CoA reductase inhibitors (statins) in dementia3. Review the literature regarding the use of HMG-CoA reductase inhibitors in the treatment of Alzheimer’s disease
and prevention of vascular dementia4. Formulate a recommendation regarding the use of HMG-CoA reductase inhibitors in dementia

Sanchez 2
I. Dementia A. General term used to describe the decline in cognitive function affecting a person’s ability to independently perform
activities of daily living (ADLs)1,2
B. Dementia is now subsumed under new entity of major and mild neurocognitive disorders (NCD) based on the
Diagnostic and Statistical Manual of Mental Disorders (DSM-V) further specified into subtypes due to Alzheimer’s disease, Parkinson’s disease, frontotemporal, Lewy bodies, or other conditions
2,3
C. Significant cognitive decline from previous level in ≥1 cognitive domains: complex attention, executive function, learning and memory, language, perceptual-motor, or social cognition
2,3
II. Cognitive Domains
3
A. Complex attention i. Sustained attention, divided attention, selective attention, processing speed
Major—increased difficulty with multiple stimuli; easily distracted; difficulty with multistep tasks; difficulty holding new information in mind
Mild—normal tasks take longer; needs more double checking than before; find errors in routine tasks B. Executive function
i. Planning, decision making, working memory, responding to feedback/error correction, overriding habits/inhibiton, mental flexibility
Major—abandons complex projects; needs to focus on one task at a time; rely upon others for planning instrumental daily activities (iADLs) or make decisions
Minor—increased difficulty multitasking or resuming a task when interrupted; extra effort required to plan, organize, and make decisions
C. Learning and memory i. Immediate memory, recent memory, very-long-term memory
Major—repeats self often in conversation; requires frequent reorientation and reminders; cannot keep track of short list of items when shopping or of plans for the day
Mild—difficutly recalling recent events; relies more on written lists and reminders; loses track of bills paid
D. Language i. Expressive language (naming, grammar and receptive language)
Major—significant impairment in understanding or expressing language; difficulty naming things or people; reduced output of spoken communication
Mild—word-finding difficulty; subtle grammatical errors E. Perceptual-motor
i. Visual perception
Major—significant difficulty with previous familiar tasks (driving, using tools) or navigating in familiar environments
Mild—more reliance on others for directions or maps; greater effort needed for spatial tasks such as sewing or knitting
F. Social cognition i. Recognition of emotions, theory of mind
Major—clear unacceptable social behavior in terms of dress, grooming, or topics of conversation; no regard or awareness of the reactions of others; no insight to changes; makes decisions without regard to safety
Mild—subtle changes in personality; less able to recognize social cues or facial expressions; decreased empathy, decreased inhibition, or episodic apathy or restlessness
III. Epidemiology
A. Dementia affects about 1-2% of the population over 65 years of age and 30% of people over 85 yearsof age3
B. Alzheimer’s disease (AD) is the most common type of dementia accounting for 60-80% of dementia cases1-5
i. AD is not a normal part of aging
5
C. Vascular dementia (VaD) is the second most common type of dementia accounting for 20-30% of dementia cases1-3
D. Dementia with lewy bodies (DLB) is the third most common cause of dementia accounting for 10-25% of cases
1,3
E. Frontotemporal dementia (FTD) believed to be less common than AD, VaD, and DLB1
i. FTD accounts for 10-15% of dementia cases1
Dementia

Sanchez 3
F. Others2,3
i. Mixed dementia
ii. Parkinson’s disease dementia iii. Creutzfeldt Jakob disease iv. HIV infection
IV. Pathophysiology & Presentation of Dementias
Table 1. Pathophyisology & Presentation of Specific Neurocognitive Disorders1,3-7
Specific Neurocognitive Disorders
Pathophysiology Presentation
Alzheimer’s Disease (AD)
Amyloid plaques from β-amyloid (Aβ) peptide accumulation [extracellular]
Neurofibrillary tangles from abnormally hyperphosphorylated tau proteins [intracellular]
Insidious onset and gradual worsening progression of cognitive and behavioral symptoms
Manifests with memory and learning impairment
Vascular Dementia (VaD)
History of stroke or TIA
Large and small artery infarctions, recurrent infarctions, or hypoperfusion
Mood and personality changes
Memory loss occurs later in disease
Vascular changes on MRI or CT
Dementia with Lewy Bodies (DLB)
Lewy bodies are round, eosinophilic, intracytoplasmic inclusions found in neurons
α-synuclein protein aggregates in neurons in brain stem, cortex, substantia nigra and limbic system
Fluctuating cognition in attention and alertness (major cognitive deficits observed at least 1 year before the motor symptoms)
Recurrent visual hallucinations
Spontaneous parkinsonism
Rapid eye movement (REM) sleep disorder
Autonomic dysfunction (orthostatic hypotension, incontinence)
Frontotemporal Dementia (FTD)
Atrophy of brain’s frontal and/or temporal lobes
o Behavioral variant FTD (bvFTD) o Primary progressive aphasia (PPA) o FTD movement disorders
Onset around 50-60s
Early behavioral disinhibition
Personality changes
Decline in language ability “aphasia”
Parkinson’s Disease
Dementia (PDD)
Lewy bodies (α-synuclein protein) aggregate in substantia nigra
Parkinson’s disease history
Cognitive deficits occurs ~ 1 year after onset of motor symptoms [one year rule]
Mixed Dementia
Presence of one or more types of dementia at the same time (ex. Alzheimer’s disease + vascular dementia)
V. “Reversible” Causes of Cognitive Impairment
2,5
A. Conditions i. Vitamin B12 deficiency
ii. Thyroid dysfunction iii. Electrolyte abnormalities iv. Uremia v. Neurosyphilli
vi. Liver dysfunction B. Medications
i. Anticholinergic agents ii. Opioids
iii. Benzodiazepines iv. Corticosteroids v. Antiparkinsonian medications

Sanchez 4
VI. Diagnostic Criteria
Table 2. Diagnostic Criteria for Dementia/Neurocognitive Disorder3,8,9
DSM-IV DSM-V NINCDS-ADRDA
A. Memory impairment
B. One of more of the following cognitive disturbances:
Aphasia
Apraxia
Agnosia
Executive functioning
C. Cognitive deficits cause considerable impairment in social or occupational functioning and represent a decline from previous functioning
D. Onset is gradual, with continuing cognitive decline
E. Cognitive deficits cannot be attributable to other causes
F. Deficits are not caused by delirium
Major NCD A. Evidence of significant
cognitive decline from a previous level of performance in ≥1 cognitive domains based on:
1. Concern of the individual, knowledgeable informant, or the clinician
2. Impairment in cognitive performance by standardized neuropsychological testing, or another quantified clinical assessment
B. Cognitive deficits interfere with independence in everyday activities
C. Cognitive deficits do not occur exclusively in the context of a delirium
D. Cognitive deficits are not better explained by another mental disorder (depression, schizophrenia)
Mild NCD A. Evidence of modest
cognitive decline from a previous level of performance in ≥1 cognitive domains based on:
1. Concern of the individual, knowledgeable informant, or the clinician
2. Impairment in cognitive performance by standardized neuropsychological testing, or another quantified clinical assessment
B. Cognitive deficits do not interfere with independence in everyday activities
C. Cognitive deficits do not occur exclusively in the context of a delirium
D. Cognitive deficits are not better explained by another mental disorder (depression, schizophrenia)
I. Interfere with the ability to function at work or at usual activities; and
II. Represent a decline from previous level of functioning and performance; and
III. Are not explained by delirium or major psychiatric disorder; and
IV. Cognitive impairment is detected and diagnosed through a combination of 1.
history & 2.
cognitive assessment
V. Cognitive or behavioral impairment involving a minimum of 2 of the following domains: a. Impaired ability to acquire
and remember new information
b. Impaired reasoning and handling of complex tasks, poor judgment
c. Impaired visuospatial abilities
d. Impaired language functions (speaking, reading, writing)
e. Changes in personality, behavior, or comportment
Specify whether due to: Alzheimer’s disease, frontotemporal lobar degeneration, Lewy body disease, vascular disease, or
Parkinson’s disease DSM-IV & V-Diagnostic and Statistical Manual of Mental Disorders, 4th & 5th edition; NINCDS-ADRDA-National Institute of Neurological and Communicative Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association
Table 3. DSM-V Specific Diagnostic Criteria for Alzheimer’s Disease & Vascular dementia3
[see Appendix 1 for other types of dementia]
Specific Neurocognitive
Disorders
Diagnostic Criteria
Alzheimer’s Disease (AD)
A. Meet criteria for major or mild neurocognitive disorder B. Insidious onset and gradual progression of impairment in one or more cognitive domains (for major NCD, at
least two domains must be impaired) C. Meet criteria for probable or possible AD as follows:
For major neurocognitive disorder: Probable AD is diagnosed if either of the following is present; otherwise, possible AD should be diagnosed.
1. Evidence of a causative AD genetic mutation from family history or genetic testing 2. All three of the following are present:
a. Clear evidence of decline in memory and learning and at least one other cognitive domain (based on history or neuropsychological testing)

Sanchez 5
b. Steadily progressive, gradual decline in cognition, without extended plateaus c. No evidence of mixed etiology
For mild neurocognitive disorder: Probable AD is diagnosed if there is evidence of a causative AD genetic mutation from either genetic testing or family history. Possible AD is diagnosed if there is no evidence of a causative AD genetic mutation from either genetic testing or family history, and all three of the following are present:
1. Clear evidence of decline in memory and learning 2. Steadily progressive, gradual decline in cognition, without extended plateaus 3. No evidence of mixed etiology
D. The disturbance is not better explained by cerebrovascular disease, another neurodegenerative disease, the effects of a substance, or another mental, neurological, or systemic disorder
Vascular Dementia (VaD)
A. Meet criteria for major or mild neurocognitive disorder B. The clinical features are consistent with a vascular etiology, as suggested by either of the following:
1. Onset of the cognitive deficits is temporally related to one or more cerebrovascular events 2. Evidence for decline is prominent in complex attention (including processing speed) and frontal-
executive function C. There is evidence of the presence of cerebrovascular disease from history, physical examination, and/or
neuroimaging considered sufficient to account for the neurocognitive deficits D. The symptoms are not better explained by another brain disease or systemic disorder
Probable vascular NCD is diagnosed if one of the following is present; otherwise possible vascular NCD should be diagnosed: 1. Clinical criteria are supported by neuroimaging evidence of significant parenchymal injury attributed to
cerebrovascular disease 2. The neurocognitive syndrome is temporally related to one or more documented cerebrovascular events 3. Both clinical and genetic evidence of cerebrovascular disease is present
Possible vascular NCD is diagnosed if the clinical criteria are met but neuroimaging is not available and the temporal relationship of the neurocognitive syndrome with one or more cerebrovascular events is not established
VII. Screening Tools
Table 4. Dementia Screening Tests10-15
Exam Name Description Scoring
Mini Mental Status Exam (MMSE)
0-30 point scale (0=worst)
Average decline in score is 3-4 points per year without treatment
Normal: ≥27 Mild: 20-26
Moderate: 10-20 Severe: < 10
Alzheimer’s Disease Assessment Scale-Cognitive Section
(ADAS-cog)
Used for clinical trials; extensive comprehensive test
Measures language & memory skills
0-70 point scale
Higher score=more impairment
Alzheimer’s Disease Cooperative Study Clinical Global Impression
of Change (ADCS-CGIC)
Clincian’s impression of change
1-7 point Likert-type scale assessing change from baseline in 15 areas
Representative of improvement or worsening in a patient
Not “scored” per se o 1= marked improvement o 2= moderate improvement o 3=minimal improvement o 4= no change o 5= minimal worsening o 6=moderate worsening o 7= marked worsening
Neuropsychiatric Inventory (NPI)
12 symptoms rated on frequency of 1-4 and severity of 1-3; product=total score
Measures psychiatric and behavioral symptoms
0-144 point scale
Higher score=more impairment
Saint Louis University Mental Status Examination (SLUMS)
30 point scale
Higher score=less impairment
Accounts for education status & detects mild cognitive impairment
High School Less High School
27-30 Normal 25-30
21-26 Mild Cognitive Disorder
20-24
1-20 Dementia 1-19

Sanchez 6
VIII. Treatment
I. Cholesterol & AD Relationship
A. β-Amyloid (Aβ) formation & lipid rafts i. AD pathophysiology is proposed to be due to the accumulation of Aβ
5-8,25,26
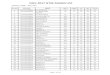
ii. Amyloidogenic processing, Aβ formation, of amyloid precursor protein (APP) takes place in the small membrane-bound domains known as lipid rafts within the cell membrane
6,25,26 [see Figure 2]
a. Lipid rafts are tightly packaged membrane micro-environments enriched in cholesterol and sphingolipids
6,25,26
Figure 2. Processing of Amyloid Precursor Protein (APP)6
Table 5. Pharmacological Treatment for Dementia16-24
Class Cholinesterase Inhibitors NMDA Inhibitor
Medication Donepezil (Aricept) Rivastigmine (Exelon) Galantamine (Razadyne) Memantine (Namenda)
Indication
FDA: Mild-severe AD Non-FDA: Mild-
moderate PDD & DLB
FDA: Mild-moderate AD & PDD
Non-FDA: DLB
FDA: Mild-moderate AD Non-FDA: Severe dementia AD,
mild-moderate PDD & DLB
FDA: Moderate-severe AD Non-FDA: Moderate-
severe vascular dementia
Dose & Titration
Tablet Tablet Patch IR Tablet ER Capsule IR Tablet ER Capsule
Starting: 5 mg/day Titration: 10 mg/day after 4-6 wks 23 mg/day after ≥ 12 wks
Starting: 1.5 mg BID Titration: ↑3 mg daily q 2 wks Max: 6 mg BID
Starting: 4.6 mg/day Titration: 9.5 mg/day after 4 wks 13.3 mg/day after 4 wks
Starting: 4 mg BID Titration: 8 mg BID after 4wks 12 mg BID after 4 wks
Starting: 8 mg QD Titration: 16 mg QD after 4 wks 24 mg QD after 4 wks
Starting: 5 mg QD Titration: ↑5 mg after ≥1 wk Max: 20 mg/day (divided doses)
Starting: 7 mg QD Titration: ↑ 7 mg weekly Max: 28 mg/day
MOA
Reversible, selective acetylcholinesterase inhibitor
Pseudo-irreversible, nonselective actetyl-and butylcholinesterase inhibitor
Reversible, selective acetylcholinesterase inhibitor & nicotine receptor modulator
N-methyl-D-aspartate (NMDA) receptor antagonist
Side Effects SLUDGE (salivation, lacrimation, urination, defecation, gastrointestinal upset, emesis), bradycardia, syncope, anorexia
Constipation, dizziness, confusion, headache
Administration
Take with or without food Available in ODT
Take with food Therapy is stopped ≤3 days, restart at same or lower dose Therapy is stopped >3 days, restart at lowest dose & titrate
Take with or without food
Cholesterol & Dementia: What's the relationship?

Sanchez 7
iii. Enzymes β-secretase (BACE-1) and γ-secretase are responsible for the production of Aβ and are located and active in these lipid rafts
25-27
iv. In vivo and in vitro studies have shown that an increase in cholesterol levels lead to enhanced β- and γ-secretase activity APP metabolism via the amylodigenic pathwayAβ production
6,25, 26
v. A decrease in intracellular cholesterol leads to rupture of the lipid rafts thus favoring α-secretase non-amyloidogenic pathway decrease in Aβ levels
6,26
B. Cholesterol levels
i. Cholesterol is a vital component of cell membranes and plays a role in the maintenance of neuronal plasticity and function with all cholesterol used in the brain synthesized within the CNS
27
ii. Blood and brain cholesterol pools are separated by the blood brain barrier (BBB) with homeostasis of brain cholesterol being critical
a. Two oxidized cholesterol metabolites: 24S-hydroxychloesterol and 27-hydroxycholesterol can pass across the BBB into the plasma
25-28
b. Higher levels of 24S-hydroxycholesterol in the cerebral spinal fluid (CSF) and peripheral blood could be indicative of increased cholesterol load and metabolism in the brain
26,27
c. Reports of increased 24S-hydroxycholesterol levels in AD patients when compared to control subjects
25-27,32
iii. Elevated serum cholesterol levels have also been proposed to be a risk factor for the development of Alzheimer’s disease and other dementias
2,25,28-32
a. Studies have shown high cholesterol levels during midlife increases the risk for developing AD later in life
2,25,28,32
iv. Studies in in vitro cell cultures and animal models have shown the strongest evidence correlating increased cholesterol levels as a factor in the development of AD
23,28,30,32
a. Increased cholesterol levels leads to an increase in Aβ production and accumulation in the brain, while a decrease in cholesterol levels has shown a reduction in Aβ levels
25, 29-31
b. However, in vivo studies don’t translate with the same results v. Prospective studies have shown an association between elevated serum cholesterol levels and an
increased susceptibility to AD25,32-34
II. Cholesterol and VaD Relationship
A. Risk factor for VaD25,26
i. Elevated cholesterol levels play a role in the development of atherosclerosis or atherosclerotic plaques
which reduce the patency of intracranial blood vessels causing hypoperfusion and ischemic brain damage
26
a. Within 3 months following a stroke, 20-30% of individuals are diagnosed with dementia3
ii. High levels of LDL and low levels of HDL are established risk factors for coronary artery disease and carotid artery atherosclerosis which can lead to cognitive impairment through cerebral hypoperfusion or embolism
25
iii. Treatment with statins have shown clinical significance in reducing cardiovascular and cerebrovascular disease amongst a wide patient population
iv. Stroke is a major risk factor for VaD and clinical trials indicate statins significantly decrease stroke risk in vascular patients including patients with stroke. By reducing risk of stroke, statins may also reduce the incidence of post-stroke dementia
25
I. Pharmacokinetic Properties of Statins25,35
i. Classification based on lipophilicity or hydrophilicity
Kivipelto
Notkola
Prospective, population-based study
Found ApoE4 allele, high total cholesterol levels and elevated systolic blood pressure at midlife to be risk factors for AD
o Midlife blood pressure obtained once for most participants
o Questionable midlife cholesterol levels obtained
Prospective study
Found high serum cholesterol levels increased the risk of developing AD after adjusting for the presence of ApoE4 allele and age
o Small sample size
HMG-CoA Reductase Inhibitors

Sanchez 8
ii. Lipophilic statins are able to cross the BBB and penetrate cell membranes more effectively and may be more efficient in the treatment of dementia than the hydrophilic statins
II. Side Effects of Statins
Table 7. Side Effects of Statins36-41
Lovastatin
Simvastatin
Atorvastatin
Fluvastatin
Pravastatin
Rouvastatin
Gastrointestinal 2.5-3.5% 5.4-7.3% 6-14.1% 1.4-7.9% 4-10.5% 1.9-6.3%
Myalgia 3% 3.7% 8.4% 3.8-5% 1-2.9% 1.9-12.7%
Arthralgia 5-6% - 11.7% - - 3.8-10.1%
Increased liver enzymes 1.9% 1% 0.2-2.3% 0.2-4.9% 1.2% 2.2%
Rhabdomyolysis - 0-0.4% - - - -
III. 2013 ACC/AHA Lipid Guidelines
IV. Current Guideline Recommendations on Statins & Dementia
V. 2012 Food and Drug Administration (FDA) Safety Warning
46
i. FDA warned against non-serious and reversible cognitive impairment (memory loss, forgetfulness and confusion) experienced by some statin users with cardiovascular benefits outweighing the small increased side effect risk
ii. Warning was based on post-marketing adverse event reports and not associated with fixed or progressive dementia iii. FDA review did not reveal an association between the adverse event and a specific statin, age of the individual, statin
dose, or concomitant medication use iv. Data from observational and clinical studies did not suggest that cognitive changes associated with statin use are v. common or lead to clinically significant cognitive decline
Table 6. Properties of Statins
Drug Name Lipophillic
Lovastatin (Mevacor) Yes
Simvastatin (Zocor) Yes
Atorvastatin (Lipitor) Yes
Fluvastatin (Lesol) Yes
Pravastatin (Pravachol) No
Rouvastatin (Crestor) No
Table 8. 2013 ACC/AHA Guidelines Recommendations42
Four Statin Benefit Groups
1. Individuals with clinical atherosclerotic cardiovascular disease (ASCVD)/“secondary prevention” 2. Individuals with primary elevations of LDL ≥190 mg/dL 3. Individuals 40-75 years of age with diabetes mellitus (DM) with LDL 70-189 mg/dL without clinical ASCVD 4. Individuals without clinical ASCVD or DM, 40-75 years old with LDL 70-189 mg/dL and an estimated 10-yr ASCVD risk ≥7.5%
High-Intensity Statin Therapy Moderate-Intensity statin
Clinical ASCVD/secondary prevention*
LDL ≥ 190 mg/dL
Individuals 40-75 years of age with DM and an estimated 10-year ASCVD risk ≥ 7.5%
Individuals 40-75 years of age with diabetes with LDL 70-189 mg/dL without clinical ASCVD
Individuals without clinical ASCVD or DM, 40-75 years old with LDL 70-189 mg/dL and an estimated 10-year ASCVD risk ≥7.5%**
*If >75 years old or intolerant, use moderate intensity statin **Reasonable to treat with moderate-to-high intensity statin
Table 9. Guideline Recommendations on Statin Therapy for Dementia Management43-45
2008 American College of Physicians Guidelines
2001 American Academy of
Neurology Guidelines 2006 National Institute for Health and Care Excellence (NICE)
Guidelines
No recommendation stated
Statins should not be prescribed as a specific treatment for the primary prevention of dementia
For secondary prevention of dementia, vascular and modifiable risk factors (including raised cholesterol) should be reviewed in people with dementia and if appropriate, treat

Sanchez 9
I. Statins in Prevention of Vascular Dementia
Heart Protection Study Collaborative Group. Lancet 2002;360:7-22.47
[HSP Study]
Objective To assess the long term effects of cholesterol-lowering therapy on vascular and non-vascular mortality and major morbidity in a wide range of circumstances
Trial Design Randomized, placebo-controlled study
Population
Inclusion Criteria
Men or women aged 40-80 years
Non-fasting blood total cholesterol concentration of at least 135 mg/dL
High risk of death from coronary heart disease over the next 5 years from past medical history defined as: (i). coronary disease (MI, unstable or stable angina, coronary artery bypass graft, or angioplasty); or (ii). occlusive disease of non-coronary arteries (non-disabling stroke not thought to be hemorrhagic, transient cerebral ischemia, leg artery stenosis, carotid endarterectomy, other arterial surgery or angioplasty); or (iii). diabetes mellitus (type 1 or 2); or (iv). treated hypertension
Exclusion Criteria
Chronic liver disease (cirrhosis or hepatitis) or evidence of abnormal liver function (ALT >1.5 X ULN)
Severe renal disease or evidence of impaired renal function
Inflammatory muscle disease (dermatomyositis or polymyositis) or evidence of muscle problems (creatinine kinase >3 x ULN)
Concurrent treatment with cyclosporine, fibrates, high dose niacin
Child-bearing potential
Severe heart failure
Some life-threatening condition other than vascular disease or diabetes
Conditions that might limit long-term compliance (severely disabling stroke, dementia, or psychiatric disorder)
Intervention Simvastatin 40 mg daily (n=10,269) vs. placebo (n=10,267)
Outcomes
Primary Outcome: Effects on death from all causes, from coronary heart disease, and from all other causes
Secondary Outcome: Effects on (i). specific non-coronary causes of death; (ii). major coronary events (non-fatal MI or death from coronary disease), and major vascular events (major coronary events, strokes of any type, and coronary or non-coronary revascularizations) during the first 2 years and during last year of scheduled treatment; and (iii). non-fatal or fatal strokes of any type
Tertiary Outcomes: Site specific cancer, cerebral hemorrhage, vascular procedures, hospitalizations from angina and for fractures, cognitive impairment and loss of respiratory function
o Cognitive function assessed by modified Telephone Interview for Cognitive Status (TICS-m) questionnaire either face-to face or over the telephone (score of 22/39 was prespecified as indicative of some cognitive impairment)
Results
Baseline Characteristics
28% of individuals were ≥ 70 years of age
25% of individuals were women
41% of individuals had previous MI
9% of individuals had cerebrovascular disease
Mean total cholesterol: 106 mg/dL
Mean LDL: 61 mg/dL
Tertiary Outcomes
Mean TICS-m score at end of trial o Simvastatin vs. placebo: 24.08 vs. 26.06; difference 0.02 [standard error 0.07]
No significant differences were observed overall in participants classified as cognitively impaired o Simvastatin: 23.7%; Placebo: 24.2%
No significant differences were observed over in subgroup defined with respect to their age at study entry o Simvastatin vs. placebo: <65 years-17.1% vs. 17.8%; 65-69 years: 25.8% vs. 25.4%; 70-80 years: 34.6% vs. 36.2%
No significant differences were observed in subgroup defined with respect to history of cerebrovascular disease o No prior stroke—simvastatin vs. placebo: 22.8% vs. 23.3% o Prior stoke—simvastatin vs. placebo: 31.9% vs. 33.3%
Development of dementia o Simvastatin vs. placebo: 31 (0.3%) vs. 31 (0.3%)
Lipids/Cholesterol
Mean difference in concentrations (simvastatin minus placebo)
Follow-up (years) Total Cholesterol (mg/dL) LDL Cholesterol (mg/dL)
1 -30.6 ±1.44 -23.4 ±1.08
3 -21.6 ± 1.62 -16.2 ± 1.44
5 -14.4 ± 0.54 -12.6 ± 0.54
Study Average -21.6 ±3.6 -18 ± 3.6
Safety Data
Clinical Evidence

Sanchez 10
Results
Symptom Simvastatin (n=10,269) Placebo (n=10,267)
Elevated ALT 2-4 X ULN 139(1.35%) 131 (1.28%)
Elevated ALT >4 X ULN 43 (0.42%) 32 (0.31%)
Elevated CK 4-10 X ULN 19 (0.19%) 13 (0.13%)
Elevated CK >10 X ULN 11 (0.11%) 6 (0.06%)
Myopathy no rhabdomyolysis 5 (0.5%) 1 (0.1%)
Myopathy with rhabdomyolysis 5 (0.5%) 3 (0.03%)
Author’s Conclusions
No significant change in cognitive function was observed over 5 years between simvastatin vs. placebo in high risk vascular and non-vascular patients
Critique
Strengths
Randomized, placebo-controlled clinical trial with large patient population
Lager numberof high CV risk patients (DM, stroke, HTN, history of CV disease)
Mean follow-up was 5 years
Excluded patients diagnosed with dementia
Limitations
Cognitive function measured based on modified Telephone Interview for Cognitive Status (TICS-m)
No baseline cognitive function assessed
Study was not powered to assess the tertirary outcome
Cognitive function was only assessed at the end of the study
Take Home Points
No significant differences noted in overall cognition and in respect to age or previous stroke history between patients treated with simvastatin versus placebo over a 5 year period
Shepherd J, et al. Lancet 2002;360:1623-30.48
[PROSPER Study]
Objective To ascertain if treatment with pravastatin reduces the risk of cardiac events, stroke, cognitive decline, and disability in those with existing (secondary prevention) and in those at high risk of developing (primary prevention) vascular disease
Trial Design Randomized, multicenter, double-blind, placebo-controlled study
Population
Inclusion Criteria
Men and women from Scotland, Ireland, and Netherlands
Men and women 70-82 years if they have pre-existing vascular disease (coronary, cerebral, or peripheral) or raised risk of such disease because of smoking, hypertension, or diabetes
Total cholesterol 72-162 mg/dL & triglycerides <108 mg/dL
Exclusion Criteria
Those using < 75% or > 120% of the placebo medication in lead-in period
Poor cognitive function (MMSE <24)
Intervention Pravastatin 40 mg daily (n=2,891) vs. placebo (n=2,913)
Outcomes
Primary Outcome: Combined endpoint of definite or suspect death from coronary heart disease, non-fatal myocardial infarction, and fatal or non-fatal stroke
Secondary Outcome: Examination of coronary and cerebrovascular components separately
Tertiary Outcome: Assessment of transient ischemic attack, disability, and cognitive function
Results
Baseline Characteristics
Mean age in both groups: 75 years
Mean total cholesterol in both groups: 102.7 mg/dL
Mean MMSE baseline score in both groups: 28
Mean Barthel index score in both groups: 13.6
Mean instrumental assessment of activities of daily living score (iADLs) in both groups: 13.6
11% of patients enrolled history of stroke or TIA ; 44% of patients with a history of vascular disease
Tertiary Outcome
Cognitive function declined at the same rate in both treatment groups
No difference between the 2nd
baseline & last on-treatment value for the number of correct letter digit codes o Pravastatin-placebo -0.01 (95%CI -0.24—0.23, p=0.95)
No difference between the 2nd
baseline & last on-treatment value in the number of words remembered in the picture word learning test
o Pravastatin-placebo 0.02 (95%CI -0.12—0.16, p=0.80)
No difference between the 2nd
baseline & last on-treatment value for the time needed to complete the Stroop test o Pravastatin-placebo 0.8s (95%CI -0.4—2, p=0.19)
No difference between the 2nd
baseline & last on-treatment value for the MMSE score o Pravastatin-placebo 0.06 (95%CI -0.04—0.16, p=0.26)
No difference between the 2nd
baseline & last on-treatment value in activity levels over time as measured by the Barthel index
o Pravastatin-placebo 0.06 (95%CI -0.03—0.15, p=0.18)
No difference between the 2nd
baseline & last on-treatment value in instrumental activities of daily living (iADL) questionnaire
o Pravastatin-placebo 0.03 (95% CI -0.08—0.14, p=0.59)

Sanchez 11
II. Statin in Treatment of Alzheimer’s Disease
Results
Lipids/Cholesterol
After 3 months of therapy mean LDL:
Pravastatin: 45.05 mg/dL o Pravastatin group: 34% lower than the placebo group for compliant individuals; 32% lower for entire cohort
At second annual visit:
Pravastatin group: LDL decreased 33% in compliant individuals; 27% lower for the entire cohort
Safety Data
After 3 months of therapy:
No cases in either group with a creatine kinase concentration > 10 X ULN
One case in each group with increased plasma concentration of alanine and aspartate transaminases >3 X ULN
Symptom Pravastatin (n=2891) Placebo (n=2913)
One or more adverse events 1608 (56%) 1604 (55%)
Myalgia 36 32
Rhabdomyolysis 0 0
Author’s Conclusions
Pravastatin therapy didn’t show benefit in slowing the decline in cognitive function over the 3 years in patients with or at high risk of developing cardiovascular disease and stroke
Critique
Strengths
Randomized, double-blind, placebo-controlled study design
Large population
Mean follow up of 3.2 years
Accounted for baseline assessment exams
Included those with existing and high risk of developing cardiovascular and cerebrovascular disease including vascular disease, stroke & TIA history
Limitations
Study was not powered to assess the tertiary outcome
No mention on patient’s enrolled with a diagnosis of dementia
Statin used in the study was hydrophillic
Take Home Points Pravastatin had no significant effects on cognitive decline among patients with existing vascular disease and those at high risk of developing vascular disease
Feldman HH, et al. Neurology 2010;74(12):956-964.20,42
[LEADe Study]
Objective To evaluate the efficacy and safety of atorvastatin in patients with mild to moderate AD receiving therapy with acetylcholinesterase inhibitor (AchEI), donepezil
Trial Design Randomized, international, multicenter, double-blind, placebo-controlled, parallel-group study
Population
Inclusion Criteria
Male or female aged 50-90 years
Diagnosis of probable AD according to the DMS-IV criteria and NINCDS-ADRDA
Mild to moderate AD defined by MMSE score of 13-25 at screening
MRI or cranial CT within 12 months of entry consistent with diagnosis of AD
Receiving donepezil 10 mg for at least 3 months before screening
DM enrolled patient: stable blood sugars with diet or treatment were permitted with a HgbA1c <10% and fasting glucose levels <170 mg/dL and LDL between 95-135 mg/dL
LDL 95-195 mg/dL
Not requiring another lipid-lowering agent at the opinion of the investigator
Caregiver who was in contact at least 5 days/week for a minimum of 10 waking hour/week
Modified Hachinski Ischemic Score ≤4
Exclusion Criteria
Taking medications that affect lipid metabolism or cholinesterase activity other than donepezil within 3 months of screening
Hypersensitivity to HMG-CoA reductase inhibitors
Clinically significant or unstable medical condition including dermatologic, hematologic, pulmonary, cardiovascular, renal, hepatic, gastrointestinal, genitourinary, endocrine or neurologic disease
Medical conditions that could impact the bioavailability or metabolism or the study medication or affect results of the study
Intervention
18 months (treatment period) of placebo + donepezil 10 mg daily (n=317) or atorvastatin 80 mg + donepezil 10 mg daily (n=297); followed by 2-month atorvastatin withdrawal period which participants either continued atorvastatin 80 mg + donepezil 10 mg daily or switched to placebo + donepezil 10 mg daily ; participants receiving placebo + donepezil 10 mg contued to receive same therapy
Outcomes
Primary outcome: Change in ADAS-cog & ADCS-CGIC score at month 18 from baseline Secondary outcome: Change in NPI, modified ADAS-cog, MMSE, Clinical Dementia Rating Sum of Boxes (CDR-SB), and Alzheimer’s Disease Functional Assessment and Change Scale (ASDFACS) score at month 18 from baseline

Sanchez 12
Results
Baseline Characteristics
Mean age in both groups: 74 years
Mean donepezil use in both groups: 409 days
Mean total cholesterol in both groups: 224 mg/dL
Mean ApoE4 frequency in both groups: 60%
Mean ADAS-cog in both groups: 23
Mean MMSE in both groups: 22
Primary Outcome
No significant difference in (A). ADAS-cog & (B). ADCS-CGIC score change between treatment groups
Visit Treatment difference between atorvastatin 80 mg + donepezil 10 mg vs. placebo + donepezil 10 mg
ADAS-cog Score
LS Means Difference (SE)
95% CI of LS Means Difference
P-value between Treatment
Overall (month 0-18) -0.532 (0.467) [-1.450-0.386] 0.2556
LOCF -1.112 (0.640) [-2.268-0.144] 0.0827
ASCD-CGIC Score
Overall (month 0-18) 0.021 (0.061) [-0.099-0.141] 0.7292
LOCF 0.160 (0.086) [-0.009-0.328] 0.0628 LS-least squares; SE-standard error; LOCF-last observations carried forward
Secondary Outcome
No significant difference in NPI, ADFACS, CDR-SB, MMSE, and modified ADAS-cog between treatment groups
Lipids/Cholesterol
Lipids: Mean LDL decrease (after 3 months of therapy):
Atorvastatin: -72.4 mg/dL (-50.2%)
Placebo: -1.0 mg/dL (-0.2%) o Changes remained constant through month 18
Safety Data
Treatment-Related Atorvastatin (n=324) Placebo (n=325)
Number of adverse events 192 102
Subjects with adverse events 103 (32.8%) 61 (18.8%)
Subjects with severe adverse events* 6 (1.9%) 3 (0.9%)
Incidence of persistent elevations in AST/ALT levels**
24 (11.9%) 25 (10.3%)
Myalgia 10 (4.9%) 11 (5.4%)
*hepatitis, acute renal failure/rhabdomyolysis/pancreatitis, abdominal pain/nausea/chest discomfort, transaminase elevation, liver disorder, and gastrointestinal hemorrhage **3 X upper limit of normal on 2 consecutive measures 4 to 10 days apart
Author’s Conclusions
Therapy with atorvastatin as a treatment for mild to moderate AD was not associated with significant clinical benefit over 18 months compared with placebo

Sanchez 13
Sano M, et al. Neurology. 2011;77:556-563.
21
Objective To determine if the lipid-lowing agent simvastatin slows the progression of symptoms in Alzheimer disease
Trial Design Randomized, multicenter, double-blind, placebo-controlled study
Population
Inclusion Criteria
Age ≥ 50 years
Probable AD meeting NINCDS-ADRDA criteria that were medically stable
MMSE score between 12 and 26
Exlusion Criteria
Other neurologic or psychiatric diagnosis that could interfere with cognitive function
Taking lipid-lowering drugs or conditions requiring cholesterol lowering treatment as defined by ATP III guidelines
LDL <80 mg/dL or TG >500 mg/dL
Drug taken recently with significant central anticholinergic effects, sedatives, antiparkinsonian medications, or any investigational treatment for AD
Taking medications that were contraindicated with simvastatin & those that could interact with CYP-3A4 to ↑ or ↓the levels of simvastatin
Intervention Simvastatin 20 mg daily X 6 wks, then 40 mg daily X 16.5 months (n=204) vs. placebo (n=202)
Outcomes Primary outcome: Rate of change on the cognitive portion of the ADAS-cog score
Secondary outcome: Rate of change on ADCS-CGIC, MMSE, dependence scale, ASCS-ADL, and NPI
Results
Baseline Characteristics Average age of both groups: 74.6
Average duration of disease of both groups: 4.13 years
Mean total cholesterol of both groups: 211.9 mg/dL
Mean ADAS-cog score slightly higher in placebo vs. simvastatin: 68.6 vs. 67.2 (respectively, p=0.0414)
Mean MMSE score for both groups: 20.4
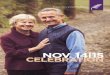
Primary Outcome No significant difference in rate of change in ADAS-cog score between placebo and simvastatin (95% CI -0.0462-0.1680,
P=0.25)
(A). Total Score (B). Change in Score
Critique
Strengths
Randomized, double-blind, placebo-controlled study design
Assessed for baseline ADAS-cog and ADCS-CGIC scores at 3 month intervals
Statin used in the study was lipophilic
Limitations
Excluded patients with significant CV, cerebrovascular, and peripheral vascular disease
Allowed selected atypical antipsychotics, antidepressants, and low-dose benzodiazepines if stable for 3 months before baseline visit
Primary endpoints were not met and withdrawal phase was not reported
Short follow-up time period of 18 months
Take Home Points
Therapy with atorvastatin as a treatment for mild to moderate AD was not associated with significant clinical benefit over 18 months

Sanchez 14
Results
Cognitive Exam & Functional Measures
Placebo (n=202) Simvastatin (n=204)
Change in score from baseline
ADAS-cog
3 months 6 months 12 months 18 months
Placebo 1.11 ± 5.32 2.32 ± 5.90 5.36 ± 6.95 8.18 ± 8.70
Simvastatin 1.89 ± 5.35 2.51 ± 5.61 5.79 ± 7.76 9.51 ± 9.48
Secondary Outcome
No significant differences in rate of change in MMSE, dependence scale, ADSC-ADL & NPI scores between placebo and simvastatin
Cognitive Exam & Functional Measures
Placebo (n=202) Simvastatin (n=204)
Change in score from baseline
MMSE
3 months 6 months 12 months 18 months
Placebo
-0.10 ± 3.10 -0.89 ± 3.23 -2.28 ±4.08 -3.75 ±4.28
Simvastatin -0.52 ± 2.74 -0.72 ±3.26 -2.47 ± 3.80 -4.23 ± 4.77
Dependence Scale Placebo -0.15 ± 0.87 -0.21±0.83 -0.36 ± 0.96 -0.53 ± 1.10
Simvastatin -0.04 ± 0.85 -0.10 ± 1.04 -0.26 ± 1.02 -0.48 ± 1.09
ADAS-ADL Placebo -1.20 ± 6.09 -3.95 ± 8.42 -6.21 ± 10.94 -9.62 ± 12.86
Simvastatin -1.54 ±7.44 -3.66 ± 8.18 -7.45 ± 10.18 -10.47 ±13.37
NPI Placebo 0.21 ± 8.02 1.26 ± 9.16 3.60 ± 10.38 3.78 ± 10.73
Simvastatin -0.64 ± 8.61 -0.09± 9.61 1.95 ± 10.64 3.21 ± 12.71
Lipids/Cholesterol Total cholesterol [simvastatin vs. placebo]: ↓ 23% (p<0.001)
LDL [simvastatin vs. placebo]: ↓ 37% (p<0.001)
Safety Data One or more adverse events
Placebo: 181/202 (89.6%)
Simvastatin: 189/204 (92.7%) p=0.30
Symptom Placebo group (n=202) Treatment group (n=204)
Agitation 47 (23.3%) 50 (24.5%)
Asthenia 43 (21.3%) 43 (21.1%)
Diarrhea 28 (13.9%) 40 (19.6%)
Arthralgia 24 (11.9%) 25 (10.3%)
Myalgia 10 (4.9%) 11 (5.4%)
Author’s Conclusions
Treatment with simvastatin for 18 months had no effect on the progression of symptoms based upon ADAS-cog assessment in individuals with mild to moderate AD & no noted change in the secondary outcomes including MMSE or ADAS-CGIC
Critique
Strengths
Primary and secondary outcomes measured at 3, 6, 12, and 18 months
Screened for ApoE4 genotype for those consenting
Baseline ADAS-cog assessment score
Baseline ADAS-cog score was significantly higher in the placebo group
Allowed for the use of acetylcholinesterase inhibitors (AChEi) and memantine
Sample size was met
Adjusted for covariates
Stated compliance of medication (no significant difference between groups)
Statins used in the study was lipophillc
Limitations
ApoE4 allele was not included in the primary analysis
Short follow-up time with of median of 17.9 months
Take Home Point
Simvastatin had no additional benefit to slowing the progression of symptoms of AD based on the ADAS-cog exam over 18 months in mild to moderate AD

Sanchez 15
I. Are statins beneficial for the prevention of vascular dementia?
a. Review of the literature does not support the use of statins for the clinical indication of prevention of dementia associated with vascular disease to help prevent cognitive impairment, possible due to short study durations
i. However, the use of statins in primary and secondary prevention of cardiovascular and cerebrovascular events still remains beneficial in elderly patients
II. Are statins beneficial for the treatment of Alzheimer’s Disease?
a. Review of the literature does not support the use of statins for the clinical indication of treatment of dementia associated with Alzheimer’s disease to help slow progression of cognitive impairment
b. Studies, including patients with high cardiovascular or cerebral vascular disease, does not support the use of statins for the clinical indication of treatment of dementia associated with Alzheimer’s disease
III. Do statins worsen Alzheimer’s disease or vascular dementia?
a. The 2012 FDA safety warning was developed using case-reports, adverse drug event reporting from consumers and health care professions and observational studies, which should warrant further investigation
b. Review of randomized clinical trials with primary, secondary and tertiary endpoints did not slow the progression of Alzheimer’s or vascular dementia with an overall low incidence of side effects
Clinical Recommendation/Summary

Sanchez 16
1. What is Dementia? Alzheimer’s Association. http://www.alz.org/what-is-dementia.asp. Accessed September 24, 2014. 2. Alzheimer’s Association. 2014 Alzheimer’s disease facts and figures. Alzheimers Dement 2013;10(2):e47-92.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th
edition). Arlington, VA; American
Psychiatric Publishing; 2013.
4. What is Alzheimer’s? Alzheimer’s Association. http://www.alz.org/alzheimers_disease_what_is_alzheimers.asp. Accessed
September 14, 2014.
5. Slattum PW, Peron EP, Hill A. Chapter 38. Alzheimer's Disease. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey
L. eds. Pharmacotherapy: A Pathophysiologic Approach, 9e. New York, NY: McGraw-Hill; 2014.
http://accesspharmacy.mhmedical.com/content.aspx?bookid=689&Sectionid=45310488. Accessed September 01, 2014.
6. Querfurth HW and LaFerla FM. Mechanisms of disease: Alzheimer’s disease. N Engl J Med 2010;362:329-44.
7. Cummings JL. Drug Therapy: Alzheimer’s disease. N Engl J Med 2004;352:56-67.
8. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th
edition). Washington, DC.;
American Pyshciatric Publishing; 1994.
9. McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from
the National institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer
Dement 2011;7(3):263-69.
10. Folsetin MF, Folstein SE, and McHugh PR. “Mini-mental state.” A practical method for grading the cognitive state of patient for
the clinician. J Psychiatr Res 1975;12(3):189-98.
11. Royall DR, Cordes JA, and Polk M. CLOX: an executive drawing task. J Neurol Neurosurg Psychiatry 1998;64:588-94.
12. Tariq SH, Tumosa N, Chibnall JT, Perry III HM, and Morley JE. Comparison of the Saint Louis University mental status (SLUMS)
examination and mini-mental state examination fo detecting dementia and mild neurocognitive disorder—a pilot study. Am J
Geriatr Psych 2006;14(11):900-10.
13. Schnieider LS, Olin JT, Doody RS, et al. Validity and reliability of the Alzheimer’s disease cooperative study-clinical global
impression of change: the Alzheimer’s disease cooperative study. Alzheimer Dis Assoc Disord 1997;11(Suppl 2):S22-32.
14. Cummings JL. The Neuropsychiatric Inventory: Assessing psychopathology in dementia patients. Neurology 1997;48(Suppl
6):S10-16.
15. Alzheimer’s Disease Cooperative Study. Administration manual for the Alzheimer’s disease assessment scale.
http://www.dementia-assessment.com.au/cognitive/adas_packet.pdf. Accessed October 25, 2014.
16. Donepezil. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed September 24, 2014.
17. Aricept (donepezil) [package insert]. Woodcliff Lake, NJ: Eisai Inc; Revised August 2013.
18. Rivastigmine. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed September 24, 2014.
19. Exelon Patch (rivastigmine transdermal system) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals; Revised July 2013.
20. Exelon (rivastigmine tartrate) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals; Revised October 2013.
21. Galantamine. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed September 24, 2014.
22. Galantamine [package insert]. Horsham, PA: Patriot Pharmaceuticals; Revised June 2014.
23. Memantine. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed September 24, 2014.
24. Namenda (memantine) [package insert]. St. Louis, MO: Forest Pharmaceuticals; Revised October 2013.
25. McGuinness B, O’Hare J, Craig D, et al. Statins for the treatment of dementia. Cochrane Database Syst Rev 2010;(8):CD007514.
DOI: 10.1002/14651858.CD007514.pub2.
26. Silva T, Teixeira J, Remiao F, and Borges F. Alzheimer’s disease, cholesterol, and statins: the junctions of important metabolic
pathways. Angew Chem Int Ed Engl 2013;52(4):1110-21.
27. Shobab LA, Hsiung GYR, and Feldman HH. Cholesterol in Alzheimer’s disease. Lancet Neurol 2005;4:841-52.
28. Jones RW, Kivipelto M, Feldman H, et al. The atorvastatin/donepezil in Alzheimer’s disease study (LEADe): design and baseline
characteristics. Alzhimer Dement 2008;4:145-53.
29. Feldman HH, Doody RS, Kivipelto M, et al. Randomized controlled trial of atorvastatin in mild to moderate Alzheimer
disease(LEADe Study). Neurology 2010;74(12):956-64.
References

Sanchez 17
30. Sano M, Bell KL, Galasko D, et al. A randomized, double-blind, placebo-controlled trial of simvastatin to treat Alzheimer
disease. Neurology 2011;77:556-63.
31. Sparks DL, Sabbagh MN, Connor DJ, et al. Atorvastatin for the treatment of mild to moderate Alzheimer disease: preliminary
results. Arch Neurol 2005;62(5):753-57.
32. Wood WG, Li L, Muller WE, and Eckert GP. Cholesterol as a causative factor in Alzheimer’s disease: a debatable hypothesis. J
Neurochem 2014;129(4):559-72.
33. Kivipelto M, Helkala EL, Laakso MP, et al. Apolipoprotein E epsilon4 allele, elevated midlife total cholesterol level, and high
midlife systolic blood pressure are independent risk factors for late-life Alzheimer disease. Ann Intern Med 2002;137(3):149-55.
34. Notkola IL, Sulkava R, Pekkanen J, et al. Serum total cholesterol, apolipoprotein E epsilon 4 allele, and Alzheimer’s disease.
Neuroepidemiology 1998;17(1):14-20.
35. Vaughan CJ and Gotto AM. Update on statins: 2003. Circulation 2004;110(7):886-92.
36. Lovastatin. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed October 24, 2014.
37. Simvastatin. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed October 24, 2014.
38. Atorvastatin. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed October 24, 2014.
39. Fluvastatin. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed October 24, 2014.
40. Pravastatin. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed October 24, 2014.
41. Rosuvastatin. In: DRUGDEX® System. Greenwood Village, Colo: Thompson Healthcare. Updated periodically.
http://www.thomsonhc.com/micromedex. Accessed October 24, 2014.
42. Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce
atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task
Force on Practice Guidelines. Circulation. J Am Coll Cardiol 2013.
43. National Collaborating Centre of Mental Health(UK). Dementia: A NICE-SCIE guideline on supporting people with dementia and
their carers in health and social care. Leicester (UK): British Pyschological Society; 2007.
44. Doody RS, Stevens JC, Beck C, et al. Practice parameter: management of dementia (an evidence-based review): Report of the
quality standards subcommittee of the American Academy of Neurology. Neurology 2001;56(9):1154-66.
45. Qaseem A, Snow V, and Cross JT Jr, et al. Current pharmacologic treatment of dementia: a clinical practice guideline from the
American College of Physicians and the American Academy of Family Physicians. Ann Intern Med 2008;148(5):370-78.
46. Food and Drug Administration. FDA Drug Safety Communication: Important safety label changes to cholesterol-lowering statin
drugs. FDA Drug Safety and Availability. http://www.fda.gov/Drugs/DrugSafety/ucm293101.htm. Updated July 03, 2012.
Accessed September 30, 2014.
47. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in
20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002;360(9326):7-22.
48. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER):a randomised
controlled trial. Lancet 2002;360(9346):1623-30.
49. Simons M, Schwarzler F, Lutjohanna D, et al. Treatment with simvastatin in normocholesterolemic patients with Alzheimer’s
disease: a 26-week randomized, placebo-controlled, double-blind trial. Ann Neurol 2002;52(3):346-50.

Sanchez 18
Specific Neurocognitive
Disorders
Diagnostic Criteria
1
Dementia with Lewy Bodies
(DLB)
A. Meet criteria for major or mild neurocognitive disorder B. Insidious onset and gradual progression C. The disorder meets a combination of core diagnostic features and suggestive diagnostic features for either
probable or possible neurocognitive disorder with Lewy bodies For probable major or mild neurocognitive disorder with Lewy bodies, the individual has two core features, or one suggestive feature with one or more core features. For possible major or mild neurocognitive disorder with Lewy bodies, the individual has only one core feature, or one or more suggestive features.
1. Core diagnostic features: a. Fluctuating cognition with pronounced variations in attention and alertness b. Recurrent visual hallucinations that are well formed and detailed c. Spontaneous features of parkinsonism, with onset subsequent to the development of
cognitive decline 2. Suggestive diagnostic features:
a. Meets criteria for rapid eye movement sleep behavior disorder b. Severe neuroleptic sensitivity
3. The disturbance is not better explained by cerebrovascular disease, another neurodegenerative disease, the effects of a substance, or another mental, neurological, or systemic disorder
Frontotemporal Dementia (FTD)
A. Meet criteria for major or mild neurocognitive disorder B. Insidious onset and gradual progression C. Either (1) or (2):
1. Behavioral variant: a. Three or more of the following behavioral symptoms:
i. Behavioral disinhibition ii. Apathy or inertia
iii. Loss of sympathy or empathy iv. Perseverative, stereotyped or compulsive/ritualistic behavior v. Hyperorality and dietary changes
b. Prominent decline in social cognition and/or executive abilities 2. Language variant:
a. Prominent decline in language ability, in the form of speech production, word finding, object naming, grammar, or word comprehension
D. Relative sparing of learning and memory and perceptual-motor function E. The disturbance is not better explained by cerebrovascular disease, another neurodegenerative disease,
the effects of a substance, or another mental, neurological, or systemic disorder. Probable frontotemporal neurocognitive disorder is diagnosed if either of the following is present; otherwise, possible frontotemporal neurocognitive disorder should be diagnosed:
1. Evidence of a causative frontotemporal neurocognitive disorder genetic mutation, from either family history or genetic testing
2. Evidence of disproportionate frontal and/or temporal lobe involvement from neuroimaging
Parkinson’s Disease
Dementia (PDD)
A. Meet criteria for major or mild neurocognitive disorder B. Disturbance occurs in the setting of established Parkinson’s disease C. Insidious onset and gradual progression of impairment D. The neurocognitive disorder is not attributable to another medical condition and is not better explained by
another mental disorder Major or mild neurocognitive disorder probably due to Parkinson’s disease should be diagnosed if 1 and 2 are both met. Major or mild neurocognitive disorder possibly due to Parkinson’s disease should be diagnosed if 1 or 2 is met:
1. There is no evidence of mixed etiology (i.e., absence of other neurodegenerative or cerebrovascular disease or another neurological, mental, or systemic disease or condition likely contributing to cognitive decline)
2. The Parkinson’s disease clearly precedes the onset of the neurocognitive disorder
Appendix 1