Embed Size (px)
Citation preview
Neurobiology of Aging 25 (2004) 771–781
Dementia severity and Lewy bodies affect circadianrhythms in Alzheimer disease
David G. Harpera,∗, Edward G. Stopab, Ann C. McKeec,Andrew Satlina, David Fisha, Ladislav Volicerd
a Geriatric Psychiatric Program, Department of Psychiatry, McLean Hospital, Harvard Medical School, Belmont, MA, USAb Department of Pathology, Program in Neuropathology, Rhode Island Hospital, Brown University School of Medicine, Providence, RI, USA
c Department of Pathology, E.N. Rogers Memorial Hospital, Boston University School of Medicine, Bedford, MA, USAd Department of Pharmacology and Psychiatry, Boston University School of Medicine, Boston, MA, USA
Received 19 August 2002; received in revised form 10 March 2003; accepted 11 April 2003
Abstract
Sleep disturbance is a symptom shared by all neurodegenerative, dementing illnesses, such as Alzheimer’s disease (AD) and dementiawith Lewy bodies (DLB), and its presence frequently precipitates decisions to seek institutional care for patients. Although the sleepdisturbances of AD and DLB are qualitatively similar, they appear to be more prominent in patients with DLB. Disturbance of the circadianrhythm has been noted and is a potential factor underlying the nocturnal sleep fragmentation and daytime sleepiness observed in thesepatients. We studied the circadian variation of core-body temperature and motor activity in a total of 32 institutionalized patients withprobable AD by NINCDS-ADRDA criteria, 9 of whom also met pathologic criteria for DLB. Eight, healthy, elderly male controls werestudied on a clinical research unit designed to simulate the hospital environment where the dementia patients were studied. Circadianvariables generally had greater deviations from normal associated with increasing AD pathology, as measured by postmortem-determinedBraak stage, supporting the hypothesis that central changes mediate circadian disturbances in AD and DLB. Patients with a postmortemdiagnosis of DLB manifested greater disturbances of locomotor activity circadian rhythms than patients with AD, possibly reflecting thegreater sleep disturbances seen in this population, but the differences from normal in the circadian rhythms of the AD and DLB patientswere qualitatively similar.© 2003 Elsevier Inc. All rights reserved.
Keywords: Rest–activity cycle; Core-body temperature rhythm; Human; Sleep; Braak stage; Parkinson’s disease; Dementia; Alzheimer’s disease; Circadianrhythm
1. Introduction
Sleep–wake regulation in normal adults can best be char-acterized as an interaction between two discrete processes.The first, circadian process promotes alertness as a func-tion of time of day. The second, homeostatic process buildsneed to sleep as a function of the duration of prior wake-fulness[5,11]. Aging has been shown to contribute to a de-terioration in sleep quality and an increased incidence ofreported sleep disturbance[34], including increased wake-fulness and decreased time in slow-wave and REM sleep[19,28]. Age-associated changes in sleep appear to be a con-sequence of changed homeostatic[8] rather than altered cir-cadian function[12].
∗ Corresponding author. Tel.:+1-617-855-3160; fax:+1-617-855-3246.E-mail address: [email protected] (D.G. Harper).
Sleep disturbance is a frequent symptom in patientsclinically diagnosed with age-associated, neurodegenera-tive dementias such as Alzheimer’s disease[21,28], (AD)and Pick’s disease[26], and its presence often precipitatesdecisions by families and others to seek institutional care[27]. Patients diagnosed with probable AD also show directcircadian disturbances including reduced amplitude andphase-delay of circadian variation of core-body temperatureand activity[30,35] that could be contributing to the sleepdisturbance.
These studies have not addressed the question ofwhether the circadian abnormalities and sleep–wake dis-turbances seen in patients with probable AD stem fromendogenous or exogenous influences. Dementia patientsin nursing homes[1,9], and other institutional environ-ments specializing in the care of patients with neurode-generative dementia[35] have been found to have lowerdiurnal and greater nocturnal exposure to light than
0197-4580/$ – see front matter © 2003 Elsevier Inc. All rights reserved.doi:10.1016/j.neurobiolaging.2003.04.009

772 D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781
community-dwelling elderly. These changes have beenlinked to sleep disturbance in residents of these facilities[31], where opportunities for social interaction and otherenvironmental time cues may be reduced and impact thesleep of nursing home patients. These exogenous influ-ences, however, are distinct from the endogenous, neu-rodegenerative features of dementing illnesses normallythought to cause the emergence of behavioral symptoms,such as sleep and circadian rhythm disturbances. Evidenceto date from the limited literature addressing this ques-tion, implicates endogenous factors as a prime contributorto circadian disturbances in patients with AD[18]. Pa-tients studied at the same institution, yet with differentdementia diagnoses, have demonstrably different circa-dian abnormalities[18] supporting the hypothesis thatthe different neurodegenerative patterns of these illnesseshad a major influence on the ultimate, observed circadiandisturbances.
However, a diagnostic distinction, that has not yet beenexamined for circadian disturbance, is dementia with Lewybodies (DLB), a relatively recently defined nosological en-tity [24]. Lewy bodies are spherical, eosinophilic, neuronalinclusions composed of low molecular-weight neurofila-ments and, when seen in the substantia nigra, are the patho-logical hallmark of Parkinson’s disease. In DLB, however,Lewy bodies are seen in cortical as well as in subcorticalregions of the brain outside of the substantia nigra. ADand DLB share some neuropathological features such asbeta-amyloid plaques, however, patients with DLB oftenlack the neurofibrillary tangles generally seen in AD[17].This intricate relationship between DLB and AD makes forgreat difficulties in accurately distinguishing DLB and ADclinically [15,22].
Patients with DLB have sleep disturbances similar to thosewith other neurodegenerative dementias, however DLB pa-tients are noted to have greater overall sleep disturbance thanpatients with AD[16]. Manifestations of their sleep distur-bance include some clearly non-circadian phenomena suchas a greater incidence of REM sleep behavior disorder, asyndrome characterized by the loss of the ability to main-tain muscle atonia during REM sleep[4,13]. The increaseddaytime sleepiness and nightime arousals seen in DLB com-pared to AD could have a source in circadian regulation[16].
In the present study, therefore, we further test the hypoth-esis that endogenous, disease-specific factors are responsi-ble for the circadian disturbances in AD. First, if central,disease-related processes govern the circadian alterationsin AD then the more severe the changes, the more pro-found the circadian disturbances should be. Braak stagingof Alzheimer-related changes[6] provides a standardizedassessment tool for the evaluation of severity of pathologywhich correlates well with clinical progression of the illness[3]. Second, if environmental influences are most important,circadian disturbances in DLB should resemble those seenin AD.
2. Methods
2.1. Patients
The subjects were 32 elderly, male, dementia patients hos-pitalized at the E. N. Rogers Memorial (ENRM) VeteransHospital in Bedford, MA. Patients were admitted with a di-agnosis of probable AD. Following institutional review andinformed consent being obtained from the next-of-kin of thesubjects, physiological recordings of activity and tempera-ture were obtained every 6 months. Upon the death of thesubjects, consent was obtained from the subjects’ next-of-kinfor autopsy and resultant donation of their brains to theAlzheimer Disease Center at the ENRM VA Hospital. Sub-jects had a mean age of 70.2 ± 1.0 years, an average ageof onset of dementia symptoms of 60.7 ± 1.1 years and amean duration of neurodegenerative dementia of 11.8± 0.7years measured from the first appearance of symptoms asreported by the next-of-kin. The subjects were all severelyimpaired and required 24-h nursing care. Except for foursubjects with a history of alcohol abuse, yet who still metcriteria for probable AD, they had no lifetime history ofmajor affective illness, schizophrenia or substance abuse.All subjects were free from significant intercurrent illnessesand were taking no anti-pyretic medication for at least 24 hprior to the time of physiological recording. Lorazepam andhaloperidol were allowed as prns for agitation. Eight, elderly,male comparison subjects were recruited from the commu-nity via the Harvard Cooperative Project on Aging and theMassachusetts Institute of Technology’s Clinical ResearchCenter. Their mean age was 72.8 ± 2.1 years, they had noevidence of dementia as verified by Mini-Mental State Ex-amination and evaluation by a board-certified psychiatrist.They met all other study inclusion and exclusion criteria.
2.2. Physiological measurements
Locomotor activity and core-body temperature recordingswere made using ambulatory monitors during a 72-h, datacollection period. Patients were studied in their normal unitenvironment following usual ward routines. No effort wasmade to control light, food, nursing care, the patient’s sleepschedule or any other masking influences during the record-ing period. Core-body temperature was measured by a rectalthermistor (YSI, Series 400, Yellow Springs, OH) insertedto 10 cm and connected to a microprocessor-based ambu-latory monitor (Mini-Logger, Mini-Mitter Co., Sun River,OR) which sampled temperature every 6 min. Activity wasmeasured by an ankle-worn, piezoelectric, activity monitorsensitive to accelerations of 0.01 g defined as one activitycount (AM-16, Ambulatory Monitoring, Inc. Ardsley, NY).We employed the monitor’s zero-crossing mode which ismore sensitive to intense movements by coding additionalactivity counts for accelerations much greater than 0.01 g.Activity counts were accumulated over 5-min epochs andthe resultant quantity written to memory. Patients were as-

D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781 773
sessed in this way every six months for the duration of theirhospitalization.
2.3. Neuropathology
All brains were subjected to a standardized neuropatho-logic examination[23]. Brains were fixed for at least 4 weeksin 10% neutral buffered formalin to standardize shrinkageduring fixation. Fourteen brain areas were sampled basedon their suitability for diagnosing AD and DLB. Brain sec-tions were stained with Luxol fast blue—H+ E and the Biel-chowski silver stains, as well as with anti-tau and anti-alphasynuclein antibodies. The diagnosis of AD was guided bythe consensus criteria established by CERAD[25] and bythe work of Braak and Braak[6], both endorsed by the inter-national working group from the National Institute on Agingand The Reagan Institute[10]. The diagnosis of DLB wasmade in accordance with the consensus criteria of the con-sortium on DLB International Workshop[24]. Patients weregiven a diagnosis of AD, DLB with Alzheimer pathologyand DLB without Alzheimer pathology by two neuropathol-ogists (EGS and ACM). Diagnosis of significant vasculardisease was based on the criteria outlined in the NationalInstitute of Neurological Disorders and Stroke-AssociationInternationale pour la Recherce et l’Enseignement en Neuro-sciences (NINDS-AIREN) International Workshop[29]. Be-cause there were only two DLB patients without Alzheimerpathology, both DLB diagnoses were treated as one diagnos-tic entity in the comparisons with AD. AD cases were stagedaccording to the criteria of Braak and Braak[6] and com-pressed into three categories (Stages 1–2, 3–4 and 5–6)[7].
2.4. Data analysis
Assessments of raw locomotor activity data were madeboth in reference to the patient’s environment (diurnal andnocturnal activity) and the patient’s most and least active pe-riods (M10 and L5). Diurnal Activity was defined as activityoccurring between 06:00 and 00:00 h and nocturnal activ-ity as activity between 00:00 and 06:00 h. These measuresyield useful clinical information about the patient’s activ-ity cycle and level of nocturnal arousal. Since AD patient’sactivity, however, can be phase-shifted away from a normaldiurnal–nocturnal cycle[18,30], we also quantified grossmotor activity by measuring the mean hourly activity of the10 most active hours and the five least active hours (M10and L5) to obtain measurement of maximal and minimal ac-tivity without reference to time of day[37]. These latter twoindices yield gross motor activity levels during the patient’ssubjective activity and rest periods without distortions thatcan be introduced by individual circadian phase shifts awayfrom the normal environmental zeitgeber.
The strength of the activity rhythm was first assessed viathe calculation of the interdaily stability and intradaily vari-ability [37]. Interdaily stability (IS), a periodogram-basedalgorithm, calculates the consistency of the activity rhythm
from day-to-day by assessing the similarity of activity levelsaccumulated at each hour across multiple days (for example,activity between 1 and 2 p.m. on days 1–3). High IS, there-fore, indicates a greater degree of circadian stability in thedata. In contrast, intradaily variability (IV) makes a quanti-tative assessment of the fragmentation of the activity rhythmby measuring and quantifying the hour-to-hour variabilityof adjacent activity epochs (hours) throughout the recordingperiod. A high IV would, therefore, indicate the presence ofdaytime naps and nocturnal arousals in the subject.
Multi-oscillator cosinor analysis[33] was also used tomathematically model a two-harmonic, circadian model tothe activity and temperature data. From this function, weextracted the mesor (central value around which the modeloscillates and analogous to the mean), amplitude (absolutedistance from the mesor to the peak of the function) andacrophase (time of the peak of the model). We also calculatedthe goodness-of-fit of the model by measuring the variance(R2) of the model to the data.
2.5. Statistics
All data are reported as mean±standard error. Two com-parisons were made.
2.5.1. Braak stage comparisonWe tested the hypothesis that circadian disturbance in AD
would deviate from normal as a function of the increasedseverity of AD, based on Braak stage determined at thetime of pathological examination. Patients were those withdiagnoses of AD or DLB with AD pathology. Nineteenpatients (8 ambulatory, 11 non-ambulatory) who had finalactivity and core-body temperature measurements made<1year prior to death were included as subjects. Two of thesepatients had a co-morbid diagnosis of significant vasculardisease.
2.6. Dementia with Lewy bodies—Alzheimer’s diseasecomparison
We tested the hypothesis that DLB pathology would affectcircadian rhythms differently than AD without DLB pathol-ogy. Thirty-two patients (13 patients ambulatory; 19 patientsnon ambulatory) met diagnostic criteria for inclusion in thiscomponent of the study. Patient’s circadian rhythms werecompared at point of entry to the study (1.7 years prior todeath). Five subjects (4 AD; 1 DLB) also had co-morbid di-agnosis of vascular dementia but still met diagnostic criteriafor AD or DLB.
AD and DLB patients with Alzheimer pathology, sortedby Braak stage, were compared by a one-way between-subjects Analysis of Variance (ANOVA) in the Braak StageComparison test. Patients with different dementia diagnoseswere compared using between subjects ANOVA in theDLB–AD test. Normality assumptions were verified withthe Kolmogorov–Smirnoff test, and the equal variance as-

774 D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781
sumption was tested by the Levene median test. All ANOVAassumptions were verified at a criterion level ofP > 0.05.All post-hoc comparisons were by Tukey post-hoc test.
3. Results
3.1. Dementia diagnosis
3.1.1. Braak stage comparisonAll patients with antemortem temperature and activity
recordings made within 1 year of death and autopsy diagno-sis of either AD or LBD with Alzheimer pathology were in-cluded in the Braak stage comparison study (n = 19). Noneof the patients were seen at stages 1–2 (a clinically silentphase of AD), five patients were at stages 3–4 and 14 wereat stages 5–6. Of these, one patient (Braak Stages 5–6) didnot have a significant circadian rhythm of core-body tem-perature and was excluded from these circadian analyses.Fifteen patients were given a final diagnosis of AD and 4patients of DLB with AD pathology.
3.1.2. AD–DLB comparisonThirty-two patients met diagnostic criteria for inclusion
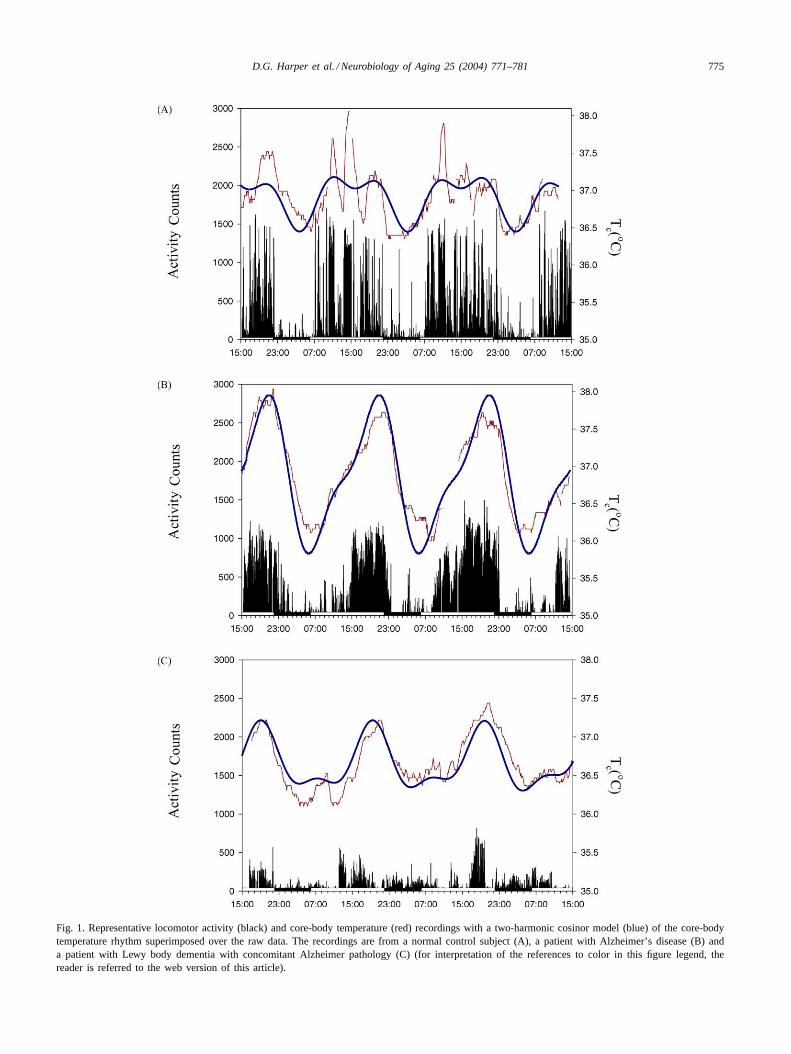
in this study. Of these, two patients (1 AD; 1 DLB) did nothave significant circadian rhythms of body temperature andtwo different patients (1AD; 1DLB) did not have significantcircadian rest–activity cycles. These patients were excludedfrom all comparisons using derived cosinor measures. How-ever, they were included in all analyses where their datawere reliable. Representative core-body temperature and lo-comotor activity data are presented inFig. 1.
3.2. Braak stage comparison
Physiological data were collected 123± 19 days (0.34±0.05 years) before death. Patients in Braak Stages 3–4 andthose in stages 5–6 did not differ in age (F1,23 = 0.41; P =0.5), duration of illness (F1,23 = 1.00; P = 0.3) or meanlength of hospitalization (F1,23 = 1.05; P = 0.3).
3.2.1. Locomotor activityMeasurements of gross locomotor activity increased in
abnormality with increased severity of illness (Table 1).Mean diurnal (F2,24 = 7.01; P = 0.003) and M10 activity(F2,24 = 7.26;P = 0.003) showed decreased locomotor ac-tivity in AD patients in both groups compared to controls.The reduction in mean diurnal activity was significant atBraak Stages 5–6, whereas M10 was also significantly re-duced at Braak Stages 3–4 (Tukey post-hocP = 0.04) andBraak Stages 5–6 (Tukey post-hoc;P = 0.002). IS showeda trend reduction at Braak Stages 5–6 (F2,24 = 3.00; P =0.07; Tukey post-hoc test;P = 0.07). IV revealed increasedfragmentation with severity of illness without attaining sta-tistical significance. Mean nocturnal activity, as well as L5,were not significantly different among the different groups,
but there was numerically greater activity at night and in theleast active hours for the dementia patients compared withthe controls.
Parametric, cosinor analysis of the rest–activity cy-cle supports the findings of the nonparametric analysis.Multi-oscillator, cosinor modeling revealed several sig-nificant effects related to Braak stage. The mesor ofthe rest–activity cycle was significantly reduced overall(F2,24 = 3.74;P = 0.047). The absolute amplitude of loco-motor activity was reduced at both Braak stages comparedto controls (F2,24 = 11.98; P < 0.001). However, whencorrecting for overall activity differences by measuring rel-ative amplitude (amplitude/mesor), locomotor activity wasstill reduced but the differences failed to reach statisticalsignificance. The acrophase of locomotor activity was sig-nificantly delayed at Braak Stages 5–6 compared to controls(F2,24 = 3.56; P = 0.44; Tukey post-hoc testP = 0.035).Finally, the goodness-of-fit of the raw data to the cosinorcurve was less than controls (F3,24 = 3.33; P = 0.04) andthis difference was significant at Braak Stages 5–6 (Tukeypost-hoc testP = 0.030).
3.2.2. Core-body temperatureChanges in the circadian rhythm were identified through
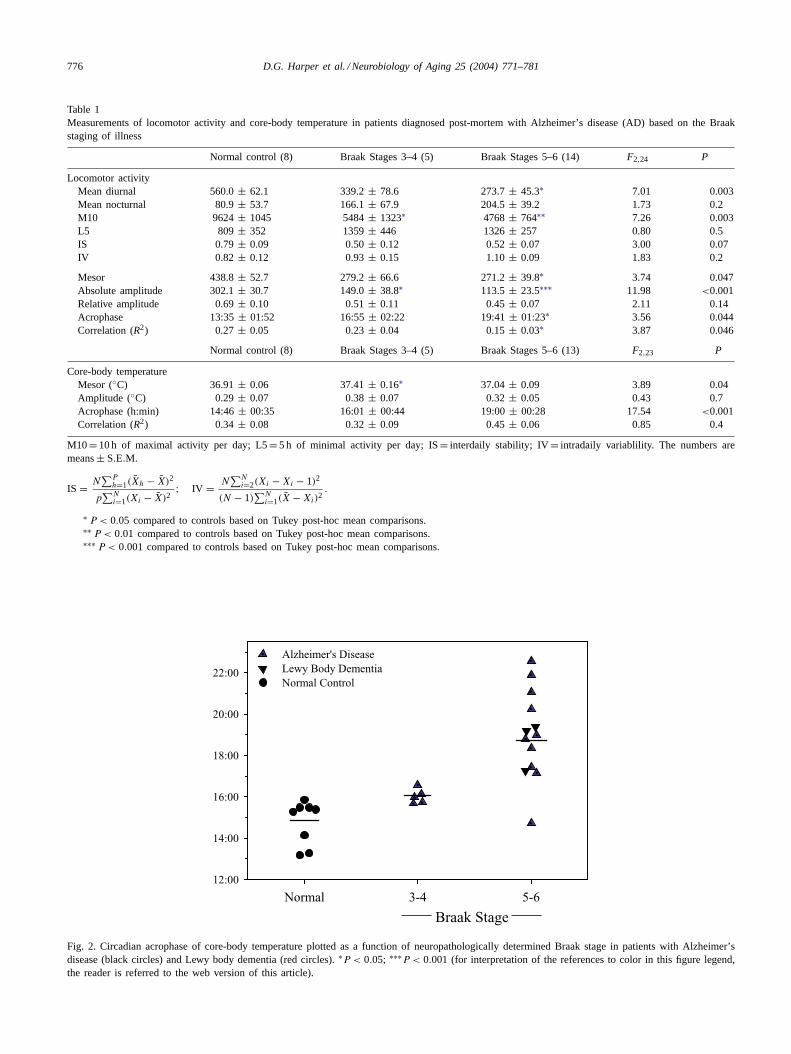
multi-oscillator cosinor analysis that appeared to be BraakStage specific. The temperature mesor (F2,23 = 3.89; P =0.04) was significantly increased at Braak Stages 3–4 fromthe level seen in controls (Tukey post-hoc;P = 0.03) re-turned to control levels at Braak Stages 5–6 but was sig-nificantly lower than at Braak Stages 3–4 (Tukey post-hoc;P = 0.02). The circadian acrophase (Fig. 2) was signifi-cantly delayed (F2,23 = 17.54; P < 0.001) at Braak Stages5–6 (Tukey post-hocP < 0.001). Circadian amplitude andgoodness-of-fit were not significantly different from thoseof normal controls.
3.3. Dementia with lewy bodies—Alzheimer’s diseasecomparison
3.3.1. Locomotor activityPatients in the DLB to AD comparison were studied
(mean± S.E.) more than 1.5 years before death (Lewybody = 2.23 ± 0.41 years; AD = 1.61 ± 0.23 years;F1,23 = 1.78; P = 0.20). The two dementia groups did notdiffer in age from each other or controls (Mean age LB=68.7 ± 2.9; AD = 71.5 ± 1.4; control= 72.8 ± 2.1 years;F2,37 = 0.73; P = 0.4), age of onset (LB= 58.0 ± 3.1;AD = 59.8 ± 1.5 years;F1,23 = 0.24; P = 0.63) or dura-tion of illness (LB= 10.7 ± 1.8; AD = 11.7 ± 0.9 years;F1,23 = 0.27; P = 0.6).
Core-body temperature and locomotor activity data aresummarized inTable 2. Diurnal (F2,37 = 5.58; P = 0.007)and M10 activity (F2,37 = 6.35; P = 0.004) were lower indementia patients than in normal elderly subjects, with thedifferences statistically significant for the DLB group. Di-urnal and M10 activity also were lower in the DLB patients
D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781 775
Fig. 1. Representative locomotor activity (black) and core-body temperature (red) recordings with a two-harmonic cosinor model (blue) of the core-bodytemperature rhythm superimposed over the raw data. The recordings are from a normal control subject (A), a patient with Alzheimer’s disease (B) anda patient with Lewy body dementia with concomitant Alzheimer pathology (C) (for interpretation of the references to color in this figure legend, thereader is referred to the web version of this article).
776 D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781
Table 1Measurements of locomotor activity and core-body temperature in patients diagnosed post-mortem with Alzheimer’s disease (AD) based on the Braakstaging of illness
Normal control (8) Braak Stages 3–4 (5) Braak Stages 5–6 (14) F2,24 P
Locomotor activityMean diurnal 560.0± 62.1 339.2± 78.6 273.7± 45.3∗ 7.01 0.003Mean nocturnal 80.9± 53.7 166.1± 67.9 204.5± 39.2 1.73 0.2M10 9624± 1045 5484± 1323∗ 4768± 764∗∗ 7.26 0.003L5 809 ± 352 1359± 446 1326± 257 0.80 0.5IS 0.79± 0.09 0.50± 0.12 0.52± 0.07 3.00 0.07IV 0.82 ± 0.12 0.93± 0.15 1.10± 0.09 1.83 0.2
Mesor 438.8± 52.7 279.2± 66.6 271.2± 39.8∗ 3.74 0.047Absolute amplitude 302.1± 30.7 149.0± 38.8∗ 113.5± 23.5∗∗∗ 11.98 <0.001Relative amplitude 0.69± 0.10 0.51± 0.11 0.45± 0.07 2.11 0.14Acrophase 13:35± 01:52 16:55± 02:22 19:41± 01:23∗ 3.56 0.044Correlation (R2) 0.27 ± 0.05 0.23± 0.04 0.15± 0.03∗ 3.87 0.046
Normal control (8) Braak Stages 3–4 (5) Braak Stages 5–6 (13) F2,23 P
Core-body temperatureMesor (◦C) 36.91± 0.06 37.41± 0.16∗ 37.04± 0.09 3.89 0.04Amplitude (◦C) 0.29± 0.07 0.38± 0.07 0.32± 0.05 0.43 0.7Acrophase (h:min) 14:46± 00:35 16:01± 00:44 19:00± 00:28 17.54 <0.001Correlation (R2) 0.34 ± 0.08 0.32± 0.09 0.45± 0.06 0.85 0.4
M10= 10 h of maximal activity per day; L5= 5 h of minimal activity per day; IS= interdaily stability; IV= intradaily variablility. The numbers aremeans± S.E.M.
IS = N∑P
h=1(X̄h − X̄)2
p∑N
i=1(Xi − X̄)2; IV = N
∑Ni=2(Xi − Xi − 1)2
(N − 1)∑N
i=1(X̄ − Xi)2.
∗ P < 0.05 compared to controls based on Tukey post-hoc mean comparisons.∗∗ P < 0.01 compared to controls based on Tukey post-hoc mean comparisons.∗∗∗ P < 0.001 compared to controls based on Tukey post-hoc mean comparisons.
Braak StageNormal 3-4 5-6
12:00
14:00
16:00
18:00
20:00
22:00
Alzheimer's DiseaseLewy Body Dementia Normal Control
Fig. 2. Circadian acrophase of core-body temperature plotted as a function of neuropathologically determined Braak stage in patients with Alzheimer’sdisease (black circles) and Lewy body dementia (red circles).∗P < 0.05; ∗∗∗P < 0.001 (for interpretation of the references to color in this figure legend,the reader is referred to the web version of this article).
D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781 777
Table 2Measurements of locomotor activity and core-body temperature in patients diagnosed post-mortem with Alzheimer’s disease (AD) and dementia withLewy bodies (DLB)
Normal control (8) Alzheimer’s disease (23) Lewy body dementia (9) F2,37 P
Locomotor activityMean diurnal 560.0± 63.0 403.4± 37.4 263.6± 59.4∗∗ 5.84 0.006Mean nocturnal 80.1± 47.6 239.9± 32.4∗ 180.8± 51.2 3.24 0.05
M10 9624± 995 6654± 610∗ 4493± 962†∗∗ 6.72 0.003L5 809 ± 394 1751± 225∗ 988 ± 356 3.11 0.05IS 0.79± 0.06 0.56± 0.04 0.60± 0.08 2.81 0.07IV 0.82 ± 0.10 0.81± 0.06 0.92± 0.10 0.57 0.6
Normal control (8) Alzheimer’s disease (22) Lewy body dementia (8) F2,35 P
Mesor 438.8± 54.5 371.6± 34.6 233.6± 55.2∗ 3.79 0.03Relative amplitude 0.69± 0.10 0.56± 0.06 0.47± 0.08 1.48 0.2Absolute amplitude 302.1± 43.1 202.8± 26.0 112.4± 40.1∗∗ 5.27 0.01Acrophase (h:min) 13:35± 01:03 16:24± 00:38 15:59± 00:55 2.64 0.08Correlation (R2) 0.27 ± 0.05 0.30± 0.04 0.21± 0.05 1.16 0.4
Core-body temperatureMesor (◦C) 36.91± 0.06 37.31± 0.12 37.28± 0.19 1.52 0.2
Amplitude (◦C) 0.29± 0.07 0.48± 0.04†,∗ 0.29 ± 0.06† 4.72 0.02Acrophase (h:min) 14:48± 00:23 17:45± 00:35∗ 17:41± 00:57 3.96 0.03Correlation (R2) 0.34 ± 0.07 0.53± 0.05 0.48± 0.08 1.74 0.2
The numbers are means± S.E.M.
IS = N∑P
h=1(X̄h − X̄)2
p∑N
i=1(Xi − X̄)2; IV = N
∑Ni=2(Xi − Xi − 1)2
(N − 1)∑N
i=1(X̄ − Xi)2.
∗ P < 0.05 compared to controls.† P < 0.05 compared to other dementia diagnosis patients based on Tukey post-hoc mean comparisons.
than in the AD group, with the difference statistically signif-icant only for the M10 comparison. The nocturnal activityof patients with AD and DLB were higher than that seen incontrol subjects (F2,37 = 3.24; P = 0.05), although noctur-nal activity in patients with DLB was less than that seen inAD and the difference from controls failed to reach statisti-cal significance.
IS and IV, the non-parametric measures of circadian ac-tivity of activity, were not significantly different among thedifferent diagnostic groups. There was a trend however fordecreases in interdaily stability (F2,37 = 2.81;P = 0.07) inthe dementia groups. Post hoc analysis showed this differ-ence approached statistical significance in AD versus con-trols (Tukey post-hocP = 0.06) but not in LBD (Tukeypost-hocP = 0.2).
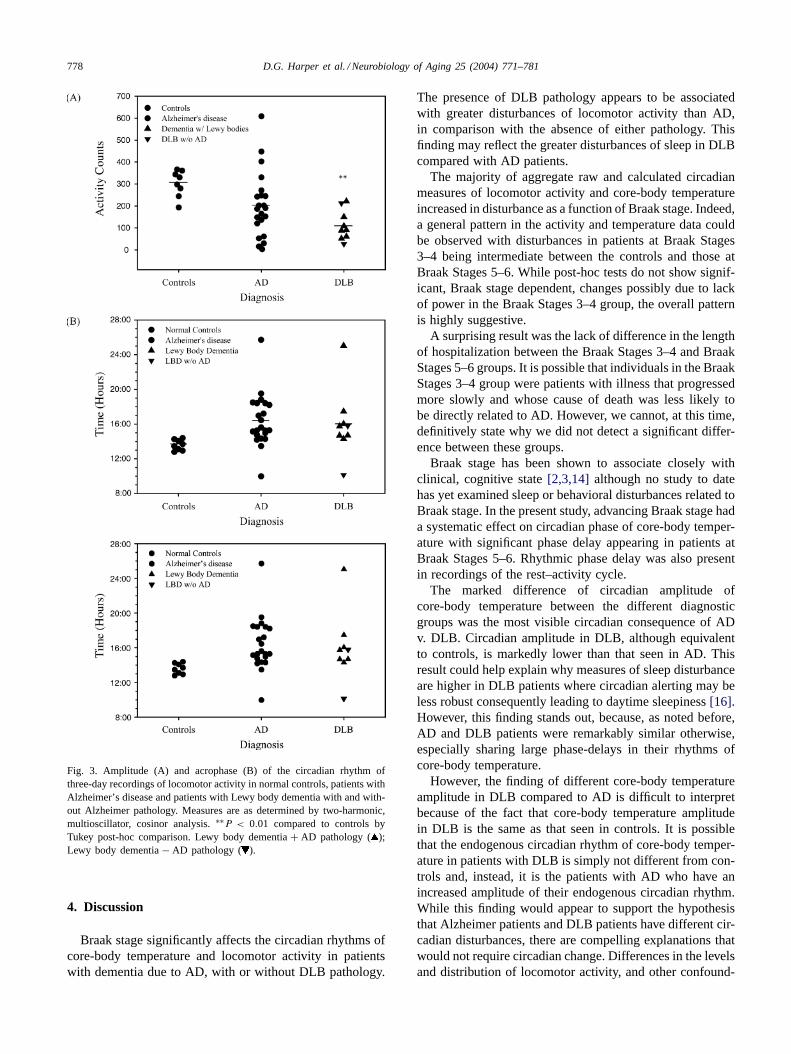
Parametric measures of circadian locomotor activityshowed several differences. As expected from measurementsof diurnal activity and M10, locomotor activity mesor wassignificantly lower in both dementia groups compared withcontrols, with the difference being statistically significantfor DLB versus control (F2,35 = 3.79;P = 0.03). A similarpattern was found for the absolute and relative amplitudesof locomotor activity, with statistical significance found forthe comparison of absolute amplitude between DLB andcontrols (F2,35 = 5.27; P = 0.01; Fig. 3A). Neither of thereductions in relative amplitude reached statistical signifi-
cance (F2,35 = 1.48; P = 0.2). There was a trend for dif-ferences in the time of peak locomotor activity between thedementia groups and the controls (F2,35 = 2.64; P = 0.08;Fig. 3B), although the phase-delays in both dementia groupswere similar (Tukey post hoc;P < 0.07). Goodness-of-fit(R2) of locomotor activity to the two-harmonic cosinormodel was not different among groups.
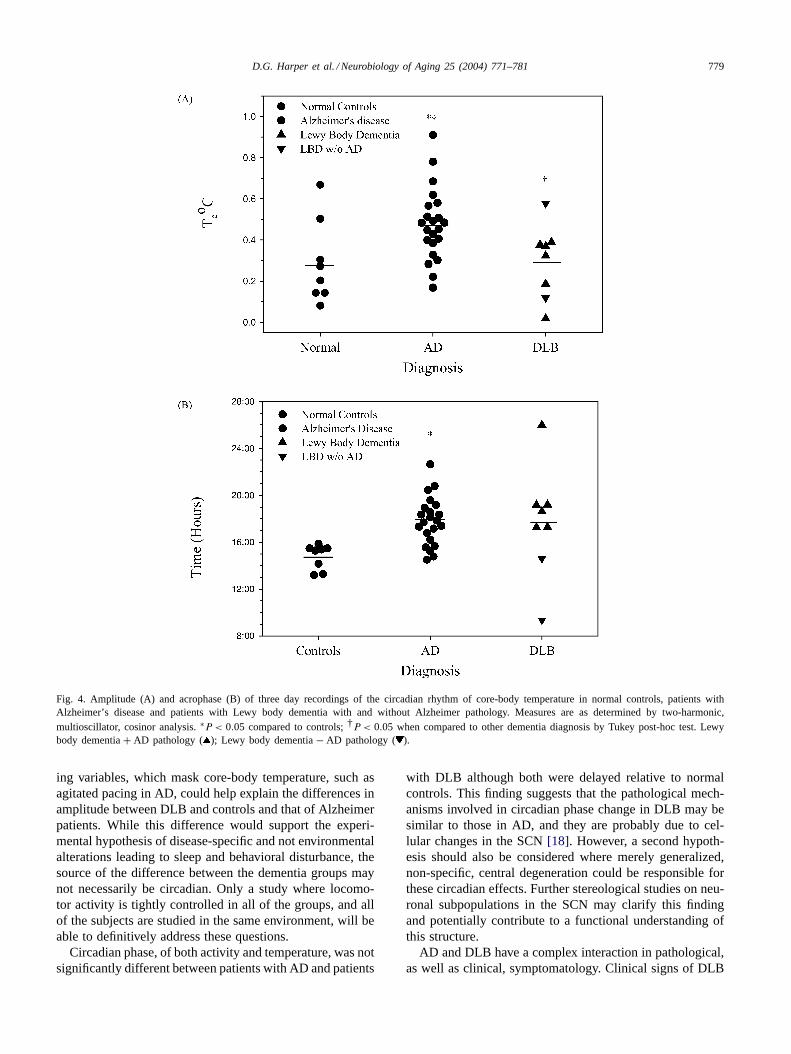
3.3.2. Core-body temperatureCore-body temperature amplitude was not different be-
tween controls and DLB, although the amplitude in theAD group was unexpectedly above both DLB and controls(AD = 0.48± 0.04◦C; DLB = 0.28± 0.08◦C; controls=0.29±0.07◦C; F2,35 = 4.72;P < 0.02;Fig. 4A). The circa-dian phase of core-body temperature was virtually identicalbetween AD and DLB although both were significantly laterthan that seen in control subjects (AD= 17 : 45; DLB =17:41; normal controls= 14:48;F2,35 = 3.96; P = 0.03;Fig. 4B). The goodness-of-fit (R2) of core-body temperaturedata to the two-harmonic cosinor model was not significantlydifferent between diagnostic groups (normal= 0.34±0.07;AD = 0.53 ± 0.05; DLB = 0.42 ± 0.08; F2,35 = 2.11;P = 0.1). The mesor of the core-body temperature rhythmwas higher in the dementia groups than the controls, how-ever these differences were not significant (F2,35 = 1.52;P = 0.2).
778 D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781
Fig. 3. Amplitude (A) and acrophase (B) of the circadian rhythm ofthree-day recordings of locomotor activity in normal controls, patients withAlzheimer’s disease and patients with Lewy body dementia with and with-out Alzheimer pathology. Measures are as determined by two-harmonic,multioscillator, cosinor analysis.∗∗P < 0.01 compared to controls byTukey post-hoc comparison. Lewy body dementia+ AD pathology ( );Lewy body dementia− AD pathology ( ).
4. Discussion
Braak stage significantly affects the circadian rhythms ofcore-body temperature and locomotor activity in patientswith dementia due to AD, with or without DLB pathology.
The presence of DLB pathology appears to be associatedwith greater disturbances of locomotor activity than AD,in comparison with the absence of either pathology. Thisfinding may reflect the greater disturbances of sleep in DLBcompared with AD patients.
The majority of aggregate raw and calculated circadianmeasures of locomotor activity and core-body temperatureincreased in disturbance as a function of Braak stage. Indeed,a general pattern in the activity and temperature data couldbe observed with disturbances in patients at Braak Stages3–4 being intermediate between the controls and those atBraak Stages 5–6. While post-hoc tests do not show signif-icant, Braak stage dependent, changes possibly due to lackof power in the Braak Stages 3–4 group, the overall patternis highly suggestive.
A surprising result was the lack of difference in the lengthof hospitalization between the Braak Stages 3–4 and BraakStages 5–6 groups. It is possible that individuals in the BraakStages 3–4 group were patients with illness that progressedmore slowly and whose cause of death was less likely tobe directly related to AD. However, we cannot, at this time,definitively state why we did not detect a significant differ-ence between these groups.
Braak stage has been shown to associate closely withclinical, cognitive state[2,3,14] although no study to datehas yet examined sleep or behavioral disturbances related toBraak stage. In the present study, advancing Braak stage hada systematic effect on circadian phase of core-body temper-ature with significant phase delay appearing in patients atBraak Stages 5–6. Rhythmic phase delay was also presentin recordings of the rest–activity cycle.
The marked difference of circadian amplitude ofcore-body temperature between the different diagnosticgroups was the most visible circadian consequence of ADv. DLB. Circadian amplitude in DLB, although equivalentto controls, is markedly lower than that seen in AD. Thisresult could help explain why measures of sleep disturbanceare higher in DLB patients where circadian alerting may beless robust consequently leading to daytime sleepiness[16].However, this finding stands out, because, as noted before,AD and DLB patients were remarkably similar otherwise,especially sharing large phase-delays in their rhythms ofcore-body temperature.
However, the finding of different core-body temperatureamplitude in DLB compared to AD is difficult to interpretbecause of the fact that core-body temperature amplitudein DLB is the same as that seen in controls. It is possiblethat the endogenous circadian rhythm of core-body temper-ature in patients with DLB is simply not different from con-trols and, instead, it is the patients with AD who have anincreased amplitude of their endogenous circadian rhythm.While this finding would appear to support the hypothesisthat Alzheimer patients and DLB patients have different cir-cadian disturbances, there are compelling explanations thatwould not require circadian change. Differences in the levelsand distribution of locomotor activity, and other confound-
D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781 779
Fig. 4. Amplitude (A) and acrophase (B) of three day recordings of the circadian rhythm of core-body temperature in normal controls, patients withAlzheimer’s disease and patients with Lewy body dementia with and without Alzheimer pathology. Measures are as determined by two-harmonic,multioscillator, cosinor analysis.∗P < 0.05 compared to controls;†P < 0.05 when compared to other dementia diagnosis by Tukey post-hoc test. Lewybody dementia+ AD pathology ( ); Lewy body dementia− AD pathology ( ).
ing variables, which mask core-body temperature, such asagitated pacing in AD, could help explain the differences inamplitude between DLB and controls and that of Alzheimerpatients. While this difference would support the experi-mental hypothesis of disease-specific and not environmentalalterations leading to sleep and behavioral disturbance, thesource of the difference between the dementia groups maynot necessarily be circadian. Only a study where locomo-tor activity is tightly controlled in all of the groups, and allof the subjects are studied in the same environment, will beable to definitively address these questions.
Circadian phase, of both activity and temperature, was notsignificantly different between patients with AD and patients
with DLB although both were delayed relative to normalcontrols. This finding suggests that the pathological mech-anisms involved in circadian phase change in DLB may besimilar to those in AD, and they are probably due to cel-lular changes in the SCN[18]. However, a second hypoth-esis should also be considered where merely generalized,non-specific, central degeneration could be responsible forthese circadian effects. Further stereological studies on neu-ronal subpopulations in the SCN may clarify this findingand potentially contribute to a functional understanding ofthis structure.
AD and DLB have a complex interaction in pathological,as well as clinical, symptomatology. Clinical signs of DLB

780 D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781
can also be caused by the presence of neurofibrillary tangles(NFT) in the substantia nigra[20] as opposed to the Lewybodies generally found concentrated in this structure. In thisstudy, we did not evaluate these clinical signs or quantifyNFT in the substantia nigra. It is, therefore, not possibleto comment on the impact of the presence of Lewy bodiescompared to the impact of other forms of damage fromneurofibrillary tangles in patients with AD in the substantianigra or other structures where Lewy bodies are frequentlyconcentrated. It is, however, possible that the destruction ofthe catecholaminergic system that can occur in DLB couldhave an impact on the maintenance of circadian rhythmicityin these patients separate from its effect of lowered motoractivity affecting core-body temperature[36].
Complexity is also added by the presence of beta-amyloidin both AD and DLB. Since elements of the circadian dis-turbance seen in AD and DLB were remarkably similar, par-ticularly phase delay, it is possible that the overexpressionof beta-amyloid is responsible for creating the conditionsunder which these abnormalities are seen. In rats, whoseSCN was grafted with cells that overexpress beta/A4 amy-loid, circadian rhythms were markedly disturbed, suggestinga possible specific role for amyloidosis in circadian dysreg-ulation [32]. A deeper understanding of these interactionswill require further comparisons of the clinical symptomsof the disorder with postmortem neuropathological exami-nation. Additional postmortem assessment of the substan-tia nigra could be of benefit in understanding the relativecontributions of Lewy bodies, NFT and amyloid plaques ingenerating these symptoms.
This study was carried out under normal, ambulatory,ward conditions. “Masking” effects of light, activity, meal-times, etc. on the endogenous core-body temperaturerhythm mean that any estimate of phase or amplitude inthese patient are relative to those conditions. Therefore,estimates of circadian phase or amplitude do not representthe true “endogenous” circadian phase or “endogenous”circadian amplitude. Understanding the usefulness of cir-cadian assessment for dementia diagnosis or treatment ofsleep disturbance will need to be informed by studies thatremove these masking influences as much as possible in thispopulation.
Acknowledgments
Supported by grants AG20654 (Dr. Harper) and AG09301(Drs. Satlin and Volicer) and AG13846 (Dr. Volicer) fromthe National Institute on Aging, Bethesda, MD, and by grantNIRG 2135 from the Alzheimer’s Association (Dr. Harper)and by the Department of Veteran’s Affairs, Washington,DC. Presented in part at the Society for Neuroscience An-nual Meeting, New Orleans, LA November 4, 2000 and the8’th International Conference on Alzheimer’s Disease andRelated Disorders, Stockholm, Sweden, July 21, 2002. Theauthors wish to thank Dr. Anna Wirz-Justice and Jennifer
Clarke Byington for helpful discussions and commentary onthe manuscript.
References
[1] Ancoli-Israel S, Jones DW, Hanger MA, Parker L, Klauber MR,Kripke DF. Sleep in the nursing home. In: Kuna ST, Suratt PM,Remmers JE, editors. Sleep and respiration in ageing adults. NewYork: Elsevier; 1991. p. 77–84.
[2] Bancher C, Braak H, Fischer P, Jellinger KA. Neuropathologicalstaging of Alzheimer lesions and intellectual status in Alzheimer’sand Parkinson’s disease patients. Neurosci Lett 1993;162:179–82.
[3] Bancher C, Jellinger K, Lassmann H, Fischer P, Leblhuber F.Correlations between mental state and quantitative neuropathologyin the Vienna Longitudinal Study on Dementia. Eur Arch PsychiatryClin Neurosci 1996;246:137–46.
[4] Boeve BF, Silber MH, Ferman TJ, Kokmen E, Smith GE, IvnikRJ, et al. REM sleep behavior disorder and degenerative dementia:an association likely reflecting Lewy body disease. Neurology1998;51:363–70.
[5] Borbely AA. A two process model of sleep regulation. HumNeurobiol 1982;1:195–204.
[6] Braak H, Braak E. Neuropathological stageing of Alzheimer-relatedchanges. Acta Neuropathol (Berl) 1991;82:239–59.
[7] Braak H, Braak E. Staging of Alzheimer’s disease-relatedneurofibrillary changes. Neurobiol Aging 1995;16:271–8;discussion278–84.
[8] Buysse DJ, Monk TH, Reynolds CFd, Mesiano D, Houck PR, KupferDJ. Patterns of sleep episodes in young and elderly adults during a36-h constant routine. Sleep 1993;16:632–7.
[9] Campbell SS, Kripke DF, Gillin JC, Hrubovcak JC. Exposure tolight in healthy elderly subjects and Alzheimer’s patients. PhysiolBehav 1988;42:141–4.
[10] Consensus Report of the Working Group on Molecular andBiochemical Markers of Alzheimer’s Disease. The Ronald andNancy Reagan Research Institute of the Alzheimer’s Association andthe National Institute on Aging Working Group. Neurobiol Aging1998;19:109–16.
[11] Dijk DJ, Duffy JF, Riel E, Shanahan TL, Czeisler CA. Ageingand the circadian and homeostatic regulation of human sleep duringforced desynchrony of rest, melatonin and temperature rhythms [InProcess Citation]. J Physiol Lond 1999;516:611–27.
[12] Duffy JF, Dijk DJ, Klerman EB, Czeisler CA. Later endogenouscircadian temperature nadir relative to an earlier wake time in olderpeople. Am J Physiol 1998;275:R1478–87.
[13] Ferman TJ, Boeve BF, Smith GE, Silber MH, Kokmen E, PetersenRC, Ivnik RJ. REM sleep behavior disorder and dementia: cognitivedifferences when compared with AD. Neurology 1999;52:951–7.
[14] Gold G, Bouras C, Kovari E, Canuto A, Glaria BG, Malky A,Hof PR, Michel JP, Giannakopoulos P. Clinical validity of Braakneuropathological staging in the oldest-old. Acta Neuropathol (Berl)2000;99:579–82;discussion 574–583.
[15] Gomez-Tortosa E, Irizarry MC, Gomez-Isla T, Hyman BT. Clinicaland neuropathological correlates of dementia with Lewy bodies. AnnNY Acad Sci 2000;920:9–15.
[16] Grace JB, Walker MP, McKeith IG. A comparison of sleep profilesin patients with dementia with lewy bodies and Alzheimer’s disease.Int J Geriatr Psychiatry 2000;15:1028–33.
[17] Hansen LA, Masliah E, Galasko D, Terry RD. Plaque-only Alzheimerdisease is usually the lewy body variant, and vice versa. J NeuropatholExp Neurol 1993;52:648–54.
[18] Harper DG, Stopa EG, McKee A, Satlin A, Harlan PC, GoldsteinRL, et al. Differential circadian rhythm disturbances in men withAlzheimer disease and frontotemporal degeneration. Arch GenPsychiatry 2001;58:353–60.
D.G. Harper et al. / Neurobiology of Aging 25 (2004) 771–781 781
[19] Lauer CJ, Riemann D, Wiegand M, Berger M. From early to lateadulthood. Changes in EEG sleep of depressed patients and healthyvolunteers. Biol Psychiatry 1991;29:979–93.
[20] Liu Y, Stern Y, Chun MR, Jacobs DM, Yau P, Goldman JE.Pathological correlates of extrapyramidal signs in Alzheimer’sdisease. Ann Neurol 1997;41:368–74.
[21] Loewenstein RJ, Weingartner H, Gillin JC, Kaye W, Ebert M,Mendelson WB. Disturbances of sleep and cognitive functioning inpatients with dementia. Neurobiol Aging 1982;3:371–7.
[22] Londos E, Passant U, Gustafson L, Brun A. Neuropathologicalcorrelates to clinically defined dementia with Lewy bodies. Int JGeriatr Psychiatry 2001;16:667–79.
[23] McKee AC. Brain banking: basic science methods. Alzheimer DisAssoc Disord 1999;13(Suppl 1):S39–44.
[24] McKeith IG, Galasko D, Kosaka K, Perry EK, Dickson DW,Hansen LA, et al. Consensus guidelines for the clinical andpathologic diagnosis of dementia with Lewy bodies (DLB): reportof the consortium on DLB international workshop. Neurology1996;47:1113–24.
[25] Mirra SS, Heyman A, McKeel D, Sumi SM, Crain BJ, BrownleeLM, et al. The Consortium to Establish a Registry for Alzheimer’sDisease (CERAD). Part II. Standardization of the neuropathologicassessment of Alzheimer’s disease. Neurology 1991;41:479–86.
[26] Pawlak C, Blois R, Gaillard JM, Richard J. La Sommeille dans lamaladie Picks. Encephale 1986;12:327–34.
[27] Pollak CP, Perlick D. Sleep problems and institutionalization of theelderly. J Geriatr Psychiatry Neurol 1991;4:204–10.
[28] Prinz PN, Peskind ER, Vitaliano PP, Raskind MA, Eisdorfer C,Zemcuznikov N, et al. Changes in the sleep and waking EEGsof nondemented and demented elderly subjects. J Am Geriatr Soc1982;30:86–93.
[29] Roman GC, Tatemichi TK, Erkinjuntti T, Cummings JL,Masdeu JC, Garcia JH, et al. Vascular dementia: diagnosticcriteria for research studies. Report of the NINDS-AIRENInternational Workshop [see comments]. Neurology 1993;43:250–60.
[30] Satlin A, Volicer L, Stopa EG, Harper D. Circadian locomotoractivity and core-body temperature rhythms in Alzheimer’s disease.Neurobiol Aging 1995;16:765–71.
[31] Shochat T, Martin J, Marler M, Ancoli-Israel S. Illumination levelsin nursing home patients: effects on sleep and activity rhythms. JSleep Res 2000;9:373–9.
[32] Tate B, Aboody-Guterman KS, Morris AM, Walcott EC, MajochaRE, Marotta CA. Disruption of circadian regulation by brain graftsthat overexpress Alzheimer beta/A4 amyloid. Proc Natl Acad SciUSA 1992;89:7090–4.
[33] Teicher MH, Barber NI. COSIFIT: an interactive program forsimultaneous multioscillator cosinor analysis of time-series data.Comput Biomed Res 1990;23:283–95.
[34] Van Cauter E, Plat L, Leproult R, Copinschi G. Alterations ofcircadian rhythmicity and sleep in aging: endocrine consequences.Horm Res 1998;49:147–52.
[35] van Someren EJ, Hagebeuk EE, Lijzenga C, Scheltens P,de Rooij SE, Jonker C, et al. Circadian rest–activity rhythmdisturbances in Alzheimer’s disease. Biol Psychiatry 1996;40:259–70.
[36] Weinert D, Waterhouse J. Diurnally changing effects of locomotoractivity on body temperature in laboratory mice. Physiol Behav1998;63:837–43.
[37] Witting W, Kwa IH, Eikelenboom P, Mirmiran M, Swaab DF.Alterations in the circadian rest–activity rhythm in aging andAlzheimer’s disease. Biol Psychiatry 1990;27:563–72.