Embed Size (px)
Citation preview
DEMENTIA
Prof. Abdulkader Daif
Consultant Neurologist
2011
Cognitive Disorders (DSM-IV)Cognitive Disorders (DSM-IV)
1.1.DementiaDementia
2. Delirium2. Delirium
3. Amnesic Disorder3. Amnesic Disorder
CognitionCognition
Brain functions including:Brain functions including:
AttentionAttention InitiationInitiation
MemoryMemory LanguageLanguage
CalculationCalculation PraxisPraxis
Executive functionsExecutive functions
Visuospatial capacityVisuospatial capacity
Time and space orientationTime and space orientation

Cognitive Disorders: DementiaCognitive Disorders: Dementia
DementiaDementiaDementiaDementia •Clinical condition/syndromeClinical condition/syndrome•Loss of cognitive functionLoss of cognitive function•Interferes with normal activitiesInterferes with normal activities•Interferes with social relationshipsInterferes with social relationships
Common signs
1. Impairment of memory2. Multiple disturbances of cognition3. Impairment of executive function.4. Disorientation.5. Behavioral changes.
Definition of DementiaDefinition of Dementia

Normal cognitive decline vs. DementiaNormal cognitive decline vs. Dementia
Cognitive function declines with age:Cognitive function declines with age:Slower learning curveSlower learning curve
Slower reaction timeSlower reaction time
Decreased/slower working memory and Decreased/slower working memory and frontal functionsfrontal functions
Maintenance of vocabulary and Maintenance of vocabulary and grammatical structuresgrammatical structures
When compared to younger adultsWhen compared to younger adults
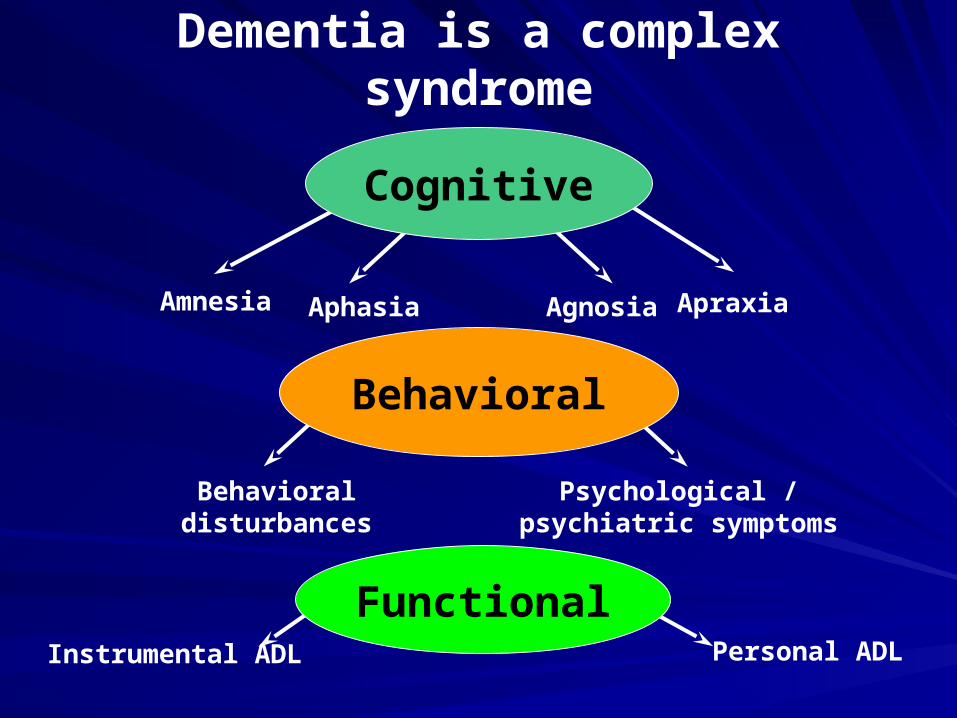
Dementia is a complex syndrome
Psychological / psychiatric symptoms
Behavioral
Behavioral disturbances
Amnesia ApraxiaAgnosiaAphasia
Functional
Cognitive
Instrumental ADL Personal ADL

Dementia? Reversible causes?
Depression? Delirium?
MCI ? CIND?
Acute onsetStepwise
Risk factorsGait
Neurological
Gradual onsetMemory loss
Normal examination
HallucinationsFluctuationsVisuospatial
Parkinsonism
BehaviouralLanguageFamily hx
Young onset
Frontotemporal Dementia
Lewy Body Dementia
Alzheimer’sDisease
Vascular Dementia

Dementia: CausesDementia: Causes
1.1.ReversibleReversible
2. Irreversible2. Irreversible
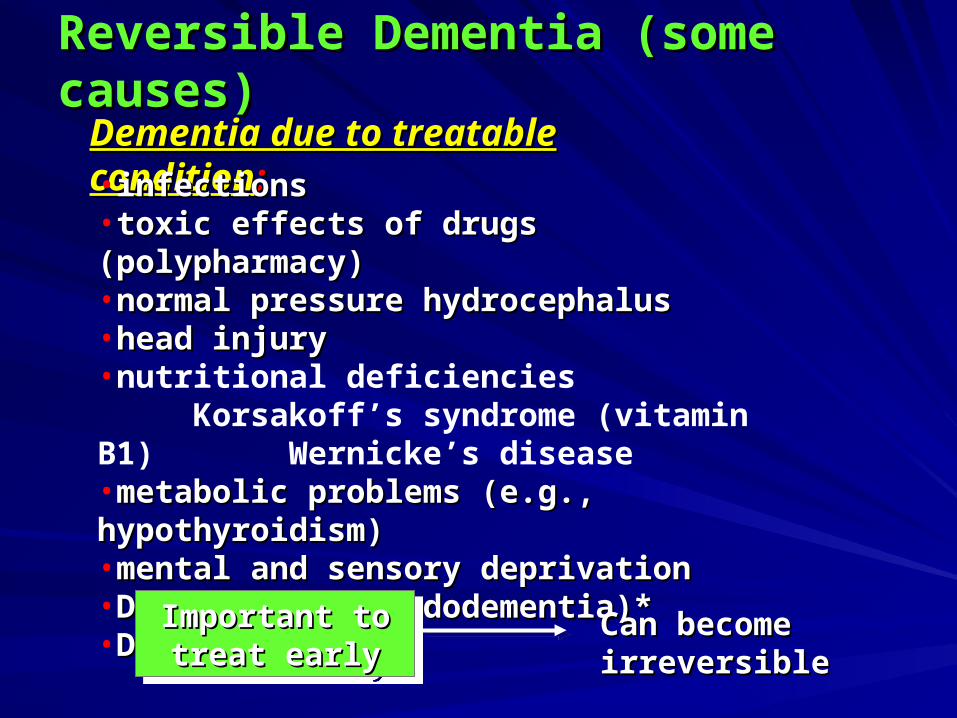
Reversible Dementia (some causes)Reversible Dementia (some causes)
Dementia due to treatable conditionDementia due to treatable condition::•infectionsinfections•toxic effects of drugs (polypharmacy)toxic effects of drugs (polypharmacy)•normal pressure hydrocephalusnormal pressure hydrocephalus•head injuryhead injury•nutritional deficiencies
Korsakoff’s syndrome (vitamin B1)Wernicke’s disease
•metabolic problems (e.g., hypothyroidism)metabolic problems (e.g., hypothyroidism)•mental and sensory deprivationmental and sensory deprivation•Depression (pseudodementia)*Depression (pseudodementia)*•Delirium*Delirium*
Important to Important to treat earlytreat early
Important to Important to treat earlytreat early
Can become Can become irreversibleirreversible

Causes of DementiaCauses of Dementia
65%10%
7%
5%
5%8% Alzheimer's Disease (AD): 65%
AD & Vascular: 10%
Lewy body: 7%
AD and Lewy body: 5%
Vascular: 5%
Other: 8%
WISCONSIN ALZHEIMER’S INSTITUTE
14

Prevalence of dementia in Canada: Canadian Prevalence of dementia in Canada: Canadian Study of Health and Aging (1991-1992)Study of Health and Aging (1991-1992)
Female to male ratio is 2:1Female to male ratio is 2:1
2.4 % for 65-74 years2.4 % for 65-74 years
34.5% for those aged 85+34.5% for those aged 85+

Prevalence of Alzheimer’s Disease and Prevalence of Alzheimer’s Disease and Vascular Dementia in CanadaVascular Dementia in Canada
Alzheimer’s Alzheimer’s 5.1%5.1% for 65+ for 65+– 1.0% for 65-74 years1.0% for 65-74 years– 26% for 85+ years26% for 85+ years
Vascular dementia Vascular dementia 1.5%1.5% for 65+ for 65+– 0.6 % for 65-74 years0.6 % for 65-74 years– 4.8 % for 85+ years4.8 % for 85+ years

Vascular Dementia: DiagnosisVascular Dementia: Diagnosis
Diagnostic criteria of memory decline, loss of Diagnostic criteria of memory decline, loss of functioning similar to AD, but:functioning similar to AD, but:Requires presence of focal neurologic deficits Requires presence of focal neurologic deficits reflecting a CVA or multiple cerebrovascular risk reflecting a CVA or multiple cerebrovascular risk factorsfactors
HypertensionHypertensionCoronary artery diseaseCoronary artery diseaseHypercholesterolemiaHypercholesterolemiaObesityObesityType II diabetesType II diabetes
EpidemiologyEpidemiology– Second most common cause of dementia next to AD.Second most common cause of dementia next to AD.
Vascular DementiaVascular Dementia
SymptomsSymptoms– Mood labilityMood lability– Stepwise course of illnessStepwise course of illness
May plateauMay plateau
Course is more variable than the progression of Course is more variable than the progression of ADAD
– Multiple medications and comorbid illnesses Multiple medications and comorbid illnesses associated with the vascular risk factors associated with the vascular risk factors increase vulnerability to delirium (confusion).increase vulnerability to delirium (confusion).
FeaturesFeatures
•Associated with damage to the cerebral blood vessels Associated with damage to the cerebral blood vessels through arteriosclerosisthrough arteriosclerosis•found in middle and later life (age of onset between 50-70)found in middle and later life (age of onset between 50-70)•accumulated effect of multiple cortical and subcortical infarctsaccumulated effect of multiple cortical and subcortical infarctslead to clinical presentationlead to clinical presentation•incidence higher in menincidence higher in men•first sign delirium or small strokefirst sign delirium or small stroke
Dementia: Vascular DementiaDementia: Vascular Dementia

Vascular DementiaVascular Dementia
MRI Imaging:Periventricular hyperintensitiesVentricular capping“Small vessel ischemia”
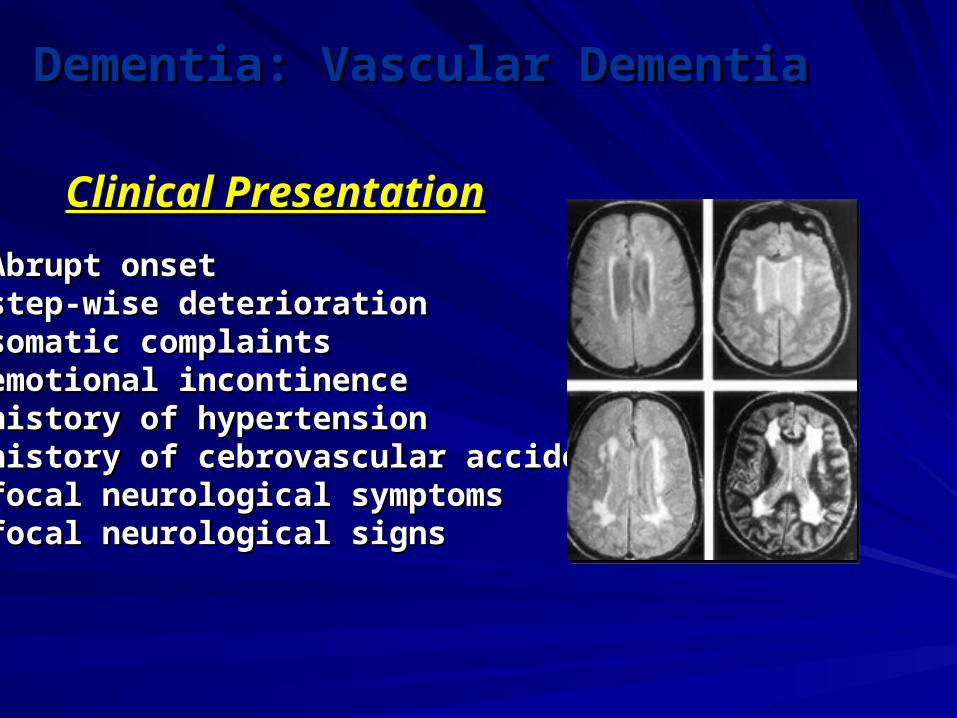
Clinical PresentationClinical Presentation
•Abrupt onsetAbrupt onset•step-wise deteriorationstep-wise deterioration•somatic complaintssomatic complaints•emotional incontinenceemotional incontinence•history of hypertensionhistory of hypertension•history of cebrovascular accidentshistory of cebrovascular accidents•focal neurological symptomsfocal neurological symptoms•focal neurological signsfocal neurological signs
Dementia: Vascular DementiaDementia: Vascular Dementia

Management of vascular dementiaManagement of vascular dementia
Risk assessment Risk assessment
– Age, hypertension, smoking, diabetes, history of Age, hypertension, smoking, diabetes, history of stroke/TIAstroke/TIA
Reduction of risk of further damageReduction of risk of further damage
– Management of stroke and risk factorsManagement of stroke and risk factors
Treatment of secondary conditionsTreatment of secondary conditions11
– Depression, anxiety, agitationDepression, anxiety, agitation
Treatment of dementia symptomsTreatment of dementia symptoms
– Cognition, global function, activities of daily livingCognition, global function, activities of daily living1Gupta A, et al. Int J Clin Pract. 2002;56:531-537.

•Patient Auguste D. had dementia Patient Auguste D. had dementia symptomssymptoms•Brain studies after her death revealed Brain studies after her death revealed microscopic changes microscopic changes
Alois Alzheimer (1864-1915)Alois Alzheimer (1864-1915)
•Symptoms due to neuronal changesSymptoms due to neuronal changes
Dementia:Dementia:Alzheimer’s Disease HistoryAlzheimer’s Disease History
•DementiaDementia•Significant cognitive deficienciesSignificant cognitive deficiencies•Progressive deteriorationProgressive deterioration•No loss of consciousnessNo loss of consciousness•40-90 years of age40-90 years of age•No other diseasesNo other diseases
Criteria for probable Alzheimer’s diagnosis=Criteria for probable Alzheimer’s diagnosis=
Also includesAlso includes
•Medical testsMedical tests•Family historyFamily history•Brain scansBrain scans•Other symptomsOther symptoms
Dementia and Related Neurological Dementia and Related Neurological Disorders: Disorders: Alzheimer’s DiseaseAlzheimer’s Disease
EarlyEarly
MiddleMiddle
LateLate
Memory loss for familiar Memory loss for familiar objects and eventsobjects and events
Personality changesPersonality changesBehavior changesBehavior changes
Loss of ability to perform simple Loss of ability to perform simple everyday functionseveryday functions
Regular progressionof loss
Alzheimer’s Disease: “Stages” of ProgressionAlzheimer’s Disease: “Stages” of Progression
Psychological SymptomsPsychological Symptoms
People do not die of Alzheimer’s per se.People do not die of Alzheimer’s per se.
Clinical PresentationClinical Presentation::
•Memory lossMemory loss•AphasiaAphasia•ApraxiaApraxia•AgnosiaAgnosia•Disturbance in executive functioningDisturbance in executive functioning
Diagnosisdone byexclusion
Diagnosisdone byexclusion
Autopsy is onlyAutopsy is onlyreliable methodreliable method
Pathologic Hallmarks of ADPathologic Hallmarks of AD
Neurofibrillary Tangles (NFT)Neurofibrillary Tangles (NFT)– Cytoskeletal proteinCytoskeletal protein– Hyperphosphorylated Tau proteinHyperphosphorylated Tau protein
Neuritic PlaquesNeuritic Plaques– Extracellular compacted insoluble amyloid Extracellular compacted insoluble amyloid
proteinprotein– AAßß4242 peptide – abnormal secretase cleavage peptide – abnormal secretase cleavage– Neurotoxic propertiesNeurotoxic properties

CSF Amyloid and TauCSF Amyloid and TauCSFCSF– AAßß4242 levels (not total Aß) are levels (not total Aß) are reducedreduced in CSF in AD in CSF in AD
compared to other dementias or control subjects.compared to other dementias or control subjects.Reduction due to insolubility of Aß42 in plaquesReduction due to insolubility of Aß42 in plaques
CSF Tau CSF Tau – ElevatedElevated in AD relative to controls in AD relative to controls– BUT also elevated in patients with other neurologic diseasesBUT also elevated in patients with other neurologic diseases
Current ConsenusCurrent Consenus– Combination of ACombination of Aß and Tau better than either aloneß and Tau better than either alone
Knopman D, Arch. Neurol, 58; 2001.Knopman D, Arch. Neurol, 58; 2001.

AD Etiology – microscopic
Neuritic PlaquesNeurofibrillary Tangles
Amyloid
Beta-amyloid deposits
Secretase
Tau microtubules hyperphosphorylation & collapse
MAP protein

Amyloid PlaquesAmyloid Plaques
•Collection of waste Collection of waste products of dead neurons products of dead neurons around a core of around a core of amyloid.amyloid.•Formation occurs long Formation occurs long before symptoms are before symptoms are evidentevident
•Amyloid-42 most common form found in plaquesAmyloid-42 most common form found in plaques
Alzheimer’s DiseaseAlzheimer’s Disease
Amyloid plaqueAmyloid plaque

Tangles and Plaques
http://www.ahaf.org/alzdis/about/AmyloidPlaques.htm

Neurofibrillary TanglesNeurofibrillary Tangles
•Made up of tau proteinMade up of tau protein•Tau maintains microtubules Tau maintains microtubules within axonswithin axons•Tangles form when tau Tangles form when tau changes chemically and can changes chemically and can no longer support the no longer support the microtubulesmicrotubules•Leads to collapse of Leads to collapse of transport system within transport system within neuronneuron
Neurofibrillarytangle
Neurofibrillarytangle
Alzheimer’s DiseaseAlzheimer’s Disease

http://www.alzheimers.org/tangle.html
Neurofibrillary TanglesNeurofibrillary Tangles
Alzheimer’s DiseaseAlzheimer’s Disease

EnvironmentalEnvironmental
Life styleLife style Head injury Head injury •Twin dataTwin data•Japanese men who moved Japanese men who moved to Hawaiito Hawaii•Nun Study on mental Nun Study on mental activityactivity
•Severe injuries Severe injuries involving loss of involving loss of consciousnessconsciousness•Causes damage to Causes damage to neuronsneurons
Alzheimer’s DiseaseAlzheimer’s Disease
Causes of Alzheimer’s DiseaseCauses of Alzheimer’s Disease

Genetic theoryGenetic theoryGenetic theoryGenetic theoryFamilial Familial Alzheimer’s Alzheimer’s DiseaseDisease
Familial Familial Alzheimer’s Alzheimer’s DiseaseDisease
ApoE gene 19
APP gene 21
PresenilinPresenilin 11 1414
Presenilin 2 1
GeneGene ChromosomeChromosome
•Early onsetEarly onset•Late onsetLate onset
supports
Alzheimer’s DiseaseAlzheimer’s Disease
Causes of Alzheimer’s DiseaseCauses of Alzheimer’s Disease
Majority of early-onset cases
Majority of early-onset cases
Genes and Alzheimer’s disease(60% - 80 % of causation)
(all known genes relate to amyloid)
Familial AD (onset < 60 y/o) (<5%)– Presenilin I, II (ch 14, 1)– APP (ch 21)
Non-familial (late onset)– APOE
Clinical studies suggest 40 – 50% due to 4If is considered, may be 95% of causation
Population studies suggest 10 – 20% cause
Evolution over last 300,000 to 200,000 years
– At least 20 other genes

Risk Factors
Advanced age
4-allele of apolipoprotein E-Gene (ApoE)
Female gender?

Focal neurodegenerative dementias: Focal neurodegenerative dementias: Frontotemporal Lobar Degeneration (FTLDFrontotemporal Lobar Degeneration (FTLD))
Focal neurodegenerative diseases, Focal neurodegenerative diseases, affecting primarily temporal and frontal affecting primarily temporal and frontal lobes:lobes:
1. Fronto-temporal dementia1. Fronto-temporal dementia
2. Primary progressive aphasia2. Primary progressive aphasia
3. Semantic dementia3. Semantic dementia

Pick’s Disease -1892 Arnold Pick
Frontotemporal dementia– Frontal lobar atrophy– Pick’s bodies – tau
protein– Chr 17 abnormality

FTLD - General FeaturesFTLD - General Features
1. Pre-senile dementias (<65 years of age)1. Pre-senile dementias (<65 years of age)
2. SPECT Scan: Anterior (frontotemporal 2. SPECT Scan: Anterior (frontotemporal defects)defects)
3. Normal EEG3. Normal EEG
4. Memory and visuospatial functions are 4. Memory and visuospatial functions are normal until the disease is advancednormal until the disease is advanced

Pick’s diseasePick’s disease
Non-specific frontal degenerationNon-specific frontal degeneration
Frontal degeneration with anterior spinal Frontal degeneration with anterior spinal neuron lossneuron loss
FTD: Pathological TypesFTD: Pathological Types
FTD: Clinical Features (I)FTD: Clinical Features (I)
Behavioral abnormalities. Behavioral abnormalities.
Inertia, loss of volition, decreased initiative.Inertia, loss of volition, decreased initiative.
Social disinhibition, loss of insight.Social disinhibition, loss of insight.
Impulsivity, overactivity.Impulsivity, overactivity.
Emotional blunting.Emotional blunting.
Stereotyped and perseverative behavior.Stereotyped and perseverative behavior.
FTD: Clinical Features (II)FTD: Clinical Features (II)
Mean age of presentation: 53 yearsMean age of presentation: 53 years
Predominantly malesPredominantly males
High familial aggregationHigh familial aggregation
Cognitive impairment mostly in areas of executive function (planning, Cognitive impairment mostly in areas of executive function (planning, judgement, problem-solving) and attentionjudgement, problem-solving) and attention
Memory, visuospatial and calculation might be relatively preserved at the Memory, visuospatial and calculation might be relatively preserved at the beginningbeginning
Speech might be either economical leading to mutism, or increased / Speech might be either economical leading to mutism, or increased / pressed in disinhibited patientspressed in disinhibited patients
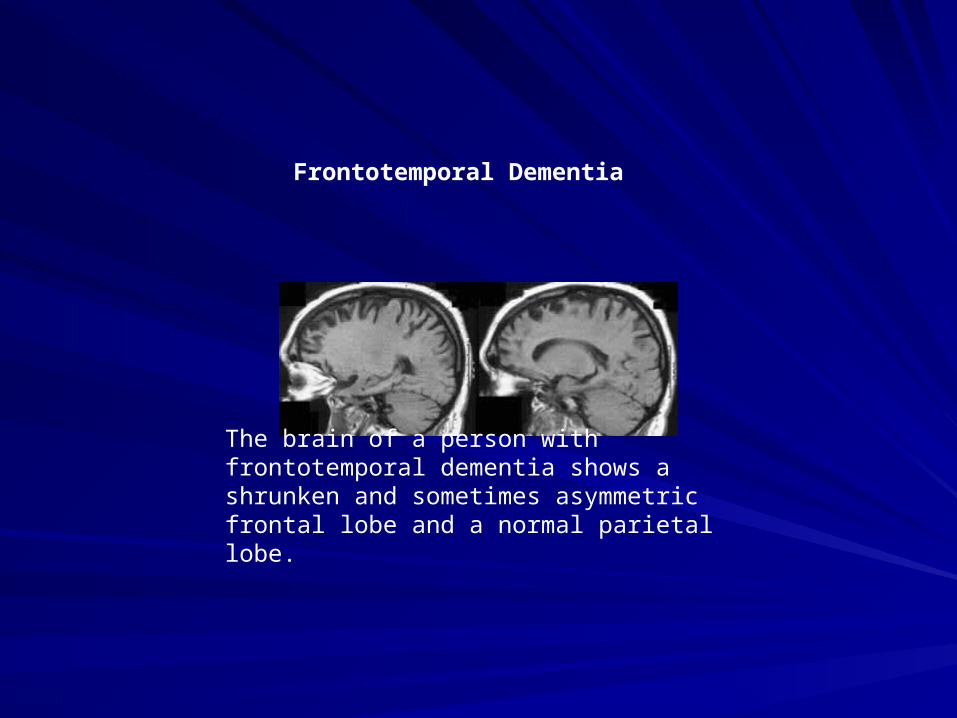
The brain of a person with frontotemporal dementia shows a shrunken and sometimes asymmetric frontal lobe and a normal parietal lobe.
Frontotemporal Dementia

4242
May appear similar to Alzheimer’s…..Early treatment may reverse cognitive changes before they become permanentTriad of symptoms: gait instability, urinary incontinence and dementia – Wide-based, shuffling gait with poor coordination– Incontinence follows gait change, includes urgency– Slow thinking/response, decreased spontaneity
Enlarged ventricles on MRI– But no evidence of atrophy: Alzheimer’s shows large
ventricles due to brain atrophy
Normal-Pressure HydrocephalusNormal-Pressure Hydrocephalus

MRI: Hydrocephalus

Dementia with Lewy BodiesDementia with Lewy Bodies
Cortical Lewy Bodies on pathCortical Lewy Bodies on pathOverlap with AD and PDOverlap with AD and PDFluctuations in mental status (may appear Fluctuations in mental status (may appear delirious)delirious)Early delusions and hallucinationsEarly delusions and hallucinationsMild extrapyramidal signsMild extrapyramidal signsNeuroleptic hypersensitivity!!!Neuroleptic hypersensitivity!!!Unexplained falls or transient changes in Unexplained falls or transient changes in consciousnessconsciousness

Dementia with Lewy Bodies (DLB)
Etiology– Lewy bodies – protein deposits containing
damaged neurons
Symptoms: decline in– memory – language – Judgment & reasoning
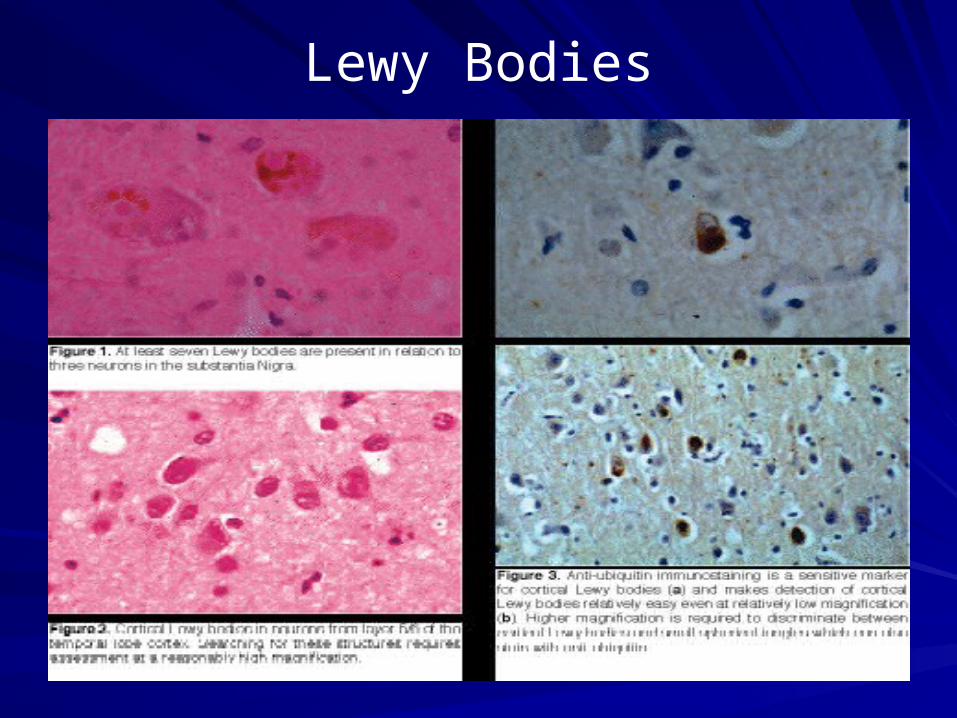
Lewy Bodies

AIDS dementia complexAIDS dementia complex
Approximately two-thirds of persons with AIDS develop dementia, mostly due to AIDS dementia complex.In some patients HIV is found in the CNS at postmortem. In others an immune mechanism or an unidentified pathogen is blamed.Dementia is initially of a "subcortical " type.CT - atrophy; MRI - increased T2 signal from white matter.Treatment with Zidovudine (AZT) halts and partially revers neuropsychological deficit.

Differential DiagnosisDifferential DiagnosisDelirium DementiaDelirium Dementia
Rapid onsetRapid onset
marked attentional marked attentional disturbancedisturbance
confusion confusion prominent/clouding of prominent/clouding of consciousnessconsciousness
fluctuating clinical coursefluctuating clinical course
agitation and behavioral agitation and behavioral symptomssymptoms
potentially reversiblepotentially reversible
Usually insidious onsetUsually insidious onset
memory systems impairedmemory systems impaired
consciousness intactconsciousness intact
slower, progressive courseslower, progressive course
subtle behavioral symptomssubtle behavioral symptoms
can be irreversiblecan be irreversible

4949
MANAGEMENTMANAGEMENT.……….………

5050
SYMPTOM MANAGEMENTSYMPTOM MANAGEMENT
Psychoses (delusions, hallucinations)
Sleep disturbances
Aggression, agitation

5151
NONPHARMACOLOGICNONPHARMACOLOGIC
Cognitive enhancement
Individual and group therapy
Regular appointments
Communication with family, caregivers
Environmental modification
Attention to safety

5252
PHARMACOLOGICPHARMACOLOGICCholinesterase inhibitors:
Inhibit cholinesterase at the synaptic cleft
Offer a small improvement : cognition and activities of daily
living
Examples: donepezil, rivastigmine, galantamine
Memantine: (Namenda): N-Methyl-D-Aspartate Antagonist: A receptor activated by glutamate: decr nmda
excessive nmda: excitotoxicity and neurotransmittter damage
Memantine is neuroprotective & disease modifying;
for moderate to severe dementia
alone or in combination
Other cognitive enhancers: estrogen, NSAIDs, ginkgo, vit. E
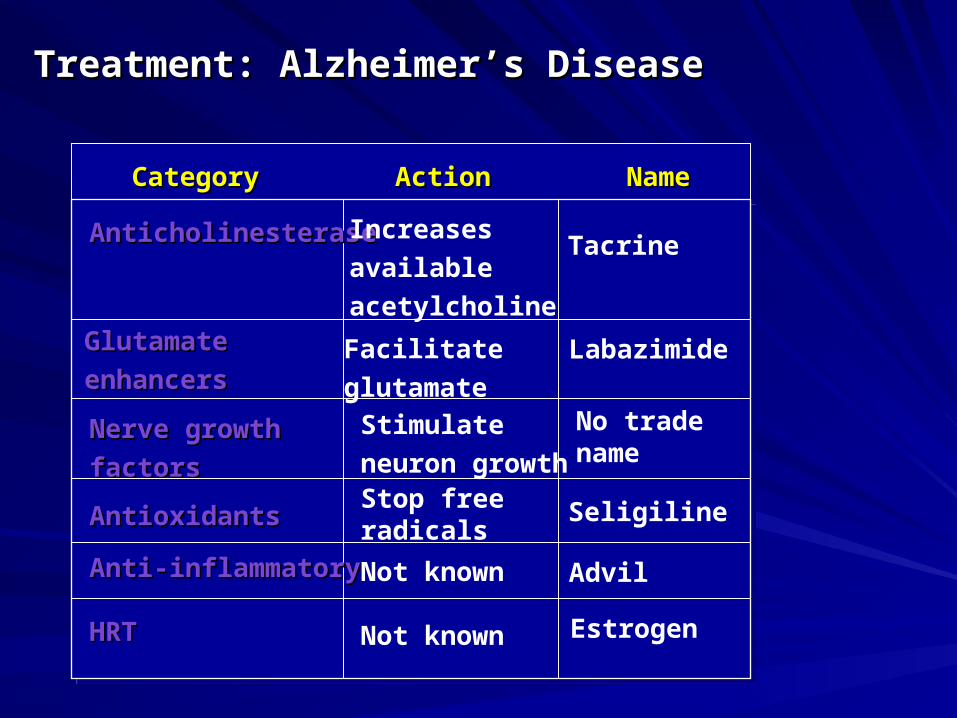
CategoryCategory
Labazimide
AnticholinesteraseAnticholinesterase
GlutamateGlutamate
enhancersenhancers
ActionAction NameName
Nerve growthNerve growth
factorsfactors
Stimulate
neuron growth
Increases
available
acetylcholine
Tacrine
No trade name
AntioxidantsAntioxidants
Anti-inflammatoryAnti-inflammatory Not known Advil
HRTHRT Not known Estrogen
Facilitate
glutamate
SeligilineStop free radicals
Treatment: Alzheimer’s DiseaseTreatment: Alzheimer’s Disease

5454
TREATING PSYCHOSIS IN TREATING PSYCHOSIS IN DEMENTIADEMENTIA
Antipsychotic medications (side effects):Higher potency: haloperidol (extrapyramidal symptoms)
Lower potency: thioridazine (anticholinergic effects, sedation, hypotension, constipation, urine retention)
Atypical antipsychotics: clozapine, risperidone, olanzapine Beware new prescribing information on some of the atypical
antipsychotics!
5555
MANAGING SLEEP MANAGING SLEEP DISTURBANCESDISTURBANCES
Improve sleep hygiene (e.g, consistent bedtime, comfortable setting)
Provide daytime activity, prevent daytime sleeping
Use bright-light therapy
Treat associated depression, delusions
If the above do not succeed, consider:trazodone 25-150 mgnefazodone 100-500 mgzolpidem 5-10 mg
Avoid benzodiazepines or antihistamines
5656
MANAGING AGITATIONMANAGING AGITATIONBehavioral interventions: distraction, supervision, routine, structure
Behavior modification using rewards
Pharmacologic interventions: antipsychotics, antidepressants, mood stabilizers, buspirone, -blockers
Avoid physical restraints

Dementia – diagnostic approachDementia – diagnostic approach