Embed Size (px)
Citation preview
Dementia & Primary Care
Dr. Robert Tobiansky (Barnet Consultant)Dr Jonathan Hare (Enfield Consultant)Dr. Michael Payne (Haringey Consultant)
Barnet, Enfield & Haringey Mental Health Trust
Overview of clinical aspects of Dementia
Definition & prevalence of Dementia Differential Diagnosis Management & investigations the role of medication, including ACHEIs Management as a GP Community services Medico-legal issues Consent & Capacity
National Dementia Strategy
Published 2 Feb 2009 Five year plan 17 interlinked objectives £150 million extra funding
Four key themes Improving awareness Early better diagnosis Improved quality of care Delivering the Strategy
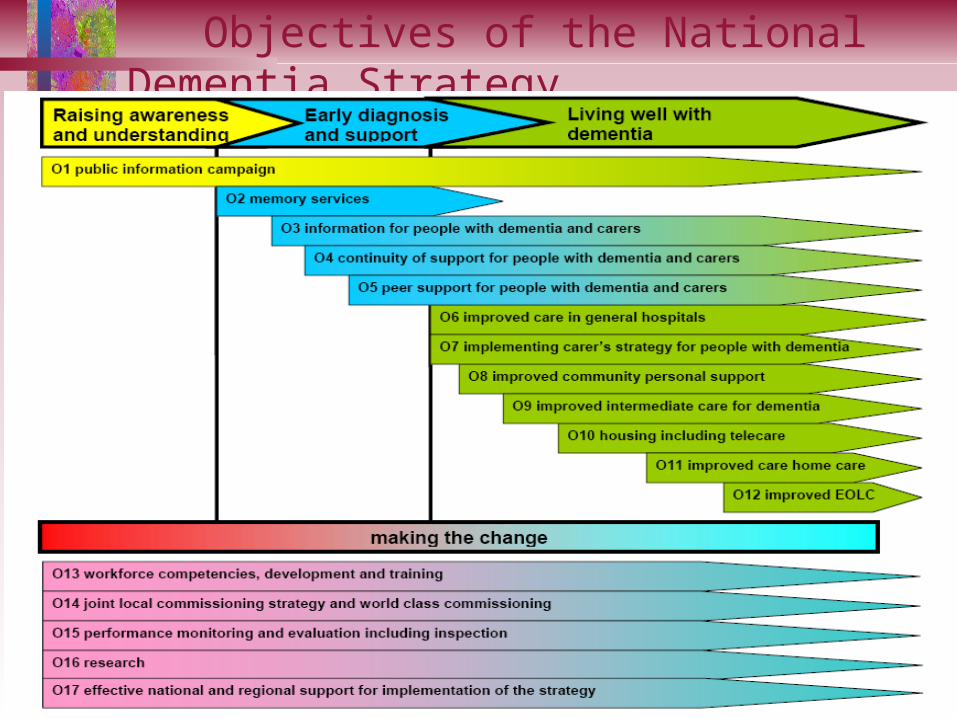
Objectives of the National Dementia Strategy
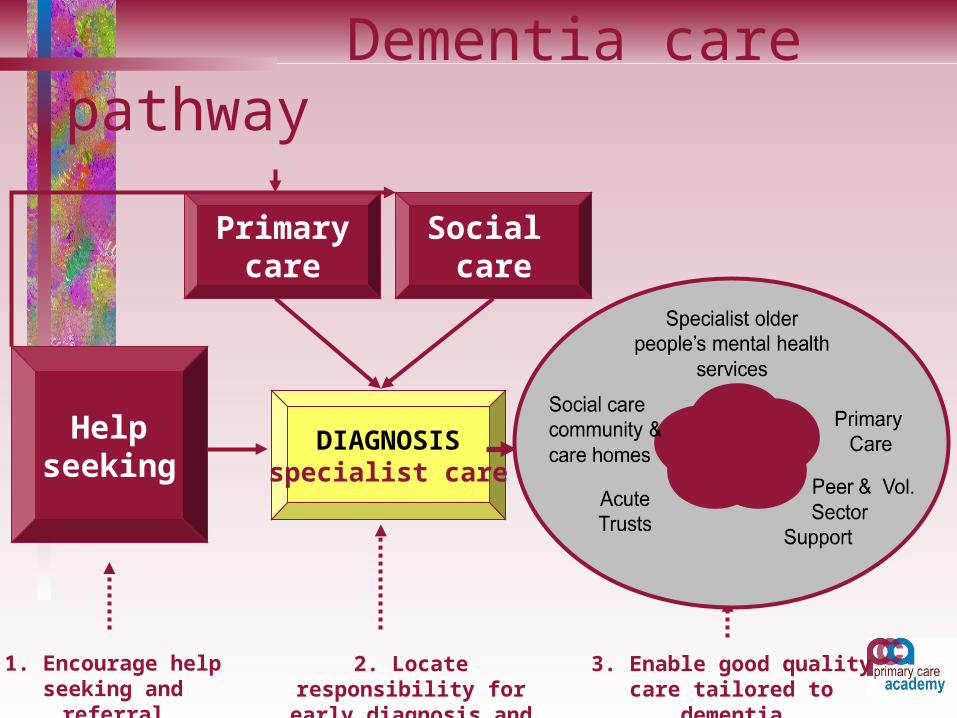
Dementia care pathway
Helpseeking
Primarycare
DIAGNOSISspecialist care
Social care
1. Encourage help seeking and referral
2. Locate responsibility for early diagnosis and
care
3. Enable good quality care tailored to
dementia

DEMENTIA: DEFINITION

Dementia A syndrome due to disease of the brain usually
of a chronic or progressive nature Multiple disturbances of higher cortical function Global impairment: intellect, memory,
personality Changes in emotional control, social behaviour,
motivation In clear consciousness Decline in usual functional abilities
EPIDEMIOLOGY OF DEMENTIA:
Nature Reviews Neurology Reitz et al 2011
Epidemiology of Dementia: Global prevalence 24 million predicted to double
every 20 years to 2040 5% over 65 years 20% over 80 years Over 65 years - prevalence doubles every 5 yrs Annual incidence c. 9 / 1000 population
Dementia: key points Prevalence increases with older age rare in < 65, if suspect in younger
patient refer to neurologist diagnosis based on History, Physical &
mental state examination & routine investigations
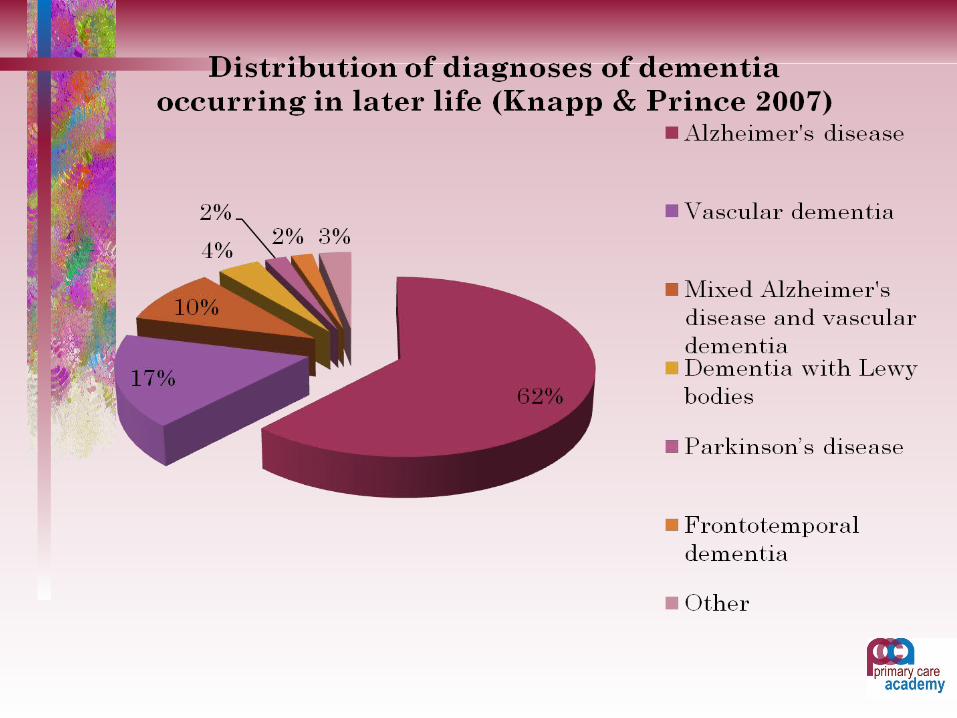
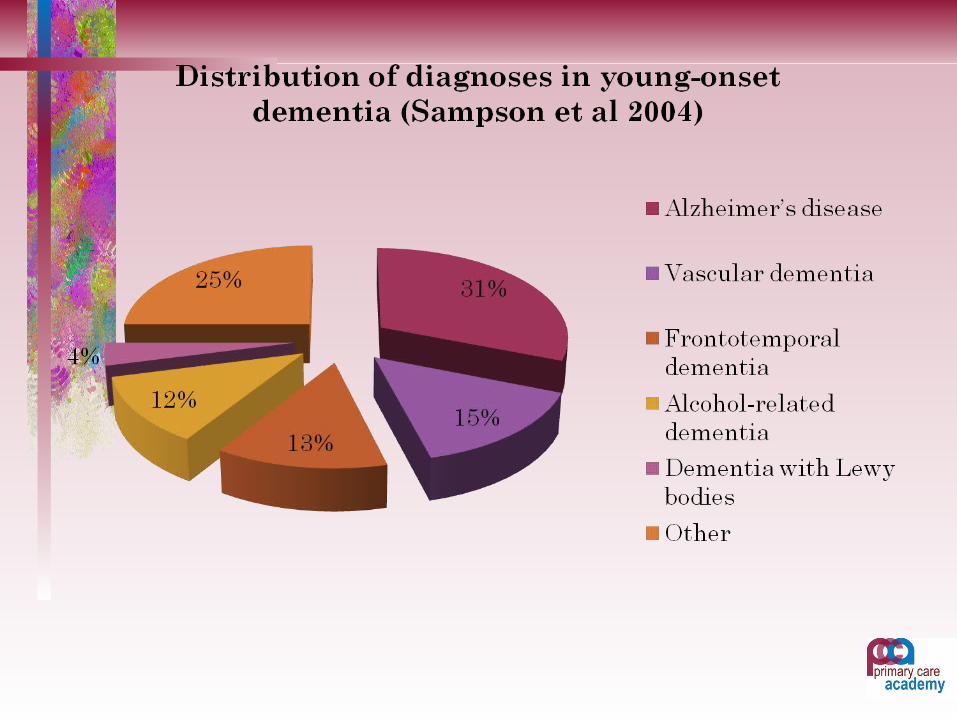
DEMENTIA: COMMONEST TYPES
DementiaMany causes but commonest are: Alzheimer’s Disease Vascular Dementia Lewy Body Dementia Alcohol related dementia Frontotemporal dementia
Alzheimer’s Disease: Neuropathology Atrophy, widened sulci, shrunken gyri Amyloid plaques: extracellular, swollen neuronal
processes with core of amyloid- Neurofibrillary tangles (NFTs): intracellular,
hyperphosphorylated Tau (microtubule assembly protein) forms insoluble aggregates = PHF
Widespread loss of neurones & synapses Granulovacuolar degeneration Gliosis, loss of dendrites Hirano bodies (eosinophilic, cigar shaped)
AD: Neurochemical changes
Best described: diminished Acetyl-Choline, CAT, cholinergic neurones (Basal n. Meynert)
Also reduction in GABA, NA, 5HT etc
Risk Factors for AD: Age Family History (genes on chromosome 21, 14, 1, 19) Down’s Syndrome Head injury Limited education Risk factors for Vascular Dementia (Diabetes,
hypertension, obesity, AF, lipids etc)
AD Genetics 1: Young-onset Familial Alzheimer’s Disease - autosomal dominant,
small minority, young onset, APP mutations– Ch21: beta amyloid precursor protein gene– Ch14: presenilin 1 gene – Ch1: presenilin 2 gene– All lead to Ab aggregation (increased Ab42)
imbalance between Ab production & clearance
AD Genetics 2: late onset Non-Mendelian AD
– great majority of cases– genetic + environmental factors– first degree relatives of late-onset AD patients have 2x
expected lifetime risk Ch19: apolipoproteinE; lipid binding protein in 3 isoforms
x fold increase in AD risk
2 x fold increase in AD riskLowers age of onset by 7 years
AD Genetics 2: late onset Various other genes implicated with weaker
effects, all thought to involve increased A e.g:– Sortilin-related receptor 1 gene (SORL1)– Clusterin gene (CLU)– Complement receptor type 1 gene (CR1)– Phosphatidylinositol-binding clathrin assembly protein
(PICALM) gene
Biomarkers for AD Contribute to increased specificity of diagnosis In AD CSF levels of Ab42 lower (less soluble) CSF elevated total TAU & Phosphorylated Tau Total Tau levels increase with AD progression Structural MRI: medial temporal lobe atrophy
Vascular Dementias Includes Multi Infarct Dementia Single strategic infarct Subcortical VAD (Binswangers) / SVD Hypoperfusion Dementia Specific Arteriopathies (eg CADASIL)
NINDS-AIREN Criteria for NINDS-AIREN Criteria for VaDVaD(Roman et al, 1993)(Roman et al, 1993) Dementia (memory and 2 or more domains)Dementia (memory and 2 or more domains) Cerebrovascular disease (focal neurology and Cerebrovascular disease (focal neurology and
CVD on brain imaging)CVD on brain imaging) Link between the 2 (3 months or Link between the 2 (3 months or
abrupt/fluctuating clinical course)abrupt/fluctuating clinical course) PossiblePossible VaD if brain imaging negative or VaD if brain imaging negative or
relationship (3/12) not clearrelationship (3/12) not clear
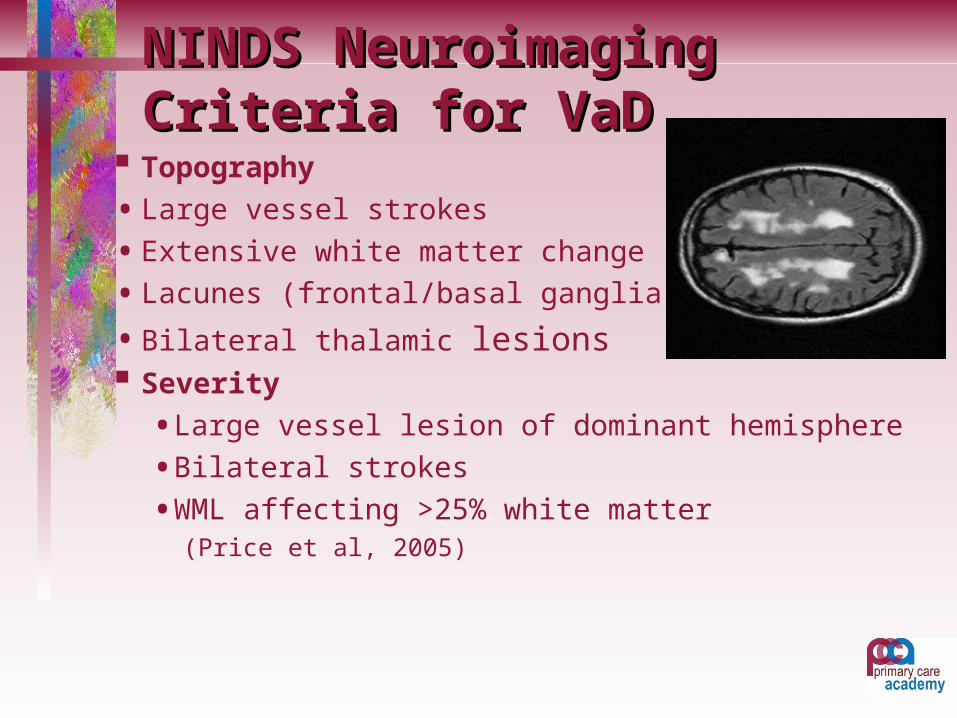
NINDS Neuroimaging NINDS Neuroimaging Criteria for VaDCriteria for VaD
Topography
• Large vessel strokes
• Extensive white matter change
• Lacunes (frontal/basal ganglia)
• Bilateral thalamic lesions Severity
• Large vessel lesion of dominant hemisphere
• Bilateral strokes
• WML affecting >25% white matter (Price et al, 2005)
VAD: Neuropathology: Micro – infarcts Cystic necrosis of infarcted areas Reactive gliosis Patches of demyelination of white matter
Risk Factors for VAD: Old Age Family history Male sex Geography & race Hypertension Smoking Diabetes Cardiac arrhythmia Hyperlipidaemia Increased homocysteine
Hachinski Ischaemic Score: Abrupt onset (2)
Stepwise deterioration (1) Fluctuating course (1) Nocturnal confusion (1) relative preservation of personality (1) Depression (1) Somatic complaints (1) Emotional incontinence (1) History of hypertension (1) History of strokes (2) Evidence of atherosclerosis (1) Focal neurological symptoms (2) Focal neurological signs (2) < 4 suggests AD > 7 suggests VAD
Dementia with Lewy Bodies a progressive degenerative brain
disease shares symptoms - and sometimes
overlaps - with Alzheimer’s and Parkinson’s
Dementia with Lewy Bodies Lewy Body = smooth round
intraneuronal inclusion bodies LBs throughout cortex, midbrain or
brainstem “abnormal protein structures” first
described in 1912 by Frederich Heinrich Lewy
Criteria for Probable DLB Criteria for Probable DLB McKeith et al, Neurology, 2005McKeith et al, Neurology, 2005
Cognitive decline sufficient to interfere with social/occupational function
CORE features (at least one core + one suggestive or 2 core features must be present):- Fluctuation- Recurrent visual hallucinations- Spontaneous parkinsonism
Suggestive features:- REM sleep behaviour disorder- Neuroleptic sensitivity- Dopaminergic abnormalities in basal ganglia on SPECT/PET
Features supportive of the Dx of DLB are: Repeated falls Syncope Transient loss of consciousness Neuroleptic sensitivity Systematized delusion Hallucinations in other modalities auditory,
olfactory or tactile
DEMENTIA: GENERAL SIGNS &
SYMPTOMS
Dementia: general signs & symptoms
Early stages: – memory impairment, loss of planning, judgement,
difficulty with administrative tasks etc Intermediate
– impaired basic ADL can’t learn new information, increasing disorientation time & place
– increased risk of falls and accidents due to confusion and poor judgment
Dementia: signs & symptoms Severe dementia: no ADL skills, totally dependent for
feeding, toileting, & mobilising. Severe global cognitive impairment
risk of malnutrition and aspiration poor mobility & malnutrition increases risk of pressure
sores Seizures, dehydration, malnutrition, aspiration, pressure
sores death from infection (resp., skin, UTI etc)
Dementia: signs & symptoms
Behavioural problems (BPSD): Persecutory delusions, suspiciousness in c. 25% wandering, aggression, agitation Depressive symptoms in c. 60% Depression in c. 25%
Dementia: Diagnosis & Investigations A clinical diagnosis History from an informant Physical examination Medication review Mental state examination & cognitive assessment (AMT or
MMSE) Bloods: FBC / ESR / U+E / LFT / TFT / Glucose / Ca + Po /
B12 + Folate / +/-Treponema serology CXR, ECG
Additional investigations: If indicated from history & examination: CT: cortical atrophy, widened ventricles in AD. Evidence
of vascular disease in VAD. Exclude SOL MRI: v. sensitive for VAD SPECT valuable in differentiating AD, VAD, FTD (DAT
scan for suspected DLB) EEG (non-specific diffuse slowing of alpha rhythm. Delta
& theta activity psychometric testing if unusual presentation or
uncertain
NICE/SCIE Guidelines for Dementia 2006 MRI is preferred modality, CT can be used Structural imaging should be used to exclude other
cerebral pathologies & help establish subtype HMPAO SPECT can be used to help differentiate
between AD, VaD and FTD if diagnosis is in doubt FP-CIT SPECT should be used to help establish The diagnosis of DLB if the diagnosis is in doubt
Additional investigations Increasing recognition of value of CSF biomarkers CSF-
tau & CSF-Aß42 as Diagnostic Markers for Alzheimer Disease
these biomarkers may have a role in the clinical workup of patients with cognitive impairment, especially to differentiate early AD from normal ageing
low CSF β-amyloid 1-42, high total tau protein, and elevated phosphorylated tau181P predict AD
Management of Dementia: Treat medical disorders & any causes of disability (mobility,
vision, hearing etc ) Treat BPSD: depression, psychosis, behaviour disturbance Assess ADLs and maximise function, assess risk
(occupational therapist) Finances: LPOA, COP, testamentary capacity, benefits
(attendance allowance), council tax exemption (social worker),
Early referral to social services (do not wait for secondary care)
Management of BPSD in Dementia: (Iliffe) P: Physical: pain, infection,
constipation A: Activities of others: misinterpretation I: Intrinsic to dementia: walking, pacing
activity D: Depression or delusions
Management of dementia: Home alone with support from social services: Home with care package eg. carer for personal
& domestic care, meal preparation, shopping, cleaning, etc. supervise medication
Meals on wheels Day centre to increase socialisation &
stimulation
Management of Dementia: Support for carers: Alzheimer’s Society / Age
Concern / BCAS advice & support groups Respite care DHTT if acute severe behavioural problems Higher prevalence of depression & anxiety in carers Alternatives to home care (dependency & risk): extra
care sheltered housing, residential & nursing homes NHS continuing care funding
Management of Dementia: Medication
Medication for cognitive impairment (cognitive enhancing drugs)
Medication for BPSD
Management of Dementia: Medication Anti-dementia drugs:
- Cholinesterase inhibitors: (Approved by NICE) Donepezil (Aricept) Rivastigmine (Exelon) Galantamine (Reminyl)
- Memantine (Ebixa) (approved by NICE for severe Dementia March 2011)
Cholinesterase Inhibitors: Cholinesterase inhibitors for Alzheimer's
disease Birks Cochrane Database of Systematic Reviews The three cholinesterase inhibitors are efficacious for mild to moderate Alzheimer's disease. Despite the slight variations in the mode of action of the three cholinesterase inhibitors there is no evidence of any differences between them with respect to efficacy.
Memantine (Ebixa) Memantine for dementia
Cochrane Database of Systematic Reviews
Authors' conclusions: Memantine has a small beneficial effect at six months in moderate to severe AD. In patients with mild to moderate dementia, the small beneficial effect on cognition was not clinically detectable in those with vascular dementia and was detectable in those with AD. Memantine is well tolerated.
Future developments: Disease modifying drugs: 2 proteases beta and gamma- secretase cleave the APP into A-beta fragments which form
amyloid plaques APP Beta secretase Gamma secretase Abeta Beta secretase (BACE= beta site APP clearing
enzyme) Future development of BACE inhibitors? Inhibitors of tangle formation?
Management of Dementia: Medication for BPSD Antidepressants Antipsychotics Anxiolytics Hypnotics
Defensible prescribing of antipsychotics in Dementia Consider non-pharmacological alternatives Address vascular risk factors Consent / capacity / best interests Discuss risks & benefits with patients or carers Identify target symptoms (psychosis, hostility, aggression) Choose effective drug & dose Choose time-frame during which to assess benefits
(discontinue if no evidence or if harm) If good response review need & aim to withdraw in c 3/12 if
possible
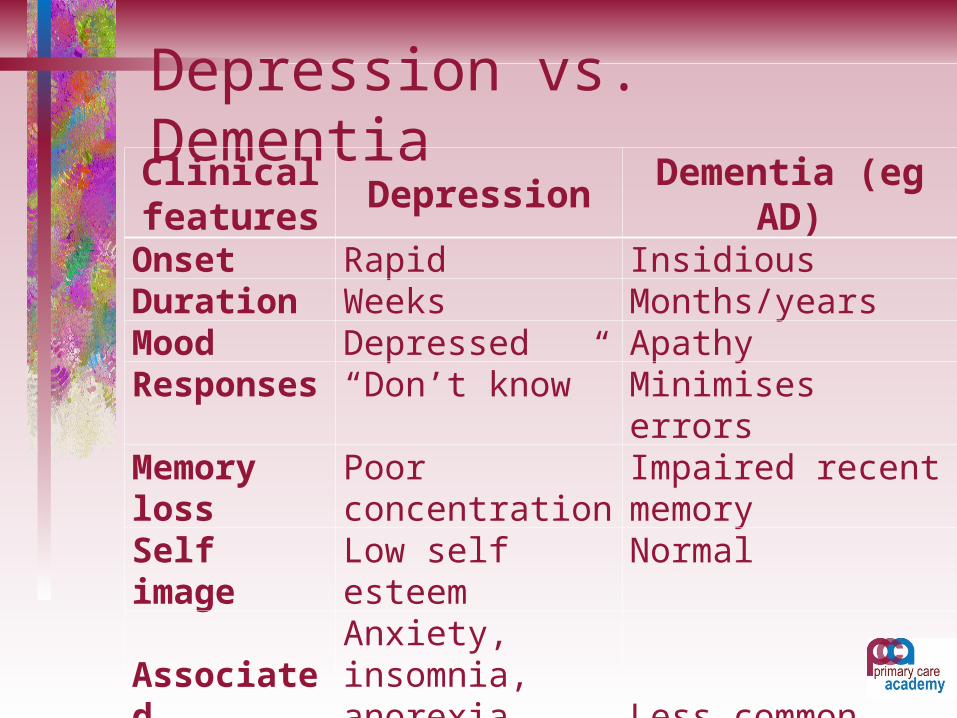
Depression vs. DementiaClinical features
Depression Dementia (eg AD)
Onset Rapid InsidiousDuration Weeks Months/yearsMood Depressed ApathyResponses “Don’t know” Minimises errorsMemory loss Poor concentration Impaired recent memorySelf image Low self esteem Normal
Associated symptoms
Anxiety, insomnia, anorexia, life not worth living
Less common
Previous history
Past or Fam. Hx. Depression
May be Fam. Hx. Dementia
Delirium: DSM 4 criteria Disturbance of consciousness with reduced
ability to focus, sustain or shift attention Change in cognitive function not due to pre-
existing or evolving dementia Development over short period of time – usually
hours or days & tendency to fluctuate during course of day
Delirium: causes Infection Drugs (prescribed & illicit, intoxication or
withdrawal) Organ failure (cardiac, resp., hepatic, renal) Electrolyte disturbance (dehyd. Na/Ca/K) Endocrine & metabolic – thyroid, glucose CNS- CVA, subdural, SOL Nutritional – thiamine Malignancy hypothermia
Delirium: risk factors Age Illness severity Dementia & other cognitive impairment Dehydration General frailty Sensory impairment Alcohol use
Delirium: clinical presentation
Hyperactive: agitated, hyper-vigilant, restless, perceptual disturbance, deluded
Hypoactive: drowsy, apathetic, decreased speech & movement
Mixed / fluctuating
Delirium: management Clarify history Assessment of physical & mental state Identify & treat underlying cause May need to treat neuropsychiatric symptoms
with modest doses of antipsychotics / sedatives Well-lit, quiet room, address sensory impairment
NICE on Delirium (CG 103) Main focus is prevention in those at risk Document delirium in all health records Familiar health carers when possible Preventive interventions (eg manage pain, sensory
imp., sleep disturbance, multiple meds etc) Identify & treat underlying cause Communication, reorientation, reassurance If distressed – haloperidol or olanzapine
Dementia in Primary care Av. Practice list c. 2000: 10-15 patients with
dementia (Iliffe, 2010) 1-2 new cases per year Much greater numbers in care homes & special
populations e.g. Barnet
Dementia in Primary care Systematic review of disease progression Shared care protocols for ACHEIs Carer needs Managing: BPSD, continence, frailty, end of life
care & hospital admission
NSF protocols on Dementia
April 2004: “GP practices, using agreed protocols, will be diagnosing,
treating and caring for older people with depression or dementia”

NSF Protocols / Pathways Care pathways: key points Where to refer? When to refer? Should you refer everyone? Chronic disease model
Dementia: when to refer? Diagnosis or care plan uncertain AD (mixed, DLB) MMSE 10 -20/30 for anti-
dementia drug treatment Marked behaviour disturbance, risk of harm to
self or others Severe mood or psychotic symptoms
Dementia: when to refer?Do not need to refer if: Diagnosis is apparent & clear management plan Patient has already been assessed in secondary
care and care needs are unchanged Vascular Dementia without behavioural concerns NB do refer directly to social services for needs
assessment
Dementia: management Always exclude Delirium May need referral to MHSOP, social services,
Alzheimer’s society, Geriatrician, Age Concern etc
“chronic disease model” - will need long term monitoring and regular reviews by primary care team and in some cases “shared care”
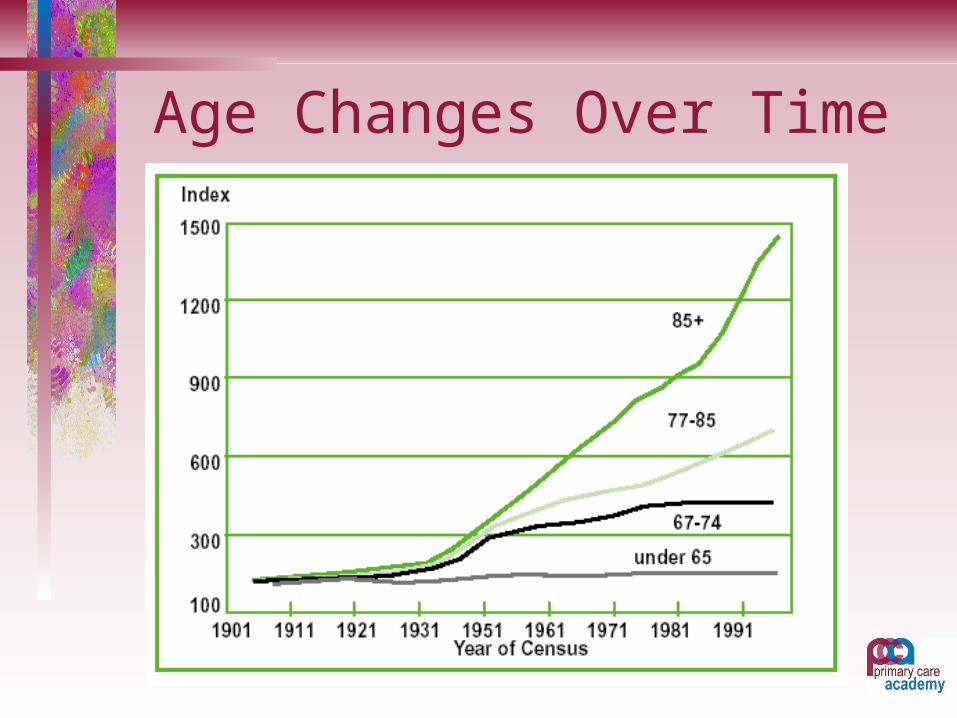
Age Changes Over Time
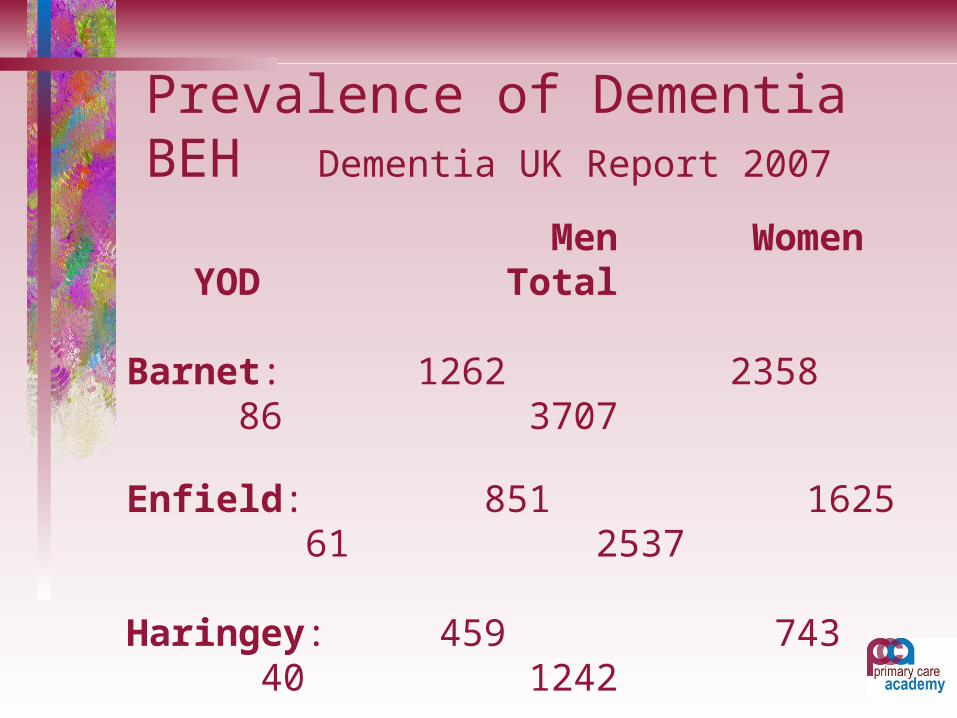
Prevalence of Dementia BEH Dementia UK Report 2007
Men Women YOD Total
Barnet: 1262 2358 86 3707 Enfield: 851 1625 61 2537
Haringey: 459 743 40 1242
TOTAL BEH 7486
NICE Dementia Guidelines: Barnet Dementia UK Report 2007
3707 people in Barnet have dementia This is the single largest number of
all London boroughs By 2021 this will have increased by
20% to 4435 people
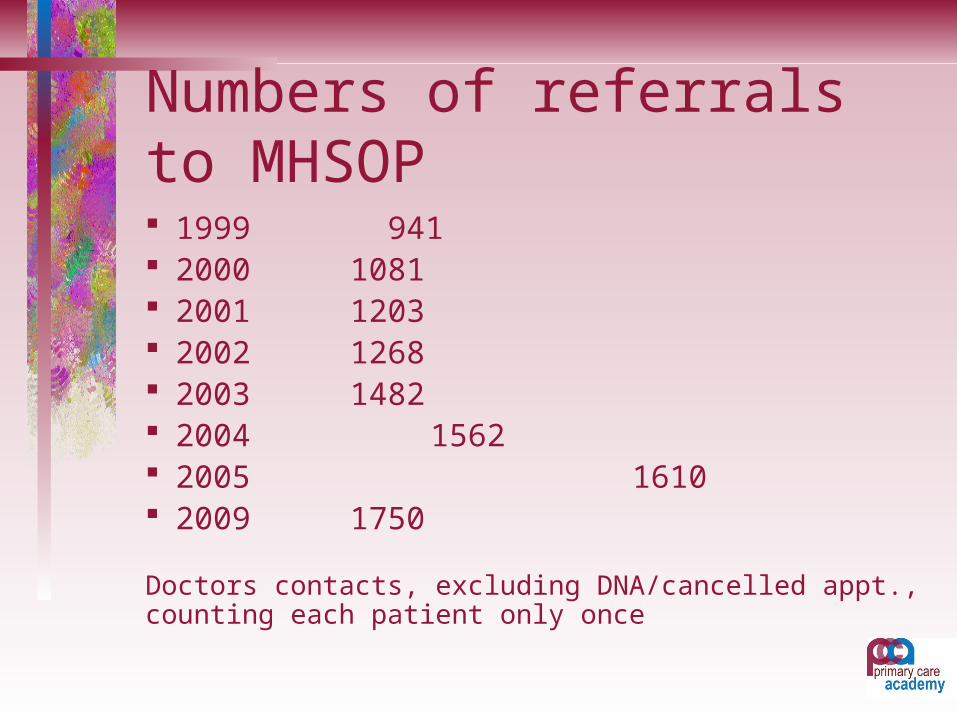
Numbers of referrals to MHSOP 1999 941 2000 1081 2001 1203 2002 1268 2003 1482 2004 1562 2005 1610 2009 1750
Doctors contacts, excluding DNA/cancelled appt., counting each patient only once
Investing in treatment of dementia: medication
Developments in novel drug treatments specifically for dementia
Currently only c. 25% receive specialist assessment & treatment
Early referrals: uncomplicated, chance for prevention of crises
Drug and non-drug costs Disease modifying compounds in development
Investing in treatment of dementia: other aspects More holistic dementia care aromatherapy, light therapy, massage interpersonal approaches training for GPs in recognition & management training & support for carers providing a spectrum of care: at home, day care
(available, appropriate), respite care, quality dementia care homes
DOES THIS PATIENT HAVE CAPACITY?
Test for Capacity – S. 3(1)(c) MCA 2005
A person is incompetent if he is unable: To understand the information relevant to the
decision; To retain that information; - (s.3(3)) To use or weigh that information as part of the
process of making the decision; or To communicate his decision (whether by
talking, using sign language or any other means)
Definition of Incapacity – (S. 2(1) MCA 2005) “A person lacks capacity in relation to a matter if
at the material time he is unable to make a decision for himself in relation to the matter because of an impairment of, or a disturbance in the functioning of, the mind or brain” -
Capacity can fluctuate and a person can therefore lack capacity in relation to one matter but not in relation to another – S.2(2)
Principles Regarding Persons who Lack Capacity A person is presumed to have capacity; S.1(2) A person is not to be treated as unable to make
a decision unless all practicable steps to help him to do so have been taken without success; S.1(3)
A person is not to be treated as unable to make a decision merely because he makes an unwise decision; S.1(4)
Capacity – MCA 2005 Consideration should be given to the person’s
past and present wishes and feelings and the beliefs, values and any other factors that would be likely to be taken into account if the person had capacity. S.4(6)
Take into account written statements made while P had capacity. S.4(6) (see explanatory notes
Capacity – MCA 2005 Take into account if practicable and appropriate views
of:-– Anyone named by the person as someone to be
consulted.– Anyone engaged in caring for the person or
interested in his welfare.– Any donee of a LPA
Will have complied with the law if you reasonably believe that what you are doing is in the P’s best interests S.4(9)
Can Dementia be prevented? Kurth & Logroscino BMJ 2010:341:310-1 Modifiable risk factors exist but too early to call
for prevention programmes
Can Dementia be prevented? Ritchie et al BMJ 2010:341:
Cohort study, 1433 people Montpellier followed from 1999 for7 years
Predictors of dementia: crystallised intelligence (vocab & gen. knowledge), Depression, Fruit & veg consumption, diabetes & apolipoprotein E4 allele
Theoretical elimination of depression & diabetes & increase in fruit & veg consumption estimated would reduce burden of dementia by 21%
Can Dementia be prevented? Age & genetic factors strongest risks Life-style risk factors modulate the risk for dementia
and Alzheimer‘s disease Cardiovascular risk factors Nutritional factors Behavioural factors (physical & psychosocial activity) Risk appears to be modulated by APO E4 status Intervention in middle age may reduce risk
Possible Protective factors:Weak evidence of protective effect for:Mediterranean dietPhysical activityIntellectual activity
Survival after diagnosis of dementia in primary care Rait et al BMJ 2010;341:337 Health improvement network primary care
database incidence of dementia in primary care 1990-2007, compare survival from diagnosis to those without dx
Cohort of 22529 recorded dx dementia Incidence 3-4/1000 person years Median survival those 60-69 years was
6.7years (range 3-11) Survival for >90 years was 1.9 years(0.7-3.6)
Survival after diagnosis of dementia in primary care Mortality rates 3x higher in first year after
diagnosis of dementia than people without(RR 3.68)
2.5x greater risk subsequently Median survival signif. lower than screened
populations

CASES FOR
DISCUSSION
Cases for discussion: Case 1
• 88 year old woman with no past psychiatric history. She lives alone at home , supported by her daughter who visits 3x weekly.
• The daughter rings you reporting that her mother has been confused over the past 2 days, is disorientated in time, claims that strangers are entering her house and accuses the cleaner of stealing her purse.
1. What is the most likely explanation for the presentation?2. How would you assess & manage this situation?
Cases for discussion: Case 278 year old man lives at home with his wife. She reports that he has a 1 year history of increasing forgetfulness. He is upset as he claims that strange people, including children, keep entering his bedroom at various times. He has poor mobility and frequent falls. He has episodes of marked confusion but at other times can be more lucid.
1. What is the most likely diagnosis and DDx?2. What neuroimaging might be useful here?3. What drugs would you consider for the hallucinations?
Cases for discussion: Case 3 You receive a letter from a solicitor, “your
patient wishes to make a new will… does he have Testamentary Capacity?”
“Could you also please tell me if he has capacity to donate Lasting power of Attorney?”
How do you proceed?