Embed Size (px)
Citation preview

INTERNATIONAL JOURNAL OF GERIATRIC PSYCHIATRY, VOL. 4: 3-9 (1989)
DEMENTIA, DEPRESSION AND SUBSEQUENT
HOME SUPPORT INSTITUTIONALIZATION-THE EFFECT OF
J A M E S LINDSEY Senior Lecturer in Psychogeriatrics. UMDS, Guy5 Hospital, London Bridge SEI 9RT. UK
and
Professor of Psychogeriatrics, UMDS, Guy5 Hospital, London Bridge SE1 9RT. UK ELAINE M U R P H Y
SUMMARY
The Guy’s/Age Concern Home Support Project is a prospective controlled intervention study of the effect of client- centred home support for elderly people with dementia. Control subjects who were in institutions at six months follow-up were significantly more depressed and physically disabled at referral than those who remained at home. Among those receiving additional home support, however, there was no difference between the depression and disability scores at referral of those who were institutionalized and those who remained at home at follow-up. These results suggest that the high prevalence of depression and physical disability in the institutionalized elderly is due to preferential selection into institutions, and that this process is prevented by providing this form of domiciliary support.
K E Y WORDS ~Dementia, depression, institutionalisation.
INTRODUCTION
There is a high prevalence of psychiatric morbidity among elderly people resident in institutions. Dementia is the commonest disorder found in surveys of this population, but a large proportion suffer from other psychiatric disorders, particularly depression. Indeed, depression appears to be much commoner in old people’s residential and nursing homes than it is in the general elderly population, with reported prevalence rates of 50% (Teeter et al., 1976), 38% (Mann et al., 1984), 24% (Rovner et al., 1986) and 22% (Snowdon, 1986).
In some cases this depression may be a response to institutionalization or a product of the institu- tional environment. Another possibility is that depressed elderly people are more likely to be admitted to institutions in the first place; according to one retrospective study (Gillis et al., 1982) depression was cited as the main problem precipit- ating admission in 23% of cases. Little is known about the process of placement or the factors that promote or prevent it, but it is likely that multiple personal, social, physical and psychiatric factors operate in determining an elderly person’s admis-
sion to institutional care. For example, physical disabilities such as reduced mobility, sensory impair- ment and incontinence are common in elderly people in residential and hospital care (Charles- worth and Wilkin, 1982), and are associated with depression in these settings (Kay and Bergmann, 1966; Mann et al., 1984).
The Guy’s Hospital/Age Concern Home Support Project (Askham er al., 1988b) is a controlled inter- vention study examining whether it is possible both cost-effectively and humanely to keep elderly people with dementia at home for longer than is currently possible with the existing pattern of services. Home support schemes are services that provide comprehensive assessment of social, psycho- logical and medical needs; appropriate treatment; a full range of practical care tasks as and when required; and the emotional and personal support necessary if the client is to be supported at home. Such schemes are highly client-centred, and this approach can only work where there are skilled case managers whose job it is to assemble a compre- hensive assessment of the client, and then recruit and organize appropriate care paid for out of a fixed budget over which the case managers have
0885-6230/ 89/ 0 1ooO3-07$05.00 0 1989 by John Wiley & Sons, Ltd
Received I Ocrober 1987 Accepted 7 March 1988

4 J. LINDSEY AND E. M U R P H Y
considerable personal control. The degree of joint planning and devolved budgetary discretion that home support schemes require presents consider- able administrative obstacles, but this model of domiciliary care can sustain hitherto unsupportable clients at home for longer than is possible with existing services (Davies and Challis, 1986).
If depression is associated with the early admission of demented elderly to residential care, then home support services may be able to support such people at home by either relieving that depression or ameliorating its causes and effects. As part of the evaluation of the Guy’s/Age Concern scheme, the relationship between depressive sympto- matology and subsequent admission into institu- tional care was prospectively examined in those subjects receiving extra home support, and in a comparable control group.
METHOD
The study sample was drawn from individuals referred to the psychogeriatric services in two sites, a London borough (Newham) and a country town (Ipswich), over 12 months between April 1984 and March 1985. Eligible subjects were aged 65 years and over and not resident in an institution at the time of referral. They had a clinical diagnosis of dementia supported by a score of three or more on the OBS scale of the C A R E Schedule at first assessment, a cut-point used in other studies to screen for dementia in community and institutional- ized samples of the elderly (Gurland et al., 1983; Macdonald et al., 1982).
The study sites were divided into Action and Control areas, matched as far as possible in terms of the age structure of the population, the proportion of elderly people living alone, their housing amenities, and the number of referrals to the psychogeriatric services in the previous year. Depending upon which area the subjects lived in, they were assigned to either an Action or a Control group. Both groups subsequently received the normal range of services available, but the Action subjects were also provided with additional ‘packages’ of home support tailored to their special needs. The weekly cost of all community support was limited to that of a typical long-stay psychogeriatric bed (f200/ week), and in most cases was much less than this. The planning and delivery of this home support are described in Murphy and Rapley (1986).
The subjects were assessed by five trained medical and non-medical interviewers at referral and six months later with a structured question- naire that included the CARE Schedule OBS and Depression scales (Gurland et al., 1977). The OBS scale has a score range of 0-10, and the Depression scale a score range of 0-30. The assessment of depression can be problematic in the context of cognitive impairment, and the usual precaution is to exclude the Depression scores of those with an OBS score of eight or more. However, this rule would have excuded a very large proportion of the subjects in this particular study (44%), so a different criterion has been applied; subjects with more than four incomprehensible responses to the CARE Depression items when interviewed either initially or at follow-up were excluded from all or part of the analysis. Also excluded were those subjects who died before follow-up. The remaining subjects in the two groups were subdivided according to residence at follow-up (either at home or institution- alized in a long-stay hospital bed or old people’s home), and the Depression scores of these subgroups at referral were compared using the Mann-Whitney U-test.
The relationship between depression and domes- tic isolation (living alone or with others) on one hand and physical disability on the other was also examined. Physical disability was assessed in most cases by the medical staff of the referring psycho- geriatric services, who rated subjects on items re- lating to mobility, manual dexterity, hearing, eye- sight and continence at the time of referral (see Appendix). In a few cases this information was not available, and the ratings were made on the basis of the interviewers’ findings. A global simple un- weighted disability score for each subject was obtained by summing the individual item scores.
Table I . Action and Control samples
Action Control ~~~
Total eligible at referral 91 71
Unrateable at referral 5 4
Sample at referral 63 50
Dead before follow-up 23 21
Unrateable at follow-up 7 6 Sample at follow-up 55 44

D E M E N T I A . D E P R E S S I O N A N D S U B S E Q U E N T INSTITUTIONALIZATION 5
RESULTS
The composition of the sample is given in Table I . Inevitably, there was a high attrition rate, with 27% of those eligible for the study dying before follow- up. At both study sites, the Action and Control groups were comparable as regards age, sex dis- tribution and mean OBS score at referral (Table 2 ) . No significant differences were found between the two sites in this analysis, and the results given here are for both sites combined.
Table 2. Characteristics of the Action and Control groups at referral
Newham lpswich Action Control Action Control
~- ~- ~~~~~~~~ ~ ~
Mean age at referral 79.1 81.3 80.8 78.5 Proportion female 67% 83% 78% 79% Mean OBS score at 6.7 6.7 6.9 6 1
referral
Depression at referral
There was no significant difference between the initial depression scores of the Action and Control groups overall (Table 3).
Fdbk 3. Total mean Depression scores for Action and Control groups
Action Control
At referral 4.9 5 4 At six months 4.8 4.6
Control groups. The Depression scores at referral of those subjects remaining at home six months later were significantly lower (p<O.OO 1 ) than those who were by then resident in institutions (Table 4). Of the 16 subjects with initial Depression scores of seven or more, three remained at home, seven were in long-stay hospital beds and six were in Part 111 residential care.
Acf ion groups. There was no significant difference between the Depression scores at referral of those at
Table 4. Mean Depression scores (CARE) at referral and at six months follow-up. (Figures in brackets are the proportion with scores of seven or more)
Resident at follow-up At home In institution
Contro l At referral 3.0 ( 1 2%) 7.4 (54%) p<O.OO I
n=26 n=24
At six months 3.2 (20%) 6.4 (53%) p<0.05 n-25 n-19
Ac rion NS At referral 4.4 (28%) 5.3 (28%)
At six months 4.8 (2 I %) 4.9 (33%)
n.3 I n=32
N s n=28 n-27
home and those in institutions six months later (Table 4). There were 19 subjects with initial Depression scores of seven or more: nine remained at home, seven were in long-stay hospital beds, and three were in Part I11 residential care.
Depression at six months
There was no significant difference between the overall Depression scores of the Action and Control groups at six months follow-up (Table 3).
Controlgroups. Those in institutions at six months follow-up were significantly more depressed @<0.05) than those who were still at home (Table 4) . Of those in institutions, lo/ 19 (53%) had Depres- sion scores of seven or more, compared with only 5 /25 (20%) at home.
A (,lion groups. There was no significant difference in the Depression scores of those at home and those in institutions at six months (Table 4). There was no evidence that the experience of institu- tionalization significantly increased levels of depres- sive symptomatology in these samples. In both groups the mean Depression scores of the institutionalized subjects in fact fell slightly between referral and follow-up (Table 4). Overall, there was no significant correlation be- tween the OBS and Depression scores either at re- ferral ( ~ 0 . 0 4 ) or at six months ( ~ 0 . 2 1 ) .

6 J. L I N D S E Y A N D E. M U R P H Y
Living alone
There was no significant difference between the proportion of subjects living alone at referral in the Control groups (33150: 67%) and in the Action groups (46/63: 73%). A smaller proportion of subjects who lived alone remained at home at follow-up, but living alone did not significantly predict institutionalization in either group. Overall, there was no significant association between living alone and Depression scores or seven or more in this study (~"0.6; df=l). In the Control groups the Depression scores at referral of those in institutions six months later were significantly higher both for those who lived alone and those who lived with others (Table 5).
Physical disability
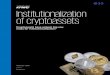
Fig. 1 shows the distribution of the Physical Disability scores in the action and control groups at referral. There were more severely disabled (score 6+) individuals in the Control groups, but overall there was no significant difference between the scores of the two groups. The Physical Disability score was significantly correlated with the Depres- sion score ( ~ 0 . 2 4 ; p<0.02) and like the Depression score, the Physical Disability score also significant- ly predicted institutionalization at six months follow-up in the Control groups but not in the Action groups (Table 6).
DISCUSSION
The difficulty of eliciting rateable responses to standardized questions and probes from subjects with cognitive impairment must limit the validity of the assessment of depression, particularly in a study such as this were most of the subjects were mode- rately or severely demented. A cut-off based upon the OBS score (8+) would have excluded nearly half of the subjects otherwise eligible for the home support project. However, the number of subjects excluded because they were unrateable on five or more items of the 30-item CARE Depression scale was relatively small: only 9/ 119 (8%) at referral and IS/ 110 (16%) at six months. For the remainder, their Depression score can be regarded as a reason- able index of severity of any mood disturbance present. Those excluded as unrateable were for the most part those with the severest degree of
Table 5. Mean Depression scores (CARE) at referral living alone or with others
Residents a t follow-up At home In institution
Conirol Alone 2.8 6.9 P<O.OI
With others 2.8 8.7 p<0.05
n.15 n-18
n=l I n.6
A<,rion Alone 4.8 5 . 5 NS
n.2 I 11.25
With others 3.6 5 . 3 NS n=IO n=l
dementia (9+ on the OBS scale in most cases), so the findings of this study may not apply to this group. Also excluded from the study were the cognitively intact elderly, so these results may not apply to them either.
These results suggest that the high prevalence of depression reported in the institutionalized elderly is due in part to the selective placement of depressed elderly people with dementia in institutions in the first place. In the Control groups those resident in Part 111 homes or hospital beds at six months follow-up already had significantly more depressive symptoms at initial referral than those who were destined to remain at home. The preferential selection of depressed, demented elderly in institu-
Table 6. Physical Disability scores at referral for Action and Control groups
Control 0-3
4i
Aclion 0-3
4+
Resident at follow-up At home In institution
22 13
4 I 1 p<0.05
28 26
3 6 1's

DEMENTIA, DEPRESSION A N D SIJ BSEQUENT INSTITUTIONALIZATION
60 -
50 -
% 40 -
30 -
20 -
10 -
0 -
7
70
60
50
% 40
30
20
10
0 01 1
CONTROL
n
213 415 617 Disability Score at referral
70 1
01 1
ACTION
n
213 415 617 Disability Score at referral
Home at 6 m
0 In institution at 6 m
Fig. I . Distribution of Physical Disability scores at referral by group and location at follow-up
tions may be encouraged by various means. Depres- sive symptoms such as early waking, apathy, agitation, irritability and importuning are poorly tolerated by relatives and other carers and may make care at home too difficult (Norman, 1987). More importantly, depression is associated with other factors such as physical frailty and social isolation that determine removal from home. This study suggests that physical disability is important in this respect, since this was correlated with depression, and in the Control groups high levels of physical disability at referral also predicted institutionalization at follow-up.
Living alone was not associated with higher Depression scores in this sample, nor did it significantly predict institutionalization in the Control groups, although a greater proportion of those who lived alone at referral were in institutions at follow-up. Bergmann et al. (1978) found that living alone was the variable that was the strongest predictor of subsequent removal from home in their psychogeriatric sample. The fact that physical disability and depression now appear to be more significant predictors suggests that there has been a change in the determinants of admission to institu- tions over the last ten years. The likeliest cause of this change is that the current overwhelming demand for long-stay places in hospitals and
residential homes means that only the most physically and mentally frail are now considered.
If it is physically disabled, depressed elderly people with dementia who are more likely to be placed in institutions, this highlights the need for proper medical and psychiatric assessment before they enter residential care. It also demonstrates that the existing domiciliary services are not able to keep such people at home. A model of home support similar t o that evaluated in this project has been shown to be cost-effective in delaying admission of the general population of frail elderly to residential care (Davies and Challis, 1986; Challis et al., 1988). However, those with dementia present particular problems and the benefits of home support for this client group are rather less clear cut, as the Guy’s/ Age Concern project was found. While there was no overall difference between the Action and Control groups in either Newham or Ipswich in terms of the length of time subjects were supported at home, if matched Action and Control cases were compared it was clear that home support was effect- ive in certain instances (Askham et al., 1988a). In particular, a group of subjects with relatively severe dementia who were living alone and unsupported by informal carers were sustained at home in the Action group for longer than equivalent Control group subjects. In other cases, home support was

8 J . LINDSEY AND E. M U R P H Y
ineffective either because extra support was not re- quired and made only a marginal difference, or else the difficulties were such that subjects could not be sustained at home despite intensive additional home support. The problems associated with the failure of home support included chronic double incontinence, intercurrent episodes of acute physical illness, wandering, falls, dangerous behav- iour in relation to stoves and heaters, and aggres- sion towards relatives. Some carers were able to tolerate and manage these problems, but in most cases they imposed insupportable strains and risks.
In general, home support appears t o be effective at meeting the needs imposed by chronic physical disability, but less so coping with behavioural disturbance. This is borne out by the finding that home support prevented the selective early institu- tionalization of those demented subjects who were also physically frail and depressed. There was no significant difference in the overall Depression scores of the Action and Control groups at follow- up, so this home support scheme was presumably meeting the physical rather than the emotional needs of these subjects. Davies and Challis (1986) did find a significant improvement in depressed mood and morale associated with the provision of home support in their study. However, the majority of their subjects were cognitively intact and better able to appreciate the care they were receiving. Moreover, depressed mood was rated according to the interviewer’s impression and not on self-report, so their measures of mood and morale may have reflected how the subjects appeared to others rather than how they described themselves. Of course, appearances may be important for carers; if subjects in receipt of home support seem less miserable and unrewarding, then this may reduce the likelihood of care at home breaking down.
The value of this model of case management does not lie merely in its ability to keep people at home longer. There are those whose particular problems and disabilities preclude their staying at home even with the most intensive home support, and identi- fying these cases and arranging early appropriate admission to residential care is as important as supporting those who can be kept at home. The Guy’s/ Age Concern project suggests that home support is feasible for those demented subjects who are physically disabled and depressed, but further research is required to establish in detail just who can and who cannot be effectively supported at
ACKNOWLEDGEMENTS
Thanks are due to the following researchers, interviewers, development officers and administrative staff Janet Askham, Jonathan Barker, Doreen Batey, Denise Murphy, Chrys Rapley, Rachel Stuchbury, Cath Thompson and Jane Valentine.
This project was funded by the Gatsby Charitable Foundation and the Special Trustees of Guy’s Hos- pital.
REFERENCES
Askham, J . , Barker, J., Lindesay, J . , Murphy, D., Rapley, C., Thompson, C. and Murphy, E. (1988a) The home care of dementia sufferers in lpswich and Newham: the Guy’s/ Age Concern Home Support Project. In Home or AM^!? (E. Murphy, Ed.). NUPRD, London.
Askham, J . and Thompson, C. (1988b) The Guy’s/Age Concern Home Support Project: Research Report (in press).
Bergmann, K., Foster, E. M., Justice, A. W. and Matthews, V. (1978) Management of the demented elderly patient in the community. Brit. J . Psyhiuf . 132. 44 1 -449.
Challis, D. J . , Chessum, R. and Luckett, R. (1988) Long term care for the elderly: evaluation of the Kent Community Care Scheme and related schemes. In Home or Awuj,?(E. Murphy, Ed.). NUPRD, London.
Charlesworth, A. and Wilkin, D. (1982) Dependency among old people in geriatric wards, psychogeriatric wards and residential homes 1977-1981. Research Report 6, Research Section, Psychogeriatric Unit, University Hospital of South Manchester.
Davies, B. P. and Challis, D. J . (1986) Marching Resources to Needs in Cornmunit). Cure. Gower. London.
Gillis, L. S., Elk, R.. Trichard, L., Le Fevre. K.. Zabow, A,, Joffe, H. and Van Schalkwyk, D. J . (1982) The admission of the elderly to places of care: a socio- psychiatric study. P s j d ~ l . Med. 12, 159- 168.
Gurland, B. J.. Kuriansky, J . B., Sharpe, L., Simon. R.. Stiller, P. and Birkett, P. (1977) The Comprehensive Assessment and Referral Examination (CARE) ~
rationale, development and reliability. In!. J . Aging Hum. Dev. 8,9-42.
Gurland, B. J . , Copeland, J . , Kelleher. M.. Kuriansky. J.. Sharp, L. and Dean, L. (1983) The Mindund Moodqf’ Ageing. Haworth, New York.
Kay, D. W. K. and Bergmann, K . (1966) Physical disability and mental health in old age. J . Ps~,chosom. Res. 10, 3-12.
Macdonald, A. J. D., Mann, A. H., Jenkins, R., Richard, home. L., Godlove, C. and Rodwell, G. (1982) An attempt to

DEMENTIA. DEPRESSION AND SUBSEQUENT INSTITUTIONALIZATION 9
determine the impact of four types of care upon the elderly in London by the study of matched groups. Psjrhol. Med. 12, 193-200.
Mann, A. H . , Graham, N. and Ashby, D. (1984) Psy- chiatric illness in residential homes for the elderly: a survey in one London Borough. Age Ageing 13, 257- 265.
Murphy, D. and Rapley, C. (1986) The Action Project in Practice. In The Mentally Frail Elder1,v: Should we Prescribe Community Cure? King's Fund Conference Report KFC 86/99.
Norman, A. (1987) Caring for the carers. In Dementia (B. Pitt Ed.). Churchill Livingstone, London.
Rovner, B. W., Kafonek, S., Filipp, L. and Lucas, M. J. (1986) Prevalence of mental illness in a Community Nursing Home. Am. J. Psychiut. 143, 1446-1449.
Snowdon, J. (1986) Dementia, depression and life satisfaction in nursing homes. Int. J . Geriut. Psychiut.
Teeter, R. B., Garetz, F. K. and Miller, W. R. (1976) Psychiatric disturbance of aged patients in skilled nursing homes. Am. J. Psychiuf. 133, 1430-1434.
1, 85-92.
APPENDIX
Physical Disability scale
1. Mobility (a) Can walk indoors and out of doors
unaided (b) Can walk indoors on one level unaided,
but needs aid (e.g. arm, stick, frame) on stairs or out of doors
(c) Needs aid to walk indoors on one level
(d) Cannot walk indoors on one level, even with aid 3
2. Manual dexterity
(b) Stiffness/ weakness in non-dominant (a) Can use both hands without difficulty
(c) Stiffness/ weakness in dominant hand (d) Cannot use dominant hand at all
(a) Hearing unimpaired 0
loudly I (c) Can hear with hearing aid
0
hand only 1 2 3
3. Hearing
(b) Can hear when addressed directly and /o r
2 (d) Cannot hear adequately even with hear-
ing aid, or cannot hear and does not have/ use hearing aid 3
4. Eyesight (a) Vision unimpaired (b) Can see adequately with glasses (c) Can see but not clearly even with glasses (d) Severe visual impairment/ blind
5. Continence (a) No incontinence (b) Incontinent of urine only, less than once
(c) Incontinent of urine only, more than once
(d) Doubly incontinent
Score a day
0 a day
0
1 2
The global disability score is obtained by summing the scores on the individual items.