Embed Size (px)
Citation preview
Delivering High Value Care Through Clinical Integration
www.TriadHealthCareNetwork.com
AMGA 2013 ACO Collaborative Meeting
Bill Hensel, MD, Operating/Executive Committee Steve Neorr, Executive Director

www.TriadHealthCareNetwork.com
2
Greetings from Cone Health Greetings from Cone Health
The Moses H. Cone Memorial Hospital A Brief History
www.TriadHealthCareNetwork.com
3
• Trust established by Bertha Cone in 1911 to build a hospital as a memorial to her late husband, Moses Cone
• Construction begins in 1949 on The Moses H. Cone Memorial Hospital
• Hospital's first patient admitted in 1953
• Articles of Incorporation state: “No patient shall be refused admittance because of an inability to pay.”
Moses H. Cone
(1857 – 1908) Bertha L. Cone
(1858 – 1947)
Cone Health System Overview
www.TriadHealthCareNetwork.com
4
• Facilities
– 5 Hospitals - 1,035 Acute Care Beds – Awaiting final FTC approval to merge with Alamance
Regional Medical Center (238 beds; 2,100 employees)
– 2 Ambulatory Surgery Centers
– 1 Nursing Home – 92 Beds
– 2 Freestanding Ambulatory Care Campuses, Including a Freestanding ED
– 100+ Outpatient and MD Facilities, Including JVs in Imaging, Cardiovascular Services, and Oncology Services
Cone Health System Overview
www.TriadHealthCareNetwork.com
5
• People
– Over 8,600 Employees
– 1,000+ Medical Staff Members; 320+ Employed Physicians in Cone Health Medical Group
• Patient Care (FY 2012)
– 49,345 Discharges;
– 229,834 Inpatient Days; 4.68
– 509,619 Outpatient Visits; 197,050 ED Visits
• Finances
– Over $1 Billion Revenues; $1.9 Billion in Assets
– Financial Ratios At or Above AA Benchmarks
– $185 Million Charity/Uncompensated Care (at cost)
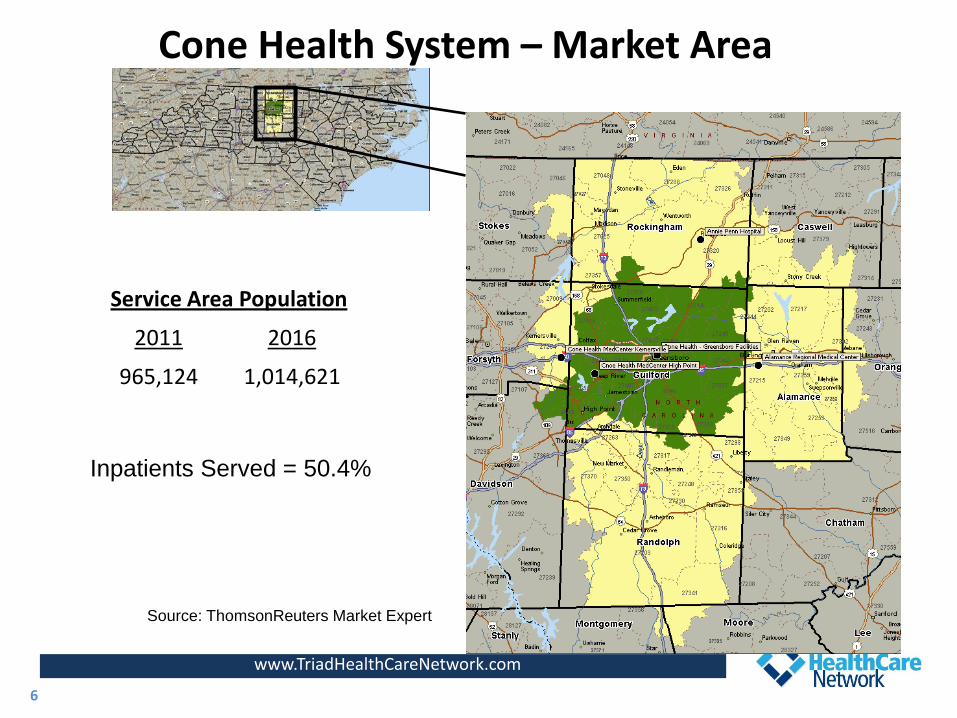
Cone Health System – Market Area
www.TriadHealthCareNetwork.com
6
Service Area Population
2011 2016
965,124 1,014,621
Inpatients Served = 50.4%
Source: ThomsonReuters Market Expert

Cone Health System Strategic Overview
www.TriadHealthCareNetwork.com
7
7
Strategic Target
Our Mission We serve our communities by preventing illness, restoring health and providing comfort, through exceptional people delivering exceptional care. Our Vision Cone Health will be a national leader in delivering measurably superior healthcare.
Triad HealthCare Network History and Overview
• Began as a 20-member physician-led steering committee in fall 2010
• Developed over eight months as collaboration between independent and employed community physicians and Cone Health
• Formed officially in 2011 as a Clinically Integrated Network serving the Piedmont Triad area
• Is an affiliate of the Cone Health System, but governance and operations is led by physicians
• Represents a new model of care – clinical integration - designed to align physicians and hospitals to improve access, improve quality and lower costs.
www.TriadHealthCareNetwork.com
8
Triad HealthCare Network Goals
• Allow physicians to have the opportunity to lead and have a voice in the necessary changes in healthcare versus simply being passive and have change dictated
• Engage physicians to develop new models of care and true “transformation” of the local healthcare delivery system
• Provide resources to physicians to meet the growing demands of accountability and transparency
• Create greater collaboration and trust among physicians, hospitals, patients and payers
• Be renowned as a national leader in delivering exceptional health care value in terms of cost, quality and service
www.TriadHealthCareNetwork.com
9
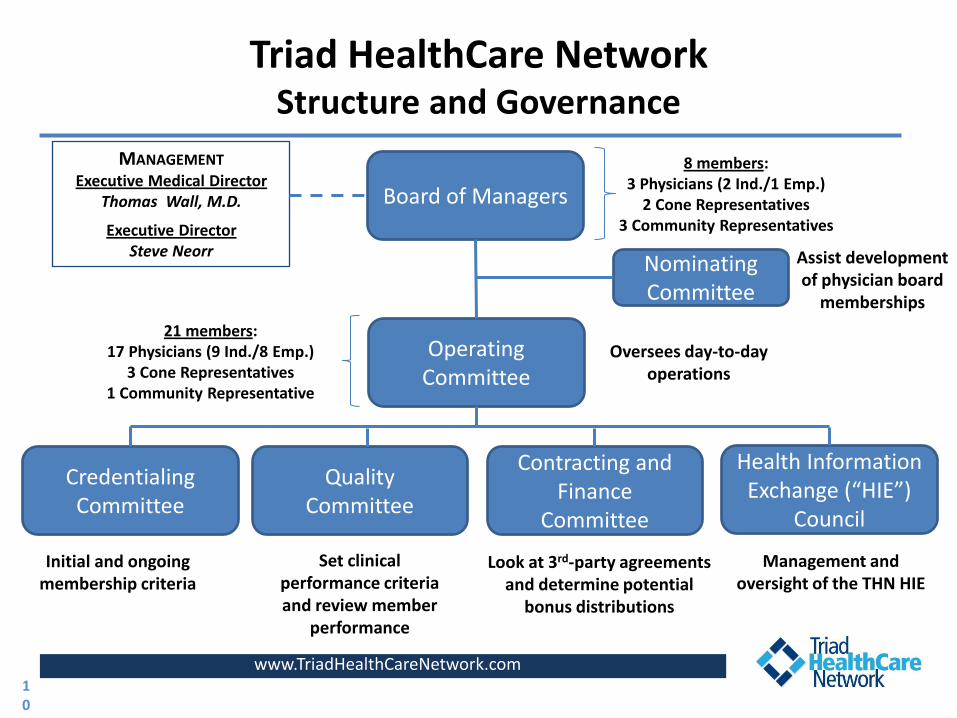
Triad HealthCare Network Structure and Governance
Board of Managers
Operating Committee
Nominating Committee
Contracting and Finance
Committee
Quality Committee
Credentialing Committee
Initial and ongoing membership criteria
Set clinical performance criteria and review member
performance
Look at 3rd-party agreements and determine potential
bonus distributions
Assist development of physician board
memberships
Oversees day-to-day operations
www.TriadHealthCareNetwork.com
8 members: 3 Physicians (2 Ind./1 Emp.)
2 Cone Representatives 3 Community Representatives
21 members: 17 Physicians (9 Ind./8 Emp.)
3 Cone Representatives 1 Community Representative
MANAGEMENT Executive Medical Director
Thomas Wall, M.D.
Executive Director Steve Neorr
10
Health Information Exchange (“HIE”)
Council
Management and oversight of the THN HIE
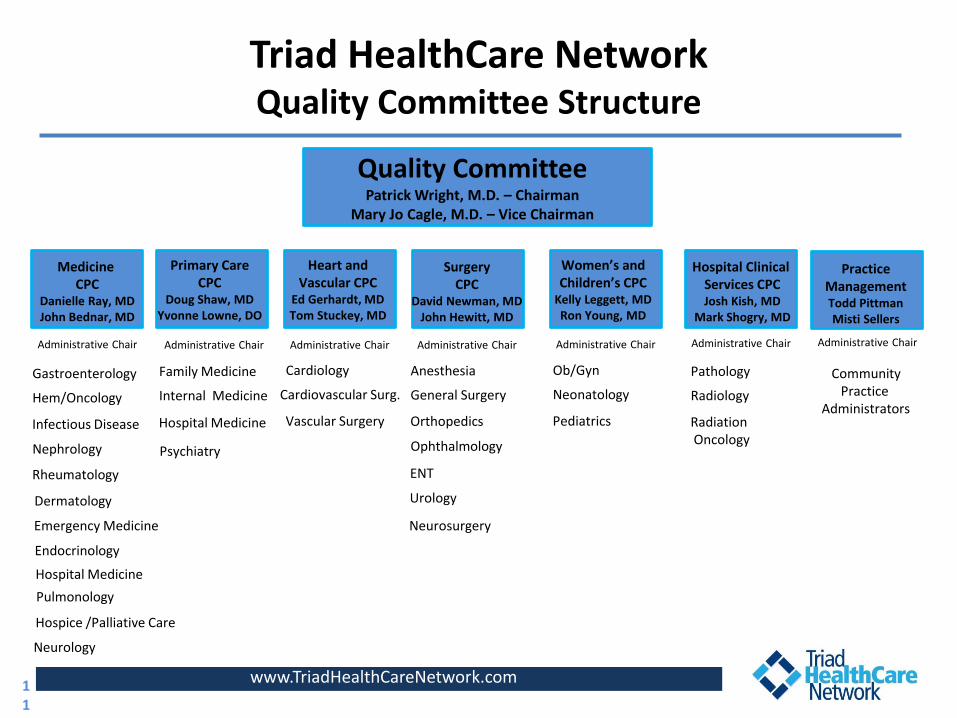
Triad HealthCare Network Quality Committee Structure
www.TriadHealthCareNetwork.com
Family Medicine
Quality Committee Patrick Wright, M.D. – Chairman
Mary Jo Cagle, M.D. – Vice Chairman
Medicine CPC
Danielle Ray, MD John Bednar, MD
Primary Care CPC
Doug Shaw, MD Yvonne Lowne, DO
Heart and Vascular CPC
Ed Gerhardt, MD Tom Stuckey, MD
Surgery CPC
David Newman, MD John Hewitt, MD
Women’s and Children’s CPC
Kelly Leggett, MD Ron Young, MD
Hospital Clinical Services CPC Josh Kish, MD
Mark Shogry, MD
Internal Medicine
Hospital Medicine
Gastroenterology
Hem/Oncology
Infectious Disease
Nephrology
Rheumatology
Dermatology
Emergency Medicine
Endocrinology
Hospital Medicine
Pulmonology
Neurology
Neurosurgery
Cardiology
Cardiovascular Surg.
Vascular Surgery
Anesthesia
General Surgery
Orthopedics
Ophthalmology
ENT
Urology
Ob/Gyn
Neonatology
Pediatrics
Pathology
Radiology
Radiation Oncology
Practice Management Todd Pittman Misti Sellers
Community Practice
Administrators
Administrative Chair
Hospice /Palliative Care
Administrative Chair Administrative Chair Administrative Chair Administrative Chair Administrative Chair Administrative Chair
Psychiatry
11
Triad HealthCare Network Structure and Membership (as of March 2013)
• Physician-led governance and committees composed of 50/50 split between PCPs and Specialists and employed and independent physicians
• 776 Affiliated physicians; 324 employed by Cone
– 55 groups; separate tax IDs
• 231 Primary Care Physicians across the community
– 180 Adult Medicine • 58 Unique clinic locations; 26 different EMR systems; 7 practices no EMR
– 51 Pediatricians
• 11 Unique clinic locations; 4 additional EMR systems
www.TriadHealthCareNetwork.com
12
www.TriadHealthCareNetwork.com
Triad HealthCare Network Driving Care Transformation
• Deployment of advanced IT resources to support population management
• Care Management team to support practices
• Assistance to achieve Patient-Centered Medical Home recognition and practice transformation
• Facilitate care process redesign
13
Triad HealthCare Network Key IT functions considered to transform delivery
www.TriadHealthCareNetwork.com
14
• Aggregate clinical data from disparate sources – EPIC, community EHRs, payer claims data, other hospitals, reference labs, radiology results, etc.
• Deliver “actionable” clinical data to physicians - at the point of care, disease registries, portals, faxes, etc.
• Proactively identify those at the highest risk – ability to make proactive interventions in disease progression
• Routinely report physician performance and compliance to national metrics, benchmarks and standards
• Report and manage cost efficiency among providers
Information Technology/Analytics Systems
• Reports performance to quality metrics • Provides clinical protocol engine; Clinical recommendations • Point-of-care reports • Patient disease registries
• Claims data integration
• Interfaces with community providers and aggregates clinical data • Hospitals • Physicians • Labs/Pharmacy/Radiology
• Master Patient Index (“MPI”) • Provides portal view to all providers
• Case Management module – care documentation, communication
• Patient stratification; Predictive risk
• Utilization and cost efficiency analytics
Clinical Performance Reporting System
Health Information Exchange (“HIE”)
Population analytics, utilization, case management module
www.TriadHealthCareNetwork.com
15
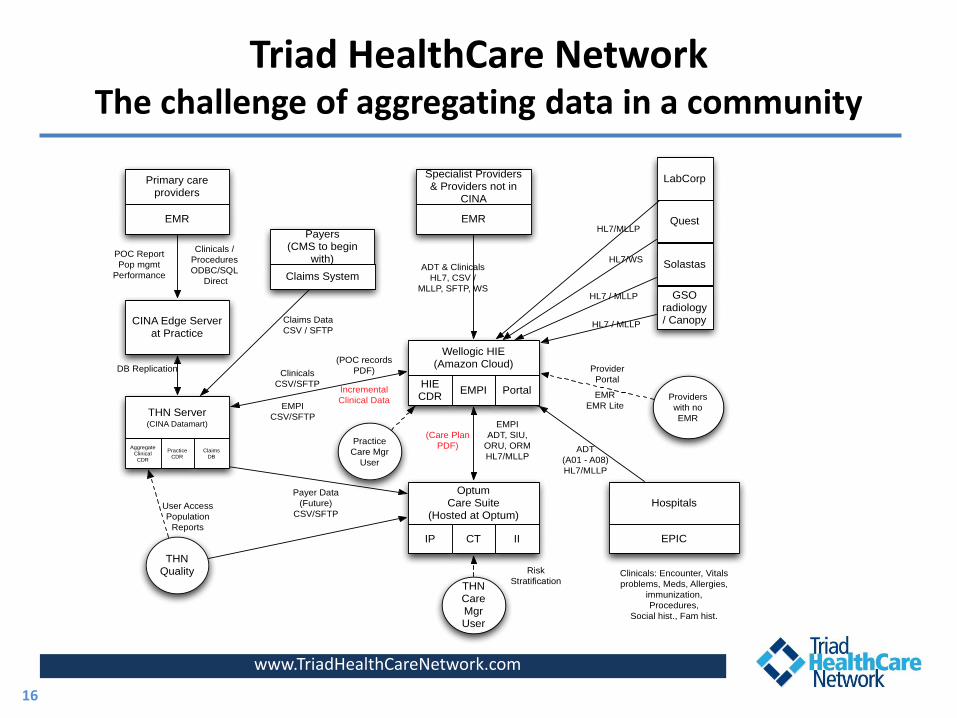
Triad HealthCare Network The challenge of aggregating data in a community
www.TriadHealthCareNetwork.com
16
Wellogic HIE (Amazon Cloud)
HIE CDR
EMPI Portal
Specialist Providers & Providers not in
CINA
EMR
ADT & Clinicals
HL7, CSV /
MLLP, SFTP, WS
Primary care providers
EMR
CINA Edge Server at Practice
Payers (CMS to begin
with)
Claims System
THN Server(CINA Datamart)
Aggregate Clinical
CDR
POC Report
Pop mgmt
Performance
Clinicals /
Procedures
ODBC/SQL
Direct
DB Replication
THN Quality
User Access
Population
Reports
OptumCare Suite
(Hosted at Optum)
IP CT II
EMPI
ADT, SIU,
ORU, ORM
HL7/MLLP
Clinicals
CSV/SFTP
EMPI
CSV/SFTP
Payer Data
(Future)
CSV/SFTP
LabCorp
Quest
Solastas
HL7/MLLP
HL7/WS
HL7 / MLLP
Providers
with no
EMR
Provider
Portal
EMR
EMR Lite
Hospitals
EPIC
ADT
(A01 - A08)
HL7/MLLP
THN Care Mgr User
Risk
StratificationClinicals: Encounter, Vitals
problems, Meds, Allergies,
immunization,
Procedures,
Social hist., Fam hist.
Claims Data
CSV / SFTP
Practice
Care Mgr
User
Incremental
Clinical Data
(POC records
PDF)
(Care Plan
PDF)
GSO radiology/ CanopyHL7 / MLLP
Practice CDR
ClaimsDB
CINA Point of Care Report
www.TriadHealthCareNetwork.com
17
• Improving Care Delivery to Patients
– Guides decision making at the Point of Care
– Drives consistent care delivery across providers / practices / THN
– Promotes team based care delivery
– Integrates data beyond the EMR – claims, hospital, community
• Encouraging Patient Responsibility
– Provides easily accessible tool for Patient Engagement
– Encourages “talking points” between the patient and care team
• Benefiting Practice Management
– Enhances current / new revenue generation
– Highlights ACO required metrics for reporting
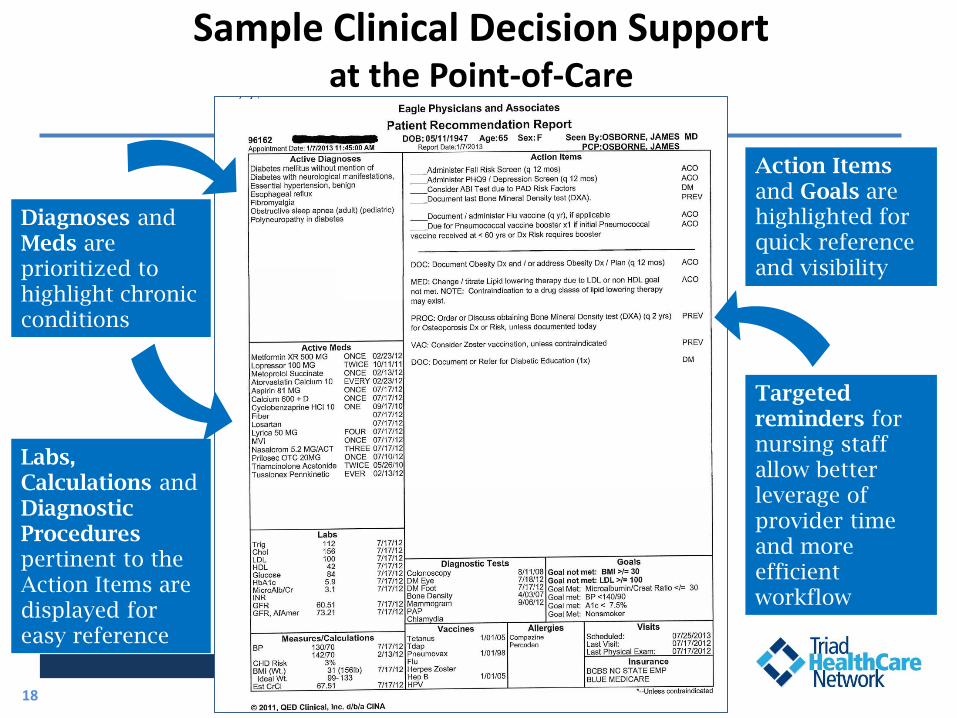
Sample Clinical Decision Support at the Point-of-Care
www.TriadHealthCareNetwork.com
Practice Performance Feedback
18
Diagnoses and Meds are prioritized to highlight chronic conditions
Action Items and Goals are highlighted for quick reference and visibility
Targeted reminders for nursing staff allow better leverage of provider time and more efficient workflow
Labs, Calculations and Diagnostic Procedures pertinent to the Action Items are displayed for easy reference
Wellogic Health Information Exchange
www.TriadHealthCareNetwork.com
19
• Connects healthcare information systems and devices across the continuum of care:
– Primary care physician & specialist offices
– Hospitals
– Long term care facilities
– Laboratories
– Imaging Centers
– Pharmacies
– Payers
• Creates “one patient one record” across all venues of care
• Delivers tests, reports, alerts, and decision support recommendations wherever necessary
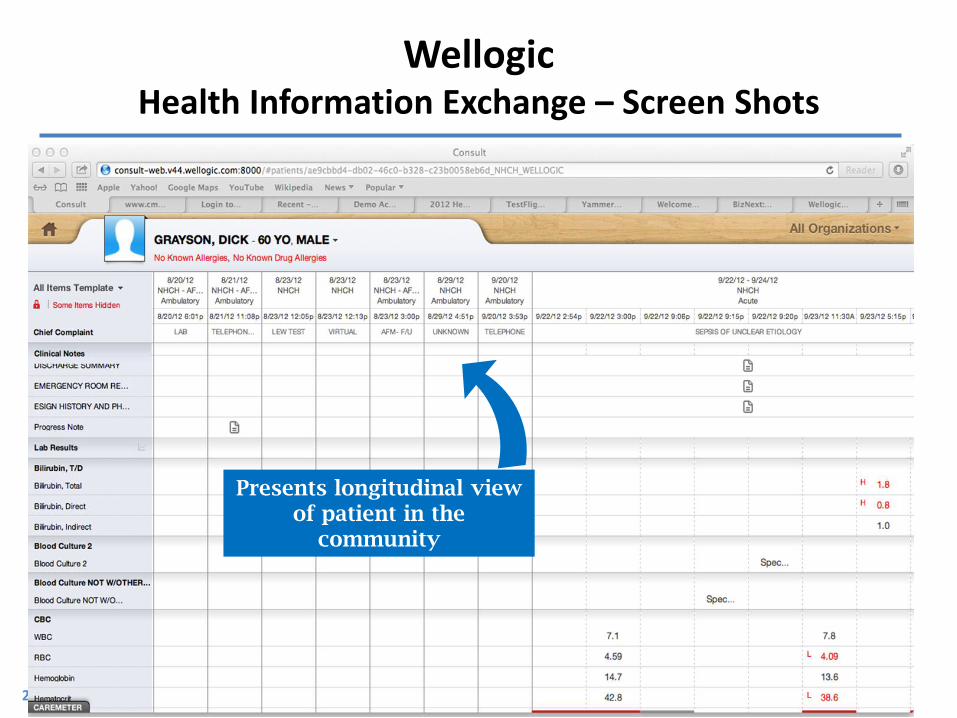
Wellogic Health Information Exchange – Screen Shots
20
Presents longitudinal view of patient in the
community
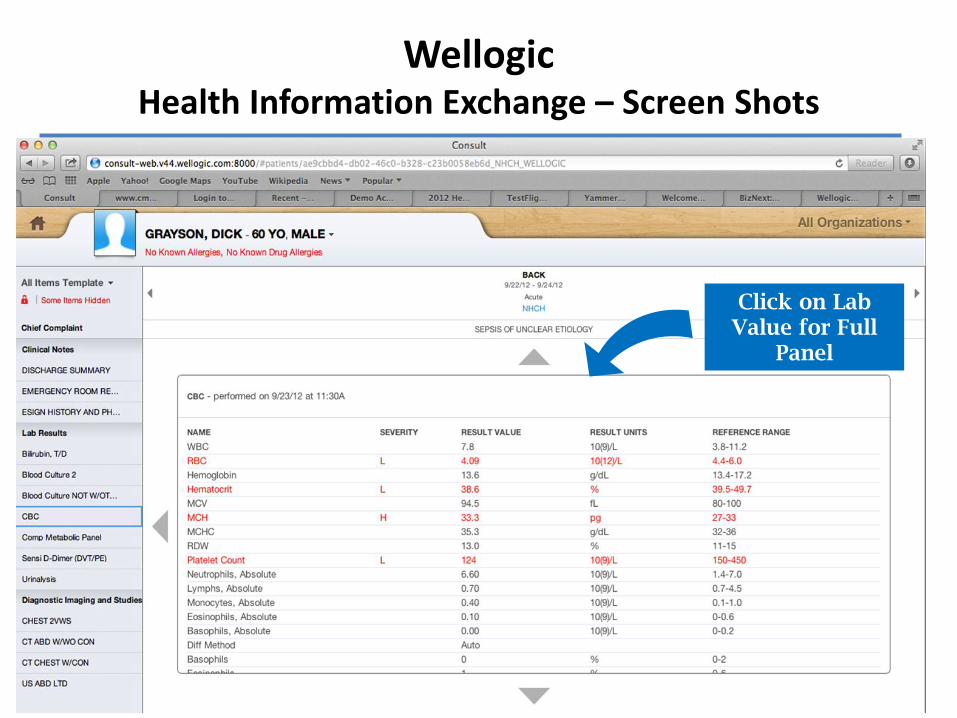
Wellogic Health Information Exchange – Screen Shots
21
Click on Lab Value for Full
Panel
Optum Population Management/Analytics
www.TriadHealthCareNetwork.com
22
• Overall impact of Optum
– Risk stratification and interventions • Who should THN Care Management help manage?
– Severity of illness determination
– Utilization, cost efficiency • PCPs, SCPs, Episode Treatment Groups (ETGs)
• Effect on day to day PCP activities
– Communication with THN Care Management
www.TriadHealthCareNetwork.com
23
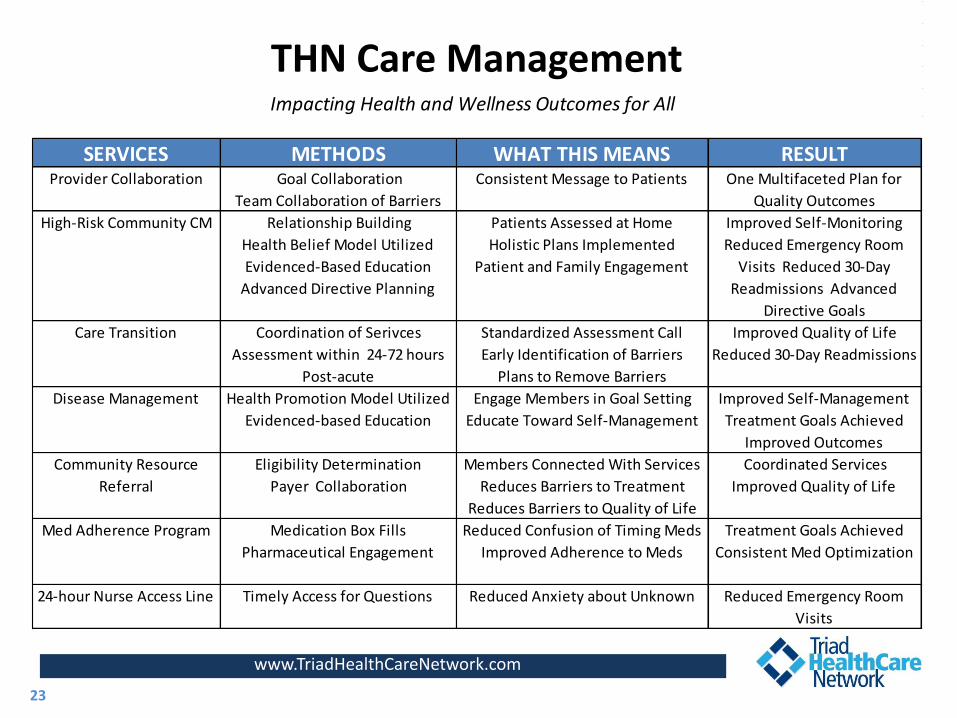
SERVICES METHODS WHAT THIS MEANS RESULTProvider Collaboration Goal Collaboration
Team Collaboration of Barriers
Consistent Message to Patients One Multifaceted Plan for
Quality Outcomes
High-Risk Community CM Relationship Building
Health Belief Model Utilized
Evidenced-Based Education
Advanced Directive Planning
Patients Assessed at Home
Holistic Plans Implemented
Patient and Family Engagement
Improved Self-Monitoring
Reduced Emergency Room
Visits Reduced 30-Day
Readmissions Advanced
Directive Goals
Care Transition Coordination of Serivces
Assessment within 24-72 hours
Post-acute
Standardized Assessment Call
Early Identification of Barriers
Plans to Remove Barriers
Improved Quality of Life
Reduced 30-Day Readmissions
Disease Management Health Promotion Model Utilized
Evidenced-based Education
Engage Members in Goal Setting
Educate Toward Self-Management
Improved Self-Management
Treatment Goals Achieved
Improved Outcomes
Community Resource
Referral
Eligibility Determination
Payer Collaboration
Members Connected With Services
Reduces Barriers to Treatment
Reduces Barriers to Quality of Life
Coordinated Services
Improved Quality of Life
Med Adherence Program Medication Box Fills
Pharmaceutical Engagement
Reduced Confusion of Timing Meds
Improved Adherence to Meds
Treatment Goals Achieved
Consistent Med Optimization
24-hour Nurse Access Line Timely Access for Questions Reduced Anxiety about Unknown Reduced Emergency Room
Visits
Impacting Health and Wellness Outcomes for All
THN Care Management
Triad HealthCare Network Care Management Team Supports Practices
www.TriadHealthCareNetwork.com
24
Rhonda Rumple, RN, MSN, CCM - Program Director
RN Care Managers (16)
Licensed Clinical Social Workers (3)
RN Hospital Liaisons (2)
Care Management Assistants (2)
Geriatric Nurse Practitioner (1)
Clinical Pharmacist Manager (1)
Access Data Base Specialist (1)
www.TriadHealthCareNetwork.com
• Engaged TransforMED to lead PCMH initiative
– Train the trainer model
• Teamed with local Area Health Education Center (AHEC) to provide “boots on the ground”
– Funding one AHEC FTE dedicated to THN PCMH initiative
• Identified 24 initial practices expressing interest to go through process
– Wave 1: 5 practices; Late March 2013
– Wave 2: 13 practices; June 2013
– Wave 3: 4 practices; September 2013
– Wave 4: 2 practices; January 2014
25
Triad HealthCare Network PCMH Assistance
www.TriadHealthCareNetwork.com
• Readmissions - System-wide breakthrough project
– CHF
– COPD
– Pneumonia
– High ED use/Past Admissions
• Care Transitions – Hand offs, access
• Chronic disease management
– CHF
– Diabetes – Sanofi support
– Hypertension
26
Triad HealthCare Network Facilitating Care Process Redesign
Triad HealthCare Network Contracting Approach
• Initial focus on quality, not joint FFS, contracting
• Practice maintains control of billing and collection
• Practice makes claims and EMR information available
– Goal to create community Clinical Data Repository (CDR)
• Focus on incentive-based contracts based on quality and cost control initiatives
– P4P, shared savings, gain sharing
• THN negotiates a “Savings/Bonus Pool” with the payers – government, insurance companies and employers
• THN is responsible for managing / distributing bonus payments
www.TriadHealthCareNetwork.com
27
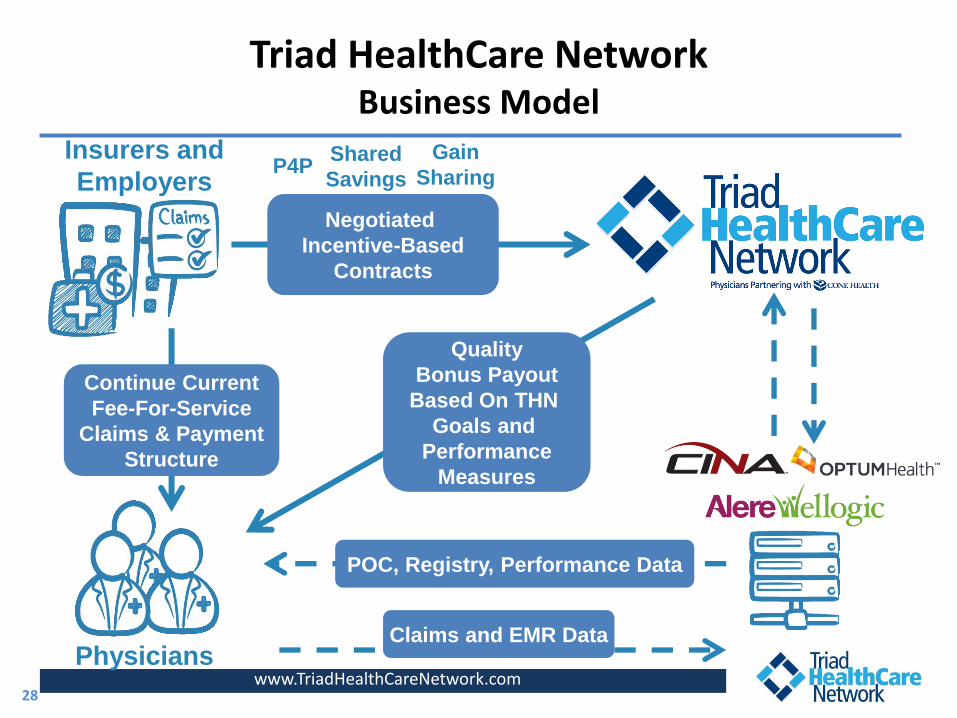
Triad HealthCare Network Business Model
www.TriadHealthCareNetwork.com
Continue Current
Fee-For-Service
Claims & Payment
Structure
Quality
Bonus Payout
Based On THN
Goals and
Performance
Measures
Insurers and
Employers
Negotiated
Incentive-Based
Contracts
Physicians Claims and EMR Data
POC, Registry, Performance Data
P4P Shared
Savings
Gain
Sharing
28
www.TriadHealthCareNetwork.com
• Affiliated with over 750 community physicians – over 50% independent
• Developed physician-led infrastructure
• Identified 129 quality metrics across all major specialties
• Approved to participate in Medicare Shared Savings Program as ACO – Over 40,000 Medicare beneficiaries
• Identified and begun deployment of Clinical Performance Reporting System, Health Information Exchange (“HIE”), and population analytics, utilization, case management modules
• Identification and hiring of case management “team”
29
Triad HealthCare Network First Year Accomplishments
www.TriadHealthCareNetwork.com
• PCP alignment/attribution is difficult
– Not prepared for initial MSSP list
• Underestimated time and effort to send letters to 40,000 patients
• Interfacing and connecting practices takes longer than anyone will tell you
• Vendors are all learning too
• EMR data is not structured and standardized and time consuming to validate
• Clinical data is difficult to aggregate and report – must standardize
30
Triad HealthCare Network Lessons Learned – Administrative Perspective
www.TriadHealthCareNetwork.com
• Need a plan to educate and train multiple clinics (physicians and staff)
• Should have required EMR use to participate
• Develop a model to distribute “maybe money’ earlier versus later
• Plan well ahead for care management and analytics
• Have a plan to manage your population assuming you do not have much data initially
• Limit your initiatives and focus on key areas
– “You can have a lot of ammunition and never get a shot off.”
31
Triad HealthCare Network Lessons Learned - Administrative Perspective
www.TriadHealthCareNetwork.com
• Take the time to develop understanding, unity and buy-in from your core physician leaders.
• Physician culture is one of skepticism. Don’t expect full buy in from all physicians at first.
• Physicians witnessing the health system committing resources based on the potential is very influential.
• ACO leadership needs a balance of internal and external representation – old and new.
• Physician engagement is key. Provide many opportunities for involvement.
32
Triad HealthCare Network Lessons Learned – Physician Perspective
www.TriadHealthCareNetwork.com
• Be cognizant of and transparent about hot button topics – money, employed vs. independent, PCP vs specialists; MEC
• Focus on Primary Care.
• Need to expand physician definition of professionalism to include a vision of a team and bigger picture.
• Be aware and sensitive to ‘change overload.’
• Don’t expect too much help from the government
33
Triad HealthCare Network Lessons Learned – Physician Perspective
Questions?
For further information, please visit www.TriadHealthCareNetwork.com
www.TriadHealthCareNetwork.com
34






![[sv] Validity date from LAND Vietnam 00269 [SV] SECTION ... · 2 / 33 [sv] List in force Godkännandenum mer Namn Ort [sv] Regions [sv] Activities [sv] Remark [sv] Date of request](https://img.pdfslide.us/doc/110x75/5d66deeb88c99332038b89d9/sv-validity-date-from-land-vietnam-00269-sv-section-2-33-sv-list.jpg)

![[sv] Validity date from LAND Marocko 00258 [SV] SECTION … · 2020. 5. 22. · 1 / 35 LAND [SV] SECTION Marocko Fiskeriprodukter [sv] Validity date from 10/08/2007 [sv] Date of publication](https://img.pdfslide.us/doc/110x75/5fbce723db71870cc10035f6/sv-validity-date-from-land-marocko-00258-sv-section-2020-5-22-1-35-land.jpg)




















![[Irina Nikolaeva] Finiteness Theoretical and Empi(Bookos.org)](https://img.pdfslide.us/doc/110x75/55cf9bf8550346d033a810bc/irina-nikolaeva-finiteness-theoretical-and-empibookosorg.jpg)