Embed Size (px)
Citation preview

Delivering an Integrated Age Inclusive
Pathway Making sure young people don’t fall into gaps
Dr Sarah Maxwell
Dr Jon Wilson

Overview
• Improving CAMHS/AMHS services
– What is or isn’t working
• How do we remove the gaps during transition?
• Moving forward

Improving CAMHS/AMHS services
• What is or isn’t working

CAMHS perspective
• Stakeholder days & Service user feedback (local and national); – Need to improve
• Accessibility
• Communication
• Partnership or joint working
• Consultation and liaison
• Training and supervision
• Consistency
• Problems with transfer to AMHS
• Crisis or out of hours services

AMHS/EI perspective
• Young people with emerging disorders who are
not psychotic don’t get a service – Central Norfolk EIT - Team C
• Service to young people with emerging disorders
• Mentioned as an example of good practice in SCIE website
• AMHS inclusion criteria – “severe & enduring mental illness”
– Young people don’t present like this so don’t fit

CLARHC Research utilised to measure problem of transitions
and access and engagement – local relevance
Transition CAMHS to AMHS

McGorry, P 2009
• “the surge of new morbidity between the
ages of 15 and 25 is paired with the worst
access to services, the system is
weakest where it needs to be
strongest.”

Whole system issue
• Not just a mental health service problem also need to look at whole range of services offered to young people
– Local Authority
– Voluntary sector
– Service user input

funded by CLAHRC

The Norfolk Youth Mental Health Model: Pathways to care of young people accessing
a pilot youth mental health service
Submitted for publication

What do we mean by Pathways to Care?
What were our aims and rationale?
What did we do?

Measuring pathways:

Measuring pathways:
1.36 Years (0 – 10.59) 2.27 Years (0.05 – 11.84)

Measuring pathways:

Measuring pathways:
3.74 Years (0.64 – 12.84)

5.53 (1–20) Pathways

(b) Example of short “stepped-care” pathway (3.53 years)
(a) Example of short “direct” pathway (2.5 weeks)
Distinct patterns of pathways:

(b) Example of long “stepped-care” pathway (3.53 years)
(a) Example of short “direct” pathway (2.6 weeks)
Distinct patterns of pathways:

(d) Example of complex pathway of short duration (1.07 years)

(d) Example of complex pathway of short duration (1.07 years)

Bridging the gaps
“We can’t solve problems by using the same kind of thinking we used when we created them…..”

How do we remove the gaps during transition?
• Within our services
– Essentially we got rid of the transition at 18y
– But created 2 new ones?
• With external services
– Partnership working
– Consultation with other agencies
– Integrated commissioning – a pipe dream?!

Pilot
• 12 months focusing on most severe
• 3 pilot sites
• 14 – 25 year olds with complex mental health problems
– HoNOS Clusters 5 to 17
– CGAS score, 50 and below
• Caseload – 225 CAMHS and 75 AMHS
• Consultant and teams provided by Adult and Adolescent practitioners including Dr’s, MHP’s, OT’s, Psychologists etc

Beck Depression Inventory
78%
13%
9%
Severe depression (score of >29)
Moderate depression (score of 20 to 28)
Mild depression (score of 14 to 19)

Social Interaction Anxiety Scale
44%
35%
21%
Social anxiety (score of 42+)
Social phobia (score of 34 to 42)
Below clinical cut-off for socialanxiety (score of <34)

Trauma History Questionnaire
84%
72%
45%
39%
25%
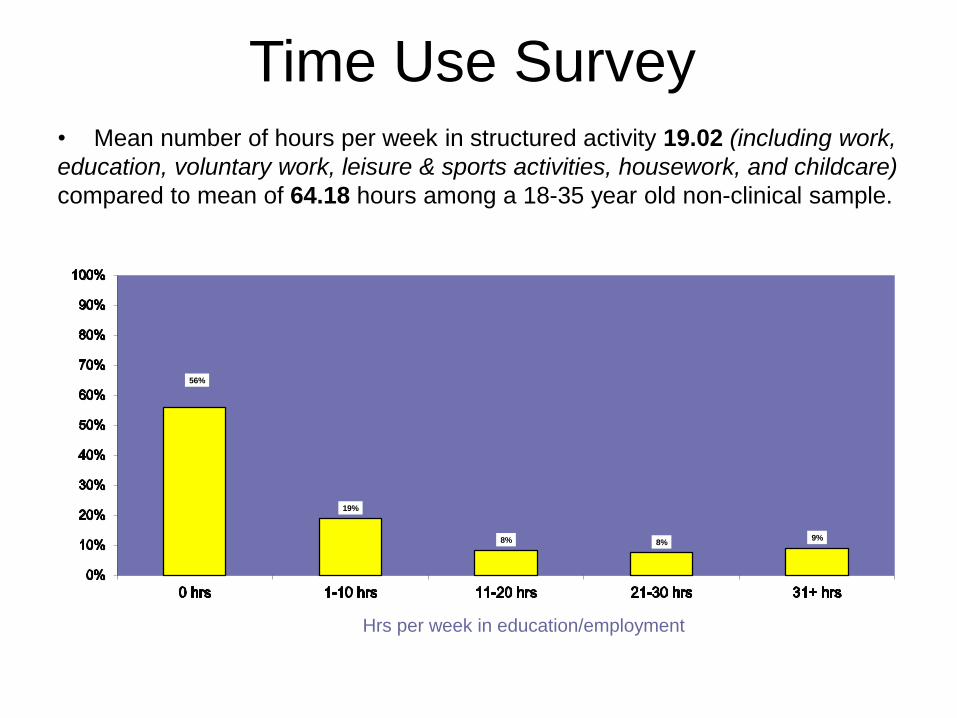
Time Use Survey • Mean number of hours per week in structured activity 19.02 (including work,
education, voluntary work, leisure & sports activities, housework, and childcare)
compared to mean of 64.18 hours among a 18-35 year old non-clinical sample.
56%
19%
8% 8% 9%
Hrs per week in education/employment

Hofstra et al 2001, Harrington 1990, Jones et al 1993
• Amongst this group it is the emergence of social decline in association with a pattern of
co-morbid non-specific psychopathology (depression and social anxiety) which appears to be a key indicator of social disability across
disorders

Move to full Youth Service
• Service for all young people aged 14 to 25 with severe of complex mental health problems

taken from Early Intervention in Psychosis key principles
Youth Service principles • Being and to engage this group early
in severe mental illness (allowing staff to develop skills required)
• Being to minimise functional disability and maximise potential
• Offer with a service user involved approach
• Having an assertive outreach component
• Aiming to / mental health act use
• Working with
• Promoting
with other support agencies
• Using and seeking to where none exists.

Aims of the service
young people at highest risk of developing enduring mental health difficulties
• Provide support
• Get young people well enough to engage with the Norfolk Wellbeing Service or:
• Well enough to engage in treatment
where possible through risk management with the IST / CRHT
• Then ensure that a service user is linked into appropriate (education, youth groups etc)
• Provide support

Tim’s Picture of the service???

Outcomes
Changes in mean scores at the different time points were analysed using paired t-tests.
Time point 1 Time point 2 Result
Baseline 6 months Significant improvement across all measures
Baseline 1 year No significant difference
6 months 1 year No significant difference
6 months Discharge No significant difference
1 year Discharge No significant different
Baseline Discharge Significant improvement across all measures

Transition revisited
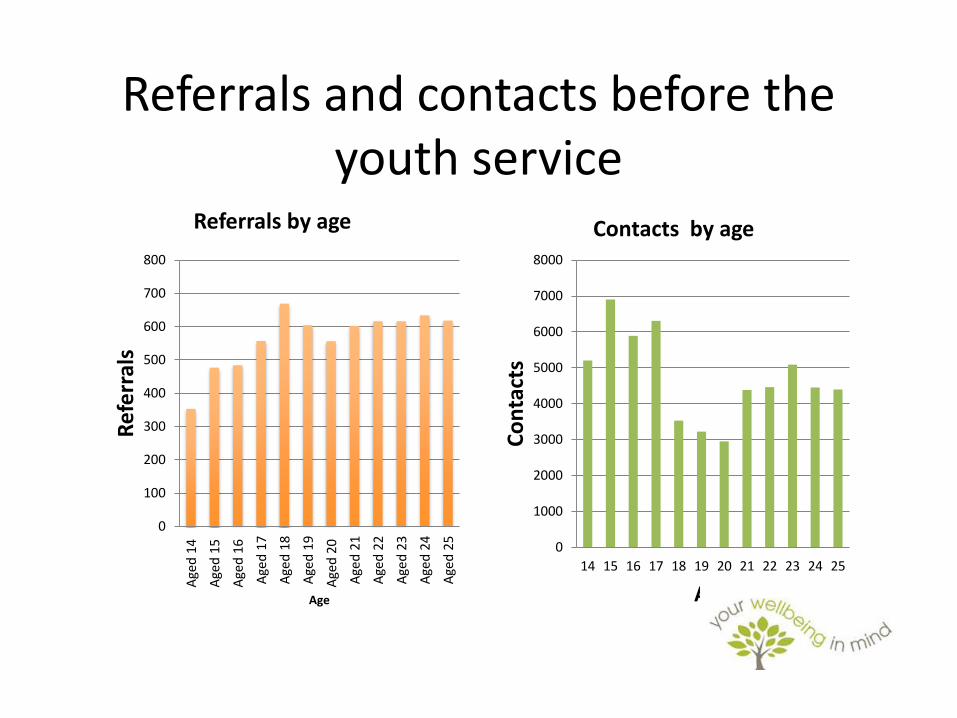
Referrals and contacts before the youth service
0
100
200
300
400
500
600
700
800
Age
d 1
4
Age
d 1
5
Age
d 1
6
Age
d 1
7
Age
d 1
8
Age
d 1
9
Age
d 2
0
Age
d 2
1
Age
d 2
2
Age
d 2
3
Age
d 2
4
Age
d 2
5
Ref
err
als
Age
Referrals by age
0
1000
2000
3000
4000
5000
6000
7000
8000
14 15 16 17 18 19 20 21 22 23 24 25
Co
nta
cts
Age
Contacts by age

Referrals and contacts after the youth service
0
100
200
300
400
500
600
700
800
900
1000
14 15 16 17 18 19 20 21 22 23 24 25
Ref
err
als
Age (years)
Referrals by age
0
2000
4000
6000
8000
10000
12000
14 15 16 17 18 19 20 21 22 23 24 25
Co
nta
cts
Age (years)
Contacts by age

Number of contacts per referral by age
Before the Youth Service
0
2
4
6
8
10
12
14
16
14 15 16 17 18 19 20 21 22 23 24 25
Nu
mb
er
of
con
tact
s p
er
refe
rral
Age (years)
After the Youth Service
0
2
4
6
8
10
12
14 15 16 17 18 19 20 21 22 23 24 25
Nu
mb
er
of
con
tact
s p
er
refe
rral
Age (years)

Moving Forward

Challenges/Opportunities
• Huge change with resistance from both CAMHS and AMHS
• Challenge to maintain culture of accessibility in face of demand – how not to default back to saying “no”?
• Leadership from both CAMHS and AMHS
• Need wider system change – Partnership boards, Commissioners, collaboration overall
• Diversity of funding options

• “If you want to build a ship, don’t drum up people together to collect wood and don’t assign them tasks and work, but rather teach them to long for the endless immensity of the sea”
Antoine de Saint-Exupery French pilot, author “The Little Prince”