Embed Size (px)
Citation preview

Deliverable 4.1.5
Relevant Scientific Paper for Health Impacts of Disasters
Draft document with unpublished data.
UniversitätsKlinikum Heidelberg
Abt. Tropenhygiene und Öffentliches GesundheitswesenIm Neuenheimer Feld 324, D- 69120 Heidelberg, Germany.Tel. +49-6221-56 5040, Fax +49-6221-56 5051(www.heidelberg-university-hospital.com/)

Revati Phalkey Page 2 Draft document_12/1/2009
Injuries reported at a rural hospital after the Gujarat, IndiaEarthquake of 2001 – A call for standardization of earthquakeinjury data recording and reporting.
Phalkey, R* and Marx, M. *
* Department of Tropical Hygiene and Public Health, University of Heidelberg, Heidelberg, Germany.
Abstract
The paper presents a retrospective analysis of injuries treated at a secondary rural hospital inthe Kutch district, Gujarat, India following the January 26, 2001 earthquake. Discharge reportsof patients admitted to the hospital over 10 weeks from January 26, 2001 to April 1, 2001 wereanalyzed for earthquake related injury data. Orthopedic injuries, (particularly fractures of thelower limbs) were predominant and serious injuries like head, chest, abdominal, and crushsyndrome were minimal. The most frequently performed surgical procedures were openreduction with internal fixations, and cleaning and debridement of contaminated wounds. Foursecondary deaths and 102 transfers to tertiary care are reported.
A review of 29 published studies reporting earthquake injuries (1976-2007) rendered data thatwas incomparable due to non-standardized assessment and reporting procedures used. Despite ahigh mortality to injury ratio of 1:3, no international disaster database to date maintainsepidemiological records of earthquake injuries. Given that early effective response strategiesform the mainstay of earthquake impact reduction, standardization of recording and reportingearthquake injuries is urgently mandated. Homogeny is essential to ensure data comparabilityand to guide evidence-based preparedness and response. The authors recommend a uniforminjury case reporting form as a first step towards data standardization.
Key words: disaster, earthquake, injury-epidemiology, data- standardization
Introduction
Over 281 earthquakes occurred in 58 countries between 1996-2005, causing more
than 162,986 deaths and affecting over 39 million people (CRED, 2006). The number
of injured far exceeds those dead and the average injury to mortality ratio in
earthquakes has been marked at 3:1 (C. De Ville de Goyet and M.F Lechat, 1976).
Immediate effective medical response significantly influences injury outcome and
hence the overall health impact of earthquakes. Inadequate or mismanagement of
injuries may lead to disabilities and additionally contribute to the disability burden of
the population thus creating future vulnerabilities. This has important ramifications in

Revati Phalkey Page 3 Draft document_12/1/2009
developing countries especially in Asia where most earthquakes strike in densely
populated areas (Guha-Sapir, 1986).
Lack of precise data from immediate aftermath is seen as a remarkably weak point in
overall disaster epidemiology (Guha-Sapir, 2006; Lechat, 1979). Compiling injury
data in very early stages of an earthquake is rather unwelcome as the focus, and
rightly so, is upon saving lives and up-scaling infrastructure to surge capacity for
adequate response.
Given that earthquakes are difficult to predict with a narrow pre warning period the
two points of entry for mitigating their health impacts include anti seismic building
and effective early rescue and first aid (Lechat 1989). The prohibitive costs of seismic
hazard proof construction compromises the adherence to and the implementation of
anti-seismic building codes in most developing countries. The information on injury
patterns from previous earthquakes then becomes crucial in guiding effective
preparedness and successful response programs in resource poor settings. However,
to date few studies have been completed at a population level in detail. An analysis of
existing studies revealed sparse, incomplete, inconsistent, non-standardized and often
missing data.
The rational of the paper is to further the knowledge of the injury epidemiology after
earthquakes to ensure appropriate timely response and help reduce and prevent
disabilities arising from mismanagement of injuries. The authors see the study as a
reasonable contribution for missing population-based non-fatal earthquake injury

Revati Phalkey Page 4 Draft document_12/1/2009
epidemiology information and aim to understand the issues in quality and quantity of
injury data reporting and recording.
The last earthquake with its epicenter in India was the Kutch district, Gujarat
earthquake that struck on January 26, 2001 at 08.46 hrs at a magnitude of 6.9. The
epicenter was located in North-East of Bhuj city and the quake lasted 80-150 seconds
affecting over 8792 villages, in 171 Talukas (Governmental administrative units) of
the 21 districts in Gujarat (GOG, 2007b; IMD, NA). The worst affected regions
included predominantly rural areas of Bhuj, Anjar, Rapar, and Bachau. Significant
damage was reported from the urban areas of Ahmedabad, Gandhidham, Rajkot,
Jamnagar, Surat, Surendranagar and Morbi (GOG, 2007b). Human impact of the
earthquake included 20,000 deaths and over 1.6 million (including 20,717 serious)
injuries (Roy et al., 2002). The district of Kutch accounted for more than 92% of the
deaths and 82% of the total injuries reported (Benedick et al., 2001).
Primary failure of the health care facilities in the district due to structural damage
delayed much required early response. The G.K General civil hospital a 44 -year-old
structure (with 250- beds), a crucial secondary referral centre in Bhuj was completely
damaged and collapsed killing 150 patients, 7 nurses and 4 employees (Sharma,
2001). Three other main hospitals in Bhuj city, the Jubilee hospital, the Mental
hospital, and the Branch hospital also collapsed. Almost all of the hospital facilities in
Kutch at Bhuj, Anjar, Bachau and Gandhidham were destroyed including 2 hospitals,
8 community health centers, 42 primary health care centers, 37 dispensaries and 227
sub-centers (Bremer, 2003; Vatsa, 2001).

Revati Phalkey Page 5 Draft document_12/1/2009
Bidada Sarvodaya hospital was an intact health care facility 60 kilometers from the
epicenter. This trust run, private, charitable, hospital organizes an annual health camp
(in January) for the Kutch district population for the last 20 years covering operative,
boarding, lodging and travel costs. Funded by Indian Diaspora mainly in the United
States many of them super-specialty consultants with medical students and
professionals from the larger cities in Gujarat join to assist with primary as well as
super-specialty care. Since the January 26, 2001 earthquake closely followed the
completion of the annual camp, the voluntary network was immediately activated.
Figure 1: The study site.
Materials and Methods
The study is a retrospective cross sectional analysis of secondary data obtained from the
Bidada Sarvodaya hospital, Kutch, Gujarat, India completed in August 2007. Approval
for the site visit was obtained from the Director, Bidada Rehabilitation Centre and the

Revati Phalkey Page 6 Draft document_12/1/2009
Chairman of the hospital. Access to these data resulted from the author’s own work in the
Bidada hospital during the earthquake in 2001 within a relief and rehabilitation project.
Patients treated for earthquake related injuries and illnesses in the hospital over the ten-
week post quake period (January 26, 2001 to April 4, 2001) were included in the study.
Earthquake injuries were defined as those for which health care was sought, had resulted
from the January 26, 2001 earthquake, and did not result in death. In the authors opinion
the use of standard protocols Abbreviated Injury Severity (AIS) or the Injury Severity
Score (ISS) to code the injuries would defeat the precise purpose of the study to segregate
the injury types by distribution frequency and were hence not applied.
Data on the variables were extracted from the actual patient discharge case report forms.
A total of 1248 report series were reviewed by hand and analyzed for sex, age, village for
geographic origin, date of admission, date of discharge, diagnosis, injury types
(compound/ crush/ multiple/ soft tissue), anatomical side of injury, anatomical site of
injury, level and type of fractures, presence of infection, treatment imparted, hospital
procedure performed and outcome of treatment (including transfer to tertiary care). The
data obtained was entered in Microsoft™ Excel: Mac® for a descriptive analysis. All of
the 1248 discharge reports were included in the analysis for geographical origin and the
demographic data of age and sex. Of these 852 (68.2%) case reports were missing or
incomplete and hence were separated out. A total of 396 (31.7%) reports were
individually verified by the author. Although also incomplete, a careful crosschecking by
name, age, sex and origin of the patient and matched serial number to the corresponding
discharge case reports, sufficient details of additional 179 patients were recovered from
computerized information of earthquake related admissions. Thus a total of 575 (46.0%)

Revati Phalkey Page 7 Draft document_12/1/2009
patient reports were analyzable for distribution of injury by frequency and 673 (53.9%)
case reports were excluded from the analysis due to insufficient data on the study
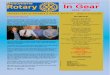
variables. The structure of the database is described in Figure 2.
Figure 2: Structure of the database.
Further, a bibliographic review of articles was performed. PubMed, Lexis Nexis, Medline,
Blackwell Synergy and Science Direct databases were used to search for the following
N - 1248
Verified 396
Non Verified852
Computerized data179 (21%)
Sufficient variabledata not available
673 (79%)
575 (396 +179) Analyzedfor distributionof injury type
673 excludedfrom injurydistribution
analysis 673
Analyzed forDemographic
data andGeographic
origin1248
N = 1248n = 575
31.7% 68.2%
100%
53.9%46.0%%

Revati Phalkey Page 8 Draft document_12/1/2009
key words: earthquake, trauma, injury, epidemiology, seismology, field hospital, Gujarat,
musculoskeletal, disasters response and natural disasters. A total of 29 studies were
identified for review that reported earthquake morbidity data. These studies published
between 1976-2007 covered 18 locations in 13 countries and reported earthquakes
between 1976-2005 (See Annex II).
Results
Descriptive analysis of the dataset
Of the 1248 case reports 100 (8.0%) had missing information for the village of origin.
The hospital received patients from almost all of the affected Talukas (Government
administrative units). Over half of the patients (51%) came from the epicenter city of
Bhuj reason being the collapsed civil hospital (G.K General Hospital) in Bhuj.
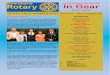
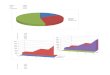
Date of admission was available for 397 of the 575 patients (Figure 3). The maximum
admissions were reported on the second day after the earthquake.
The first admission was reported on January 26, 2001 and the last on 01.04.2001. The
first discharge was reported on January 27, 2001 and the last on April 15, 2001. A
total of 185 admissions (highest for a week) and 86 discharges were recorded in the
first week. From week two to ten they were uniformly balanced. On the day of the
earthquake only 6 admissions were recorded. There was an initial lag period before
the number of discharged per day increased. It peaked on day 5 (31.01.2001) after the
earthquake, which coincided with the admissions returning to baseline (day 6). There
was a classic second wave of admissions that peaked (15 admissions) on 4th of
February, day 9 after the earthquake. The number of discharges increased in the last

Revati Phalkey Page 9 Draft document_12/1/2009
week (26.03.2001- 31.03.2001). No new admissions were recorded during this
period.
Figure 3: Admissions and discharge per day in the week following the
earthquake.
The date of admission (DOA) was missing in 33 reports and was assumed to be
26.01.2001 and these reports were included in the final analysis. The date of
discharge (DOD) was missing in 10 case report forms. These cases were excluded
from the analysis of duration of hospital stay. Thus a total of 420 patients were
analyzed for the duration of hospital stay, which ranged from 0 to 64 days. 35.3%
patients were hospitalized for less than a week and a majority of them (25.3%) stayed
between 2 to 4 days. The highest number of patients 45 (10.7%) stayed for a period of
three days followed by 40 (9.5%) who stayed for two days.
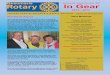
The mean age of the patients treated at the hospital was 30.7 years (± 20.87) with a
range of 0 to 90 years (See Figure 4). A total of 314 (25.1%) individuals were18
First Week185 Admissions
86 Discharge
02
5
15
8
32
17
76
32
65
46
12
75
12
0
10
20
30
40
50
60
70
26.01.2001 27.01.2001 28.01.2001 29.01.2001 30.01.2001 31.01.2001 01.02.2001 02.02.2001
Date
Nu
mbe
r of
Pat
ien
ts
Discharge
Admissions

Revati Phalkey Page 10 Draft document_12/1/2009
years old or younger and 136 (13.0%) were 60 years or older. The data showed a
predominance of middle-aged males. The gender distribution of the study group was
uniform with 621 (49.7%) males and 551 (44.1%) females. Information pertaining to
the gender of the patient was missing in 76 (6.0%) reports and that pertaining to the
age was missing in 91 (7.2%) reports.
Figure 4: Demographic information of those treated.
N=1248
0
50
100
150
200
250
-99 0-4 05-14 15-24 25-34 35-44 45-54 55-64 65-74 75-84 85-94
Age in years
Freq
uenc
y
U
M
F
-99 = Age Data not Available

Revati Phalkey Page 11 Draft document_12/1/2009
Clinical analysis of the injuries
The injuries sustained to the left (173, 39%) were marginally higher than the right
side (154, 35%) in the 441 reports that identified the anatomical side of injury. The
incidence of axial and bilateral injuries was 67 (15%) and 47 (11%) respectively. A
total of 136 patients reported multiple injuries and compound injuries were reported
in 76 out of 575 patients.
Figure 5: Anatomical site of the injury
Of the 575 patients, extremity injuries (260, 46%) predominated followed by soft
tissue injuries that mainly included cuts, bruises, contusions and lacerations (119,
20%). Two cases of abdominal injury were of burst abdomen type. Head injury (12,
2%) included minor conditions mainly fractures of the mandible. Chest injuries (11,
2%) included multiple fractures of the ribs and three cases required inter-costal drain
tube insertion for restoring respiratory function. Spinal cord injuries were low(12,
SPINE12 (2%)
TRUNK 24 (4%)
NERVE INJURIES6 (1%)
SOFT TISSUE INJURIES 119 (20%)
MULTIPLE INJURIES 136(23%)
HEAD12 (2%)
ABDOMEN 2 (0%)
CHEST11(2%)
EXTREMITIES 260 (46%)
N=575

Revati Phalkey Page 12 Draft document_12/1/2009
2%) and two cases of paraplegia reported. Nerve injuries included Brachial Plexus
Injury (3), Radial nerve (2) and Radio-Ulnar nerve (1) injuries respectively.
31 cases (5.3%) of crush injury were reported mainly of the hand and foot. The
distribution of the incidence of crush injury across the age groups was uniform with
no significant differences.
Figure 6: Frequency of fractures by fracture type.
A total of 293 cases of fractures were recorded. Lower extremity particularly Tibia-
Fibular (38.5%) and Femur (22.1%) fractures were most common followed by
Radius-Ulna fractures (9.5%). Ankle fractures (8.8%) were more common compared
to wrist (1.0%) fractures. Pelvic girdle fractures (6.8%) mainly included Acetabular
and Pubic-rami fractures. Spinal fractures (4.0%) were of burst vertebral nature.
WRIST3 (1%)
FEMUR65 (22%)
TIBIA FIBULA113 (38%)
RADIUS ULNA28 (10%)
ANKLE26 (9%)
HUMERUS21 (7%)
PELVIC GIRDLE20 (7%)
SPINAL12 (4%)
CLAVICLE5 (2%)
N= 293

Revati Phalkey Page 13 Draft document_12/1/2009
Upper extremity fractures were less frequent at 48 (16.3%) than lower extremity
fractures 203 (69.2%) amongst the 293 reported fractures. 9 patients (3.0%) reported
fractures of both upper as well as lower extremities. Dislocations (13) were less
frequent than fractures including ankle dislocations (4, 31%) followed by hip (3,
23%), radius-ulna (2, 15%) and shoulder joint (2, 15%). Wrist and elbow dislocations
were reported one each (1, 8%).
In the treatment front operative treatment was more frequent than conservative.
Plaster of Paris (POP) cast for closed fractures (17%) was most common conservative
procedure. Open Reduction and Internal Fixation (17%) was the most common
surgical procedure followed closely by cleaning and debridement of wounds (15%).
This correlates to the finding that fractures and soft tissue injuries were the two major
types of injuries sustained. Ten percent of the cases required split thickness skin
grafting.
A total of 38 amputations were recorded. Below-ankle amputations involving the foot
(36%) were most frequent followed by below-knee amputations (26%). This was in
accordance to the crush injuries, which were more common in the foot and the most
common Tibia-Fibular fractures. The level of amputation was unknown in 3 (8%)
cases.

Revati Phalkey Page 14 Draft document_12/1/2009
Figure 7: Treatment procedures performed at the hospital.
The most common general surgery procedure reported was Hernioplasty (10, 13.3%).
A total of 72 (12.1%) cases were considered unrelated directly to the earthquake by
the author. Of these conditions the single most common complaint was Hernia
followed by 9 (12.5%) cases of COPD, 4 (5.5%) cases of Tuberculosis, 4 (5.5%) of
Ischaemic Heart Disease, and 6 (8.3%) cases of diabetic complications. The operative
procedures in the general surgery domain and the general medical conditions were
reflective of baseline conditions requiring attention as a result of the destroyed health
care system.
DRESSING29 (5%)
OR EXTERNAL FIXATION5 (1%)
MEDICATIONS71 (13%)
SKIN GRAFTING55 (10%)
AMPUTATION38 (7%)
SUTURING12 (2%)
CONSERVATIVE16 (3%)
INTERCOSTAL DRAINAGE
3 (1%)
OPEN REDUCTION12 (2%)
INCISION AND DRAINAGE 18 (3%)
EXPLORATORY LAPRATOMY
24 (4%)
CLEANING AND DEBRIDEMENT
87 (15%)
POP CAST100 (17%)
OR INTERNAL FIXATION 94 (17%)
N= 575

Revati Phalkey Page 15 Draft document_12/1/2009
Table 1: General Medical conditions treated at the hospital during 10-weekperiodGeneral medical conditionsCondition Frequency Condition FrequencyAbdominal pain 1 (1.3%) Hernia 10 (13.8%)Adenoma 2 (2.7%) Hydrocoele 2 (2.7%)Appendicitis 3(4.1%) C a r d i o V a s c u l a r
Disease4 (5.5%)
Acute Renal Failure (Diabetic) 1(1.3%) Infection 2 (2.7%)Burst Abdomen 1(1.3%) Lipoma 2 (2.7%)Carcinoma 1(1.3%) Low Back Pain 1 (1.3%)COPD 9(12.5%) Muscular pain 5 (6.9%)CTEV 2(2.7%) Neoplastic Growth 1 (1.3%)Cyst 1(1.3%) Rheumatoid Arthritis 1 (1.3%)Diabetes 6(8.3%) Syndactaly 1 (1.3%)Diarrhea 2(2.7%) Tuberculosis 4 (5.5%)Fever 3(4.1%) Torticollis 1 (1.3%)Fistula 1(1.3%) Urethral Stricture 2 (2.7%)Hemi-paresis 2(2.7%) Vaginal Tear 1 (1.3%)Total 72
A total of 78 of the 575 patients (13.5%) reported infected wounds at the time of
admission. A look at corresponding dates of admission revealed 41 (52.5%) cases in
the first week. Day three (29.01.2001) following the earthquake recorded the highest
number of admissions with infected wounds at 13 (16.6%). The distribution of wound
infections was substantially low for a disaster situation. The cases were uniformly
distributed over the 10-week period despite the increase in the number of admissions
in week 4, 7 and 8 respectively.

Revati Phalkey Page 16 Draft document_12/1/2009
Figure 8: Reported wound infection including those at the time of admission ona weekly basis.
Analysis of patient outcome
A large majority of the patients (42%) underwent operative procedures. The
definitive outcomes are as described in Figure 9. The cause of death in these patients
was not ascertained as the case reports were sent to the coroners. The date of death
was known for three of the four patients and was 30.01.2001 (45 yrs, female, crush
injury), 01.02.2001(22 yrs, male) and 08.02.2001(70 yrs, female) respectively. The
fourth patient was 17-year-old male. A total of 102 patients were transferred for
tertiary care. Seventy-eight patients were transferred in the descending order of
frequency to Mandvi, Mumbai, Bhojay, Ahmedabad, Anand and Jamnagar cities.
Details for the destination of transfer for 24 cases (23%) was not available.
173
64
16
30 28
17
31 31
61
41
16
4 6 3 3 1 3 1 00
20
40
60
80
100
120
140
160
180
200
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8 Week 9 Week 10
Weeks
Freq
uen
cy
Number ofAdmissonsInfection
DOA known= 397 Infections reported= 78

Revati Phalkey Page 17 Draft document_12/1/2009
Figure 9: Definitive outcomes in the patient treatment.
Discussion
We report orthopaedic injuries particularly extremity fractures (78.0%) of the lower
limbs (tibia-fibula, femur, radius-ulna and humerus in this order of frequency) as the
most common injuries. Head, spine, and chest injuries were low at 2% each
respectively. The findings of the study are in accordance with the 29 published
studies reporting earthquake injury data (1976-2007) accessible for review.
We report the predominance of young males (25- 45 yrs) compared to other studies
from Gujarat. This anomaly is difficult to explain sufficiently. However, two of the
four studies from Gujarat reported more female patients than males, 1 study did not
mention this information and one found no gender difference. Similar inconsistencies
are reported in other studies that report gender as a vulnerability factor for injuries
EXPIRED4 (1%)
TRANSFERRED78 (14%)
ABSCONDED1 (0%) CONSERVATIVE
94 (16%)
CLOSED REDUCTION22 (4%)
OPERATIVE244 (42%)
DISCHARGED 132 (23%)
N= 575

Revati Phalkey Page 18 Draft document_12/1/2009
which was not statistically correlated. Nearly half (15, 51.7%) of the 29 studies we
reviewed did not report gender differences in the patients. The number of female
patients was higher than the males in 5 and lower in 4 of the 29 studies. These data
were not mentioned in 6 of the studies. Independent age and gender associated risk
factors may explain increased injuries in females or children and elderly. (Shoaf et
al., 1998, Peek-Asa et al., 2003) A further investigation about the social structure and
gender equation of the society and its influence in health seeking behavior alongside a
thorough statistical analysis of injury data may provide useful information in
resolving these anomalies.
The mechanism of injury may explain some of the vulnerabilities. Our study could
not record the mechanism of injury due to absent data. This is a major drawback and
further research is required for formulating building codes and infrastructure
construction. Limited studies (17, 58.6%) correlate the cause and mechanisms of
injury to the nature of injury sustained. The most common causes of injury were
identified as ‘being trapped’ by 6, ‘falls’ by 3, and ‘being hit by falling debris or
objects’ by 6 of the 29 studies. (add references) Only one of the study investigated
human and environmental factors for causing injuries (Peek-Asa, 2003). However,
none of the studies provide concrete statistical evidence to assist in identifying
vulnerabilities. Three studies of the four from Gujarat attributed ‘being trapped’ and
‘falling debris’ as the main cause of injury. (reference)

Revati Phalkey Page 19 Draft document_12/1/2009
The time of strike is associated with the vulnerability to injuries principally due to
level of alertness and body position at strike (C. de Ville De Goyet 1976). However,
even though the time of strike in 14 of the 29 (48.2%) studies was between midnight
and 06.00 am the nature of injuries reported were largely similar to the 9 other studies
reporting earthquakes occurring in later part of the day. Six studies did not report the
time of the earthquake in the publications. The Gujarat earthquake occurred at 08.46
am and the injury epidemiology we report is in general agreement with most studies.
A thorough investigation is required to identify vulnerability associated with the time
of strike and the nature of injury sustained.
The nature and seriousness of injuries sustained along with other vulnerabilities
determine mortality rate. A study of injury patterns amongst survivors only, needs to
be approached with great caution since most primary mortality (impact deaths) is
caused by serious injuries (Guha-Sapir, 1993). Given that earthquakes cause high
number of impact deaths/ primary mortality a study of the actual cause of death in
those found dead at rescue could yield substantial information about the serious
injuries sustained after an earthquake. Although the autopsies were not completed in
the Northridge earthquake, common injuries seen in those dead were head (48.5%),
thoracic (42.4%) followed by abdominal and lower extremity injuries (Peek-Asa et
al., 1998). However, autopsies are a rare possibility in the emergency phase
particularly in developing countries given that mass management of dead bodies is a
challenge in itself. Besides the emotional aspects and the logistical capacities
involved in conducting autopsies are resource consuming. (reference)

Revati Phalkey Page 20 Draft document_12/1/2009
The number of non fatal serious injuries like chest and head injuries were limited to a
mere 2% in our study and only 2 abdominal burst injuries were reported. Other
important serious injuries of specific concern following earthquakes are Crush
Injuries and Crush Syndrome. Crush Injury (CI) occurs when a body part is subjected
to a high degree of force or pressure that leads to bleeding, bruising, increased
pressure in the compartment, fracture and lacerations (Medline Plus, NS-a). Thirty-
one (5.39%) cases of crush injuries were observed in our study. Children are more
prone to crush syndrome following crush injuries and also develop acute renal failure
at a higher rate. Since they are more difficult to diagnose both clinically and
diagnostically close monitoring of children is solicited to detect early signs (Iskit et
al., 2001). However, the age distribution for crush injuries was uniform in our study
with no significant increase in the pediatric or geriatric age group. The other aspect
with crush injuries is the secondary complications with infection, gangrene, and
amputation of the affected limb(s).i Crush injuries of the foot were more common in
our study and correspondingly 14 below ankle amputation (36%) were reported.
“Crush syndrome (CS) is the systemic manifestation of Rhabdomyolysis caused by
prolonged continuous pressure on muscle tissue. It is characterized by hypovolaemic
shock, hyperkalemia, acute renal failure and muscle necrosis (Dönmez et al., 2001).
Crush Syndrome is more common in concrete multi-story building collapse as seen in
the earthquakes in Japan and Armenia. In the study of morbidity after the Hanshin-
Awaji Earthquake of 1995, 262 cases of crush syndrome (of which 202 developed

Revati Phalkey Page 21 Draft document_12/1/2009
acute renal failure requiring dialysis) were reported. The Armenian earthquake of
1988 reported 385 cases of Crush syndrome (Tanaka et al., 1999). Far lower numbers
were reported in Nicaragua, Guatemala and Iran due to the mud and adobe
construction and due to poor rescue operations. Reference Secondary deaths due to
crush syndrome are associated with lack of dialysis infrastructure to cope with the
mass casualties (Vanholder et al., 2007). This problem is however pertinent only
when the search and rescue level is effective enough to retrieve these patients alive in
large numbers, which was not the case in the Gujarat earthquake (Roy et al., 2002).
Less than two percent cases of crush syndrome were reported in Gujarat (Cooper,
2006). No cases of crush syndrome were recorded in our study. One case of diabetes
related Acute Renal Failure (ARF) was reported. This could be first due to the poor
rescue time after the Gujarat earthquake, second that CS is related to the building
design and most of the region affected was predominantly rural with mixed
construction designs and third that often first responders, rescue workers, paramedics,
and even untrained nephrologists are unfamiliar with recognizing early symptoms
(Dhar et al., 2007).
Secondary deaths (deaths after rescue) are relatively low following earthquakes and
have been associated with the efficiency of the search and rescue performance (De
Bruycker et al., 1983). If a greater number of serious injuries are rescued alive, then
the secondary mortality may rise proportionately and was seen where the total
percentage of head, abdominal and thoracic injuries constituted less than 7.5% of the
total injured but the secondary mortality in this group was the highest (Tanaka et al.,

Revati Phalkey Page 22 Draft document_12/1/2009
1999). Our study reported four secondary deaths. The cause of death could not be
ascertained due to missing files and so the actual diagnosis and the clinical condition
for these patients remained unknown. The low mortality in our study can be
explained by the low number of serious injuries treated and the transfer of more
serious cases for tertiary care to Mumbai and Ahmedabad (102 transfers reported in
our study, see Figure 9).
Moderate and serious injuries requiring admission are better reported than minor soft
tissue injuries that are often treated at site or on an outpatient basis. Soft tissue
injuries are wounds which may be torn (lacerations), injury without laceration
(contusion), an injury transmitted through unbroken skin to underlying tissue, causing
rupture of small blood vessels and escape of blood into the tissue with resulting
discoloration (bruise) or a combination of these (Medline Plus, NA-b). These can be
effectively managed on site by simple first aid techniques to prevent unnecessary
overcrowding and overburdening of hospitals and to allow effective use of available
scarce resources. This leads to unintentional selective exclusion of minor injuries
being reported. This is critical given that most earthquake injuries are soft tissue
injuries resulting from falling objects or debris. (reference)
We reported single hospital inpatient data a criticism we raise for the Fifteen (51.7%)
of the 29 studies other studies that reported analysis of inpatient data and 19 (65.5%)
of them reporting single hospital data. However, we report 119 (20%) of the 575
cases with soft tissue injuries in our study. 15% of the fractures sustained were

Revati Phalkey Page 23 Draft document_12/1/2009
compound injuries -open wounds with fractures. Proportionately, 15% of the surgical
operation theatre procedures were of cleaning and debridement of contaminated
wounds (see Figure 7). The reasons for high number of admissions for minor soft
tissue injuries at our hospital were, first the individual delay in seeking health care
that led to complications, second the long commuting distances which made travel for
most patients both logistically and monetarily less feasible for daily dressings and
third, more relevant that Bidada has a long-standing history of charity. People with
lost homes preferred to stay in the hospital tents where free food and accommodation
was provided free of cost for accompanying family members as well.
Soft tissue injuries are more prone to primary and secondary infections. Most injuries
after earthquakes were either contaminated and or infected due to delay in arrival to
health care. The potential of tetanus with open contaminated wounds particularly in
disasters is a concern (Waring and Brown, 2005). However, none of the 29 studies
reviewed mentioned risks of tetanus. Furthermore, limited information is available
about the hospital-acquired secondary infections after disasters particularly despite
that adequate hygiene in mass casualty situations is problematic (Öncul et al., 2002).
In Gujarat, generally low rates of secondary post-operative infections were reported.
Partly due to the high sensitivity of the rural population to antibiotics that were
largely unused in these areas (Roy et al., 2005). This finding was similar in our study.
Over the 10 weeks, the infection rates remained low probably also indicating
appropriate postoperative care. Most crush injuries in our study were managed

Revati Phalkey Page 24 Draft document_12/1/2009
conservatively. However cases with gangrene (death of tissue due to inadequate
blood supply and superadded infections) required elective amputation (surgical
removal or loss of a body part). Amputations of the foot, below the ankle were
reported in 36% cases and Below Knee (BK) in 25% cases in our study. This is
explained by the common injuries sustained.
Amputations and traumatic paraplegia (paralysis of both lower limbs usually a result
of spinal fractures involving damage to the spinal nerves) are the most common
secondary outcomes after earthquake injuries. As per Government records over 268
amputees, about 500 spinal cord injuries which recovered completely and 104 cases
of complete spinal paraplegia were reported in Gujarat. There were several deaths in
the last seven years amongst the paraplegics and currently as per the Government
pension scheme records a total of 94 paraplegics were receiving stipend from the
pension scheme. We report 2 cases of spinal cord injury patients who later developed
paraplegia. Peripheral Nerve Injuries (PNI) leading to distal paralysis accounts for
significant disability. Nerve injuries reported in our study included Brachial Plexus
Injury (3), Radial nerve (2) and Radio-Ulnar nerve (1) respectively. Brachial Plexus
Injuries result mainly from traction injuries to the Axilla commonly seen during
rescue activities, when holding the arms one pulls up the body weight.
Physical disability is an enormous psychological and financial burden on the
population in terms of resources. Activities of daily living and more importantly,
income generation are greatly affected besides contributing to future vulnerabilities.

Revati Phalkey Page 25 Draft document_12/1/2009
A study in Japan showed that individuals with physical disabilities were 5.6 times
more vulnerable to earthquake impacts (Osaki and Minowa, 2001). However,
disabilities both partial and permanent are often neglected after earthquakes.ii Since
orthopaedic trauma constitute the bulk of the injuries after earthquakes, non-union
and mal-union are a concern.
In post disaster conditions, physical disabilities often result from unintentional
negligence, inadequate or mismanaged injuries due to lack of infrastructure
availability at a mass scale. A study conducted two years after the Gujarat earthquake
reported 10% of the injuries (mainly spinal in multiple injury and double fractures)
were missed during diagnosis and over 30.5% patients underwent re-surgeries, 23%
had non-union and 12% experienced joint range of motion (ROM) restriction.
Another hospital experienced a 100% surgery failure rate in the 30 spinal cord injury
patients operated reasons for which are beyond the current scope. Reassessment and
review of all patients before discharge is necessary to detect missed injuries and more
importantly training in mass casualty management for surgeons and medical staff
should be mandatory (Emami et al., 2005).
In Gujarat, aggressive orthopedics especially with respect to implant operations was
observed along with serious compromises in implant type (Roy et al., 2005).
Symbolically, 76 of the 575 cases in our study (13%) were open compound fractures.
Ideally, external fixators are mandated in open contaminated fractures. However, The
number of external fixations in our study were 5 (1%) and in contrast internal

Revati Phalkey Page 26 Draft document_12/1/2009
fixations were comparatively high at 94 (17%). A common problem faced by the
Bidada hospital was lack of continuous competent manpower. Postoperative
management was occasionally compromised due to the short-term commitments
offered by these volunteers. The surgeons often operated and left within a week or
visited in rotations. Often the coordination amongst the therapeutic plans of one
surgeon and the next one was difficult.
Inadequate fixation materials besides inexperienced surgeons (mainly registrars from
city teaching hospitals with short time commitments in Gujarat) may have
compromised treatment resulting in high number of re-surgeries. This explains the
presence of surgical cases at Bidada hospital; long after the initial phase was over. In
parts of Gujarat, external devices (new to local specialists) were used which were
initially effective. However, led to Osteomyelities (death of bone and muscle tissue
due to infections), due to delayed removal (Jain et al., 2003). The competence of local
orthopedic surgeons is critical when deciding complex therapies that achieve near
similar results to standard local practices. However, it may be incorrect to judge the
surgical decisions in disaster situations retrospectively. Especially in view of the
availability of fixation instruments at a specific time and the need for clinical
accuracy.
The preparedness and functional surge capacity of the health care system is crucial
and determines local response capacity. The ability to cope with the transient excess
need alongside baseline function is demanding. Time is an important factor as health

Revati Phalkey Page 27 Draft document_12/1/2009
care needs are dynamic in nature and evolve (Figure 10). Most often the baseline
diseases and routine chronic conditions present at health care facilities throughout all
the emergency phases. The most common complaint not directly related to the
earthquake impact in our study was Chronic Obstructive Pulmonary Disease (COPD).
42% of the 72 patients with non-earthquake related health issues were operated for
Hernia and 13% for acute appendicitis. Besides these, Tuberculosis (TB), Diabetes
and Cardio Vascular cases.
0-3 days 3-10 days 10-14 days
EARTHQUAKE TIME
Irrespective of time after the earthquake
Figure 10: Dynamics of health needs following earthquakes.
Strengthening reporting of morbidity following earthquakes is therefore crucial to
improve preparedness. Injury epidemiology is especially critical to reduce impact and
to prevent mismanagement of injuries leading to disabilities. Although most studies
Follow-up careand surgicalcomplications
Return tobaselinefunction
Routine emergency cases including Accidents, Obstetrics andPediatric emergencies, acute exacerbations of routineconditions
Immediate medical care,maximal need Orthopedictrauma and soft tissueinjuries

Revati Phalkey Page 28 Draft document_12/1/2009
including ours have small sample size (11 to 3619 cases) compared to actual numbers
of injured in the earthquakes, they contribute to current understanding of the field.
Methodological issues identified with recording and reporting patient data
Some of the methodological issues identified with reporting and recording patient
information are one, that majority of the studies (19, 65.5%) report single hospital
data. Drawing generalizations based on single hospital data may leave some aspects
un-addressed. Although, it is reassuring that the pattern of injuries we observed is
representative in general of earthquake injuries, large multi hospital studies should be
initiated to arrive at adequate statistical evidence base for policy decisions.
Two, studies reflect the findings in the individuals who actively seek medical care,
largely excluding those were unable to reach the facility. The proportion of cases
actively seeking medical care is greatly influenced by factors such as population
density, the time of strike, successful rescue, survival of the injured, availability of
transport facilities, distance to the nearest functional health facility and most
importantly availability of an intact operational health care facility with access. In a
rural setting especially as in Kutch, there is a strong possibility that access could have
been a challenge.

Revati Phalkey Page 29 Draft document_12/1/2009
Three, often it is unclear if the studies reviewed the injuries in each patient or the total
number of injuries sustained. This is relevant as multiple injuries in single patients are
common.
Four, the correlation between mechanism of injury and injury severity and the
relationship between nature of severity and patient outcome is not sufficiently
reported.
Five, the sources of bias in recording injury data are high and more varied than those
known to affect normal medical records since wide variety of professionals from
different training schools complete patient reports in disasters (Sanchez-Carriallo,
1989).
Six, emerging concern about the close interactions between psychological symptoms
and physical manifestations is inadequately addressed. Seven of the 29 (24.1%)
studies reported the importance of considering it. Four studies reported the recorded
incidence in patients. One of four studies on Gujarat mentions psychological trauma.
Professional management of psychological stress is necessary to mitigate long-term
effects. Our study did not ascertain this aspect due to data in-availability.
Seven, disaster data has inherent “incomplete” nature. Table 2 represents the
percentage of missing data on variables in our study dataset. Further assessment is
mandated to detect under or over reporting of injury data.

Revati Phalkey Page 30 Draft document_12/1/2009
Table 2: Missing data by dataset variable (N=1248)
Variable Dataavailable
Percentagemissing
Analysis of Injury Epidemiology 575/1248 53.9%Geographical origin 1148/1248 8.0%Date of Admission 397/1248 68.1%Date of Discharge 420/1248 66.3%Sex 1172/1248 6.0%Age 1157/1248 7.2%Anatomical site of Injury 575/1248 53.9%Anatomical side of Injury 441/575 23.3%Mortality cause 0/4 100%Outcome in transferred patients 78/102 23.5%Level of Amputation 35/38 7.8%
Eight, health outcome in the patients is insufficiently addressed. About half (51.7%)
of the studies discussed patient outcome and none discussed disability as an outcome
in treated patients. In our study data of those transferred to tertiary care after initial
care was not recorded. A total of 102 patients were transferred and the location of
transfer was missing in 24 patients. The case papers were missing and so the reason,
date and treatment imparted before transfer could not be assessed. This calls for
ensuring that a double copy of inpatient and outpatient records is maintained to
improve hospital records for future retrospective studies.
Nine, follow up time in the studies is inconsistent. Pre-morbid and chronic diseases in
patients with earthquake injuries is under reported.

Revati Phalkey Page 31 Draft document_12/1/2009
Current challenges
There are general discrepancies in definitions, classification, and reporting of disaster
data internationally (Tschoegl et al., 2006). In the wake of increase in the frequency
of natural disasters and their human impacts a consensus is urgent on these
fundamental issues especially for earthquake morbidity data. International databases
report number of injuries collectively. None of them reported injury epidemiology.
Although a large number of scattered databases exist, currently no national disaster
database is active in India. As per Emergency Events Database (EM-DAT) at Center
for Research on the Epidemiology of Disasters (CRED), Brussels, the pilot project
“Indis Data” was launched in 2002 and expanded to 4 other states in 2005. However,
to date no standard guidelines exist for effective injury database management. Most
of the published studies report haphazard, patchy, inadequate, selective data and none
report disability burden resulting from injuries sustained from earthquakes. There is
no agreement on standardized methodology to assess or report the injuries. This
makes comparability of data across earthquakes within the country as well as
internationally difficult.
Evidence based response programmes need statistically significant data. Given the
challenges of non-standardized data reported from the past earthquakes in India as
well as internationally, the authors proposes a simple Patient Case Reporting Form
for earthquake injury data reporting in the early phases of the earthquakes.
Information provided in the basic form may assist in acquiring an overview of the
types, nature, mechanism and frequency of injuries sustained. A registry may be

Revati Phalkey Page 32 Draft document_12/1/2009
maintained for the outpatient departments recording the same information. A state or
national level database should be maintained and regularly updated. Efforts in this
direction are underway in India with the National Disasters Management Authority,
Delhi. Incidentally, not all studies reporting injury data were publicly accessible.
Conclusion
Although substantial data on epidemiology of injuries following earthquakes
currently exists, drawing consolidated statistical conclusions is difficult due to non
standardized methodologies and approaches. Coordinated standardization of
recording and reporting earthquake injury data is therefore a pressing need to help
guide preparedness and emergency response programmes globally.

Revati Phalkey Page 33 Draft document_12/1/2009
Annex I Variables mentioned in the studiesVariable Number of
studiesreporting
Variable asmostfrequentinjury
Rangeamongstthoseenrolled
4 GujaratEarthquakeStudiesfindings
BidadaHospital studyN=575
PsychologicalTrauma
7 0-32% 1 study Not assessed
Orthopaedicinjuries
8 2 (both inGujarat)
15-45% 42-45% 83.3%
General Surgery 2 6-13% Not reported 4.1%Medicine 6 1 30-79% 29.2% 12.5%Gynaecology 5 5-22 5-22% 0%Paediatric Cases 2 1 23-37% 22.2% 25.1%CardiovascularDisease
3 3-16% 15.7% 5.5%
Fractures 5 1 20-55% 38.7% 50.9%Crush Syndrome 6 1-26% 0-2% 0%Crush Injury 5 5-46% Low incidence 5.3%Acute Rena lFailure
6 2-69% 0% 0.1%
ExtremityInjuries
9 6 19-55% 50.4% 46%
Upper Extremity 10 Humerus 10-30% 11-13% 18.4% (RU)Lower ExtremityInjuries
10 7, Femur 30-54%, 1study 4%, 1study 7%
53-56% 78.0%(TF)
Clavicle 7 0 - 1 % , 1study 11%
Not reported 2%
Spinal 11 4-16% 8-17% 4%Pelvis 6 3-13% 11% 7%Trunk 2 1 6-55% 4%Head 12 0-30% 7% 2%Chest 7 3-19% 2% 2%Abdominal 9 0-15% 2% 0% (2)Burns 5 2-16% 10% 0%CompoundInjuries
2 4-6% Not reported 15%
Multiple Injuries 7 3-50% 43% 23%Infections 6 5-47% 8-19% 13.5%S o f t T i s s u eInjuries
16 6 10-83% 10-42% 20%
Peripheral NerveInjuries
6 1-9% 0 1%
Deaths 8 2-23% 1% 0.6%Amputations 7 1-20% 2-12% 6.6%Transfers 5 0-25% 7% 14%Others 9 3-77% 6% NoneUnknown 1 10% Not reported See Table ?

Revati Phalkey Page 34 Draft document_12/1/2009
Annex II: Details of published papers reviewedFirst Author, Year Location Date Time Intensity
de Ville de Goyet, C 1976 Guatemala February 4, 1976 03.02 7.2
De Bruycker, M 1985 Southern Italy November 23, 1980 19.34 NM
Sanchez-Carriallo, C 1989 Mexico City September 19-20, 1985 Not Mentioned 8.1, 6.5
Sapir, DG, 1992 Yunnan Province, China November 6, 1988 21.03, 21.06 7.6, 7.2
Yoshimura, N 1996 Southern Hyogo, Japan, January 17, 1995 05.46 7.2
Tanaka, H 1997 Hanshin Awaji, Japan January 17, 1995 05.46 7.2
Armenian, H 1997 Armenia December 7, 1998 11.41 6.9
Shoaf, K 1998 Whittier Narrow, USA October 1987 Not Mentioned 5.9
Shoaf, K 1998 Loma Preita, USA October 1989 Not Mentioned 7.1
Shoaf, K 1998 Northridge, USA January 17, 1994 04.31 6.7
Peek –Asa, C 1998 Northridge, USA January 17, 1994 04.31 6.7
Mahue-Giangreco, M 2001 Northridge, USA January 17, 1994 04.31 6.7
Yi-Szu, W 2000 Chi Chi Taiwan September 21, 1999 01.47 7.3
Bar-Dayan, Y 2000 Marmara, Turkey August 17, 1999 03.04 7.4
Dönmez, O 2001 Marmara, Turkey August 17, 1999 01.37 7.4
Iskit, S 2001 Marmara, Turkey August 17, 1999 03.02 7.4
Öncül, O 2002 Marmara, Turkey August 17, 1999 03.02 7.4
Sarisözen, B 2003 Marmara, Turkey August 17, 1999 03.01 7.4
Bar-Dayan, Y 2005 Marmara, Turkey November 12, 1999 22.00 7.2
Roschin, G 2002 Kutch, Gujarat, India January 26, 2001 08.46 6.9
Jain, V 2003 Kutch, Gujarat, India January 26, 2001 08.46 6.9
Roy, N 2003 Kutch, Gujarat, India January 26, 2001 08.53 6.9
Roy, N 2005 Kutch, Gujarat, India January 26, 2001 08.46 6.9
Woersching, J.C 2003 El Salvador January -February 2001 Not Mentioned Not Mentioned
Emami, MJ 2005 Bam, Iran December 26, 2003 05.26 6.5
Naghi, TM 2005 Bam, Iran December 26, 2003 05.30 6.8
Dhar, S 2006 Kashmir, Pakistan October 8, 2005 09.20 IST* 7.6
Vanholder, R 2007 Kashmir, Pakistan October 8, 2005 08.50 PST** 7.6
Bozkurt, M 2007 Kashmir, Pakistan October 8, 2005 Not Mentioned 7.6
* Indian Standard Time, ** Pakistan Standard Time

Revati Phalkey Page 35 Draft document_12/1/2009
References:
Armenian, H. K., A. Melkonian, et al. (1997) ‘Deaths and injuries due to theearthquake in Armenia: a cohort approach’. International Journal of Epidemiology.26(4). pp. 806-813.
Bar-Dayan, Y., D. Mankuta, et al. (2000) ‘An earthquake disaster in Turkey: Anoverview of the experiences of the Israeli defence forces field hospital in Adapazari’Disasters. 24(3). pp. 262-270.
Bar-Dayan, Y., A. Leiba, et al. (2005) ‘A multidisciplinary field hospital as asubstitute for medical hospital care in the aftermath of an earthquake: The experienceof the Israeli defense forces field hospital in Duzce, Turkey, 1999’. Prehospital andDisaster Medicine. 20(2). pp. 103-106.
Bendick, R., R. Bilham, S. E. Fielding, V. Gaur, S. E. Hough, G. Kier, M. N.Kulkarni, K. Martin, K. Mueller and M. Mukul, (2001) ‘The January 26, 2001 Bhujearthquake, India’. Seismological Research Letters. 72. pp. 328-335.
Bremer, R. (2003) ‘Policy development in disaster preparedness and management:Lessons learned from the January 2001 earthquake in Gujarat, India’. Prehospital andDisaster Medicine. 18. pp. 370-382.
Bozkurt, M., A. Ocguder et al. (2007) ‘The evaluation of trauma patients in TurkishRed Crescent field hospital following the Pakistan earthquake in 2005’ Injury. 38. pp.290-297.
Chou, Y.-J., N. Huang, C.-H. Lee, S.-L. Tsai, L.-S. Chen and H.-J. Chang (2004)‘Who is at risk of death in an earthquake’. American Journal of Epidemiology. 160.pp. 688-695.
Cooper, D. (2006) Mass casualty management in disasters. Health Action in Crisis,World Health Organization, Geneva.
CRED (2006) Earthquake disasters, CRED Crunch, University Catholic Louvain,Brussels.
De Bruycker, M., D. Greco, I. Annino, M. A. Stazi, N. D. Ruggiero, M. Triassi, Y. P.De Kettenis and M. F. Lechat (1983) ‘The 1980 earthquake in Southern Italy: Rescueof trapped victims and mortality’. Bulletin of the World Health Organization. 61. pp.1021-1025.
De Bruycker, M., D. Greco, and M. F. Lechat (1985) ‘The 1980 earthquake inSouthern Italy morbidity and mortality’. International Journal of Epidemiology. 14.pp. 113-117.

Revati Phalkey Page 36 Draft document_12/1/2009
De Ville de Goyet, C., E. del Cid et al. (1976) ‘Earthquake in Guatemala:Epidemiologic evaluation of the relief effort’. Bulletin of the Pan AmericanOrganization. X(2). pp. 95-109.
Dhar, S. A., M. A. P. Halwai, M. M. Ramzan, M. R. Wani, M. F. Butt, M. I. Bhat andA. Hamid (2007) ‘The Kashmir earthquake experience’. European Journal of Trauma.33. pp. 74-80.
Dönmez, O., A. Meral, M.Yavuz and O.Durmaz (2001) ‘Crush syndrome of childrenin the Marmara earthquake, Turkey’. Pediatrics International. 43. pp. 678-682.
Emami, M., A. R. Tavakoli, et al. (2005) ‘Strategies in evaluation and management ofBam earthquake victims’. Prehospital and Disaster Medicine. 20(5). pp. 327-330.
Emami, M., A. R. Tavakoli, H. Alemzedeh, F. Abdinejad, G. Shahcheraghi, M.Erfani, K. Mozafarian, S. Solooki, S. Rezazadeh, A. Ensafdaran, H. Nouraie, F. M.Jaberi and M. Sharifian (2005) ‘Strategies in evaluation and management of Bamearthquake victims’. Prehospital and Disaster Medicine. 20. pp. 327-330.
GOG (2007a) Gujarat- Official portal of the Gujarat Government.
GOG (2007b) Statistics. Available at http://gujhealth.gov.in. Accessed on October 28,2007.
Guha-Sapir, D. (1986) ‘Reducing the impact of natural disasters: Why aren't webetter prepared’. Health Policy and Planning. 1. pp. 118-126.
Guha-Sapir, D., and V. C. Panaccione (1992) ‘Health sector implications of the 1988Earthquake in Yunnan Province, China’. Disasters. 16(2). pp. 145-151.
Guha-Sapir, D. (1993) ‘Health effects of earthquakes and volcanoes: Epidemiologicaland policy issues’. Disasters. 17. pp. 251-262.
IFRC (2006) World disasters report: Focus on neglected crisis. InternationalFederation of the Red Cross and the Red Crescent Societies, Geneva.
IMD (NA) Seismology. http://www.imd.gov.in. Accessed on September 19, 2007.
Iskit, S. H., H. Alpay, H. Tugtepe, C. Özdermir, S. H. Ayyildiz, K. Özel, M.Bayramicli, C. Tetik and T. E. Dagli (2001) ‘Analysis of 33 pediatric trauma victimsin the 1999 Marmara, Turkey earthquake’. Journal of Pediatric Surgery. 36. pp. 368-372.

Revati Phalkey Page 37 Draft document_12/1/2009
Jain, V., R. Noponen and B. M. Smith (2003) ‘Pediatric surgical emergencies in thesetting of a natural disaster: Experiences from the 2001 earthquake in Gujarat, India’.Journal of Pediatric Surgery. 38. pp. 663-667.
Lechat, M. F. (1979) ‘Disasters and Public Health’. Bulletin of the World HealthOrganization. 57(1). pp. 11-17.
Lechat, M. F. (1989) ‘Corporal damage as related to building structure and design:The need for an international survey.’ Paper presented at international workshop onearthquake injury epidemiology for mitigation and response, Johns HopkinsUniversity.
Mahue-Giangreco, M., M. Mack, et al. (2001) ‘Risk factors associated with moderateand serious injuries attributable to the 1994 Northridge Earthquake, Los Angeles,California’. Annals of Epidemiology. 11(5). pp. 347-357.
Medline Plus (NA-a) Medical Dictionary.http://www.nlm.nih.gov/medlineplus/mplusdictionary.html, Accessed on October 27,2007.
Medline Plus (NA-b) Medical Encyclopedia.http://www.nlm.nih.gov/medlineplus/ency/article/000024.htm, Accessed on October22, 2007.
Öncul, O., O. Keskin, H. V. Acar, Y. Kücükardali, R. Evrenkaya, E. M. Atasoyu, C.Top, S. Nalbant, S. Özkan, G. Emekdas, S. Cavuslu, M. H. Us, A. Pahsa and M.Gökben (2002) ‘Hospital-acquired infections following the 1999 Marmaraearthquake’. Journal of Hospital Infections. 51. pp. 47-51.
Osaki, Y. and M. Minowa, (2001) ‘Factors associated with earthquake deaths in thegreat Hanshin-Awaji earthquake, 1995’. American Journal of Epidemiology. 153. pp.153-156.
Peek-Asa, C., J. F. Kraus, L. B. Bourque, D. Vimalachandra, J. Yu and J. Abrams(1998) ‘Fatal and hospitalized injuries resulting from the 1994 Northridgeearthquake’. International Journal of Epidemiology. 27. pp. 459-465.
Peek-Asa, C., M. Ramirez, H. Seligson and K. Shoaf (2003) ‘Seismic, structural, andindividual factors associated with earthquake related injury’. Injury Prevention. 9. pp.62-66.
Roshchin, G. G., and O. V. Mazurenko (2002) ‘Ukranian’s disaster medicine teammission to India following the earthquake of 2001’. Prehospital and DisasterMedicine. 17(3). pp. 163- 166.

Revati Phalkey Page 38 Draft document_12/1/2009
Roy, N., H. Shah, V. Patel and H. Bagalkote (2005) ‘Surgical and psychologicaloutcomes in the rural injured- A follow-up study of the 2001 earthquake victims’.Injury. 36. pp. 927-934.
Roy, N., H. Shah, V. Patel and R. R. Coughlin (2002) ‘The Gujarat earthquake (2001)experience in a seismically unprepared area: Community hospital medical response’.Prehospital and Disaster Medicine. 17. pp. 186-195.
Sanchez-Carriallo, C. (1989) ‘Morbidity following Mexico city’s 1985 earthquakes:Clinical and epidemiologic findings from hospitals and emergency units’. PublicHealth Reports. 104(5). pp. 482-488.
Sarisözen, B. and K. Durak (2003) ‘Extremity injuries in children resulting from the1999 Marmara earthquake: An epidemiologic study’. Journal of Pediatric Surgery.12(4). 288-291.
Sharma, R. (2001) ‘India plans massive hospital rebuilding after earthquake’. BritishMedical Journal. 322. pp. 451.
Shoaf, K. I., L. H. Nguyen, H. Sareen and L. B. Bourque (1998) ‘Injuries as a resultof California earthquakes in the past decade’. Disasters. 22. pp. 218-235.
Tahmasebi, M. N., K. Kiani, et al. (2005) ‘Musculoskeletal injuries associated withearthquake. A report of injuries of Iran’s December 26, 2003 Bam earthquakecasualties managed in tertiary referral centers’. Injury. 36. pp. 27-32.
Tanaka, H., J. Oda, A.Iwai, , Y. Kuwagata, T. Matsuoka, M. Takaoka, M. Kishi, F.Morimoto, K. Ishikawa, Y. Mizushima, Y. Nakata, H. Yamamura, A. Hiraide,T. Shimazu and T. Yoshioka (1999) ‘Morbidity and mortality of hospitalized patientsafter the 1995 Hanshin-Awaji earthquake’. American Journal of EmergencyMedicine. 17. pp. 186-191.
Tschoegl, L., R. Below and D. Guha-Sapir (2006) ‘An analytical review of selecteddata sets on natural disasters and impacts’. UNDP/CRED workshop on improvingcompilation of reliable data on disaster occurrence and impact. Bangkok, Thailand.
Vanholder, R., A. V. D. Tol, M. D. Smet, E. Hoste, M. Koc, A. Hussain, S. Khan andM. Sever (2007) ‘Earthquakes and crush syndrome casualties: Lessons learned fromthe Kashmir earthquake’. Kidney International. 71. pp. 17-23.
Vatsa, K. (2001) ‘The Bhuj earthquake disaster of Kutch, state of Gujarat, IndiaJanuary 26, 2001, A reconnaissance report- identification of priority issues’. WorldInstitute for Disaster Risk Management, March 14, 2001. pp.1.

Revati Phalkey Page 39 Draft document_12/1/2009
Waring, S. C. and B. J. Brown (2005) ‘The threat of communicable diseasesfollowing natural disasters: A public health response’. Disaster Management andResponse. 3. pp. 41-47.
Woersching, J. C., and A. Snyder (2003) ‘Earthquakes in El Salvador: A descriptivestudy of health concerns in a rural community and the clinical implications, Part I’.Disaster Management and Response. 1(4). pp. 105-109.
Yi-Szu, W., H. Chung-Ping, et al. (2000) ‘Chest injuries transferred to trauma centresafter the 1999 Taiwan earthquake’. American Journal of Emergency Medicine. 18(7).pp. 825-827.
Yoshimura, N., S. Nakayama, et al. (1996) ‘Profile of chest injuries arising from the1995 Sourthern Hyogo prefecture earthquake’. Chest. 110(3). pp. 759-761.
i This relates to the personal observation of the author during her work in Gujarat,after the earthquake.
ii This relates to the personal observation of the author during her work in Gujarat,after the earthquake.