Embed Size (px)
Citation preview

RAPID PUBLICATION
DELETION OF PTEN IN A PATIENT WITH BANNAYAN-RILEY-RUVALCABA SYNDROME SUGGESTS ALLELISMWITH COWDEN DISEASE
E.M. Arch1,2, B.K. Goodman5, R.A. Van Wesep4,6, D. Liaw7, K. Clarke1,3, R. Parsons7, V.A. McKusick1,3, M.T. Geraghty1,2.
Center for Medical Genetics1, Dept. of Pediatrics2, Dept. of Medicine3, Dept. of Pathology4, Kennedy Krieger Institute5, The
Johns Hopkins University School of Medicine, Baltimore, MD 21287-3914. Dept. of Pathology, Sinai Hospital of Baltimore6.
Dept. of Pathology, College of Physicians and Surgeons, Columbia University NY, NY7.
We report on an 18-month-old boy with an interstitialdeletion at 10q23.2-q24.1. This region includes thePTENgene, mutations of which have been reported to causeCowden disease. Our patient presented with manifestationsof Bannayan-Riley-Ruvalcaba (BRR) syndrome. The BRRsyndrome is a rare disorder which presents most commonlyin childhood. Cowden disease is a disease of adulthood andis inadequately described in children. Because of theconsiderable phenotypic overlap between the two disorders,and the cytogenetic and molecular findings in our patient, wesuggest that BRR syndrome and Cowden disease are allelic.Am. J. Med. Genet. 71:489–493, 1997.© 1997 Wiley-Liss, Inc.
KEY WORDS
Bannayan-Riley-Ruvalcaba syndrome; Bannayan-Zonanasyndrome; Ruvalcaba-Myhre syndrome; Riley-Smith syndrome;Cowden disease;PTEN; interstitial deletion; 10q23.2-q24.1;intestinal polyps.
INTRODUCTION
The Bannayan-Riley-Ruvalcaba (BRR) syndrome is anautosomal dominant trait comprised of macrocephaly withsubcutaneous and visceral lipomas and hemangiomas [Gorlin etal., 1990]. Bannayan [1971] and Zonana et al. [1976]independently described patients with macrocephaly andsubcutaneous and visceral lipomas and hemangiomas. TheRuvalcaba-Myhre syndrome consists of macrocephaly, intestinalpolyposis and pigmented spotting of the penis [Ruvalcaba et al.,
1980]. Riley and Smith [1960] had earlier noted a similaranomaly complex in association with pseudopapilledema.Evidence of overlap of all 3 syndromes was reported later andthe designation Bannayan-Riley-Ruvalcaba (BRR) syndromewas suggested for this condition [Gorlin et al., 1992]. Cowdendisease or multiple hamartoma syndrome is a rare autosomaldominant condition comprised of macrocephaly, mucocutaneouslesions, and hamartomatous neoplasms [Lloyd and Dennis, 1963;Mallory, 1995]. There is a strong association of this disorderwith cancers of the breast and thyroid, making it the subject ofmany recent investigations into the hereditary nature ofmalignancies.
The gene for Cowden disease was localized to 10q22-q23using linkage analysis in 12 families [Nelen et al., 1996].Recently a tumour suppressor gene,PTEN, was isolated andcharacterized from this region and mutations inPTEN werereported in patients with Cowden disease [Li et al., 1997; Liawet al., 1997]. We describe a patient with an interstitial deletionof 10q23.2-q24.1 in whom absence ofPTEN was confirmed byfluorescencein situ hybridization (FISH). His manifestationsoverlap both the BRR syndrome and Cowden disease. A similarphenotype was reported in members of 2 kindreds diagnosedwith BRR syndrome, who later developed skin lesionspathognomonic of Cowden disease and, in addition, had severalmalignancies uncommon in BRR syndrome [Fargnoli et al.,1996]. The phenotypic overlap between BRR syndrome andCowden disease, the clinical and molecular cytogenetic findingsin our patient and the recent genetic findings in Cowden diseasesuggest that both disorders are caused by loss of function of thePTENgene.
METHODS
Cytogenetics: Mitosis in lymphocytes was synchronized usingstandard methods [Yunis and Chandler, 1977]. Prometaphasechromosome spreads were G-banded using trypsin pretreatmentfollowed by Wright’s staining (GTW), and analyzed at aresolution of 650 bands per haploid set. G-banded cells wereanalyzed with a Zeiss Axioskop and the Cytovision computer-assisted karyotyping system (Applied Imaging, Santa Clara,
Address reprint requests to Michael T. Geraghty, MB, MRCPI,Assist. Prof. of Pediatrics, Center for Medical Genetics, Blalock1008, Johns Hopkins University School of Medicine, 600 N.Wolfe St., Baltimore, MD 21287-4922, USA, (410) 955-3071,(410) 955-7397 (FAX), e-mail,:[email protected] on 16 June 1997accepted on 2 July 1997Contract grant sponsor: KKI/Hopkins NICH Mental Retardation
Center Core Grant; Contract grant number: HD24061.
American Journal of Medical Genetics 71:489–493 (1997)
© 1997 Wiley-Liss, Inc.

CA). FISH was performed using the BAC clone 265N13, whichcontains thePTENgene (a gift from Dr. Ramon Parsons). Theprobe was labeled with biotin-dUTP by nick translation(BioNick, GibCo, Inc.), and prepared for hybridization usingstandard methods [Lichter et al., 1991]. Hybridization wascarried out at 370C for 20 hours, followed by successive washesin 50% formamide and 2xSSC at 420C, and a final wash in4xSSC and 0.5% Tween-20 at room temperature. The probe wasdetected using FITC-avidin and one round of signalamplification with anti-avidin. A Zeiss Axioskop equipped withepiflourescence and a dual band-pass filter set was used withKodak Ektachrome Elite II 400 film.
Pathology: Endoscopically resected polyps were fixed in 10%buffered formalin, embedded in paraffin, sectioned and stainedwith hematoxylin and eosin.
CLINICAL REPORT
The propositus is an 18-month- old Caucasian boy whowas referred for a second opinion, with a diagnosis of BRRsyndrome. He was born after an uncomplicated pregnancy andwas delivered by Caesarean section at 42 weeks for failure toprogress. The mother was a 32-year-old gr3p1 woman with ahistory of two first trimester miscarriages. Both parents were ingood health and the family history was otherwise unremarkable.The patient’s birth weight was 4904 g, length 58.5 cm, and OFC42 cm, all >95th centile. During the first year, he was followedas an outpatient for macrosomia. Weight and length for ageslowly approached the 75th centile. Head circumferenceremained markedly elevated, a pattern typical of the BRRsyndrome. He presented at 18 months of age with a recenthistory of hematochezia which required endoscopic intervention.
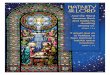
On examination at 18 months height and weight were atthe 75th to 90th centile, while OFC was 58 cms, 7SD above themean for age. Rate of head growth based on previous recordswas normal. He had evident brachycephaly, a prominentforehead, hypertelorism, and mild mid-face hypoplasia (Fig. 1).A 3x4 cm lipoma was present on the right abdomen, and another,measuring 1x1/2 cm, was found on the right thumb. Two smallhemangiomas were present on the back and shoulder, and twoskin tags were noted at the base of the spine and in the groinarea. Axial hypotonia was present, with otherwise normalneurologic findings. Cardiorespiratory and abdominal status waswithin normal. He had an undescended right testicle.Development was delayed, with an approximate motordevelopmental quotient of 60%, and language developmentalquotient of 90%. Hearing was normal as were brain auditoryevoked responses. Ophthalmologic examination showedbilateral pseudopapilledema and anisometropia. Neither parenthad any signs of Cowden disease or BRR syndrome. Their headcircumferences were at the 98th-99th centile.
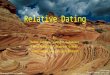
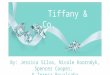
Previous investigations in this patient included a CT scanof the brain which showed normal structure and ventricles ofnormal size. Upper and lower GI endoscopy demonstratedmultiple sessile hamartomatous polyps throughout the duodenumand large intestine (Fig 2). Small bowel follow-through wasnormal. Muscle biopsy showed no evidence of myoliposis.Blood was taken for general biochemical studies, plasma aminoacid, plasma free fatty acid and plasma carnitine levels and anacyl-carnitine profile. All results were normal. Qualitative urineorganic acid analysis was normal. Results of thyroid functiontests were also normal. Muscle carnitine was not measured. Thelymphocyte karyotype was 46,XY,del(10)(q23.2q24.1); in eachof 22 cells examined one copy of chromosome 10 had aninterstitial deletion of the long arm resulting in loss of thematerial from band q23.2 to the interface between bands q23.3and q24.1 (Fig. 3). FISH, using a probe specific for thePTENgene, demonstated the absence ofPTEN from the deletedchromosome 10. The patient’s parents had normalchromosomes.
Fig. 1: Patient at age 18 months, showing macrocephaly, promi-nent forehead, depressed nasal root and lipoma on right abdomen(photograph courtesy of the mother).
490 Arch, et al.

DISCUSSION
Clinically, this patient fits the BRR phenotype. Thisincludes macrosomia at birth with isolated persistentmacrocephaly, developmental delay, hamartomatousgastrointestinal polyps, l ipomas, hemangiomas, andpseudopapilledema. Gastrointestinal polyps are common in theBRR syndrome. They are usually hamartomatous, but aregenerally confined to the distal ileum and colon [Gorlin et al.,1992]. Cowden disease is inadequately described in infants andchildren. In adults, pathognomonic criteria for this disorderinclude facial tricholemmas, present in nearly all cases, acralkeratosis, papillomatous lesions and mucosal lesions [Nelen etal., 1996]. However, these lesions are rarely present before thesecond to third decade making it difficult to diagnose thiscondition in children. Other signs of Cowden disease include GIpolyps, which are often hamartomatous and distributedthroughout the bowel, macrocephaly, mental retardation, andmalignancy reported in several tissues [Marra et al., 1994].Thus, BRR syndrome and Cowden disease share manymanifestations [see Table I]. Our patient fits the clinicaldiagnosis of BRR syndrome but clearly he has anomalies
common to both disorders.
Interstitial deletions of the region of chromosome 10 seenin our patient are rare, only 3 cases having been reported.. Twopatients were described independently in 1985 by Shapiro et al.and Morey et al. The deletion in the first patient involvedthe region 10q22.3-q24, while the second patient’s deletion wasidentical to that observed in our patient del(10)(q23.2q24.1).Both children were reported to have minor anomalies. The firstwas macrosomic at birth and had a flat nasal bridge, apparentlylow set ears and telecanthus. Few clinical findings are given onthe second patient. Significantly, both children had rectalprolapse but no gastrointestinal endoscopic or radiologicinvestigations were reported. The third patient described byMori et al. [1988] had macrocephaly at the age of 6 months, adeletion at 10q22-q24 and was also said to have a flat nasalbridge, hypertelorism, and apparently low set ears. Nogastrointestinal investigations were reported in this patient. Thepatient we describe has an interstitial deletion of 10q23.2-24.1and is clearly deleted for more than just thePTEN gene.However, all of the clinical anomalies found in our patient arealso seen in BRR syndrome and Cowden disease. This suggeststhat hemizygosity forPTEN is the most important factor indetermining the phenotype in our patient.
Cowden disease was mapped to 10q23.1-q24.1 by Nelenet al., [1996]. Loss of heterozygosity at this locus was reportedin sporadic tumors of the thyroid and prostate [Gray et al., 1995;Ittman, 1996; Marsh et al., 1997]. Li et al. [1997] isolated andcharacterized a gene from this region and called itPTEN. Theyproposed that the protein product ofPTEN is a tumor suppressorand demonstrated mutations inPTEN in breast, prostate andglioblastoma tumour cell lines. A second group of investigatorsalso isolated this gene (but called itMMAC1) and identified
Fig. 2: Resected hamartomatous polyp showing an admixture ofbenign epithelial and stromal elements as described previously inCowden disease and BRR syndrome [Hizawa et al., 1994;Carlson et al., 1984]. Focal erosion and inflammation is alsopresent (hematoxylin and eosin, original magnification 22x).
Fig. 3: Panel A shows a chromosome ideogram at 550 bandlevel on the left and the patient’s normal (center) and deletedchromosomes 10 to the right. Panel B shows a representativemetaphase cell and interphase nucleus hybridized withBAC265N13 containingPTEN,showing only one signal on thenormal chromosome 10.
Deletion of PTEN in BRR Syndrome 491

mutations in this gene in DNA from glioma, prostate, kidney andbreast tumor samples [Steck et al., 1997]. Subsequentlygermline point mutations inPTEN were reported in familialcases of Cowden disease [Liaw et al., 1997]. Our patient isdeleted forPTEN on FISH analysis. Clinically he fits thediagnosis of the BRR syndrome. We have described above thesubstantial overlap between BRR syndrome and Cowden diseaseand the lack of information on the latter disorder in childhood.Based on the above evidence, we suggest that the Bannayan-Riley-Ruvalcaba syndrome and Cowden disease are allelic. We
further suggest that all patients with a diagnosis of the BRRsyndrome be tested for mutations at thePTEN locus, so thatappropriate anticipatory guidance can be given to patients andfamilies concerning tumor risk and management.
Acknowledgments This work was in part supported byKKI/Hopkins NICHD Mental Retardation Center Core GrantHD24061. We would like to thank Dr. R. Parsons for thegenerous gift of the BAC clone 265N13.
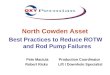
Table I: Comparison of clinical manifestations of BRR syndrome, Cowden Disease and the Patient
Cowden disease BRR syndrome Patient
Inheritance Autosomal dominant Autosomal dominant Sporadic
Mucocutaneous TricholemmaOral papillomasAcral keratosis
Palmoplantar keratosisHemangiomas
Multiple skin tags
LipomasAngiolipomasHemangiomas
Penile lentigines
LipomasHemangiomas
Skin tags
Gastrointestinal Polyps-varied histology-entire GI tract
Polyps-hamartomas-distal ileum and colon
Polyps-hamartomas-entire GI tract
Thyroid Goiter/AdenomaHyper/Hypothroidism
Thyroid carcinoma
Anomalies Macrocephaly MacrocephalyMacrosomia
HypertelorismDown slanting palpebral
fissures
MacrocephalyMacrosomia
Hypertelorism
CNS Mental retardationLhermitte-Duclos disease
Mental retardationLearning disabilities
SeizuresLipoid myopathy
Developmental delay
Ophthalmologic PseudopapilledemaProminent Schwalbe linesStrabismus / Amblyopia
PseudopapilledemaAnisometropia
Skeletal KyphoscoliosisPectus excavatum
ScoliosisPectus excavatum
Joint hyperextensibility
Joint hyperextensibility
Malignancy Carcinoma of breastthyroid, cervix, bladder.,
liver, GI and lung.Basal cell carcinoma
Squamous cell carcinomaMelanoma
Non-Hodgkins lymphomaAcute myeloid leukemia
Liposarcoma
Breast (1 patient) Unknown
[Gorlin et al., 1992; Hanssen and Fryns, 1995; Marra et al., 1994; Vinchon et al., 1994; Wells et al., 1994; Albrecht et al., 1992]
492 Arch, et al.

REFERENCES
Albrecht S, Haber RM, Goodman JC, Duvic M (1992):Cowden syndrome and Lhermitte-Duclos disease. Cancer70: 869-876.
Bannayan, GA (1971): Lipomatosis, angiomatosis andmacrocephaly: A previously undescribed cogenitalsyndrome. Arch Pathol 92:1-5.
Carlson GJ, Nivatvongs S, Snover DC (1984): Colorectalpolyps in Cowden’s disease (multiple hamartomasyndrome). Am J Surg Pathol 8:763-770.
Fargnoli MC, Orlow SJ, Semel-Concepcion JS, Bolognia JL(1996): Clinicopathologic findings in the Bannayan-Riley-Ruvalcaba syndrome. Arch Dermatol 132:1214-1218.
Gorlin RJ, Cohen MM, Levin LS (1990) ‘‘Syndromes of thehead and neck’’. 3rd ed. New York: Oxford UniversityPress; pp. 336-338.
Gorlin RJ, Cohen MM, Condon LM, Burke BA (1992):Bannayan-Riley-Ruvalcaba syndrome. Am J Med Genet44:307-314.
Gray IC, Phillips SMA, Lee SJ, Neoptolemos JP, WeissenbachJ, Spurr NK (1995): Loss of the chromosomal region10q23-25 in prostate cancer. Cancer Res 55:4800-4803.
Hanssen AMN, Fryns JP (1995): Cowden syndrome. J MedGenet 32:117-119.
Hizawa K, Iida M, Matsumoto T, Kohrogi N, Suekane H, YaoT, Fujishima (1994): Gastrointestinal manifestations ofCowden’s disease. Report of four cases. J Clin Gastro18(1):13-18.
Ittman M (1996): Allelic loss on chromosome 10 in prostateadenocarcinoma. Cancer Res 56:2143-2147.
Li J, Yen C, Liaw D, Podsypanina K, Bose S, Wang SI, Puc J,Miliaresis C, Rodgers L, McCombie R, Bigner SH,Giovanella BC, Ittmann M, Tycko B, Hibshoosh H,Wigler MH, Parsons R (1997):PTEN,a putative proteintyrosine phosphatase gene mutated in human brain, breast,and prostate cancer. Science 275:1943-1947.
Liaw D, Marsh DJ, Li J, Dahia PLM, Wang SI, Zheng Z, BoseS, Call KM, Tsou HC, Peacocke M, Eng C, Parsons R(1997): Germline mutations of thePTENgene in Cowdendisease, an inherited breast and thyroid cancer syndrome.Nature Genet 16:64-67.
Lichter P, Boyle AL, Cremer T, Ward DC (1991): Analysis ofgenes and chromosomes by nonisotopicin situhybridization. Genet Anal Techn Appl 8:24-35.
Lloyd KM, Dennis M (1963): Cowden disease: a possiblenew symptom complex wi th mul t ip le systeminvolvement. Ann Intern Med 58:136-142.
Mallory SB (1995): Cowden syndrome (multiple hamartomasyndrome). Dermatol Clinics 13:27-31.
Marra G, Armelao F, Vecchio FM, Percesepe A, Anti M(1994): Cowden disease with extensive gastrointestinalpolyposis. J Clin Gastroenterol 18:42-47.
Marsh DJ, Zheng Z, Zedenius J, Kremer H, Padberg GW,Larssen C, Longy M, Eng C (1997): Differential loss ofheterozygosity in the region of the Cowden locus within10q22-23 in follicular thyroid adenomas and carcinomas.Cancer Res 57:500-503.
Morey M, Harris DJ (1985): A 10q deletion syndrome. Am JHum Genet 37:A107.
Mori MA, Gomez-Sabrido F, Diaz di Bustamente A, Pinel I,Martinez-Frias ML (1988):De novo 10q23 interstitialdeletion. J Med Genet 25:209-212.
Nelen MR, Padberg GW, Peeters EAJ, Lin AY, van den HelmB, Frants RR, Coulon V, Goldstein AM, van Reen MMM,Easton DF, Eeles RA, Hodgson S, Mulvihill JJ, MurdayVA, Tucker MA, Mariman ECM, Starink TM, PonderBAJ, Ropers HH, Kremer H, Longy M, Eng C (1996):Localization of the gene for Cowden disease tochromosome 10q22-23. Nature Genet 13:114-116.
Ri ley HD, Smith WR (1960) : Macrocephaly ,pseudopapilledema and multiple hemangiomata.Pediatrics 26:293-300.
Ruvalcaba RHA, Myhre S, Smith DW (1980): Sotossyndrome with intestinal polyposis and pigmentarychanges of the genitalia. Clin Genet 18:413-416.
Shapiro SD, Hansen KL, Pasztor LM, DiLiberti JH, JorgensonRJ, Young RS, Moore CM (1985): Deletions of the longarm of chromosome 10. Am J Med Genet 20:181-196.
Steck PA, Pershouse MA, Jasser SA, Yung W.K., Lin H,Ligon AH, Langford LA, Baumgard ML. Hattier T, DavisT, Frye C, Hu R, Swedlund B, Teng DHF, Tavtiglian SV(1997): Identification of a candidate tumour suppressorgene, MMAC1, at chromosome 10q23.3 that is mutated inmultiple advanced cancers. Nature Genet 15:356-362.
Vinchon M, Blond S, Lejeune JP, Krivosik I, Fossati P,Assaker R, Christiaens JL (1994): Association ofLhermitte-Duclos and Cowden disease: report of an newcase and review of the literature. J Neurol NeurosurgPsychiatry 57; 699-704.
Wells GB, Lasner TM, Yousem DM, Zager EL (1994):Lhermitte-Duclos disease and Cowden’s syndrome in anadolescent patient. J Neurosurg. 81 133-136.
Yunis JJ, Chandler ME (1977): High resolution chromosomeanalysis in clinical medicine. In Stefanini M, Nossaini A.(eds): ‘‘Progress in clinical pathology.’’ New York:Grune and Stratton, pp. 267-288.
Zonana J, Rimoin DL, Davis DC (1976): Macrocephaly withmultiple lipomas and hemangiomas. J Pediatr 89:600-603.
Deletion of PTEN in BRR Syndrome 493