Embed Size (px)
Citation preview

There are a few descriptions of the characteristics ofepilepsy in patients with this chromosomal aberration, norare the characteristics of the seizures or EEG featuresavailable.
In conclusion, it is very complicated to define whetherthe epileptic seizures are part of 18p DS, and to our knowl-edge, this is the first report of intractable epilepsy in a casewith 18p DS. Additional reports are necessary to betterdefine the characteristics and outcome of epilepsy in thischromosomal aberration.
Conflict of interest: We confirm that we have read the Journal’s positionon issues involved in ethical publication and affirm that this report is con-sistent with those guidelines. None of the authors has any conflict of inter-est to disclose.
Caterina [email protected]
Adriana Lo CastroLuigi D’Argenzio
Cinzia GalassoPaolo Curatolo
Pediatric Neurology UnitDepartment of Neuroscience
Tor Vergata University, Rome, Italy
REFERENCES
Grosso S, Pucci L, Di Bartolo RM, Gobbi G, Bartalini G, Anichini C,Scarinci R, Balestri M, Farnetani MA, Cioni M, Morgese G, BalestriP. (2005) Chromosome 18 aberrations and epilepsy: a review. Am JMed Genet A 134:88–94.
Vaquerizo J, Gomez Martin H, Galan E, Cardesa JJ. (1995) [Infantilespasms in a patient with 18p monosomy]. Rev Neurol 23:453–454.
Wester U, Bondeson ML, Edeby C, Anneren G. (2006) Clinical andmolecular characterization of individuals with 18p deletion: a geno-type-phenotype correlation. Am J Med Genet A 140:1164–1171.
Delayed responses in TMS-EEG aredifferent from SPES
To the Editors:We read with great interest the paper by Valentin and col-
leagues recently published in Epilepsia (Valentin et al.,2008). This report was the first to evaluate transcranial mag-netic stimulation electroencephalography (TMS-EEG)responses in epileptic patients, in comparison to healthy
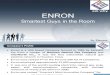
Figure 1.
Sleep EEG recording (stage II) performed at 7 years. EEG showing interictal spike and slow waves localized over fron-
tal-central leads that occur synchronously. In the right side: Amplitude map of paroxysmal activity (maximal activity
under F electrodes).
Epilepsia ILAE
GRAY MATTERS
Epilepsia, Vol. 49, No. 10, 2008 1814

subjects, as a noninvasive tool for the diagnosis of focal epi-lepsy. This study can be seen as the extension of their earlierwork with single-pulse electrical stimulation (SPES)(Valentin et al., 2002, 2005a, 2005b). The authors concludethat this work has opened a number of new ave-nues forfuture research, some beyond the diagnosis of epilepsy.
Within their conceptual framework, the authors sug-gested that delayed TMS-EEG responses appear to beequivalent to delayed responses produced by SPES inpatients with intracranial electrodes. In particular, whenthey stimulate extratemporal structures, repetitive TMS-EEG responses were seen. According to the authors, theseTMS-EEG responses represented the scalp correlate ofrepetitive responses to SPES, but altered by averaging andattenuation due to brain coverings. However, there is a fun-damental difference between the physiology of tissue exci-tation due to TMS and direct electrical stimulation of brain.In TMS, the induced current in the brain flows in parallel tothe surface of the coil (i.e., in parallel with the horizontalfibers in the cortex), with a preferential activation ofhorizontally oriented neural elements (Abbruzzese &Trompetto, 2002). In contrast, the electric field generatedby subdural electrodes has a complex shape distributedthroughout the brain. This field is applied to the complexthree-dimensional geometry of the surrounding neuralprocesses, resulting in their stimulation (Nair et al., 2008).Both experimental and computer modeling studies haveshown that cells and fibers of passage have similar thres-holds to stimulation using conventional stimuli (Mcintyre& Grill, 2000). Hence, TMS-EEG and SPES have differentsubstrates of stimulation. This fact is responsible for thedifference between these two modalities in activation ofindirect and direct waves. Electrical stimulation evokesfewer indirect waves than TMS (Abbruzzese & Trompetto,2002). Hence, despite superficial resemblance of EEGresponses, the underlying physiology of late responsegeneration and their clinical implications may be differentin SPES and TMS-EEG responses.
It would be very interesting to know if the authors hadcompared their novel TMS-EEG technique with traditionalTMS markers of cortical excitability, such as resting motorthreshold (RMT), cortical silent period (CSP), intracorticalinhibition (ICI), and intracortical facilitation (ICF).Results with these traditional measurements, in cases ofpartial seizures, have been variable (Macdonell et al.,2002). A future study comparing the late response in TMS-EEG with traditional parameters may give us new insightinto the genesis of the late response.
ACKNOWLEDGMENTS
Conflict of interest: We confirm that we have read the Journal’s positionon issues involved in ethical publication and affirm that this report is con-sistent with those guidelines. The authors have no conflicts of interest todisclose.
Abhijit Das1
[email protected]. Dinesh Nayak1,2
1Sree Chitra Tirunal Institute of MedicalScience and Technology
Trivandrum, India2R. Madhavan Nayar Center for
Comprehensive Epilepsy CareSCTIMST, Trivandrum, India
REFERENCES
Abbruzzese G, Trompetto C. (2002) Clinical and research methods forevaluating cortical excitability. J Clin Neurophysiol 19:307–321.
Macdonell RAL, Curatolo JM, Berkovic SF. (2002) Transcranial mag-netic stimulation and epilepsy. J Clin Neurophysiol 9:294–306.
Mcintyre CC, Grill WM. (2000) Selective Microstimulation of CentralNervous System Neurons. Ann Biomed Eng 28:219–233.
Nair DR, Burgess R, McIntyre CC, Luders H. (2008) Chronic subduralelectrodes in the management of epilepsy. Clin Neurophysiol 119:11–28.
Valentin A, Anderson M, Alarcon G, Seoane JJ, Selway R, Binnie CD,Polkey CE. (2002) Responses to single pulse electrical stimulationidentify epileptogenesis in the human brain in vivo. Brain 125:1709–1718.
Valentin A, Alarcon G, Garcia-Seoane JJ, Lacruz ME, Nayak SD, Hona-var M, Selway RP, Binnie CD, Polkey CE. (2005a) Single-pulse elec-trical stimulation identifies epileptogenic frontal cortex in the humanbrain. Neurology 65:426–435.
Valentin A, Alarcon G, Honavar M, Garcia Seoane JJ, Selway RP,Polkey CE, Binnie CD. (2005b) Single pulse electrical stimulation foridentification of structural abnormalities and prediction of seizureoutcome after epilepsy surgery: a prospective study. Lancet Neurol4:718–726.
Valentin A, Arunachalam R, Mesquita-Rodrigues A, Garcia Seoane JJ,Richardson MP, Mills KR, Alarcon G. (2008) Late EEG responsestriggered by transcranial magnetic stimulation (TMS) in the evalua-tion of focal epilepsy. Epilepsia 49:470–480.
NEXT MONTH IN Epilepsia
The November issue of Epilepsia features two interest-ing review articles. The first (from Dr. Asadi-Pooya andcolleagues) takes up the issue of ‘‘Nutritional supplements,foods, and epilepsy.’’ The second (from Dr. Theodore andcolleagues) focuses on the important question of whetherhuman herpes virus 6B has a possible role in epilepsy. Thefull-length research reports in this issue have a generallypediatric theme, with articles on Childhood AbsenceEpilepsy (behavioral, cognitive, and linguistic comorbidi-ties), growing up with epilepsy (cognitive development inchildren with new onset epilepsy), absence seizures, and anumber of other childhood-related issues (e.g., hypsar-rhythmia and autism). This issue also presents a set ofstudies dealing with electroencephalographic phenomena(interictal spikes, high frequency oscillations, paroxysmalfast runs) and their interpretations.
GRAY MATTERS
Epilepsia, Vol. 49, No. 10, 20081815