Embed Size (px)
Citation preview

Vol. 155, 1831-1840. June 1996 Prtnted in (J.S.A.
Review Article
DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION: ETIOLOGY, MANAGEMENT AND LONG-TERM SIGNIFICANCE
DANIEL A. SHOSKES AND PHILIP F. HALLORAN From the Division of Urology, Department of Surgery, UCLA School of Medicine, Harbor UCLA Medical Center, Torrance, California, and
Division of Nephrology and Immunology, Department of Medicine, University of Alberta Edmonton, Alberta, Canada
ABSTRACT
Purpose: In cadaveric renal t ransplan ta t ion a period of delayed graft funct ion postoperatively i s n o t uncommon and often associated with a poor outcome. We reviewed the biology of reper- fusion in jury and delayed graft function in renal t ransplan ta t ion , as well as its prevent ion, management and long-term effects.
M a t e r i a l s and Methods: The medical literature covering acute tubular necrosis, delayed graft funct ion i n renal transplantation and immunology of ischemia reperfusion injury was reviewed.
Results: Delayed graft funct ion is clearly associated with poor allograft survival , and is caused b y an interact ion of ischemic and immunological factors. Technical and pharmacological maneu- v e r s c a n improve ear ly funct ion rates. The response to ischemic injury i s complex, and may increase graft immunogenici ty and promote the chronic proliferative changes seen in chronic a l lograf t nephropathy .
Conclusions: Improvement in early renal function should be a pr imary goal in renal trans- plantation t o e n h a n c e early and long-term results. Basic research in to the injury response m a y yield insights i n t o renal pathophysiology.
KEY WORDS: kidney transplantation; organ transplantation; kidney failure, acute; reperfusion injury; immunology
Nonspecific injury in cadaveric renal transplants is a sig- nificant clinical problem but may also represent a potential source of major biological insights. Renal transplantation represents an opportunity to study the renal response to various types of injury, including ischemic, immunological and pharmacological. In cadaveric renal transplantation some injury to the kidney is inevitable and initial function often is poor or absent. Most kidneys that exhibit delayed graft function eventually recover and many achieve long- term survival. Early effects of delayed graft function include prolonged hospital stay, additional imaging studies, addi- tional biopsies and excessive or inappropriate immunosup- pression. Increased costs and decreased patient satisfaction are frequent consequences.’-” In addition, a n emerging body of evidence suggests that delayed graft function may have deleterious long-term effects related to acute and chronic rejection. These harmful effects may be mediated by factors that a re ischemic and/or immunological. The study of this set of problems represents an opportunity to examine how non- specific and immunologically specific injuries interact in re- nal inflammation.
The nomenclature of early allograft dysfunction is incon- sistent and can be misleading when studies using different definitions are compared. Delayed graft function is a clinical diagnosis and transplant acute tubular necrosis is a patho- logical diagnosis but the terms are often used interchange- ably. Most studies define delayed graft function as the need for any or more than 1 dialysis sessions in a specified post- operative period. Other studies also include urine output and
Supported by grants from the Harbor-UCLA Research and Edu- cational Institute, Kidney Foundation of Canada, Alberta Heritage Foundation for Medical Research, Medical Research Council of Can- ada, Sandoz Canada and Muttart Foundation.
1
decrease in creatinine as criteria to distinguish delayed graft function from early function. Grafts with delayed function that is never regained are referred to a s never functioning or primary nonfunction. While most delayed graft function is due to transplant acute tubular necrosis, technical and im- munological factors can also delay graft function in the ab- sence of classical histological acute tubular necrosis findings.
In this review we discuss the clinical and basic data on the nature and pathogenesis of nonspecific and specific injuries in renal transplants, and outline some hypotheses and sup- portive evidence to explore the interrelationships between the 2 conditions. We believe that the problem of ischemic and immune injury in renal transplants may have some lessons for the wider issues in renal responses to injury and disease.
ETIOLOGY OF TRANSPLANT ACUTE TUBULAR NECROSIS
As mentioned, delayed graft function may be due to isch- emic and/or immunological causes, which may act synergis- t i ~ a l l y . ~ Despite recent progress in the understanding of the cellular and molecular mechanisms involved with acute tu- bular necrosis of the native kidneys,”G it does not necessarily follow that identical mechanisms are in effect in transplant acute tubular necrosis. Nevertheless, most data on the mech- anisms of acute tubular necrosis come from nontransplant models, and so currently extrapolations to the transplant population are necessary.
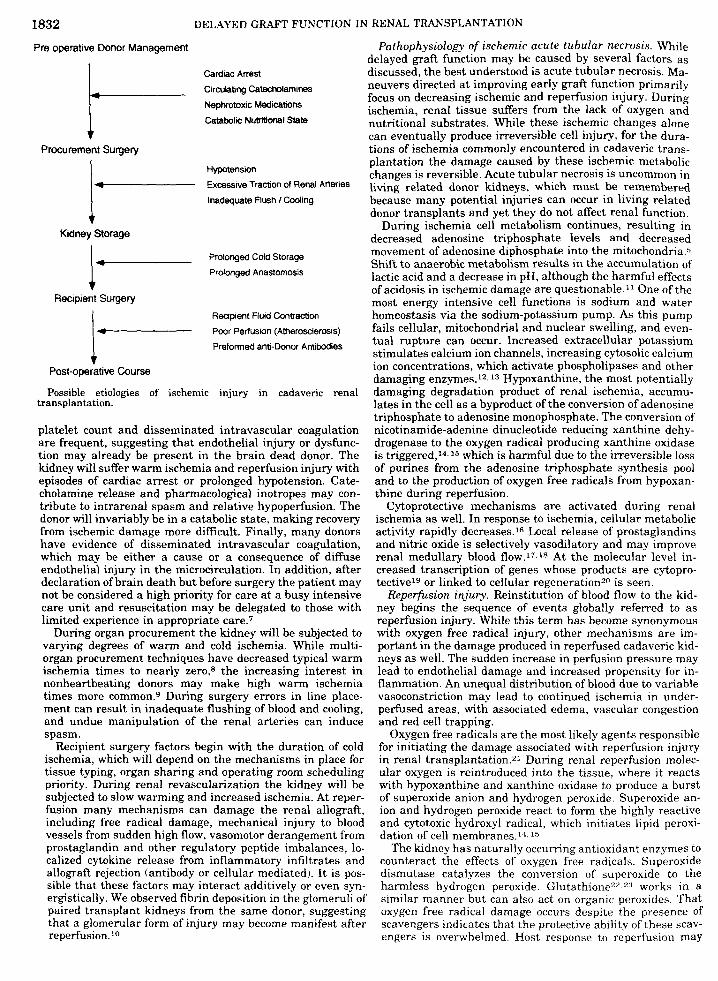
The cadaveric kidney is subject to damage at every step along the path from procurement to reperfusion (see figure). Before the declaration of brain death, the kidney may be damaged by the underlymg disease process, or from the ther- apeutic maneuvers instituted in a n attempt to revive the patient or maintain circulation after brain death. Decreasing
83 1
1832 DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION
Pre operative Donor Management
Cardiac Arrest
Circuhang Catecholamines
Nephrotoxic Medicamns
Catnbolic Nutritional State
Procurement Surgery
Hypotension
Excessive Tracbon of Renal Arteries
Inadequate Flush I Cooling
Prolonged Cold Storage
Prolonged Anastomosis
I. i- i.
Kidney Storage
Recipient Flurd Contracbon
Pwr Perfusion (Atherosclerosis)
Preformed ana-Donor Ambodies
Recipient Surgery
Post-operative Course
Possible etiologm of ischemic injury in cadavenc renal transplantation
platelet count and disseminated intravascular coagulation are frequent, suggesting that endothelial injury or dysfunc- tion may already be present in the brain dead donor. The kidney will suffer warm ischemia and reperfusion injury with episodes of cardiac arrest or prolonged hypotension. Cate- cholamine release and pharmacological inotropes may con- tribute to intrarenal spasm and relative hypoperfusion. The donor will invariably be in a catabolic state, making recovery from ischemic damage more difficult. Finally, many donors have evidence of disseminated intravascular coagulation, which may be either a cause or a consequence of diffuse endothelial injury in the microcirculation. In addition, after declaration of brain death but before surgery the patient may not be considered a high priority for care at a busy intensive care unit and resuscitation may be delegated to those with limited experience in appropriate care.7
During organ procurement the kidney will be subjected to varying degrees of warm and cold ischemia. While multi- organ procurement techniques have decreased typical warm ischemia times to nearly zero,8 the increasing interest in nonheartbeating donors may make high warm ischemia times more common.9 During surgery errors in line place- ment can result in inadequate flushing of blood and cooling, and undue manipulation of the renal arteries can induce spasm.
Recipient surgery factors begin with the duration of cold ischemia, which will depend on the mechanisms in place for tissue typing, organ sharing and operating room scheduling priority. During renal revascularization the kidney will be subjected to slow warming and increased ischemia. At reper- fusion many mechanisms can damage the renal allograft, including free radical damage, mechanical injury to blood vessels from sudden high flow, vasomotor derangement from prostaglandin and other regulatory peptide imbalances, lo- calized cytokine release from inflammatory infiltrates and allograft rejection (antibody or cellular mediated). I t is pos- sible that these factors may interact additively or even syn- ergistically. We observed fibrin deposition in the glomeruli of paired transplant kidneys from the same donor, suggesting that a glomerular form of injury may become manifest after reperfusion. 1"
Pathophysiology of ischemic acute tubular necrosis. While jelayed graft function may be caused by several factors as liscussed, the best understood is acute tubular necrosis. Ma- neuvers directed at improving early graft function primarily Focus on decreasing ischemic and reperfusion injury. During ischemia, renal tissue suffers from the lack of oxygen and nutritional substrates. While these ischemic changes alone can eventually produce irreversible cell injury, for the dura- tions of ischemia commonly encountered in cadaveric trans- plantation the damage caused by these ischemic metabolic changes is reversible. Acute tubular necrosis is uncommon in living related donor kidneys, which must be remembered because many potential injuries can occur in living related donor transplants and yet they do not affect renal function.
During ischemia cell metabolism continues, resulting in decreased adenosine triphosphate levels and decreased movement of adenosine diphosphate into the mitochondria.5 Shift to anaerobic metabolism results in the accumulation of lactic acid and a decrease in pH, although the harmful effects of acidosis in ischemic damage are questionable.ii One of the most energy intensive cell functions is sodium and water homeostasis via the sodium-potassium pump. As this pump fails cellular, mitochondria1 and nuclear swelling, and even- tual rupture can occur. Increased extracellular potassium stimulates calcium ion channels, increasing cytosolic calcium ion concentrations, which activate phospholipases and other damaging enzymes.12.13 Hypoxanthine, the most potentially damaging degradation product of renal ischemia, accumu- lates in the cell as a byproduct of the conversion of adenosine triphosphate to adenosine monophosphate. The conversion of nicotinamide-adenine dinucleotide reducing xanthine dehy- drogenase to the oxygen radical producing xanthine oxidase is triggered,*4,15 which is harmful due to the irreversible loss of purines from the adenosine triphosphate synthesis pool and to the production of oxygen free radicals from hypoxan- thine during reperfusion.
Cytoprotective mechanisms are activated during renal ischemia as well. In response to ischemia, cellular metabolic activity rapidly decreases.16 Local release of prostaglandins and nitric oxide is selectively vasodilatory and may improve renal medullary blood flow.17.18 At the molecular level in- creased transcription of genes whose products are cytopro- tectiveig or linked to cellular regenerationz" is seen.
Reperfusion injury. Reinstitution of blood flow to the kid- ney begins the sequence of events globally referred to as reperfusion injury. While this term has become synonymous with oxygen free radical injury, other mechanisms are im- portant in the damage produced in reperfused cadaveric kid- neys as well. The sudden increase in perfusion pressure may lead to endothelial damage and increased propensity for in- flammation. An unequal distribution of blood due to variable vasoconstriction may lead to continued ischemia in under- perfused areas, with associated edema, vascular congestion and red cell trapping.
Oxygen free radicals are the most likely agents responsible for initiating the damage associated with reperfusion injury in renal transplantation.2' During renal reperfusion molec- ular oxygen is reintroduced into the tissue, where it reacts with hypoxanthine and xanthine oxidase to produce a burst of superoxide anion and hydrogen peroxide. Superoxide an- ion and hydrogen peroxide react to form the highly reactive and cytotoxic hydroxyl radical, which initiates lipid peroxi- dation of cell membranes.*j. 16
The kidney has naturally occurring antioxidant enzymes to counteract the effects of oxygen free radicals. Superoxide dismutase catalyzes the conversion of superoxide to the harmless hydrogen peroxide. Glutathione". 2:j works in a similar manner but can also act on organic peroxides. That oxygen free radical damage occurs despite the presence of scavengers indicates that the protective ability of these scav- engers is overwhelmed. Host response to reperfusion may
DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION 1833 potentiate oxygen free radical damage. Chemokines released during lipid peroxidation attract granulocytes and neutro- phils,15.24’25 which have the ability to release additional ox- ygen reactive species and further potentiate the renal dam- age.
Vasospasrn and new ischemiat reperfusion due to endothe- Zial dysfunction. Following reperfusion the ischemic kidney has varying degrees of cellular and functional damage. On the cellular level the cells are either dead, irreparably dam- aged, damaged but salvageable or unharmed. On the func- tional level the heterogeneous nature of renal architecture results in the possibility of a spectrum of nephron and vas- cular damage, which again may be partial or complete.26 Whether the kidney can recover from the ischemic insult will depend on the ability of the noninjured cells to develop growth factors and proliferate, as well as on the nonlethally damaged cells to recover function. In a renal transplant set- ting restitution of blood flow serves to end the ischemic period and begin the immunological allograft response. These highly anabolic events must occur in the relative cat- abolic state of a postoperative patient, and in the presence of pharmacological agents that may have catabolic and nephro- toxic properties and block the production of growth factors and cytokines.
The pathophysiology of the post-ischemic kidney has been described as vasomotor nephropathy,27 which is character- ized by elevated renovascular resistance, increased afferent arteriolar resistance, decreased glomerular capillary hydrau- lic pressure and decreased glomerular capillary permeabili- ty.28-30 Some element of increased vascular resistance de- rives from back pressure from congested tubules, which have been obstructed with cellular debris.31 The vasomotor insta- bility probably reflects the effects of vasoactive molecules released as part of inflammatory or immunological reactions. Damaged vascular endothelium is a primary source of these regulatory molecules. Ischemic renal damage disrupts the balance of eicosanoid metabolism, causing vasoconstriction due to excess thromboxane, and decreased prostacyclin and prostaglandin 12.17-32 In addition, nitric oxide helps maintain vascular relaxation and medullary oxygenation,%.% and is important in overcoming post-ischemic vasoconstriction.l8P 35
As recently reviewed by Toback: renal epithelial regener- ation after ischemic damage is mediated by growth factors and cytokines secreted in response to extracellular signals. These factors may stimulate growth by induction of cell di- vision (for example epidermal growth factor) or inhibit growth by preventing the cell from leaving the resting state (for example transforming growth factor-@. Other factors may facilitate renal regrowth by induction of adhesion mol- ecules (for example interferon-?), recruitment of other in- flammatory cells or stimulation of extracellular matrix pro- duction.
A particular focus of research into ischemic renal injury is the addition of exogenous growth factors to accelerate recov- ery. Epidermal growth factor is an attractive candidate due to its strong mitogenic properties in renal tubule cells and the fact that renal epidermal growth factor synthesis de- creases after injury.36.37 Indeed, the exogenous delivery of epidermal growth factor in rodent models of ischemic acute tubular necrosis hastens renal epithelial r e ~ a i r . ~ ~ , ~ ~ In a pig
~ model, however, this accelerated cellular recovery did not 1 translate into improved renal function.40 Nevertheless, a fur- , ther dissection of the pathways and mediators involved in
renal regeneration may produce strategies for improving hu- man renal ischemic recovery.
PREVENTION OF DELAYED GRAFT FUNCTION
With improved understanding of the pathophysiology of ,renal ischemia and reperfusion injury, strategies to decrease the rates of delayed graft function have evolved, focusing on I
donor management, organ procurement and preservation techniques, recipient fluid management and pharmacological agents. Nevertheless, rates of delayed graft function in ca- daveric renal transplantation range from 10 to 60%. When one compares serum creatinine levels in cadaveric and living related transplants, one must conclude that most cadaveric kidneys have some degree of renal injury, albeit nonoliguric.
Donor factors before and during procurement surgery re- main an important predictor of eventual graft function. Kid- neys from donors at the extremes of age (younger than 4 or older than 55 years) have higher rates of delayed graft func- t i ~ n . ~ . ~ l Not surprisingly, kidneys from nonheartbeating do- nors or those with prolonged warm ischemia from other causes also have increased rates of delayed graft function.42 Donor urine output during procurement also correlates with recipient urine 0utput.~~.43 Animal experiments suggested that the state of brain death leads to impaired left ventricu- lar contractility and decreased cardiac output.44845 Therefore, the mainstay of donor management is aggressive fluid and inotrope therapy to ensure adequate perfusion of the kid- neys, followed by rapid cooling and flushing of the kidneys to minimize warm ischemia, and accelerating organ removal. Additional pharmacological treatments, such as diuretics, al-blockers or oxygen free radical scavengers, appear to offer no increased benefit.*
Duration of cold ischemia has been implicated as a factor in delayed graft function. At centers where cold ischemia times are consistently short or within a narrow range they do not appear to be a risk factor.47 Prolonged cold ischemic time is now more common and appears to be an independent risk factor for delayed graft function.4.48-50 The anastomosis time (second warm ischemia) has also been strongly correlated with delayed graft function and, in fact, was identified as the strongest independent predictor of delayed graft function in 2 s tud ies .4~~~ Obvious remedies for prolonged ischemia are de- creased storage times, timely access to operating moms and maintaining surface cooling of the kidney during anastomo- sis.
Preservation solutions have been designed to minimize ischemic damage during storage. Components are added to decrease cell swelling, maintain calcium homeostasis, de- crease free radical substrate formation and provide high energy substrates. For long-term cadaveric renal storage the University of Wisconsin solution of Belzer and Southard52 has proved efficacious and superior to the older Collins solu- tion.41 The method of preservation may also have a role in delayed graft function. I t is controversial whether storage on a pulsatile p e b i o n machine is superior to simple cold stor- age. In a randomized prospective trial the rate of delayed graft function decreased from 44% with cold storage to 31% with pulsatile perfusion but no benefit was noted in patient or graft survival.53 In a study in which the 2 kidneys from each donor were split between cold storage and pulsatile perfusion, no significant improvement in early function or graft survival was noted in the pulsatile perfusion group even with cold ischemia times of more than 24 hours.” More recently, pulsatile pefision is again being evaluated to im- prove early function rates and as a test of renal viability.55
Immunological risk factors also increase the rate of de- layed graft function, including the number of previous trans- plants, level of anti-histocompatibility locus antigen (HLA) panel reactive antibodies4 and presence of donor specific an- tibodies against HLA class I targets.56 In children ischemic and immunological factors were synergistic in effect on early graR fmction.4 While there is currently no reliable way to decrease sensitization, early function rates could be im- proved in patients with high immunological risk by selecting kidneys with minimal ischemic risk factors.
During recipient surgery the volume status is a predictor of initial function. Patients before transplantation are often volume contracted, having possibly undergone recent dialysis
1834 DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION
to Ydry weight” and having received nothing by mouth for several hours. Central venous monitoring and aggressive fluid management by perioperative fluid expansion with col- loid (1 mg.kg. albumin) can improve initial f u n ~ t i o n . ~ ~ . ~ ~ Diuretics in the well hydrated recipient have also been used to improve early graft function. Mannitol has been shown to improve early function when given to the recipient just before reperfusion,59.60 which may be due to its diuretic andlor oxygen free radical scavenger properties. Furosemide is often given after reperfusion to promote diuresis, although whether it actually improves early function or simply in- creases urine output from an otherwise functioning kidney is unclear.61
Pharmacological agents have been used in organ preserva- tion and recipient management to improve early function. Calcium channel blockers have been shown to improve initial graft function and decrease the nephrotoxic effects of cyclo- sporine. Possible mechanisms are a direct vasodilatory effect on proximal arterioles and a decrease in lipid peroxidation during reperfusion. l2 In 3 prospective randomized trials treatment with diltiazem in either the donor or recipient improved initial function (donor pretreatment 90 versus 59% in controls, recipient treatment 70 versus 55%).62 A similar benefit has been noted with recipient pretreatment with ni- fedipine,46.6:’ felodipine64 or verapamil.58 Allopurinol and ox- ygen free radical scavengers have been used perioperatively to decrease free radical damage. Early results of randomized trials showed no statistically significant benefit in early func- tion rates.6s Long-term followup suggested improvement in acute rejection and 4-year graft survival rates in patients treated with oxygen free radical scavengers.66 Prostacyclin (prostaglandin 12) has been shown in vitro32 and in viv067 to improve the resistance of kidneys to ischemic damage. How- ever, a prospective trial of the prostaglandin E analogue, enisoprost, failed to show any beneficial effects.68 Atrial na- triuretic factor has also been effective in decreasing ischemic renal injury in vit1-06~ but clinical studies have been disap- pointing.70 Finally, the 21-aminosteroids, a new class of agents that prevent lipid peroxidation, have shown promis- ing eariy results in the prevention of experimental renal reperfusion i n j ~ r y . ~ l
CLINICAL MANAGEMENT OF DELAYED GRAFT FUNCTION
Post-transplant oliguria is a common event in cadaveric renal transplantation that adds to the distress of the patient and work load of the clinician. Evaluation of delayed graft function requires the integration of clinical, laboratory, im- aging and possibly histological data. The differential diagno- sis can be divided into prerenal, renal and postrenal causes as with other cases of oliguria. The most common prerenal cause of post-transplant oliguria is recipient hypovolemia, which may be a result of overaggressive pre-transplant dial- ysis, underestimated surgical fluid losses or inadequate in- traoperative fluid administration. By definition, fluid chal- lenge with crystalloid or colloid will improve the urine output. An uncommon cause of prerenal anuria is vascular thrombosis.7‘ Immediate noninvasive imaging (Doppler or nuclear scan) followed by angiography and possible surgical exploration are indicated if thrombosis is suspected. Postre- nal causes of oligo-anuria are usually urological. Before any other course is taken the urinary catheter must be assessed for proper position and lack of obstruction. Ureteral compli- cations occur in approximately 4% of recipients, with leakage being much more common than obstruction in the immediate postoperative period.73 The best screening tests are ultra- sound and nuclear scan, with a definitive diagnosis being made by an antegrade nephrostogram (which can be con- verted to placement of a nephrostomy tube if the patient is not stable enough for immediate repair) or open surgery.74.75
When prerenal and postrenal causes are ruled out, and the
nuclear scan and ultrasound findings are typical of a renal :ause, the primary differential diagnosis of oliguria from renal causes includes hyperacute or antibody mediated rejec. tion, cyclosporine nephrotoxicity, acute tubular necrosis or, more rarely, recurrence of primacy renal disease. With the advent of more advanced crossmatching techniques hyper- acute rejection is now fortunately rare but clerical and tech- nical errors can still occur. In patients receiving cyclosporine induction therapy blood levels may be helpful in implicating drug nephrotoxicity but they can neither prove nor exclude cyclosporine as the cause of oliguria. Finally, acute tubular necrosis is a diagnosis of exclusion but i t may be expected more in the face of risk factors, S U C ~ as extremes of donor age, donor instability, increasing donor creatinine, prolonged ischemic times or high pressures measured during pulsatile perfusion p r e ~ e r v a t i o n . ~ ~
Diagnostic modalities. Ultrasound is often the first imag- ing study used in early graft dyshnction. Postrenal etiologies may be suggested by hydronephrosis or large perinephric fluid collections. Color Doppler techniques also allow demon- stration of adequate vascular flow to rule out thrombosis. Many attempts have been made to differentiate acute tubu- lar necrosis from rejection or drug toxicity by measuring intrarenal blood flow and calculating a pulsatility index.76 Unfortunately, all renal causes of delayed graft function may produce elevated renovascular resistance, resulting in signif- icant overlap of Doppler findings and making the test of minimal value in this ~ e t t i n g . ~ ~ . ~ ~
Nuclear scanning is often the most useful test in delayed graft function. The most commonly used agents are currently 99”technetium-pentetic acid and mercaptoacetyl triglycine. In acute tubular necrosis there typically is normal perfusion with delayed uptake and no clearance.79 With rejection there usually is decreased perfusion as well, although a slight decrease may be seen in both conditions. Serial scans may be required to differentiate the 2 conditions.
When clinical, laboratory and imaging studies remain in- conclusive closed renal biopsy is useful, especially to rule out the simultaneous occurrence of acute tubular necrosis with rejection. Fine needle aspiration biopsy, which is less inva- sive, may demonstrate activated immune cells.78 The renal core biopsies in the early post-transplant period must be interpreted with care, since leukocyte infiltration may be a feature of acute tubular necrosis alone. Solez et a1 noted features that distinguish transplant and nontransplant acute tubular necrosis.80
Treatment. Once acute tubular necrosis has been diag- nosed in the patient with delayed graft function the treat- ment is essentially supportive. Dialysis should be used when needed, balanced against the possibility that vasomotor changes associated with hemodialysis may prolong delayed graft function. Maneuvers to avoid the necessity for dialysis, such as reduction of unnecessary crystalloid infusions, potas- sium restriction and pharmacological blood pressure control, may be helpful. The benefit of low dose dopamine infusion in transplant acute tubular necrosis is controversial.81 Patients with acute tubular necrosis on cyclosporine may benefit from conversion to a n antilymphocytic preparation, since cyclospo- rine has been shown to increase the recovery time from transplant acute tubular necrosis.82 Furthermore, the high incidence of undiagnosed rejection in acute tubular necrosisa3 makes treatment with monoclonal antibody induction ther- apy (for example OKT3) theoretically attractive.
The usual pattern of recovery is progression from oliguric to nonoliguric acute tubular necrosis to a decrease in serum creatinine. During prolonged acute tubular necrosis regular nuclear imaging and possibly fine needle aspiration biopsies are helpful to rule out concurrent rejection or vascular com- promise. If the kidney does not recover despite prolonged supportive measures and biopsy suggests extensive necrosis, then the allograft should be removed.
1835 DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION
LONG-TERM EFFECTS OF DELAYED GRAFT FUNCTION
A possible link between delayed graft function and poor long-term graft survival has been debated since Whittaker e t al first proposed such a relationship in 1973.84 This issue has been particularly important since donor criteria have become more liberalized with a n attendant increased risk of delayed graft function from more marginal kidneys. A significant negative impact of delayed graft function on graft survival might prompt centers to refuse these more marginal kidneys, resulting in a further overburdening of waiting lists.
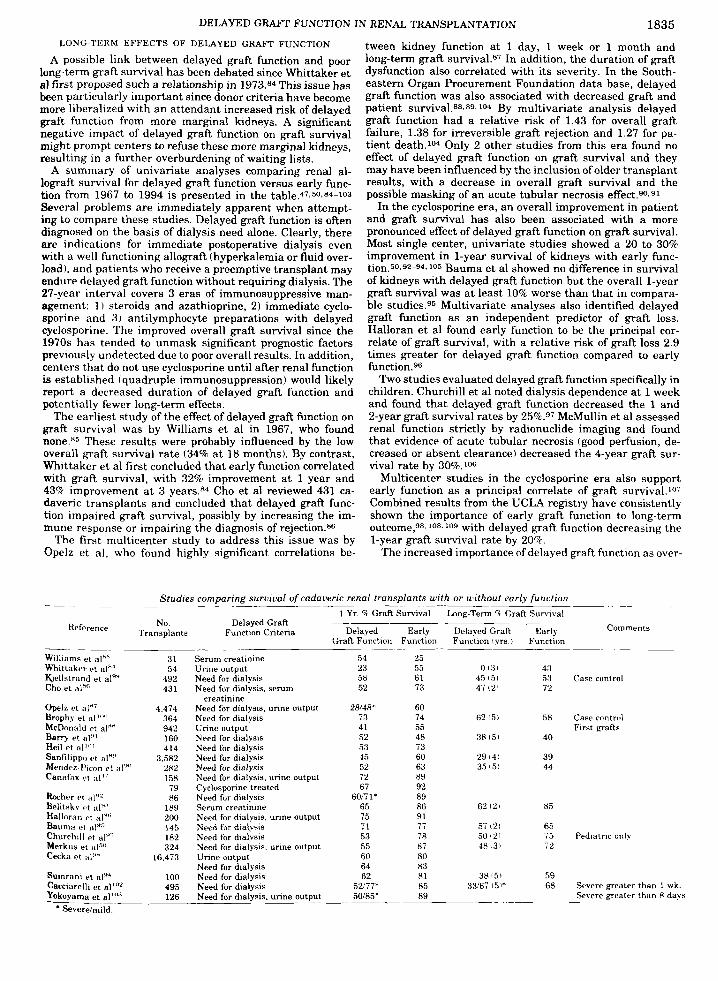
A summary of univariate analyses comparing renal al- lograft survival for delayed graft function versus early func- tion from 1967 to 1994 is presented in the table.47-50.84-103 Several problems are immediately apparent when attempt- ing to compare these studies. Delayed graft function is often diagnosed on the basis of dialysis need alone. Clearly, there are indications for immediate postoperative dialysis even with a well functioning allograft (hyperkalemia or fluid over- load), and patients who receive a preemptive transplant may endure delayed graft function without requiring dialysis. The 27-year interval covers 3 eras of immunosuppressive man- agement: 1 ) steroids and azathioprine, 2) immediate cyclo- sporine and 3) antilymphocyte preparations with delayed cyclosporine. The improved overall graft survival since the 1970s has tended to unmask significant prognostic factors previously undetected due to poor overall results. In addition, centers that do not use cyclosporine until after renal function is established (quadruple immunosuppression) would likely report a decreased duration of delayed graft function and potentially fewer long-term effects.
The earliest study of the effect of delayed graft function on graft survival was by Williams et al in 1967, who found
These results were probably influenced by the low overall graft survival rate (34% at 18 months). By contrast, Whittaker e t al first concluded that early function correlated with graft survival, with 32% improvement a t 1 year and 43% improvement a t 3 years.*4 Cho e t a1 reviewed 431 ca- daveric transplants and concluded that delayed graft func- tion impaired graft survival, possibly by increasing the im- mune response or impairing the diagnosis of rejection.s6
The first multicenter study to address this issue was by Opelz e t a], who found highly significant correlations be-
tween kidney function at 1 day, 1 week or 1 month and long-term graft survival.87 In addition, the duration of graft dysfunction also correlated with its severity. In the South- eastern Organ Procurement Foundation data base, delayed graft function was also associated with decreased graft and patient survival.88~89~104 By multivariate analysis delayed graft function had a relative risk of 1.43 for overall graft failure, 1.38 for irreversible graft rejection and 1.27 for pa- tient death.104 Only 2 other studies from this era found no effect of delayed graft function on graft survival and they may have been influenced by the inclusion of older transplant results, with a decrease in overall graft survival and the possible masking of a n acute tubular necrosis effect.90.91
In the cyclosporine era, a n overall improvement in patient and graft survival has also been associated with a more pronounced effect of delayed graft function on graft survival. Most single center, univariate studies showed a 20 to 30% improvement in 1-year survival of kidneys with early func- tion.50.92-94.105 Bauma e t al showed no difference in survival of kidneys with delayed graft function but the overall 1-year graft survival was a t least 10% worse than that in compara- ble studies.95 Multivariate analyses also identified delayed graft function as a n independent predictor of graft loss. Halloran e t al found early function to be the principal cor- relate of graft survival, with a relative risk of graft loss 2.9 times greater for delayed graft function compared to early function.96
Two studies evaluated delayed graft function specifically in children. Churchill e t al noted dialysis dependence at 1 week and found that delayed graft function decreased the 1 and 2-year graft survival rates by 25%.97 McMullin e t a1 assessed renal function strictly by radionuclide imaging and found that evidence of acute tubular necrosis (good perfusion, de- creased or absent clearance) decreased the 4-year graft sur- vival rate by 30%.'o6
Multicenter studies in the cyclosporine era also support early function as a principal correlate of graft survival.1'" Combined results from the UCLA registry have consistently shown the importance of early graft function to long-term outcome,98. lo8. log with delayed graft function decreasing the 1-year graft survival rate by 20%.
The increased importance of delayed graft function as over-
~ _ _ _ _ . ~ . Studies comparing suruival of cadaveric renal transplants with or without early function _- -~ _ _ ~
1 Yr. 1 GraR Survival Long-Term 1 Graft Survival
Comments No. Delayed Graft Reference Transplants Function Critena Delayed Early Delayed Graft Early
Graft Function Function Function 1 yrs. i Function -~ Williams et alhS Whittaker et a]"' &ellstrand et al" Cho et a\"'
Opelz et alyi Brophy et aI1'*I McDonald et al"" Berry et aI4' Heil et d'"' Sanfilippcr et HI'!'
Mender-l'lcon ct al'" Canafax P I
Rocher et alw2 Belitxky 1.t t ~ l ! ~ ' Halloren P t :i1"',
Baumti et n~"" Churchill Pt Merkus et al"" Cecka et a l "
Sumrani e t a1*4 Cacciarelli et aI'u' Yokoyama e t al"'"
* Severelmild. --___--
31 54
492 43 1
4,474 364 942 160 414
3.582 282 158
79 86
189
145 182 324
16.473
100 495 126
200
Serum creatinine Urine output Need for dialysis Need for dialysis, serum
Need for dialysis, urine output Need for dialysis Unne output Need for dialysis Need for dialysis Need for dialysis Nerd for dialysis Nerd for dialysis. urine output Cyclosporine treated Need for dialysis Serum creatinine Need for dialysis, unne output Need for dialysis Need for dialysis Need for dialysis. urine output Unne output Need for dialysis Need for dialysis Need for dialysis Need for dialysis. urine output
creatinine
54 23 58 52
28/4R3' 73 41 52 53 45 52 72 67
60/7 1 * 65 75 71 53 55 60 64 62
5 W 7 f 50185: -
25 55 61 73
60 74 55 40 73 60 63 89 92 89 86 91
78 87 80
81 85 89
7- I ,
83
~
0 13, 45 (51 47121
62 15)
38 15,
29 14) 35 151
62 121
57 121
40 131 50 121
38151 33/67 I5 I*
43 53 72
58
40
39 44
85
65 7 5 72
59 68
~~
Case control
Case control First grafts
Pediatric only
Severe greater than 1 ak Severe greater than H days _ _ ~ _ _ _ _ _ _ _ ~
1836 DELAYED GRAFT FUNCTION IN RENAL "IUNSPLANTATION
all graft survival improves is evidenced by the evolving Minnesota experience. Early reports showed no effect of de- layed graft function on graf? survival,%.lOO which was reversed in 1984.10' In a prospective randomized trial of cyclosporine versus antilymphocyte globulin and azathio- prine, delayed graft function decreased the 1-year graft ~ u r - vival rate by 17% in all patients and by 19% in those given cyclosporine.47 In a recent report early functioning kidneys were further subdivided according to the quality of initial function based on serum creatinine rate of decrease and nadir at 1 week.110 Patient and graft survival rates were improved for recipients with a serum creatinine of less than 3 mgJdl. by day 5 compared to those with a serum creatinine of more than 3 mgJdl. by day 7 or those requiring dialysis.
Other recent studies have also confirmed that the duration as well as the presence of delayed graft function is a sign6 cant prognostic factor. Cacciarelli et al found that dialysis dependence for greater than 1 week provided significantly worse 1 and 5-year graft survival rates compared to early functioning kidneys or those with dialysis confined to post- operative week 1.1°2 Yokoyama et al subdivided their pa- tients similarly but assigned never functioning kidneys to a separate fourth group, and found a 5-year graft survival rate of 89% in early functioning kidneys, 85% in those on dialysis for less than 1 week and 50% in those on dialysis for greater than 1 week.103
In summary, most modern studies have found that delayed graft function is a strong independent predictor of graft loss, particularly in the cyclosporine era. In addition, the duration of delayed graft function and even the quality of early func- tion, which are measures of the degree of vasomotor nephrop- athy and potential immunological damage, have correlated strongly with graft survival.
POSSIBLE MECHANISMS EXPLAINING DECREASED GRAFT SURVIVAL IN DELAYED GRAFT FUNCTION
In contrast to the extensive interest and reports on the link between delayed graft function and graft survival, there has been little research into the possible mechanisms to explain this relationship. Immunological and nonimmunological mechanisms have been invoked as possible explanations.
Immunological mechanisms. Because not all delayed graft function is due to pure acute tubular necrosis, intercurrent undiagnosed rejection may complicate the clinical picture. Recipients at higher immunological risk are more prone to have delayed graft function,4 and cellular and antibody me- diated rejection may present as primary nonfunction. In par- ticular, accelerated rejection due to preformed anti-class I antibodies may present as prolonged delayed graft function and may be less responsive to conventional immunosuppres- sion.56~ 111 Since early rejection episodes are an independent predictor of long-term graft loss,112,113 part of the deleterious effects of delayed graft function could be explained by undi- agnosed rejection associated with delayed function due to acute tubular nemsis.f'6.110 However, other studies sug- gested that delayed graft function, even in the absence of acute rejection, is deleterious to graft ~urvival.~.114 In a multicenter analysis of the UCLA registry data, Lim and Terasaki reported the best 1-year graft survival rate in kid- neys with early function and no rejection (88.7%), the worst rate in kidneys with delayed graft function and acute rejec- tion (50.9%) and an intermediate rate in kidneys with de- layed graft function but no rejection (72%).'08
Ischemic renal injury may increase the risk of graft loss due to rejection because of ischemic changes that affect the immune system. It is interesting to note that many of the inflammatory cytokines and other chemical mediators re- leased during the recovery from ischemic renal damage are identical to those released during the alloimmune response, including interferon- y, transforming growth factor-p,
I
nterleukin-6, prostaglandins and nitric oxide. It is likely that the pathways of renal regeneration and allograft rejec- tion interact in complex ways, which could lead to an altered immune response, a decrease in the rate of renal recovery and potentially an initiation of the proliferative cellular re- sponses that lead to chronic dlo& failure. Current para- digms for the pathogenesis of chronic rejection emphasize the importance of endothelial activation with cytokine and growth factor release, probably instigated by episodes of acute rejection.116 Renal ischemia may provide this local endothelial activation directly or indirectly through the pro- motion of acute rejection.
A research interest of ours is the potential for ischemic damage to increase the immunogenicity of the allograft. Ma- jor histocompatibility complex antigens can elicit strong im- mune responses, either via direct recognition of allo-major histocompatibility complex antigen molecules on the surface of the graft or via indirect recognition of processed peptides derived from these molecules and presented to the recipient immune system by recipient antigen presenting cells.116 EX- pression of major histocompatibility complex antigen mole- cules may be up regulated by a variety of stimuli in vivo, especially interferon-y.117 This up regulation of major histo- compatibility complex antigen on allografts is a feature of experimental and clinical renal transplant rejection,118.119 and may increase immunogenicity by providing a higher density of targets for allo-recognition.120
To study the effects of ischemia on renal major histocom- patibility complex antigen expression we developed a model of unilateral renal ischemia in the mouse in which the left kidney was subjected to warm ischemia and then reperfused, with the right kidney serving as a paired We found that ischemia resulted in increased major histocompatibility complex antigen class I expression on renal tubule cells and increased class 11 expression on interstitial cells. The class I up regulation appeared to be related to local interferon-? release.122.123 Furthermore, recovery from ischemia was as- sociated with an inflammatory infiltrate similar to that seen in human transplant acute tubular ne~rosis.12~ However, noninterferon-y cytokines must also be involved, since block- ade with anti-interferon- y monoclonal antibodies only par- tially blocks major histocompatibility complex antigen induc- tion. This up regulation of major histocompatibility complex antigens from ischemia has since been confirmed by other investigators in the rat kidney125 and rat lung.126 Finally, Wakabayashi et a1 found increased major histocompatibility complex antigen class I, interleukin-2R and ICAM-1 expres- sion on hepatocytes following liver warm ischemia.127
Goes et al subsequently showed that the response to isch- emia includes an increase in messenger ribonucleic acid (mRNA) levels for a number of cytokines, including interferon- y, interleukin-2, interleukin-10, granulocyte- macrophage colony-stimulating factor and transforming growth factor-p. At the same time, the mRNA in pre pro epidermal growth factor becomes undetectable in this model and remains low for weeks.128
We would postulate from these findings that recovery from ischemic damage may promote acute rejection through sev- eral pathways. Release of cytokines, such as interferon- y, as part of the regenerative process leads to increased expression of major histocompatibility complex antigen molecules and adhesion molecules, and promotes an inflammatory infil- trate. Induced donor class I1 major histocompatibility com- plex antigen molecules on the graft may be recognized di- rectly by infiltrating recipient CD4' cells. Infiltrating recipient macrophages or dendritic cells can also present processed peptides from the up regulated major histocompat- ibility complex antigen classes I and I1 molecules to recipient cells in the graft or in secondary lymphoid organs (lymph nodes or spleen).116 Recent evidence suggests that antigen presentation by dendritic cells is triggered by local tissue

DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION 1837 injury.129 Cytotoxic CD8’ T cells could then damage the graft with higher efficiency due to the induction of major histocom- patibility complex antigen class I targets. Such immune dam- age may itself induce an inflammatory, that is an injury, response.
Whether major histocompatibility complex antigen induction following delayed graft function after transplantation is clini- cally relevant or an epiphenomenon is unclear. To address this question clinically, Shoskes et al compared the effect of delayed graft function in patients whose ludneys were completely matched for the 6 HLA loci tested (6-antigen match) versus those with a total mismatch (0-antigen match).130 If induction of HLA antigen expression and increased immunogenicity are significant mechanisms for the deleterious effects of delayed graft function, one would expect that the 6-antigen matched kidneys would not be affected by delayed graft function, since the up regulated HLA antigens would be seen as “self antigens. Indeed, we found that delayed graft function sigmficantly de- creased short-term and long-term graft survivals in the 0-antigen match group but had no effect on the survival of the 6-antigen matched recipients. Interestingly, the 0-antigen match kidneys with early function had just as favorable long- term graR survivals as the 6-antigen match group overall.
Nonimmunological mechanisms. While the early graft loss associated with delayed graft function has several potential immunological mechanisms, chronic loss of renal function may be more complex. The entity of chronic rejection of renal transplants is still undergoing redefinition.’3* Rather than destruction of renal tissue, chronic rejection is characterized by cellular proliferation, such as intimal arterial thickening, interstitial fibrosis and cellular infiltration, which leads to progressive loss of renal function and appears to be indepen- dent of ongoing immunological stimulation. Tullius e t a1 showed in a rat model of chronic renal allograft rejection that re-transplantation of the renal allograft into a donor strain animal does not reverse the progression of chronic rejection unless the retransplantation is performed within 12 weeks of the initial transplant.13‘ Consequently, the cytokine release that accompanies the recovery from ischemic damage may initiate the cascade of events leading to chronic rejec-
It is possible that ischemic transplant acute tubular necro- sis resulting in a lower eventual nephron mass could contrib- ute to graft loss due to glomerular hyperfiltration. Experi- mental data indicate that decreased renal mass leads to increased single nephron glomerular filtration rate, glomer- ular sclerosis, proteinuria and h y p e r t e n ~ i 0 n . l ~ ~ This effect is supported clinically by chronic changes noted in patients with decreased renal mass due to cancer surgery.i37 Further- more, Brenner et a1 suggested that a mismatch between donor nephron mass and recipient size may be a pathogenic mechanism in chronic rejection,138.139 which is supported by the biopsy finding that chronic renal rejection is associated
tion, 133-135
with a- larger glgmerular size.140 However, recent studies have shown no correlation between renal and recipient size disparity with short-term or long-term graft survivals.141
change in gene expression in parenchymal cells. It is likely that this event reflects a pattern of response common to many forms of renal injury, possibly including rejection, and that these changes increase the immunogenicity of the kid- ney and probability of acute rejection. In turn, rejection causes injury and a new injury response. Thus, the injury response, with its cytokinehnflammatory element, forms a potential self-perpetuating cycle that could contribute to progressive renal injury, such as recurrent and chronic re- jection.
Renal injury associated with transplantation represents a clinical situation in which the reality of the biological pro- cesses triggered by injury is readily apparent. It also pre- sents physicians with a mandate for intervention to improve transplant outcomes and evaluate the general use of manip- ulations of the injury response. The potential lessons could have significance in understanding the more general rules governing the response to renal injury.
REFERENCES
1. Almond, P. S., Matas, A. J. and Canafax, D. M.: Fixed-rate reimbursement fails to cover costs for patients with delayed graR function. Pharmacotherapy, 11: 126S, 1991.
2. Almond, P. S., Troppmann, C., Escobar, F., Frey, D. J. and Matas, A. J.: Economic impact of delayed graR function. Transplant. Proc., part 2, 2 3 1304, 1991.
3. Rosenthal, J. T., Danovitch, G. M., Wilkinson, A. and Ettenger, R. B.: The high cost ofdelayed graft function in cadaveric renal transplantation. Transplantation, 51: 1115, 1991.
4. Shoskes, D. A,, Churchill, B. M., McLorie, G. A. and Khoury, A,: The impact of ischemic and immunologic factors on early graft function in oediatric renal transulantation. Transolantation. 5 0 877, 1960.
5. Weinbere, J . M.: The cell biology of ischemic renal iniury. Kidney -. - - Int., 39: 476, 1991.
6. Toback, F. G.: Regeneration atter acute tubular necrosis. Kidney Int., 41: 226, 1992.
7. Darby, J. M., Stein, K., Grenvik, A. and Stuart, S. A,: Approach to management of the heartbeating ‘brain dead’ organ donor. J.A.M.A., 261: 2222, 1989.
8. Starzl, T. E., Miller, C., Broznick, B. and Makowka. L.: An improved technique for multiple organ harvesting. Surg., Gy- nec. & Obst., 165: 343, 1987.
9. Wynen, R. M., Booster, M., Speatgens, C.. Yin, M.. van Hoof, J. P., de Boer, J. and Kootstra, G.: Long-term follow-up of transplanted non-heart-beating donor kidneys: preliminary results of a retrospective study. Transplant. Proc., part 2. 2 5 1522, 1993.
10. Parmar, M. S., Kjellstrand, C. M., Solez, K. and Halloran, P. F.: Glomerular endothelial cell detachment in paired cadaver kidney transplants: evidence that some cadaver donors have pre-existing endothelial injury. Clin. Transplant., 8: 120, 1994.
11. Levine, R. L.: Ischemia: from acidosis to oxidation. FASEB J.. 7 1242. 1993.
HYPOTHESIS THE LINK BETWEEN IN.JURY AND REJECTION
Delayed graft function and transplant acute tubular necro- sis are common and important entities that are potentially treatable or even preventable. They are morbid and costly, and increase graft loss, mainly due to rejection. Nonspecific injury to the kidney triggers a remarkably complex series of events that we termed the injury response, analogous to the highly structured events in the immune response. Injury, probably through the events in the in-jury response, can Influence the likelihood of a specific immune response. Our mouse model of ischemic injury suggests that many cytokines are induced, and pre pro epidermal growth factor mRNA is greatly decreased. A cellular infiltrate appears, as well as a
12. Green,’C. J.. Gower, J. D., Healing, G., Cotterill. L. A., Fuller, B. J. and Simpkin, S.: The importance of iron, calcium and free radicals in reperfusion injury: an overview of studies in isch- aemic rabbit kidneys. Free Radical Res. Commun., 7: 255. 1989.
13. Burke, T. J., Singh, H. and Schrier, R. W.: Calcium handling by renal tubules during oxygen deprivation injury to the kidney prior to reoxygenation. Cardiovasc. Drugs Ther., 4 1319,1990.
14. McCord, J. M.: Oxygen-derived free radicals in postischemic tissue injury. New Engl. J. Med., 312: 159, 1985.
15. Granger, D. N.: Role of xanthne oxidase and granulocytes in ischemia-reperfusion injury. Amer. J. Physiol., part 2, 255: H1269, 1988.
16. Hochachka, P. W.: Defense strategies against hypoxia and hy- pothermia. Science. 231: 234, 1986.
17. Klausner, J. M., Paterson, I. S., Kobzik. L., Rodzen, C.. Valeri, C. R., Shepro, D. and Hechtman. H. B.: Vasodilating prosta- glandins attenuate ischemic renal injury only if thromboxane is inhibited. Ann. Surg., 209: 219. 1989.
18. Chintala, M. S., Chiu, P. J., Vemulapalli. S., Watkins. R. W. and
1838 DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION
Sybertz, E. J.: Inhibition of endothelial derived relaxing factor (EDRF) aggravates ischemic acute renal failure in anesthe- tized rats. Naunyn Schmiedebergs Arch. Pharmacol., 348: 305, 1993.
19. Emami, A,, Schwartz, J. H. and Borkan, S. C.: Transient isch- emia or heat stress induces a cytoprotectant protein in rat kidney. Amer. J . Physiol., part 2, 280: F479, 1991.
20. Bonventre, J. V., Sukhatme, V. P., Bamberger, M., Ouellette, A. J. and Brown, D.: Localization of the protein product of the immediate early growth response gene, Egr-1, in the kidney after ischemia and reperfusion. Cell Regulation, 2 251, 1991.
21. Paller, M. S.: Free radical-mediated postischemic injury in renal transplantation. Renal Failure, 1 4 257, 1992.
22. Deneke, S. M. and Fanburg, B. L.: Regulation of cellular gluta- thione. h e r . J. Physiol., 257: L163, 1989.
23. Weinberg, J. M.: Glutathione and glycine in acute renal failure. Renal Failure, 14: 311, 1992.
24. Hall, T. S., Breda, M. A,, Baumgartner, W. A,, Borkon, A. M., Brawn, J., Hutchins, G. M. and Reitz, B. A.: The role of leu- kocyte depletion in reducing injury to the lung after hypother- mic ischemia. J. Curr. Surg., 44: 137, 1987.
25. Welbourn, C. R., Goldman, G., Paterson, I. S., Valeri, C. R., Shepro, D. and Hechtman, H. B.: Pathophysiology of isch- aemia reperfusion injury: central role of the neutrophil. Brit. J . Surg., 7 8 651, 1991.
26. Conger, J . D., Robinette, J . B. and Kelleher, S. P.: Nephron heterogeneity in ischemic acute renal failure. Kidney Int., 2 6 422, 1984.
27. Oken, D. E.: Acute renal failure (vasomotor nephropathy): mi- cropuncture studies of the pathogenetic mechanisms. Ann. Rev. Med., 2 6 307, 1975.
28. Hollenberg, N. K., Retik, A. B., Rosen, S. M., Murray, J . E. and Merrill, J. P.: The role of vasoconstriction in the ischemia of renal allograft rejection. Transplantation, 6 59, 1968.
29. Myers, B. D., Miller, D. C., Mehigan, J . T., Olcott, C. O., IV, Golbetz, H., Robertson, C. R., Derby, G., Spencer, R. and Friedman, S.: Nature of the renal injury following total renal ischemia in man. J . Clin. Invest., 7 3 329, 1984.
30. Conger, J. D., Falk, S. A., Yuan, B. H. and Schrier, R. W.: Atrial natriuretic peptide and dopamine in a rat model of ischemic acute renal failure. Kidney Int., 35: 1126, 1989.
31. Tanner, G. A,, Sloan, K. L. and Sophasan, S.: Effects of renal artery occlusion on kidney function in the rat. Kidney Int., 4: 377,1973.
32. Finn, W. F., Hak, L. J . and Grossman, S. H.: Protective effect of prostacyclin on postischemic acute renal failure in the rat. Kidney Int., 3 2 479, 1987.
33. Bhardwaj, R. and Moore, P. K: The effect of arginine and nitric oxide on resistance blood vessels of the perfused ra t kidney. Brit. J . Pharmacol., 97: 739, 1989.
34. Brezis, M., Heyman, S. N., Dinour, D., Epstein, F. H. and Rosen, S.: Role of nitric oxide in renal medullary oxygenation. Studies in isolated and intact rat kidneys. J. Clin. Invest., 88: 390, 1991.
35. Lieberthal, W., Wolf, E. F., Rennke, H. G., Valeri, C. R. and Levinsky, N. G.: Renal ischemia and reperfusion impair endothelium-dependent vascular relaxation. h e r . J. Physiol., part 2, 256 F894, 1989.
36. Safirstein, R., Zelent, A. Z. and Price, P. M.: Reduced renal prepro-epidermal growth factor mRNA and decreased EGF excretion in ARF. Kidney Int., 3 6 810, 1989.
37. Safirstein, R., Price, P. M., Saggi, S. J. and Harris, R. C.: Changes in gene expression after temporary renal ischemia. Kidney Int., 37: 1515, 1990.
38. Humes, D., Cieslinski, D., Coimbra, T., Messana, J. and Galvao, C.: Epidermal growth factor enhances renal tubule cell regen- eration and repair and accelerates the recovery of renal func- tion in postischemic ARF. J. Clin. Invest., 84: 1757, 1989.
39. Norman, J., Tasu, Y., Bacay, A. and Fine, L.: Epidermal growth factor accelerates functional recovery from ischaemic acute tubular necrosis in the rat: role of the EGF receptor. Clin. Sci., 78: 445, 1990.
40. Killion, D., Canfield, C., Norman, J. and Rosenthal, J. T.: Exog- enous epidermal growth factor fails to accelerate functional recovery in the autotransplanted ischemic pig kidney. J. Urol., 150 1551, 1993.
41. Ploeg, R. J . , van Bockel, J . H., Langendijk, P. T., Groenewegen, M.. van der Woude, F. J.. Persijn, G. G . , Thorogood, J. and
Hermans, J.: Effect of preservation solution on results of ca- daveric kidney transplantation. The European Multicentre Study Group. Lancet, 340: 129, 1992.
42. Wijnen, R. M., Booster, M. H., Stubenitsky, B. M., de Boer, J., Heineman, E. and Kootstra, G.: Outcome of transplantation of non-heart-beating donor kidneys. Lancet, 345: 1067, 1995.
43. &banal, 3. M., Teja, J . L., Quesada, A. and Cotorruelo, J.: Does diabetes insipidus in brain dead organ donors protect acute tubular necrosis in renal grafts? Transplant. Proc., 25: 3143, 1993.
44. Thoren, 0.: Ischemia time and time for onset of graft function after cadaveric kidney transplantation. Scand. J . Urol. Neph- rol., 3 8 33, 1976.
45. Mertes, P. M., el Abassi, K., Jaboin, Y., Burtin, P., Pinelli, G . , Carteaux, J. P., Burlet, C., Boulange, M. and Villemot, J. p.: Changes in hemodynamic and metabolic parameters following induced brain death in the pig. Transplantation, 58: 414,1994,
46. Ferguson, C. J . , Hillis, A. N., Williams, J. D., Griffin, P. J. and Salaman, J. R.: Calcium-channel blockers and other factors influencing delayed function in renal allografts. Nephrol. Di- alysis Transplant., 5: 816, 1990.
47. Canafax, D. M., Torres, A., Fryd, D. S., Heil, J. E., Strand, M. H., Ascher, N. L., Payne, W. D., Sutherland, D. E., Simmons, R. L. and Najarian, J. S.: The effects of delayed function on recipi- ents of cadaver renal allografts. A study of 158 patients ran- domized to cyclosporine or ALG-azathioprine. Transplanta- tion, 41: 177, 1986.
48. Kahan, B. D., Mickey, R., Flechner, S. M., Lorber, M. I., Wideman, C. A., Kerman, R. H., Terasaki, P. and Van Buren, C. T.: Multivariate analysis of risk factors impacting on immediate and eventual cadaver allograft survival in cyclosporine-treated recipients. Transplantation, 43: 65, 1987.
49. Halloran, P. and Aprile, M.: Factors influencing early renal function in cadaver kidney transplants. A case-control study, Transplantation, 45: 122, 1988.
50. Merkus, J. W., Hoitsma, A. J . and Koene, R. A,: Detrimental effect of acute renal failure on the survival of renal allografts: influence of total ischaemia time and anastomosis time. Neph- rol. Dialysis Transplant., 6 881, 1991.
51. Halloran, P. F. and Shoskes, D. A.: Early transplant nonfunc- tion-influence on ultimate graft survival and function. In: Acute Renal Failure: Diagnosis, Treatment and Prevention. Edited by K. Solez and L.C. Racusen. New York: Marcel Dekkar, Inc., p. 387, 1991.
52. Belzer, F. 0. and Southard, J. H.: Principles of solid-organ pres- ervation by cold storage. Transplantation, 45: 673, 1988.
53. Halloran, P. and Aprile, M.: A randomized prospective trial of cold storage versus pulsatile perfusion for cadaver kidney preservation. Transplantation, 43: 827, 1987.
54. Merion, R. M., Oh, H. K., Port, F. K., Toledo-Pereyra, L. H. and Turcotte, J. G.: A prospective controlled trial of cold-storage versus machine-perfusion preservation in cadaveric renal transplantation. Transplantation, 50: 230, 1990.
55. Tesi, J., Elkhammas, E. A,, Davies, E. A,, Henry, M. L. and Ferguson, R. M.: Pulsatile kidney perfusion for preservation and evaluation: use of high-risk kidney donors to expand the donor pool. Transplant. Proc., 25: 3099, 1993.
56. Halloran, P. F., Wadgymar, A., Ritchie, S., Falk, J., Solez, K. and Srinivasa, N. S.: The significance of the anti-class I antibody response. 1. Clinical and pathologic features of anti-class I-mediated rejection. Transplantation, 49: 85, 1990.
57. Dawidson, I. J., Sandor, 2. F., Coorpender, L., Palmer, B., Peters, P., Lu, C., Sagalowsky, A,, Risser, R. and Willms, C.: Intraop- erative albumin administration affects the outcome of cadaver renal transplantation. Transplantation, 53: 774, 1992.
58. Dawidson, I. J . and Ar’Rajab, A,: Perioperative fluid and drug therapy during cadaver kidney transplantation. Clin. Trans- plants, p. 267, 1992.
59. Tiggeler, R. G., Berden, J. H., Hoitsma, A. J . and Koene, R. A.: Prevention of acute tubular necrosis in cadaveric kidney trans- plantation by the combined use of mannitol and moderate hydration. Ann. Surg., 201: 246, 1985.
60. Lauzurica. R., Teixido, J., Serra, A,, Torguet, P., Bonet, J., Bonal, J., Borras, M., Romero, R. and Caralps, A,: Hydration and mannitol reduce the need for dialysis in cadaveric kidney transplant recipients treated with CyA. Transplant. Proc., 24 46, 1992.
61. Lachance, S. L. and Barry, J. M.: Effect of furosemide on dialysis
1839 DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION
requirement following cadaveric kidney transplantation, J. Urol., 133: 950, 1985.
62. Neumayer, H. H., Kunzendorf, U. and Schreiber, M.: Protective effects of calcium antagonists in human renal transplantation. Kidney Int., suppl., 3 6 S87, 1992.
63. Suthanthiran, M., Haschemeyer, R. H., Riggio, R. R., Adubor, C., Friedman, G. S., Cheigh, J. S., Wang, J. C., Fotino, M., Stubenbord, W. T. and Saal, S. D.: Excellent outcome with a calcium channel blocker-supplemented immunosuppressive regimen in cadaveric renal transplantation. A potential strat- egy to avoid antibody induction protocols. Transplantation, 55: 1008, 1993.
64. Nyberg, G., Haljamae, U., Herlitz, H., Norden, G. and Blohme, I.: Early renal graft function in recipients treated with the cal- cium channel blocker felodipine. Scand. J . Urol. Nephrol., 2 8 17, 1994.
65. Pollak, R., Andrisevic, J. H., Maddux, M. S., Gruber, S. A. and Paller, M. S.: A randomized double-blind trial of the use of human recombinant superoxide dismutase in renal transplan- tation. Transplantation, 5 5 57, 1993.
66. Land, W., Schneeberger, H., Schleibner, S., Illner, W. D., Abendroth, D., Rutili, G., Arfors, K. E. and Messmer, K.: The beneficial effect of human recombinant superoxide dismutase on acute and chronic rejection events in recipients of cadaveric renal transplants. Transplantation, 57: 211, 1994.
67. Forth, H. J. , Rebmann, U., Heynemann, H., Schabel, J., Pauer, H. D., Mehlhorn, G., Scharf, R. and Mest, H. J.: The improve- ment of the tolerance of the kidney for ischemia with the prostacyclin analog iloprost. 2. Exp. Chir. Transplant. Kun- stliche Organe, 23: 79, 1990.
68. Adams, M. B.: Enisoprost in renal transplantation. The Eniso- prost Renal Transplant Study Group. Transplantation, 5 3 338, 1992.
69. Gianello, P., Squifflet, J. P., Carlier, M., Lambotte, L., Ketelslegers, J. M. and Alexandre, G . P.: Atrial natriuretic factor: a protective role after acute renal ischemia? Is there room for it in kidney transplantation? Transplant. Int., 3: 41, 1990.
70. Lewis, R., Katz, S., Van Buren, C., Kerman, R. and Kahan, B.: Mechanisms and amelioration of acute renal allograft failure in the cyclosporine era. Renal Failure, 1 4 267, 1992.
71. Stanley, 3. J., Coldblum, J. R., Frank, T. S., Zelenock, G. B. and DAlecy, L. G.: Attenuation of renal reperfusion injury in rats by the 21-aminosteroid U74006F. J. Vasc. Surg., 17: 685,1993.
72. Jordan, M. L., Cook, G . T. and Cardella, C. J.: Ten years of experience with vascular complications in renal transplanta- tion. J. Urol., 128 689, 1982.
73. Shoskes, D. A,, Hanbury, D., Cranston, D. and Moms, P. J.: Urological complications in 1,000 consecutive renal transplant recipients. J. Urol., 153 18, 1995.
74. Smith. T. P., Hunter, D. W., Letourneau, J. G., Cragg, A. H., Darcy, M. D., Castaneda-Zuniga, W. R. and Amplatz, K.: Urine leaks after renal transplantation: value of percutaneous pye- lography and drainage for diagnosis and treatment. AJR, 151: 511, 1988.
75. Cullmann, H. J. and Prosinger, M.: Necrosis of the allograft ureter-evaluation of different examination methods in early diagnosis. Urol. Int., 4 5 164, 1990.
76. Rigsby, C. M., Burns, P. N., Weltin, G . G., Chen, B., Bia, M. and Taylor, K. J.: Doppler signal quantitation in renal allografts: comparison in normal and rejecting transplants, with patho- logic correlation. Radiology, 162: 39, 1987.
77. Pelling, M. and Dubbins, P. A,: Doppler and color Doppler im- aging in acute transplant failure. J. Clin. Ultrasound, 2 0 507, 1992.
78. Delaney, V., Ling, B. N., Campbell, W. G., Bourke, J. E., Fekete, P. S., OBrien, D. P., 111, Taylor, A. T. and Whelchel, J. D.: Comparison of fine-needle aspiration biopsy, Doppler ultra- sound, and radionuclide scintigraphy in the diagnosis of acute allograft dysfunction in renal transplant recipients: sensitiv- ity, specificity, and cost analysis. Nephron, 63: 263, 1993.
79. Shanahan, W. S., Klingensmith, W. C., 111 and Weil, R., 111: 99mTc-DTPA renal studies for acute tubular necrosis: speci- ficity of dissociation between perfision and clearance. AJR, 136: 249, 1981.
80. Solez, K., McGraw, D. J., Beschorner, W. E. and Burdick, J. F.: Pathology of "acute tubular necrosis" and acute rejection: ob- servations on early systematic renal transplant biopsies. In
Kidney Transplant Rejection. Diagnosis and Treatment. Ed- ited by G. M. Williams, J. F. Burdick and K. Solez. New York: Marcel Dekker, Inc., chapt. 10, pp. 207-224, 1986.
81. Kadieva, V. S., Friedman, L., Margolius, L. P., Jackson, S. A. and Morrell, D. F.: The effect of dopamine on graft function in patients undergoing renal transplantation. Anesth. Anal., 7 6 362, 1993.
82. Novick, A. C., Hwei, H. H., Steinmuller, D., Streem, S. B.. Cunningham, R. J., Steinhilber, D., Goormastic, M. and Buszta, C.: Detrimental effect of cyclosporine on initial func- tion of cadaver renal allografts following extended preser- vation. Results of a randomized prospective study. Trans- plantation, 42: 154, 1986.
83. Howard, R. J., Pfaff, W. W., Brunson, M. E., Ramos, E. L., Peterson, J. C., Croker, B. P., Scornik, J. C. , Pams, C. J. and Fennell, R. S.: Delayed graft function is associated with an increased incidence of occult rejection and results in poorer graft survival. Transplant. Proc., part 2, 2 5 884, 1993.
84. Whittaker, J. R., Veith, F. J. and Soberman, R.: The fate of the renal transplant with delayed function. Surg., Gynec. & Obst., 136 919, 1973.
85. Williams, G. M., White, H. J. and Hume, D. M.: Factors influ- encing the long term functional success rate of human renal allografts. Transplantation, suppl., 5 837, 1967.
86. Cho, S. I., Olsson, C. A., Bradley, J . W. and Nasbeth, D. C.: Regional program for kidney preservation and transplantation in New England. h e r . J. Surg., 131: 428. 1976.
87. Opelz, G., Sasaki, N. and Terasaki, P. I.: Prediction of long-term kidney transplant survival rates by monitoring early graft function and clinical grades. Transplantation, 2 5 212, 1978.
88. McDonald, J. C., Vaughn, W., Filo, R. S., Picon, G . M., Niblack, G., Spees, E. K. and Williams, G. M.: Cadaver donor renal transplantation by centers of the Southeastern Organ Pro- curement Foundation. Ann. Surg., 193 1, 1981.
89. Sanfilippo, F., Vaughn, W. K.. Spees, E. K. and Lucas, B. A.: The detrimental effects of delayed graft function in cadaver donor renal transplantation. Transplantation, 3 8 643, 1984.
90. Mendez-Picon, G., Posner, M. P., McGeorge, M. B., Baquero, A., Goldman, M. H., Monahanakumar. T. and Lee, H. M.: The effect of delayed function on long term survival of renal al- lografts. Surg., Gynec. & Obst., 161: 351, 1985.
91. Barry, J. M., Norman, D., Fuchs, E. F.. Fischer. S. and Bennett, W. M.: Influence of acute tubular necrosis on first cadaver kidney transplant function. J. Urol., 132: 234, 1984.
92. Rocher, L. L., Landis, C., Dafoe, D. C.. Keyserling. C.. Swartz, R. D. and Campbell, D. A., Jr . : The long-term deleterious effect of delayed graft function in cyclosporine-treated renal allograft recipients. Transplant. Proc., part 3, 1 9 2093, 1987.
93. Belitsky, P., MacDonald, A. S., Gajewski, J., Boudreau, J., Bitter-Suermann, H. and Cohen. A.: Significance of delayed function in cyclosporine-treated cadaver kidney transplants. Transplant. Proc., 1 9 2096, 1987.
94. Sumrani, N. B., Miles, A. M.. Daskalakis, P., Hong, J. H.. Markell, M. S., Friedman, E. A. and Sommer, B. G.: Intermediate-term outcome of renal retransplants in the cy- closporine era. ASAIO J., 3 9 47, 1993.
95. Bauma, W. D., Tang, I. Y., Maddux, M. S., Veremis, S. A,, Pollak. R. and Mozes, M. F.: Delayed graft function following cadaver renal transplantation in the cyclosporine era: analysis of acute rejection and graft survival. Transplant. Proc., part 2, 21: 1276, 1989.
96. Halloran, P. F., Aprile, M. A,, Farewell, V., Ludwin, D., Smith, E. K., Tsai, S. Y., Bear, R. A., Cole. E. H., Fenton. S. S. and Cattran, D. C.: Early function as the principal correlate of graft survival. A multivariate analvsis of 200 cadaveric renal transplants treated with a protocol incorporating antilympho- cyte globulin and cyclosporine. Transplantation, 4 6 223, 1988.
97. Churchill, B. M., Mchrie. G. A.. Williot, P. and Merguerian, P. A.: Influence of early function on long-term pediatric cadav- eric renal allograft survival. J. Urol.. 143: 326, 1990.
98. Cecka, J. M., Cho, Y. W. and Terasaki. P. I.: Analyses of the UNOS Scientific Renal Transplant Registry at three years- early events affecting transplant success. Transplantation. 53: 59. 1992.
99. Kjellstrand, C. M., Casali, R. E., Simmons, R. L.. Shideman, J. R., Buselmeier, T. J . and Najarian, J. S.: Etiology and prognosis in acute post-transplant renal failure. Amer. J. Med., 61: 190, 1976.
1840 DELAYED GRAFT FUNCTION IN RENAL TRANSPLANTATION
100. Brophy, D., Najarian, J. S. and Kjellstrand, C. M.: Acute tubu- lar necrosis after renal transplantation. Transplantation, 29: 245, 1980.
101. Heil, J., Sutherland, E. R.. Fryd, D. S., Ascher, N. L., Simmons, R. L. and Najarian, J. S.: Acute tubular necrosis of cadaver renal allografts does not correlate with organ sharing or pres- ervation time but portends a poorer prognosis for long-term graR survival. Transplant. Proc., 1 6 270, 1984.
102. Cacciarelli, T., Sumrani, N., Delaney, V., Hong, J. H., DiBenedetto, A. and Sommer, B. G.: The influence of delayed renal allograft function on long-term outcome in the cyclospo- rine era. Clin. Nephrol., 3 9 335, 1993.
103. Yokoyama, I., Uchica, K., Kobayashi, T., Tominaga, Y., Orihara, A. and Takagi, H.: Effect of prolonged delayed graft function on long-term graft outcome in cadaveric kidney trans- plantation. Clin. Transplant., 8 101, 1994.
104. Sanfilippo, F., Vaughn, W. K., LeFor, W. N. and Spees, E. K.: Multivariate analysis of risk factors in cadaver donor kidney transplantation. Transplantation, 42: 28, 1986.
105. Paramasivan, 0. N., Griffin, P. J., Ross, W. B. and Salaman, J. R.: The effect of acute tubular necrosis on cyclosporine-treated hdney transplants. Transplant. Proc., part 3 , l S 2085, 1987.
106. McMullin, N. D., Koffman, C. G., Rigdon, S. P., Haycock, G., Chantler, C. and Bewick, M.: The negative influence of delayed renal allograft function on longer-term graft survival in a pediatric population. J. Ped. Surg., 2 9 66, 1994.
107. A randomized clinical trial of cyclosporine in cadaveric renal transplantation. Analysis at three years. The Canadian Mul- ticentre Transplant Study Group.-New Engl. J. Med., 314: 1219, 1986.
108. Lim, E. C. and Terasaku, P. I.: Early graft function. Clin. Trans- plants, pp. 401-407, 1991.
109. Cecka, J. M. and Terasaki, P. I.: The UNOS Scientific Renal Transplant Registry-1990. Clin. Transplants, pp. 1-10,1990.
110. Najarian, J. S., Gillingham, K. J., Sutherland, D. E., Reinsmoen, N. L., Payne, W. D. and Matas, A. J.: The impact of the quality of initial graft function on cadaver kidney trans- plants. Transplantation, 57: 812, 1994.
111. Halloran, P. F., Schlaut, J., Solez, K. and Srinivasa, N. S.: The significance of the anti-class I response. 11. Clinical and patho- logic features of renal transplants with anti-class I-like anti- body. Transplantation, 53: 550, 1992.
112. Gulanikar, A. C., MacDonald, A. S., Sungurtekin, U. and Belitsky, P.: The incidence and impact of early rejection epi- sodes on graft outcome in recipients of first cadaver kidney transplants. Transplantation, 53: 323, 1992.
113. Ferguson, R.: Acute rejection episodes-best predictor of long- term primary cadaveric renal transplant survival. Clin. Trans- plant., part 2, 8: 328, 1994.
114. Nicholson, M. L., Horsburgh, T., Edwards, C. M., Morgan, J. D. T., Veitch, P. S. and Bell, P. R. F.: Relative influence of delayed graft function and acute rejection renal transplant survival. Abstracts of the British Transplantation Society, p. 41, 1994.
115. Orosz, C. G.: Endothelial activation and chronic allograft rejec- tion. Clin. Transplant., part 2, 8: 299, 1994.
116. Shoskes, D. A. and Wood, K. J.: Indirect presentation of MHC antigens in transplantation. Immunol. Today, 1 5 32, 1994.
117. Halloran, P. F. and Madrenas, J.: Regulation ofMHC transcrip- tion. Transplantation, 5 0 725, 1990.
118. Milton, A. D. and Fabre, J. W.: Massive induction of donor-type class I and class I1 histocompatibility complex antigens in rejecting cardiac allografts in the rat. J. Exp. Med., 161: 98, 1985.
119. Fuggle, S. V., McWhinnie, D. L. and Moms, P. J.: Precise specificity of induced tubular HLA-class I1 antigens in renal allografts. Transplantation, 44: 214, 1987.
120. Bekkhoucha, F., Naquet, P., Pierres, A., Marchetto, S. and Plerres, M.: Efficiency of antigen presentation to T cell clones by (B cell x B cell lymphoma) hybridomas correlates quanti- tatively with cell surface ia antigen expression. Eur. J. Immu- nol., 14: 807, 1984.
121. Shoskes, D. A., Parfrey, N. A. and Halloran, P. F.: Increased major histocompatibility complex antigen expression in uni- lateral ischemic acute tubular necrosis in the mouse. Trans- plantation, 4 9 201, 1990.
122. Shoskes, D. A. and Halloran, P. F.: Ischemic injury induces altered MHC gene expression in kidney, by an interferon-
gamma-dependent pathway. Transplant. Proc., 2 3 599, 1991, 123. Goes, N., Urmson, J., Ramassar, V. and Halloran, P. F.: Isch-
emic acute tubular necrosis induces an extensive local cyto- kine response. Evidence for induction of interferon-gamma, transforming growth factor-beta 1, granuhfle-macrophage colony-stimulating factor, interleukin-2, and interleukin-10. Transplantation, 5 9 565,1995.
124. Solez, K., McGraw, D. J., Beschorner, W. E., Kone, B. C., Racusen, L. C., Whelton, A. and Burdick, J. F.: Reflections on use of the renal biopsy as the "gold standard" in distinguishing transplant rejection from cyclosporine nephrotoxicity. Trans- plant. Proc., suppl. 1, 17: 123, 1985.
125. Shackleton. C. R., Ettinger. S. L., McLoughlin, M. G., Scudamore, C. H., Miller, R. R. and Keown, P. A.: Effect of recovery from ischemic injury on class I and class I1 MHC antigen expression. Transplantation, 4 9 641, 1990.
126. Compeau, C. G., Ma, J., DeCampos, K. N., Waddell, T. K., Brisseau, G. F., Slutsky, A. S. and Rotstein, 0. D.: In situ ischemia and hypoxia enhance alveolar macrophage tissue factor expression. Amer. J. Respiratory Cell Molec. Biol., 11: 446, 1994.
127. Wakabayashi, H., Miyauchi, A., Karasawa, Y., Hamamoto, I., Maeba, T. and Tanaka, S.: Effect of warm ischemia and reper- fusion injury on inducing major histocompatibility complex antigens on hepatocytes and nonparenchymal cells in the rat liver. Transplant. Proc., 2 6 3205, 1993.
128. Goes, N., Urmson, J., Ramassar, V., Vincent, D. and Halloran, P. F.: Effect of rh insulin like growth factor I on the inflam- matory response to acute renal injury. J. Amer. SOC. Nephrol., in press.
129. Ibrahim, M. A., Chain, B. M. and Katz, D. R.: The injured cell: the role of the dendritic cell system as a sentinel receptor pathway. Immunol. Today, 1 6 181, 1995.
130. Shoskes, D. A,, Hodge, E. E., Goormastic, M., Goldfarb, D. A. and Novick, A. C.: HLA matching determines susceptibility to harmful effects of delayed graft function in renal transplant recipients. Transplant. Proc., 21: 1068, 1995.
131. Solez, K.: International standardization of criteria for histologic diagnosis of chronic rejection in renal allografts. Clin. Trans- plant., part 2, 8: 345, 1994.
132. Tullius, S. G., Hancock, W. W., Heemann, U., Azuma, H. and Tilney, N. L.: Reversibility of chronic renal allograft rejection. Critical effect of time after transplantation suggests both host immune dependent and independent phases of progressive injury. Transplantation, 5 8 93, 1994.
133. Yilmaz, S., Paavonen, T. and Hayry, P.: Chronic rejection of rat renal allografts. 11. The impact of prolonged ischemia time on transplant histology. Transplantation, 5 3 823, 1992.
134. Clinton, S. K. and Libby, P.: Cytokines and growth factors in atherogenesis. Arch. Path. Lab. Med., 116: 1292, 1992.
135. Yamamoto, T., Noble, N. A,, Miller, D. E. and Border, W. A,: Sustained expression of TGF-beta 1 underlies development of progressive kidney fibrosis. Kidney Int., 45: 916, 1994.
136. Hostetter, T. H., Olson, J. L., Rennke, H. G., Venkatachalam, M. A. and Brenner, B. M.: Hyperfiltration in remnant nephrons: a potentially adverse response to renal ablation. Amer. J. Physiol., 241: F85, 1981.
137. Novick, A. C., Gephardt, G., Guz, B., Steinmuller, D. and Tubbs, R. R.: Long-term follow-up after partial removal of a solitary kidney. New Engl. J. Med., 325: 1058, 1991.
138. Brenner, B. M., Cohen, R. A. and Milford, E. L.: In renal transplantation, one size may not fit all. J . h e r . SOC. Neph- rol., 3: 162, 1992.
139. Brenner, B. M. and Milford, E. L.: Nephron underdosing: a programmed cause of chronic renal allograft failure. Amer. J. Kidney Dis., suppl. 2, 21: 66, 1993.
140. Bamentos, A,, Portoles, J., Herrero, J. A., Torralbo, A,, Prats, D., Gutierrez-Millet, V. and Blanco, J.: Gloinerular hyperfil- tration as a nonimmunologic mechanism of progression of chronic renal rejection. Transplantation, 57: 753, 1994.
141. Gaston, R. S., Hudson, S. L., Julian, B. A., Laskow, D. A., Deierhoi, M. H., Sanders, C. E.. Phillips, M. G., Diethelm. A. G. and Curtis, J. J.: Impact o f donorhecipient size matching on outcomes in renal transplantation. Transplantation, 61: 383, 1996.









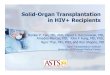













![Wednesday 19 November2014 · Haplo 48 46 50 42 42 21 Haploidentical hematopoietic cell transplantation compared to transplantation from other graft sources 2005[53] Haplo‐ALL 74](https://img.pdfslide.us/doc/110x75/5f261b354659702f973220d1/wednesday-19-november2014-haplo-48-46-50-42-42-21-haploidentical-hematopoietic-cell.jpg)





