Embed Size (px)
Citation preview

Investigating the potential risk factors related to residual infections of Schistosoma japonicum in the
endemic areas of Bohol, Philippines
Clarence Londres de Guzman
This scholarly paper has been submitted in partial fulfillment of the requirements for the Degree of Master of Science (M.S.) in Global Health at Georgetown University
January 18, 2016

TABLE OF CONTENTS
ACKNOWLEDGEMENTS ........................................................................................................ iii
ACRONYMS AND ABBREVIATIONS .................................................................................... iv ABSTRACT ................................................................................................................................... v
INTRODUCTION ......................................................................................................................... 1 BACKGROUND & SIGNIFICANCE ........................................................................................ 2
Schistosomiasis in Bohol ........................................................................................................................ 2 Demographic and Socioeconomic Factors ............................................................................................ 4 Health Infrastructure and Personnel .................................................................................................... 4 Disease Status .......................................................................................................................................... 5
RESEARCH QUESTION ............................................................................................................ 5 Research Objectives ................................................................................................................................ 6
LITERATURE REVIEW ............................................................................................................ 7 Overview of schistosoma parasites and intermediate snail vectors ................................................... 7 History of schistosomiasis control in the Philippines .......................................................................... 8 The Health System: National & Local Levels .................................................................................... 10 DOH’s 4-Pronged Approach ............................................................................................................... 12
METHODS .................................................................................................................................. 13 Design Overview ................................................................................................................................... 13 Data: Context, Population, and Sampling .......................................................................................... 14 Dependent Variable .............................................................................................................................. 15 Key Independent Variables ................................................................................................................. 16 Basic Conceptual Framework ............................................................................................................. 16 Estimation Approach & Data Analysis .............................................................................................. 16 Procedures ............................................................................................................................................. 17
RESULTS .................................................................................................................................... 19
DISCUSSION .............................................................................................................................. 26 Mass Drug Administration .................................................................................................................. 26 Vector Control ...................................................................................................................................... 28 Environmental Sanitation .................................................................................................................... 30 Safe Water Supplies .............................................................................................................................. 31 Advocacy and Health Education ......................................................................................................... 33 Other Determinants .............................................................................................................................. 34
CONCLUSION ........................................................................................................................... 36 Design Critique & Limitations ............................................................................................................ 36 Current Needs & Future Outlook ....................................................................................................... 36 Recommendations for Future Study & Final Remarks .................................................................... 37
REFERENCES ............................................................................................................................ 39
APPENDIX .................................................................................................................................. 42

iii
ACKNOWLEDGEMENTS
This research project is part of the National Schistosomiasis Control and Elimination Program’s
(NSCEP) routine monitoring and evaluation activity for schistosomiasis in the province of
Bohol. The Malaria, other Vectorborne and Parasitic Diseases (MVP) Unit of the World Health
Organization Representative Office in the Philippines has collaborated with the Department of
Health to plan and successfully carry out this project.
The following individuals and their respective staff have provided great support and significant
contributions towards the completion of this study:
Team Leader: Dr. Winston A. Palasi, NSCEP
Team Members from the Philippines
Dr. Joanri T. Riveral and Staff, Regional Health Office, Region VII
Dr. Reymoses A. Cabagnot and Staff, Provincial Health Office, Bohol
Dr. Francisco Ngoboc and Staff, Municipal Health Office, Talibon
Dr. Analita N. Auza and Staff, Municipal Health Office, Trinidad
NDP Nurses Talibon
NDP Nurses Trinidad
Department of Education Representatives
Department of Agriculture Representatives
WHO
Dr. Zaixing Zhang, WHO Philippines Country Office, MVP Unit
Volunteer
Ragine Valente, Municipal Nurse, Cavinti, Laguna

iv
ACRONYMS AND ABBREVIATIONS
BBC Behavior Change Communication
BHW Barangay (Village) Health Workers
BHS Barangay Health Station
DALYs Disability-Adjusted Life Years
DMO Development Management Officer
DOH Department of Health
ELISA Enzyme Linked Immunosorbent Assay
EPG Eggs Per Gram of feces
IEC Information, Education, Communication
IRA Internal Revenue Allotment
KAP Knowledge, Attitude and Practice
LGU Local Government Unit
M&E Monitoring and Evaluation
MDA Mass Drug Administration
MHO Municipal Health Office(r)
MSI Municipal Sanitary Inspector
MVP Malaria, other Vectorborne and Parasitic diseases unit
NIA National Irrigation Administration
NDP Nurse Deployment Program
NSCEP National Schistosomiasis Control and Elimination Program
PHN Public Health Nurse
PHO Provincial Health Office(r)
PPE Personal Protective Equipment
PSI Provincial Sanitation Inspector
RHM Rural Health Midwife
RHO Regional Health Office
RHU Rural Health Unit
WHO World Health Organization

v
ABSTRACT
The province of Bohol in the Philippines’ Region VII has had two endemic areas for
schistosomiasis. However, recent national surveys and reports have suggested that those two
municipalities, Talibon and Trinidad, are near elimination levels for the disease. According to a
2009-2014 Sentinel Surveillance Report, Bohol has consistently reported virtually zero cases of
active or heavy infections for schistosomiasis.15 With a prevalence rate of less than 1%, Bohol
has essentially reached the category of elimination level. In addition, a recent snail survey
conducted in 2013 by the University of the Philippines, Los Baños research team has indicated
zero infection rates for the known intermediate hosts.10 Such findings corroborate the province’s
asserted status of having eliminated the disease as a public health concern. However, a more
recent assessment by Belizario, et al. (2015)16 revealed that there is still a significant amount of
residual infections for schistosomiasis in the province.
This project documents and examines the current strategies, particularly the major public
health interventions and programs that have contributed to the reduced prevalence rates of
schistosomiasis in the region over the last five years. The main objective of this study, which
entails a qualitative research component, is to better assess the validity of the aforementioned
surveillance reports. Furthermore, through a quantitative research approach, and given the
persistent presence of residual infections, this paper aims to provide verifiable evidence and
specific clues for future recommendations on elimination and control efforts. A nested case-
control study design is used to determine the relationship between risk factors and residual
infections of schistosomiasis in Bohol. The results indicate a validation of the integrative multi-
component approach currently being implemented in the province, with an emphasis being
placed on access to potable water, sanitation infrastructure, animal vector control, and health
education in schools.

1
INTRODUCTION
Schistosomiasis, also known as bilharzia, is a
parasitic disease that currently infects over
200 million people worldwide, resulting in the
loss of approximately 25 million disability-
adjusted life years (DALYs).1, 2 Although it
has a relatively low mortality rate, with
estimates ranging from as low as 10,000 and
up to 200,000 deaths annually, it ranks only
second to malaria in the number of
individuals infected and at risk for the
disease.3 It remains a significant public health
concern in 78 countries, with endemicity
established in regions of Africa, East and
Southeast Asia, the Pacific Islands, Brazil,
and the Caribbean Islands. Among those, the
disease inflicts the heaviest burden in Sub-
Saharan Africa, accounting for roughly 77%
of the total number of DALYs globally.4, 5
The World Health Organization classifies
schistosomiasis as “a disease of poverty that
leads to chronic ill-health.” 6 Infections in
humans elicit various symptoms, depending
on the severity and developmental stage of the
disease. This may include cognitive disability
in children, nutrient and energy deficiencies,
as well as liver fibrosis.4 The presence of
worms, compounded with reactions to the
eggs produced by adult female worms, comes
with considerable immunologic and energetic
consequences.4 As a result, the human host
experiences an array of functional deficits.
The individual’s immune system, duration of
disease pathogenesis, infection intensity, and
location of egg deposition in the body are
some of the major factors that determine the
severity of the disease.1, 4 On a population
level, researchers typically measure the
severity of the disease by looking at the
prevalence, intensity (mean EPG in feces),
and incidence in a given year.4 These metrics
are then integrated and correlated to estimate
disease transmission and contamination
potential in a given population or area.
Although prevalence and intensity of
infection usually vary with age, its general
pattern shows more intense infections and
higher prevalence rates as age increases up to
the teenage years, after which these rates
begin to decline.4, 6
There are five known blood fluke species of
the genus Schistosoma that cause the disease
in humans: S. mansoni, S. japonicum, S.
mekongi, S. intercalatum, and S.
haematobium. For endemic areas where S.
japonicum and S. mekongi are found, zoonotic
transmission makes control measures
especially even more challenging.1 S.
japonicum is mainly endemic in Asian

2
countries including China, Indonesia, and the
Philippines. In the Philippines, the disease is
currently endemic in 12 regions, 28
provinces, 14 cities, 203 municipalities and
1,593 barangays.10, 11 This places more than
12 million people at risk for the disease, of
which approximately 2.5 million are directly
exposed.10, 12 The Philippine Department of
Health’s Disease Prevention and Control
Bureau established the National
Schistosomiasis Control and Elimination
Program (NSCEP) in order to address this
issue. The program has been working closely
with the World Health Organization to
formulate public health strategies, implement
effective interventions, and develop technical
guidelines and tools for its control and
successive elimination in the future.
When considering the most effective
measures for disease prevention and control,
studies have shown that the optimal approach
is to break the S. japonicum lifecycle through
a multi-component integrated control.1 In
essence, this scholarly paper is a case study
that aims to validate such claim by examining
the major contributing factors to the
successful development of disease control and
elimination currently and notably taking place
in the province of Bohol, Philippines. By
designing and conducting an investigation
regarding the potential risk factors related to
residual infections of the disease in the
province, its main purpose is to provide
important clues and lessons for future
directions on how to effectively control and
eliminate schistosomiasis in other parts and
even more highly endemic areas of the
Philippines.
BACKGROUND & SIGNIFICANCE
Schistosomiasis in Bohol
Bohol is an island province located in the
country’s Region VII group of islands. (See
map: Appendix, Figure 2A) Schistosomiasis
is considered endemic in 2 of Bohol’s 47
municipalities, namely Talibon and Trinidad.
The two adjacent municipalities are located
on the northeastern coast of the island.
Within each municipality, there are four
barangays (the smallest administrative
division in the country) where schistosomiasis
is endemic.
Talibon is a 1st class income municipality
with a population of 64,761. It has a total
land are of approximately 22,400 hectares and
is consisted of 25 barangays, 8 of which are

3
islands.17 Its major industries include farming,
fishing, cottage industries, mining, and auto
repair shop. Its major products include rice,
fish, corn, seaweeds, copra, hat and mat.17
The four schistosomiasis-endemic barangays
are San Agustin, San Carlos, San Jose, and
San Roque. (See map: Appendix, Figure 2B)
Trinidad is a 3rd class income municipality
with an estimated population of 30,104.18 It
has a total land area of 15,211 hectares and is
consisted of 20 barangays.18 Like Talibon, it
is considered an agricultural community
where farming is the predominant occupation.
The four schistosomiasis-endemic barangays
are Kinan-oan, Mabuhay Cabiguhan, San
Vicente, and Santo Tomas. (See map:
Appendix, Figure 2C)
Since 1988, the efforts have been focused on
the eight endemic barangays of the two
municipalities. The Department of Health
Regional Office (Region VII) initially
established a Schistosomiasis Control Team
Office to oversee both municipalities. The
advantage of being geographic neighbors
allowed Talibon and Trinidad to collaborate
and integrate their meetings, activities and
plans of action to address their common
health problem.19 As a result, it fostered a
symbiotic relationship between the two
municipalities that strengthened their efforts
and encouraged inter-communal development
projects to combat schistosomiasis. Activities
such as active case finding through stool
collection from the general population of the
endemic barangays and treatment of positive
cases were conducted on a regular basis.19
Moreover, quarterly surveys of snail site
colonies were done and when necessary,
clearing and mollusciciding activities were
carried out. Continuous sanitary toilet
construction and advocacies on toilet
utilization were also prioritized, especially at
the local barangay levels. Many of such
health promotional campaigns were
concentrated in public schools of the endemic
barangays, in full coordination with the
Department of Education.20
After 2008, however, with the national
implementation of Mass Drug Administration
(MDA) for praziquantel, active case finding
was no longer practiced. Patients from
endemic barangays sought consultations at the
RHUs for examinations.18 Specifically, a
medical technologist, either locally trained or
as assigned by the MHO (e.g. a ‘visiting’
med-tech), would perform a parasitological
test, which is a stool exam via a Kato-Katz
technique, and the subsequent diagnosis for
schistosomiasis. MDA to schoolchildren in

4
the endemic barangays was initiated in 2009
and annually until 2013. Due to a
miscommunication, the two municipalities
had assumed that the protocol for MDA as set
by the national Department of Health was to
complete a consecutive 5-year period of
implementation.19, 20 Thus, MDA was not
carried out in 2014. With further clarification
and instruction from DOH, MDA was deemed
mandatory until a complete assessment and
comprehensive evaluation of the endemic
areas proved otherwise. As such, even with
already low prevalence rates and incidence
for schistosomiasis, both Talibon and
Trinidad resumed MDA activities in 2015.
Demographic and Socioeconomic Factors
Across all endemic barangays, the percentage
of school-age children (6-16 years old)
account, on average, for about 20% of the
total population.17, 18 This is currently the
target population for MDA in the two
municipalities, since they are considered
among the most at-risk groups in the
population for schistosomiasis. Farmers and
fishermen are also among those at-risk, and
they constitute approximately 20-30% of the
population in Talibon and Trinidad.17, 18
Those are significant numbers when
considering the economic impact and burden
of the disease. The main source of income is
from the agricultural sector and it places a
huge financial burden on the communities if
those workers are incapacitated due to health
problems. A study in Cambodia has found
that the return investment for each dollar
invested for the schistosomiasis control
program yields US$ 3.84, while the cost per
death avoided amounts to US$ 6,531, a hefty
sum in comparison to cost-effective public
health interventions that the government
could potentially invest in.2
Health Infrastructure and Personnel There is currently one provincial hospital
(Garcia Memorial Provincial Hospital) in
Talibon that serves the surrounding
municipalities in the region. Both Talibon
and Trinidad have a Municipal Health Center,
supervised by the MHO. There are 26
barangay health stations in Talibon and 20 in
Trinidad, both of which employ municipal
nurses (3-5 per RHU) and midwives (1 per
barangay).17, 18 For each RHU, there is one
public doctor, one medical technologist (or
microscopist), one sanitary inspector, and a
number of barangay health workers (BHWs)
assigned in each barangay. The Nurse
Deployment Program (NDP) has provided

5
about 10 nurses per RHU, and function under
the direction of the MHOs.17, 18
Disease Status
To date, schistosomiasis is still considered
endemic in the two municipalities. However,
in Trinidad, no human cases have been
recorded since 2007. Talibon on the other
hand, reported two consultation cases in 2014
that have histories of schistosomiasis from
Mindanao, the Philippines southern group of
islands wherein schistosomiasis remains the
most heavily endemic. After a series of
diagnostic tests, only one was found to still be
positive for the disease and was immediately
referred for treatment. The other patient
tested negative via Kato-Katz and was given a
single dose of praziquantel. In 2015, another
consultation case indicated a history of
schistosomiasis from Mindanao, but was later
diagnosed negative for the disease based on
Kato-Katz.17, 18
In Trinidad, there are approximately 6,000
people directly at risk for the disease, while
Talibon accounts for another roughly 15,000
inhabitants at risk. Direct sources of
transmission are from the nineteen snail-
infested bodies of water where O. quadrasi
colonies have been found.22 The latest snail
survey conducted in 2013 by the University of
the Philippines, Los Baños Research Team
showed zero infection rates of S. japonicum
among snails collected from those sites.
However, a recent national assessment in
2014 confirmed that a significant number of
residual infections of schistosomiasis still
exist among school-age children from the two
endemic areas of Bohol.
RESEARCH QUESTION
As previously mentioned, the province of
Bohol has two known endemic areas for
schistosomiasis. However, national surveys
and reports have suggested that those two
municipalities, Talibon and Trinidad, are near
elimination levels for the disease. According
to the 2009-2014 Sentinel Surveillance
Report, Bohol has consistently reported
virtually zero cases of active or heavy
infections of schistosomiasis.15 With a
prevalence rate of less than 1%, Bohol has, in
theory, reached the category of elimination
level for an endemic area as categorized by
the national DOH office.15 Furthermore, a
recent snail survey conducted in 2013 by the
University of the Philippines, Los Baños
research team has indicated zero infection
rates for the known intermediate snail hosts.15

6
Such findings corroborate the province’s
asserted status of having eliminated the
disease as a public health concern.
In 2014, however, Belizario’s Assessment of
schistosomiasis endemic areas through
parasitological and serological techniques,
(Belizario, et al., 2015) indicated that there
are still in fact a significant number of
schistosomiasis infections in the province.
Serological tests via ELISA Antibody and
ELISA Antigen confirmed the presence of
these residual infections. Thus, the goal of
this study is to investigate why those
infections still exist despite initial surveillance
reports that have stated otherwise. Since
current public health intervention programs
are already in place and have been proven to
successfully reduce prevalence rates, this
research specifically explores those major
contributing factors and how exposure rates to
a particular ‘intervention’ are related to risk
factors for disease infection.
Research Objectives This project aims to describe the current
strategies, particularly the major public health
interventions and programs that have
contributed to the reduced prevalence rates of
schistosomiasis in Bohol, particularly over the
last five years, essentially alleviating the
heavy burden of the disease in the region.
More importantly, it entails an analytical
research component done via a mixed
methods approach (i.e. qualitative and
quantitative research) to better assess the
validity of the initial surveillance reports, as
well as to investigate the potential risk factors
related to the residual infections. The
analytical research component involves a
follow-up assessment of Belizario’s study
conducted in 2014, which included samples
collected from school-age children in Talibon
and Trinidad.16 Using the selected sample
from this previous study, a qualitative study
on schistosomiasis in the two endemic
municipalities using a nested case-control
study design is applied. By collecting school-
based data and evaluation surveys, the goal of
the study is to investigate the potential risk
factors related to residual infections of
Schistosoma japonicum at the individual
level.16 The quantitative analytical
component, which utilizes statistical
techniques, could thereby validate current
public health records and surveillance data of
disease status in the community. In doing so,
the study intends not only to extract key
lessons from the case of Bohol, but given the
existing presence of residual infections, to
also provide a feasible course of action and

7
strategies in confronting these persistent
infections moving forward.
LITERATURE REVIEW
Considered a neglected tropical disease,
schistosomiasis is both an environmental
disease and a disease of poverty. It is an
environmental disease because
“anthropogenic and natural parameters
influence the distribution of the parasite
population in aquatic systems by defining the
ecological niches where the snail intermediate
hosts can survive.” 4 In addition, the disease is
transmitted from the final vertebrate host to
the aquatic environment through urinary and
fecal contamination of bodies of water,
including artificial waterways.4 It is a disease
of poverty because “its geographic
distribution reflects a community’s access to
safe water, sanitation infrastructure,
socioeconomic status, and access to
medication.”4 Praziquantel, currently the
standard drug used to treat schistosomiasis, is
an anthelmintic that kills the adult worms
inside the final human host. Although this
drug has been effective in decreasing
morbidity in many endemic regions, studies
have shown it to be an unsustainable option
for treatment because it lacks the capacity to
address the issue of parasitic risk in the
environment.4, 7 Bodies of evidence suggest
that elimination of schistosomiasis using
MDA as the major approach will not be
sustainable in the long run. One study, for
example, examined the long-term impact of
intensive case finding using praziquantel as
treatment, supported by a compliance rate of
more than 80% during the 10-year lifespan of
the study. Despite significant reductions in the
prevalence rates and incidence of infections
that occurred in the subsequent 3 to 4 years, it
was immediately followed by marked
rebound rates for the disease.8, 9
Overview of schistosoma parasites and intermediate snail vectors
Schistosomiasis in the Philippines is caused
by an infection of the blood fluke
Schistosoma japonicum.3 To complete their
zoonotic life cycle, schistosome parasites
infect an intermediate snail host and a final
vertebrate host (i.e. humans). Schistosome
ova pass from the mammalian host to the
environment via fecal matter and remain
viable for up to seven days. Upon contact
with freshwater, the embryonated eggs hatch
and release free-swimming, sexually
differentiated miracidia that infect the
intermediate snail host Oncomelania hupensis
quadrasi. 4 The miracidia then asexually

8
reproduces through a series of stages called
sporocysts, generating juvenile cercariae, the
infective larval stage for humans. The
cercariae penetrate human skin, lose their tail
thereafter, and become schistosomula that
migrate through the blood stream via the
lungs, onto the heart, and finally to the liver,
where they mature and mate for life.1 They
produce eggs that the animal host, if left
untreated, will repeatedly shed back into the
environment, ultimately restarting the
schistosome life cycle. On average, the adult
worms can produce up to 3,000 eggs per day,
making it the most pathogenic among the
schistosoma species.3
History of schistosomiasis control in the Philippines
In 1906, the first case of schistosomiasis in
the Philippines was reported. The following
describes the account and discovery of this
significant index case in the country:
“The [patient] was a Filipino man who had
never been out of the country. He eventually
died with clinical impressions of amebiasis
and bacterial infection. Autopsy confirmed
the diagnosis of amebiasis, but with additional
findings of Schistosoma ova in sections of the
large intestine, liver, and lungs.
Subsequently, schistosome ova were found in
several cases among 500 autopsies reported in
1908 and in the feces of some prisoners
admitted to Bilibid Prison, in the City of
Manila in 1914. Several years later, in 1928,
a case of Katayama disease (a toxemic
syndrome with fever in the acute, early egg-
laying phase of schistosomiasis) presenting as
chronic appendicitis was reported. Attempts
to demonstrate the intermediate host of the
parasite were not successful until the
discovery of the snail Oncomelania hupensis
quadrasi in Palo, Leyte in 1932.” 1
Despite research disruption due to Word War
II, the disease gained further attention when
in 1945, an outbreak in Leyte occurred among
Americans and the Allied Armed Forces. In
1953, the Philippines finally recognized
schistosomiasis as a public health concern.
Extensive research activities such as studies
on parasite biology, transmission, and control
to clinical and pathological aspects of the
disease were conducted. In 1975, S.
japonicum endemic regions were identified,
with an estimated 5 million people living in
those endemic areas and over 800,000
individuals with active infections. This
included the island of Bohol, with the major
foci of the disease located in the islands of
Leyte, Samar, and Mindanao, a situation that
largely remains today. These endemic

9
regions have no distinct dry season, and
predominantly comprised of rice growing
areas, which maximizes the physical contact
between humans and the intermediate hosts,
O. quadrasi snails.1
The disease threat of schistosomiasis to public
health proved to be a daunting one. Climatic
conditions and rice farming methods have
made vector control difficult. Prior to the
introduction of praziquantel in the
Philippines, different methods were used in an
attempt to decrease transmission by reducing
O. quadrasi snail populations and by
preventing human exposure to the infective
form of the parasite (i.e. cercariae).
Environmental engineering, such as improved
irrigation systems, along with the use of
molluscicides was utilized.1 Unfortunately,
these approaches were expensive and had
only yielded very limited results in lowering
human transmission rates. Another
component of the program was to provide and
encourage better sanitation. However, this
also became more difficult to sustain with
time, especially in rural and impoverished
communities, where very little of the
populations had access to sanitary toilets.
Furthermore, preventive chemotherapy was
only used on a case-by-case basis, as the
available medications caused side effects
before therapeutic levels were even reached.1
Thus, even though the early public health
intervention programs of the time ultimately
resulted in positive health outcomes, they
were clearly not effective enough in reducing
the prevalence, incidence, or morbidity of S.
japonicum infections in the country.
Praziquantel was first introduced in the
Philippines in 1980, which led the national
schistosomiasis control program to transition
to a chemotherapy-based program. Case
finding and treatment also continued to
contribute in lowering national prevalence
rates for the disease. By 1990, the Philippine
National Schistosomiasis Control Program
(PNSCP) had gained enough funding, mainly
through a substantial loan, which enabled
them to intensify active case finding and
treatment in all endemic areas.1 The country
had been reporting at least a 10% national
prevalence rate prior to this, but by 1995, this
figure was reduced to less than 5%.13
However, subsequent marked budget cuts
resulted in reduced financial support and the
loss of schistosomiasis control teams in each
of the endemic municipalities. After 1995,
the chemotherapy-based control program then
shifted from case finding and treatment to
Mass Drug Administration (MDA). Despite
the decrease in financial manpower support

10
for the control program, the annual national
prevalence data on schistosomiasis in the
Philippines reported by the PNSCP had been
seemingly maintained at less than 5%. This
reportedly low national prevalence data had
given the idea that schistosomiasis was not a
major public health concern anymore and
could even be soon eliminated in some
endemic areas via MDA alone.1, 13 However,
as indicated by previous studies regarding
underestimation of prevalence rates, many of
those areas experienced significant rebound
rates for schistosomiasis infections.21 The
following decade ushered in a new era for the
Department of Health with the National
Schistosomiasis Control & Elimination
Program (NSCEP). It called for a more
sustainable and integrative approach to
disease control, especially at the local levels
of the endemic regions. MDA was still very
much part of the big picture, and has been
strongly supported by international
organizations such as the WHO.
Nevertheless, there is still clearly a great
demand for more action from the government
side and a better response from the public to
solve the problem of schistosomiasis in the
Philippines. (See Figure 1 in Appendix for
diagram of the historical evolution of
schistosomiasis control in the Philippines)
The Health System: National & Local Levels As shown in Figure 3A (Appendix), the
National Schistosomiasis Control &
Elimination Program (NSCEP) operates
under the Elimination Division for Neglected
Tropical Diseases, which is part of the
Infectious Diseases Office (IDO) of the
Disease Prevention & Control Bureau within
the Department of Health. Currently, NSCEP
collaborates with the WHO, which provides
technical assistance for the national program,
including drafting policies, guidelines, and
planning to help achieve their objectives and
support the national program agenda. The
partnership maintains a clear understanding of
their respective roles, wherein the WHO
serves to fortify the national office and its ties
with the international community; namely,
China, in its most recent technical cooperation
agreement on schistosomiasis, given that the
two countries share the same type of species
for the disease.
The main challenge for the DOH national
office is the implementation and management
of the program at the local levels. The
country’s political structure is devolved,
making it a decentralized health system that
completely functions at the national, regional,
and provincial levels, but not at the municipal

11
level, where the LGUs have full authority and
control of how to conduct and implement
public health programs (refer to Figure 3B,
Appendix). DOH advises, provides technical
guidance, and supports the LGUs as they see
fit, but ultimately, the LGUs make the final
decisions on how to run and manage their
programs. Such arrangement can create a
potential ‘disconnect’ between the central
DOH office and the LGUs, especially in
prioritization and supervision of any given
program. The process and flow of
information, for example, comes to a halt at
the municipal level, which can then either
fully digest or reject it. Theoretically, LGUs
will implement health programs from the
DOH and carry out the design and strategies
in full cooperation. However, LGUs may
recognize other programs to be more
beneficial to their communities and therefore
focus their efforts on those more than others.
Thus, it is important that in working with
LGUs, to build stronger relationships by
maintaining open lines of communication and
a mutual understanding of how to best serve
the people. This relationship is key to
fostering effective implementation and
realizing program objectives, such as those of
the NSCEP. In Bohol, both LGUs, with the
health sector operating under the MHOs of
Talibon and Trinidad, have established a solid
relationship with DOH. This is manifested
through the current state and several avenues
of the local public health sector, including
recent health indicators for schistosomiasis.
At the local level, the Municipal Health
Officer (of the MHO or also referred to as the
RHU) operates and directly reports to the
Municipal Mayor’s Office. The MHO
typically employs a number of municipal
nurses, a public health nurse (PHN), a
municipal sanitation inspector (MSI), a
microscopist (or a visiting medical
technologist from PHO), and rural health
midwives (RHM). In addition, the DOH has
established the Nurse Deployment Program
(NDP), which hires nurses, usually recruited
locally, and assigns them to the MHO, which
designates them for various duties, such as
supplementing a barangay health station,
where a midwife is typically in charge. (refer
to Figure 3C, Appendix)
The DOH assigns a Development
Management Officer (DMO), who serves as
the DOH Representative to the MHO. The
DMO is also responsible for the NDP nurses
working at the MHO. There is also a
Provincial Sanitation Inspector (PSI) from the
PHO, who works in partnership with the
DMO and supervises the MSI. Other

12
positions within the RHU are contracted by
the MHO, as necessary and as the LGU
budget permits. The organizational system in
Talibon and Trinidad follows this precise
structure, with well-defined responsibilities
and properly delegated tasks. The RHUs
work fluidly with the DMO in ensuring that
program objectives are carried out and
constant communication from the PHO, RHO,
and central DOH office is maintained. In
both Talibon and Trinidad, the MHOs are
very supportive of the national programs,
especially that of the NSCEP. They make the
necessary adjustments to adapt the programs
to their localities based on needs, but their
support and advocacy for a program such as
the NSCEP is clearly palpable in their routine
activities and health service provisions related
to schistosomiasis. In essence, the MHO
serves as the bridge between the LGUs and
the central DOH office, making it a crucial
position that defines the success of any given
public health program in the province.
DOH’s 4-Pronged Approach The newly reorganized NSCEP has outlined
specific areas of prioritization in addressing
schistosomiasis in endemic areas. They
include the following four aspects: 14
1. Preventive Chemotherapy or Selective
Treatment (Praziquantel)
a. Kill the adult worms in humans
(reservoir host) via praziquantel
based therapy
2. Vector (Snail) Control
a. Kill or replace the intermediate
hosts via biological control (e.g.
competitor snails and snail-eating
fish), chemical control
(molluscicides), and
environmental management
3. Environmental sanitation, IEC, and BCC
a. Prevent the snails from getting
infected, hence preventing
contamination of the water by
infected individuals or animals
using IEC, proper sanitation, and
behavior change
4. Safe water supplies, IEC, and PPE
a. Stop humans and animals from
getting infected by preventing
contact with water containing
infected snails or cercariae
(achieved through IEC and potable
or safe water supply)
This study examines the compliance and
implementation of the above four elements in
the province of Bohol. It also provides
empirical evidence for successful control and

13
elimination of schistosomiasis if such a multi-
component integrated approach is followed.
Lastly, it shows that a province like Bohol,
given the proper support and adequate
intersectoral cooperation at the local levels,
can competently fulfill its capacity in
effectively mobilizing local citizens into
timely action, creating a potent system that
can respond to a serious public health threat.
METHODS
Design Overview
The descriptive research involves extensive
literature reviews of the disease history,
epidemiology, and efforts for control and
elimination for schistosomiasis in Bohol.
Additionally, comparable studies of disease
control in other endemic regions of the world
have been referenced. The scope of the case
study is to demonstrate how Bohol has been
able to address the problem of schistosomiasis
and put into practice technical
recommendations from DOH, which
collaborates with WHO, to combat this
neglected tropical disease. Among such
recommendations include preventive
chemotherapy, environmental sanitation,
vector surveillance and control, and behavior
change communication.5 The study assessed
the compliance as well as effectiveness of
service delivery and program implementation
at the local level (i.e. municipalities of
Talibon and Trinidad). It therefore not only
illustrates Bohol’s recent success in reducing
prevalence rates for schistosomiasis, but also
validates the efficacy of specific public health
measures and interventions for the disease.
The analytical research component involves a
follow-up assessment of a recent study
conducted in 2014 by Belizario, et al.,
Assessment of schistosomiasis endemic areas
through parasitological and serological
techniques, which included samples from
Talibon and Trinidad. Using a select sample
from this previous study, we conducted a
qualitative analysis of schistosomiasis in the
two endemic municipalities of Bohol using
the methodology of a nested case-control
study design. Collecting household data and
surveys enabled us to evaluate the
contributing factors to Schistosoma
japonicum infections at the individual level.
We determined and measured ‘exposure’ by
designing questionnaires specific for each
type of intervention. We also tried to
corroborate our findings with available public
records and surveillance data.

14
As we will describe in the Data section, the
total sample size for this study is n = 65
(cases) + 250 (controls) = 315. We used the
samples from Belizario’s report to ‘recruit’
our cases for the ‘disease’ group (n=65),
which have been classified based on a
positive test result for ELISA (Enzyme
Linked Immunosorbent Assay) Antibody or
ELISA Antigen, serological tests for
schistosomiasis that detect previous or active
infections. The controls were then selected
from a randomized sample of individuals
from the same cohort who did not develop the
disease based on their ELISA Ab/Ag test
results. The referenced study had a total
sample size of n=414 from Talibon and
Trinidad. Ideally, all 414 subjects would be
surveyed at the end of the study; however,
realistic considerations are expected to reduce
that number. In the end, a total of 315 school
children were interviewed, of which 65 tested
positive for ELISA Ab/Ag. As such, a case
(i.e. ‘Disease Status’) was defined as any
individual who tested positive for ELISA
Ab/Ag through Belizario’s study, and each
was thus classified as a ‘residual infection’ of
schistosomiasis. Using a ‘survivor sampling’
approach, the controls consisted of
individuals from the same source population
who did not have the outcome of interest, in
this case, those who tested negative for
ELISA Ab/Ag in Belizario’s study. From the
315 total collected surveys, 250 had tested
negative for ELISA Ab/Ag.
Data: Context, Population, and Sampling The geographic area of interest includes the
two municipalities of Talibon and Trinidad in
the province of Bohol, Philippines. Along
with the comprehensive schistosomiasis case
ELISA Ab (+) [Prevalent cases of schistosomiasis]
n = 65
EXPOSED
NOT EXPOSED
Negative for schistosomiasis
n = 250
EXPOSED
NOT EXPOSED

15
study report documented in this region, the
research investigation utilized data samples
from Belizario’s study in 2014, Assessment of
schistosomiasis endemic areas through
parasitological and serological techniques
(Belizario, et al., 2015). At the time, study
participants were public elementary school
children ages 9-17 years old from two
selected village or barangay schools from
each municipality. The recruited students had
not received any treatment of praziquantel
within the last six months of the study period
in March 2014. According to the National
Schistosomiasis Control and Elimination
Program, “among difference age groups,
children ages 5-15 to have the highest
intensity of infection.”14 The sample
therefore expected to capture what evidently
seems to be the most vulnerable group of the
population, increasing its external validity and
reliability. This follow-up study occurs
approximately 1.5 years after Belizario’s
study. Thus, the study participants’ ages
range from 10-18 years old (with a mean of
13 years).
The study examined schistosomiasis-related
public health interventions in Bohol as factors
that helped prevent Schistosoma japonicum
infections. As stated earlier, infected
individuals (ELISA Ab/Ag positive) were
selected from a previous study conducted in
2014. A total sample size of n=315 was used,
and all were given questionnaires to assess
their knowledge and use of existing public
health interventions (e.g. MDA, access to
potable water, environmental sanitation, etc.)
in their localities.
Preliminary Data Collected:
Group Sample size (n)
ELISA Ab/Ag (+) 65
Other samples (-) 250
Total: 315
Dependent Variable
The outcome or dependent variable is the risk
for Schistosoma japonicum infections. We
defined ‘risk’ by using the cases that tested
positive via serological tests. While ELISA
antibody is a serological test that cannot
distinguish between both old and active
infections, ELISA antigen is able to detect
active infections within the past two years.
As such, they are considered categorical
variables, either testing positive for ELISA
Ab/Ag or not (i.e. disease risk). For study
purposes, all samples that tested positive for
ELISA Ab or ELISA Ag have been classified
as ‘residual infections’ of schistosomiasis.

16
Key Independent Variables
The key independent variables are a number
of public health intervention programs that
include: knowledge of MDA (praziquantel),
access to safe drinking water, sanitation
infrastructure, hand hygiene practices,
exposure to potential animal vectors,
exposure to potential snail sites, and exposure
to disease awareness, advocacy or health
education (e.g. BCC, IEC). We measured the
‘exposure’ to each of these interventions
through surveys and questionnaires designed
to assess the knowledge, attitudes, and
practices (KAP) of the entire population
sample.
Basic Conceptual Framework
H0 = There is no association between S.
japonicum infections and the ‘risk factor’.
§ OR = 1 would indicate that the
estimated disease risk is the same
for the exposed and unexposed.
HA = There is an association between S.
japonicum infections and the ‘risk factor’.
These factors reduce the risk or protect
against S. japonicum infections.
§ OR < 1 would indicate that the
exposure protects against
occurrence of disease (or reduces
the disease risk)
Estimation Approach & Data Analysis A major assumption in this study is that the
public health interventions in place yield a
100% success rate for eliminating the disease.
In other words, given full compliance to
DOH’s integrated approach, there should be
no remaining infections in the province.
Thus, we can treat each intervention as a
potential risk factor if an individual has failed
to fully comply or the lack thereof. Utilizing
a nested case-control study design, we
conducted a qualitative analysis of
knowledge, attitudes, and practices related the
existing public health interventions and
determine associations with risks of getting
infected with schistosomiasis. Using STATA
13, we then calculated the odds-ratio and
MDA
Access to safe water
Sanitation
Other Interventions

17
statistical significance for each variable,
which allows us to evaluate how a specific
public health intervention program affects the
risks for Schistosoma japonicum infections.
Lastly, we formulated a logistic regression
model to further explore possible interactions
between variables and draw out relationships
and their confounding effects on one another.
Procedures
Questionnaire
The survey questions were designed in
consultation with WHO and DOH,
particularly inputs from scientific experts in
fields of epidemiology, environmental
sanitation, water safety, and agriculture. It
was important to ensure that the questions are
clear and concise, as well as appropriate to the
age level of understanding of the subjects.
The main objective of the questions is to
determine exposure to a specific intervention
related to schistosomiasis. The complete list
of questions used in this study is found in the
Annex 4 (Appendix). The questions were
written in English, which is considered a
second language in the country. The
country’s official language, Tagalog, is also
widely used. Thus, the primary investigator,
a fluent Tagalog speaker, did not have any
problem communicating with local residents.
Nevertheless, for reliability purposes, the
survey questions were translated into the main
dialect, Bisaya. The questions were then
uploaded digitally using the mHealth (mobile
health) platform MAGPI. Data collectors
were only able to use a smartphone or a tablet
with the MAGPI app installed. Utilizing a
digital platform for data collection enabled us
to expedite and consolidate the process,
making data management more efficient, and
reducing human error (e.g. record, systematic
errors, etc.).
Human Subject
Since this study is considered a follow-up
from Belizario’s 2014 study, consent forms
have already been collected, which made it
easier to obtain support and full cooperation
from participants through their respective
schools. Belizario and his research team were
also directly contacted to secure their
officially signed endorsement, which linked
the two studies together. Furthermore, it is a
project endorsed by the national DOH office
and is considered a part of their M&E routine
activities, circumventing the need for an
ethics review. Lastly, the study was purely
qualitative in nature, and no additional
specimen of any kind was collected for
testing. Specific protocols as outlined by

18
DOH and WHO were followed and an
updated protection of privacy was drafted.
Endorsement of LGUs
Another important, yet often overlooked,
aspect of conducting this type of study is
ensuring that all stakeholders involved are not
only aware of the full scope of the project, but
also that their support is properly solicited. A
successful study necessitated open lines of
communication with all corresponding DOH
offices (national, regional, and provincial
levels), LGU officials (municipal mayor,
sanitation inspector, municipal health officers,
and rural health units), and the Department of
Education (school principals, teachers, parent
representatives, and departmental nurse
representative). Prior to the start of data
collection, all personnel were notified of the
national DOH endorsement and upon arrival
in Talibon, an integrative stakeholder meeting
was conducted at the local RHU to introduce
the project, coordinate technical details,
acquire additional human-resource assistance
on the ground during data collection, and
address any other concerns.
Training of NDP Nurses
The study recruited data collectors through
DOH’s Nurse Deployment Program. The
program employs locally based nurses in
Talibon and Trinidad. For this study, 10
nurses were recruited from Talibon and an
additional 8 from Trinidad. All nurses were
trained in using the MAGPI app, and the pre-
tests for the surveys were conducted with
each other. Each question was carefully
reviewed during the training, and
transcription into the local Bisayan dialect
was also performed. The data collectors were
then instructed regarding specific research
protocols such as the participants’ rights to
opt-out and how to maintain confidentiality.
School Site Visits & Data Collection
The main school sites were composed of 4
different high schools in 4 endemic barangays
(2 from each municipality), and a few other
students were tracked down in two other
elementary schools. A full day was allotted
for each school, and data collection was
coordinated through the Department of
Education nurse representative. Surveys were
conducted in a classroom setting and each
NDP nurse randomly received a unique code
ID number for the student being interviewed,
which corresponds with their undisclosed
ELISA Ab/Ag test result and allows the
primary investigator to determine whether the
subject was a case or a control. The answers
were then uploaded at the end of the day at
the RHU where Wi-Fi or Internet connection

19
was available. This provided the primary
investigator to review the data, detect errors
or discrepancies, and make any necessary
corrections or acquire additional information
from the data collector the following working
day. Data collection required 5 full working
days, where a total of 315 questionnaires were
successfully uploaded onto MAGPI.
RESULTS
Table 1 below provides the descriptive
statistics for data collected in Bohol. Among
the total of 315 study participants, 49.8%
(157) were males, while 50.2% (158) were
females. Relevant demographic data was also
gathered. The highest education level of
parents for the majority of the participants,
45.4% (143), is high school. As expected,
54% (170) could not provide information
regarding their families’ annual household
income.
For schistosomiasis-related questions, it is
important to note that the timeline of exposure
to these ‘risk factors’ must occur prior to
2014, or before Belizario’s study, since we
want to measure disease risk as detected by
the serological tests in that study. Beginning
with MDA, the majority or 44.1% (139) of
the participants recall having taken
praziquantel at least 5 times. Overall, their
knowledge of MDA seems to be very high.
85.7% (270) know the purpose of
praziquantel and 95.2% (300) believe in the
drug’s effectiveness. Significantly, 35.9%
(113) of the students have experienced an
adverse event immediately following
praziquantel intake; the largest value being
headache (18.1%), followed by dizziness
(13.3%), and thirdly, abdominal pain (8.9%).
With regards to access to safe drinking water,
only approximately 32.1% (101) of the
participants could be considered as having
had access to potable water. Conversely, a
notably high number, 93.7% (295) of the
students have had access to a functional toilet
or latrine (water-sealed) at home.
Furthermore, 84.4% (266) would wash their
hands after using the toilet at home, of which
77.1% (243) use soap. In school, this practice
seems to decrease as only 73.3% (231) would
wash their hands, of which 48.3% (152) use
soap. There are also a high number of
participants who have been exposed to
potential animal vectors, 80.6% (254) having
kept domesticated animals or pets (dogs, cats,
or rodents) at home, while 70.5% (222)
having had direct contact with bovine or farm
animals (pigs, water buffaloes, cows, etc.).

20
Table 1: Descriptive statistics of variables
VARIABLE STATISTICS Gender n = 315 Proportion Cases Controls
Male
157 49.8% 25.5% n = 40
74.5% n = 117
Female
158 50.2% 15.8% n = 25
84.2% n = 133
Highest education level of parents n = 315 Proportion Elementary 97 30.8%
High School 143 45.4% College 45 14.3%
Post-graduate or Advance degree 0 0% Unknown
30 9.5%
Annual household income n = 315 Proportion <5,000 pesos 38 12.1%
5,000-15,000 pesos 15,000-25,000 pesos 25,000-50,000 pesos
>50,000 pesos Unknown
31 24 26 26 170
9.8% 7.6% 8.3% 8.3% 54%
MDA participation (praziquantel intake) n = 315 Proportion Never 1 0.3% 1 time 19 6.0%
2 times 3 times 4 times
>5 times Unsure
51 47 48 139 10
16.2% 14.9% 15.2% 44.1% 3.2%
Knowledge of praziquantel n = 315 Yes No Unsure Purpose of praziquantel 270 85.7% 11.7% 2.5%
Belief in praziquantel’s effectiveness
300
95.2%
2.2%
2.5%
Experience with adverse events
Dizziness Headache
Malaise Drowsiness
Fatigue
113 42 57 5 3 8
35.9% 13.3% 18.1% 1.6% 1.0% 2.5%
62.9% 86.7% 81.9% 98.4% 99.0% 97.5%
1.3%

21
Abdominal pain Diarrhea Vomiting
Nausea Bodily pain
Fever Numbness
Others not listed
Future participation in MDA
28 6 13 9 0 3 0 2
307
8.9% 1.9% 4.1% 2.9% 0% 1.0% 0% 0.6% 97.5%
91.1% 98.1% 95.9% 97.1% 100% 99.0% 100% 99.4% 2.5%
---
Access to safe drinking water n = 315 Proportion Mineral water (e.g. bottled or purchased) 89 28.3%
Boiled Tap
Pump or borehole Ground well water
Rainwater Water from stream, creek, or river
4 8 17 196 1 0
1.3 2.5% 5.4% 62.2% 0.3% 0%
Sanitation infrastructure n = 315 Yes No Functional toilet or latrine (water sealed) used at home. If not, list other methods:
295 93.7%
6.3%
Communal or shared Dug pit in the ground
Open space in the backyard Closest stream, creek, or river
Anywhere convenient
Other methods of feces disposal: Trash collection by LGUs
Burned in the backyard Buried in the ground
Thrown in nearby stream, creek, or river Thrown anywhere convenient
Others not listed above Not applicable
6 3 7 0 4 0 0 87 7 12 62 165
1.9% 1.0% 2.2% 0% 1.3% 0% 0% 27.6% 2.2% 3.8% 19.7% 52.4%
Hand hygiene practices n = 315 Yes No At home:
After toilet use With soap
In school: After toilet use
With soap
266 243
231 152
84.4% 77.1% 73.3% 48.3%
15.6% 7.6% 26.7% 25.1%

22
Exposure to potential animal vectors n = 315 Yes No N/A
Household pets (dogs, cats, or rodents)
Farm animals (pigs, water buffaloes, cows, or other bovines)
254
222
80.6% 70.5%
14.9% 19.4%
4.4% 10.1%
Exposure to potential snail sites n = 315 Yes No Freshwater aquatic environments such as ponds, creeks, streams, or rivers, as well as artificial waterways:
Laundry practices Bathing practices
Water collection practices
130 225 19
41.3% 71.4% 6%
58.7% 28.6% 94%
Exposure to disease awareness, advocacy campaigns, and health education
n = 315
Yes
No
Community awareness or campaigns School-related activities
177 223
56.2% 70.9%
43.8% 17.8%
Social media or platforms: TV
Radio Magazine
Newspaper Internet
Others not listed
122 24 5 8 3
134
38.7% 7.6% 1.6% 2.5% 1% 42.5%
61.3% 92.4% 98.4% 97.5% 99% 57.5%
For those who have had exposure to
potential snail sites (which includes
freshwater aquatic environments and
artificial waterways) prior to Belizario’s
2014 assessment, 41.3% (130) of the
participants reported having been involved
in laundry practices, an even much higher
number at 71.4% (225) with bathing
practices, but a relatively low number at 6%
(19) involving water collection practices.
Lastly, among all study participants, 56.2%
(177) have been exposed to community
awareness or health campaigns regarding
schistosomiasis; 70.9% (223) have
participated in school-related activities that
promoted health education for the disease;
and among all social media or platforms,
38.7% (122) remember having seen or
learned about schistosomiasis awareness on
television, the highest among all other listed
choices.

23
Table 2 below shows the odds ratio for each
risk factor and their corresponding statistical
significance. In theory, an OR that is less
than 1 and is statistically significant (i.e. at
the 95% level), means that exposure to the
risk factor protects against the occurrence of
the disease (i.e. schistosomiasis) or reduces
disease risk. One of the major assumptions
involved in such statistical analyses is that
the test assumes independent data. In other
words, there is no association between or
among the data sets being collected and
tested. Another assumption is that the data
set has a normal distribution. For the
purpose of this study, we have set the alpha
at 0.05 to determine statistical significance.
The sample size is n=315, which we
estimated to be sufficient (i.e. power and
effect size) in carrying out the desired
statistical tests.
Solely interpreting the odds ratio in Table 2
indicates that access to potable water, hand
hygiene practices, and exposure to social
media or platforms (TV and newspaper)
seem to have a protective effect for the
disease, or reduce the disease risk. On the
contrary, the estimated disease risk for those
who have been exposed to potential animal
vectors and snail sites (laundry and bathing
practices), seem to be greater for the
exposed group. Sanitation infrastructure,
community awareness, and school-related
activities seem to have a neutral effect.
However, when we consider statistical
significance, only exposure to television (i.e.
promoting advocacy or health education
regarding schistosomiasis), is statistically
significant, with a p-value of 0.011 and CI
of 0.23-0.87 (i.e. excludes the value 1.0, and
allows us to reject the null hypothesis).
In order to account for interactions among
the variables, we ran a logistical regression
model, as shown in Table 3 below. The
results now indicate that 1) sanitation
infrastructure, 2) exposure to potential
animal vectors (specifically bovine or farm
animals), and 3) exposure to school-related
activities that promote health education, are
all statistically significant. As all other
independent variables are held constant,
their respective coefficient values suggest
that sanitation infrastructure (-2.01) and
participation in school-related activities or
health education (-0.781) could significantly
be considered protective factors for the
disease, while exposure to potential bovine
or farm animal hosts (2.27) likely increases
the risk for the disease.

24
Table 2: Odds ratio of potential risk factors for S. japonicum infections among school-age children in Bohol RISK FACTORS p-value Odds Ratio CI (Odds; 95%) Knowledge of MDA
Purpose of praziquantel Belief in praziquantel’s effectiveness
Experience with adverse events
Access to safe drinking water Mineral, boiled, and tap vs.
Borehole and Ground water well
Sanitation infrastructure Functional toilet or latrine (water sealed)
Hand hygiene practices
At home; after toilet use At home; with soap
In school; after toilet use In school; with soap
Exposure to potential animal vectors
Household pets (dogs, cats, rodents) Farm animals (pigs, water buffaloes, cows)
Exposure to potential snail sites (i.e. aquatic environment such as ponds, creeks, streams, or rivers)
Laundry practices Bathing practices
Water collection practices
0.776 1.00† 0.827
0.357
1.00†
0.468 1.00†
0.142 0.414
0.789 0.591
0.092 0.428 0.774†
0.895 1.59 1.07 0.765 1.04 0.767 0.960 0.645 0.753 1.11 1.22 1.60 1.29 0.708
0.40 - 2.16 0.19 - 74.5 0.57 - 1.95 0.42 - 1.42 0.32 - 4.44 0.36 - 1.73 0.32 - 3.45 0.35 - 1.23 0.36 - 1.60 0.49 - 2.78 0.57 - 2.81 0.89 - 2.87 0.67 - 2.58 0.13 - 2.59
Exposure to disease awareness, advocacy campaigns, and health education
Community awareness School-related activities
TV Radio
Magazine Newspaper
Internet Others not listed
0.883 0.672 0.011* 1.00†
1.00†
1.00† 0.508†
0.095
1.04 1.16 0.451 0.989 0.940 0.530 1.90 1.47
0.58 - 1.87 0.53 - 2.43 0.23 - 0.87 0.28 - 2.91 0.02 - 9.74 0.01 - 4.27 0.03 - 36.9 0.90 - 2.36
CI indicates Confidence Interval; †Fisher’s exact test; *Significant of p<0.05

25
Table 3: Logistic regression model for ‘Disease Status’ among school-age children in Bohol Disease Status (Outcome Var.) Coef. Std.
Err. z P > z 95% CI
Gender: Female Knowledge of MDA
Purpose of praziquantel Belief in praziquantel
Adverse events
Access to safe drinking water
Sanitation infrastructure Functional toilet or latrine
Hand hygiene practices
At home; after toilet use At home; with soap
In school; after toilet use In school; with soap
Exposure to animal vectors
Household pets Farm animals
Exposure to snail sites (i.e. aquatic environments)
Laundry practices Bathing practices
Water collection practices
-0.358
1.03 0
-0.268
-1.09
-2.01
0
0.342
0 -0.413
-0.682 2.27
0.187 -0.1
-0.477
0.503 0.909 --- 0.491 0.133 0.979 --- 0.874 --- 0.495 0.712 1.09 0.566 0.619 0.925
-0.71 1.14 --- -0.55 -0.82 -2.05 --- 0.39 --- -0.83 -0.96 2.08 0.33 -0.16 -0.52
0.477 0.254 --- 0.585 0.413 0.040* --- 0.695 --- 0.405 0.338 0.037* 0.741 0.871 0.606
-1.34; 0.63 -0.75; 2.82 --- -1.23; 0.69 -3.91; -0.08 -3.93; -0.09 --- -1.37; 2.06 --- -1.38; 0.56 -2.08; 0.71 0.13; 4.42 -0.92; 1.30 -1.31; 1.11 -2.29; 1.34
Exposure to disease awareness, advocacy, and health education
Community awareness School-related activities
TV Radio
Magazine Newspaper
Internet Others not listed
-0.645 -0.781 -0.483
0
0.541
0 0
0.093
0.340 0.385 0.569 --- 1.56 --- --- 0.846
-1.89 2.03 -0.85 --- 0.35 --- --- 0.11
0.058 0.042* 0.395 --- 0.728 --- --- 0.913
-1.31; 0.02 0.03; 1.53 -1.60; 0.63 --- -2.51; 3.60 --- --- -1.57; 1.75
CI indicates Confidence Interval; *Significant of p<0.05; Log likelihood= -59.76; Number of observations= 136; LR chi2(3)= 18.79; Prob>chi2= 0.22; Pseudo R2= 0.14

26
DISCUSSION
Mass Drug Administration
MDA is a term used for community drug
distribution. In Bohol, community health
providers, BHWs, and individual volunteers
have been trained for protocols and
procedures regarding proper administration
of praziquantel.14 Currently, praziquantel is
the only medicine recommended by WHO
for treatment of all forms of schistosomiasis
in both children and adults.5 A single oral
dose of 40-mg/kg body weight is considered
adequate to provide cure rates of between
60-90% and reductions of 90-95% in the
average number of excreted eggs.14
Unfortunately, despite the significant cost
reductions that have followed patent expiry,
praziquantel remains one of the most
expensive anthelminthics on the market.5
For the time being, DOH has partnered with
WHO to procure sufficient annual supply of
the medicine. If the disease continues to
persist, it poses the question of sustainability
in acquiring this essential drug.
During the past decade, the Philippine
national government, spearheaded by the
Department of Health, released
Administrative Order No. 2007-0015, which
declared praziquantel as the standard drug of
treatment for schistosomiasis. It regulated
the administration of praziquantel at a dose
of 60-mg/kg body weight for 1 day taken in
2 divided doses at 4-6 hour interval.14
Furthermore, it has declared July as the
Annual Schistosomiasis Awareness and
MDA Month. This approach has not only
created a sense of solidarity and purpose, but
has also significantly boosted the
knowledge, especially among school-age
children regarding schistosomiasis and the
best practices for prevention.
The results of this study indicate that a high
percentage of school-age children in Bohol
possess sound knowledge of MDA, its
purpose, and consequence. The majority
also trusts in its ability to treat the disease.
In Bohol, MDA is methodically
implemented through the gathering of at-risk
school-age children (i.e. primary schools in
endemic barangays), as well as making
house visits to those who are not in school
due to absenteeism or dropouts. The
commitment and coordinated efforts from
different sectoral groups, including the
LGUs, the Department of Education, and
DOH have ensured the timely and high
coverage rates of MDA in Talibon and
Trinidad from 2009 to 2013, and again in

27
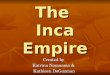
2015. Figures 4A and 4B indicate the high
percentage rates of MDA accomplishment in
the two municipalities.17,18 Talibon was able
to administer praziquantel among 76% of its
total population target during its first year of
MDA in 2009. Since then, that figure has
increased consistently in the following four
years, achieving 80%, 83%, 96%, and 97%
successively. Even with the one-year gap or
missed MDA in 2014, the MDA coverage
was highly maintained at 96%.
Figure 4A. MDA accomplishment in Talibon, Bohol (2009-2013, 2015)
Figure 4B. MDA accomplishment in Trinidad, Bohol (2009-2013, 2015)
Trinidad has virtually accomplished a
similar feat. Its first MDA year in 2009 had
a coverage rate of 84%. This increased
significantly the next four years, recording
at 89%, 98%, 99.8%, and 99.9%; and an
impressive 100% accomplishment in 2015.
Nonetheless, the successful implementation
of MDA during those six years was not
without its challenges. Yet the actions
taken, especially by the RHUs, in response
to such issues can serve as important
learning points for other endemic regions.
For example, after its first year of
implementation in 2009, there were a
decreased number of children given parental
consent for MDA. This was attributed to
several factors, including the adverse effects
experienced by children after taking
praziquantel and false rumors regarding the
drug’s negative impact on the body. Thus,
the RHUs set out to cultivate stronger
advocacy and health promotional campaigns
to increase disease awareness and the
importance of MDA. This also addressed
the rumors about the ill effects of
praziquantel and other misinformation
regarding the drug. Just as crucial to note is
that advocacy and health education were
directed through proper channels such as the
LGUs and the Department of Education.
76% 80% 83%
96% 97% 96%
0%
25%
50%
75%
100%
2009 2010 2011 2012 2013 2015
Accomplishm
ent (%)
84% 89% 98% 99.8% 99.9% 100%
0%
25%
50%
75%
100%
2009 2010 2011 2012 2013 2015
Accomplishm
ent (%)

28
Conscious efforts were made to involve
LGU personnel, local leaders, and
schoolteachers in health trainings for
MDA.19, 20 Another concern that arose was
that the administering of praziquantel would
be time consuming. To tackle this issue, the
RHUs prepared the drugs in advance before
the actual day of MDA. This involved
preparing the praziquantel per anticipated
student (i.e. with body weight records
already collected to determine proper
dosage) and with divided doses for the
morning and afternoon sessions.19, 20
Finally, the challenge of high incidence of
adverse effects, especially during the first
year (2009) needed to be addressed. In the
subsequent years, a separate budget from the
regional DOH office was allotted for meals,
as school children were provided breakfast
and lunch prior to taking praziquantel. This
effectively minimized adverse events and
reactions to praziquantel. In addition,
supportive medicines were made available
and given as prescribed by a community
health professional. Health education also
played an important role in reassuring
parents and their children the markedly
reduced difference in adverse effects of
praziquantel during the first year of taking
the drug (i.e. severe cases of adverse advents
are correlated to larger egg counts in the
body), compared to the successive years of
receiving such treatment.17, 18
Vector Control The WHO states that vector and
intermediate host control “serve as an
important cross-cutting activity aimed at
enhancing the impact of preventive
chemotherapy and intensified disease
management.” 2 For the S. japonicum
species in the Philippines, the known
intermediate host is the snail Oncomelania
hupensis quadrasi. These snails inhabit
shallow muddy sediments of lentic, lotic,
freshwater systems including ponds,
streams, rivers, lakes, irrigation canals, and
heavily irrigated agricultural fields. The
primary ecological determinants of their
habitat suitability include temperature,
sunlight, water flow, and presence of
macrophytic aquatic plants.4 Studies have
found that light intensity and the number of
O. quadrasi in a given site are inversely
related. The reduced activity of snails
during the day and their avoidance of bright
light indicate the necessity of cover.7
Furthermore, high temperatures over long
periods of time have been known to limit
snail fecundity. Experimental studies have

29
suggested that direct sunlight can have lethal
effects on snails, as they tend to avoid direct
sunlight exposure and prefer shaded areas
usually provided by dense vegetation.4
In the 1990s, many of the citizens living
near or around the snail sites in Talibon and
Trinidad remained hesitant to clear the snail
sites where the native ‘gabi’ (taro) plant has
been commonly found. The very broad taro
leaves provided the ideal shade for O.
quadrasi snails. At the same time, however,
they also provided a source of food for the
local inhabitants during the dry season.
Therein lies the problem of community
cooperation, as with any public health
intervention programs.23 With the support
from LGUs and the Department of
Agriculture, the MHOs have successfully
convinced many of these landowners to
convert their lands into rice fields.
Certainly, it took considerable time, effort,
and financial resources to accomplish such
feat, and it remains to be perhaps one of the
unique aspects of the effective vector control
for schistosomiasis in Bohol. Currently, the
two municipalities conduct quarterly (i.e. 4
times a year) clearing of snail sites in the 19
known sites where O. quadrasi snails have
been found.17, 18 With funding and personal
protective equipment (PPE) provided by the
RHO, local staff from the MHO and the
Schistosomiasis Task Force Team, organize
and conduct the clearing of snail sites. Their
goal is to primarily get rid of dense
vegetation that provides the desirable shade
for snail vectors. Furthermore, several of
the snail sites have already been converted
into rice fields, many of which have proper
irrigation systems, in accordance to
regulations set forth by the National
Irrigation Administration (NIA).
In relation to the study conducted, results
have shown that 41.3% of the participants
are possibly at risk for exposure to potential
snail sites through their laundry practices,
while 71.4% are at risk due to bathing
practices. Although without statistical
significance, the ORs indicate that both
practices do seem to increase the disease
risk (Table 2). Furthermore, a one-unit
increase of exposure to other known animal
vectors such as bovine or farm animals
indicate a 2.27 increase in the log-odds of
disease risk at the significant level (Table 3).
It is therefore crucial moving forward to
maintain robust strategies for vector control,
as what they have already pioneered in
Bohol. In the past, mollusciciding was the
other option for snail vector control.24
However, in an effort to support

30
environmental health and protection, the
Philippine government has banned the use of
molluscicides in the country. Thus, the
NSCEP has been conducting snail control
via active disease surveillance and
promoting other practical solutions.
Malacological surveys, albeit limited, are
also conducted on a periodic basis and are
usually contracted out to independent
research institutions, such as that of
university-affiliated groups.17, 18
Environmental Sanitation Environmental sanitation encompasses the
control of animal movement, proper use of
toilet, access to clean and safe water supply,
and the use of footbridges when crossing
infected canals or waterways.11 The two
endemic municipalities in Bohol have
prioritized the provisions of sanitary toilets
in their communities, especially in the
endemic barangays. Currently, there is a
budget allotted so households in need may
obtain water-sealed toilets at an affordable
price (the cost is about 50 pesos each, or
equivalent to roughly US$ 1), including
instructions for installation and free cement
supply provided by the barangay units. For
families below a certain income level, the
toilets are subsidized by the LGUs. From
the total supply for toilets, about 30% are
acquired through donations. The LGUs
provide assistance with the proper
construction and installation of toilets. They
also conduct annual inventory of households
with sanitary toilets to determine their needs
and targets for the next fiscal year.17, 18
Figure 5A. Households with access to sanitary toilets in Talibon (2014-2015)
Figure 5B. Households with access to sanitary toilets in Trinidad (2014-2015)
81%
89%
93%
86%
92%
90%
95%
94%
0% 20% 40% 60% 80% 100%
San Agustin
San Carlos
San Jose
San Roque
2015 2014
93%
87%
93%
98%
95%
92%
95%
100%
0% 20% 40% 60% 80% 100%
Kinan-‐oan
Mabuhay Cabiguhan
San Vicente
Santo Tomas
2015 2014

31
Figures 5A and 5B show the 2014-2015
inventory reports of households with
sanitary toilets in the endemic barangays of
Talibon and Trinidad. In 2014, Barangay
San Agustin in Talibon had the lowest
percentage of households with sanitary
toilets at 81%. The following year, as with
the rest of the endemic barangays, this
number increased to 92%. As of 2015, the
percentage of households with sanitary
toilets ranges from 90% to 95%. Similarly,
Trinidad has shown remarkable numbers in
their indicators, as the percentage of
households with sanitary toilets in the four
endemic barangays in 2015 range from 92%
to 100%, with steady increases from the
previous year. Statistical analyses from the
study indicate that the proper use of
sanitation infrastructure significantly
contributes to the reduction of disease risk
among study participants (0.04 p-value), and
that a one-unit increase in the use of
functional, water-sealed toilets or latrines
results in a 2.01 decrease in the log-odds of
disease risk (Table 3).
Moreover, the NSCEP constantly
encourages alternative and practical
solutions, especially for a neglected tropical
disease like schistosomiasis. This includes
building safety measures such as bridges,
over bodies of water identified to have the
snail disease carrier.11 These measures are
clearly visible in Talibon and Trinidad.
Working with the RHUs, the barangay
LGUs recognize the importance of investing
in these types of complementary public
health interventions. As with other health
programs, education and advocacy play
important roles in securing the support of
LGUs and their willingness to take action.
It also increases the demand from the public
to prioritize these programs in their
communities. By taking action, it shows not
only their strong commitment in fighting the
disease, but also their active participation in
community development.
Safe Water Supplies
According to a recent report by the United
Nations, over 900 million people lack access
to safe drinking water, while 2.5 billion live
without proper sanitation.3 The WHO has
stated that “until this situation improves,
many neglected tropical diseases and other
communicable diseases will not be
eliminated, and certainly not eradicated.” 3
This perhaps is one of the most critical
roadblocks in Bohol’s path to becoming a
100% schistosomiasis-free province.
Among the four major approaches

32
recommended by DOH for disease control
and elimination, access to safe water supply
is evidently the one that needs the most
attention. Schistosomiasis is mainly
transmitted through unsanitary practices of
inhabitants in communities and their lack of
access to safe and potable water.11 For
example, many families are left no choice
but to collect water in natural reservoirs
nearest to them. The collected survey data
indicate that although a large portion of
children may have access to safe drinking
water via consumption of mineral water
bought in stores, many still tend to collect
water in streams or rivers and is used for
other household needs, such as laundry,
bathing, and cleaning. According to the
LGUs, one challenge for them is the lack of
infrastructure for water supplies as well as
incentive for water companies to build them,
limiting the amount of safe water supplies
that can reach the remote areas of the
endemic barangays. In this regard,
intersectoral discourse must be initiated and
stakeholders, both public and private, must
be engaged to find a suitable solution.
Figures 6A and 6B show the recent survey
reports of households with access to safe
water supply (at all source levels) in the
endemic barangays of the two municipalities
in the previous two years. As expected,
Talibon, being a 1st income class
community, shows the higher percentages of
households compared to Trinidad. Although
the majority has at least a 90% of total
households with access, one of its endemic
barangays, San Roque, only has 65% of
households with access. Conversely,
Trinidad’s endemic barangays have
relatively low percentages, all of which
coming below 50% (22%, 30%, 34%, and
49%). These values are corroborated by the
study results, wherein only 32.1% of the
participants reported having access to
potable water, while 67.9% are considered
without access. With further studies, such
findings could imply an indirect relationship
between the participants’ access to water
and their exposure to potential snail sites.
Figure 6A. Households with access to safe water supply in Talibon (2014; *2015 data currently unavailable)
92%
90%
95%
65%
0% 20% 40% 60% 80% 100%
San Agustin
San Carlos
San Jose
San Roque
2014

33
Figure 6B. Households with access to safe water supply in Trinidad’s endemic barangays (2014-2015)
Advocacy and Health Education Perhaps the most underrated, yet one of the
most effective tools of public health
intervention is through advocacy and health
education.24 This involves teaching citizens
of the community about best hygiene
practices, such as hand washing, proper
sanitation, and other practical preventive
measures against the disease. Furthermore,
resources from the government and other
implementing partners, such as the WHO,
will be insufficient if the people themselves
along with their local leaders do not feel
ownership and recognition of the program.
Such is attained through intensive advocacy
and social mobilization to empower and
ensure that the people possess the right
knowledge and information regarding the
disease. A fundamental and critical aspect
of Talibon and Trinidad’s success against
schistosomiasis is their understanding of the
disease, particularly the agent S.
japonicum’s life cycle. The MHOs
recognize that interrupting transmission
requires an understanding of the parasitic
life cycle.19, 20 It is one of their main
winning ingredients in their recipe for
disease control and elimination. As a result,
they continue to support and develop a
multi-component integrated approach to
fight the disease. This includes all health
intervention activities as discussed: MDA,
vector control, environmental sanitation,
safe water supplies, and health advocacy and
education. In both RHUs, health providers
regularly (e.g. NDP nurses) circulate around
endemic barangays and public schools to
teach both adults and children about
schistosomiasis, including its prevention and
treatment, emphasizing the current public
health programs being implemented. This
encourages a participatory and collaborative
environment, and strengthens the overall
structure and effectiveness of the program.
Remarkably, the results indicate that a one-
unit increase in exposure to school-related
activities (i.e. health education for
schistosomiasis) decreases the log-odds of
disease risk by 0.781 at a statistically
significant level (0.042 p-value).
55%
22%
41%
38%
30%
22%
49%
34%
0% 20% 40% 60% 80% 100%
Kinan-‐oan
Mabuhay Cabiguhan
San Vicente
Santo Tomas
2015 2014

34
Other Determinants
‘Schistosomiasis Task Force’
The DOH Region VII office has established
a ‘Schistosomiasis Task Force’ to regularly
conduct meetings, report, and assess the
overall situation of the disease in each
endemic barangay. A team for each
endemic barangay is consisted of 50
individuals representing LGU officials,
DOH representatives, and other local civil
servants.17, 18 Currently, they conduct
quarterly meetings to evaluate the status and
progress of the four major public health
programs in their respective barangays.
They are also in charge of scheduling
regular clearings of snail sites in their areas,
coordinating plans, and gathering
volunteers. The task force is composed of
the following individuals:
1 Midwife
1 Nurse
10 Barangay Health Workers
10 Barangay Officials
16 Barangay Workers
1 Barangay Nutrition Scholar (BHW)
3 Utility Personnel
3 Department of Education representatives
5 from Sectorial Working Group
- Mothers’ Organization (1)
- Pastoral (President & Secretary) (2)
- Farmers and Fishermen Organization
Representative (1)
- Women’s Association
Representative (1)
Financial Resources and Funding
The availability of budget for any public
health program is a major factor determining
its proper and timely implementation. Many
public health interventions, such as
environmental sanitation, aim to address
multiple diseases by preventing transmission
and infection. The funding provided by the
NSCEP for schistosomiasis funnels down to
the DOH Regional Office and then to the
PHO, which determines the allotment of
budgets for its municipalities based on needs
for the fiscal year. MHOs may receive
funding for specific types of intervention.
For example, the meal budget for MDA is
provided by DOH, while the LGUs may
choose to supplement an activity at their
own expense. The LGUs at the barangay
levels also receive national funding from the
Internal Revenue Allotment (IRA), and may
use part of that budget to support a public
health program. For instance, in a fiscal
year, a barangay may receive roughly 3
million pesos from IRA, of which
approximately 20% of is allocated as
Development Fund, while another 9% is

35
used for Maintenance Operation and Other
Expenses.17, 18 The endemic barangays in
Talibon and Trinidad utilize this specific
fund to subsidize sanitary toilets for families
with qualified needs. With advocacy from
the RHUs, the LGUs have prioritized and
allocated a portion of their annual budget to
support complementary public health
interventions. Through health education,
they are also aware of the benefits of
sanitary toilet provisions, which not only
help prevent disease transmission, but also
improve the overall health and wellbeing of
their communities.
Comprehensive planning and coordination
among different sectors can help detect
sources for funding and extend a program’s
lifespan. This not only saves money, but
also saves time, and promotes accountability
for sectoral groups responsible and
committed to such projects. Since the
majority of financial resources come from
the central offices, they must be more
involved and committed to adequate budget
acquisition and appropriate fund utilization.
The MHOs and LGUs are limited to what
they can accomplish in their programs by
what they have been provided and
administered to do so. Thus, the central and
local offices must work in unison to ensure
positive results from public health projects
and maximize budget efficiency.
Local Incentivization
Talibon and Trinidad have also developed
the value of incentivizing health outcomes
beyond the individual and household levels.
The Annual Foundation Day dispenses
rewards and recognition to barangays that
have attained positive health outcomes
based on specific health indicators such as
sanitation infrastructure and access to safe
water.19, 20 The annual event takes place in
February or March, and the evaluation is
conducted by officials from the LGUs and
MHOs, assessing which barangays have
achieved the highest marks from the
previous year. This creates a sense of
healthy competition among the barangays,
which motivates them to work together in
finding ways to continually improve the
health conditions in their communities.
Barangay Spot Maps
Another component of Talibon and
Trinidad’s program is the utilization of
‘barangay spot maps’. The maps show
select health indicators such as households
with unmet needs. These may vary slightly
by barangay, but generally, they include
income level, indicators for maternal and

36
child health, environmental sanitation
indicators such as sanitary toilets, access to
safe drinking water, and even house
construction materials. 17, 18 Every
household in the barangay is accounted for,
with the BHWs responsible for collecting
the data and updating them on an annual
basis. This is extremely useful for the
disease control and elimination efforts of
schistosomiasis, as they provide the most
reliable information to LGUs and RHUs that
determine unmet needs and other ways to
improve specific elements of a given public
health intervention.
CONCLUSION
Design Critique & Limitations Considering the timeline of two and a half-
months (September-November), the project
benefitted from having a nested case-control
study design, as they are generally simple to
organize. By retrospectively comparing two
groups within a nested sample, we were able
to identify predictors of an outcome (i.e.
how public health interventions affect the
risk for S. japonicum infections). To assess
the influence of predictors on the outcome,
we then calculated the odds ratio of disease
risk based on exposure. Nevertheless, as
with any other studies, a case-control design
has its limitations. This includes sample bias
(i.e. where we obtained our cases and
controls), as well as observation and recall
biases (e.g. from the participant, the
investigator, and/or data collectors). Specific
characteristics of the participants selected
also determine the bounds for which we can
make generalizations for the larger
population groups (i.e. external validity).
Lastly, this type of study design allows us to
look at only one outcome, since we recruited
based on disease status. To mitigate some of
these weaknesses, we maximized the
number of our control group (n=250), and
recruited our controls from the same pool
(i.e. age range, residential geography,
school, etc.) that was tested for ELISA
Ab/Ag. In theory, this should yield similar
chances of risks for the disease and chances
of exposure to any given intervention.
Careful consideration of other confounding
factors should therefore result in more
robust and reliable conclusions.
Current Needs & Future Outlook
Most of the routine data collection for this
case study took place in the last quarter of
2015. Although the areas of concern are

37
diverse, immediate attention is needed to
address issues related to both the short and
long-term successes of public health
programs currently in place. Along with the
quantitative results, the recommended
course of action is to carefully examine the
following items in order to support and
further enhance the schistosomiasis control
and elimination program in Bohol.
¨ Provision of safe water supplies: As
indicated, recent data suggest that
there is a significant need for
families in the endemic areas to have
better access not only to potable
water, but also for other daily
household use.
¨ Agricultural sector: Considerations
of treating animals (i.e. bovine or
farm animals) with praziquantel.
Although they conduct regular
deworming and treatment of farm
animals for other diseases, there is
currently no available treatment for
schistosomiasis in animals. Other
alternatives, such as the use of
machinery should also be explored to
address the risks posed by disease
transmission in animals.24, 25
¨ Malacological trainings: There
should be a concerted effort to
increase and develop the surveillance
and surveying of the snail vectors.24
¨ Health Education & Awareness: As
reinforced by the study, these
components play a vital role and
should not only be sustained, but
also continually improved upon.
Recommendations for Future Study & Final Remarks
The study could be greatly enhanced in the
future by utilizing GIS technology and
techniques that could provide more definite
geographical clues and epidemiological
support, especially in evaluating residual
infections that still persist in the region.
Surveys could also be applied to a larger
population sample, or other at-risk
subgroups of the community, which will
likely increase the study’s external validity
and reliability.
Moving forward, both MHOs in Talibon and
Trinidad believe that with the current
progress of their strategies to tackling
schistosomiasis, the road to elimination is
not far in sight. Timely MDA, proper
environmental sanitation, added focus on
animal transmission, consistent modification
of endemic sites, advocacy and health
education, and diligent surveillance that

38
involves active case finding and treatment,
all contribute to their success. Coordination
with the LGUs, particularly at the barangay
levels, must be maintained and amplified as
necessary. Those involved must realize that
ending the neglect will never be successful
without the full cooperation of the local
communities at risk. The experience of
Bohol and its two endemic municipalities
can serve as useful blueprints for other areas
in the country that continue to suffer from
the heavy burden of this disease. Each area
may bring unique challenges that are
specific to the capacity of the current system
in place. Nonetheless, with strong
commitment and by cultivating a synergistic
intersectoral collaboration among all
stakeholders involved, as Bohol has aptly
demonstrated, the foundation and path to
disease elimination can be decisively laid.

39
REFERENCES 1Olveda, D. U., Li, Y., Olveda, R. M., Lam, A. K., McManus, D. P., Chau, T. N., . . . Ross, A. G.
(0910). Bilharzia in the Philippines: Past, present, and future [Bilharzia; Control;
Philippines; Schistosoma japonicum; Schistosomiasis. 10.1016/j.ijid.2013.09.011 [doi].
2World Health Organization. (2010). Working to overcome the global impact of neglected
tropical diseases. (First WHO report on neglected tropical diseases No. 1). Geneva,
Switzerland: WHO Press.
3World Health Organization. (2012). Accelerating work to overcome the global impact of
neglected tropical diseases: A roadmap for implementation. (Executive Summary).
Geneva, Switzerland: WHO Press.
4Akullian, N. A. (2007). Spatial patterns of schistosomiasis: A watershed approach to measuring
S. japonicum environmental risk and human and animal disease outcomes. Providence:
Brown University.
5World Health Organization. (2013). Schistosomiasis: Progress Report 2001-2011 and Strategic
Plan 2012-2020. France: World Health Organization.
6World Health Organization. (2015). Schistosomiasis: A major public health problem. Retrieved
from http://www.who.int/schistosomiasis/en/
7Blas, B. L. (Ed.). (1988). Surveys, studies, and control work on schistosoma japonicum infection
in the Philippines. Manila: Schistosomiasis Control Service, DOH.
8Blas, B. L., Velasco, P. F., Alialy, O. B., Basas, J. C., & Bautista, E. S. (1990). Epidemiology
and control of schistosomiasis in the Philippines. (Review). Manila, Philippines:
Schistosomiasis Control Service, DOH.

40
9Blas, B. L., & Dazo, B. C. (1968). Schistosomiasis survey and preliminary control work in the
province of Bohol. The Journal of the Philippine Medical Association, 44(2), 80-87.
10Palasi, W. A. (2015). Schistosomiasis in the Philippines. (Presentation). Manila: Department of
Health: Disease Prevention and Control Bureau.
11Department of Health, P. (2014). Neglected tropical diseases in the Philippines (1st ed.). Sta.
Cruz, Manila: National Disease Prevention and Control Bureau, DOH.
12Blas, B. L., Bautista, E. S., & Lipayon, I. L. (Eds.). (1990). An atlas on the endemicity of
Schistosomiasis japonica in the Philippines (2nd ed.). Manila: Schistosomiasis Control
Service, Department of Health.
13A national baseline prevalence survey of schistosomiasis in the Philippines using stratified
two-step systematic cluster sampling design (2012). Retrieved from
http://dx.doi.org/10.1155/2012/936128
14National Schistosomiasis Control and Elimination Program (Ed.). (2012). Schistosomiasis:
Clinical practice guidelines for the diagnosis, treatment, and prevention of Schistosoma
japonicum infections in the Philippines: 2012 update. Manila: Department of Health.
15National Schistosomiasis Control and Elimination Program. (2015). Sentinel surveillance
report 2009-2014. (Surveillance). Manila: Department of Health: NSCEP.
16Belizario, V. J., Gabanuda, R. R., Amarillo, M. L., & de Veyra, C. (2015). Assessment of
schistosomiasis endemic areas through parasitological and serological techniques. (Final
Report). Manila: University of the Philippines, Manila.
17Talibon Municipal Health Office. (2015). Routine data collection in Talibon's rural health unit.
(Health Reports). Talibon, Bohol: Talibon RHU.

41
18Trinidad Municipal Health Office. (2015). Routine data collection in Trinidad's rural health
unit. (Health Reports). Trinidad, Bohol: Trinidad RHU.
19Ngoboc, F. (2015). In de Guzman C. (Ed.), Interview with the municipal health officer of
Talibon, Bohol. Manila: Department of Health, Philippines.
20Auza, A. N. (2015). In de Guzman C. (Ed.), Interview with the municipal health officer of
Trinidad, Bohol. Manila: Department of Health, Philippines.
21Lin, D. D., Fau, L. J., Hu, F., Wu, H. W. (0909). Routine Kato-Katz technique underestimates
the prevalence of Schistosoma japonicum: A case study in an endemic area of the
People's Republic of China.
22Hairston, N. G., & Santos, B. C. (1961). Ecological control of the snail host of Schistosoma
japonicum in the Philippines. Bulletin of the World Health Organization, 25(4-5), 603-
610. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2555717/
23Ross, A. G., O. R., Acosta L., Harn, Donald,A., H. D., Chy, D. F., Li Y., Gray, Darren, J., . . .
Williams, G. M. (0707). Road to the elimination of schistosomiasis from Asia: The journey
is far from over [Asia; Control; Elimination; Neglected tropical disease; Schistosomiasis
AID - S1286-4579(13)00152-4 [pii] AID - 10.1016/j.micinf.2013.07.010 [doi].
24Wang, L., Chen, H., Guo, J., Zeng, X., Hong, X., Xiong, J., . . . Zhou, X. (2009). A strategy to
control transmission of schistosoma japonicum in China. N Engl J Med, 360(2), 121-128.
doi:10.1056/NEJMoa0800135
25Fernandez, T., Jr., T. M., Balolong E., Jr., Joseph, L., Joseph L., Willingham,
A.L., 3rd, W. A., Belisle P., Webster, J.P., . . . Carabin, H. (0927). Prevalence of
Schistosoma japonicum infection among animals in fifty villages of Samar province, the
Philippines.

42
APPENDIX
Figure 1. Historical evolution of schistosomiasis control in the Philippines
• 1st case reported 1906
• Recognized as a public health concern 1953
• Schistosoma japonicum regions classified 1975
• Praziquantel introduced • Control shifted from a case-by-case basis to a chemotheraphy-based program
1980
• Intensified case-finding and treatment in all endemic areas 1990
• Decreased financial capacity and support led to loss of control teams in each of the endemic municipalities
• Transition of control program to Mass Drug Administration (MDA)
1995

43
Figure 2A. Map of Bohol and the two endemic municipalities

44
Figure 2B. Map of Talibon with markers for its 4 endemic barangays

45
Figure 2C. Map of Trinidad with markers for its 4 endemic barangays

46
DISEASE PREVENTION & CONTROL BUREAU
Infectious Disease Of/ice (IDO)
Elimination Division
Malaria Rabies
Leprosy Neglected Tropical Diseases
Lympathic Filariasis
Schistosomiasis
Prevention & Control Division
Integrated Helminth Control Program
Environmental & Occupational Health
Of5ice (EOHO)
Degenerative Disease Of5ice (DDO)
Family Health Of5ice (FHO)
Figure 3A. Organizational structure
of schistosomiasis control in the
Philippines’ Department of Health
DEPARTMENT OF HEALTH
Regional Health OfWice
Provincial DOH OfWice
Development Management OfWicer
Provincial Health OfWicer
Municipal Health OfWicer (Rural Health
Unit (RHU))
Barangay Health Station Midwife
Public Health Nurse
Sanitation Inspector
Medical Technologist
Nurse Deployment Program (NDPs)
Figure 3B. Hierarchical structure of DOH’s administrative system

47
Restituto B. Auxtero , CPA
(Municipal Mayor)
Dr. Francisco C. Ngoboc, Jr.
(Municipal Health Officer)
Simplicio L. Torreon
(DOH Representativ
e)
Mario Carusos
Provincial Sanitation Inspector I
Jocelyn C. Evangelista
( M
unicipal Nurse )
Jona
A. A
lvarez
( M
unicipal Nurse )
Ma. Tan
ia Dolorito
s ( M
unicipal Nurse )
ZONE 1
Poblacion RH
M
Eugenia Jasm
in (M
idwife III)
Sag RH
M
Editha Polo (RHM)
Nocnocan RH
M:
Angelita Lugod (RHM)
Charito Cresencio (RHM)
ZONE 3
San Jose RHM:
Marivelle Salicina (Midwife II)
Balitaw
ak RHM:
Natividad Abastas (M
idwife II)
Madonna Tidong (RHM)
ZONE 5
San Agustin RHM:
Cecile Garcia ( RHM)
Zamora RHM:
Imelda Bongao (RHM)
ZONE 10
Suba RHM
Lorna Menesis (M
idwife III)
Busalian RH
M
Jennelyn Casam
ayo (RHM)
Cataban RH
M:
Estrella Saludo (RHM)
ZONE 7
San Carlos RHM
Luzviminda Juntilla (Midwife III)
Sto. Nino RH
M
Wellina Gonzaga (RHM)
Sikatuna RHM:
Marivic Rosales (RHM)
Anecita P. Paredes
PHN ( Nurse II)
ZONE 2
San Francisco RHM:
Rem
edios Mum
ar (M
idwife III)
Risara Buri (RH
M)
Tangaligue RHM:
Vivian Sabior (RHM)
ZONE 4
San Isidro RHM:
Teresita Rosales (M
idwife II)
San Pedro RH
M:
Rhea Meijas (RHM)
ZONE 6
San Roque RHM:
Fredelina Polestico (Midwife II)
Magsaysay RHM:
Milquedesa Deocariza (RHM)
ZONE 8
Bagacay RHM:
Isaida Garcia (Midwife II)
Burgos RHM:
Joaniflor Tubo (RHM)
Rizal RHM:
Neria Bitoonan (RHM)
ZONE 10
Calituban RHM:
Elsa Cabugason (M
idwife II)
Ana Mae Gabison (RHM)
Guindacpan RHM:
Estrella Torrevillas (RHM)
Mahanay RHM:
Dom
inga Cabilez(RH
M)
Melchor Carcallas
Municipal Sanitation Inspector I
Talibon Municipal Birthing
Center
Natividad Abastas
( Midwife II)
Ma. Concepcion Lincuna
(Mun. Nurse)
Charito Cresencio
(RHM)
Leah Evangelista
(Mun. Nurse)
Arlene
Garcia/ Vicen
ta Can
tone
s (Birthing
Aide)
Jhona Mum
ar
(Clerk)
Imperatriz Boiser
(Encoder)
Gorgonio Cantones
(Utility/Carpenter)
An
a Breche
l A. Eyas
(San
itatio
n Aide
)
Clau
dio Evan
gelista
(San
itatio
n Aide
)
Rhoda Bernales
Microscopist
Re
na Ombo
y (Lab
oratory Aide)
NDP Nurses
Ariane N. Madlangbayan
Jesfer G. Ngoboc
Melisa Mae B. Carcallas
Dianne Zen A. Avenido
Lady Lou S. Auguis
Peter Jane Q. Diacor
Jhenlee B. Valmores
Fatim
a Joie R. Autentico
Marimar S. Salise
HFEP Nurse
Diona C. Auza
Franknel A. Ngoboc
Figure 3C. Talibon Municipal Health
Office Organizational Chart (2015).
(Similar to Trinidad)

48
Annex 4: Questionnaire Form 37 Questions 1. Please record the subject's unique ID number. 2. Please record the subject's gender. Choose one response - Male - Female 3. When is your birthdate? 4. What is the highest level of education your parents have completed? Choose one response - Elementary - High School - College - Post graduate or Advance degree - I don't know 5. Which category best describes your annual household income? Choose one response - <5000 pesos - 5000 – 15,000 pesos - 15,000 – 25,000 pesos - 25,000 – 50,000 pesos - 50,000 pesos or more - I don't know 6. Before 2014, how many times did you participate in the annual ‘Mass Drug Administration’ for schistosomiasis (and was administered with praziquantel)? Choose one response - Never - 1 time - 2 times - 3 times - 4 times - 5 times or more - I'm not sure 7. Before 2014, did you know why you took praziquantel? Choose one response - Yes - No If this response, jump to 9 - I'm not sure If this response, jump to 9
8. If yes, please specify. 9. I believe that taking praziquantel will help me prevent from getting infected by schistosomiasis. Choose one response - Yes - No - I'm not sure 10. Before 2014, I had experienced adverse events from taking praziquantel. Choose one response - Yes - No If this response, jump to 13 - I'm not sure If this response, jump to 13 11. If yes, which times? Choose one response - The first year - Every year - It varied 12. Those adverse events included: (Check all that apply.) Choose all that apply - Dizziness - Headache - Malaise - Drowsiness - Fatigue - Abdominal pain - Diarrhea - Vomiting - Nausea - Bodily pain - Fever - Numbness - Others not listed 13. I plan on continuing my participation with the annual MDA as recommended by the Department of Health and as provided and implemented in my local municipality. Choose one response - Yes - No

49
14. At home, what kind of water are you drinking now? Choose one response - Mineral water (e.g. bottled products, delivered water from store) - Boiled water - Tap water (gripo) - Pump/borehole water (poso) - Well water (balon) - Rainwater - Water from stream, creek, or river 15. Before 2014, what was the best available water you drank at home? Choose one response - Mineral water (e.g. bottled products, delivered water from store) - Boiled water - Tap water (gripo) - Pump/borehole water (poso) - Well water (balon) - Rainwater - Water from stream, creek, or river 16. Before 2014, did you have a functional toilet/latrine that you used regularly at home? Choose one response - Yes If this response, jump to 18 - No 17. If not, where did you usually go when you needed to use the bathroom (to defecate/urinate)? (Check all that apply.) Choose all that apply - Communal/shared restroom - Dug pit in the ground - Any open space in the backyard - Closest stream, creek, or river - Anywhere it is convenient 18. What other methods did your family use to dispose of feces? (Check all that apply.) Choose all that apply - In the trash that is collected by the barangay or the municipality - Burned in our backyard - Buried in the ground - In the nearby stream, creek, or river - Thrown anywhere convenient
- Other places not listed above - Not applicable 19. If "Other places..." was selected, please specify. If not, skip this question. 20. Before 2014, did you wash your hands regularly after you use the toilet? Choose one response - Yes - No If this response, jump to 22 21. If yes, did you wash your hands with soap? Choose one response - Yes - No 22. Before 2014, at school, did you wash your hands after you use the toilet? Choose one response - Yes - No If this response, jump to 24 23. If yes, did you wash your hands with soap? Choose one response - Yes - No 24. Before 2014, did you allow any animals or pets (dogs, cats, rats etc.) to roam freely inside and outside your house? Choose one response - Yes - No - Not applicable 25. Before 2014, did you keep any farm animals (e.g. pigs, water buffalos (kalabaw), or cows) in fenced or properly secluded areas? Choose one response - Yes - No - Not applicable 26. Before 2014, did you regularly wash your clothes in creeks, streams, or rivers? Choose one response - Yes

50
- No If this response, jump to 28 27. Please provide the name of the site where you regularly washed your clothes. 28. Before 2014, did you bathe or swim in ponds, creeks, streams, or rivers? Choose one response - Yes - No If this response, jump to 30 29. Please provide the name of the site where you bathed. 30. Before 2014, did you collect water from creeks, streams, or rivers? Choose one response - Yes - No If this response, jump to 32 31. Please provide the name of the site where you collected water. 32. Before 2014, I have seen or notice warning signs about schistosomiasis posted around my community within: Choose one response - The past 6 months - The past year - The past 5 years or more - I don’t remember seeing any 33. Before 2014, I have seen or participated in school advocacy campaigns for schistosomiasis: Choose one response - The past 6 months - The past year - The past 5 years or more - I don’t remember seeing any 34. Before 2014, I have seen or notice advertisements about schistosomiasis on one or more of the following mediums: (Check all that apply.) Choose all that apply - TV - Radio - Magazine - Newspaper - Internet - None of the above - Others not listed above 35. If "Others..." was selected, please specify. If not, skip this question.
36. Scan your GPS coordinates. 37. End of Survey. Thank you for participating!