Embed Size (px)
Citation preview

Ahuja and Cagna
It is important to diagnostically evaluate available restorative space prior to implant placement. Failure to accurately assess restorative space may result in esthetically and structurally compromised prostheses and patient dissatisfaction. This article describes various techniques for evaluating restorative space in edentulous patients. Information gained will help dentists during treatment planning, attachment selection, and prosthesis design prior to surgical implant placement. (J Prosthet Dent 2010;104:133-136)
Defining available restorative space for implant overdentures
Swati Ahuja, BDS, MDS,a and David R. Cagna, DMD, MSb
University of Tennessee Health Science Center, College of Dentistry, Memphis, Tenn
aAssistant Professor, Department of Restorative Dentistry.bProfessor and Director, Advanced Prosthodontics Program, Department of Restorative Dentistry.
Adequacy of restorative space is an important consideration in successful implant overdenture therapy.1 Often mistaken for interarch distance, re-storative space can be defined as the 3-dimensional (3-D) oral space avail-able to receive the proposed prosth-odontic restoration. In edentulous patients, available restorative space is bounded by the occlusal plane, sup-porting tissues of the edentulous jaw, facial tissues (cheeks and lips), and the tongue. For implant overdenture patients, this space must accommo-date a denture base of sufficient di-mensions, appropriately positioned denture teeth, and an implant attach-ment system. Factors such as interoc-clusal rest space, phonetics, and es-thetics must also be considered when defining available restorative space.
Critical evaluation of available re-storative space during the diagnostic phase of implant overdenture therapy is necessary.2 All too often, this im-portant factor is first assessed follow-ing implant placement, when prosth-odontic alternatives are limited. Attempts to fabricate prostheses with inadequate restorative space may re-sult in physiologically inappropriate contours, structurally weak prosthe-ses, esthetic compromise, encroach-ment into interocclusal rest space,
and/or suboptimal retention and sta-bility of the treated result.1
A reported minimum space require-ment for implant-supported overden-tures with Locator attachments (Zest Anchors, Escondido, Calif ) is 8.5 mm of vertical space and 9 mm of hori-zontal space.3 A separate report on maxillary implant overdentures sug-gested that a minimum of 13-14 mm of vertical space is required for bar-supported overdentures, and 10-12 mm for overdentures supported by individual attachments.4
The restorative dentist must be equipped with clinical tools and di-agnostic procedures that define avail-able restorative space. These proce-dures should be implemented prior to implant placement, when treatment options are being considered. The purpose of this report is to detail 2 procedures for diagnosing available restorative space for implant overden-tures prior to implant placement.
Matrix capture of denture teeth
With patient-approved wax trial dentures on their respective articula-tor-mounted casts, fabricate 1 of 2 denture tooth matrixes: a facial ma-trix or an occlusal matrix. To fabricate a facial denture tooth matrix, use ei-
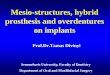
ther dental stone (Microstone; Whip Mix Corp, Louisville, Ky) or laborato-ry putty (Lab-Putty; Coltène/Whale-dent, Inc, Cuyahoga Falls, Ohio). Place keyways in the land area of the cast to assist in accurate removal and repositioning of the completed defini-tive matrix. To fabricate a dental stone matrix, use rope wax (Wax Square Ropes; Heraeus Kulzer, Armonk, NY) to physically define the area of the planned matrix (Fig. 1). Apply an ap-propriate separator to the stone cast (Super-Sep; Kerr Corp, Orange, Ca-lif ). Next, with the wax trial denture sealed to the edentulous cast, apply a 5-mm layer of dental stone (Micros-tone; Whip Mix Corp) to facial, oc-clusal, and incisal aspects of the trial denture, engaging the land area of the cast and all prepared keyways. When the dental stone has set, eliminate all wax using boiling water, remove the matrix from the cast, trim as needed, and reposition any displaced denture teeth into the matrix. Replace the ma-trix on the edentulous cast and visu-ally assess available restorative space from a lingual perspective (Figs. 2 and 3). The vertical and horizontal restor-ative space can be assessed using a measuring tool, such as a periodontal probe.
To fabricate an occlusal denture
134 Volume 104 Issue 2
The Journal of Prosthetic Dentistry Ahuja and Cagna
tooth matrix, seal the wax trial den-ture to the edentulous cast in the articulator. Adapt laboratory putty (Lab-Putty; Coltène/Whaledent, Inc) to the occlusal and incisal thirds of the denture teeth. Integrate retentive features in the putty, such as under-cut areas or incorporated paper clips. With the occlusal matrix accurately positioned on the wax trial denture, mount the matrix to the opposing member of the articulator with den-tal stone (Mounting Stone; Whip Mix Corp). When the mounting stone has set, open the articulator, remove the wax trial denture from the cast, re-move the denture teeth from the wax trial denture, and reposition the teeth into the occlusal matrix (Fig. 4). Close the articulator and observe the rela-tionship between the denture teeth and the associated edentulous ridge (Fig. 5).
Both facial and occlusal denture tooth matrixes permit 3-D visualiza-tion of the available space between the denture teeth of the planned pros-thesis and the edentulous ridge. How-ever, with elimination of the denture base to gain visual access to the full contour of the denture teeth, informa-tion critical to calculation of available restorative space may also be eliminat-ed. Additionally, denture tooth matrix-es do not permit direct visualization of available osseous structures neces-sary to accurately coordinate implant position and trajectory with available restorative space.
CBCT and computer-based planning
Develop a wax trial denture using standard techniques5 and process the trial denture into a radiographic tem-plate. With the radiographic template
properly seated intraorally, acquire a cone beam computerized tomography (CBCT) image.6 Evaluate tomographic information using one of several com-puter software programs designed for this task (NobelGuide; Nobel Biocare USA, Yorba Linda, Calif; or SimPlant; Materialise Dental, Glen Burnie, Md). In general, these computer-based di-agnosis and treatment planning tools permit: (1) visualization of osseous structures in various 3-D and cross-sectional perspectives; (2) visualiza-tion of the planned prosthesis in 3 dimensions and its relationship to underlying bone; (3) visualization of available restorative space in 3 dimen-sions to assist in prosthesis design and attachment selection; (4) virtual placement of dental implants in bone; and (5) fabrication of accurate and stable surgical templates7 (Fig. 6).
3 Measurement of vertical restorative space using stone facial matrix.
4 Repositioning denture teeth in occlusal matrix.
2 Stone facial matrix positioned accurately on cast. 1 Preparation of cast for fabrication of stone facial matrix.
135August 2010
Ahuja and Cagna
Other methods of space assessment
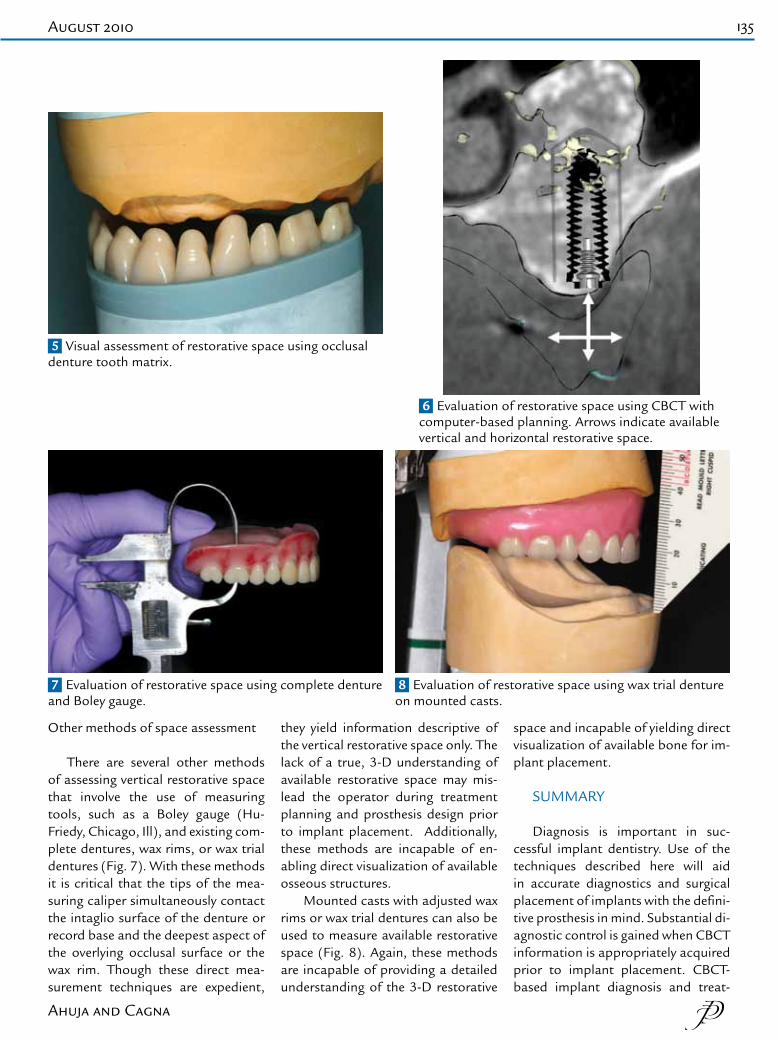
There are several other methods of assessing vertical restorative space that involve the use of measuring tools, such as a Boley gauge (Hu-Friedy, Chicago, Ill), and existing com-plete dentures, wax rims, or wax trial dentures (Fig. 7). With these methods it is critical that the tips of the mea-suring caliper simultaneously contact the intaglio surface of the denture or record base and the deepest aspect of the overlying occlusal surface or the wax rim. Though these direct mea-surement techniques are expedient,
they yield information descriptive of the vertical restorative space only. The lack of a true, 3-D understanding of available restorative space may mis-lead the operator during treatment planning and prosthesis design prior to implant placement. Additionally, these methods are incapable of en-abling direct visualization of available osseous structures.
Mounted casts with adjusted wax rims or wax trial dentures can also be used to measure available restorative space (Fig. 8). Again, these methods are incapable of providing a detailed understanding of the 3-D restorative
space and incapable of yielding direct visualization of available bone for im-plant placement.
SUMMARY
Diagnosis is important in suc-cessful implant dentistry. Use of the techniques described here will aid in accurate diagnostics and surgical placement of implants with the defini-tive prosthesis in mind. Substantial di-agnostic control is gained when CBCT information is appropriately acquired prior to implant placement. CBCT-based implant diagnosis and treat-
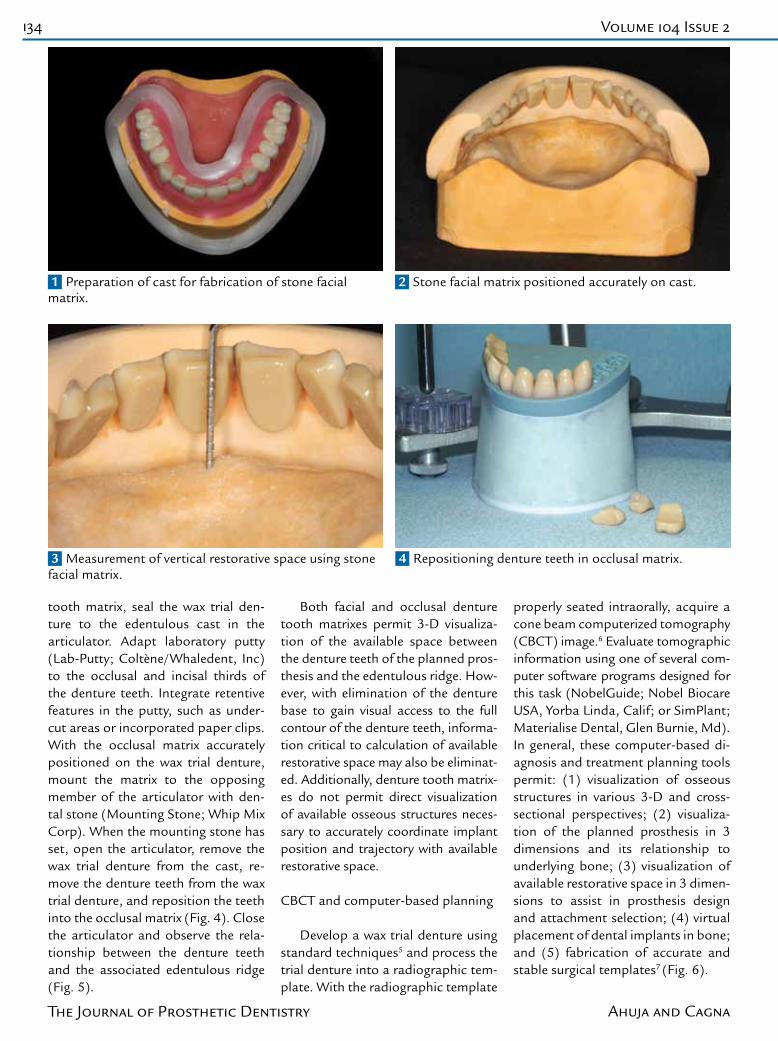
5 Visual assessment of restorative space using occlusal denture tooth matrix.
6 Evaluation of restorative space using CBCT with computer-based planning. Arrows indicate available vertical and horizontal restorative space.
7 Evaluation of restorative space using complete denture and Boley gauge.
8 Evaluation of restorative space using wax trial denture on mounted casts.

136 Volume 104 Issue 2
The Journal of Prosthetic Dentistry Ahuja and Cagna
ment planning permit detailed 3-D visualization of available restorative space and its relationship to available osseous structures. Supported by clinical fabrication of a radiographic template that accurately represents planned prosthesis contours, predict-able implant placement and accurate definitive prosthesis fabrication are possible.
REFERENCES
1. Chaimattayompol N, Arbree NS. Assess-ing the space limitation inside a complete denture for implant attachments. J Prosthet Dent 2003;89:82-5.
2. AbuJamra NF, Stavridakis MM, Miller RB. Evaluation of interarch space for implant restorations in edentulous patients: a laboratory technique. J Prosthodont 2000;9:102-5.
3. Lee CK, Agar JR. Surgical and prosthetic planning for a two-implant-retained mandibular overdenture: a clinical report. J Prosthet Dent 2006;95:102-5.
4. Sadowsky SJ. Treatment considerations for maxillary implant overdentures: a system-atic review. J Prosthet Dent 2007;97:340-8.
5. Zarb GA, Bolender CL, Eckert SE, Jacob RF, Fenton AH, Mericske-Stern R. Prosth-odontic treatment for edentulous patients: complete dentures and implant-supported prostheses. 12th ed. St. Louis: Elsevier; 2003. p. 268-96.
6. Verstreken K, Van Cleynenbreugel J, Marchal G, Naert I, Suetens P, van Steenberghe D. Computer-assisted planning of oral implant surgery: a three-dimensional approach. Int J Oral Maxillofac Implants 1996;11:806-10.
7. Van Steenberghe D, Glauser R, Blombäck U, Andersson M, Schutyser F, Pettersson A, et al. A computed tomographic scan-derived cus-tomized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a pro-spective multicenter study. Clin Implant Dent Relat Res 2005;7 Suppl 1:S111-20.
Corresponding author:Dr Swati AhujaUniversity of Tennessee Health Science CenterCollege of DentistryDepartment of Restorative Dentistry, S-501875 Union AveMemphis, TN 38163Fax: 901-448-1294E-mail: [email protected]
Copyright © 2010 by the Editorial Council for The Journal of Prosthetic Dentistry.
Noteworthy Abstracts of the Current Literature
Mold filling and dimensional accuracy of titanium castings in a spinel-based investment
Fischer J, Ebinger A, Hägi T, Stawarczyk B, Wenger A, Keller E.Dent Mater 2009;25:1376-82. Epub 2009 Aug 7.
Objectives. Aim of the study was to analyze the mold filling capacity and the dimensional accuracy of a spinel-based investment for titanium castings.
Methods. Expansion of the investment in dependence of the preheating temperature was measured in a dilatometer. The degree of transformation of MgO and Al2O3 to spinel (MgAl2O4) was evaluated by means of X-ray powder dif-fraction. Mold filling capacity was assessed by casting a grid and calculating the percentage of completed segments. Dimensional accuracy was analyzed by casting a hollow cylinder and measuring the difference between the inner diameter of the resin pattern and the resulting titanium casting.
Results. Spinel formation starts at 819°C. Diffraction patterns prove the formation of spinel from MgO and Al2O3. The amount of spinel increases with increasing preheating temperature. The final expansion of the investment at the end of the preheating cycle at 450°C shows a linear correlation to the maximum preheating temperature. The degree of mold filling is reciprocal to the preheating temperature. The dimensional accuracy shows a linear correlation to the amount of spinel. Best dimensional accuracy was obtained at about 900°C. After a preheating temperature of 884°C, as recommended by the manufacturer, the cast specimens showed a slightly lower inner diameter as compared to the resin patterns.
Significance. The results suggest that with the spinel investment analyzed an excellent accuracy of titanium castings may be obtained.
Reprinted with permission of the Academy of Dental Materials.