Embed Size (px)
Citation preview
11/5/2020
1
Deeper Dive Into Office Visit E/M Services for CPT 2021
Karen Scott, MEd, RHIA, CCS‐P, CPC, FAHIMA
Effective Date
• Jan 1, 2021
• CPT working with CMS to assist with transition
• AMA “major commercial payers 100% said they would be adopting new E/M Guidelines”
1
2
11/5/2020
2
Only Office Visits
• Changes specific only to Office or Other Outpatient Services (99201‐99205 and 99211‐99215) codes
• Deletion of 99201
• New guidelines specific to 99202‐99215
• Changes in component scoring for both new and established patient codes (99202‐99215)
• Changes to the medical decision‐making table
• Changes to the typical times associated with each E/M code (99202‐99215)
Medicare Guidelines
• Still use all other guidelines shown in CPT
• Medicare 1995 or 1997 Guidelines
• All other E&M Codes• Observation
• Hospital Inpatient
• Consultation
• ED
• Critical Care
• Nursing Facility, Assisted Living, Home Visits, etc.
3
4
11/5/2020
3
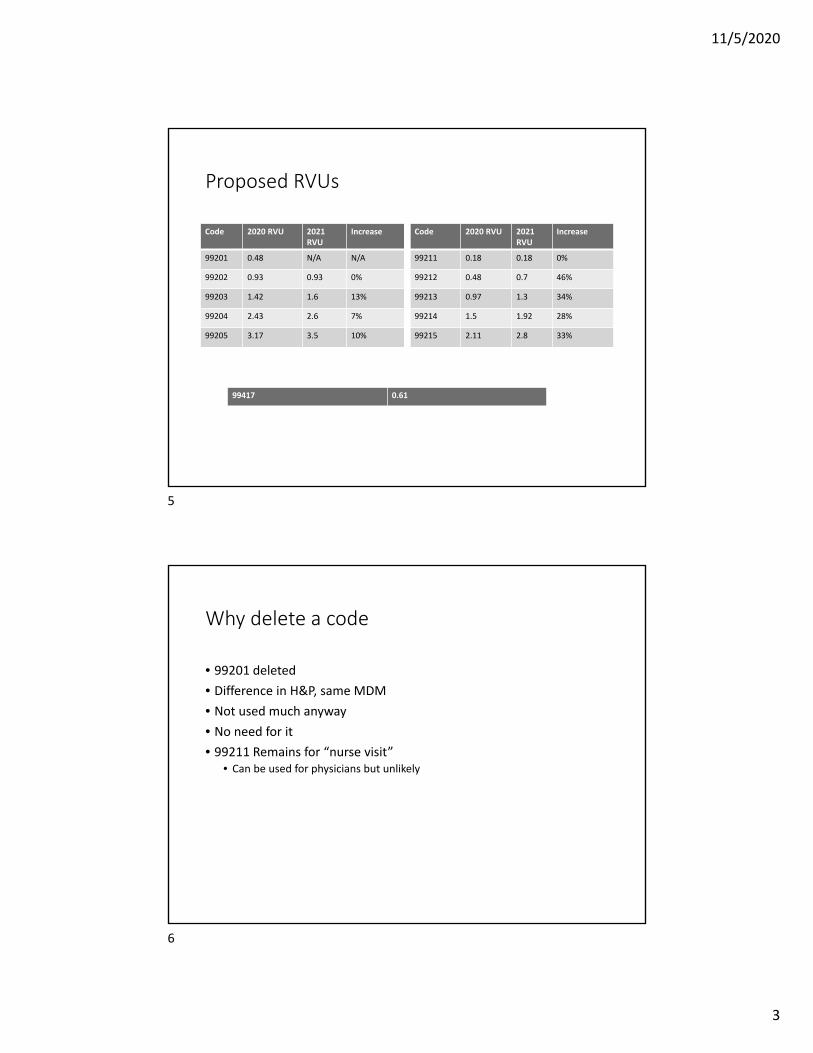
Proposed RVUs
Code 2020 RVU 2021 RVU
Increase
99201 0.48 N/A N/A
99202 0.93 0.93 0%
99203 1.42 1.6 13%
99204 2.43 2.6 7%
99205 3.17 3.5 10%
Code 2020 RVU 2021 RVU
Increase
99211 0.18 0.18 0%
99212 0.48 0.7 46%
99213 0.97 1.3 34%
99214 1.5 1.92 28%
99215 2.11 2.8 33%
99417 0.61
Why delete a code
• 99201 deleted
• Difference in H&P, same MDM
• Not used much anyway
• No need for it
• 99211 Remains for “nurse visit”• Can be used for physicians but unlikely
5
6
11/5/2020
4
How to select a code
• 1. The level of the medical decision making as defined for each service; or
• 2. The total time for E/M services performed on the date of the encounter.
7
Other Guidelines
• H&P• Medically appropriate‐not key elements
• Number and Complexity of Problems Addressed• Can address new and/or established problems
• Underlying diseases are not considered unless they are addressed and• Presence increases amount/complexity of data reviewed/analyzed
• Or risk of complications and/or morbidity/mortality
8
7
8
11/5/2020
5
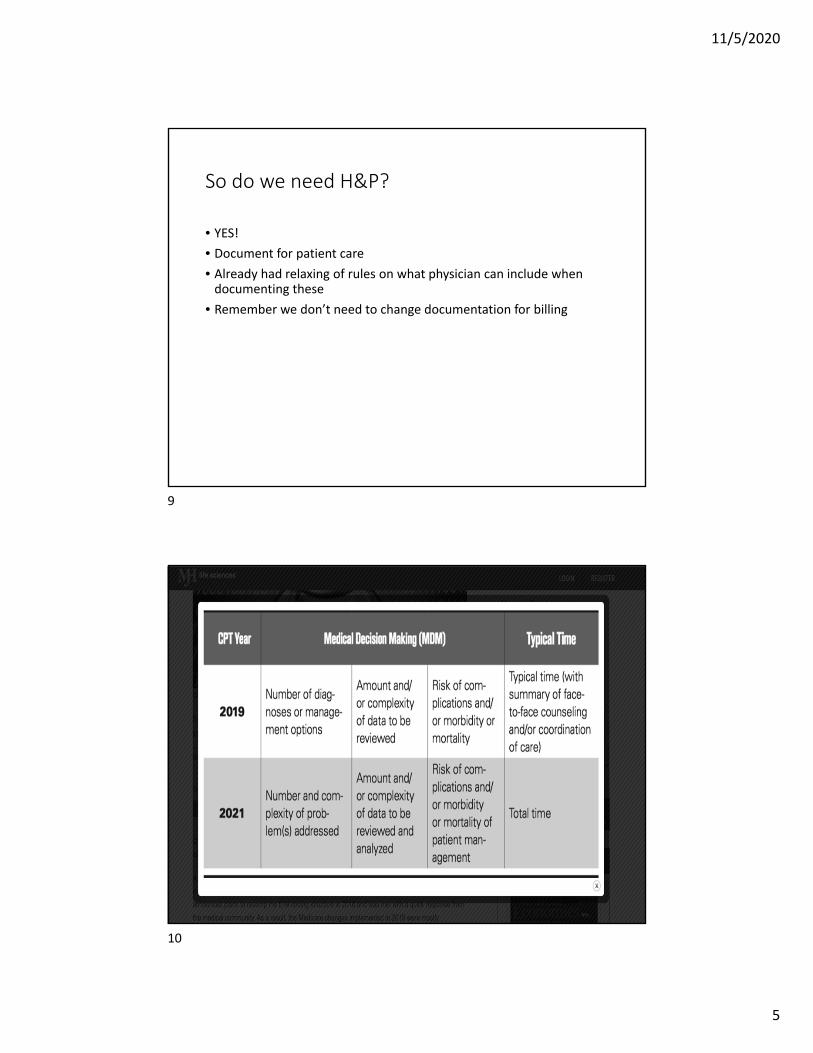
So do we need H&P?
• YES!
• Document for patient care
• Already had relaxing of rules on what physician can include when documenting these
• Remember we don’t need to change documentation for billing
9
10
11/5/2020
6
Time Based Leveling
• Time
• Changing from “implicit” to “explicit”
• Implied vs. absolute
• “time alone may be used to select the appropriate code level” for office/outpatient E&M
• Time spent counseling no longer counted• Doesn’t have to dominate the visit (no more greater than 50%)
11
Total time
• For office visits
• Total time on date of encounter
• Face to face and non included
• Not time by clinical staff
12
11
12
11/5/2020
7
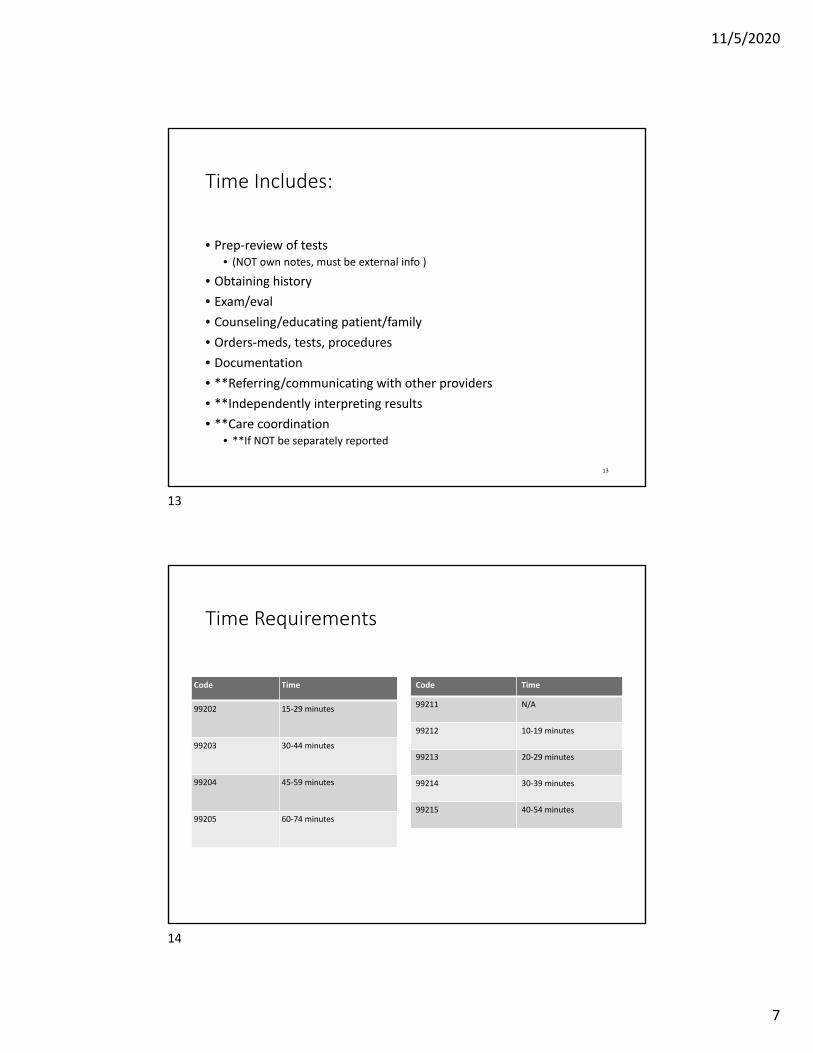
Time Includes:
• Prep‐review of tests• (NOT own notes, must be external info )
• Obtaining history
• Exam/eval
• Counseling/educating patient/family
• Orders‐meds, tests, procedures
• Documentation
• **Referring/communicating with other providers
• **Independently interpreting results
• **Care coordination • **If NOT be separately reported
13
Time Requirements
Code Time
99202 15‐29 minutes
99203 30‐44 minutes
99204 45‐59 minutes
99205 60‐74 minutes
Code Time
99211 N/A
99212 10‐19 minutes
99213 20‐29 minutes
99214 30‐39 minutes
99215 40‐54 minutes
13
14
11/5/2020
8
New Prolonged Service Code
• To be used with the highest level of office visit code only
• Use other prolonged service codes with other E&M codes
• Added note with time shown on codes
• With or without patient contact• 99417
• Only used with 99205 or 99215
• Only billed when time spent is minimum 15 minutes over the allowable time on date of service
• Question on CMS vs AMA definition • AMA starts using at first minute over, CMS counts starting at 15 minutes over
Pitfalls and Benefits of Time Method
• On surface, seems to be an overall easier way to calculate
• But have to document total time
• Have to be cautious, don’t slow down documentation to “milk” time
• Work 8 hour day can’t bill for 15
• How do you capture all time outside of the actual visit
• Start stop time?
15
16
11/5/2020
9
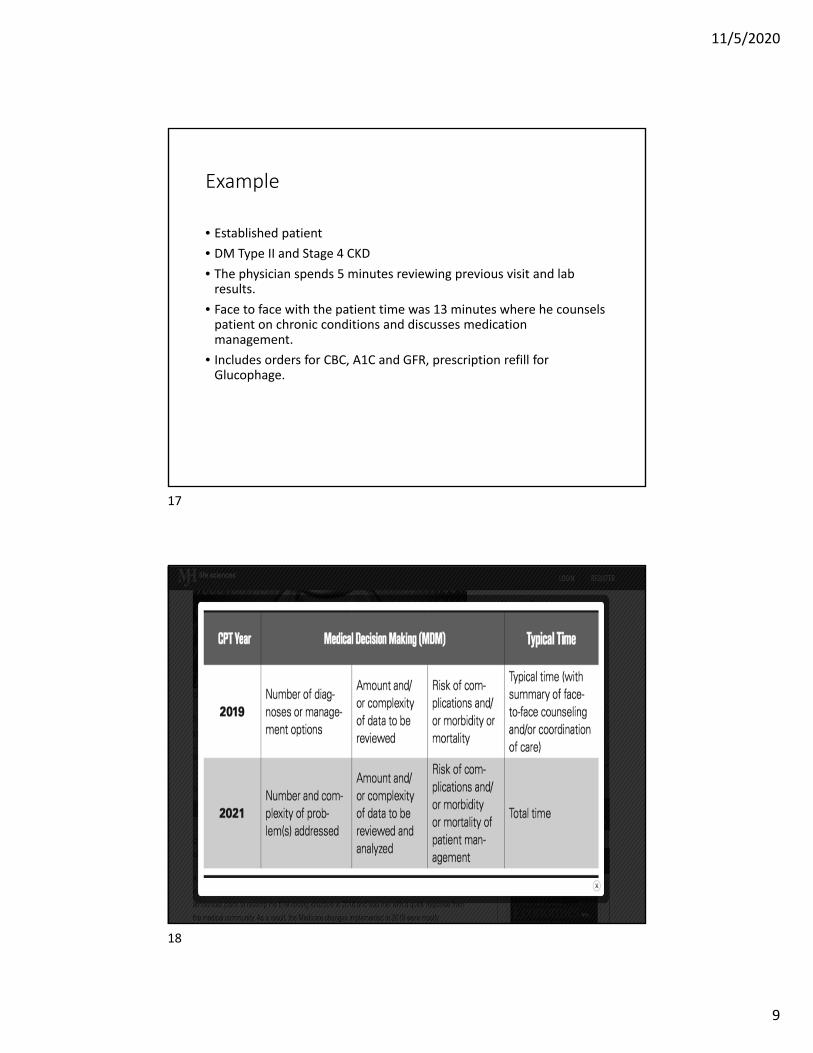
Example
• Established patient
• DM Type II and Stage 4 CKD
• The physician spends 5 minutes reviewing previous visit and lab results.
• Face to face with the patient time was 13 minutes where he counsels patient on chronic conditions and discusses medication management.
• Includes orders for CBC, A1C and GFR, prescription refill for Glucophage.
17
18
11/5/2020
10
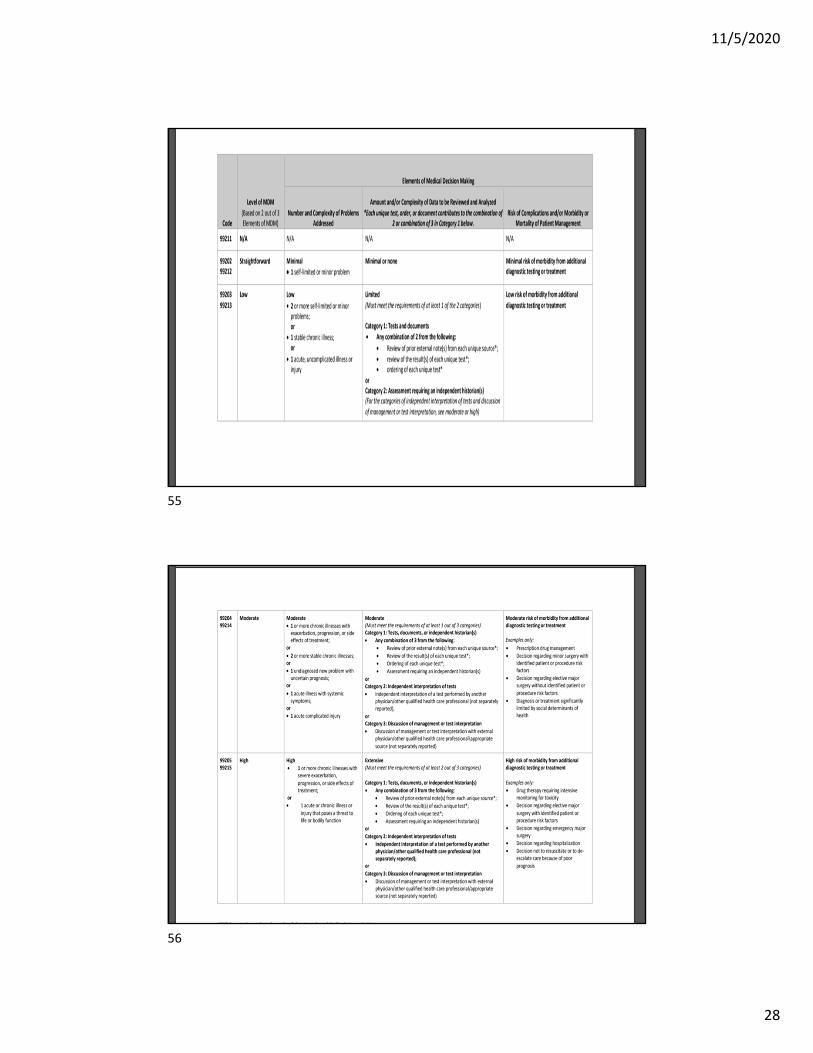
Medical Decision Making
• Same 4 complexities• Straightforward
• Low Complexity
• Moderate Complexity
• High Complexity
• Three Elements• Still 2/3 required to get a “level”
• Highest two scoring elements
19
Three elements: ▪
• The number and complexity of problem(s) that are addressed during the encounter.
Amount/Complexity of Data reviewed and/or analyzed• Risk of patient management
19
20
11/5/2020
11
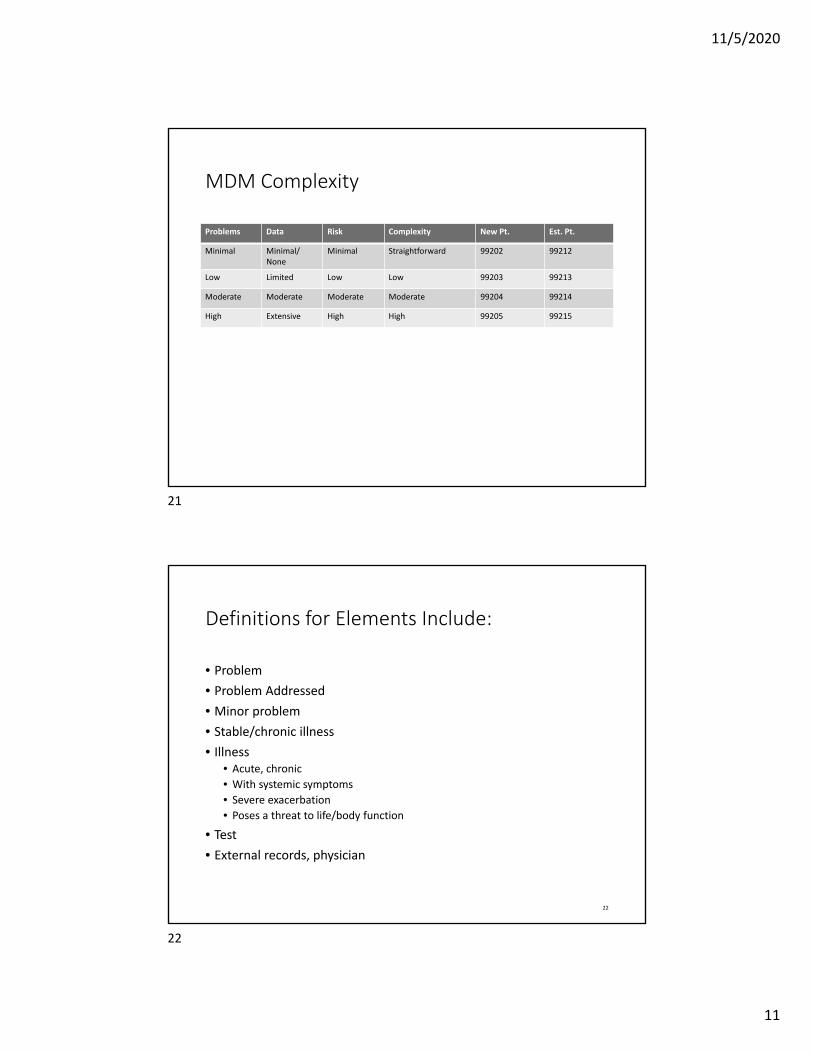
MDM Complexity
Problems Data Risk Complexity New Pt. Est. Pt.
Minimal Minimal/None
Minimal Straightforward 99202 99212
Low Limited Low Low 99203 99213
Moderate Moderate Moderate Moderate 99204 99214
High Extensive High High 99205 99215
Definitions for Elements Include:
• Problem
• Problem Addressed
• Minor problem
• Stable/chronic illness
• Illness• Acute, chronic
• With systemic symptoms
• Severe exacerbation
• Poses a threat to life/body function
• Test
• External records, physician
22
21
22
11/5/2020
12
#1 Problems Addressed
• Diagnosis itself does not show complexity or risk
• Ties in information needed to come up with differential diagnoses, rule out certain diagnoses
• Also combination of diagnoses may impact complexity
• Symptom that is integral part of diagnosis should not be counted separately
• Complex workup required sometimes when actual findings don’t seem as severe
Problem
• Problem: A problem is a disease, condition, illness, injury, symptom, sign, finding, complaint, or other matter addressed at the encounter, with or without a diagnosis being established at the time of the encounter
23
24
11/5/2020
13
Definition of Problem Addressed
• Problem addressed: A problem is addressed or managed when it is evaluated or treated at the encounter by the physician or other qualified health care professional reporting the service. This includes consideration of further testing or treatment that may not be elected by virtue of risk/benefit analysis or patient/parent/guardian/surrogate choice. Notation in the patient’s medical record that another professional is managing the problem without additional assessment or care coordination documented does not qualify as being ‘addressed’ or managed by the physician or other qualified health care professional reporting the service. Referral without evaluation (by history, exam, or diagnostic study[ies]) or consideration of treatment does not qualify as being addressed or managed by the physician or other qualified health care professional reporting the service.
What do we count?
• Any diagnoses that impact care
• Remember the MEAT acronym for HCCs
• Monitor, Evaluate, Assess, Treat• Only need one of the 4
• Additional risk
• Addressed vs managed
• Referral without evaluation does not count
• Not just listed
25
26
11/5/2020
14
Official Coding Guidelines
• G. ICD‐10‐CM code for the diagnosis, condition, problem, or other reason for encounter/visit
• List first the ICD‐10‐CM code for the diagnosis, condition, problem, or other reason for encounter/visit shown in the medical record to be chiefly responsible for the services provided. List additional codes that describe any coexisting conditions. In some cases, the first‐listed diagnosis may be a symptom when a diagnosis has not been established (confirmed) by the provider.
• H. Uncertain diagnosis
• Do not code diagnoses documented as "probable", "suspected," "questionable," "rule out," "compatible with", "consistent with", or "working diagnosis" or other similar terms indicating uncertainty. Rather, code the condition(s) to the highest degree of certainty for that encounter/visit, such as symptoms, signs, abnormal test results, or other reason for the visit.
• I. Chronic diseases
• Chronic diseases treated on an ongoing basis may be coded and reported as many times as the patient receives treatment and care for the condition(s)
• J. Code all documented conditions that coexist
• Code all documented conditions that coexist at the time of the encounter/visit, and require or affect patient care treatment or management. Do not code conditions that were previously treated and no longer exist. However, history codes (categories Z80‐Z87) may be used as secondary codes if the historical condition or family history has an impact on current care or influences treatment.
Levels of Problems
• Minimal problem: A problem that may not require the presence of the physician or other qualified health care professional, but the service is provided under the physician’s or other qualified health care professional’s supervision (see 99211).
• Self‐limited or minor problem: A problem that runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status.
27
28
11/5/2020
15
Stable, chronic illness
• A problem with an expected duration of at least a year or until the death of the patient. For the purpose of defining chronicity, conditions are treated as chronic whether or not stage or severity changes (eg, uncontrolled diabetes and controlled diabetes are a single chronic condition). ‘Stable’ for the purposes of categorizing medical decision making is defined by the specific treatment goals for an individual patient. A patient that is not at their treatment goal is not stable, even if the condition has not changed and there is no short term threat to life or function. For example, a patient with persistently poorly controlled blood pressure for whom better control is a goal is not stable, even if the pressures are not changing and the patient is asymptomatic. The risk of morbidity without treatment is significant. Examples may include well‐controlled hypertension, non‐insulin dependent diabetes, cataract, or benign prostatic hyperplasia.
Chronic illness with exacerbation, progression, or side effects of treatment
• A chronic illness that is acutely worsening, poorly controlled or progressing with an intent to control progression and requiring additional supportive care or requiring attention to treatment for side effects, but that does not require consideration of hospital level of care.
29
30
11/5/2020
16
Chronic illness with severe exacerbation, progression, or side effects of treatment
• The severe exacerbation or progression of a chronic illness or severe side effects of treatment that have significant risk of morbidity and may require hospital level of care.
Undiagnosed new problem with uncertain prognosis:
• A problem in the differential diagnosis that represents a condition likely to result in a high risk of morbidity without treatment. An example may be a lump in the breast.
31
32
11/5/2020
17
Acute, uncomplicated illness or injury
• A recent or new short‐term problem with low risk of morbidity for which treatment is considered. There is little to no risk of mortality with treatment, and full recovery without functional impairment is expected. A problem that is normally self‐limited or minor, but is not resolving consistent with a definite and prescribed course is an acute uncomplicated illness. Examples may include cystitis, allergic rhinitis, or a simple sprain.
Acute illness with systemic symptoms:
• An illness that causes systemic symptoms and has a high risk of morbidity without treatment. For systemic general symptoms such as fever, body aches or fatigue in a minor illness that may be treated to alleviate symptoms, shorten the course of illness or to prevent complications, see the definitions for ‘self‐limited or minor’ or ‘acute, uncomplicated.’ Systemic symptoms may not be general, but may be single system. Examples may include pyelonephritis, pneumonitis, or colitis
33
34
11/5/2020
18
Acute, complicated injury
• An injury which requires treatment that includes evaluation of body systems that are not directly part of the injured organ, the injury is extensive, or the treatment options are multiple and/or associated with risk of morbidity. An example may be a head injury with brief loss of consciousness.
Acute or chronic illness or injury that poses a threat to life or bodily function
• An acute illness with systemic symptoms, or an acute complicated injury, or a chronic illness or injury with exacerbation and/or progression or side effects of treatment, that poses a threat to life or bodily function in the near term without treatment. Examples may include acute myocardial infarction, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failure, or an abrupt change in neurologic status.
35
36
11/5/2020
19
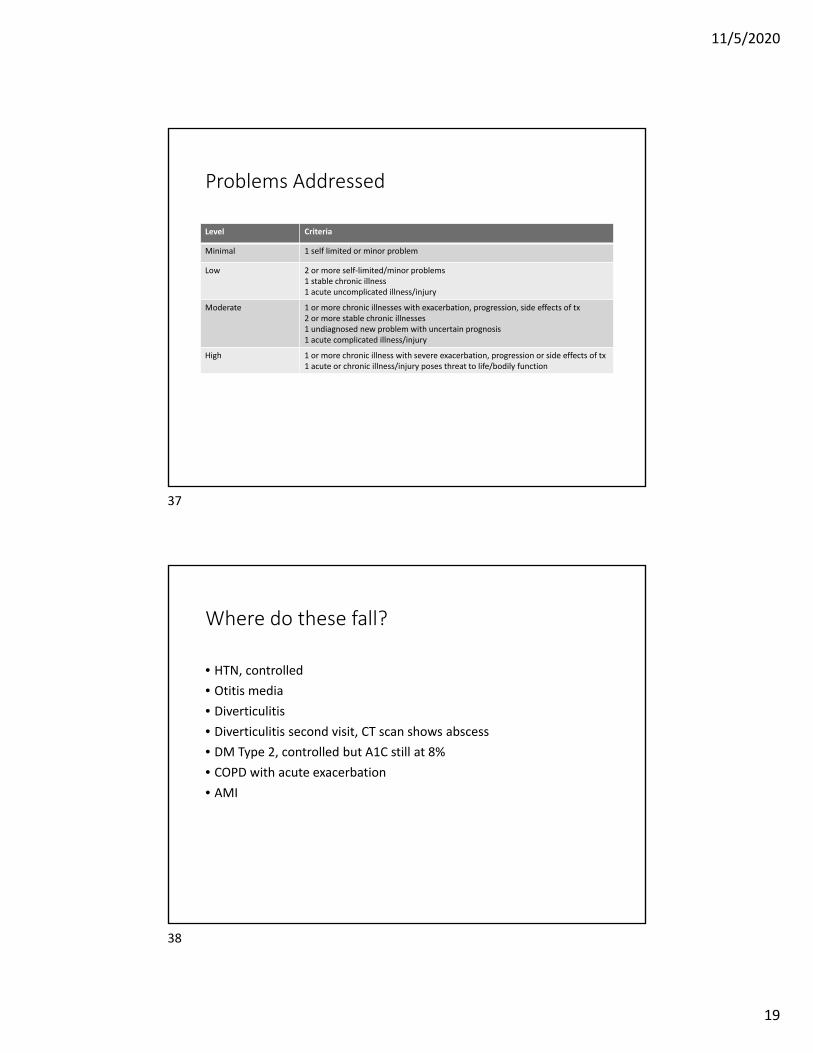
Problems Addressed
Level Criteria
Minimal 1 self limited or minor problem
Low 2 or more self‐limited/minor problems1 stable chronic illness1 acute uncomplicated illness/injury
Moderate 1 or more chronic illnesses with exacerbation, progression, side effects of tx2 or more stable chronic illnesses1 undiagnosed new problem with uncertain prognosis1 acute complicated illness/injury
High 1 or more chronic illness with severe exacerbation, progression or side effects of tx1 acute or chronic illness/injury poses threat to life/bodily function
Where do these fall?
• HTN, controlled
• Otitis media
• Diverticulitis
• Diverticulitis second visit, CT scan shows abscess
• DM Type 2, controlled but A1C still at 8%
• COPD with acute exacerbation
• AMI
37
38
11/5/2020
20
#2 Amount/Complexity of Data
• Medical records, tests, and/or other information• must be obtained, ordered, reviewed, and analyzed
• from multiple sources
• interpretation of tests
• Ordering a test is included in the category of test result(s) and the review of the test result is part of the encounter
39
Data
• Data is divided into three categories:• Tests, documents, orders, or independent historian(s). (Each unique test, order or document is counted to meet a threshold number)
• Independent interpretation of tests.
• Discussion of management or test interpretation with external physician or other qualified healthcare professional or appropriate source
39
40
11/5/2020
21
Definition of Tests
• Test: Tests are imaging, laboratory, psychometric, or physiologic data. A clinical laboratory panel (eg, basic metabolic panel [80047]) is a single test. The differentiation between single or multiple unique tests is defined in accordance with the CPT code set.
External
• External: External records, communications and/or test results are from an external physician, other qualified health care professional, facility or healthcare organization.
• External physician or other qualified healthcare professional: An external physician or other qualified health care professional is an individual who is not in the same group practice or is a different specialty or subspecialty. It includes licensed professionals that are practicing independently. It may also be a facility or organizational provider such as a hospital, nursing facility, or home health care agency.
41
42
11/5/2020
22
Independent
• Independent historian(s): An individual (eg, parent, guardian, surrogate, spouse, witness) who provides a history in addition to a history provided by the patient who is unable to provide a complete or reliable history (eg, due to developmental stage, dementia, or psychosis) or because a confirmatory history is judged to be necessary. In the case where there may be conflict or poor communication between multiple historians and more than one historian(s) is needed, the independent historian(s) requirement is met.
Independent Interpretation:
• The interpretation of a test for which there is a CPT code and an interpretation or report is customary. This does not apply when the physician or other qualified health care professional is reporting the service or has previously reported the service for the patient. A form of interpretation should be documented, but need not conform to the usual standards of a complete report for the test.
43
44
11/5/2020
23
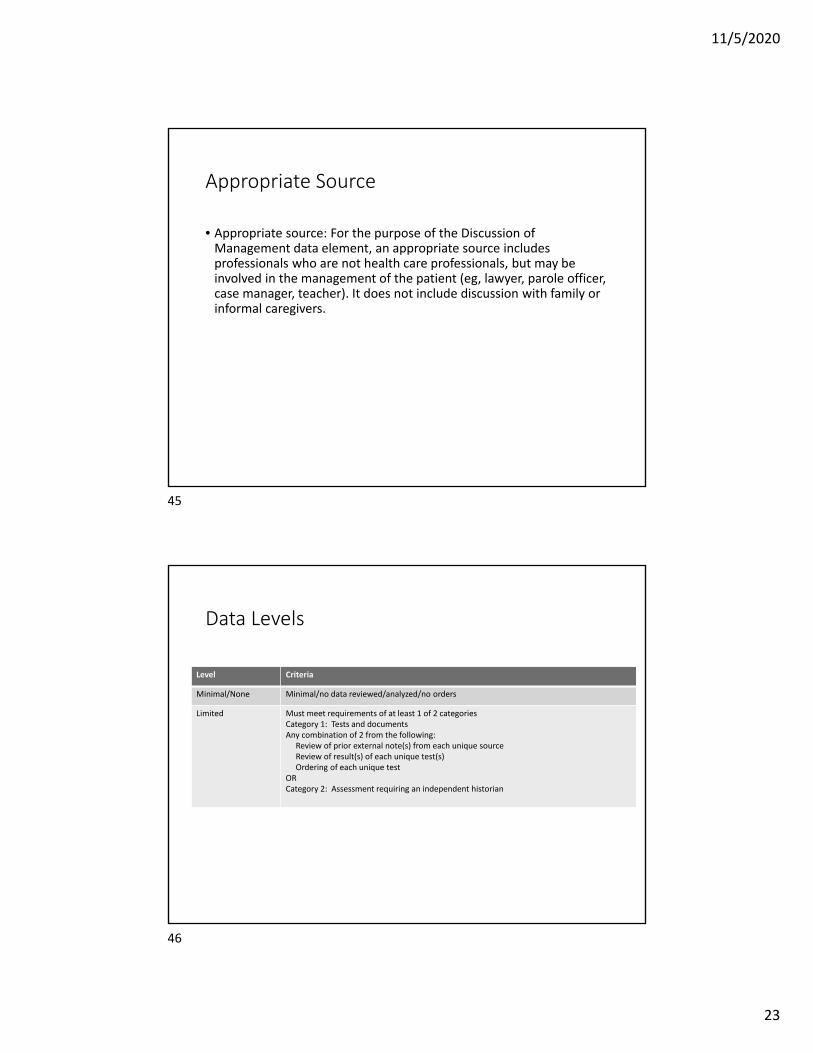
Appropriate Source
• Appropriate source: For the purpose of the Discussion of Management data element, an appropriate source includes professionals who are not health care professionals, but may be involved in the management of the patient (eg, lawyer, parole officer, case manager, teacher). It does not include discussion with family or informal caregivers.
Data Levels
Level Criteria
Minimal/None Minimal/no data reviewed/analyzed/no orders
Limited Must meet requirements of at least 1 of 2 categoriesCategory 1: Tests and documentsAny combination of 2 from the following:
Review of prior external note(s) from each unique sourceReview of result(s) of each unique test(s)Ordering of each unique test
ORCategory 2: Assessment requiring an independent historian
45
46
11/5/2020
24
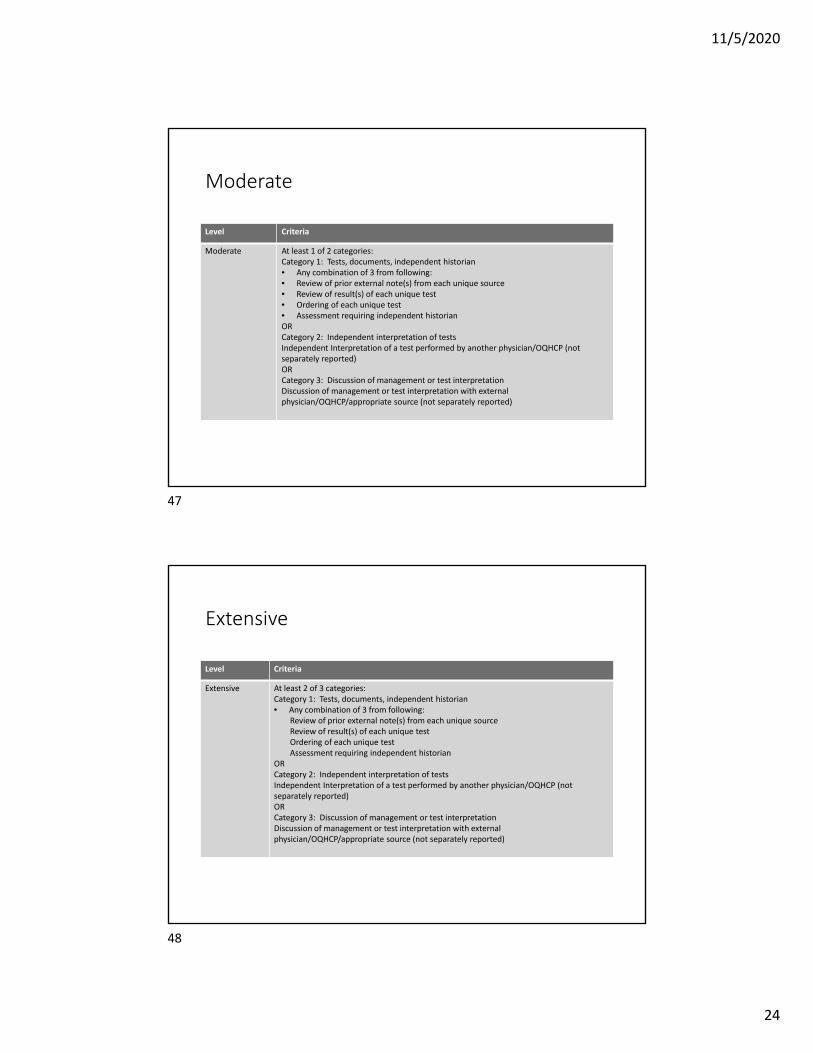
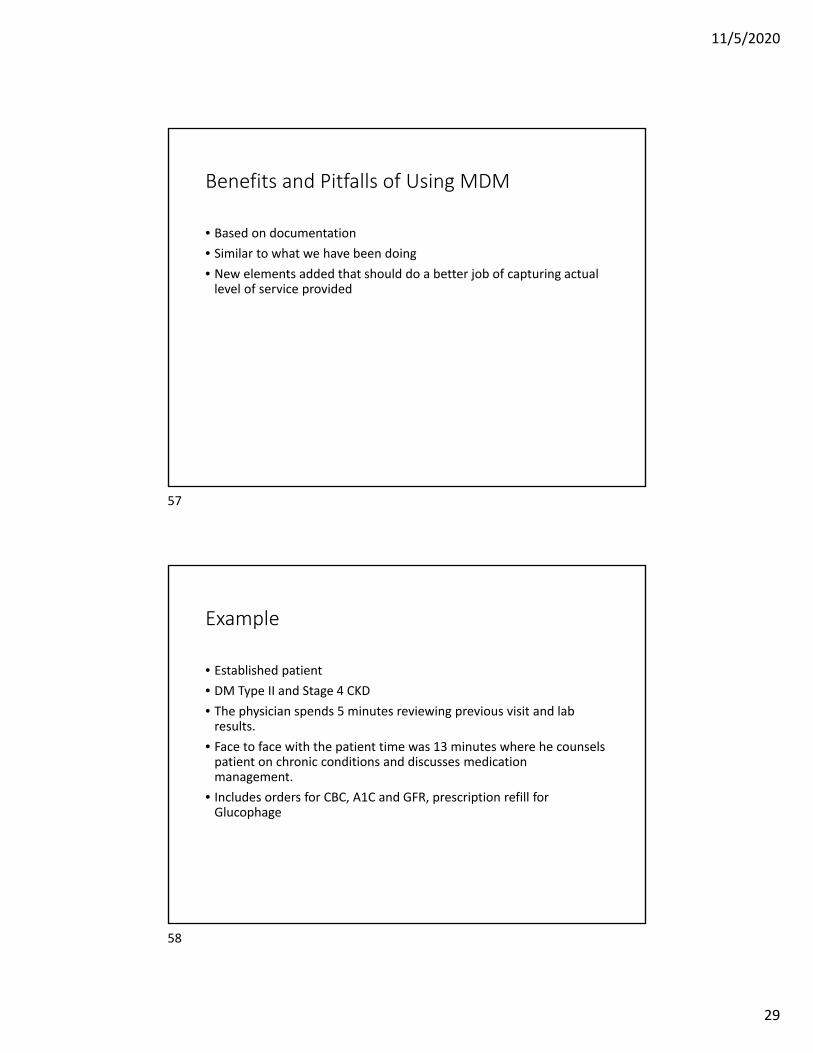
Moderate
Level Criteria
Moderate At least 1 of 2 categories:Category 1: Tests, documents, independent historian• Any combination of 3 from following:• Review of prior external note(s) from each unique source• Review of result(s) of each unique test• Ordering of each unique test• Assessment requiring independent historianORCategory 2: Independent interpretation of testsIndependent Interpretation of a test performed by another physician/OQHCP (not separately reported)ORCategory 3: Discussion of management or test interpretationDiscussion of management or test interpretation with external physician/OQHCP/appropriate source (not separately reported)
Extensive
Level Criteria
Extensive At least 2 of 3 categories:Category 1: Tests, documents, independent historian• Any combination of 3 from following:
Review of prior external note(s) from each unique sourceReview of result(s) of each unique testOrdering of each unique testAssessment requiring independent historian
ORCategory 2: Independent interpretation of testsIndependent Interpretation of a test performed by another physician/OQHCP (not separately reported)ORCategory 3: Discussion of management or test interpretationDiscussion of management or test interpretation with external physician/OQHCP/appropriate source (not separately reported)
47
48

11/5/2020
25
#3 Risk
• Possible management options selected
• Also includes options considered but not used
• “Level of risk is based upon consequences of the problem(s) addressed at the encounter when appropriately treated. Risk also includes medical decision making related to the need to initiate or forgo further testing, treatment and/or hospitalization.” AMA
Risk Defined
• Risk: The probability and/or consequences of an event. The assessment of the level of risk is affected by the nature of the event under consideration. For example, a low probability of death may be high risk, whereas a high chance of a minor, self‐limited adverse effect of treatment may be low risk. Definitions of risk are based upon the usual behavior and thought processes of a physician or other qualified health care professional in the same specialty. Trained clinicians apply common language usage meanings to terms such as ‘high’, ‘medium’, ‘low’, or ‘minimal’ risk and do not require quantification for these definitions, (though quantification may be provided when evidence‐based medicine has established probabilities). For the purposes of medical decision making, level of risk is based upon consequences of the problem(s) addressed at the encounter when appropriately treated. Risk also includes medical decision making related to the need to initiate or forego further testing, treatment and/or hospitalization.
49
50
11/5/2020
26
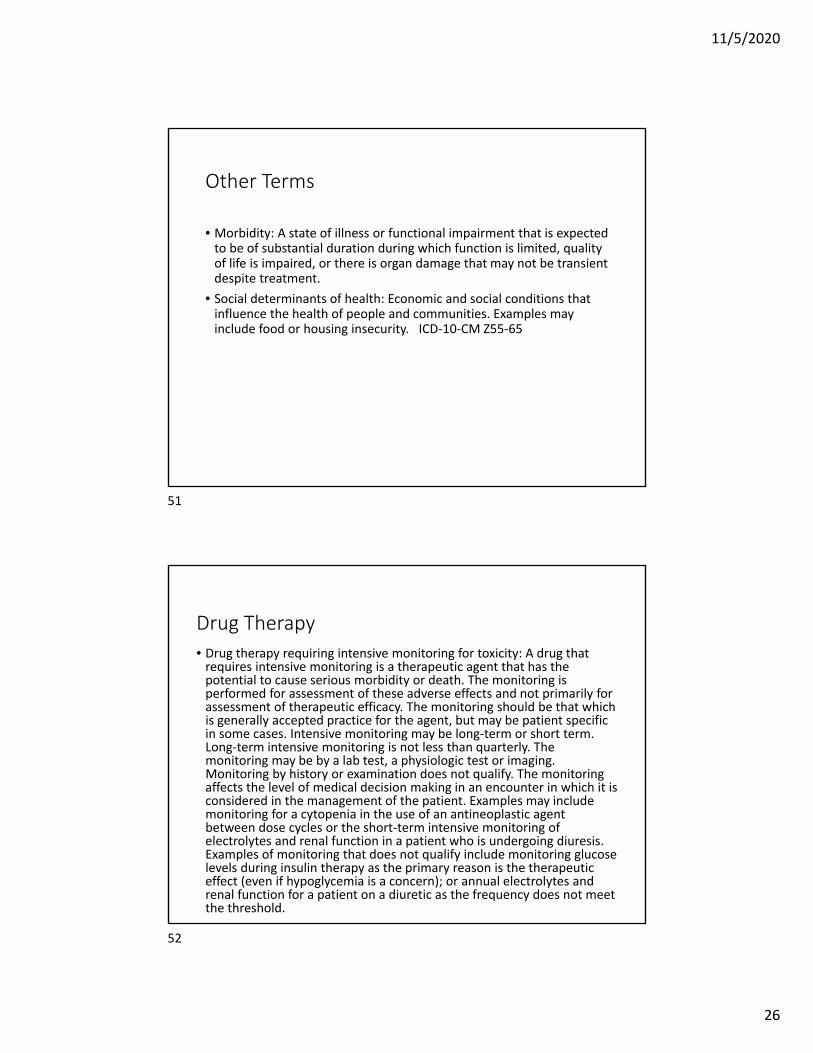
Other Terms
• Morbidity: A state of illness or functional impairment that is expected to be of substantial duration during which function is limited, quality of life is impaired, or there is organ damage that may not be transient despite treatment.
• Social determinants of health: Economic and social conditions that influence the health of people and communities. Examples may include food or housing insecurity. ICD‐10‐CM Z55‐65
Drug Therapy
• Drug therapy requiring intensive monitoring for toxicity: A drug that requires intensive monitoring is a therapeutic agent that has the potential to cause serious morbidity or death. The monitoring is performed for assessment of these adverse effects and not primarily for assessment of therapeutic efficacy. The monitoring should be that which is generally accepted practice for the agent, but may be patient specific in some cases. Intensive monitoring may be long‐term or short term. Long‐term intensive monitoring is not less than quarterly. The monitoring may be by a lab test, a physiologic test or imaging. Monitoring by history or examination does not qualify. The monitoring affects the level of medical decision making in an encounter in which it is considered in the management of the patient. Examples may include monitoring for a cytopenia in the use of an antineoplastic agent between dose cycles or the short‐term intensive monitoring of electrolytes and renal function in a patient who is undergoing diuresis. Examples of monitoring that does not qualify include monitoring glucose levels during insulin therapy as the primary reason is the therapeutic effect (even if hypoglycemia is a concern); or annual electrolytes and renal function for a patient on a diuretic as the frequency does not meet the threshold.
51
52
11/5/2020
27
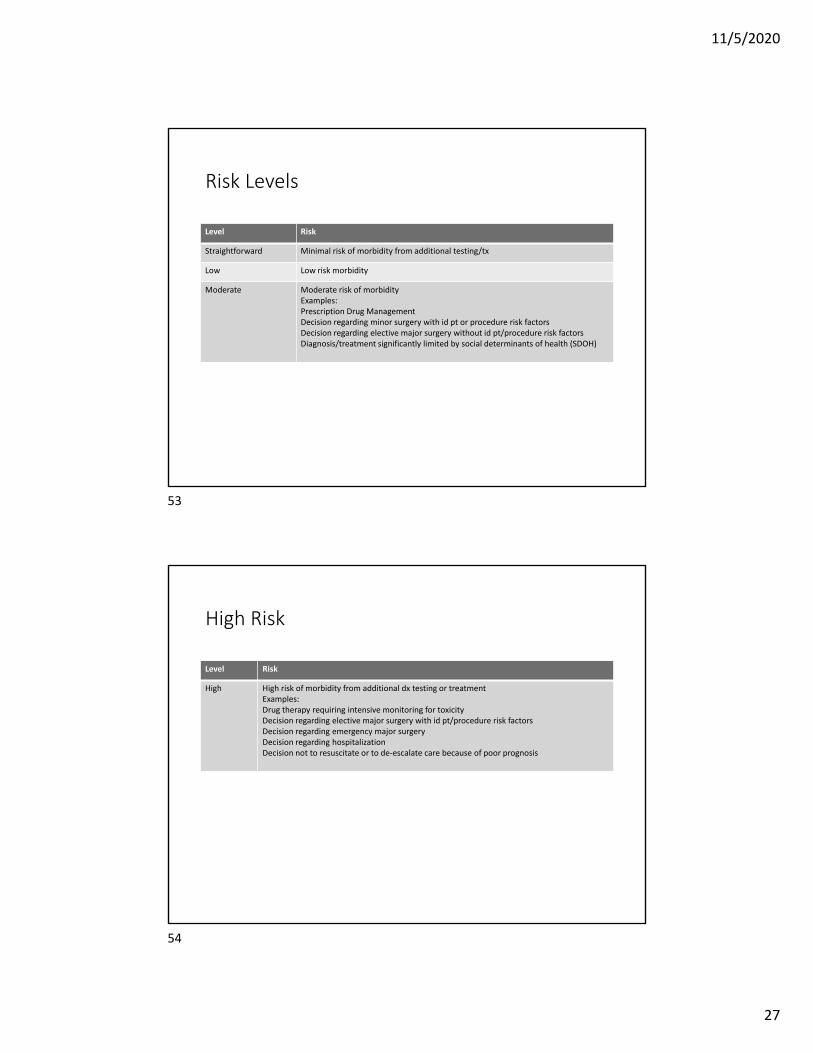
Risk Levels
Level Risk
Straightforward Minimal risk of morbidity from additional testing/tx
Low Low risk morbidity
Moderate Moderate risk of morbidityExamples:Prescription Drug ManagementDecision regarding minor surgery with id pt or procedure risk factorsDecision regarding elective major surgery without id pt/procedure risk factorsDiagnosis/treatment significantly limited by social determinants of health (SDOH)
High Risk
Level Risk
High High risk of morbidity from additional dx testing or treatmentExamples:Drug therapy requiring intensive monitoring for toxicityDecision regarding elective major surgery with id pt/procedure risk factorsDecision regarding emergency major surgeryDecision regarding hospitalizationDecision not to resuscitate or to de‐escalate care because of poor prognosis
53
54
11/5/2020
28
55
56
11/5/2020
29
Benefits and Pitfalls of Using MDM
• Based on documentation
• Similar to what we have been doing
• New elements added that should do a better job of capturing actual level of service provided
Example
• Established patient
• DM Type II and Stage 4 CKD
• The physician spends 5 minutes reviewing previous visit and lab results.
• Face to face with the patient time was 13 minutes where he counsels patient on chronic conditions and discusses medication management.
• Includes orders for CBC, A1C and GFR, prescription refill for Glucophage
57
58
11/5/2020
30
Example 2
• Established pt
• Rash on rt leg after hunting in woods
• Dx: Poison oak
• TX: Use over the counter corticosteroid cream
• Return if rash does not show improvement in several days or gets worse.
Example 3
• Patient with known diverticula presents with abdominal pain
• CT ordered, shows uncomplicated diverticulitis
• Urinalysis and CBC within normal limits
• Prescription for antibiotics and pain meds given
• Discussion of diet restrictions
• Return if not better or if symptoms worsen
59
60
11/5/2020
31
Example 4
• New patient evaluated for epilepsy management
• Patient has tremors on current medication
• Review of most recent EEG
• Prescribes different medication that is known to have less side effects
Using MDM
• 2 or more stable chronic illnesses=Moderate
• Ordering each unique test=Moderate (3)
• Prescription drug management=Moderate
• 99214
61
62
11/5/2020
32
Getting prepared
• Have discussions of your process
• Time or MDM?
• Are your physicians going to code these?
Assessment
• Review records using new methods
• Could you even use time at this point?
• How does the MDM look?
• What impact will this have on your practice financially?
• Run report to show frequency of codes used.
•
63
64
11/5/2020
33
Vendors
• Does your practice utilize any software, forms, etc. to assist with E&M Leveling?
• What about your EHR?
• Contracts
Training
• Train the Trainer?
• All Coders?
• All Physicians?
• What documentation will you use to train?
• Forms?
65
66
11/5/2020
34
Don’t Forget About Medical Necessity
• Documentation should always support level of service billed
• Overdocumentation does not mean you can bill higher if it doesn’t make sense based on the issues addressed.
• Audits will still be happening!
AMA
•https://edhub/ama‐assn.org/•Https://www.ama‐assn.org/practice‐management/cpt/em‐prep‐your‐house‐practice‐checklist‐2021‐transition
•https://www.ama‐assn.org/practice‐management/cpt/10‐tips‐prepare‐your‐practice‐em‐office‐visit‐changes
•https://www.ama‐assn.org/system/files/2019‐06/cpt‐office‐prolonged‐svs‐code‐changes.pdf
68
67
68