Embed Size (px)
Citation preview

Deep dive in Acetaminophen
Adel KorairiR4

1st case report
•Thomson J, Prescott LF. Liver damage and impaired glucose tolerance after paracetamol over dosage.
Br Med J1966;2:506-507.
•16 y.o female presented by family after ingestion if 20 tab Adol
•What next?


Define acute exposure?

Definition
•A toxic exposure to acetaminophen is suggested when an adult ingests
(l) >10 grams or 200 milligrams/kg as a single ingestion,
(2) >10 grams or 200 milligrams/kg over a 24-hour period, or
(3) >6 grams or 150 milligrams/kg per 24-hour period for at least 2 consecutive days.

•16 y.o female presented by family after ingestion if 20 tab Adol, 10 tab 4 hr ago and 10 tab 10 min ago

From when to count if multiple acute ingestion?

When to count if multiple acute ingestion?•From 1st dose, worst case scenario •You might need to repeat the level


WHO
•10- 7.5 Gm, or 15 tab extra strength




Conclusion
•Immediate release level at 4hr•Extended release level at 4hr then repeat
4-6 hr

Metabolism

Stages ?



LFT


Which is worse?
16 y.o female healthy presented by family after ingestion if 20 tab Adol once, 4hr ago, while been drunk.
86 y.o male on anti TB, cachectic , chronic alcoholic, smoker ingested 20 tabs of adol 9 hr ago.

Risk factors for liver injuries?

Risk factors for liver injuries
●Excessive intake of acetaminophen●Excessive cytochrome P450 activity (
carbamazepine, phenobarbital, and phenytoin) and antituberculosis drugs (eg, isoniazid and rifampin), (Tobacco)
●Decreased capacity for glucuronidation or sulfation (Chronic liver disease, Starvation, old age)
●Depletion of glutathione stores (Chronic alcohol)



What are the indication of liver transplant center?


GUIDELINES• The United Kingdom National Health Service guideline
recommends treating patients at 200 μg per milliliter at 4 hours after ingestion and high-risk
high-risk line that begins at 100 μg per milliliter at 4 hours.
• The American Academy of Pediatrics recommends acetylcysteine therapy for acetaminophen poisoning, but it does not suggest indications or support any treatment protocol.
• The American College of Emergency Physicians recommends at 150 μg per milliliter at 4 hours, as well as for any patient with liver injury or liver failure.


Duration?•72-hour PO protocol:1- A loading dose of 140 mg/kg PO2- 70 mg/kg PO every four hours for a total of
17 doses
•21-hour IV protocol: total dose of 300 mg/kg:1- 150 mg/kg in 200 ml over the first hour2- 50 mg/kg in 500 ml over the next 4 hours3- 100mg/kg in 1 L over the next 16 hours


When to stop?
•At the completion of these protocols, NAC may be discontinued if the metabolism of acetaminophen is complete
•1- serum acetaminophen concentration > 10 μg/mL [66 μmol/L]) and
•2- there is no evidence of liver injury (normal AST concentration).

ACEP

1. What are the indications for N-acetylcysteine (NAC) in the acetaminophen overdose patient with a known time of acute ingestion who can be risk stratified by the Rumack-Matthew nomogram?• Level B recommendations. (1) Administer
NAC to acute acetaminophen overdose patients with either possible or probable risk for hepatotoxicity as determined by the Rumack-Matthew nomogram to reduce the incidence of severe hepatotoxicity and mortality, ideally within 8 to 10 hours postingestion. (2) Do not administer NAC to acute acetaminophen overdose patients with no risk for hepatotoxicity as determined by the Rumack-Matthew nomogram.

2. What are the indications for NAC in the acetaminophen overdose patient who cannot be risk stratified by the Rumack-Matthew nomogram?• Level B recommendations. Administer NAC to
patients with hepatic failure thought to be due to acetaminophen.
• Level C recommendations. Administer NAC to patients who have hepatotoxicity thought to be due to acetaminophen and have a suspected or known acetaminophen overdose, including repeated supratherapeutic ingestions.


Define chronic exposure?


supratherapeutic ?

supratherapeutic




Supratherapeutic approach?


Combined


Gastric emptying




Conclusion
•?? The only indicated is gastric lavage in 1st hr after massive overdose.
• (usually more than 40 g, with peak plasma paracetamol concentrations typically over 800 mg l).

16 y.o female healthy presented by family after ingestion if 20 tab Adol once, 1 hr ago, while been drunk.
•Level 990 umol/l = 150 ug/l•Umol/l /6.6 = ug/l
•What is next?

Charchol
•1 g/kg, 25-100 g PO•Alternatively 10 g charcoal/1 g drug ratio•Minimum dose = 25 g





Cochrane 2006

Conclusion
•Conceder charcoal almost only in the 1st hr, if no contraindication is expected (LOC, vomiting, bowel obstruction …)


Oral NAC + Charchol



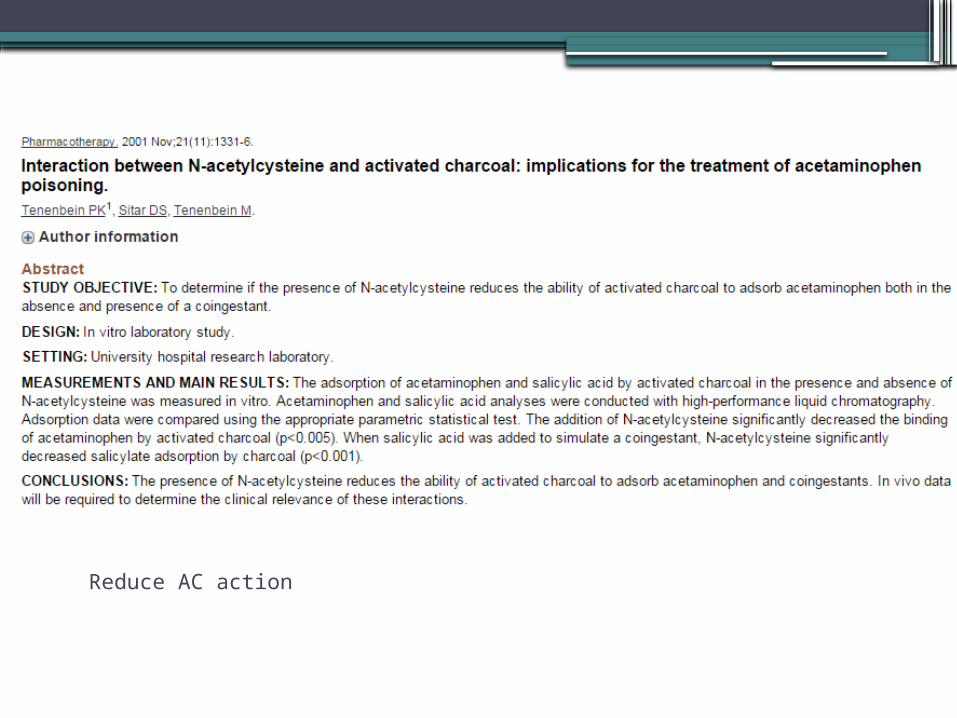
Reduce AC action


Conclusion
•Charcoal reduce the oral NAC absorption, but over all improve outcome

NAC

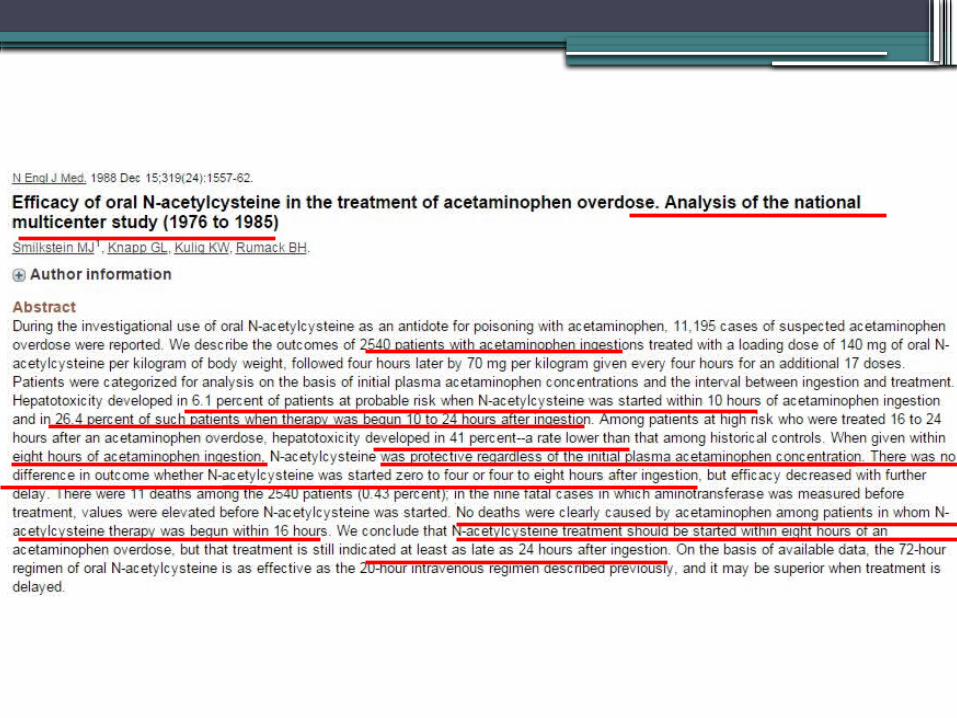






Cochrane 2006




????????????? UK guideline

86 y.o male on anti TB, cachectic , chronic alcoholic, smoker ingested 20 tabs of adol 9 hr ago.
Level 1000 umol/l
•Which NAC shall I use?

Side effect & effectiveness








Conclusion
•No clinical significant deference.•IV is cost effective

Metoclopramide



•33 y.o old female K/c mood disorder pregnant ingested 12 gm adol, next in regard tratment and prognosis
•1st trimester?•2nd trimester?•3rd trimester?

pregnancy





Risk Assessment in Pregnant Women• Fetal acetaminophen toxicity is rare, but
adverse outcomes have been reported in all stages of pregnancy.
• In the early gestational period, acetaminophen toxicity can be associated with fetal death.
• CYP enzymes appear in the fetus during the second trimester, and third trimester or newborn at risk of toxicity.
• The risk assessment for and diagnostic approach to pregnant women are the same as those for nonpregnant women.

Rosen's


PSI




Conclusion
•PSI may replace rock-Mathieu in the future

Methionine

•60 y.o male with multiple co morbidities brought by relative obtunded, hypothermic and hypotensive after ingestion of 50 Gm adol.
•Level 1000 ug/l = 6600 umol/ l•Lactat 8•Failed NAC therapy

HD






Thank You