Embed Size (px)
Citation preview

Deep Brain Stimulation
Punit Agrawal, DOMovement Disorder DivisionDepartment of NeurologyThe Ohio State University

• This lecture reviews DBS patient selection and management with a focus on approved FDA indication for Movement Disorders
– No conflicts of interests to disclose

FDA Approved Indications– Essential Tremor
• FDA approved in 1997
– Parkinson’s disease• FDA approved in 2002
– Dystonia• FDA approved (HDE*) in 2003
– Obsessive Compulsive Disorder• FDA approved (HDE**) in 2009
• Medicare and Insurance reimbursed for FDA approved indications
*Humanitarian Device: Authorized by Federal (U.S.A) law for the use as an aid in the management of chronic, intractable (drug refractory) primary dystonia, including generalized and segmental dystonia, hemidystonia, and cervical dystonia, for individuals 7 years of age and older.
**Humanitarian Device: Authorized by Federal (U.S.A) law for use as an adjunct to medications and as alternative to anterior capsulotomy for treatment of chronic, severe, treatment-resistant obsessive-compulsive disorder (OCD) in adult patients who have failed at least three selective serotonin reuptake inhibitors (SSRIs). The effectiveness of this device for this use has not been demonstrated.

• Offers hope to severely impaired patients when symptoms are intractable despite optimal medication and other available therapies.
• > 22 years of safety• > 80,000 DBS Implants worldwide• >3000 published articles on DBS
• With proper patient selection, there is improvement seen with:– Standard scales/measures of disease– Quality of life measures– Co-morbid conditions– Medication intake– Chronic care costs

DBS Target Sites for Movement Disorders
Vim Thalamus: Essential Tremor
Subthalamic Nucleus: Parkinson’s disease
and Dystonia
Globus Pallidus: Parkinson’s disease
and Dystonia

Movement Disorders Patient Evaluation
– Movement Disorder Neurology• Evaluate medications and disease
– Levodopa ON-OFF assessment in Parkinson’s disease
– Neurosurgery• Discuss surgery, implantable devices, risks
– MRI of the brain– Neuropsychological testing– Review and Discussion at Patient Management
Meeting– Team recommendation

Approach to Improve Outcomes
• Multidisciplinary Team:– Neurology, neurosurgery, psychiatry, psychology,
physical medicine and rehabilitation, neuroradiology, neuroanesthesia, PT/OT/ST, social worker/case manager.
• Proper Patient Selection• Patient screening for appropriate candidates for DBS therapy
and education• Realistic and proper expectations from DBS therapy
• Psychosocial assessment

Poor Candidates for DBS• Significant dementia or cognitive impairment
– Neuropsychological compromise
• Untreated depression, anxiety, psychosis, or other co-morbid psychiatric illness
• Unable to cooperate during surgical procedure• Unable to cooperate during programming visits• Unrealistic expectations of outcomes• Co-existing medical problems that significantly increase risks of surgery
– Uncontrolled heart disease, lung disease, cerebrovascular disease, uncontrolled hypertension, or diabetes.
• Significant structural abnormalities detected by brain MRI that would pose higher risk of brain surgery
• Additional features suggesting poor candidates for parkinsonism– Minimal or absent response to levodopa– Atypical Parkinsonian syndromes

DBS for Tremor• Severe debilitating medication refractory
tremorPropranolol Primidone KeppraNeurontin Anticholinergic PD medications
• Resting Tremor > Postural Tremor > Intention Tremor
• Expectations: Improve quality of life and that it may not completely eliminate all tremor
• Target: VIM thalamic DBS

Tremor Outcomes with VIM Thalamic DBS
0%10%20%30%40%50%60%70%80%90%
100%
PD ET MS Post-Traumatic
PreOPPostOP>80% >75%
40-50% 50%
- Essential tremor: 60-80% improvementEssential tremor: 60-80% improvement- MS, traumatic brain injury and cerebellar tremor: 50% improvement

DBS for Parkinson’s Disease• Multiple prospective randomized controlled trials have
demonstrated benefits– Tremor– Rigidity and bradykinesia similar to levodopa– Reduced motor fluctuations including less dyskinesia and
improved “ON” time.– Reduction in medications– Reduction in maintenance cost of disease
• 10-20% of individuals with Parkinson’s disease may be candidates for DBS therapy*
• Brain Targets: STN / GPi / VIM
• Aspects important with regards to patient education and expectations
– Not a cure and does not stop disease progression.– Does not reverse disease.– Does not prevent dementia.– May be minimally helpful for gait trouble, imbalance, or posture
changes. – Excluding tremor, minimal help of symptoms not responsive to
levodopa.– Does not help non-motor symptoms.
*AAN Guideline Summary for Patients and their Families: Medical and Surgical Treatment for Motor Fluctuations and Dyskinesia in Parkinson Disease, 2006

PD with DBS Off verse On

Good PD Candidates• Clear diagnosis of idiopathic Parkinson’s disease
• Atypical Parkinson’s or Parkinson’s like syndromes do not improve with surgery
• Good response to levodopa with levodopa challenge showing at least 33% improved UPDRS motor score
• Issues include one or more of the following– 1) Significant Motor fluctuations and/or disabling dyskinesia– 2) Disabling tremor despite optimal medication treatment:
Levodopa Ropinirole/PramipexoleSelegiline/rasagiline BenzodiazepinesAmantadine Parsitan/benztropine/
trihexyphenidyl
– 3) Medication Intolerance
• Stable cognition (absence of significant dementia)• Realistic expectations and good family support• No co-morbid psychiatric/behavioral problem• Greater than 5 years of disease duration

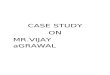
“ON” Time Without Dyskinesias Improves from 27% to 74%
‘ON’ without Dyskinesia‘ON’ with Dyskinesia ‘OFF’
Before Surgery(n=96)
49%
27%
23%
6 Months After SurgeryBilateral STN Activa® Implant
(n=91)
74%*
19%
7%
* The Deep-Brain Stimulation for Parkinson’s Disease Study Group. Deep-brain stimulation of the subthalamic nucleus for the pars interna of the globus pallidus in Parkinson’s disease. N Eng J Med. 2001;345:956-63.
DBS Improvement in PD

PD Motor Symptoms Improvement Maintained After 5 Years
• In a 5-year study, DBS significantly improved OFF-medication assessments of tremor, rigidity, and akinesia/bradykinesia
OFF-Medication Motor Score Improvements*
6-month 1-year 3 years 5 years
Tremor 79% 75% 83% 75%
Rigidity 58% 73% 74% 71%
Akinesia 42% 63% 52% 49%
*Results for STN

Economic Benefits of DBS
Cost Analysis in PD: Multiple comparisons of medical resource use before and after DBS show that DBS significantly reduces the cost of care
DBS reduces the daily dosage of levodopa and dopamine agonists, significantly reducing drug costs by 12 months (Spottke et al, 2002)

DBS for Dystonia• Most effective for primary dystonia
• Generalized, segmental, hemi-dystonia, and focal dystonia including cervical dystonia
– DYT -1 • Secondary dystonia such as those caused by trauma or metabolic disorders can be
less responsive to DBS therapy with inconsistent results– Those with structural lesions can worsen– Tardive dystonia are exceptions with often good response
• Significantly impairment of normal activities and quality of life
• Failed maximal combinations of medication trials:- Muscle relaxants - Benzodiazepines- Anticholinergics - Levodopa
- Failure of botulinum toxin therapy or the dystonia affects too large of an area for this modality of treatment
• Ages 7 and older
• Targets– Globus pallidus internus (Gpi)– Thalamus
• Vop,Voa
• Outcome 23-91% improvement

•Double blind, class I study
•40 pts with GPi DBS randomized to Stimulation or Sham for 3 months
•At 3 months, all patients received open label active stimulation until the 6-month outcome measure•Stim ON: 15.8±14.1points Sham: 1.4±3.8 points (P<0.001)
•BFMDRS score reduction

OCD Candidates for DBS
– The most severely disabled patients– 5 years of disease– Multiple medication and behavioral therapy
resistant– Predominant contamination behaviors
– Requires multidisciplinary team for patient selection including psychiatry, psychology, neuropsychology, neurosurgery, and ethics.

DBS for Obsessive Compulsive Disorder
60% of Patients with severe end stage OCD were responders with DBSImprovement in OCD scores (YBOCS), Quality of life (GAF)And depression (HAM-D)-------Led to new indication for depressionFDA approval US-HDE 2009

DBS for OCD• Clinical Trial:
– The most severely disabled patients– 5 years of disease, multiple medication resistant, 20 in-
patient admissions
• Results-- 60% of patients were significantly improved– Decreased obsessions, compulsion, improved functioning, – Improved self care, social and occupational functioning,
Quality of life, functioning, working, dating, getting married, living independently

Surgical Procedure• Brain imaging• Computerized guidance• Micro-robotics• Electrical recording of
brain function• mm precision

STN
STN
RN
RN
SNr
SNr
Direct targeting

Anatomical Atlas morphing and Targeting

Physiological Mapping• Microelectrode recording
(MER)
• microstimulation
• Macrostimulation with DBS electrode

Intraoperative mapping

Intra-operative DBS Testing

Potential Complications/Risks
– Hemorrhage (inherent in any stereotactic procedure); may be silent or symptomatic
– Transient confusion
– Infection (typically occurs at neurostimulator site in chest when it does occur)
– Device related
– Stimulation related• Usually can be minimized or eliminated
by adjusting stimulation settings• Reversible paresthesia, dysarthria,
muscle contraction

Overview of Programming
• Anode/Cathode• Variables
– Contacts – 4 for each electrode
– Amplitude– Rate– Pulse Width– Monopolar vs Bipolar– Constant Current vs
Constant Voltage
• Soft Start• Impedance• Battery Status

0
1
2
3
DBS Lead Electrode Selection
* The negative electrode exerts the therapeutic effect
Lead Electrodes
BipolarUnipolar
0 1 2 3
0
1
2
3off
off
(-)
off
(+) positive off off
(+)
(-)
off

Monopolar vs Bipolar
• Bipolar stimulation can limit the spread and is beneficial to shaping field of stimulation

Stimulation Parameters
Rate(Hertz)
number of pulses per second
Pulse Width(sec)
duration of each stimulus
Amplitude(Volts)
intensity of stimulation

Movement Disorder DBS Management
• DBS programming goal– Deliver the therapy to the brain target of interest with avoiding
stimulation of surrounding structures
• Typically, initial programming of DBS is 2 - 4 weeks after DBS electrode implant
• Subsequent programming can be every 2-8 weeks for the first 3 months, and then every 3-6 months thereafter
• Commonly takes 6 months to obtain the best settings
• Many patients will require concurrent medication adjustments

Systematic Approach: Initial Programming
• Identify patients prominent symptoms and review expectation of DBS.
• Inspect and palpate hardware• Monopolar review – should be done with every initial
programming and when side effects suspected: – With constant rate (130) and pulse width (90) assess individual
contacts with monopolar settings with regards to threshold of stimulation and apparent improvement of symptoms while slowly increasing the amplitude
• Useful to identify anatomy and position within the target nuclei• Useful for future programming sessions and trouble shooting
• Trial of bipolar vs monopolar if low threshold• Check impedances and battery• Educate patient on use of patient programmer and/or
recharger if applicable

Systematic Approach: Subsequent DBS Programming
• Identify any problems or side effects related to DBS• Inspect and palpate hardware• Check impedances, battery and for activations• Adjust DBS parameters: common strategy is to make one parameter
change with little adjustments to other parameters. – Adjust amplitude with little or no change in rate or pulse width– Adjust rate with little or no change to amplitude or pulse width– Adjust pulse width with little or no change to amplitude or rate– Change bipolar and assess for threshold with resetting at tolerable level
• For PD, best to program with patients in the “Off” state
• If PD, have patient take typical dose of PD medications and wait for medications to have taken effect
• Adjust medication if indicated

DBS Common Settings
• Settings for different indications and target
PW (µs) Rate (Hz) STN – PD 60-90 130-185
GPi - PD 90-120 130-185
VIM Tremor 60-90 100-185
GPi Dystonia 120-450 60-145

DBS Problem Solving
• No improvement
• Contracture/slurred speech
• Persistent numbness
• Double vision
• Visual disturbances
• Dyskinesia
• Autonomic symptoms
Review anatomical location of stimulation with monopolar review

Regional STN Anatomy
– Target is the dorsal-lateral portion of STN
• Medial lemniscus – posterior– Stimulation can cause
intolerable paresthesia• Internal Capsule – anterior,
lateral and ventral– Stimulation can cause tonic
contracture• CN III – medial caudal
– Stimulation can cause diplopia• Hypothalamus – medial rostral
– Stimulation can cause autonomic symptoms
• Ventral Medial STN– Stimulation can cause mood
changes IC = internal capsule
STN = subthalamic nucleus
ML = medial lemniscus
RN = red nucleus

Regional VIM Anatomy
– Internal Capsule – ventral and lateral
• Stimulation can cause tonic contracture
– Ventral Caudal (Vc) thalamus (sensory relay) – posterior
• Stimulation can cause intolerable paresthesia
– Ventral Oralis Posterior (Vop) thalamus – anterior
• Stimulation may cause no effect on tremor
Vo = ventral oral (pallidal relay)Vim = ventral intermediate (cerebellar relay)Vc = ventral caudal (principle somatosensory nucleus)IC = internal capsule

Regional GPi Anatomy
• Internal Capsule - posterior– Stimulation can cause
tonic contracture
• Optic Tract – ventral– Stimulation can cause
visual disturbances
GP = globus pallidusIC = internal capsuleOT = optic tract

Long term Maintenance
• No MRI other than of the head with use of specific restrictions.• Avoid activities that cause excessive torque on the neck• Awareness of electromagnetic fields that can cause DBS devices to
turn on/off.• Battery drain – monitor battery status• Watch for signs of skin breakdown or irritation around DBS
hardware, and inspect for signs of disconnections or lead wire migration
• Check and reset activations with each programming session, and check impedance levels.
• If concern for device failure, check unit if on/off, number of activations, battery status, hardware malfunction (imaging), and impedances