Embed Size (px)
Citation preview

Decreasing Time to Antibiotics inFebrile Patients With Central Lines inthe Emergency DepartmentMeghan Jobson, PhDa, Moses Sandrof, MSb, Timothy Valeriote, RNb, Abigail Lees Liberty, BSa, Christine Walsh-Kelly, MDc,Cheryl Jackson, MDb,c
abstractBACKGROUND AND OBJECTIVE: Rapid antibiotic administration is essential for thesuccessful management of patients who have central lines and present withfever. We conducted an emergency department (ED) improvement initiative todeliver antibiotics to 90% of patients within 60 minutes and to minimizeprocess variation.
METHODS: Our setting was an academic ED. We assembled a multidisciplinaryteam, identified contributing factors to the care delivery problem, determinedkey drivers and intervention steps, implemented changes, and used strategiesto engage ED staff and promote sustainability. Outcomes were analyzed byusing a time series design with baseline data and continuous postinterventionmonitoring. Outcomes included percentage of patients receiving antibioticswithin 60 minutes, time to antibiotic administration, and accuracy for triageacuity and chief complaint.
RESULTS: An 8-month baseline period revealed that 63% of patients receivedantibiotics within 60 minutes of arrival, with a mean time to antibiotics of 65minutes. Multiple Plan-Do-Study-Act (PDSA) cycles were used to improvepatient identification and initial management processes. The percentage ofpatients receiving antibiotics within 60 minutes of arrival was increased to99% (297 of 301), and mean time to administration decreased to 30 minutes(95% confidence interval: 28–32). These gains were sustained for 24 months.Subanalysis identified a racial discrepancy, with African American patientsexperiencing significantly longer delays than patients of other races (95 vs 61minutes; P , .05); this discrepancy was eliminated with our initiative.
CONCLUSIONS: Our initiative exceeded our goal of 90% antibiotic delivery within60 minutes for a sustained period of at least 24 months, decreased processvariation and mean time to antibiotic administration, and eliminated race-based discrepancies in care.
Central venous access devices placepatients at risk for bacterial entry intothe bloodstream, facilitate systemicspread, and contribute to thedevelopment of sepsis.1 Rapidrecognition and antibiotic interventionin these patients, when febrile, arecritical. Delays in time to antibiotic(TTA) delivery have been correlatedwith poor outcomes in febrile
neutropenic patients.2 TTA wasidentified as a measure of quality ofcare in pediatric oncology centers, anda survey reported that most centersused a benchmark of ,60 minutesafter arrival, with .75% of pediatriccancer clinics having a mean TTA of,60 minutes.3 The same study,however, noted that more than half ofthe emergency departments (EDs)
aSchool of Medicine, Departments of bEmergency Medicine,and cPediatrics, Division of Emergency Medicine, Universityof North Carolina, Chapel Hill, North Carolina
Dr Jobson conceptualized and designed the study,created the database, collected and analyzed thedata, was research leader in the improvement focusgroup, and drafted the manuscript; Mr Sandrofprovided guidance on the data collection tool,performed statistical analyses, and drafted andedited the manuscript; Mr Valeriote conceptualizedand designed the study, collected the data, was thenursing leader in the improvement focus group, andedited and approved the manuscript; Ms Libertycollected the data, provided guidance on theanalysis and data collection tool, and edited andapproved the manuscript; Dr Walsh-Kelly providedguidance on data analysis and drafting of themanuscript, and edited and approved themanuscript; Dr Jackson provided guidance on studyquestions, was a physician leader in theimprovement focus group, and edited and approvedthe manuscript; and all authors approved the finalmanuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-1192
DOI: 10.1542/peds.2014-1192
Accepted for publication Jul 14, 2014
Address correspondence to Meghan Jobson, PhD,Department of Pediatrics, University of NorthCarolina, 231 MacNider CB 7225, Chapel Hill, NC27519. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,1098-4275).
Copyright © 2015 by the American Academy ofPediatrics
FINANCIAL DISCLOSURE: The authors have indicatedthey have no financial relationships relevant to thisarticle to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors haveindicated they have no potential conflicts of interestto disclose.
PEDIATRICS Volume 135, number 1, January 2015 QUALITY REPORTby guest on April 12, 2017Downloaded from

examined had a mean TTA .60minutes for these patients. Timelydelivery of antibiotics in the ED canbe a challenge. A retrospective studyfrom 2004 reported a mean of 170minutes from triage to antibioticdelivery in this population.4
Recent studies have describedinterventions to decrease TTA infebrile pediatric patients.5 However,to the best of our knowledge, nostudy has addressed sustainability,which is one of the most significantchallenges for quality improvementefforts. One goal of these efforts is todetermine whether, after cessation ofthe active intervention, the effect hasbeen stably sustained.
The University of North Carolina(UNC) Hospitals ED provides care for∼65 000 patients annually, including14 000 pediatric patients aged ,19years. Acute management ofambulatory patients who have centrallines and fever often occurs in theED. Ongoing management of pediatricpatients with central lines isprovided by multiple pediatricspecialists, including oncologists,gastroenterologists, and hematologists.ED management of these patients,when febrile, varies significantly,making it challenging to provideefficient, effective, and standardizedED care. In addition to the challengespresented by this variation in care,several UNC Hospitals ED staffbelieved that febrile pediatric patientswith central lines experiencedunacceptable delays before receivingantibiotics. To validate this perception,a system to identify and review EDpatient encounters was developed andtested. Examination of a 10-monthsample revealed that only 63% ofpatients received antibiotics within60 minutes of arrival, and the meanTTA was 65 minutes (range: 6–358minutes). Seeing an opportunity toreduce the TTA and minimizevariability, an improvement team wasformed comprising frontline nursingstaff, volunteer research assistants,and attending physicians.
We designed an ED initiative toaddress our key care deliveryproblem (ie, delayed antibioticadministration) in our targetpopulation: children with centrallines presenting with fever as thechief complaint, regardless ofunderlying condition. The primaryaim of the initiative was to achieve90% of patients receiving antibioticswithin 60 minutes of ED arrival; oursecondary goal was to reduce meanTTA to ,60 minutes and narrow thevariation. We organized our initiativeto actively engage caregiving staff ina structured approach to developa consistent and sustainable processto expedite antibiotic delivery.Specifically, we planned to identifya benchmark and characterize andresolve any factors that wereassociated with delayed antibioticadministration.
METHODS
Setting
UNC Hospitals is a large, suburban,academic medical center that servesthe southeastern region of the UnitedStates and all 100 counties in NorthCarolina. Tertiary pediatric care,including pediatric and neonatal levelIV intensive care, level I trauma care,and emergency care, are provided.Pediatric emergency medicinephysicians provide care in thepediatric ED between 8:00 AM and2:00 AM. During the remaining hours,board-certified emergency medicinephysicians in the general ED care forpediatric cases.
Planning the Intervention
A multidisciplinary improvementteam was formed. We analyzed theresults of the 8-month baselineanalysis of current performance,reviewed the oncology literature andreports from other hospitals,obtained expert opinion to determinea benchmark for TTA, and establishedthe initiative aims. The teamconsulted with other hospital staffinvolved in the care of pediatric
patients with central lines andidentified several additionaloperational factors that could beimproved. The improvement teamoutlined the current process,identified key factors contributing tothe delay in antibiotic administration,and suggested potential solutions totest using the PDSA model. Key areasfor improvement included patientidentification at triage, appropriatelevel of triage assigned, antibioticavailability, and a standardmanagement process.
The initiative was conducted in 3phases. Phase I focused on definingthe problem, communicating theresults of the baseline analysis andTTA benchmark to the ED staff,mapping the existing process,eliminating the step to contact thepatient’s subspecialist before theinitial treatment, and implementingsolutions to address patientidentification, triage acuityassignment, and access to antibiotics.Phase II focused on refining andembedding the patient identificationand acuity assignment processes intostandard practice through PDSAcycles, structured communicationwith staff, and transparency ofperformance data for key measures toenhance learning. Phase III used thekey lessons learned and datacollected from phases I and II tofurther redesign a standard patientidentification and initial managementprocess and to develop a guideline forthe updated process. Finally, duringthe sustainability phase, activeintervention ceased, outcomes weremonitored, and communication withED staff continued.
The primary strategies used in thepresent initiative focused on staffengagement and learning fromcollected and analyzed data. Effectivecommunication, awareness of staffperformance (by using datacollection, analysis, and resultreporting in real-time), and timelyindividual feedback provided theframework to deploy these strategies.
e188 JOBSON et alby guest on April 12, 2017Downloaded from

We created a system in whichsupervisors monitored staffmembers’ performance andconducted individual staff coachingsessions to identify factorscontributing to performance lapsesand to invite suggestions forimprovement.
Planning the Study of theIntervention
Key measures selected for thisinitiative included the primaryoutcome, proportion of patientsreceiving antibiotics within 60minutes of ED arrival, anda secondary outcome (ie, mean TTA).Process measures were also includedand defined: correct chief complaintrecorded (fever/central line) andaccurate triage acuity (2) assigned.Data for race, primary language, andage were collected to identifypossible patient-level contributors toincreased TTA. These patientcharacteristics were obtained by self-report at the time of ED registration.
Analysis
Outcomes of the initiative werestudied by using a time series designwith baseline data obtained from thepreceding 8 months and continuousmonitoring after cessation of activeinterventions. The primary outcomeanalyzed was the percentage ofpatients receiving antibiotics within60 minutes of ED arrival. Accuratetriage classification and chiefcomplaint were monitored to assessadoption and adherence to thesechanges. A statistical process controlchart was used to monitorimprovement, with control limits setat 3 SDs and a shift of $8 pointsabove or below the mean beingindicative of special cause variation(equivalent to P , .01).6 Significancewas also measured by using a 2-samplet test, with P , .05 indicatingsignificance. Characteristics werecompared preintervention andpostintervention by using a Student’st test for ED shift, length of stay foradmitted patients, race, gender, age,
and primary language spoken. Theinstitutional review board of UNCHospitals approved this project.
RESULTS
Outcomes
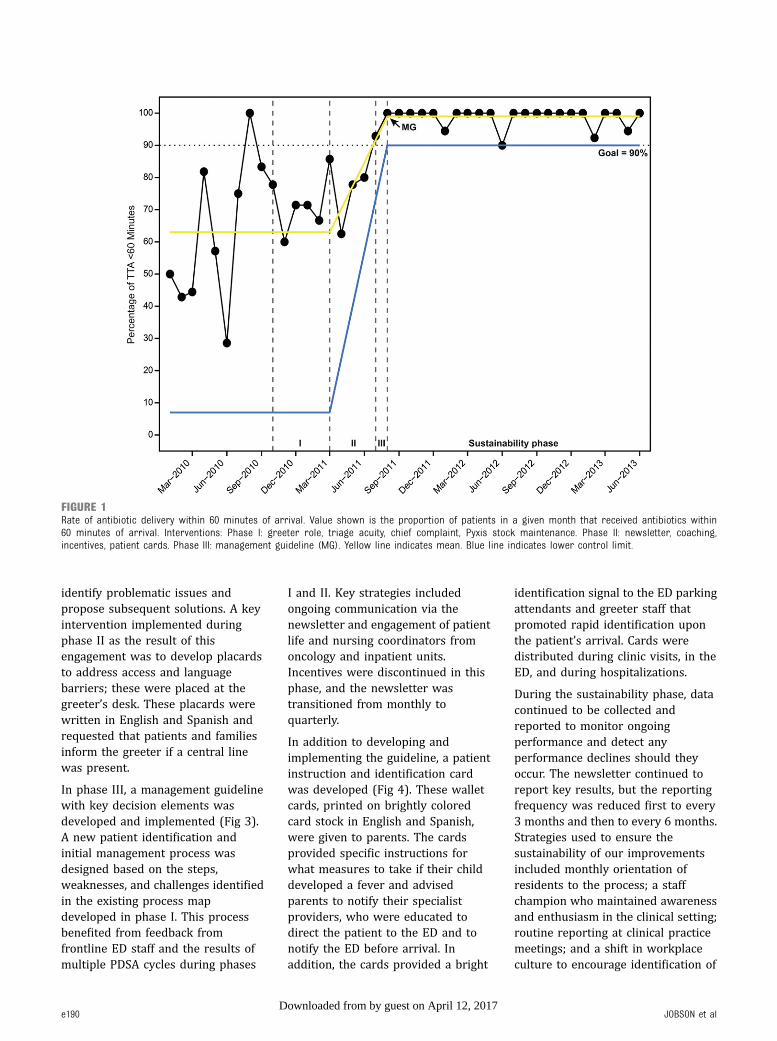
Over the course of this initiative, 479patient encounters that met criteriatook place (Table 1). TTA deliverywas tracked, and the percentage ofpatients receiving antibiotics within60 minutes of arrival increased from63% to 99% after 8 months,exceeding our goal of 90% (Fig 1).TTA was lowered from a monthlymean of 65 minutes to 30 minutes,and variation was significantlydecreased (Fig 2). Control chartsdemonstrated that antibioticadministration was reliably ,1 hourby phase III and has been sustainedfor 24 months since our initiative goalwas first met in June 2011.
Key improvement areas and specificinterventions for the initiative arelisted in Table 2. During phase I, theexisting processes for identifying andmanaging febrile patients with centrallines were mapped and analyzed. Keyinterventions that were tested andimplemented included revision of thegreeter role to include identificationof patients with central linespresenting with fever and notificationof the triage nurse, designation ofchief complaint as “fever/centralline,” re-education and re-emphasis oftriage acuity as 2 for these patients,and routine stocking of the Pyxismachine (CareFusion Corporation,San Diego, CA) with requiredantibiotics. ED nurses and greeterswere informed of the baselineperformance results, the benchmark
suggested in the literature and bylocal experts, the improvementinitiative goals, and their new roleexpectations. Reminders printed onbright card stock were attached to themonitor of every computerworkstation used to access theelectronic health record. Phase Iinterventions alone had little effect ontimeliness. However, retrospectivedata analysis of the phase I changeshelped the team to identify areas inneed of improvement.
In phase II, strategies focused onimproving performance by providingdata and other information forlearning, using a monthly newsletter,public sharing of aggregatecompliance data tracking, individualreports of personal performance,personal coaching of noncompliantstaff, and rewards for compliance.The monthly newsletter includedgraphs displaying performance fortimely antibiotic administration,accurate triage acuity designation,and appropriate chief complaintdesignation. The newsletter alsoprovided information about theinitiative, highlighted a staff membereach month who successfullyachieved the initiative outcomes, andoffered solutions to emergingproblems with the initiative (ie, how toadminister drugs if the central lineport is blocked). The ED suppliedhospital dining gift cards as incentivesfor performance. Newsletters wereposted throughout the ED, in breakrooms, and in high traffic areas withhigh visibility, and they were designedto be visually appealing, brief,motivating, and fun to read.
An additional key strategy used wasthe active encouragement of staff to
TABLE 1 Patient Demographic Characteristics (N = 479), January 2010 to June 2013
Characteristic Value
Mean age 6.6 yGender 54% maleRace 59% White, 23% Hispanic, 10% African American, 2% Asian, 1%
Native American, 5% otherPreferred language 77% English, 23% SpanishManaging specialty 75% oncology, 11% gastroenterology, 8% hematology, 6% other
PEDIATRICS Volume 135, number 1, January 2015 e189by guest on April 12, 2017Downloaded from
identify problematic issues andpropose subsequent solutions. A keyintervention implemented duringphase II as the result of thisengagement was to develop placardsto address access and languagebarriers; these were placed at thegreeter’s desk. These placards werewritten in English and Spanish andrequested that patients and familiesinform the greeter if a central linewas present.
In phase III, a management guidelinewith key decision elements wasdeveloped and implemented (Fig 3).A new patient identification andinitial management process wasdesigned based on the steps,weaknesses, and challenges identifiedin the existing process mapdeveloped in phase I. This processbenefited from feedback fromfrontline ED staff and the results ofmultiple PDSA cycles during phases
I and II. Key strategies includedongoing communication via thenewsletter and engagement of patientlife and nursing coordinators fromoncology and inpatient units.Incentives were discontinued in thisphase, and the newsletter wastransitioned from monthly toquarterly.
In addition to developing andimplementing the guideline, a patientinstruction and identification cardwas developed (Fig 4). These walletcards, printed on brightly coloredcard stock in English and Spanish,were given to parents. The cardsprovided specific instructions forwhat measures to take if their childdeveloped a fever and advisedparents to notify their specialistproviders, who were educated todirect the patient to the ED and tonotify the ED before arrival. Inaddition, the cards provided a bright
identification signal to the ED parkingattendants and greeter staff thatpromoted rapid identification uponthe patient’s arrival. Cards weredistributed during clinic visits, in theED, and during hospitalizations.
During the sustainability phase, datacontinued to be collected andreported to monitor ongoingperformance and detect anyperformance declines should theyoccur. The newsletter continued toreport key results, but the reportingfrequency was reduced first to every3 months and then to every 6 months.Strategies used to ensure thesustainability of our improvementsincluded monthly orientation ofresidents to the process; a staffchampion who maintained awarenessand enthusiasm in the clinical setting;routine reporting at clinical practicemeetings; and a shift in workplaceculture to encourage identification of
FIGURE 1Rate of antibiotic delivery within 60 minutes of arrival. Value shown is the proportion of patients in a given month that received antibiotics within60 minutes of arrival. Interventions: Phase I: greeter role, triage acuity, chief complaint, Pyxis stock maintenance. Phase II: newsletter, coaching,incentives, patient cards. Phase III: management guideline (MG). Yellow line indicates mean. Blue line indicates lower control limit.
e190 JOBSON et alby guest on April 12, 2017Downloaded from

barriers, recommendations forchanges, and self-reporting of lapses.In addition, a nursing order set wasdeveloped to hardwire key elementsof the management guideline into ournew electronic health record beingimplemented in the hospital. Therollout of this system did not takeplace before the end of the studyperiod; however, this changedemonstrates our ongoingcommitment to sustain our improvedprocess.
Ongoing analysis of data collectedduring the initiative revealed that dayshifts, when pediatric emergencyphysicians provide care, were the firstto meet goals. Initially, TTA exceeding60 minutes tended to occur after7:00 PM and in the general EDversus the pediatric ED. Enhancedcommunication efforts directedtoward both nursing and physiciannight shift staff resulted ina resolution of this discrepancy byphase III of the initiative.
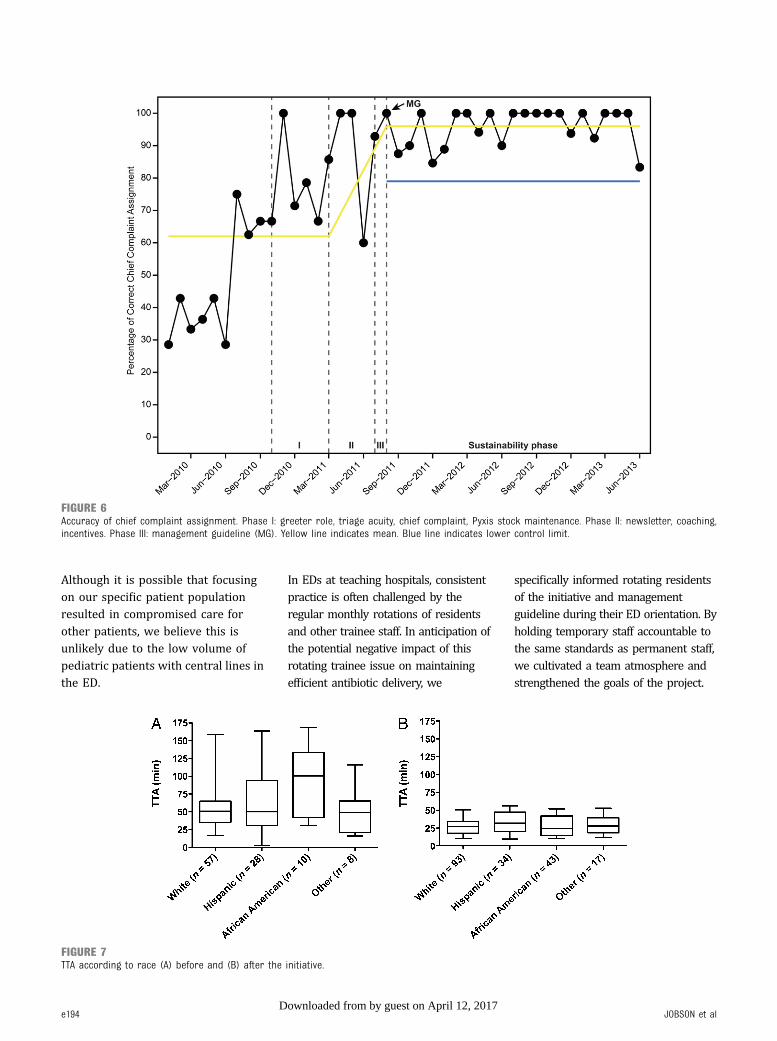
For all staff involved in encounterswith antibiotic administration delays,loop closure was ensured via bothe-mail and an in-person consultationencounter. Emphasis was placed onmotivating the staff and solicitinginput on how to ensure compliance toencourage ownership andengagement. Accurate assignment ofacuity correlated with timeliness ofTTA in the preintervention period(P = .04, Pearson’s r = 0.21) (Fig 5).Although there was no correlationbetween timeliness of TTA andcorrect chief complaint assignment(“fever/central line”) before theintervention, there was a strongcorrelation during the sustainabilityphase (P , .0001, R = 0.33) (Fig 6).
Analysis of baseline data from 2010revealed significantly longer delays inantibiotic delivery specifically inAfrican-American patients (Fig 7).Although these patients comprisedonly 10% of our study population, thedifference was striking andstatistically significant (P , .05).
FIGURE 2Time from ED arrival to administration of antibiotics. Phase I: greeter role, triage acuity, chief complaint, Pyxis stock maintenance. Phase II: newsletter,coaching, incentives. Phase III: management guideline (MG). Yellow line indicates mean. Blue lines indicate upper and lower control limits.
TABLE 2 Key Improvement Areas and Specific Interventions for the Initiative
Key Improvement Area Improvement Step Improvement Group
Patient identification at triage 1. Greeter role clarified to identifypotential patients
ED nurses, project team
2. Posted placards at triageHematology-oncology and
inpatient staff3. Wallet card for families
Triage acuity assignment 1. Re-educated nurses on correcttriage acuity of 2
ED nurses
2. Nurse education3. Compliance reports4. Monthly newsletter
Antibiotic availability 1. Pyxis stocked routinely with antibiotics ED nursesStandard process 1. Guideline developed ED nurses, project team,
volunteers2. Patient identification cards
PEDIATRICS Volume 135, number 1, January 2015 e191by guest on April 12, 2017Downloaded from

Although no specific interventionswere implemented, the gap waseliminated when our timeliness goalswere met. During the sustainabilityphase, TTA was similar between allracial groups. In the years before andafter the intervention, no differencesin TTA based on gender, diagnosis, orpreferred language were identified.
DISCUSSION
Our pediatric ED staff identified TTAadministration in febrile patients withcentral lines as an area forimprovement. Over the course of ourinitiative, the proportion of patientsreceiving antibiotics within 60minutes of ED arrival rose from 63%to 99% and the mean TTA waslowered from 65 to 30 minutes,a 51% decrease. In addition, race-based differences in TTA that existedbefore our initiative were eliminated.Numerous PDSA cycles wereconducted and several changesimplemented during the course of theinitiative. Changes implementedduring phases I and II did notimmediately result in a significantreduction in TTA administration.Significant improvement wasultimately achieved and sustainedwith the redesign of our EDmanagement process andimplementation of our practiceguideline.
Multiple studies in the past decadehave revealed the need for systematicand rapid administration ofantibiotics in pediatric patients withcentral lines. Typically, such patientsare medically complex, and thedevelopment of sepsis can be a life-threatening event. Most cancercenters successfully use a benchmarkmaximum of 60 minutes to antibioticdelivery in febrile patients witha central line, and we adopted thisbenchmark as the primary initiativegoal and outcome measure.3 Recently,a quality improvement initiativefocused on introducing sucha benchmark in a pediatric ED.5 Theinitiative achieved 88.5% of patients
FIGURE 3Guideline for initial ED management of febrile pediatric patients with central lines. CBC/diff, com-plete blood cell count with differential; GI, gastroenterology; IV, intravenous; N/S, normal saline; PED,pediatric ED.
FIGURE 4Identification card for families of pediatric patients with central lines.
e192 JOBSON et alby guest on April 12, 2017Downloaded from

receiving antibiotics within 60minutes. Although this initiativesuccessfully lowered TTA, variableresults arose with time during the 15months after implementation,especially toward the end of theobservation period. This project listedparents’ refusal of central line accessand complications of analgesiaplacement as challenges to loweringTTA. Staff user fatigue was listed asa possible barrier to sustainability ofthe measure, possibly due to a lack ofcontinuous feedback regardingoutcomes.
The present initiative achieved andconsistently sustained a goal ofrapidly delivering antibiotics tofebrile pediatric patients with centrallines. We attribute much of thesuccess of our efforts to both theinvolvement of an effective staffcaregiver champion who encourageda culture shift from complacentroutine to active engagement and
a deliberate plan to seek feedbackfrom the front line to improve theprocess. Discussions of recentlyreported performance results werecommon during work hours,indicating a high level of staffmember ownership of the initiative.Additional factors contributing to thesuccess of the initiative were physicalreminders of the initiative oncomputers and elsewhere throughoutthe department.
Elimination of racial and otherdisparities in health care is a keyfocus of many national agencies,including the Centers for DiseaseControl and Prevention, the Agencyfor Healthcare Research and Quality,and the Office of Minority Health,among many others. In the analysis ofour preintervention data, weidentified a racial disparity in TTA asAfrican-American patientsexperienced greater delays inantibiotic administration. Similarly,
a highly publicized study identifiedracial/ethnic disparities in ED painmanagement, finding that non-Hispanic black patients waited longerfor pain medication than othergroups.7 Although our initiative didnot focus on identifying the reasonsfor our racial disparity and did notimplement any specific interventions,we believe it is important documentand report these disparities. It is alsoof interest to report the elimination ofthis disparity, which may haveresulted from a number of factors,including staff awareness andimplementation of a standardmanagement process.
Our improvement initiative had onesignificant limitation. Althoughinclusion of a balancing measure isoptimal for improvement initiatives,we were unable to identify aneffective and meaningful balancingmeasure and did not measure impacton the care of other ED patients.
FIGURE 5Accuracy of triage acuity assignment. Phase I: greeter role, triage acuity, chief complaint, Pyxis stock maintenance. Phase II: newsletter, coaching,incentives. Phase III: management guideline (MG). Yellow line indicates mean. Blue line indicates lower control limit.
PEDIATRICS Volume 135, number 1, January 2015 e193by guest on April 12, 2017Downloaded from
Although it is possible that focusingon our specific patient populationresulted in compromised care forother patients, we believe this isunlikely due to the low volume ofpediatric patients with central lines inthe ED.
In EDs at teaching hospitals, consistentpractice is often challenged by theregular monthly rotations of residentsand other trainee staff. In anticipation ofthe potential negative impact of thisrotating trainee issue on maintainingefficient antibiotic delivery, we
specifically informed rotating residentsof the initiative and managementguideline during their ED orientation. Byholding temporary staff accountable tothe same standards as permanent staff,we cultivated a team atmosphere andstrengthened the goals of the project.
FIGURE 6Accuracy of chief complaint assignment. Phase I: greeter role, triage acuity, chief complaint, Pyxis stock maintenance. Phase II: newsletter, coaching,incentives. Phase III: management guideline (MG). Yellow line indicates mean. Blue line indicates lower control limit.
FIGURE 7TTA according to race (A) before and (B) after the initiative.
e194 JOBSON et alby guest on April 12, 2017Downloaded from

CONCLUSIONS
We conducted an improvementinitiative in the pediatric ED thatconsistently lowered TTA in febrilepediatric patients with a central line.This change was sustained in the2 years after active intervention thatwe continued to monitor outcomes. Inaddition, we discovered and
eliminated a race-based TTAdiscrepancy in African-Americanpatients.
ACKNOWLEDGMENTS
The authors acknowledge JamesCompton, RN and Daniel Macklin, MDfor their initial work on this project,the Pediatric Emergency Nursing
Clinical Practice Group forcontributing to the study design, andAshley Quattlebaum, RN andKatherine Sabo, RN for datacollection. The authors alsoacknowledge Stuart Gold, MD forassistance with oncology patientguidelines and comments on themanuscript.
REFERENCES
1. Blanchard AC, Fortin E, Rocher I, et al.Central line-associated bloodstreaminfection in neonatal intensive care units.Infect Control Hosp Epidemiol. 2013;34(11):1167–1173
2. Fletcher M, Hodgkiss H, Zhang S, et al.Prompt administration of antibiotics isassociated with improved outcomes infebrile neutropenia in children with cancer.Pediatr Blood Cancer. 2013;60(8):1299–1306
3. McCavit TL, Winick N. Time-to-antibioticadministration as a quality of caremeasure in children with febrile
neutropenia: a survey of pediatriconcology centers. Pediatr Blood Cancer.2012;58(2):303–305
4. Perrone J, Hollander JE, Datner EM.Emergency department evaluation ofpatients with fever and chemotherapy-induced neutropenia. J Emerg Med. 2004;27(2):115–119
5. Volpe D, Harrison S, Damian F, et al.Improving timeliness of antibiotic deliveryfor patients with fever and suspectedneutropenia in a pediatric emergencydepartment. Pediatrics. 2012;130(1).
Available at: www.pediatrics.org/cgi/content/full/130/1/e201
6. Langley GJ, Moen RD, Nolan KM, Nolan TW,Norman CL, Provost LP. The ImprovementGuide: A Practical Approach to EnhancingOrganizational Performance. 2nd ed. SanFrancisco, CA: Jossey-Bass; 2009
7. Johnson TJ, Weaver MD, Borrero S, et al.Association of race and ethnicity withmanagement of abdominal pain in theemergency department. Pediatrics. 2013;132(4). Available at: www.pediatrics.org/cgi/content/full/132/4/e851
PEDIATRICS Volume 135, number 1, January 2015 e195by guest on April 12, 2017Downloaded from

DOI: 10.1542/peds.2014-1192; originally published online December 8, 2014; 2015;135;e187Pediatrics
Walsh-Kelly and Cheryl JacksonMeghan Jobson, Moses Sandrof, Timothy Valeriote, Abigail Lees Liberty, Christine
Emergency DepartmentDecreasing Time to Antibiotics in Febrile Patients With Central Lines in the
ServicesUpdated Information &
/content/135/1/e187.full.htmlincluding high resolution figures, can be found at:
References
/content/135/1/e187.full.html#ref-list-1at:This article cites 6 articles, 2 of which can be accessed free
Citations /content/135/1/e187.full.html#related-urls
This article has been cited by 5 HighWire-hosted articles:
Subspecialty Collections
/cgi/collection/quality_improvement_subQuality Improvement
/cgi/collection/administration:practice_management_subAdministration/Practice Management
/cgi/collection/emergency_medicine_subEmergency Medicinethe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints /site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2015 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 12, 2017Downloaded from

DOI: 10.1542/peds.2014-1192; originally published online December 8, 2014; 2015;135;e187Pediatrics
Walsh-Kelly and Cheryl JacksonMeghan Jobson, Moses Sandrof, Timothy Valeriote, Abigail Lees Liberty, Christine
Emergency DepartmentDecreasing Time to Antibiotics in Febrile Patients With Central Lines in the
/content/135/1/e187.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2015 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 12, 2017Downloaded from



























