Embed Size (px)
Citation preview

Muhammad Arif
M.Phil Health Economics (2012-14)
Supervised by
Dr. Mahmood Khalid
Mr. Ajmal Jahangeer
Friday, November 20, 2015
DECOMPOSING THE SOCIOECONOMIC
INEQUALITIE IN CHILD MORTALITY IN
PAKISTAN

INTRODUCTION
Inequalities in health discovered in 19th century, But, from two decades received meticulous attention in developing countries(Wagstaff, 2000)
Leading Health Economic issue in higher-, middle- and low -income countries(Mackenbach, 2006), as well as in Pakistan (Alam, Nishtar, Amjad, & Bile, 2010)
Goal of several international, national organizations and governments to reduce inequalities
e,g. World Bank, WHO, Government programmes, policies (WHO, 2013)
“economic inequalities in health ” Effects different social groups, economy, and development of a country (Wagstaff, 2000)
poor segment of population become more vulnerable to disease, dies more than rich, (Marmot & Wilkinson 1999)
2

INTRO----CONT..
Since neonatal, post-neonatal and under-five mortality
in more developed countries have progressively
dropped and presently have been reduced to nearly negligible points
However, in Pakistan, not encouraging
as neonatal MR =55, post-neonatal MR=19 and under-
five MR= 89 (PDHS, 2012-13), Very far from MDGS Target
Inadequate literature on child mortality inequality with
reference to Pakistan,
It is likely need to investigate the levels and underlining
reasons, drivers behind these inequalities, which helps to reduce health inequalities and derive the related
policy implications
3

OBJECTIVE OF THE STUDY
The objective of this study is
To measure the economic-related inequalities
in child mortality, and,
To quantify the determinant’s contribution to
child mortality inequality
4

RESEARCH QUESTIONS
Does child mortality inequality between
the poor and rich exist in Pakistan?
What are the major contributing factors
to inequality in child mortality?
5

HYPOTHESES
The study test the following hypotheses:
There is no inequality in child mortality
between poor and non-poor in Pakistan
Socioeconomic determinants have no
significant contribution in child mortality
inequality
Demographic determinants do not have
any significant contribution in child
mortality inequality
6

SIGNIFICANCE OF THE STUDY
May fill the knowledge gap on
inequalities in health in Pakistan
The finding may help to support better
design of health policies that aim at
reducing inequalities in child health
The study will help policy makers and
programmers to allocate resources
equitably and efficiently.
7

THEORETICAL FOUNDATION
Mosely and Chen (1984) presented an
analytical framework for the study of
child survival in developing countries
Production Function of health
8

9
ECONOMIC
-RELATED
INEQUALITY
Environmental
Geographic
and cultures
Demographic
Socioeconomic
HEALTH OUT-
COMES
Demographic, socioeconomic, geographic and
cultural Determinants of health
A Simplified Conceptual Framework of the Relationship between economic-related Inequality and Health
Outcomes

OUTCOME VARIABLES
Neonatal mortality: - Deaths of the newborn baby within the first
month of life (0-28 days)
Post-neonatal mortality: - It is the difference between the infant
and neonatal mortality. Deaths at age 1-11 months (from
completed age 1 month till before completed age 12 months)
Under-five mortality: – Deaths from birth till completed age 60
months is considered as deaths under the age of five
10

DETERMINANTS
Child characteristics
Gender, Birth order of the child
Parental Characteristics
Maternal age at time of birth,
Type of delivery( normal , C-section)
Birth interval (Risky, non risky)
Mother’s previous history of pregnancy loss
Antenatal care (prenatal visits)
Parental Education
Job/employment
House Hold characteristics
Economic status/ wealth index (quintile)
Type of fuel used for coking(solid, Gas, electricity & liquid)
Type of drinking water (improved, not improved)
Toilet facility (unhygienic and Hygienic)
Area of residence (rural/urban),
Region (Provinces)
11

DATA
PDHS (2012-2013)
Ever married questioner
Data set “Kids Record” Children under-Five
Sample of under-five children born a live 11,763
Neonatal deaths 551
Post-Neonatal deaths 277
Under-five deaths 828
12

Methodology
13

Concentration curve
L(p) concentration curve
Line of equality (45˙ line)
Y-axis=cumulative proportion of outcome variable
X-axis=cumulative proportion of individuals ranked by economic status
If concentration curve is above the diagonal, the concentration index value will be is negative and concentrated to poor and vice versa
the concentration curve coinciding with the diagonal, the value of the concentration index is zero.
14

CONCENTRATION INDEX
𝐶 =2
𝜇 𝐶𝑜𝑣(𝑦𝑖 , 𝑟)
µ= mean health outcome,
y=health outcome variable,
r =is the rank of the individual in the wealth distribution
It measures the values between -1 and +1.
Negative sign =pro-poor
Positive sign = pro-rich
0=No inequalities
15

DECOMPOSITION OF CONCENTRATION
INDEX
Decomposition analysis helps to measure the pure
contribution of the determinant of health outcome
variable
Adam Wagstaff Suggested
𝑦𝑖 = 𝛼 + 𝛽 𝑋𝑖 + 𝜀𝑡 ,
𝑦𝑖 =health outcome variable,
𝑋𝑖= set of socioeconomic determinants of health
outcome,
𝛽 is coefficient of determinant of 𝑋𝑖 and 𝜀𝑡 is a residual
term
16

Steps in Decomposition In the first step regression model of health outcome variable (y) on all
explanatory variable (x) was estimated and saved the β𝑘 coefficients of each explanatory variable X𝑘𝑖.
In the next step the mean of 𝑿 𝒌 of each 𝑿𝒌𝒊 and mean 𝝁 of outcome variable 𝑦𝑖 were calculated.
Then calculated the concentration index (CI) of outcome variable as well as the concentration index (CI) for each of the explanatory variable.
In this step the elasticity of 𝒚𝒊 with respect to each of X𝑘𝑖 were estimated.
𝑒𝑙𝑎𝑠 𝑦
𝑥𝑘 = β𝑘 𝑋 𝑘 / 𝜇
The pure contribution of each explanatory variable X𝑘𝑖 to the concentration index of outcome variable CI(𝑦𝑖 ) was estimated by multiplying the elasticity to concentration index of each determinant.
𝑐𝑜𝑛𝑡 X𝑘𝑖/CI(𝑦𝑖 ) = 𝑒𝑙𝑎𝑠 𝑦
𝑥𝑘 ∗ 𝐶𝐼(X𝑘𝑖)
The last step was to obtain the percentage contribution of an explanatory variable x to the concentration index of the outcome variable, simply the contribution is divided by concentration index of outcome variable and multiplied by 100.
17

DESCRIPTIVE STATISTICS
18

CHILD CHARACTERISTICS
Pearson’s Chi Square𝑋2=Significant
49.1 50.9
4.7 4.5 2.3 2.3 7.1 6.9
FEMALE MALE
CHILD MORTALITY
BY SEX OF CHILD
Live BirthsNeonatal MortalityPost-Neonatal MortalityUnder-Five Mortality
22.4 19.8
16.2
12.5
29
4.8 3.3 4.1 4.3 6
1.4 2.1 1.9 2.6 3.3 6.3 5.5 6 6.9
9.4
1 2 3 4 5+
CHILD MORTALITY BY BIRTH
ORDER
Live Births (%) Neonatal Mortality
Post-Neonatal Mortality Under Five Mortality
Pearson’s Chi Square𝑋2=Insignificant

PARENTAL CHARACTERISTICS
Pearson’s Chi Square𝑋2=Significant
Pearson’s Chi
Square𝑋2=Insignificant
87.8
12.1 4.7 4.2 2.4 1.8 7.1 6
NORMAL DELIVERY CAESAREAN
SECTION
CHILD MORTALITY
BY TYPE OF DELIVERY
Live Births
Neonatal Mortality
Post-Neonatal Mortality
Under Five Mortality
39.9 42
14
3.3 4.8 4.3 5.3 4.8 2.7 2.5 1.1 1 7.5 6.8 6.5 5.8
UNDER 19 20-24 25-29 30 AND ABOVE
CHILD MORTALITY BY AGE OF
MOTHER AT TIME OF BIRTH
Live Births Neonatal Mortality
Post-Neonatal Mortality Under Five Mortality

Pearson’s Chi Square𝑋2=Significant
Pearson’s Chi
Square𝑋2=Significant
16.2
6.8 7.9
44.5
24.5
5.1 3.3 3.6 5.7 3.2 2.4 1.4 1.2 3.4 1.2 7.5
4.7 4.8
9.1
4.3
NO VISIT 1 VISIT 2 VISITS 3 VISITS 4 + VISITS
CHILD MORTALITY BY PRENATAL VISITS
Live Births Neonatal Mortality
Post-Neonatal Mortality Under-Five Mortality
70.9
29
3.7 6.9 1.5 4.2 5.3 11.1
NON RISKY
INTERVAL
RISKY BIRTH
INTERVAL
CHILD MORTALITY BY
BIRTH INTERVALS
Live BirthsNeonatal MortalityPost-Neonatal MortalityUnder Five Mortality

Pearson’s Chi SquareX2=Significant Pearson’s Chi Square𝑋2=Significant
67.7
32.3
4.1 5.8 1.8 3.4 5.9 9.3
EDUCATED UN-EDUCATED
CHILD MORTALITY BY
FATHER’S EDUCATION
Live Births
Neonatal Mortality
Post-Neonatal Mortality
Under Five Mortality
57.2
14.3 17.6
10.8 5.4 4.7 3.8 2.4 3.01 2.5 1.2 0.5 8.4 7.2 5.01 2.9
NO EDUCATION PRIMARY SECONDARY HIGHER
CHILD MORTALITY BY MOTHER’S
EDUCATION LEVEL
Live Births Neonatal Mortality
Post-Neonatal Mortality Under-Five Mortality

Pearson’s Chi Square𝑋2=Significant Pearson’s Chi Square𝑋2=Insignificant
78.8
21.2
4.2 6.4 2.1 3.3 6.3 9.6
NOT WORKING WORKING
CHILD MORALITY BY MOTHER’S
WORKING STATUS
Live Births (%)Neonatal MortalityPost-Neonatal MortalityUnder Five Mortality
97.5
2.5 4.7 3.4 2.4 2.4 7.07 5.7
WORKING NOT WORKING
CHILD MORTALITY BY FATHER’S
WORKING STATUS
Live Births (%)Neonatal MortalityPost-Neonatal MortalityUnder Five Mortality

Pearson’s Chi Square𝑋2=Insignificant Pearson’s Chi Square𝑋2=Significant
92.8
7.2 4.6 4.7 2.4 1.8 7.1 6.6
MALE FEMALE
CHILD MORTALITY BY HEAD
OF HOUSEHOLD
Live Births (%)Neonatal MortalityPost-Neonatal MortalityUnder Five Mortality
68.2
31.8
4.5 5.1 2.2 2.7 6.6 7.8
NOT LOST LOST PREGNANCY
CHILD MORTALITY BY PREVIOUS
HISTORY OF PREGNANCY LOSS
Live Births (%)
Neonatal Mortality
Post-Neonatal Mortality
Under Five Mortality

HOUSEHOLD CHARACTERISTICS
Pearson’s Chi Square𝑋2=Significant
23.4
20 19.3
18.6 18.5
6 5.3
4.7 3.8
3 3.6
2.8 2 1.8 0.9
9.7
8.1 6.7
5.6
3.9
POOREST POOR MIDDLE RICH RICHEST
CHILD MORTALITY BY ECONOMIC STATUS OF
HOUSEHOLD
Live Births (%) Neonatal Mortality Post-Neonatal Mortality Under Five Mortality

15.1
84.8
4.3 4.7 2.8 2.2 7.2 7
NOT IMPROVED IMPROVED
CHILD MORTALITY BY TYPE
OF DRINKING WATER
Live Births (%) Neonatal Mortality
Post-Neonatal Mortality Under Five Mortality
Pearson’s Chi Square𝑋2=Insignificant
42.3
57.7
3.9 5.2 1.8 2.6 5.8 7.9
URBAN RURAL
CHILD MORTALITY BY AREA
OF RESIDENCE
Live Births Neonatal Mortality
Post-Neonatal Mortality Under Five Mortality
Pearson’s Chi Square𝑋2=Significant

Pearson’s Chi Square𝑋2=Significant Pearson’s Chi Square𝑋2=Significant
38.9
61.1
3.7 5.2 1.6 2.7 5.4 8
LIQUID, GAS & OTHER SOLID COOKING FUEL
CHILD MORTALITY BY TYPE OF
COOKING FUEL
Live Births Neonatal Mortality
Post-Neonatal Mortality Under-Five Mortality
69.3
30.7
4.2 5.7 1.9 3.2 6.2 8.9
IMPROVED TOILET FACILITY UN-IMPROVED TOILET
FACILITY
CHILD MORTALITY BY TYPE OF
TOILET FACILITY
Live Births (%) Neonatal Mortality
Post-Neonatal Mortality Under Five Mortality

Pearson’s Chi Square𝑋2=Significant
27.7
21.4
19.3
16.2
9.3
6.03 5.7 5
3.1
5.3 4.2
2.6 2.05 2.7 1.9 3.3 2.8 0.5
7.7 7.7
5.1
8.6
7
3.2
PUNJAB SINDH KHYBER
PAKHTUNKHWA
BALOCHISTAN GILGIT-
BALTISTAN
ISLAMABAD (ICT)
CHILD MORTALITY BY REGION
Live Births (%) Neonatal Mortality Post-Neonatal Mortality Under Five Mortality

MEASURES OF INEQUALITY
29

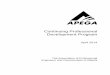
CONCENTRATION CURVES
30
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
0.00 0.20 0.40 0.60 0.80 1.00
Cu
mu
lativ
e %
of o
utc
om
e
va
ria
ble
Cumulative % of population, ranked from poorest to richest
Line of equality
under five mortality
neonatal mortality
post-neonatal
Concentration Curve & Concentration Index of Neonatal, Post-neonatal and Under-Five Mortality in Pakistan
Outcome Variables Concentration Index
Neonatal Mortality -.1528
Post-Neonatal Mortality -.2443
Under Five Mortality -.1834

DECOMPOSITION RESULTS
31

32
Regression
Result
Significant, at *1%. **5%, ***10%
Determinants
Neonatal Post-Neonatal Under-Five
Coef. P value Coef. P value Coef. P value
Child is Male -0.034* 0.000 -0.006 0.156 -0.007 0.233
Birth Order of Child 2 -0.051* 0.000 -0.003 0.292 -0.032* 0.000
Birth Order of Child 3 0.028 0.115 0.005*** 0.077 0.001 0.948
Birth Order of Child 4 -0.051* 0.002 -0.009 0.429 -0.013*** 0.073
Birth Order of Child 5 plus -0.020** 0.058 0.001 0.815 0.008 0.287
Age of Mother at Time of Birth -0.033* 0.000 -0.003 0.125 -0.004 0.633
Head of Household is Female -0.013 0.292 0.003 0.653 -0.009 0.432
Delivery by Caesarean 0.005* 0.003 0.007* 0.001 0.054*** 0.075
Father is Uneducated 0.052* 0.000 0.010* 0.002 0.004 0.457
Mother is Uneducated 0.062* 0.002 0.010** 0.032 0.013 0.564
Mother’s Primary Edu. -0.037** 0.041 -0.014* 0.000 -0.013 0.506
Mother’s Secondary Edu . -0.030*** 0.08 -0.005*** 0.077 -0.002 0.934
Father is Working -0.366* 0.000 -0.006 0.219 -0.004 0.85
Mother is Working 0.007 0.487 0.007* 0.006 0.008 0.378
Risky Birth Intervals 0.032* 0.000 0.025* 0.000 0.053* 0.000
History of Pregnancy Loss 0.049* 0.000 0.007 0.227 0.000 0.935
Prenatal one visit -0.036** 0.017 -0.011*** 0.082 -0.023* 0.002
Prenatal two visits -0.030** 0.037 -0.013 0.13 -0.008 0.443
Prenatal three visits 0.018*** 0.095 0013** 0.057 0.031* 0.000
Prenatal four plus visits 0.066* 0.001 -0.001 0.876 0.003 0.693
Poorest 0.017 0.503 0.007 0.26 0.024** 0.044
Poor 0.068* 0.000 0.013 0.231 0.029** 0.024
Middle 0.022** 0.043 0.002 0.725 0.008 0.433
Rich -0.018*** 0.084 -0.004*** 0.066 -0.000 0.951
Solid cooking Fuel 0.010 0.266 0.000 0.92 0.009 0.152
Un Hygienic toilet -0.011 0.384 -0.006 0.371 -0.003 0.551
Improved drinking Water -0.031** 0.021 -0.002 0.653 -0.021* 0.000
Rural 0.038* 0.002 -0.001 0.787 0.007 0.378
Sindh 0.001 0.956 0.008* 0.004 0.022 0.244
KPK -0.018** 0.053 0.014* 0.004 -0.001 0.846
Balochistan 0.028** 0.014 0.011* 0.003 0.013 0.276
Gilgit-Baltistan 0.097** 0.002 0.009** 0.052 -0.002 0.825
Islamabad -0.009 0.584 -0.006** 0.026 -0.030* 0.000

Determinants of Neonatal Mortality
Elasticity Concentration
Index Contribution
Percentage Contribution
Agrigated percentage contribution
Child is Male 0.032 0.003 0.000 -0.1 -0.1
Birth Order of Child 2 -0.12 0.094 -0.011 7.4
12 Birth Order of Child 3 -0.074 0.054 -0.004 2.6
Birth Order of Child 4 -0.06 -0.036 0.002 -1.4
Birth Order of Child 5 plus 0.026 -0.196 -0.005 3.4
Age of Mother at Time of Birth 0.2 0.059 0.012 -7.7 -7.7
Head of Household is Female 0.02 0.037 0.001 -0.5 -0.5
Delivery by Caesarean 0.034 0.449 0.015 -10 -10
Father is Uneducated -0.073 -0.377 0.027 -18 -18
Mother is Uneducated 0.31 -0.294 -0.091 59.5
39.8 Mother’s Primary Edu. 0.064 0.16 0.01 -6.7
Mother’s Secondary Edu . 0.048 0.415 0.02 -13
Father is Working 0.169 0.005 0.001 -0.6 -0.6
Mother is Working 0.058 -0.248 -0.014 9.5 9.5
Risky Birth Intervals 0.266 -0.077 -0.02 13.4 13.4
History of Pregnancy Loss -0.034 -0.022 0.001 -0.5 -0.05
Prenatal one visit -0.02 -0.225 0.004 -2.9
-5.3 Prenatal two visits -0.01 -0.039 0.000 -0.3
Prenatal three visits 0.196 -0.029 -0.006 3.7
Prenatal four plus visits 0.024 0.372 0.009 -5.8
Poorest 0.111 -0.793 -0.088 57.6
64.6 Poor 0.067 -0.341 -0.023 14.9
Middle 0.064 0.071 0.004 -2.9
Rich 0.017 0.467 0.008 -5
Solid cooking Fuel 0.045 -0.325 -0.015 9.6 9.6
Un Hygienic toilet 0.048 -0.463 -0.022 14.4 14.4
Improved drinking Water 0.248 0.054 0.013 -8.7 -8.7
Rural 0.014 -0.276 -0.004 2.5 2.5
Sindh -0.026 -0.046 0.001 -0.8
-10.8 KPK -0.057 0.036 -0.002 1.3
Balochistan -0.051 -0.236 0.012 -7.8
Gilgit-Baltistan -0.039 -0.351 0.014 -9.1
Islamabad -0.015 0.579 -0.009 5.6
Total Observed 103.7 103.7
Residual 0.006 -3.7 -3.7
Total 100 100
33

Determinants of Post-Neonatal
Mortality Elasticity
Concentration
Index Contribution
Percentage
Contribution
Aggregated
percentage
contribution
Child is Male -0.138 0.003 0 0.1 0.1 Birth Order of Child 2 -0.023 0.094 -0.002 0.9
3.2 Birth Order of Child 3 -0.033 0.054 -0.002 0.7
Birth Order of Child 4 0.048 -0.036 -0.002 0.7
Birth Order of Child 5 plus 0.012 -0.196 -0.002 0.9
Age of Mother at Time of Birth -0.224 0.059 -0.013 5.4 5.4 Head of Household is Female 0.009 0.037 0 -0.1 -0.1 Delivery by Caesarean 0.038 0.449 0.017 -7 -7
Father is Uneducated 0.144 -0.377 -0.054 22.2 22.2 Mother is Uneducated 0.237 -0.294 -0.07 28.6
16.6 Mother’s Primary Edu. 0.083 0.16 0.013 -5.5
Mother’s Secondary Edu . 0.039 0.415 0.016 -6.5
Father is Working 0.237 0.005 0.001 -0.5 -0.5 Mother is Working 0.064 -0.248 -0.016 6.5 6.5 Risky Birth Intervals 0.306 -0.077 -0.023 9.6 9.6 History of Pregnancy Loss 0.091 -0.022 -0.002 0.8 0.8 Prenatal one visit -0.033 -0.225 0.007 -3
0.9 Prenatal two visits -0.045 -0.039 0.002 -0.7
Prenatal three visits 0.252 -0.029 -0.007 3
Prenatal four plus visits -0.01 0.372 -0.004 1.6
Poorest 0.068 -0.793 -0.054 21.9
30.5 Poor 0.107 -0.341 -0.037 14.9
Middle 0.013 0.071 0.001 -0.4
Rich 0.031 0.467 0.014 -5.9
Solid cooking Fuel -0.009 -0.325 0.003 -1.2 -1.2 Un Hygienic toilet -0.074 -0.463 0.034 -14.1 -14.1 Improved drinking Water 0.078 0.054 0.004 -1.7 -1.7 Rural -0.024 -0.276 0.007 -2.7 -2.7 Sindh 0.074 -0.046 -0.003 1.4
15.8
KPK 0.112 0.036 0.004 -1.6
Balochistan 0.073 -0.236 -0.017 7
Gilgit-Baltistan 0.037 -0.351 -0.013 5.3
Islamabad -0.016 0.579 -0.009 3.7
Total Observed 84.4 84.4 Residual -0.038 15.6 15.6 Total 100 100
34

Determinants of Under-five Mortality Elasticity Concentrat
ion Index Contribution
Percentage
Contribution
Agrigated
percentage
contribution
Child is Male 0.024 0.003 0 0 -0.1 Birth Order of Child 2 -0.089 0.094 -0.008 4.6
9.9 Birth Order of Child 3 -0.047 0.054 -0.003 1.4
Birth Order of Child 4 -0.032 -0.036 0.001 -0.6
Birth Order of Child 5 plus 0.042 -0.196 -0.008 4.5
Age of Mother at Time of Birth 0.095 0.059 0.006 -3.1 -3.1
Head of Household is Female 0.011 0.037 0 -0.2 -0.2
Delivery by Caesarean 0.036 0.449 0.016 -8.8 -8.8 Father is Uneducated 0.018 -0.377 -0.007 3.8 3.8 Mother is Uneducated 0.309 -0.294 -0.091 49.5
32.4 Mother’s Primary Edu. 0.081 0.16 0.013 -7.1
Mother’s Secondary Edu . 0.044 0.415 0.018 -10
Father is Working 0.146 0.005 0.001 -0.4 -0.4 Mother is Working 0.065 -0.248 -0.016 8.8 8.8 Risky Birth Intervals 0.279 -0.077 -0.021 11.7 11.7 History of Pregnancy Loss -0.024 -0.022 0.001 -0.3 -0.3 Prenatal one visit -0.013 -0.225 0.003 -1.6
-8.3 Prenatal two visits -0.006 -0.039 0 -0.1
Prenatal three visits 0.29 -0.029 -0.008 4.6
Prenatal four plus visits 0.055 0.372 0.021 -11.2
Poorest 0.072 -0.793 -0.057 31.3
36.3 Poor 0.067 -0.341 -0.023 12.4
Middle 0.034 0.071 0.002 -1.3
Rich 0.024 0.467 0.011 -6.1
Solid cooking Fuel -0.022 -0.325 0.007 -3.9 -3.9 Un Hygienic toilet 0.045 -0.463 -0.021 11.3 11.3 Improved drinking Water 0.111 0.054 0.006 -3.3 -3.3 Rural 0.017 -0.276 -0.005 2.6 2.6 Sindh 0.009 -0.046 0 0.2
6.4
KPK -0.027 0.036 -0.001 0.5
Balochistan 0.013 -0.236 -0.003 1.6
Gilgit-Baltistan -0.003 -0.351 0.001 -0.6
Islamabad -0.015 0.579 -0.009 4.7
Total Observed 94.9 94.9 Residual -0.009 5.2 5.2 Total 100 100
35

36
-20
-10
0
10
20
30
40
50
60
70
Ch
ild is
Ma
le
Birth
Ord
er
of
Ch
ild
Ag
e o
f M
oth
er
at
Tim
e o
f B
irth
He
ad
of
Ho
use
ho
ld is
Fe
ma
le
De
live
ry b
y C
ae
sare
an
Fa
the
r is
Un
ed
uc
ate
d
Ma
tern
al E
du
ca
tio
n
Fa
the
r is
Wo
rkin
g
Mo
the
r is
W
ork
ing
Ris
ky B
irth
In
terv
als
His
tory
of
Pre
gn
an
cy L
oss
Pre
na
tal V
isits
Ec
on
om
ic S
tatu
s
So
lid c
oo
kin
g F
ue
l
Un
Hyg
ien
ic t
oile
t
Imp
rov
ed
drin
kin
g W
ate
r
rura
l
Re
gio
n (
Pro
vin
ce
s)
Pe
rce
nta
ge
co
ntr
ibu
tio
n
Determinants
Decomposition of Concentration Index of Neonatal, Post-
Neonatal and Under-five Mortality,(Pakistan 2012-13)
Neonatal Post-Neonatal Under-Five

CONCLUSION
Findings Indicate that in the socioeconomic Inequality in child morality the major positively contributing determinants are
Economic status
Education
Risky Birth Intervals
Birth order of child
Unhygienic toilets
Living in rural area
Negatively contributing determinants
Delivery by caesarean section
Prenatal visits
Improved drinking water
37

POLICY IMPLICATIONS
Economic Status Eradicate Poverty
Distribution of resources Equality and Need
Maternal Education
Adult Literacy
Improve antenatal care services
Access to Health care services
Invest in water and sanitation infrastructure and
programmes
38

References
Agha, S. (2000). The determinants of infant mortality in Pakistan. Social Science and medicine, 199-208. Retrieved from www.elsevier.com/locate/socsimed
Akram, M., & Khan, F. J. (2007). Health Care Services and Government Spending in Pakistan. PIDE Working Papers.
Alam, A. Y. (2011). Health equity, quality of care and community based approaches are key to maternal and child survival in Pakistan. JPMA Journal of Pakistan Medical Association.
Alam, A., Nishtar, S., Amjad, S., & Bile, K. (2010). Impact of wealth status on health outcomes in Pakistan. Eastern Mediterranean Health journal, 6.
Andersen, R. M. (1995). Revisiting the behavioral model and access to medical care: does it matter? health social behavior, 1-10. Retrieved from http://www.jstor.org/discover/10.2307/2137284?uid=2&uid=4&sid=21104138058943
Bassani, D. G., Jha, P., Dhingra, N., & Kumar, R. (2010). Child mortality from solid-fuel use in India:a nationally-representative case-control study. BMC public health. Retrieved from www.biomedcentral .com/1471-2458/10/491
Carr-Hill, R., & Chalmers-Dixon, P. (2005). The Public Health Observatory Handbook of Health Inequalities Measurement. England: South East Public Health Observatory.
Chalasani, S. (2012). Understanding wealth-based inequalities in child health in India: A decomposition approach. Elservier: social science and medicine, 2160-2169. Retrieved from www.elsevier.com/locate/socscimed
CSDH. (2007). A Conceptual Framework for Action on Social Determinants of Health. CSDH framework for action.
Goli, S., Doshi, R., & Perianayagam, A. (2013, March). Pathways of Economic Inequalities in Maternal and Child Health in Urban India: A Decomposition Analysis. PLOS ONE, 8(3). Retrieved from www.plosone.org
Heshmati, A. (2004). Inequalities and Their Measurement. Germany: IZA.
Hosseinpoor, A. R., Doorslaer, E. V., Speybroeck, N., Naghavi, M., Mohammad, K., Majdzadeh, R., . . . Vega, J. (2006). Decomposing socioeconomic inequality in infant mortality in Iran. International Journal of Epidemiology, 1211–1219.
Huda, S. N., & Burke, F. (2011). SOCIAL AND ECONOMIC DISPARITIES, SINDH, BALUCHISTAN AND PAKISTAN - A COMPARATIVE STUDY. The Research Journal of Sciences and Technology, 49-66.
Kakwani, N., Wagstaft, A., & Doorslaer, e. v. (1997). Socioeconomic Inequalities in Health: Maesurment, Computation, and Statical Inference. Journal of Econometrics, 87-103.
Mackenbach, P. D. (2006). Health Inequalities: Europe in Profile. University Medical Center Rotterdam, Department of Public Health. Netherlands: erasmus mc.
MAIO, F. D., MAZZEO, J., & RITCHIE, D. (2013). Social Determinants of Health: A View on Theory and Measurement. Rohad Island Medical Jouranl .
Manzoor, I., Hashmi, N. R., & Mukhtar, F. (2009). DETERMINANTS AND PATTERN OF HEALTH CARE SERVICES UTILISATION IN POST GRADUATE STUDENTS. Journal of Ayub Medical Collage Abbottabad, 100-105.
39

Refrences Contn…. Minujin, A., & Delamonica, E. (2004, april 16). Socio-economic inequalities in mortality and health in the developing world. DEMOGRAPHIC RESEARCH, 331-354.
Mosley, W., & Chen, L. C. (1984). An Analystical framework for the study of Child Survival in Developing Countries . bulletin of world health organization 2003, .
Mosquera, P. A., Hernández, J., Vega, R., Martínez, J., Labonte, R., Sanders, D., & Sebastián, M. S. (2012). The impact of primary healthcare in reducing inequalities in
child health outcomes, Bogotá – Colombia: an ecological analysis. International journal of equity in health. Retrieved from http//www.equityhealthj.com
/content/11/1/66
Nisar, Y. B., & Dibley, M. J. (2014). Determinants of neonatal mortality in Pakistan: secondary analysis of Pakistan Demographic and Health Survey 2006–07. BMC Public
Health. Retrieved from www.biomedcentral.com/1471-2458/14/663
O’Donnell, O., Doorslaer, E. v., Wagstaff, A., & Lindelow, M. (2008). Analyzing Health Equity Using Household Survey Data, A Guide to Techniques and Their
Implementations. Washington, D.C: The World Bank.
Omran, A. R. (2005). The Epidemiologic Transition: A Theory of the Epidemiology of Population Change. The Milbank Quarterly, 83(4), 731-751.
Pathak, P. K., Singh, A., & Subramanian, S. V. (2010). Economic Inequalities in Maternal Health Care: Prenatal Care and Skilled Birth Attendance in India, 1992–2006.
PLoS One www.plosone.org, 5(10), e13593.
PDHS. (2013). Pakistan Demographic and Health Survey 2012-13, Preliminary Report. Islamabad: National Institute of Population Studies.
Rosenstock. ( 1974). The Health Belief Model and preventive health behavior. Health Educ Monogr, 2, 354-386. Retrieved from
http://heb.sagepub.com/content/2/4/354.full.pdf
Shehzad, S. (2004). How Can Pakistan Reduce Infant and Child Mortality Rates? A Decomposition Analysis. Sustainable Development Policy Institute. Retrieved from
www.sdpi.org
Vásquez, F., Paraje, G., & Estay, M. (2013). Income-related inequality in health and health care utilization in Chile, 2000–2009. Rev Panam Salud Publica, 98-106.
Wagstaff, A. (2000). Socioeconomic inequalities in child mortality: comparison across nine developing countries. Bulletin of World Health Organization, 19-29.
Wagstaff, A., Doorslaer, E. v., & Watanabe, N. (2003). On Decomposing the Causes of Health Sector Inequalities with an Application to Malnutrition Inequalities in
Vietnam. journal of economics, 219-227.
WHO. (2013). Health Inequality with a special focus on low- and middle-income countries. Geneva: World Health Organization.
Wildman ; Shen. (2014). Impact of Income Inequality on Health (Vol. 2). Elsevier. Retrieved March 2014
Wilkinson, R. G. (1997). Health inequalities: relative or absolute material standards? BMJ, 314.
Williams, A., & Cookson, R. (2005, january). EQUITY IN HEALTH. England: Centre for Health Economics university of york.
Yiengprugsawan, V., Lim, L. L., Carmichael, G. A., Dear, K. B., & Sleigh, A. C. (2010). Decomposing socioeconomic inequality for binary health outcomes: an improved
estimationthat does not vary by choice of reference group. BMC research note. Retrieved from http://www.biomedcentral.com/1756-0500/3/57
Zere, E., Moeti, M., Kirigia, J., & Mwase, T. (2007, May 15). Equity in health and healthcare in Malawi: analysis of trends. BMC Public Health.
Zere, E., Oluwole, D., Kirigia, J. M., Mwikisa, C. N., & Mbeeli, T. (2011). Inequities in skilled attendance at birth in Namibia: A decomposition analysis. BMC pregnancy
and child health. Retrieved from www.biomedcentral.com/1471-2393/11/34
Zhou, Z., Gao, J., Fox, A., Rao, K., Xu, K., Xu, l., & Zhang, Y. (2011). Measuring the equity of inpatient utilization in Chinese rural area. BMC health service research.
Retrieved from http://www.biomedcentral.com/1472- 963/11/201
40

41