-
7/31/2019 Declining Clinical Autopsy
1/7
924 Arch Pathol Lab MedVol 125, July 2001 Autopsy Rates in
Halifax, Nova ScotiaWood & Guha
Historical Perspective
Declining Clinical Autopsy Rates Versus IncreasingMedicolegal
Autopsy Rates in Halifax, Nova Scotia
Why the Difference? A Historical Perspective
Marnie J. Wood, BSc; Ashim K. Guha, MD, PhD
The downward trend in the rate of clinical autopsies hasbeen
extensively documented in the literature. This declineis of concern
when the benefits of the clinical autopsy areconsidered. In
contrast, the rate of medicolegal autopsies
has not been studied in such detail. What little referencethere
is to medicolegal autopsy rates suggests an absenceof the same
downward trend. A retrospective review ofautopsy data over a
13-year period from the Queen Eliz-abeth II Health Sciences Centre
in Halifax, Nova Scotia,and from the Office of the Chief Medical
Examiner of NovaScotia was conducted. This review showed a
difference be-tween the rates of clinical and medicolegal autopsies
forthe metro Halifax area. The clinical autopsy rate was
con-sistently less than 30% and declined to 15% in 1999, whilethe
medicolegal autopsy rate was consistently greater than40% and rose
to 62% in 1999. The literature proposesmany reasons for the decline
in the clinical autopsy rate,but none for this difference between
rates. The explanation
proposed here is the changing and currently uncertain pur-pose
of the clinical autopsy versus the clear, and consistentover time,
purpose of the medicolegal autopsy.
(Arch Pathol Lab Med. 2001;125:924930)
The word autopsy is from the Greek, meaning to see foroneself.
Along with the terms necropsy (literally, tolook at the dead) and
postmortem examination (which mayinclude external and/or internal
examination), autopsyhas come to refer to the systematic
examination of a deadperson for medical, legal, and/or scientific
purposes.1 Theautopsy is the ultimate medical consultation. 2
Histori-cally, the autopsy played a very important role in the
de-
velopment of medicine. Early clinical autopsies were doneby
researchers and clinicians who had followed their pa-tients
throughout life and the course of their diseases. Au-topsies were
more limited several centuries ago, when thepostmortem examination
was carried out only until thesuspected cause of death had been
demonstrated, and
Accepted for publication February 13, 2001.From the Faculty of
Medicine, Dalhousie University, Halifax, Nova
Scotia (Ms Wood and Dr Guha); and the Department of
Pathology,Queen Elizabeth II Health Sciences Centre, Halifax, Nova
Scotia (DrGuha).
Reprints: Ashim K. Guha, MD, PhD, Division of Anatomical
Pathol-ogy, Mackenzie Bldg, Room 720, Queen Elizabeth II Health
SciencesCentre, Victoria General Site, Halifax, Nova Scotia, Canada
B3H 1V8(e-mail: [email protected]).
may only have included examination of 1 organ or a smallarea of
the body.3 In those cases, the recorded cause ofdeath may have been
unrelated to the actual cause or mayhave been merely a complication
of the unrecognized fatal
disease. Teachers of anatomy also used the autopsy as ateaching
tool. Gradually, pathology became a separatespecialty, defined by
Virchow as the science that studiesthe causes, mechanisms, and
consequences of diseases. 4
The task of autopsy performance has fallen to patholo-gists, and
the autopsy has become a more complete andconsistent procedure. The
procedure is done in an autopsysuite equipped with all the
necessary tools, which may belocated at a variety of sites, such as
the hospital or medicalexaminers building, but which is usually
away from thegeneral hustle and bustle. Modern techniques, such as
mi-croscopy, immunofluorescence, and immunoperoxidasestaining have
added new dimensions to this very old pro-cedure.
Two basic types of autopsy exist. The clinical or aca-demic
autopsy (also referred to as a hospital autopsy5) isdone at the
request of the family or the physician (withpermission from the
family) of the deceased.6 In this case,the cause of death is
usually known. The purposes of thistype of autopsy include
determining the cause of death (ifunknown), providing correlations
between clinical diag-noses and symptoms, determining the
effectiveness oftreatment, studying the course and extent of
disease pro-cesses, and educating medical personnel.7 The
secondtype, a forensic or medicolegal autopsy, is performedwhen the
cause of death is not certain, usually in the caseof unexpected,
unexplained, or unnatural deaths.8 These
medicolegal cases may be further divided into criminalcases,
which are suspicious in nature, and noncriminalcases, in which no
foul play is suspected.6 A medicolegalautopsy may be ordered by an
official death investigatorto assist in determining the cause and
manner of death.7
This information must be determined accurately for thedeath
certificate. In all medicolegal cases, the legal au-thority (such
as the provincial medical examiner in NovaScotia) has the sole
power to order an autopsy, and nopostmortem procedures may be
carried out without his orher permission.9 The medical examiner, if
also a patholo-gist, may perform an autopsy or may refer the
autopsy tobe done by a hospital pathologist.8,10
Even the general public has a vague idea of what the
performance of an autopsy entails, although they may not
-
7/31/2019 Declining Clinical Autopsy
2/7
Arch Pathol Lab MedVol 125, July 2001 Autopsy Rates in Halifax,
Nova ScotiaWood & Guha 925
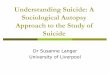
Comparison of clinical and medicolegal au-topsy rates for
Halifax, Nova Scotia, from1987 to 1999. Each point represents the
au-topsy rate for a particular calendar year. Theclinical autopsy
rate was calculated as thenumber of clinical autopsies performed
divid-ed by the number of in-hospital deaths (ex-cluding medical
examiner cases) for the sameyear multiplied by 100. The medicolegal
au-topsy rate was calculated as the number of
medicolegal autopsies performed divided bythe number of deaths
reported to the medicalexaminer for the same year multiplied
by100.
fully understand why autopsies are done. Indeed, this lackof
understanding may also exist within the medical com-
munity itself. In the last half of the century, the rate
ofclinical autopsy performance has dropped.2,1113 The liter-ature
suggests medicolegal autopsies are not experiencingthe same trend.
Rates of autopsy are now so low thatpostmortem examination other
than for medicolegal pur-poses is in jeopardy. 14 This article
demonstrates a dif-ference in rate between clinical and medicolegal
autopsiesusing local data and then considers reasons this
differencemight exist.
CURRENT STATUS OF THE AUTOPSY
Clinical autopsy rates have been in decline for the lasthalf of
the century. The figures cited are American, but
similar traits have been noted in Canada.13
As early as the1950s, concerned persons were expressing alarm
over thefalling rates.14 In the early 1940s, the autopsy rate for
in-hospital deaths was approximately 50%.2,13 In the 1950s,the
required rate for accreditation was 25% in teachinghospitals and
20% in nonteaching hospitals.2 In the early1970s, the required rate
was dropped and the numbersplummeted.2,13 By 1973, rates had fallen
to 22%, and by1984, to 13.2%.2 A national study in 1994 by the
Collegeof American Pathologists found 75% of hospitals had
anautopsy rate less than 13.5%, and 50% had rates less than8.5%.15
In 1995, some North American hospitals had ratesas low as 7%.13 A
1996 survey of 2 major teaching hospitalsfound rates of 5% and
15%.2 In contrast, there is less lit-
erature on the rate of medicolegal autopsies. It has, how-ever,
been suggested that medicolegal autopsy rates arenot falling as
steeply as clinical autopsy rates.14
A retrospective review of data from the Queen Eliza-beth II
Health Sciences Centre in Halifax, Nova Scotia, andthe Office of
the Nova Scotia Medical Examiner confirmsa difference between
clinical and medicolegal autopsyrates in the metro Halifax area.
The Figure illustrates thesefindings. The rate of clinical
autopsies is consistently lessthan 30%, falling to less than 20% in
the final 4 yearsexamined. The medicolegal rate is consistently
greaterthan 40%, rising to 62% in the last 2 years examined.
Al-though the clinical autopsy rates are higher than rates
re-corded in the literature, the clinical autopsy rate is far
lessthan the medicolegal autopsy rate in each of the 13 years
examined. The data also demonstrate that the clinical au-topsy
rate has decreased over time, while the medicolegal
autopsy rate has increased.The literature suggests a variety of
reasons for the de-
crease in the number of clinical autopsies. The increasingcost
of the autopsy, which fewer people seem willing topay, is almost
certainly a factor. A single autopsy, depend-ing on the extent and
number of extra procedures used,may cost between US $1200 and
$3000.14 In Canada, thecost of clinical autopsies is covered by the
hospital, andmany administrators want to spend only a small
portionof their budget on autopsies.13 The budget for
medicolegalautopsies is covered by the Department of Justice. A
min-imum autopsy rate is no longer required for hospital
ac-creditation, so there is no push to maintain a certain stan-
dard rate.
14
Also, physicians do not realize the importanceof the autopsy
because medical education no longer em-phasizes this procedure.14
Physicians graduating in thepast 10 years from two thirds of
medical schools have notbeen exposed to an autopsy. Why should
doctors careabout having autopsies performed when they dont
evenunderstand what the procedure involves? 13 Physicianswho do not
realize the importance of clinical autopsiesare probably less
likely to request permission to performautopsies. Many physicians
take comfort in the perceivedcertainty that new clinical diagnostic
tools can replace theautopsy, making it out-of-date and
unnecessary. Thisopinion has led to a reduction in the clinical
autopsy rate.The clinical autopsy might, however, still be useful
in elu-
cidating the limits and weak areas of new diagnostic tools.The
fear physicians have that an autopsy will reveal a mis-take in
treatment and lead to litigation prevents manyfrom requesting an
autopsy. No one wants to know abouterrors in this time of
litigation. 16 There is evidence tosuggest these fears are
ungrounded. A study by Haque etal17 at the University of Texas
Medical Branch at Galvestonfound only 2 of 6168 clinical autopsies
provided resultsleading to malpractice suits. Many more autopsies
provideevidence that exonerates hospital staff of
wrong-do-ing.10,14,17 The clinical autopsy is also losing
prestigeamong pathologists and is competing for time with
otherlaboratory duties. In addition, family objections based
onmisconceptions may result in permission for a clinical au-
topsy not being granted. It is also possible that physicians
-
7/31/2019 Declining Clinical Autopsy
3/7
926 Arch Pathol Lab MedVol 125, July 2001 Autopsy Rates in
Halifax, Nova ScotiaWood & Guha
are simply not asking for the familys permission to per-form a
clinical autopsy because they are not trained todeal with this
uncomfortable situation.14,18
These reasons may explain the decline in number ofclinical
autopsies; however, they do not explain why therate of medicolegal
autopsies is not declining as well. Thecost of both procedures is
equally high, and neither typeof autopsy is emphasized in medical
education. Granted,families of the deceased are not able to refuse
permission
for a medicolegal autopsy to be performed, but patholo-gists may
be equally reluctant to perform this time-con-suming procedure if
newer techniques exist to obtain thesame information. An
examination of the history of theclinical and medicolegal autopsy
may provide some in-sight into the recent difference in performance
rates.
THE CLINICAL AUTOPSY
The knowledge of normal versus abnormal anatomydates as far
back, and perhaps further, as 1500 BC, whenanimal entrails were
examined for clues to the future.1
During the mummification process, the Egyptians alsogathered
such information about humans. As early as 400BC, Hippocrates
believed that disease resulted from nat-ural causes,3 in contrast
to the belief in supernatural, spir-itual, and humor disturbance
causes held by the major-ity of the population at that time. These
mistaken beliefswould initially prevent the clinical autopsy from
findingan accepted place in medicine. It took a long time for
theconnection to be made between disease and associatedchanges in
the organs of the body. The autopsy did havean early place in
medicolegal cases and in the furtherstudy of anatomy. Around 300
BC, Herophilus was usingdissections to teach anatomy, and he wrote
a treatise onhuman anatomy but paid no attention to abnormalities
ofstructure.1 In this manner, empirical knowledge of anato-my was
gradually gathered. In 200 BC, Erasistratus was
probably the first to carry out dissections to look forchanges
due to disease. However, when Galen popular-ized disturbances in
the 4 body humors as the cause ofdisease,3 he sent medicine on a
long-lasting wild goosechase.
In the 13th century, dissections were being done duringplagues
in order to better understand the illness. 4
These procedures were paid for by the state and illustratethat
people were beginning to see the autopsy as morethan a way to learn
anatomy. The first recorded autopsyperformed in the New World was
in 1533. Female con-joined twins were dissected to determine if
they had 1soul or 2.3 At the end of the 15th century, the Italian
phy-sician Antonio Benivieni was the champion of the autopsy.
In 1507 he published the first book of anatomical pathol-ogy,
titled Remarkable Hidden Causes of Disease.3,4 This wasthe very
beginning of clinicopathologic correlation and setthe stage for
wider acknowledgement of the link betweendisease and body
structure.
During the 17th century, clinical autopsies and the re-cording
of their results became more common. While theprevailing view was
still that clinical autopsies were awaste of time, in 1679 the
Sepulchretum was published. TheSepulchretum contained a collection
of autopsy reportsfrom noted physicians of the time.3 The reports
were in-consistent and contained few clinicopathologic links,
butthis book set the stage for the clinical autopsy to assumea
place of importance in medicine. By the 18th century,reference to
clinical autopsy reports could be found in
many journals.3 Physician Hermann Boerhaave was pub-lishing far
more detailed reports than had been seen be-fore. Boerhaave was
also the first to begin placing impor-tance on the complete
clinical history of the patient, stat-ing, Everything pertaining to
the case must be listed: northat least thing neglected which a
critical reader mightrightly seek to understand the malady.3 This
attitude canbe seen throughout the following century, as the
clinicalautopsy became the end of the complete story of an ill-
ness. The clinical autopsy was gaining a major place inmedicine.
Italian physician Morganis work at the Univer-sity of Padua
solidified the correlation between clinicalsymptoms and pathologic
findings, and pathology becamethe basis for medicine of the
time.3,19
Xavier Bichat, a French physician in the 19th century,felt very
strongly about the place of the clinical autopsyin medicine: You
can take notes for 25 years, from morn-ing to evening, by the
patients bedside on diseases of thelung, heart and stomach, and the
result will be a long listof confusing symptoms, leading to
incoherent conclusions.Open a few bodies, and you will see darkness
immediate-ly recede. 4 Bichat was also the first to consider
lookingfarther than the organs and examine their component
tis-sues. This was before the time of the microscope, but hestill
made much progress in this area. At this point, au-topsies were
still done by clinicians. Clinicopathologic cor-relations allowed
diseases to be defined much more clearlyand their progression over
time noted. The developmentof the microscope allowed others to pick
up where Bichathad left off, and pathology was revolutionized. The
grossexamination of the body was joined by the first of
manyhigh-tech companions. In fact, the limits of gross exami-nation
alone were being recognized.
Rokitansky (mid-19th century) worked at the Patholog-ical
Institute at Vienna and began the separation betweenpathologists
and clinicians. Rokitansky performed or ob-
served autopsies on almost every patient who died in thehospital
(more than 30 000).1 He attempted to work back-ward, using autopsy
results to determine the clinical find-ings.19 Although many of his
theories proved incorrect,Rokitansky provided a huge databank of
autopsy infor-mation. His advances were spread throughout the
world.Around the same time, a German physician, Virchow, be-lieved
that pathology was a science in its own right, sep-arate from the
clinical side of medicine. Virchow was alsoa leader in setting
forth a regular and definite techniquefor the autopsy, and he
emphasized a long, complete au-topsy.3,4,19
At the beginning of the 20th century, most clinicianswere still
spending a great deal of time in the autopsy
room, confirming or clarifying diagnoses. ProminentAmerican
physicians spent time in Europe learning ana-tomical pathology from
the masters.19 Sir William Oslerwas a Montreal physician who worked
at Johns Hopkinsand turned the place upside down. 19 Osler
championedthe autopsy, following his patients to the autopsy
roomand even leaving detailed instructions for his own autop-sy.19
He is quoted as writing, To investigate the causes ofdeath, to
examine carefully the condition of organs, aftersuch changes have
gone on in them as to render existenceimpossible, and to apply such
knowledge to the preven-tion and treatment of disease, is one of
the highest objectsof the physician. 19 This expresses the use of
the clinicalautopsy at the time, which was to elucidate disease
pro-cesses and the effects of treatment. Clinical autopsies
soon
-
7/31/2019 Declining Clinical Autopsy
4/7
Arch Pathol Lab MedVol 125, July 2001 Autopsy Rates in Halifax,
Nova ScotiaWood & Guha 927
came to have another use. In 1910, an American report byFlexner
was published. The report stated that good hos-pitals had high
autopsy rates, otherwise physicians couldbury their mistakes.3 This
report was followed by the Ca-bot Report in 1912, which revealed
many diagnostic errorswere occurring in American hospitals and
could be foundonly through autopsies. Through these reports, the
clinicalautopsy became associated with quality control.3,19
The purpose of the clinical autopsy has shifted since its
beginnings as a tool for teaching anatomy and a way tosearch for
the soul. As information about human anatomywas gathered, the
autopsy gradually became a way to ex-plore disease processes.
Pathology, and the autopsy as itstool, then became a science in its
own right for gatheringmore information about disease processes. In
the first partof this century, the clinical autopsy became a method
ofmonitoring the quality of care and the diagnostic abilitiesof
physicians and their equipment. Throughout the lasthalf of the 20th
century, the importance of the autopsy tothe medical community and
the public had to be defend-ed. This is a long fall from the
esteemed position the au-topsy held a short 100 years ago.
Administrators, physi-cians, and the public may be falling into the
same trap.There is a tendency to place much faith in new,
high-techdiagnostic techniques, such as ultrasound, magnetic
res-onance imaging, computed tomography, and endoscopy.The belief
is that these procedures illustrate all there is tobe known about a
particular disease and make autopsyresults redundant. However, this
faith in high-tech diag-nostic tools over the clinical autopsy may
be somewhatmisplaced. As Lundberg20 pointed out, there is a gap
be-tween how well high-tech diagnostic medicine performsin theory
and how well it performs when human decisionmaking (how and when to
use the technology) is addedto the equation. Several studies have
shown that the au-topsy should still be considered the gold
standard in di-
agnosis and that autopsies are absolutely necessary to as-sure
the quality of care given to patients, both those treat-ed
successfully and, especially, those who die. In a studyby Nichols
et al21 at a major tertiary-care center, 44.9% ofautopsies found at
least 1 undiagnosed cause of death. Forexample, a patient with
cirrhosis had what was interpret-ed radiologically to be a scar. On
necropsy, a rare mixedhepatocellular and cholangiocarcinoma was
discovered. Intwo thirds of these cases the undiagnosed cause of
deathwas determined to have been treatable. These misdiag-noses
were often related to patient inability to relatesymptoms or the
masking of symptoms by other treat-ments. In another study, Burton
et al22 found a 44% dis-cordance between the clinical and autopsy
diagnosis of
neoplasms at the Medical Center of Louisiana at New Or-leans.
Furthermore, Roosen et al23 looked at autopsies per-formed on
patients dying in the medical intensive careunit. In spite of more
modern diagnostic techniques, 16%of these autopsies found missed
major diagnoses, thetreatment of which might have prolonged
survival. Final-ly, Sonderegger et al24 showed a drop in the
frequency ofmajor missed diagnoses from 30% to 14% over 20
years,mainly due to a decrease in the misdiagnosis of
cardio-vascular disease. The autopsy rate at this facility in
Zurich,Switzerland, was approximately 90% consistently over
thestudy period, a record that enhances the credibility of
thefindings. While the purpose of the clinical autopsy maynot be as
clear as in the past, it can be seen from thesestudies that the
autopsy has a large role to play in quality
assurance and in elucidating the limitations of
diagnostictechniques. It can therefore be concluded that the
autopsyis still a cost-effective and useful procedure.
THE MEDICOLEGAL AUTOPSY
Forensic pathology is generally considered a recentlydeveloped
subspecialty of pathology dealing with the ex-amination of living
or dead persons to provide expertopinion regarding the cause,
mechanism, and manner of
disease, injury, or death. This discipline is also concernedwith
identifying persons, determining the significance ofbiological and
physical evidence, correlating and recon-structing wounds,
performing comprehensive medicolegaldeath investigations,7 and
applying medical knowledge tolegal issues. However, the history of
forensic medicine andthe postmortem examination actually dates back
to antiq-uity, when bodies were most often examined to determineif
death occurred as a result of suicide or homicide. Theancient
Greeks felt suicide to be a rebellion against thegods and the
Romans saw it as a crime against the state.As such, there was great
stigma attached to the familiesof those who committed suicide. In
1184, the Roman Cath-olic Church added suicide to canon law,
further adding tothe importance of distinguishing it from other
manners ofdeath.16
During the 6th century, Justinian law called medicolegalexperts
to testify in cases of rape, criminal abortion, andmurder.
Attitudes at the time were still against openingthe bodies of the
deceased, but external postmortem ex-aminations were done and the
evidence obtained wasused in court.16 Subsequently, during the
medieval period,dissections of corpses were done in Italy at the
Universityof Bologna under the control of the faculty of law to
solvelegal matters. There is also a report dating from 1302 of
acourt-ordered autopsy done at the University of Bolognato
investigate the suspicious death of a nobleman.3 Fur-
thermore, there was a Chinese publication in the 13th cen-tury
that was much ahead of its time. Titled His Yuan Luor Instructions
to the Coroner, it dealt with findings in casesof infanticide,
drowning, hanging, poisoning, and assault.In Germany during the
16th century, the code of Bam-burg, and later the broader penal
codes, brought about arequirement for medical testimony in putative
forensiccases. These codes also allowed the opening of bodies
toexamine the depth of and damage caused by wounds.16
Today, a murder case would be thrown out of court with-out
complete autopsy results.
Throughout history, there have always been religiousbarriers to
the performance of autopsies. Clinical autopsiesin some cultures
were forbidden. For example, Jewish laws
stated that an autopsy was a disgrace to the body, andprior to
the 18th century, clinical autopsies were not per-mitted. However,
there is a passage in the Talmud allow-ing an autopsy if the
evidence provided might save thelife of an accused murderer.16 This
illustrates that even re-ligious authorities at times have
recognized the impor-tance of the forensic autopsy and its
difference from aclinical autopsy.
The field of legal medicine continued to grow, and inthe 18th
century the first series of lectures on the topicwas given at the
University of Edinburgh by Sir AndrewDuncan. As the field expanded,
Europeans developed 2different ways of providing medicolegal
professionals forsociety to use. On the continent and in Scotland,
the uni-versities and associated hospitals took over the
provision
-
7/31/2019 Declining Clinical Autopsy
5/7
928 Arch Pathol Lab MedVol 125, July 2001 Autopsy Rates in
Halifax, Nova ScotiaWood & Guha
of specially trained physicians. In England, the coronersystem
was established under the constabulary. A coronerwas an official of
the court with no medical training. Thecoroners responsibility was
to investigate deaths fallingunder his jurisdiction. During the
investigation, the coro-ner often consulted a police surgeon,
usually a generalpractitioner with some special training. A
pathologist wasconsulted only if an autopsy was required. The term
cor-oner was derived from crowner. A crowner was a represen-
tative of the King, who collected taxes, convened court,and
distributed the property of those found guilty of mur-der. Because
of the latter responsibility, the crowner be-came associated with
death and its investigation.16
The coroner system began in America in the 17th cen-tury, but
was gradually abolished because of the potentialfor political
interference. This system was replaced by thedistrict attorneys
office, which took over the legal aspectsof death investigation,
and the medical examiners office,which took over the medical
aspects of the investigation.The medical examiners office is
staffed by trained forensicpathologists.16 The College of American
Pathologists firstformed the Committee on Forensic Pathology in
1952.2 Itspriority was to increase forensic training for
pathologistsand raise the standards in what was becoming a
subspe-cialty. Through the 1960s and 1970s, funding becameavailable
for fellowships in this subspecialty.
In Nova Scotia, Canada, the medical examiners office isunder the
jurisdiction of the Department of Justice. It isthe budget of this
department that pays for medicolegalautopsies. Deaths falling under
the jurisdiction of themedical examiner include death from any
unnatural en-tity, when a medical cause of death cannot be
establishedwith reasonable accuracy, death occurring while a
personis in custody (jail or psychiatric), and death by unduemeans
or when there may be medical culpability.7 Alldeaths meeting one of
these descriptions must be reported
to the medical examiner, who becomes responsible for
theinvestigation and for the ordering of a medicolegal autop-sy if
deemed necessary.6,7
The medicolegal autopsy differs from the clinical autop-sy in
several ways, one of which is that it has not expe-rienced the same
decline in rate or prestige. If anything,the forensic autopsy has
had a recent gain in popularity,especially among the general
public. Autopsy results arefeatured in news reports of suspicious
deaths. Televisionnetworks, such as A&E and TLC, are full of
specials onmedical examiners offices and forensic medicine.
Evenpopular television shows, like the X-Files, often featurescenes
of an autopsy (usually done by the female charac-ter, alone, late
at night in a dark and spooky room). An-
other difference is that the medicolegal autopsy seeks toanswer
a specific legal question: What is the cause andmanner (natural,
homicide, suicide, accidental) of death inthis case?16 This
question has remained constant for themedicolegal autopsy
throughout time, in contrast to theclinical autopsy, which seeks to
answer many questions.While the point of a medicolegal autopsy
remains focused,the adequate answering of this question often
requires anextensive investigation. The medical examiner has
thepower to determine the extent of the autopsy to be per-formed,
but medicolegal autopsies are rarely limited.7 Tocontribute as much
as possible to the prosecution of theguilty and the defense of the
innocent, there is an extraemphasis on completeness during a
forensic case. Theonly thing worse than no autopsy is a partial
autopsy in
forensic cases.25 A partial autopsy may lead to a later
ex-humation of the body, as what seemed to be unimportantat the
time turns out to be vital to the case. While theactual dissection
is often the same as the clinical autopsy,the medicolegal
postmortem examination often begins atan earlier stage, the place
of death. Here the position, lo-cation, clothing, personal effects,
signs of death, and in-juries are correlated with the circumstances
and docu-mented.6,7 Careful observations of the surroundings
must
be made and meticulous notes kept.16 Also, a forensic
in-vestigation may involve trying to determine informationreadily
available in a clinical case, such as the identity ofthe deceased
and time of death. The external examinationmay also take on
additional importance in a forensic case.There is often much
information to be gathered from ex-ternal wounds. The speed and
angle of a striking auto-mobile may be determined from the
characteristics ofabrasions. Bullet exit wounds can be
distinguished fromthe entrance wounds and help distinguish a
homicidefrom a suicide.16 All of this information is key to a
medi-colegal case. The objectives of the medicolegal autopsy,
aslisted by Knight,6 are to make a positive identification ofthe
body and to assess the size, physique, and nourish-
ment; to determine the cause of death; to determine themode of
dying and the time of death when necessary andpossible; to
demonstrate all external and internal abnor-malities,
malformations, and diseases; to detect, describe,and measure any
external and internal injuries; to obtainsamples for analysis,
including microbiological and his-tologic examination, as well as
any other necessary inves-tigations; to retain relevant organs and
tissues as evidence;to obtain photographs and video films for
evidential andteaching use; to provide a full written report of the
autop-sy findings; to offer an expert interpretation of those
find-ings; and to restore the body to the best possible
cosmeticcondition before release to relatives.
The autopsy is a vital tool in medicolegal investigationsfor
which there is no substitute. The nature of a medico-legal case is
that there is not an adequate clinical picturewith which to
determine a cause and manner of death.The information gathered
through an autopsy is especiallyimportant in cases of suspected
foul play. The medicolegalautopsy does not seem to be facing the
same problem asthe clinical autopsy, that is, a decline in the rate
of perfor-mance. One reason may be that medicolegal autopsies
arenot funded by the hospital and therefore do not competefor
limited funds with treatments and diagnostic proce-dures, which are
often perceived to provide greater yield.The political reality is
that stable funding of medicolegalcases generally exists as a
result of jurisdiction lying withthe Department of Justice and not
with the Department ofHealth in most systems. This reality may play
a role incausing the observed rate differences between
medicolegaland clinical autopsies. Or, perhaps it is because the
pur-pose of the medicolegal autopsy has remained clear andunchanged
through the centuries. Also, there is no pro-cedure that could
provide the same amount of informationwith which to replace the
medicolegal autopsy. OscarSchultz in 1932 in a study for the
National Academy ofSciences of the United States said, The
determination ofthe cause of death in an exact and scientific
manner re-quires a necropsy. 16
CONCLUSIONS
The decline of clinical autopsy rates means the benefitsthese
autopsies could provide are being missed. The pur-
-
7/31/2019 Declining Clinical Autopsy
6/7
Arch Pathol Lab MedVol 125, July 2001 Autopsy Rates in Halifax,
Nova ScotiaWood & Guha 929
poses of the clinical autopsy may have changed, but itappears
there is still much it can contribute. The clinicalautopsy is still
valuable as the gold standard by whichdiagnostic tools, treatment
methods, and clinical decision-making procedures can be measured.26
How do you as-sess the quality of care given to your sickest
patients, theones who die? 27 We have shown in this article that
thelimitations of diagnostic tools can be defined through clin-ical
autopsies. Furthermore, there is a need to evaluate
clinical decision-making procedures to prevent the sameerrors
being made repeatedly.3 Autopsy results can alsoshow otherwise
unknown adverse effects of treatments,such as the dose-related
cardiotoxicity of doxorubicin. Thetoxic effects of many
chemotherapy drugs can be moni-tored through autopsy results, and
future doses and treat-ment protocols then can be altered
appropriately. Clinicalautopsy performance is very important in the
study, treat-ment, and prevention of disease. Even at the current
lowrates, autopsies have helped elucidate conditions such asshock,
cardiovascular disease, aging, and cancer.14 In 1case that was
reported, a male infant with hypoplastic leftheart syndrome died
after corrective surgery. Those in-volved in his care attended the
autopsy, which providedan opportunity to learn more about the
syndrome, to eval-uate the surgical technique, and to perform
quality as-sessment.28 New environmental diseases, such as
someforms of asthma, are constantly being discovered, andsome may
be missed due to the low clinical autopsy rate.The hazards of
occupational exposures to agents like as-bestos have been proven
through clinical autopsies. Thishas resulted in major changes to
working conditions. Aclinical autopsy may reveal the presence of a
contagiousdisease and allow the quick treatment of unknowingly
ex-posed individuals.27 An epidemic may be averted throughearly
warning. Another case illustrating the great impor-tance of
incidental autopsy findings is one in which a
breast lump found on autopsy was determined to be in-vasive
ductal carcinoma. Informing female family mem-bers of this finding
and advising them of their increasedrisk could potentially save a
life.29 Clinical autopsies mayalso be used to monitor public health
and ensure the ac-curacy of vital statistics.14,27 Vital statistics
are used to de-termine the public health policies and to assess the
effec-tiveness of public health services. These statistics are
com-piled from the information on death certificates. Kircheris
cited30 as having found that there is approximately a10% error rate
in death certificate diagnoses when com-pared to autopsy results.
The death statistics, which areused to develop public health
strategies, are based on theless-representative facts on the death
certificates. The per-
formance of autopsies at a high rate may correct the
mis-information and have a great impact on public health pol-icy.
For example, Kircher also found the death certificatediagnosis of
heart disease is an inaccurate reflection ofthe actual incidence,
which is lower.30 This is significantwhen the amount of money spent
on preventive strategiesfor heart disease is considered. Clinical
autopsies are alsovery important in the monitoring of levels of
clinically si-lent diseases, such as coronary artery disease.14
Withoutthe performance of autopsies, only guesses can be madeas to
their incidence. There are also extensive benefits forthe families
of those on whom clinical autopsies are per-formed. Relatives often
do not understand how everythinghappened. An autopsy can provide
information about howa loved one died and ease the familys mind
regarding the
extent of suffering. A family may also be made aware ofthe
benefits autopsy research can provide for future treat-ments. In
this way, the family may be able to see somegood come out of the
death. However, for the family toreap these benefits, autopsy
results must be made avail-able in an understandable format.
It may be that a lack of perceived purpose for the clin-ical
autopsy, whereas that of the medicolegal autopsy re-mains constant
and clear, has contributed to the isolated
decline in the clinical autopsy rate. The guidelines of
theCollege of American Pathologists25 state the current pur-poses
of the autopsy as follows: to establish a cause ofdeath, determine
the manner of death, compare premor-tem and postmortem diagnoses,
produce vital statistics,and to monitor the health of the public.
These purposesare as important to medicine today as past purposes
werein their time. These purposes would be better served byan
increase in the clinical autopsy rate. There is a fairlylarge
amount of literature expressing concern over the de-cline in
frequency and illustrating the many positives tobe gained through
clinical autopsies. This suggests theprocedure does not suffer from
a complete loss of interestbut, more likely, is lagging behind in
the fight for limitedfunds. The clinical autopsy rate at the Queen
Elizabeth IIHealth Sciences Centre in Halifax, Nova Scotia, is not
aslow as has been published for other hospitals, but the rateis
falling. The medical community might benefit from at-tempts to
increase the rate of clinical autopsy performance.Future research
into ways of increasing the clinical autop-sy rate is needed.
References
1. Dada MA, Ansari NA. The postmortem examination in diagnosis.
J ClinPathol. 1996;49:965966.
2. Derman H, Wagner LR. Anatomic and consultative pathology
practice. ArchPathol Lab Med. 1997;121:12141222.
3. King LS, Meehan MC. A history of the autopsy. Am J Pathol.
1973;73:514542.
4. Rosai J. Pathology: a historical opportunity. Am J Pathol.
1997;151:36.5. Cotton D, Cross S. The Hospital Autopsy. Toronto,
Ontario: Butterworth-
Heinemann Ltd; 1993.6. Knight B. Forensic Pathology. 2nd ed. New
York, NY: Arnold/Oxford Uni-
versity Press Inc; 1996.7. Randall B, Fierro M, Froede R.
Practice guideline for forensic pathology.
Arch Pathol Lab Med. 1998;122:10561064.8. What Deaths Are
Notifiable to the Medical Examiner? Advice for Doctors
and Other Medical Professionals in Nova Scotia. Halifax, Nova
Scotia: Depart-ment of Justice, Office of the Chief Medical
Examiner; 2000.
9. Campbell K. Post-mortems: how and why they are carried out.
Nurs Times.1997;93(16):5254.
10. Geller SA. Autopsy. Sci Am. 1983;248:124136.11. Nemetz PN,
Leibson C, Naessens JM, Beard M, Tangalos E, Kurland LT.
Determinants of the autopsy decision: a statistical analysis. Am
J Clin Pathol.1997;108:175183.
12. Goldman L, Sayson R, Robbins S, Cohn SH, Bettmann M,
Weisberg M.The value of the autopsy in three medical eras. N Engl J
Med. 1983;308:1000
1004.13. Lowry F. Failure to perform autopsies means some MDs
walking in a fog
of misplaced optimism. CMAJ. 1995;153:811814.14. AMA Council on
Scientific Affairs. Autopsy: a comprehensive review of
current issues. Arch Pathol Lab Med. 1996;120:721726.15.
Hanzlick R, Baker P. Institutional autopsy rates. Arch Intern Med.
1998;
158:11711172.16. Hill RB, Anderson RE. The Autopsy: Medical
Practice and Public Policy.
Toronto, Ontario: Butterworths; 1988.17. Haque AK, Patterson RC,
Grafe MR. High autopsy rates at a university
medical center: what has gone right? Arch Pathol Lab Med.
1996;120:727732.18. McPhee SJ. Maximizing the benefits of autopsy
for clinicians and families:
what needs to be done. Arch Pathol Lab Med. 1996;120:743748.19.
Hill RB, Anderson RE. The recent history of the autopsy. Arch
Pathol Lab
Med. 1996;120:702712.20. Lundberg G. Low-tech autopsies in the
era of high-tech medicine: contin-
ued value for quality assurance and patient safety. JAMA.
1998;280:12731274.21. Nichols L, Aronica P, Babe C. Are autopsies
obsolete? Am J Clin Pathol.
1998;110:210218.
-
7/31/2019 Declining Clinical Autopsy
7/7
930 Arch Pathol Lab MedVol 125, July 2001 Autopsy Rates in
Halifax, Nova ScotiaWood & Guha
22. Burton E, Troxclair D, Newman W. Autopsy diagnoses of
malignant neo-plasms: how often are clinical diagnoses incorrect?
JAMA. 1998;280:12451248.
23. Roosen J, Frans E, Wilmer A, Knockaert D, Bobbaers H.
Comparison ofpremortem clinical diagnoses in critically ill
patients and subsequent autopsyfindings. Mayo Clin Proc.
2000;7:562567.
24. Sonderegger-Iseli K, Burger S, Muntwyler J, Salomon F.
Diagnostic errorsin three medical eras: a necropsy study. Lancet.
2000;355:20272031.
25. Hutchins GM, ed. Autopsy Performance and Reporting.
Northfield,Ill: Col-lege of American Pathologists; 1990.
26. Pellegrino ED. The autopsy: some ethical reflections on the
obligations of pa-thologists, hospitals, families, and society.
Arch Pathol Lab Med. 1996;120:739742.
27. Lundberg GD. College of American Pathologists Conference
XXIX on Re-structuring Autopsy Practice for Health Care Reform:
lets make this autopsy con-ference matter. Arch Pathol Lab Med.
1996;120:736738.
28. Bennett A, Collins K, Hanzlick R. Outcome analysis and
quality assess-ment. Arch Intern Med. 1999;159:13991400.
29. Collins K, Bennett A, Hanzlick R. The autopsy and the
living. Arch InternMed. 1999;159:23912392.
30. Hill RB, Anderson RE. The evolving purposes of the autopsy:
twenty-first-century values from an eighteenth-century procedure.
Perspect Biol Med. 1989;32:223233.