Embed Size (px)
Citation preview

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
1
azzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz
December 2014 Journal Email: [email protected] Website: www.namigdm.org
Mailing address: Box 12174, Des Moines 50312 Phone number: (515) 277-0672
“Education, Support, Advocacy and Research” Serving Polk, Dallas, Warren, and Madison counties
Mission statement Empowering individuals, families and community by providing
hope and education about brain disorders In this issue –
Page 1 DM Bed Charts, Membership information, Advocacy Page 2 MH Statistics and locations for more information Page 3-4 Resources, Support Groups, Crisis Services Page 5-12 Articles of interest Page 13 NAMI GDM information Page 14 How Can You Help, Calendar Events
Help Our Membership Grow!!
Join NAMI on-line to become a member at the local, state, and national
level. www.namigdm.org (at the top of the
screen, click on blue “donate” box in the upper right of the task bar) - or –
go to www.nami.org/JOIN – or -
Please make checks payable to NAMI Greater Des Moines.
$35 for an individual or family membership - $3 for persons with
limited income
Name ___________________________________
Address _________________________________
________________________________________
Email ___________________________________
Phone __________________________________
Do you want to receive our monthly newsletter by mail _____ or
email _____?
We need your support to continue to provide this newsletter. If paying by check, please mail to NAMI
GDM, Box 12174, Des Moines, Iowa 50312
Acute Care Psychiatric Hospital Beds
Available in the Des Moines Area
Location Adult Geriatric Children & Adolescent
Total Beds
Mercy Hospital downtown
18 16 34
Iowa Lutheran -4 more in NovDec?
36* 12 16 64
Broadlawns 30 30
Des Moines VA 10 10
Total 138
These beds are full every day, 365 days a year and access is difficult.
Advocacy Training – NAMI Smarts
Do you want to advocate for better mental health care, for more mental health services?
NAMI Smarts is an advocacy training program NAMI Greater Des
Moines will be offering on:
Sunday, December 7, 2014
Iowa Lutheran Hospital
700 E. University, Des Moines
2:30 to 4:30 PM
Conference Room A & B (cafeteria level)
The training is free
Module 1: Telling Your Story
Real stories are the most potent motivator for legislators. Telling Your Story guides you through writing and delivering a concise and compelling version of your story that will serve as the springboard for your advocacy.
Module 2: Emails and Phone Calls
Don't think you emails and phone calls are making an impact? Emails and Phone Calls shows you how to write emails that get attention and make phone calls that policy makers remember.
Please pre-register by sending an email to [email protected] We will need an accurate count of attendees so we have adequate training materials prepared.
Find your voice and make a difference!

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
2
6% of Iowa’s population has severe mental illness or approximately
180,000 people. Listed above are the beds available for acute
care. 762 vs. 180,000 – no wonder the beds are full every day,
365 days a year and access is difficult.
Must Reads: The Cost of Not Caring http://www.usatoday.com/longform/news/nation/2014/10/09/suicide-mental-health-prevention-research/15276353/ - 40,000 Suicides Annually, Yet America Shrugs - Cost of Not Caring: Stigma Set in Stone - Cost of Not Caring: Nowhere to Go
The Power of Mindfulness – How a Meditation Practice Can Help
Kids Remain Focused, Less Anxious http://www.childmind.org/en/posts/articles/2012-4-9-power-of-mindfulness
NAMI Websites
Public Policy Platform: www.nami.org/platform State Advocacy: www.nami.org/stateadvocacy Other Policy Issues: www.nami.org/policy Child & Adolescent Action Center: www.nami.org/caac CIT Resource Center: www.nami.org/cit CIT for Youth Resource Center: www.nami.org/citforyouth Multicultural Action Center: www.nami.org/multicultural Legislative Branch www.legis.iowa.gov
Iowa Senate: (515) 281-3271 Iowa House: (515) 281-3221 Executive Branch www.governor.iowa.gov
(515) 281-5211 MHDS Website http://dhs.iowa.gov/
Iowa Medicaid http://dhs.iowa.gov/ime/about
Check out www.infonetiowa.org/ for legislative
information, too.
Mental Health Institutes (MHI)
Total # of Beds
# adult beds
# child & adolescent beds
# geriatric beds
PMIC Beds*
Dual Diagnosis Beds
Substance Abuse Beds
Some of the prison mental health bed numbers compared to bed numbers outside corrections system
Cherokee MHI
36 24 12 100 bed Civil Commitment Unit for Sexual Offenders at Cherokee MHI
Clarinda MHI
35 15 20 Co-campused with a 795 bed prison and a 147 bed minimum security unit at the Clarinda MHI – the Director of both is a Corrections person.
Independence MHI
60 40 20 15
Mt. Pleasant MHI
9 9 19 50 Co-campused with a 914 bed prison at the Mt. Pleasant MHI
Total MHI beds
140 88 32 20 15 19 50 Iowa is 47th in the nation for the number of hospital beds based on our population.
Staffed Hospital Beds Statewide
622 471 90 61
Total 762 559 122 81
These are Medicaid waiver programs Iowa offers eligible residents to allow persons to receive necessary services to remain in their home and community rather than an institutional setting. Waiver Programs # slots there
are $’s for # on Waiting
List June 2014
FY 2013 Ave. Cost per person
Health & Disability 2651 3067 $10,356
AIDS/HIV 34 0 $10,889
Elderly 8873 0 $8824
Intellectual Disabilities 12536 0 $36,021
Brain Injury 1339 1050 $22,353
Physical Disability 1024 2474 $5872 Children's Mental Health 1144 1816 $11,617 27601 8407
http://dhs.iowa.gov/sites/default/files/6%201%2014%20Monthly%20Slot%20and%20Waiting%20list%20%28public%29.pdf
Licensed mental health professionals in Iowa Iowa is 47th in the nation for # of psychiatrists based on our population 202 adult psychiatrists in practice 35 child psychiatrists Iowa is 46th in the Nation for # of psychologists based on our population 486 psychologists 96 nurse practitioners and 14 physician assistants with a mental health specialty 4162 social workers with a bachelors or master’s degree 234 marital and family therapists 995 licensed mental health counselors 89 counties are designated as mental health professional shortage areas Iowa is 48th in the nation for # of mental health courts (2 - Woodbury and Black Hawk Counties) and law enforcement crisis intervention teams (CIT).

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
3
Community Resources
Polk County Mental Health Services Polk County River Place – 2309 Euclid Avenue, DM – 243-4545
http://polk.ia.networkofcare.org/mh/
Warren County Mental Health Services 1011 N. Jefferson Way, Suite 900 (west bldg.)Indianola, IA 50125
515-961-1068 email: [email protected] http://www.co.warren.ia.us/mental_health.shtml
Dallas County Mental Health Services 902 Court Street, Suite 1, Adel, IA 50003 515-993-5869
Toll free: 877-286-3227 E-mail: [email protected] http://www.co.dallas.ia.us/department-services/community-
services
Madison County Mental Health Services 209 East Madison, Winterset, IA 50273 515-462-2931
http://www.madisoncoia.us/OFFICES/comservices/index.htm
Polk County Community Mental Health Centers Child Guidance Center – 808 5th Ave – 244-2267
Eyerly Ball Community MH Center 1301 Center St. – 243-5181 Broadlawns Medical Center- 1801 Hickman Road – 282-6770
Eyerly Ball Golden Circle – 945 19th St – 241-0982
Dallas County Mental Health Center
Eyerly Ball Community Mental Health Center
109 S. 9th St., Adel – 515-993-2158
Madison County Mental Health Center
Bridge Counseling Center
300 West Hutchings St. – 515-462-3105
Primary Health Care & Behavioral Health
Engebretsen Clinic, 2353 SE 14th St. – 248-1400 The Outreach Project, 1200 University, Suite 105 – 248-1500
East Side Center, 3509 East 29th St. – 248-1600 Primary Health Care Pharmacy,1200 Univ.,Suite 103 262-0854
Clubhouse Passageway,305 15th St., Des Moines 515-243-6929
Iowa Medicaid Non-Emergency Medical Transportation Program
When you have a need for Non-Emergency Medical Transportation, call TMS. Once you have provided all the necessary information, a TMS operator will explain how your trip request will be met. To request a ride please call 1-866-572-7662. To find out more about
forms and policies, go to: http://tmsmanagementgroup.com/index.php/iowa-medicaid-net-program
Joy Ride Transport
Joy Ride is a transportation service available in the greater Des Moines area and surrounding communities To make a reservation, call 515-331-
1100 or 855-225-7433 [email protected] http://ridejoyride.com/
Office Hours: Monday – Friday 8:00 AM – 5:00 PM They try to
accommodate same-day requests for transportation. Weekend and holiday transportation is also available with advance notice.
SUPPORT GROUPS for Family Members
Eating Disorders - Coffee Connection for Parents
The Coffee Connection is open to parent(s) who have a child of any age struggling with an eating disorder and would like to connect in a supportive effort with other parents. We will meet the 2nd Sunday of the month from 4:00-5:30 pm at the Cafe Diem, 2005 S. Ankeny Blvd., Ankeny, IA. Check under Events Calendar for specific dates. Direct your questions to [email protected]
Des Moines - Third Sunday of the month –Family members, if
you are interested in participating in a NAMI family support group, please contact Susie & Richard McCauley 274-5095 or [email protected] Meetings are at Eyerly-Ball Community Mental Health Center-1301 Center 2:30-4 S
4th Monday of each month – 5:30 – 7 PM – a support group for
Polk County parents and caregivers of children and adolescents with severe emotional disturbance (SED) or mental illness – a sibling support group meets separately - at Capitol Hill Lutheran Church, 511 Des Moines St., in the basement – child care provided, can also provide free transportation and interpretation services – pre-register, if possible – call Angie at 558-9998.
Ankeny – 1st Tuesday of each month – Family members if you
are interested in participating in a NAMI family support group, please contact Nora Breniman at 964-1593 or Regina Murphy at 777-0191, Group meets at Ankeny First United Methodist Church, 206 SW Walnut, Ankeny, RM 310/314 at 7-8:30 PM
2nd Thursday of each month – 6:30 P.M. – a support group for
Family members – Lutheran Church of Hope, 925 Jordan Creek Parkway, West Des Moines–in Conference room (main floor behind offices across from small chapel. Supper (free will offering) is available at 5:30 prior to the support group. Bonnie and Randy are facilitators.
Friends of Iowa Prisoners has a meeting at Noon on the 3rd
Tuesday of the month at Wesley United Methodist Church, 800
12th St., Des Moines.
1st and 3rd Tuesdays of each month –Voices to be Heard Support
group – Union Park United Methodist Church –East 12th & Guthrie - Light meal at 5:30 P.M. Support group for adults and program for children from 6 PM to 7PM. –If you have a loved one in prison or parole system you are concerned about or if you are concerned about those in prison, please feel free to join us. If you have questions, please call Melissa Nelson at 280-9027.
Due to the fourth Thursdays falling on holidays for November and December, the Indianola
family support group is changing the room and date of meeting for November and December. We will meet on the third Thursday for November (20thl) and December (18th) at 6:30p.m. in Room 216
on the south side of First United Methodist Church- 6:30 to 8 PM at
307 W. Ashland. For more information, please contact Grace 205-9765 [email protected]
Tell Me Where to Turn Support for Family Members

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
4
SUPPORT GROUPS for Persons in Recovery
Every Monday evening 7-8:30
P.M. – a support group for persons with mental illness – facilitated by
persons with mental illness - at the Plymouth Congregational Church, 42nd & Ingersoll – Room 305 - contact Jim Goodrich 490-2758 or [email protected]
First Monday of each month – 7-9 P.M. –GDM CHADD Support
Group – support for those families struggling with ADHD – Attention Deficit Disorder - West Des Moines Public Library, 4000 Mills Civic Parkway –call Julie for more info –515-223-6730.
2nd & 4th Mondays of each month – 7 P.M. – depression and
bipolar support group., St. Boniface Catholic Church, 1200 Warrior
Lane, Waukee. [email protected] Julie 710-1487
Every Tuesday afternoon 2-3:30
P.M. – a support group for persons with mental illness – facilitated by
persons with mental illness – at Plymouth Congregational Church, 42nd and Ingersoll in the Burling Room. For more information, contact Matthea Little Smith 783-2763 [email protected]
Every Tuesday evening – 8-10 P.M. - Recovery Inc., a self-help
group for people who have nervous and mental troubles – at St. Mark’s Episcopal Church, 3120 E. 24th St., Des Moines – Call 266-2346 – Marty Hulsebus.
Tuesday evenings 5:30-7:00 Dual Diagnosis support group at
Eyerly Ball Mental Health Services – call 243-5181 for more info.
Tuesday evenings 7:30 PM - 4211 Grand – Friends House – in the Meeting House – Meditation and Mindfulness Group –
sponsored by Crossroads of Iowa 633-7968-please pre-register
Every Wednesday afternoon at 1 PM - Emotions Anonymous at
Central Iowa Center for Independent Living, 655 Walnut (enter on the 7th St. side) - contact Duane at 243-1742 for more information
Every Thursday evening 6:30-7:30 PM – 4211 Grand – Friends
House – in the Conference Room – H30 - a support group with a focus on opiate, heroin and prescription pill addiction for Women –
sponsored by Crossroads of Iowa 633-7968 – please pre-register
Every Thursday evening – 7:45 – 9:45 P.M. – Recovery, Inc. - a
self-help group for people who have nervous and mental troubles – at St. Timothy’s Episcopal Church, 1020 24th St., in West Des Moines. Call – 277-6071-Deb Rogers.
Every Saturday afternoon – 2:00 – 3:30 P.M. – the Depression
and Bipolar Support Alliance meets at Iowa Lutheran Hospital – University at Penn Avenue – Level B – private dining room. Contact Ron at [email protected] or call 279-5710
For persons suffering from postpartum depression – a support
group entitled “Amazing Girls Accepting Peace Everyday (AGAPE)”. Information can be found at Meetup.com – enter AGAPE. You need to request to be a part of the group – contact Tricia at [email protected]
An Epilepsy Support group is held the 4th Thursday of every
month at 6 PM at Mercy Medical Center, East Tower, Room 3, 1111 6th Avenue, Des Moines. For more information, contact Roxanne Cogil 515-238-7660 or [email protected]
Every Saturday evening-“The Road”-Christian Life Center
location, 710 NE 36th street in Ankeny (easy access from the new exit off I-35) – the schedule: 6 PM Pizza supper with free will offering, 7:15 PM Worship, 8 PM recovery groups. Child care available for infants and toddlers. For further questions, call 515-777-8333 to speak to a team member. Facebook page:
TheRoad@AFUMC
Suicide is now the first cause of injury deaths, followed by car crashes, poisoning, falls and murder. Suicides are terribly undercounted. There may be 20 percent or more unrecognized suicides. –Sept. 20, 2012 American Journal of Public Health
Suicide Prevention Lifeline 1-800-273-8255
If you are thinking of hurting yourself, tell someone who can help. If you cannot talk to your parents, your spouse, a sibling - find someone else: another relative, a friend, or someone at a health clinic. Or, call the National Suicide Prevention Lifeline at (800) 273-TALK (8255) - http://ok2talk.org/
Coping After a Suicide Support Group – Polk Co. Crisis and
Advocacy Services – Contact: Joann-286-3600 - Meeting day – 2nd Thursday of each month 6-7:30 P.M. and last Saturday of each month 9-10:30 A.M. Meeting place is 2309 Euclid Avenue - park at the west end of the building near the flags and come in the glass doors. Victim Services Phone: 515-286-3600
Excellent Magazines to Subscribe to:
Esperanza http://www.hopetocope.com/
for articles on Anxiety and Depression BP magazine http://www.bphope.com/ for articles on Bipolar SZ Magazine http://www.mentalwellnesstoday.com for articles on Schizophrenia – only offered on-line
Bullying, Suicide Hotline - Available 24/7, Your Life Iowa is a
phone call or text away at www.Yourlifeiowa.org or 855-581-8111. Trained counselors will provide guidance and support about bullying, and critical help to youth
Consult www.namigdm.org for more community resources.
Crisis Services in Polk County
Mobile Crisis Response Team
Emergency Calls: 911 – 6:30 AM to 2:30 AM Non-Emergency Calls: 515-564-5742 Pre-Commitment Screening Service
During Business Hours: 515-729-1772- 8 AM to 4 PM After Business Hours: 515-564-5742 Crisis Observation Center – open 24/7
1420 Mulberry St, West entrance, Des Moines Phone: 515-564-5742 Crisis Stabilization Center – transitional housing up to 90 days
1212 E. McKinley Avenue, Des Moines Phone: 515-777-1972 Fax: 515-777-1794
Support for Persons with Lived Experience
Warning: Regular or heavy alcohol use can worsen most psychological states, such as anxiety, depression, bipolar, schizophrenia, or eating problems. Alcohol can change the way a person feels in the short run; however, the overall effect only worsens a disorder. Marijuana and other drugs can have similar or more serious effects on the brain.

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
5
If you have a mental health crisis in your family and are in need of emergency assistance – call 911. Be clear with the dispatcher what the situation is,
that it is a mental health crisis, and you need the Polk County Mobile Crisis Response Team to assist. The goal is to keep everyone safe and to seek the appropriate level of assistance for the ill family member or friend.
The Mobile Crisis Response Team provides short term on-site crisis assessment and intervention for children, youth and adults experiencing a mental health crisis. The non-emergency phone number for the mobile crisis team is 564-5742. The police liaison to the Mobile Crisis Team is Officer Kelly Drane. Her hours are 8 to 4 Mon-Fri phone is 205-2270. The Mobile Crisis Unit team leader is Torry Simmons. Torry can be reached at 564-5742 if you have questions or concerns.
If the crisis situation is in Polk County - in response to your phone call, the first people to arrive to the situation will be police officers. Officers will determine if it is a mental health related issue and maintain safety at the scene. Officers make a request through dispatch if the Mobile Crisis Team is needed. Mobile Crisis only takes referrals from law enforcement.
When the Polk County Mobile Crisis Team staff arrive, a mental health assessment will be done, on-site counseling and problem solving, crisis plan development, coordination with hospitals if transport to a medical facility is necessary, and medication can be given, if needed and appropriate. The Mobile Crisis Team is available 6:30 AM to 2:30 AM – 7 days week. It is staffed by licensed mental health professionals and registered nurses.
Know the biological underpinnings of mental
illness to debunk myths suggesting brain and behavior disorders are not bona fide illnesses. These myths—and the stigma they create—often keep people from getting the help they need to lead full, productive and happy lives.
Giving through NAMI GDM Endow Iowa fund at the Community Foundation of Greater Des Moines is rewarding—
in more ways than one.
Nathaniel Ayers of ‘Soloist’ Fame and Forced Medications
Pete Early Blog
What became of Nathaniel Ayers, the talented musician who
was diagnosed with a severe mental illness and ended up homeless on the streets of Los Angeles? You will recall that he was the subject of Steve Lopez’s best-selling book, The Soloist as well as the powerful movie based on that book.
Steve tells us in a thought-provoking column printed last night that explores the difficult choices that many of us with loved ones face.
A tough call on medication * Nathaniel Ayers has won victories in his battle to function despite
schizophrenia. But he lands in a courtroom, and hard decisions await.
By Steve Lopez
Howard Askins grew up in New York, the son of blue-collar transit authority employees who expected him to go far, and he did. His first stop was Brown University, and then he was off to Harvard, where he earned both medical and law degrees before moving on to psychiatric residency at UCLA.
Nathaniel Ayers, like Askins, grew up working class — in his case, Cleveland was home. His dream was music, not medicine, and his hard work landed him at the prestigious Juilliard School for the Performing Arts in New York City, where he played for a time in the same orchestra as Yo-Yo Ma.
On Monday, the two African American men sat across from each other in a former pickle factory on San Fernando Road that serves as the mental health division of Los Angeles County Superior Court. The two have a deep mutual respect for one another, but a great difference of opinion.
As he stated from the witness stand, Dr. Askins believes Mr. Ayers is a highly intelligent, charming and talented gentleman who suffers from a mental disorder so severe he can’t fully grasp how ill he is. The doctor has recommended medication that he believes could help control Mr. Ayers’ paranoia and emotional swings, along with occasional threatening behavior of the sort that landed him in court.
Mr. Ayers has a decidedly different take. Yes, he told the Commissioner Laura Hymowitz, he has acted inappropriately at times and deeply regrets it. But he is adamantly opposed to forced medication and believes he can function well without it. He disputed the doctor’s comments about his paranoia, telling Hymowitz that his neighbors in Hollywood are too lovely to be feared. He also said he likes music, and that the Hollywood Bowl is a beautiful place where the seats are often filled. If you can’t get a ticket, he said, you just wait until the next concert.
I managed to hold it together pretty well until that point. And then I lost it. His humility, his 40 years of torment, the lost career he’d wanted so badly — it all got to me.
There’s no one I admire more than Mr. Ayers; no one who has taught me more about courage and about believing in something and remaining faithful to it regardless of the challenges. The journey we began more than nine years ago has taken us from skid row to the White House, where Mr. Ayers performed and met President Obama.
But along with the great moments, I’ve also witnessed Mr. Ayers’ daily struggle with a relentless and debilitating disease that often clouds reason and judgment. As I sat in court, I wrestled again with my enduring conflict, part of me respecting Mr. Ayers’ wishes not to take medication, and part of me wishing he would at least try to do it Dr. Askins’ way.
Thousands of people confront these issues for years on end. Forced psychiatric commitments, and forced medication, are at the center of a decades-long legal, moral and medical debate over the civil liberties of people with mental disorders. There are compelling arguments on all sides, no stock answers, and no two cases alike.

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
6
When his condition worsened a month ago, Mr. Ayers was taken to a psychiatric hospital against his will, but without incident, by an L.A. County unit consisting of both mental health officials and police officers. He handled it pretty well, calling me daily with updates on his activities and new friends. Dr. Askins and the staff at the hospital determined that he needed medication, but Mr. Ayers refused, and he prevailed at his first two court appearances.
That led to Monday’s conservatorship hearing, with the county trying to establish that Mr. Ayers was unable to care for himself and needed the appointment of a conservator — his stepsister — who will have the authority to consent to forced commitments and medication even if Mr. Ayers objects.
Mr. Ayers rejected all of that. Now 63, he remembers too vividly the zombie-like side effects of electroshock therapy and the meds he was administered as a young man. He told the commissioner his eyes rolled back and his tongue swelled, and he wasn’t buying Dr. Askins’ claim that such side effects are less likely with newer drugs.
And yet, what’s the alternative?
Mr. Ayers’ life is a concert of disjointed movements, with sweet reckonings and crashing dissonance. He sometimes turns on those working hardest to help him. Two highly regarded supportive housing nonprofits — LAMP Community and Housing Works — have had great success with him, but disappointments as well. There is no cure for schizophrenia, and small triumphs carry no guarantee of encores.
“I’m an optimist,” Dr. Askins said in court, arguing that with treatment, Mr. Ayers might one day prosper back in the community rather than in a locked ward.
Askins told me after court that his parents instilled in him a duty to serve people in need. He was drawn to psychiatry by a desire to “be an advocate for people who are the most vulnerable in our society,” and to “uphold people’s dignity in very trying circumstances.”
I’ve come to learn it’s not just the drugs Mr. Ayers opposes, but the idea of being controlled. And yet he often has no control over his own emotions. Can the side effects of medication be as disorienting as the direct effects of a maddening neuro-chemical disorder?
Commissioner Hymowitz would later tell me, in chambers, that she considers it a privilege to try to help the reeling patients and shattered families who come before her.
When she started in mental health court 15 years ago, she wasn’t a big advocate of forced medication. But after seeing so many lives transformed, even if only temporarily, she’s become a believer in at least trying to find pharmaceutical relief.
When the moment of truth arrived in the case of Mr. Ayers, Hymowitz ruled in favor of a conservatorship. You can’t really say she ruled against him, though. I think that she, like others in the courtroom, had his best interests in mind. Mr. Ayers declared that he will contest the ruling, and he’s entitled to a jury trial. In the meantime, though, the meds can be administered.
As he left the courthouse I handed him the violin he’d been asking for, so he could take it back to West Covina with him. He called me when he got to the hospital, but said he couldn’t remember why he had. I told him I was glad he called. When you can’t be sure what lies ahead, there’s small comfort in hearing a familiar voice. [email protected]
Using Medicaid to Prevent Recidivism in States' Corrections Systems
CSG Justice Center
Since 1997, states have been able to bill for Medicaid-enrolled inmates who leave prisons or jails longer than 24 hours for health treatment in a hospital or nursing facility. That provision is an important but little-known exception to the federal prohibition on spending Medicaid funds for health services to inmates of state prisons and local jails. According to The Pew Charitable Trusts in a recent report, states spent $7.7 billion on inmate health care in 2011. These costs are expected to increase as the inmate population becomes older and sicker.
For inmates leaving prison or jail, “the highest risk of recidivism is in the first six months.” Data indicate 30 percent of former inmates
recidivate in those first six months following releasel. In addition, health risks are elevated. Individuals coming out from behind the walls, face a twelvefold risk of death in the two-week period post release.
States are being encouraged to adopt policies to suspend inmates’ Medicaid enrollment rather than terminate it when they are incar-cerated. When a person’s Medicaid enrollment is suspended rather than terminated, it can easily be reactivated upon release, facili-tating the transition to appropriate health, behavioral health and substance use treatment services in the community. Reactivating Medicaid enrollment upon release is much easier than reapplying.
In checking with Iowa Medicaid, we received this response “Yes, we received guidance from the Center for Medicare and Medicaid Services (CMS) in 1997 indicating that once an inmate is admitted as an inpatient to a medical facility (such as a hospital or nursing facility), that person is no longer considered to be an inmate of a public institution and may be eligible for Medicaid. The person would only be eligible for Medicaid during the time he or she is an inpatient. The guidance from CMS indicated the critical factor is that the person is admitted as an inpatient. There was no indication that there was any time factor such as 24 hours.
Since 1997, Iowa has been determining eligibility for Medicaid for inmates who are admitted to a medical facility whenever that person files an application. Starting in 2012, Iowa has been suspending Medicaid for Medicaid recipients when they become inmates if they remain otherwise eligible and DHS is notified of their incarceration by the penal institution through our automated reporting system. The suspension process makes the person eligible for Medicaid coverage only for inpatient services. The inmate no longer needs to reapply for Medicaid when admitted to a hospital or nursing facility if their Medicaid is in suspended status.
Some locales have built a focus on Medicaid enrollment into their discharge planning process. In Cook County, Ill., for instance, discharge planners work with inmates to ensure they are enrolled in Medicaid if they are eligible. They also set up post-release appointments with providers.
In Massachusetts, dedicated discharge planning staff works with pre-release inmates to facilitate Medicaid enrollment. According to the Massachusetts Department of Correction, 94 percent of state prisoners returning to the community have active Medicaid upon release.

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
7
Quick Medicaid re-enrollment, especially in states that have expanded Medicaid eligibility as allowed under the Affordable Care Act, can mean seamless access to treatment after release.
A “warm handoff” includes not just a connection to benefits, but also a connection to services. Medicaid eligibility is often critical to getting community services. Sometimes the warm handoff can go as far as a community service provider meeting an individual at the exit door on his or her release from incarceration.
Iowa Medicaid has a demonstration program with the Dept. of Corrections in the discharge planning process for immediate Medicaid coverage and services upon release.
Teenagers in Prison Have a Shockingly High Suicide Rate
http://www.vox.com/2014/10/10/6957497/suicide-prison-rate-juvenile-teenager-prisoners
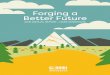
On any given day in 2012, there were about 2,400 teenagers serving time in adult state or federal prisons. And those teenagers were more likely to commit suicide than were inmates from any other age group.
This chart, based on new data from the Bureau of Justice Statistics, shows the suicide rates of state prisoners from 2001-
2012 and drive home just how at-risk teenage inmates can be:
In other words, teenagers in adult prisons are twice as likely to commit suicide as are adults in adult prisons. And they're far more likely to commit suicide than teenagers who are in juvenile detention or in alternative programs.
A 2007 report from the advocacy group the Campaign for Youth Justice found that juveniles in adult prisons are 36 times more likely to commit suicide than are juveniles in juvenile detention.
Fortunately, the number of teenagers in adult prisons has declined over the last decade. In 2002, there were 3,000 teenagers in state or federal prison; throughout 2008 to 2012, there were 2,500 or fewer.
"I can't take it anymore. I give up" A recent New Yorker article covered what it's like to be a teenager
in an adult criminal-justice system. The subject of the New Yorker piece, Kalief Browder, was in jail on Rikers Island for three years waiting to be put on trial for stealing a backpack. (The trial
never actually happened; instead, the prosecutor dismissed the charges and Browder was released.)
Browder tried to commit suicide at least three times while in jail. The chart above covers prisons, not jails, but Browder's story is a good reflection of what teenagers in adult facilities have to deal with:
For one thing, (Browder's brother) says, Browder was losing weight. "Several times when I visited him, he said, ‘They're not feeding me,' " the brother told me. "He definitely looked really skinny." In solitary, food arrived through a slot in the cell door three times a day. For a growing teen-ager, the portions were never big enough, and in solitary Browder couldn't supplement the rations with snacks bought at the commissary. He took to begging the officers for leftovers: "Can I get that bread?" Sometimes they would slip him an extra slice or two; often, they refused.
Browder's brother also noticed a growing tendency toward despair. When Browder talked about his case, he was "strong, adamant: ‘No, they can't do this to me!' " But, when the conversation turned to life in jail, "it's a totally different personality, which is depressed. He's, like, ‘I don't know how long I can take this.' "
Browder got out of the Bing in the fall of 2011, but by the end of the year he was back-after yet another fight, he says. On the night of February 8, 2012 — his six-hundred-and-thirty-fourth day on Rikers — he said to himself, "I can't take it anymore. I give up." That night, he tore his bedsheet into strips, tied them together to make a noose, attached it to the light fixture, and tried to hang himself. He was taken to the clinic, then returned to solitary. Browder told me that his sheets, magazines, and clothes were removed — everything except his white plastic bucket.
Imprisoning teenagers as adults is unsafe for them and others
Putting teenagers in adult prisons doesn't just increase their danger to themselves. They're much more vulnerable to assault from other inmates. And teenagers who get treated as hardened criminals while they're still high-school-aged are more likely to engage in violence when they do get out of prison.
The problem with trying and incarcerating teenagers as adults is that it's something of a self-fulfilling prophecy. Juveniles get treated as adults, in theory, because they've committed particularly serious or violent crimes — but even when controlling for the seriousness of the crime, and other factors, kids who have been imprisoned in adult prisons are more likely to commit further acts of violence than those who serve their time in juvenile facilities.
Much of this is because adult prisons don't have the counseling and education resources that juvenile ones do. If juvenile facilities are, at their best, designed to prevent kids from being incarcerated again, adult prisons have mostly given up on that aspiration. Instead, staff at adult prisons just hope for order — even if it comes at the hands of prison gangs and ethnic or regional cliques. Anthony Pleasant, a young man from DC who spent ten years in federal prison starting when he was 16, says, "A warden, anybody will tell you, they allow the yard to run itself."
For teenagers, serving in adult prison is a basic risk to their personal safety. "I was with a lot of people who had life, and I had peanut time compared to them," Pleasant says. "If they had wanted to harm me, they would have done it and smiled afterward, because it meant nothing to them. Because they got life."
Juveniles can also develop unsavory associates that will encourage them to commit more crimes after they get out. Pleasant knew one

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
8
boy in prison who was sentenced to adult prison at the age of 16, and ended up "put in a situation where he had to harm somebody." He got a new conviction after the incident, for 25 years.
Should a Child Offender Be Treated as an Adult?
The New York Times
The government may recommend he still sit in the back seat of a car, but a 10-year-old boy can be charged as an adult for the homicide of a 90-year-old woman and potentially spend the rest of his life in prison. Along with Somalia, the United States is one of two countries in the world that have not ratified a United Nations convention that requires countries to have a minimum age to consider a child criminally culpable. According to Amnesty International, it stands alone in sending juveniles to prison for life without the possibility of parole. In some parts of the country children are automatically charged as adults when accused of homicide. Two recent cases have exposed ambiguities in the criminal justice system and drawn criticism from those who question whether the law should ever treat children as adults. Read More.
DBT: What Is Dialectical Behavior Therapy?
A treatment for teenagers with serious trouble managing emotions www.childmind.org Juliann Garey
If you have a child with psychiatric or behavior problems, there's a good chance you've heard of mindfulness and cognitive behavioral therapy (CBT), two different approaches to helping kids with everything from test anxiety to depression. But there's another very promising therapy that combines elements of both. DBT, or dialectical behavior therapy, is an intensive, highly structured program that's been adapted specifically for adolescents with
extreme emotional instability, including self-harm and suicidal ideation.
The "dialectical" in DBT means the therapy works by dealing with two things at once that might seem contradictory: acceptance of feelings
(mindfulness) and learning to use thinking to change feelings (CBT). It's basically "'I'm doing the best I can' on the one hand," notes Dr. Alec Miller, professor in the Department of Psychiatry and Behavioral Sciences at the Albert Einstein College of Medicine "and 'I need to do better.' That's a dialectical truth."
A brief history of DBT
Dialectical behavior therapy was developed by Dr. Marsha Linehan in the 1970s to treat adult borderline personality disorder—a mental illness with symptoms ranging from chronic suicidal thoughts and/or self-harming behaviors to anxiety and depression. These patients were typically thought of as "difficult," if not impossible, to treat. Dr. Linehan redefined the disorder, reframing it as a specific problem of the emotion regulation system that can be addressed with a structured intervention.
People with borderline personality disorder have trouble regulating their moods, which leads to impulsivity and conflict in interpersonal relationship. That, in turn, often leaves them feeling misunderstood by others around them. First, Dr. Linehan tried traditional CBT, which emphasizes using conscious thoughts to confront and change problematic emotions. She was unsuccessful with her patients. So she then tried a much more acceptance-based approach that came out of her meditation and mindfulness practice. This, too, failed.
"So then she had this brilliant epiphany," says Dr. Miller. "Blending the acceptance strategies of mindfulness with the change technologies of CBT to create this dialectical behavior therapy."
How Does DBT Work?
DBT is designed to help with extreme emotional instability, which clinicians call "dysregulation"—the inability to manage intense emotions. Dysregulation leads to impulsive, self-destructive, or self-harming behaviors. The goal of DBT is to teach adolescents techniques to help them understand their emotions without judgment—the mindfulness component—and also to give them skills and techniques to manage those emotions and change behaviors in ways that will make their lives better. But it takes work and commitment.
DBT for adolescents involves individual therapy and group skills training, where parents and teenagers learn together. The feedback from parents, says Dr. Jill Emanuele, a clinical psychologist at the Child Mind Institute, is, "Where have these skills been all my life? I need these skills too." Other components include telephone consultation (patients are encouraged to call their therapists when they feel the urge to self-harm), family therapy, and weekly consultation team meetings where the therapist checks in with other professionals to consult on the case.
What skills does DBT teach?
DBT skills training is very structured; for adolescents, it consists of five modules:
Mindfulness skills: Being present in the moment and under-
standing the signs of unregulated emotions
Emotion regulation skills: Coping with difficult situations by
building pleasant, self-soothing experiences to protect from emotional extremes. "Especially with teenagers," says Dr. Emanuele, "there's a big focus on the physical body: eating properly, getting enough sleep, taking their medicine and avoiding drug use."
Interpersonal effectiveness skills: "It's often interactions with
others that are the negative triggers for impulsive behaviors," Dr. Emanuele says. The purpose is to teach adolescents how to interact more effectively with others, and enable them to feel more supported by others.
Distress tolerance skills: "It's being able to recognize urges to
do things that would be ineffective, such as hurting themselves or trying to kill themselves" and consciously controlling them, says Dr. Emanuele.
Walking the middle path skill: Kids and parents learn how to
validate one another, how to compromise and negotiate, and how to see the other person's side of things. "It has to do with acknowledging multiple truths in the teenagers' and the parents' worldview as opposed to 'I'm right and you're wrong,' " explains Dr. Miller.
What is DBT used to treat in adolescents?
Borderline personality disorder was historically considered some-thing that could not be diagnosed in a person under the age of 18. But many clinicians, including Dr. Emanuele and Dr. Miller, now feel that symptoms of the disorder do develop in some adolescents,and the debilitating roller coaster of extreme emotions that they experi-ence can be effectively treated with DBT. DBT has also proved effecttive in treating the emotional instability and severe behavioral

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
9
symptoms—self-harm and suicidal thoughts or attempts—seen in adolescents with other diagnoses, including:
Drug abuse
Eating disorders
Depression
Bipolar disorder
Disruptive behavior disorders
ADHD
Anxiety "DBT," says Dr. Emanuele, "is used to treat adolescents with multiple problems that often include suicidality or self-harming, behaviors. The keyword here is multiple."
DBT: An adolescent's perspective
Rachel Monasch did not have it easy as a kid. When she was little her mother's chronic illness kept her in the hospital for long stretches of time. She developed severe anxiety early on in
life and had trouble making friends at school. Eventually she developed an eating disorder and at 13 she began to hurt herself.
At 15, Rachel says, "I had I guess what you'd call a breakdown. I spent most of the year out of school." Rachel had been in therapy for a long time but it was mostly unstructured talk therapy along with medication. When she began struggling with suicidal thoughts she was hospitalized in an adolescent unit at a hospital that she describes as horrifying and traumatic. "I was assaulted by another patient and they didn't do anything." Rachel says she came out more depressed than when she went in.
But then she switched to a therapist who specialized in DBT. That clinician got her enrolled in a 28-day DBT "boot camp" for adolescents that also had an eating disorders program. "We learned and practiced DBT all day, every day, for 28 days," she says. Now, a year later, Rachel is doing very well. She finds some of the tools she learned in DBT more helpful than others, so that's where she focuses her energy. "Distress tolerance, mindfulness, and emotional regulation skills are the big ones for me," she says. "I don't fight with people or even really my parents so the interpersonal effectiveness skills aren't all that helpful to me."
Rachel relies heavily on diary cards—daily logs that track her moods and emotions, what triggered them, how she reacted to them both positively and negatively—and the collection of skills she has come up with to deal with uncomfortable emotions. She has 19 so far. She also does a lot of breathing to center herself.
According to Rachel's dad, "DBT saved her life." But Rachel says it's not quite that simple. "I would say lithium plus DBT and a great therapist saved my life."
FROM GED to PhD.
The Center for Reintegration is launching the 2015 Baer Reintegration scholarships, open to all persons with a diagnosis of schizophrenia or Bipolar Disorder. The scholarships range from GED to PhD. If you know of anyone who meets the criteria and could benefit from these scholarships, we invite them to go www.reintegration.com to learn more and download an application. Sidney R. Baer Jr. was an entrepreneur who had his first break
while attending Yale and was not able to complete his education. Upon his death, he left a vast fortune to the Sidney R.Baer Jr. Foundation which funds mental health projects exclusively.
Why People Think Mental Illness is “All in Your Head”
By Natasha Tracy healthyplace.com
We’ve all heard it – the condescending notion that bipolar disorder, depression or another mental illness is “all in our heads.” This is the notion that we are not ill and that we simply think we are ill. If we
stopped believing we had a mental illness, we would stop having one.
Naturally, this is hogwash. But science and medicine can’t seem to convince people out of this illogical notion and I think that’s because people have their own psychological reasons for wanting to believe that mental illness is “all in our heads.” Mostly, it’s fear.
Why People Believe Mental Illness is “All in Your Head” 1. Mental illness is scary.
Mental illness is a very scary proposition. You don’t control your brain – the very thing that controls every action you commit and every thought you have. No one wants to think that such a thing exists – they are simply too scared.
2. Mental illness can happen to anyone.
The fact of the matter is that mental illness does not discriminate and people of any age, culture and socioeconomic status have mental illnesses. This fact is enough to scare people into believing mental illness doesn’t exist because they can’t accept the fact that it could happen to them or someone they love. 3. Most people don’t understand psychology or psychiatry.
Let’s face it, the brain is a complicated place and few people walking around understand it. This is understandable as even after studying it I find it confounding. But the ignorance held by most people makes it more comprehensible to them to believe in something simple like a problem being “all in your head” rather than investigating the complexities of neurobiology. 4. There are no cures to mental illness and treatments are, well, kind of archaic.
For some reason people are more inclined to believe in something you can cure – probably because it’s less scary. And it’s also less scary to believe in things with extremely effective treatment. No one thinks diabetes is in your head because we know what causes it and how to fix it. 5. Mental illness can make you deny you are mentally ill.
And, of course, there’s anosognosia, which is the clinical state in which a person is mentally ill but the mental illness convinces them they are not. Mental illness is the only disease that can make you deny its own existence. Certainly the idea that the brain can deny its own illness is a frightening thought.
Fear Makes People Say it’s “All in Your Head”
I could go on, but in short, other people are scared of mental illness and saying “it’s all in your head” is their way of assuaging their own fear. It’s sad that other people try to make themselves feel better by dismissing the pain and suffering of others, but it’s human; it’s what we do. It’s like saying, “well of course he got AIDS, he’s gay,” when, of course, over a quarter of new HIV cases are in heterosexuals each year. But by a heterosexual denying that fact, they can write off the terrifying problem as something they will never have to deal with.

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
10
So we, the people with the illnesses, are faced by the fear of others and the lack of compassion and logic that it breeds. The only consolation, maybe, is this: we know that we have faced the big, scary fear and survived. We know that we are strong. We know that we can stand up to that which scares us. We know that we have compassion and understanding for others.
Of course, that consolation is “all in our heads.”
What Is Auditory Processing Disorder?
When kids are listening, but not taking in information
www.childmind.org
Some young children seem to find it unusually difficult to take in information verbally. Even though there's nothing wrong with their hearing, they have trouble registering—or registering correctly—what people are saying, and remembering what they hear. They have trouble learning to read and expressing themselves clearly because they confuse the sounds of different words.
These children have a condition called auditory processing disorder. They have normal hearing, but for some reason they are weak in basic skills for decoding language that most kids develop
naturally.
"The kids we see are having difficulty following directions," explains Rachel Cortese, a speech-language pathologist at the Child Mind Institute. "They ask for repetition a lot. They seem to just kind of miss things in conversations. From testing we know that their ear is hearing the signal. It's attending to the auditory information. But they have glitches when the brain is not assigning meaning—or the right meaning—to that signal." Read more at: http://www.childmind.org/en/posts/articles/2014-10-28-what-auditory-processing-disorder
A Comparison
Recovery Oriented Care Medical Model of Care
Consumers as partners in care Provider directed care
Whole person centered Symptom reduction-focused
Strengths based Problem/symptom based
Works with people who have illnesses
Treats illnesses
Engages client in proactively managing own responses to symptoms
Encourages dependence on system
Encourage Hope about the future
Can discourage consumers about their future options
Offers Psycho-education, information, choices about how consumers can meet goals
Offers support for dealing with symptoms, ways to measure symptom reduction and exacerbation
Augmented by Peer support – encourages a diverse support system
Can encourage dependence on system for support
Uses evidence based practice tools to support consumers in goal attainment
Relies on medication and support to meet symptom reduction goals
Recovery oriented care is not new. Since the mid-1980’s, a great deal has been written about mental health recovery from the perspective of the consumer (client), family member and mental health professional. The amount of research of various aspects of recovery continues to grow. Early research by Courtney Harding
(1987) and others challenged the belief that severe mental illness is chronic and that stability is the best one could hope for. They discovered there are multiple outcomes associated with severe mental illness and that many people did progress beyond a state of mere stability.
Research suggests that identification and pursuit of activities consistent with a person’s interests and learning ways to manage and minimize the destructive effects of the illness contribute to the process of recovering serious mental illness – over a period of weeks months, or years.
For example: a focus on learning how to live with auditory hallucinations appears to result in a decrease in their severity and frequency while simply waiting for the symptoms to disappear leaves a person inactive, isolated, and alone.
For example: The goal is not to be medication free, but to take the least amount necessary. Most persons with a psychiatric disorder indicate that medications are critical to their success.
Good news for School Nurses, Students and Parents
The Iowa Dept. of Public Health has
arranged for on-line “Suicide Prevention” training for school nurses statewide.
School nurses will be awarded one nationally-accredited Continuing Nursing Education (CNE) “contact hour” upon completion of each of the three K12 programs - At-Risk for Middle School Educators, At-Risk for High School Educators, and Step In, Speak Up.
The link to access the training is: http://iowa.kognito.com/ For more information, contact: Melissa Walker RN, School Nurse Consultant Bureau of Nutrition and Health Services Iowa Department of Education, Grimes State Office Building Des Moines, Iowa 50319 Office: 515-281-5327
Iowa Suicide Prevention Planning Group
The Iowa Suicide Prevention Planning Group first met in August and has been meeting monthly ever since. The group currently has three primary goals that can be summarized as: 1) Produce an updated Iowa Suicide Prevention Plan; 2) Provide recommendations for implementing the Plan and review it regularly; and 3) Provide guidance and direction to suicide prevention efforts in Iowa. The group has approximately 20 members. The updated plan should be complete by the end of the year.
The contact person for this project is Patrick McGovern Suicide Prevention and Iowa Youth Survey Coordinator Iowa Department of Public Health | Division of Behavioral Health 321 E. 12th Street | Des Moines, IA 50319 | Office: 515-281-5444 | [email protected]

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
11
Pushing Aside Daily Mental Health Triggers is Tough
www.healthyplace.com
An outsider may not understand how difficult it is to avoid and ignore the angry mental health triggers surrounding you. Those outsiders, especially those without mental illness, may not even understand
what a "trigger" really is.
In truth, everyone struggles with triggers; the elements of daily life that bring forward intense emotions and can sometimes lead to unsafe behaviors. These are things that everyone experiences – not just those with mental illness.
The question is: how do you push aside the mental health triggers that haunt your every move? The answer is not simple and depends on everyone's personal struggles and coping skills. For those who struggle with eating disorders, triggers can grow from the mere sight of food or a pound on the scale. For those who self-harm, any sharp object can trigger the urge to self-injure.
Since triggers are imprinted into everyday life, there really is no true way to avoid them. However, if you can find ways to replace those triggers with a positive activity or diversion, there is a greater possibility of successfully moving forward. You can use music or writing or being surrounded by supportive people as positive replacements. When those replacements are actively used, the mental health triggers may not affect you as much.
NAMI GDM highlights of October Activities
October newsletter emailed to 1800+, 2100+ mailed, 500 distributed to various venues and events
Newsletters and magazines to 4 area hospitals, crisis center and ICIW
NAMI family support groups meet in 4 locations 1X/month
NAMI Connections support groups meet in 2 locations weekly
2 Family to Family classes continue
Peer to Peer class continues
Basics class starts
Oct. 1-2 State Mental Health conference
Oct. 3 – Interview for AMOS Workforce Workgroup
Oct. 4 - NAMI Walks
Oct. 7 – AMOS Cluster meeting
Oct. 8 – Presentation at Easter Seals on crisis cards
Oct. 8 – NAMI GDM Board meeting
Oct. 9 – Presentation to NAMI P2P class
Oct. 10- IA Prevention of Disabilities Policy Council meeting
Oct. 10- Habilitation Services meeting for providers
Oct. 11 – AMOS meeting with both DM and Ames clusters
Oct. 14 – Star Bar House meeting
Oct 15 – Legislative workgroup
Oct. 16 – MHDS/IMHPC Commission meeting
Oct. 19 – AMOS Fall Summit Skit practice
Oct. 20 – AMOS Fall Summit
Oct. 20 – Presentation to AAUW
Oct. 21 – AMOS Workforce Workgroup meeting
Oct. 22 – Fifth Judicial District board Meeting
Oct. 23 – Systems IntegrationTaskforce meeting
Oct. 27 – AMOS MH and SA Workgroup meeting
Oct. 28 – House meetings at Central Iowa Shelter and Services and Broadlawns
Oct. 29 – Presentation to Family Support Group at Mercy First Step
World's Largest Law Enforcement Group Endorses Court-Ordered Outpatient
Treatment for At-Risk People with Severe Mental Illness
Treatment Advocacy Center – October 2014
The world’s largest law enforcement organization this week endorsed court-ordered treatment in the community for at-risk individuals with severe mental illness.
Voting at their annual convention in Florida, the International Association of Chiefs of Police (IACP) endorsed unanimously, the “authorization, implementation, appropriate funding, and consistent use of assisted outpatient treatment (AOT) laws to ensure treat-ment in the least restrictive setting possible for individuals whose illness prevents them from otherwise accessing such care voluntarily.” The IACP represents more than 20,000 members in more than 100 countries.
"AOT will help those who need help the most get the treatment they need, which will improve outcomes for this population and reduce the burden on law enforcement," said Chief of Police Richard Beary, IACP's president.
The IACP joins the National Sheriffs’ Association on record in support of AOT, which the U.S. Department of Justice has deemed an evidence-based practice for reducing crime and violence.
“Untreated severe mental illness is highly associated with arrest and incarceration,” said Chief of Police Michael Biasotti, a member of the Treatment Advocacy Center board of directors who championed the resolution. “A disproportionate number of these individuals are ending up in the criminal justice system when they should be receiving treatment.
“We expect AOT to reduce the burden of untreated severe mental illness on law enforcement and also produce taxpayer savings,” he said. “This tool will help increase law enforcement capacity and return the care of the most severely ill to the mental illness treatment system.”
Mental Health First Aid Instructors in Iowa
Statewide, there are 60 Adult Mental Health First Aid instructors. There are 22 Youth Mental Health First Aid instructors. To find the list of instructors – go to www.mentalhealthfirstaid.org/
In the Des Moines area – the next 8 hour Adult Mental Health First Aid class is being offered by
NAMI Greater Des Moines on the afternoons of Friday, Dec. 5 and Dec. 12 – 12:30 to 4:30 PM. A maximum of 25 people will be accepted into the class. To sign up, please contact [email protected]
What is Magellan Health?
Magellan Behavioral Care of Iowa has managed the Iowa Plan for Behavioral Health since 1995. The Iowa Plan serves most Medicaid recipients in the state. It offers a broad range of mental health and substance abuse services. This includes community services and supports.
The Iowa Department of Human Services (DHS) oversees the Iowa Plan for Medicaid-funded services. The Iowa Department of Public Health (IDPH) oversees the Iowa Plan for IDPH-funded substance abuse services.

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
12
For more about Magellan of Iowa and the Iowa Plan, please call (800) 638-8820 or (515) 223-0306 www.magellanofiowa.com
Magellan Health Services Program – Senior Connect
www.Magellaniowa.com
Senior Connect was developed by Magellan to address the issues of stigma, lack of understanding of the special needs of Older Adults 65+ enrolled in Medicaid with behavioral health needs and the need for collaboration among the various providers.
One of the major goals in transitioning the 65+ population to Magellan in the Iowa Plan was to increase the access to services that were not available to this population previously; services such as: Assertive Community Treatment, Peer Support, Intensive Psychiatric Rehabilitation, Community Support Services, and Mobile Counseling.
There is easy communication to access services for Enrollees 65 and older. Magellan has a dedicated information phone line—SeniorConnect Information Line—for Enrollees, family members, caregivers, primary care physicians, geriatricians, and other key stakeholders to have direct access to Magellan’s SeniorConnect team.
Contact George Dorsey for more information 1-800-638-8820 Ext. 85277 or email [email protected] or go to the website at: http://magellanofiowa.com/benefits-and-services-ia/senior-connect.aspx
Not So Modern Family
Nov. 4, 2014 | Rachel Ehmke|childmind.org
The era of asylums is long gone—they started closing in the US in the late 60s and 70s—but One Flew Over the Cuckoo's Nest-style psychiatric hospitals were alive and well in a recent episode of Modern Family.
It was the Halloween episode, and mom Claire Dunphy decorated her yard as a "haunted insane asylum" with her kids playing "deranged mental patients." One was chained to a hospital bed and another was wearing a straitjacket. She was dressed as a "sadistic nurse" and wanted her husband to be a "demented doctor."
Claire was thrilled with her decorations until she learned she upset a new neighbor who "spent six months in a cuckoo farm in Nevada." Later it's revealed the neighbors are just joking:
- "She's never been to a nut house!" - "Yeah, I ain't crazy!"
(By the way the neighbors are supposed to be ignorant Southern trailer trash-another worn out trope.)
It's all played for a joke, of course, but we're not finding it very funny.
Mental illness really is scary to a lot of people in this country. A large part of that fear is rooted in how our culture talks about mental health, and that certainly includes prime time television shows like this one. It's all the more frustrating because Modern Family has been widely lauded for its updated take on a traditional American family. Clearly their commitment to diversity only extends so far.
After watching the episode Liza Long, writer and mother who learned first-hand the cost of stigmatizing mental illness when her son developed bipolar disorder, wrote, "We talk a lot about the word 'stigma' when we talk about mental illness. But what we really mean is 'discrimination.' "
Blogger Pete Earley has written an open letter to Disney/ABC
protesting the episode, and Janine Francolini, founder of the Flawless Foundation, called it "a misguided, ignorant and prejudiced piece about people living with mental illness" in a blog on the Huffington Post.
In her blog Long also points out that one in five kids in the US will
have a serious psychiatric disorder at some point before age 18. A real modern family should acknowledge how common mental illness is-not use it as a tired punch line.
New Classes available for Persons in Recovery!
Mindfulness Workshop - No cost
Friday, January 9 from 10am until 2pm
Friends Meeting House, 4211 Grand Avenue, Des Moines
Limited to 15 individuals.
This workshop will be led by Emily Smith, LISW, Prairie Wellness.
For questions and to register, call Deborah Guthrie at Community Support Advocates, 515.883.1776, ext 328 or email [email protected].
Art/Poetry Workshop - No cost
This workshop is open to members of Integrated Health Homes in central Iowa. Depending on sign-up – persons in recovery who are not in Integrated Health Homes may be able to attend.
Classes are limited to 12 individuals.
Thursdays, January 8, 15, 22, 29 – 3 to 5 PM
ArtForceIowa, 319 SW 5th Street, Des Moines
This workshop will be provided by ArtForceIowa.
For questions and to register, call Deborah Guthrie at Community Support Advocates, 515.883.1776, ext 328 or email at [email protected]
An application to attend the class can be found at our website at https://www.namigdm.org/index.cfm?NodeID=36739&AudienceID=1&preview=1
Invitation to join Online Support Group for Parents of minor children with mental health needs:
Closed FaceBook Group: "NAMI IOWA's Casserole Club" or NICC (as in the nick of time!)
Please feel free to invite others to join - this group is limited to those in Iowa who are primary care givers to minor children with mental illness / brain disorder. It includes foster parents, grandparents, relatives, etc., that are involved in the daily care of the child. This is a safe place to find support and understanding. We are not "Casserole moms" - as they say - that is, when your child is seriously physically ill, it is common for neighbors, friends, and community members to bring casseroles, offer to help, etc. But when your child has a serious mental illness or mental health crisis, people often do not know how to respond and often simply don't. So let us be a casserole club - let us offer those needed kind words of encouragement and a listening ear. For more info, contact Tammy [email protected] 641-990-9974

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
13
NAMI GDM Educational Opportunities
Check out additional information on the education classes NAMI Greater Des Moines offers at www.namigdm.org - send an email to [email protected] or call 277-0672 for more information.
For Persons With Mental Illness Peer to Peer educational classes – 10 weeks WRAP – Wellness Recovery Action Planning – 12 hours Hearts and Minds – free on-line wellness course www.nami.org
For Family Members Family to Family educational classes – for family members of
adults with mental illness – 12 weeks Basics educational classes – for parents and caregivers of children
and adolescents with SMI – 6 weeks Homefront – for military family members – to be released soon!
Team Educational Offerings NAMI on Campus – [email protected] Raising Mental Health Awareness Among College Students Ending the Silence – presentations to high school students 30 Pearls of Wisdom in Treating a Person with MI -1 hour In Our Own Voice presentation- 1.5 hours – [email protected]
Hearing Voices that are Distressing – 2-3 hours Contact [email protected]
Video - Anderson Cooper Undergoes Hearing Voices http://www.mediaite.com/tv/anderson-cooper-undergoes-very-unpleasant-experiment-of-hearing-voices/
Parents and Teachers as Allies - 1.5 hours Provider education - 15 hours
Education for any person in the Community Mental Health First Aid – 8 hours- contact Teresa 274-6876
Presentations to Community organizations Resource tables at conferences and health fairs – contact Kay Kay at [email protected] or 252-0714
Specialized Training Part of planning team for Crisis Intervention Team training for
Des Moines Police Department
About Us Get Help Get Involved Resources FAQ’s News & Events Contact Us
Watch Our Video Message from the President
Board Members NAMI GDM Advisory Board NAMI Public Policy Standards of Excellence NAMI GDM Endow Iowa Fund
Crisis Information Do’s and Don’ts in a Crisis Illness Information
Support Groups Educational Opportunities Health Insurance Coverage Criminal Justice System Veterans Mental Health Parity Polk Co. Health Services and Provider List Become a Member
Legislation and Advocacy Volunteer Opportunties Anti-Stigma Efforts Faith Become a Member Donate
Iowa’s Mental Health System Local Resources NAMI Resources
Family Member Support Persons in Recovery
Peer Support Information School Resources Other Resources Related Files
What is a mental illness?
Who can get a mental illness?
What is the difference between a psychologist and a psychiatrist?
What is recovery?
Sign up for email Newsletters Press Releases Events Calendar
Event Videos
Mail Phone Website Email
Facebook Twitter
Please send a big THANK YOU to Cindy Gross and Plaza Printers for their assistance in printing our
newsletter - 6762 Douglas Avenue, Urbandale, IA 50322
Please send a big THANK YOU to the Ruby Van Meter students for their assistance in assembling our monthly
newsletter.
NAMI Greater Des Moines Board of Directors
Effective December 2014 President Teresa Bomhoff [email protected] 274-6876 Vice-Pres Jim Goodrich [email protected] 490-2758 Treasurer Regina Murphy [email protected] 277-0672 Secretary Gary Rasmussen 277-0672
[email protected] Board members
Terri Shipman [email protected] 277-0672 Dawn Hansen [email protected] 277-0672 Matthea Little Smith [email protected] 277-0672 Matt Connolly [email protected] 975-9600 Jen Wells [email protected] 277-0672 Sue Soriano [email protected] 277-0672 Brittany Peterson [email protected] 277-0672 Kathy Comito [email protected] 277-0672 Sherri Sinclair [email protected] 277-0672
At the Donate button, you can pay for a membership and/or make
a donation.
The newsletter can be sent by email or by mail. Sign up on the home page and enter your name to our database. Along with the
monthly newsletter, the following items will also be posted at the same location on our website:
An additional list of articles, magazines and videos from around the nation and world.
A chart of upcoming events around the community and state
Any informational flyers received for events
NAMI Greater Des Moines website: www.namigdm.org

www.namigdm.org (515) 277-0672 [email protected]
Find Help. Find Hope.
14
National Alliance on Mental Illness of Greater Des Moines Box 12174 Des Moines, Iowa 50312
RETURN SERVICE REQUESTED
How can you help individuals with mental illness and their families?
Tax Deductible Donations Become a member Dues of $35 or $3 (limited income) On-line at www.namigdm.org Or send a check payable to: NAMI Greater Des Moines
Box 12174 Des Moines, Iowa 50312 Our email is [email protected] Phone: 515-277-0672
We invite you to join us and volunteer for teaching, facilitating, committee and project work. Send an email to [email protected]
Have
NONPROFIT ORG. US POSTAGE PAID DES MOINES IA PERMIT NO. 34
Check NAMI GDM Facebook
https://www.facebook.com/NAMIGDM?ref=stream
Twitter @NAMIGreaterDSM
Ways to Donate to NAMI GDM
Cash Check Credit/Debit Card on-line at our website Through Employee Giving programs or Direct Donation programs NAMI GDM Endow Iowa Fund (see our website for more information – www.namigdm.org) NAMI Walks
We
Letters to the Editor
You are welcome to send letters to the editor by mail or E-mail. If you receive our newsletter by e-mail and would rather receive it by snail mail – or if you receive our newsletter by snail mail and would rather receive it by e-mail – communicate your preference to: Teresa Bomhoff, Box 12174, Des Moines, Iowa 50312 or E-mail: [email protected] or [email protected]
NAMI is composed of 3 levels of independently financed 501(c)(3) organizations- National, State affiliate (Iowa), and Local affiliate (NAMI GDM). If you would like to discontinue receiving the newsletter, please send an email to: [email protected] or [email protected] or call 277-0672 or 274-6876
50% of all lifetime cases of mental illness begin by age 14, 75% by age 24
13% of youth age 8-15 live with a mental illness to cause significant impairment in their day-to-day lives. This figure jumps to 21% in youth age 13-18.
Did you know that people who have experienced trauma are 3 times more likely to experience depression, 4 times more likely to abuse alcohol, and 15 times more
likely to attempt suicide?
Tuesday, Dec. 2 – Noon to 2 PM AMOS Community Conversation
38th & Grand, Central Presbyterian Church RSVP to [email protected]
Thursday, Dec. 4 – 6 to 8 PM
NAMI GDM Monthly Education meeting
“Trauma Informed Care” Plymouth Congregational Church 42nd and Ingersoll, Des Moines
Sunday, Dec. 7 – 2:30 to 4:30 PM NAMI Smarts Advocacy training
Iowa Lutheran Hospital, 700 E. University Ave. Des Moines – no cost
RSVP to [email protected]
Wed., Dec. 10 - NAMI GDM Bd Meeting
You are welcome to attend our Board meetings on the 2nd Wednesday of each
month – at Central Iowa Shelter & Services, 1420 Mulberry Street - 4:30 PM to 6 PM.
Happy Holidays! Happy
New Year!