Embed Size (px)
Citation preview
Debate: What’s the Best Way to Treat Obesity in Type 2 Diabetes? Lee M. Kaplan, MD, PhD Osama Hamdy, MD, PhD
Sunday, February 19, 2017 8:00 a.m. – 9:00 a.m.
Lee M. Kaplan, MD, PhD Despite multiple, concerted public health, behavioral and medical initiatives, effective prevention and durable control of obesity have proven elusive. Indeed, rates of obesity continue to rise worldwide, and no country or region has seen a significant, sustained reduction in either obesity prevalence or severity during the past several decades. Given its serious, pleiotropic effects on health, new strategies for prevention and treatment of obesity are needed. This is particularly true for patients with type 2 diabetes. In these patients, where obesity reduction is strongly beneficial for controlling the diabetes, most anti-obesity therapies are even less effective than in patients with normal glucose and lipid metabolism. One potential explanation for the limited effectiveness of most anti-obesity therapies is the heterogeneity of obesity itself. With several thousand genes and several hundred biological pathways contributing to the normal regulation of fat mass and body weight, it stands to reason that different defects in these regulatory systems may produce different subtypes of obesity. These different subtypes are manifest by distinct phenotypes, including differences in age of onset, body fat distribution, response to specific obesogenic environmental factors, associated comorbidities, and response to individual therapies. Optimizing outcomes in obesity treatment requires identifying the therapy or therapies that are most effective for an individual patient. With respect to diet-based treatments, many patients respond to a diet with fewer processed foods. For some, a low-carbohydrate or low-glycemic index diet is most effective, and for others, a fat-restricted diet yields better results. Similarly variable responses are seen to other lifestyle-based, pharmacological and surgical therapies for obesity. The key to optimizing clinical success comes in learning to apply each available therapeutic modality effectively, safely and confidently. Doing so will give each patient the greatest opportunity to receive the treatment that most closely matches their clinical need. Osama Hamdy, MD, PhD
Weight reduction through lifestyle modifications remains the cornerstone in preventing and managing type 2 diabetes among overweight and obese individuals. For a long time, physicians have been skeptical about the long-term maintenance of weight reduction—claiming that nonsurgical weight reduction is always temporary and is frequently followed by gradual weight regain to the starting baseline. Over the last 2 years, this view has been gradually changing. Recent clinical trials and novel clinical practice models showed that long-term maintenance of weight loss is not only possible but is also associated with significant long-term improvement in many of the metabolic and cardiovascular abnormities seen in patients with type 2 diabetes. Over the past 5 years, the introduction of several diabetes medications that induce satiety and reduce food intake (eg, glucagon-like peptide 1 analogues, SGLT-2 inhibitors and amylin analogues) gave clinicians several additional tools that allow them to help their patients in achieving better diabetes control without compromising their body weight Use of these medications in proper combinations can help patients with type 2 diabetes not only to lose weight but also to maintain the weight loss. The Why WAIT (Weight Achievement and Intensive Treatment) program showed that it is possible for patients with obesity and diabetes to maintain weight reduction for up to 5 years in real-world clinical practice. On contrary, data from bariatric surgery mainly came from poorly designed studies with a smaller number of participants and for
relatively shorter duration. Variable definition of diabetes remission as shown in surgical intervention studies falsely augmented their results and misled physicians and patients. Cost-effectiveness and safety of bariatric surgeries for obesity management in diabetes are questionable. References: 1. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, Nathan
DM; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346 (6):393–403.
2. Nathan DM, Buse JB, Davidson MB, et al. Medical Management of Hyperglycemia in Type 2 Diabetes: A Consensus Algorithm for the Initiation and Adjustment of Therapy. Diabetes Care 2008;31 (12):1–11.
3. Mitri J, Hamdy O. Diabetes medications and body weight. Expert Opin Drug Saf. 2009;8(5):573–84
4. Hamdy O, Carver C. The Why WAIT program: improving clinical outcomes through weight management in type 2 diabetes. Curr Diab Rep. 2008;8(5):413–20
5. Hamdy O, Mottalib A, Morsi A, El-Sayed N, Goebel-Fabbri A, Arathuzik G, Shahar J, Kirpitch A, Zrebiec J. Long-term effect of intensive lifestyle intervention on cardiovascular risk factors in patients with diabetes in real-world clinical practice: a 5-year longitudinal study. BMJ Open Diabetes Res Care. 2017;5(1):e000259.
64th ADA Postgraduate Course
Treatment of Type 2 Diabetes Mellitus:Medical and Surgical Options
Lee M. Kaplan, MD, PhD
Obesity, Metabolism & Nutrition InstituteMassachusetts General HospitalHarvard Medical School
February 19, 2017Fernando Botero, 1932-
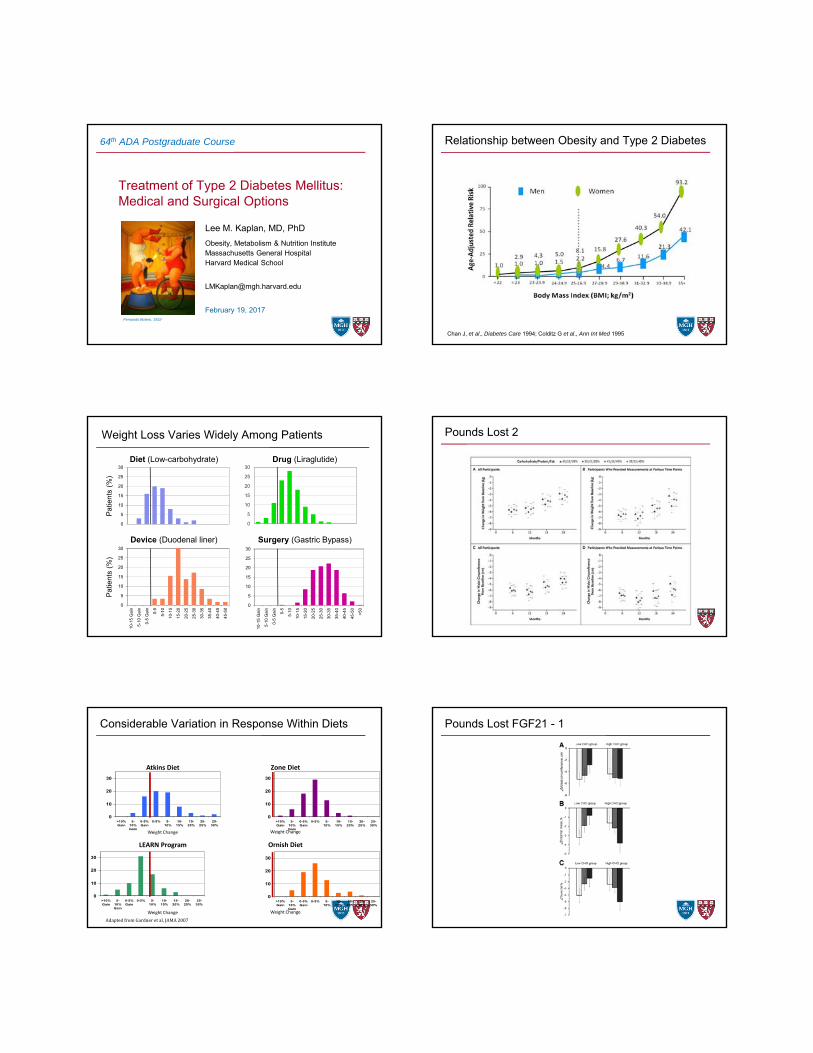
Relationship between Obesity and Type 2 Diabetes
Chan J, et al., Diabetes Care 1994; Colditz G et al., Ann Int Med 1995
0
5
10
15
20
25
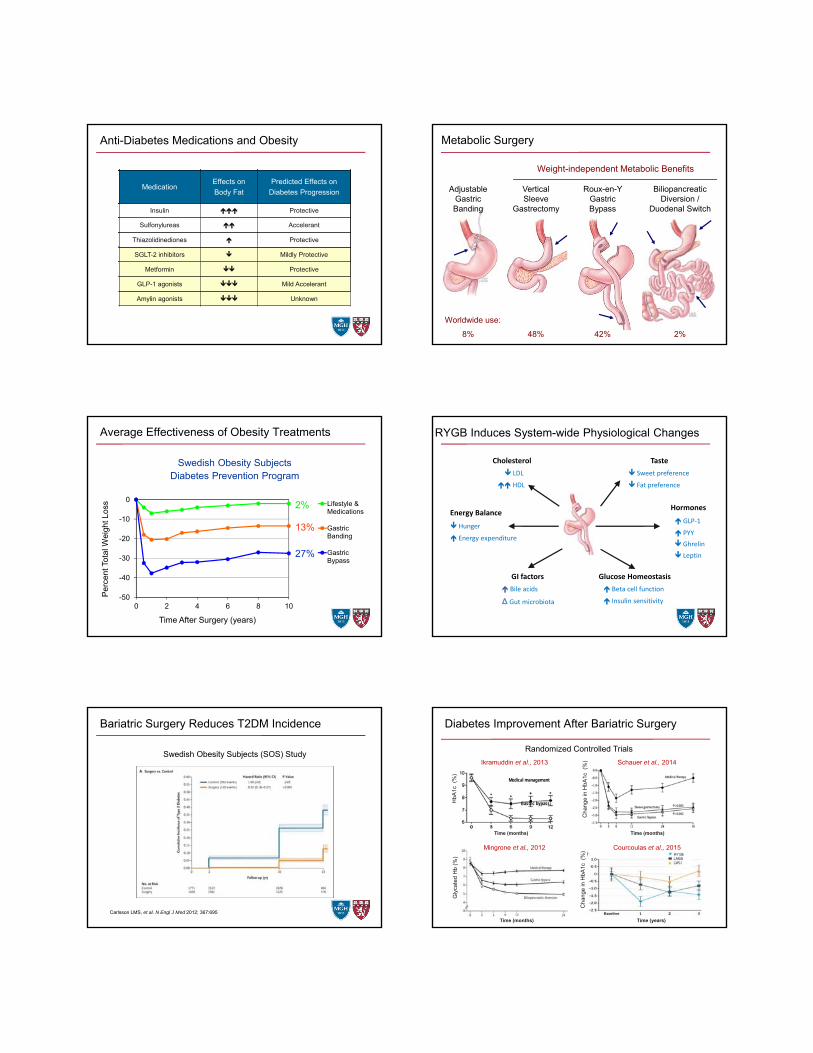
30Drug (Liraglutide)
Weight Loss Varies Widely Among Patients
0
5
10
15
20
25
30
Diet (Low-carbohydrate)
Surgery (Gastric Bypass)Device (Duodenal liner)
0
5
10
15
20
25
30
10-1
5 G
ain
5-10
Gai
n
0-5
Gai
n
0-5
5-10
10-1
5
15-2
0
20-2
5
25-3
0
30-3
5
35-4
0
40-4
5
45-5
0
0
5
10
15
20
25
30
10-1
5 G
ain
5-10
Gai
n
0-5
Gai
n
0-5
5-10
10-1
5
15-2
0
20-2
5
25-3
0
30-3
5
35-4
0
40-4
5
45-5
0
>50
Pat
ien
ts (
%)
Pat
ient
s (%
)
Pounds Lost 2
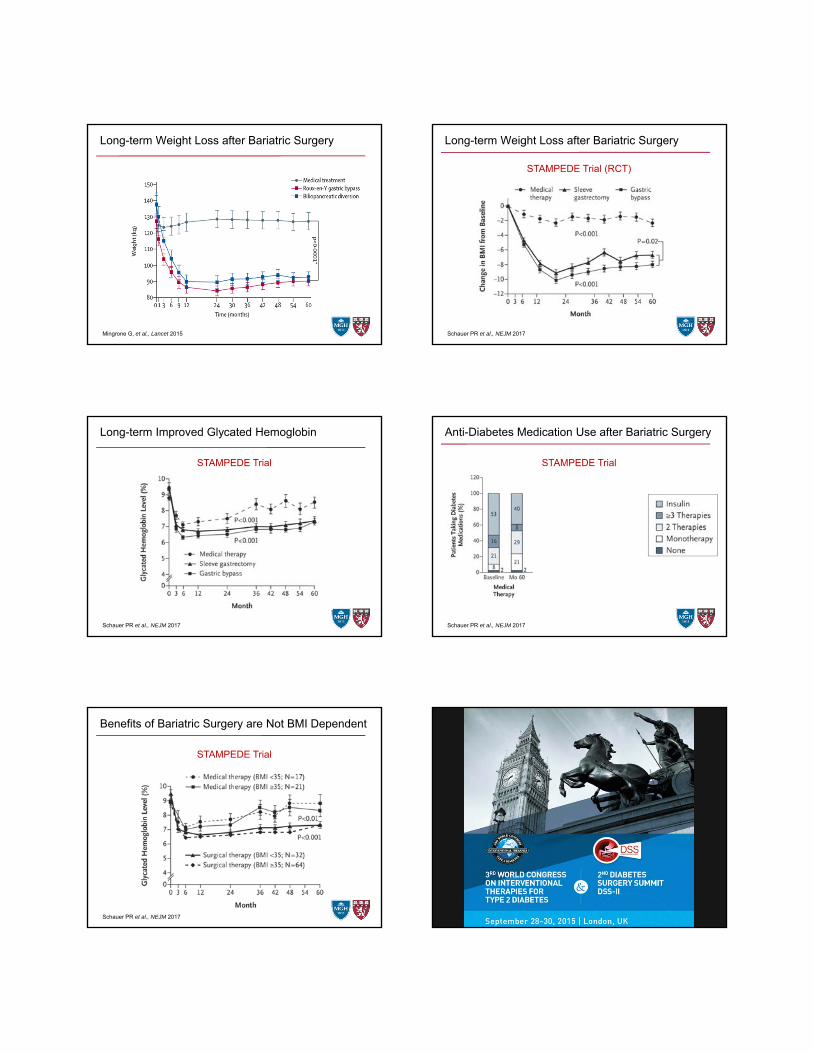
Considerable Variation in Response Within Diets
Zone DietAtkins Diet
0
10
20
30
>10%Gain
5-10%Gain
0-5%Gain
0-5% 5-10%
10-15%
15-20%
20-25%
25-30%
0
10
20
30
>10%Gain
5-10%Gain
0-5%Gain
0-5% 5-10%
10-15%
15-20%
20-25%
25-30%
0
10
20
30
>10%Gain
5-10%Gain
0-5%Gain
0-5% 5-10%
10-15%
15-20%
20-25%
25-30%
0
10
20
30
>10%Gain
5-10%Gain
0-5%Gain
0-5% 5-10%
10-15%
15-20%
20-25%
25-30%
LEARN Program Ornish Diet
Weight Change Weight Change
Weight Change Weight Change
AdaptedfromGardneretal,JAMA2007
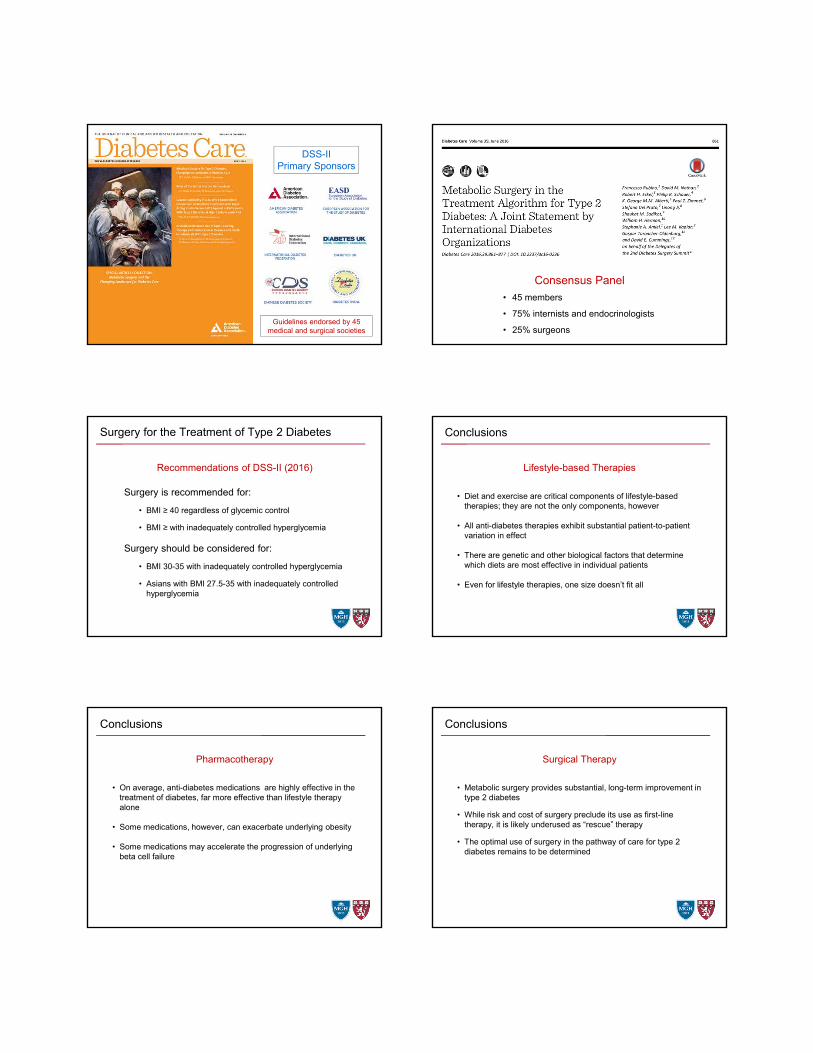
Pounds Lost FGF21 - 1
Anti-Diabetes Medications and Obesity
MedicationEffects on
Body Fat
Predicted Effects on
Diabetes Progression
Insulin Protective
Sulfonylureas Accelerant
Thiazolidinediones Protective
SGLT-2 inhibitors Mildly Protective
Metformin Protective
GLP-1 agonists Mild Accelerant
Amylin agonists Unknown
MedicationEffects on
Body Fat
Predicted Effects on
Diabetes Progression
Insulin Protective
Sulfonylureas Accelerant
Thiazolidinediones Protective
SGLT-2 inhibitors Mildly Protective
Metformin Protective
GLP-1 agonists Mild Accelerant
MedicationEffects on
Body Fat
Predicted Effects on
Diabetes Progression
Insulin Protective
Sulfonylureas Accelerant
Thiazolidinediones Protective
SGLT-2 inhibitors Mildly Protective
Metformin Protective
MedicationEffects on
Body Fat
Predicted Effects on
Diabetes Progression
Insulin Protective
Sulfonylureas Accelerant
Thiazolidinediones Protective
SGLT-2 inhibitors Mildly Protective
MedicationEffects on
Body Fat
Predicted Effects on
Diabetes Progression
Insulin Protective
Sulfonylureas Accelerant
Thiazolidinediones Protective
MedicationEffects on
Body Fat
Predicted Effects on
Diabetes Progression
Insulin Protective
Sulfonylureas Accelerant
MedicationEffects on
Body Fat
Predicted Effects on
Diabetes Progression
Insulin Protective
MedicationEffects on
Body Fat
Predicted Effects on
Diabetes Progression
Metabolic Surgery
VerticalSleeve
Gastrectomy
Roux-en-Y GastricBypass
Weight-independent Metabolic Benefits
Adjustable GastricBanding
Biliopancreatic Diversion /
Duodenal Switch
8% 48% 42% 2%
Worldwide use:
Average Effectiveness of Obesity Treatments
-50
-40
-30
-20
-10
0
0 2 4 6 8 10
Per
cent
Tot
al W
eigh
t Los
s
Time After Surgery (years)
Lifestyle &Medications
GastricBanding
GastricBypass
Swedish Obesity SubjectsDiabetes Prevention Program
2%
13%
27%
RYGB Induces System-wide Physiological Changes
LDL
HDL
Cholesterol
Hunger
Energy expenditure
Energy Balance
Bile acids
∆ Gut microbiota
GI factors
Sweet preference
Fat preference
Taste
GLP‐1
PYY
Hormones
Ghrelin
Leptin
Beta cell function
Insulin sensitivity
Glucose Homeostasis
Bariatric Surgery Reduces T2DM Incidence
Carlsson LMS, et al. N Engl J Med 2012; 367:695
Swedish Obesity Subjects (SOS) Study
Diabetes Improvement After Bariatric Surgery
Cha
nge
in H
bA1c
(%
)C
han
ge in
HbA
1c (
%)
Time (months)
Time (years)
Schauer et al., 2014
Courcoulas et al., 2015
HbA
1c (
%)
Medical management
Gastric bypass
Time (months)
Ikramuddin et al., 2013
Gly
cate
d H
b (%
)
Time (months)
Mingrone et al., 2012
Randomized Controlled Trials
Long-term Weight Loss after Bariatric Surgery
Mingrone G, et al., Lancet 2015
Long-term Weight Loss after Bariatric Surgery
Schauer PR et al., NEJM 2017
STAMPEDE Trial (RCT)
Long-term Improved Glycated Hemoglobin
Schauer PR et al., NEJM 2017
STAMPEDE Trial
Anti-Diabetes Medication Use after Bariatric Surgery
Schauer PR et al., NEJM 2017
STAMPEDE Trial
Months Following Randomization
Benefits of Bariatric Surgery are Not BMI Dependent
Schauer PR et al., NEJM 2017
STAMPEDE Trial
DSS-IIPrimary Sponsors
Guidelines endorsed by 45 medical and surgical societies
Consensus Panel
• 45 members
• 75% internists and endocrinologists
• 25% surgeons
Surgery for the Treatment of Type 2 Diabetes
Surgery is recommended for:
• BMI ≥ 40 regardless of glycemic control
• BMI ≥ with inadequately controlled hyperglycemia
Surgery should be considered for:
• BMI 30-35 with inadequately controlled hyperglycemia
• Asians with BMI 27.5-35 with inadequately controlled hyperglycemia
Recommendations of DSS-II (2016)
Conclusions
• Diet and exercise are critical components of lifestyle-based therapies; they are not the only components, however
• All anti-diabetes therapies exhibit substantial patient-to-patient variation in effect
• There are genetic and other biological factors that determine which diets are most effective in individual patients
• Even for lifestyle therapies, one size doesn’t fit all
Lifestyle-based Therapies
Conclusions
• On average, anti-diabetes medications are highly effective in the treatment of diabetes, far more effective than lifestyle therapy alone
• Some medications, however, can exacerbate underlying obesity
• Some medications may accelerate the progression of underlying beta cell failure
Pharmacotherapy
Conclusions
• Metabolic surgery provides substantial, long-term improvement in type 2 diabetes
• While risk and cost of surgery preclude its use as first-line therapy, it is likely underused as “rescue” therapy
• The optimal use of surgery in the pathway of care for type 2 diabetes remains to be determined
Surgical Therapy
Conclusions
• Lifestyle, medical and surgical care for both obesity and type 2 diabetes should be viewed as cooperative, not competitive, approaches
• New patient care models that promote integrated pathways and shared medical and surgical responsibility for care within those pathways (including post-operative care) should be encouraged
• Use and optimization of combination therapies that employ all available approaches need to be supported and further evaluated
Coordinated Care
Clinical Data Evaluation – A Serial Approach
• Statistical significance
• Effect size
• Number needed to treat
• Durability of effect
• Risk-benefit profile
• Cost-benefit profile
64th ADA Postgraduate Course
Treatment of Type 2 Diabetes Mellitus:Medical and Surgical Options
Lee M. Kaplan, MD, PhD
Obesity, Metabolism & Nutrition InstituteMassachusetts General HospitalHarvard Medical School
February 19, 2017Fernando Botero, 1932-
The Best Management of Obesity in Type 2
Diabetes
Osama Hamdy, MD, PhD, FACE
Medical Director, Obesity Clinical Program,Director of Inpatient Diabetes Management,Joslin Diabetes CenterHarvard Medical School Boston, USA
Evolution of History
2017 B.C. 2017 A.C.
After Weight-Loss Surgery, a Year of Joys and DisappointmentsEven as the pounds fell away and their health improved, two patientscontended with the feeling that life hadn’t changed as much as they’d hoped.
After Weight-Loss Surgery, a Year of Joys and DisappointmentsEven as the pounds fell away and their health improved, two patientscontended with the feeling that life hadn’t changed as much as they’d hoped.
December 27, 2016
September 11, 2016
Before You Spend $26,000 on Weight-Loss Surgery, Do ThisThe old-fashioned way to treat diabetes. It is cheaper than weight-loss surgery. And probably more effective
We are in agreement
1- Anti-obesity medications are effective for weight reduction2- Bariatric surgeries are indicated for patients with very high BMI (Class III obesity)3- Gastroscopic procedures are promising
Lorcaserin in yr 1, placebo in yr 2
Placebo yr 1 and 2
102
98
96
90
0
Body Weight (Kg)
0
Study Week
8 16 24 32 40 48 56
92
94
100
Lorcaserin in yr 1 and 2
64 72 80 88 96 104
Year 1 Year 2
Average 1-year weight loss is 5.8 kg
Placebo 2.2 Kg (p<0.001)
55.4% on lorcaserin
45.1% on placebo completed year 1
Results of Bariatric Surgery
Is this true?
Is this true?
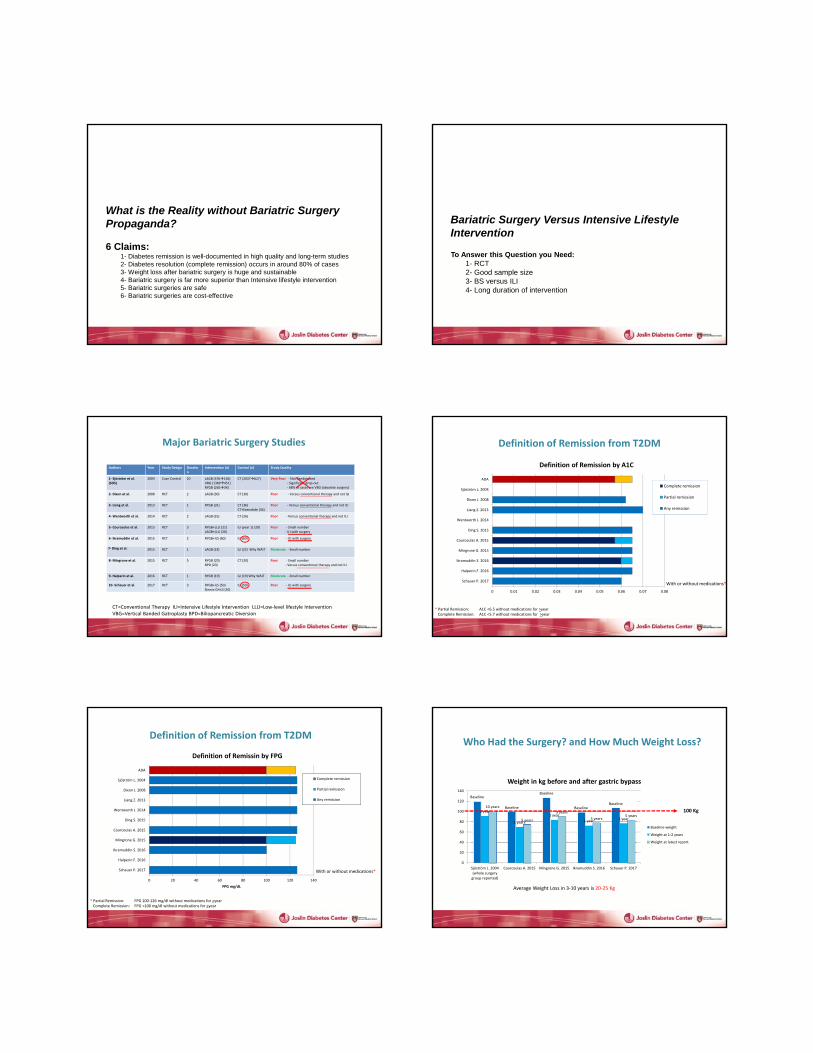
What is the Reality without Bariatric Surgery Propaganda?
6 Claims:1- Diabetes remission is well-documented in high quality and long-term studies2- Diabetes resolution (complete remission) occurs in around 80% of cases3- Weight loss after bariatric surgery is huge and sustainable4- Bariatric surgery is far more superior than Intensive lifestyle intervention5- Bariatric surgeries are safe6- Bariatric surgeries are cost-effective
Bariatric Surgery Versus Intensive Lifestyle Intervention
To Answer this Question you Need:1- RCT2- Good sample size3- BS versus ILI4- Long duration of intervention
Authors Year Study Design Duration
Intervention (n) Control (n) Study Quality
1‐ Sjöström et al. (SOS)
2004 Case‐Control 10 LAGB (376156)VBG (1369451)RYGB (26534)
CT (2037627) Very Poor ‐ Not Randomized‐ Significant drop‐out‐ 68% of cases are VBG (obsolete surgery)
2‐ Dixon et al. 2008 RCT 2 LAGB (30) CT (30) Poor ‐ Versus conventional therapy and not ILI
3‐ Liang et al. 2013 RCT 1 RYGB (31) CT (36)CT+Exenatide (34)
Poor ‐ Versus conventional therapy and not ILI
4‐Wentworth et al. 2014 RCT 2 LAGB (25) CT (26) Poor ‐ Versus conventional therapy and not ILI
5‐ Courcoulas et al. 2015 RCT 3 RYGB+LLLI (21)LAGB+LLLI (20)
ILI (year 1) (20) Poor ‐ Small number‐ ILI with surgery
6‐ Ikramuddin et al. 2015 RCT 2 RYGB+ILS (60) ILI (60) Poor ‐ ILI with surgery
7‐ Ding et al. 2015 RCT 1 LAGB (23) ILI (22) Why WAIT Moderate ‐ Small number
8‐Mingrone et al. 2015 RCT 5 RYGB (20)BPD (20)
CT (20) Poor ‐ Small number‐ Versus conventional therapy and not ILI
9‐ Halperin et al. 2016 RCT 1 RYGB (19) ILI (19) Why WAIT Moderate ‐ Small number
CT=Conventional Therapy ILI=Intensive Lifestyle Intervention LLLI=Low‐level lifestyle Intervention VBG=Vertical Banded Gatroplasty BPD=Biliopancreatic Diversion
Major Bariatric Surgery Studies
10‐ Schauer et al. 2017 RCT 3 RYGB+ILS (50)Sleeve G+ILS (50)
ILI (50) Poor ‐ ILI with surgery
Definition of Remission from T2DM
0 0.01 0.02 0.03 0.04 0.05 0.06 0.07 0.08
Schauer P. 2017
Halperin F. 2016
Ikramuddin S. 2016
Mingrone G. 2015
Courcoulas A. 2015
Ding S. 2015
Wentworth J. 2014
Liang Z. 2013
Dixon J. 2008
Sjöström L. 2004
ADA
Definition of Remission by A1C
Complete remission
Partial remission
Any remission
With or without medications*
* Partial Remission: A1C <6.5 without medications for >yearComplete Remission: A1C <5.7 without medications for >year
Definition of Remission from T2DM
0 20 40 60 80 100 120 140
Schauer P. 2017
Halperin F. 2016
Ikramuddin S. 2016
Mingrone G. 2015
Courcoulas A. 2015
Ding S. 2015
Wentworth J. 2014
Liang Z. 2013
Dixon J. 2008
Sjöström L. 2004
ADA
FPG mg/dL
Definition of Remissin by FPG
Complete remission
Partial remission
Any remission
* Partial Remission: FPG 100‐126 mg/dl without medications for >yearComplete Remission: FPG <100 mg/dl without medications for >year
With or without medications*
Who Had the Surgery? and How Much Weight Loss?
Baseline
Baseline
Baseline
BaselineBaseline
2 year
1 years
1 year
1 year 1 year
10 years
5 years
3 years
5 years5 years
0
20
40
60
80
100
120
140
Sjöström L. 2004(whole surgerygroup reported)
Courcoulas A. 2015 Mingrone G. 2015 Ikramuddin S. 2016 Schauer P. 2017
Weight in kg before and after gastric bypass
Baseline weight
Weight at 1‐2 years
Weight at latest report
100 Kg
Average Weight Loss in 3‐10 years is 20‐25 Kg
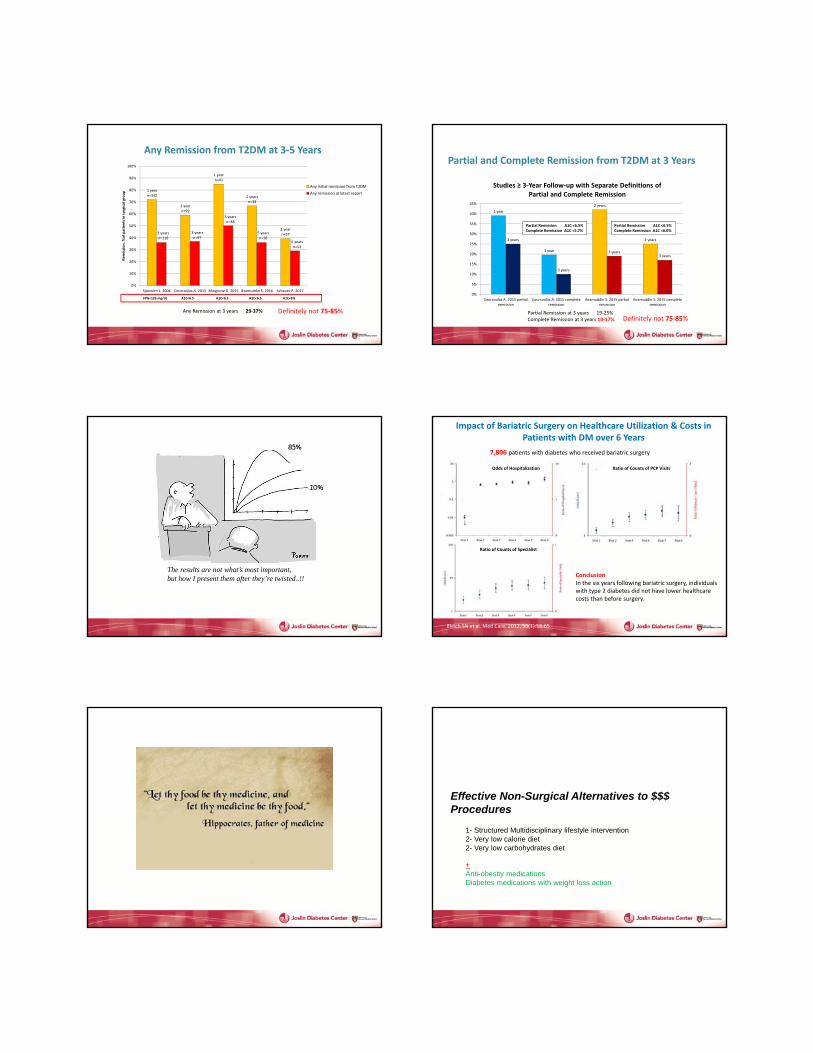
Any Remission from T2DM at 3‐5 Years
1 yearn=342
1 yearn=99
1 yearn=41
2 yearsn=38
1 yearn=573 years
n=118
3 yearsn=97
3 yearsn=38
5 yearsn=38
5 yearsn=53
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Sjöström L. 2004 Courcoulas A. 2015 Mingrone G. 2015 Ikramuddin S. 2016 Schauer P. 2017
Remission, %of patients in surgical group
Any initial remission from T2DM
Any remission at latest report
FPG<126 mg/dL A1C<6.5 A1C<6.5 A1C<6.5 A1C<6%
Any Remission at 3 years 29‐37% Definitely not 75‐85%
Partial and Complete Remission from T2DM at 3 Years
1 year
1 year
2 years
2 years3 years
3 years
3 years3 years
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Courcoulas A. 2015 partialremission
Courcoulas A. 2015 completeremission
Ikramuddin S. 2015 partialremission
Ikramuddin S. 2015 completeremission
Studies ≥ 3‐Year Follow‐up with Separate Definitions of Partial and Complete Remission
Partial Remission A1C <6.5%Complete Remission A1C <5.7%
Partial Remission A1C <6.5%Complete Remission A1C <6.0%
Partial Remission at 3 years 19‐25%Complete Remission at 3 years 10‐17% Definitely not 75‐85%
The results are not what’s most important, but how I present them after they’re twisted..!!
10%
85%
Impact of Bariatric Surgery on Healthcare Utilization & Costs in Patients with DM over 6 Years
Odds of Hospitalization Ratio of Counts of PCP Visits
Ratio of Counts of Specialist
ConclusionIn the six years following bariatric surgery, individuals with type 2 diabetes did not have lower healthcare costs than before surgery.
Bleich SN et al. Med Care. 2012, 50(1):58‐65
7,806 patients with diabetes who received bariatric surgery
Effective Non-Surgical Alternatives to $$$ Procedures
1- Structured Multidisciplinary lifestyle intervention2- Very low calorie diet2- Very low carbohydrates diet
+Anti-obesity medicationsDiabetes medications with weight loss action
Effective Non-Surgical Alternatives to $$$ Procedures
1- Structured Multidisciplinary lifestyle intervention2- Very low calorie diet2- Very low carbohydrates diet
+Anti-obesity medicationsDiabetes medications with weight loss action
Structured Multidisciplinary ILI
Why WAIT
Why WAIT ProgramLook AHEAD Study
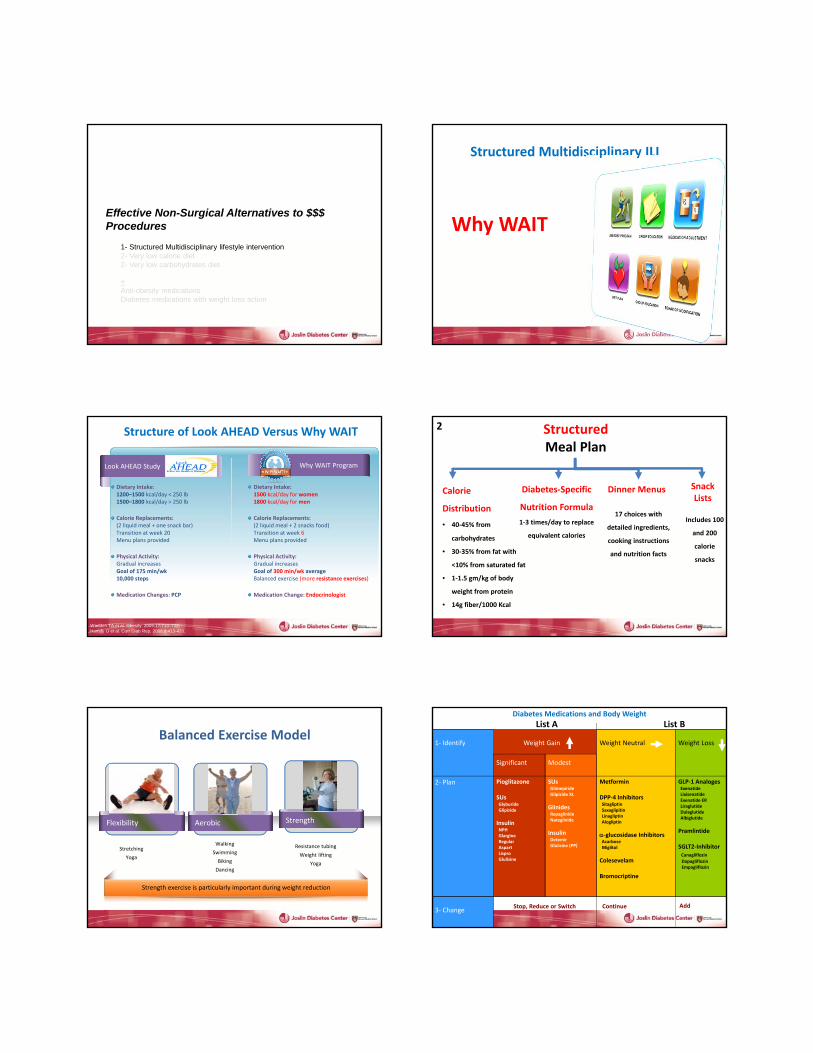
Structure of Look AHEAD Versus Why WAIT
Wadden TA et al. Obesity. 2009;17:713–722.Hamdy O et al. Curr Diab Rep. 2008;8:413-420.
Dietary Intake:1200–1500 kcal/day < 250 lb1500–1800 kcal/day > 250 lb
Calorie Replacements:(2 liquid meal + one snack bar)Transition at week 20Menu plans provided
Physical Activity:Gradual increasesGoal of 175 min/wk10,000 steps
Medication Changes: PCP
Dietary Intake:1500 kcal/day for women1800 kcal/day for men
Calorie Replacements:(2 liquid meal + 2 snacks food)Transition at week 6Menu plans provided
Physical Activity:Gradual increasesGoal of 300 min/wk averageBalanced exercise (more resistance exercises)
Medication Change: Endocrinologist
StructuredMeal Plan
Calorie
Distribution
• 40‐45% from
carbohydrates
• 30‐35% from fat with
<10% from saturated fat
• 1‐1.5 gm/kg of body
weight from protein
• 14g fiber/1000 Kcal
2
SnackLists
Dinner MenusDiabetes‐Specific
Nutrition Formula
1‐3 times/day to replace
equivalent calories
Includes 100
and 200
calorie
snacks
17 choices with
detailed ingredients,
cooking instructions
and nutrition facts
Balanced Exercise Model
Flexibility Strength
Strength exercise is particularly important during weight reduction
Aerobic
Walking
Swimming
Biking
Dancing
Resistance tubing
Weight lifting
Yoga
Stretching
Yoga
Diabetes Medications and Body Weight
Weight Gain Weight Neutral Weight Loss
Significant Modest
Pioglitazone
SUsGlyburideGlipizide
InsulinNPHGlargineRegularAspartLisproGlulisine
SUsGlimepirideGlipizide XL
GlinidesRepaglinideNateglinide
InsulinDetemirGlulisine (PP)
Metformin
DPP‐4 InhibitorsSitagliptinSaxaglipitinLinagliptinAlogliptin
‐glucosidase InhibitorsAcarboseMiglitol
Colesevelam
Bromocriptine
GLP‐1 AnalogesExenatideLixisenatideExenatide ERLiraglutideDulaglutideAlbiglutide
Pramlintide
SGLT2‐InhibitorCanagliflozin
DapagliflozinEmpagliflozin
Stop, Reduce or Switch Continue Add
1‐ Identify
2‐ Plan
3‐ Change
List A List B
‐16.0
‐14.0
‐12.0
‐10.0
‐8.0
‐6.0
‐4.0
‐2.0
0.0
0 3M 6M 9M 12M 15M 18M 21M 24M 27M 30M 33M 36M 39M 42M 45M 48M 51M 54M 57M 60M
***
*** ***
***
******
*** *** *** *** *** *** *** *** *** *** *** ***
Weight Loss (%)
Duration in Months
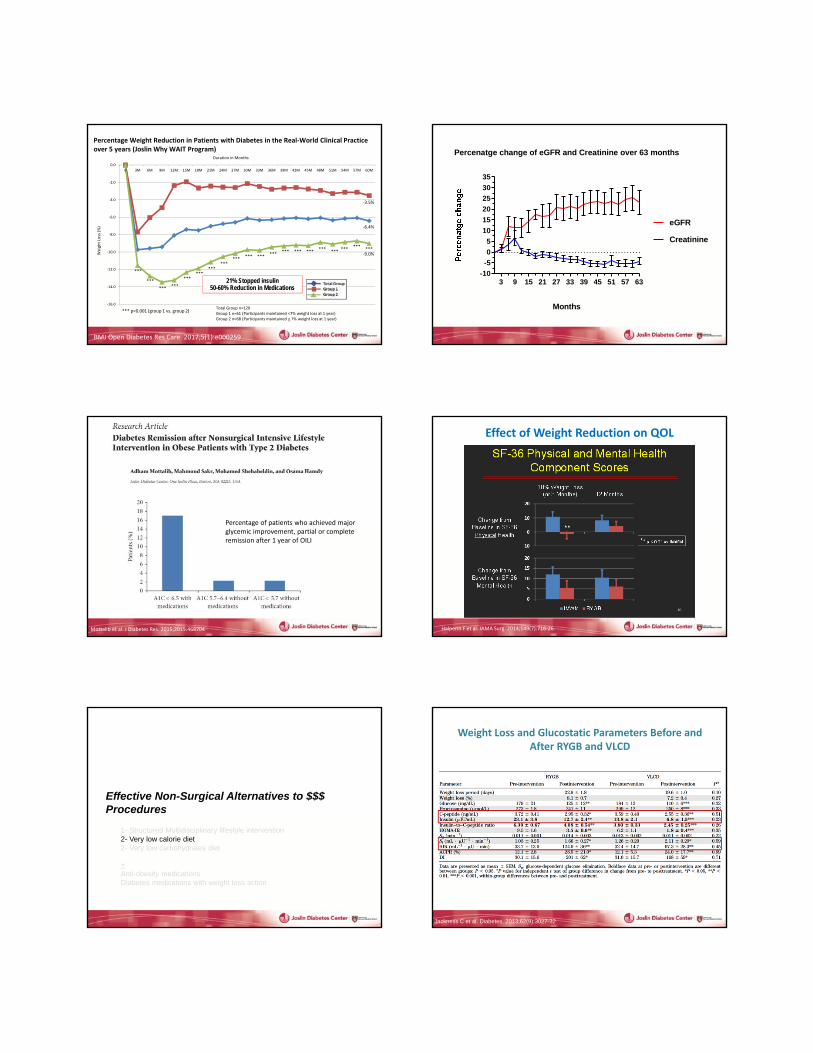
Total Group n=129Group 1 n=61 (Participants maintained <7% weight loss at 1 year)Group 2 n=68 (Participants maintained > 7% weight loss at 1 year)
*** p<0.001 (group 1 vs. group 2)
*** ***
‐9.0%
‐3.5%
‐6.4%
Percentage Weight Reduction in Patients with Diabetes in the Real‐World Clinical Practice over 5 years (Joslin Why WAIT Program)
21% Stopped insulin50-60% Reduction in Medications
BMJ Open Diabetes Res Care. 2017;5(1):e000259
3 9 15 21 27 33 39 45 51 57 63-10
-5
0
5
10
15
20
25
30
35
Percenatge change of eGFR and Creatinine over 63 months
Months
Creatinine
eGFR
Percentage of patients who achieved major glycemic improvement, partial or complete remission after 1 year of OILI
Mottalib et al. J Diabetes Res. 2015;2015:468704
Effect of Weight Reduction on QOL
Halperin F et al. JAMA Surg. 2014;149(7):716‐26.
Effective Non-Surgical Alternatives to $$$ Procedures
1- Structured Multidisciplinary lifestyle intervention2- Very low calorie diet2- Very low carbohydrates diet
+Anti-obesity medicationsDiabetes medications with weight loss action
Weight Loss and Glucostatic Parameters Before and After RYGB and VLCD
Jackness C et al. Diabetes. 2013;62(9):3027-32
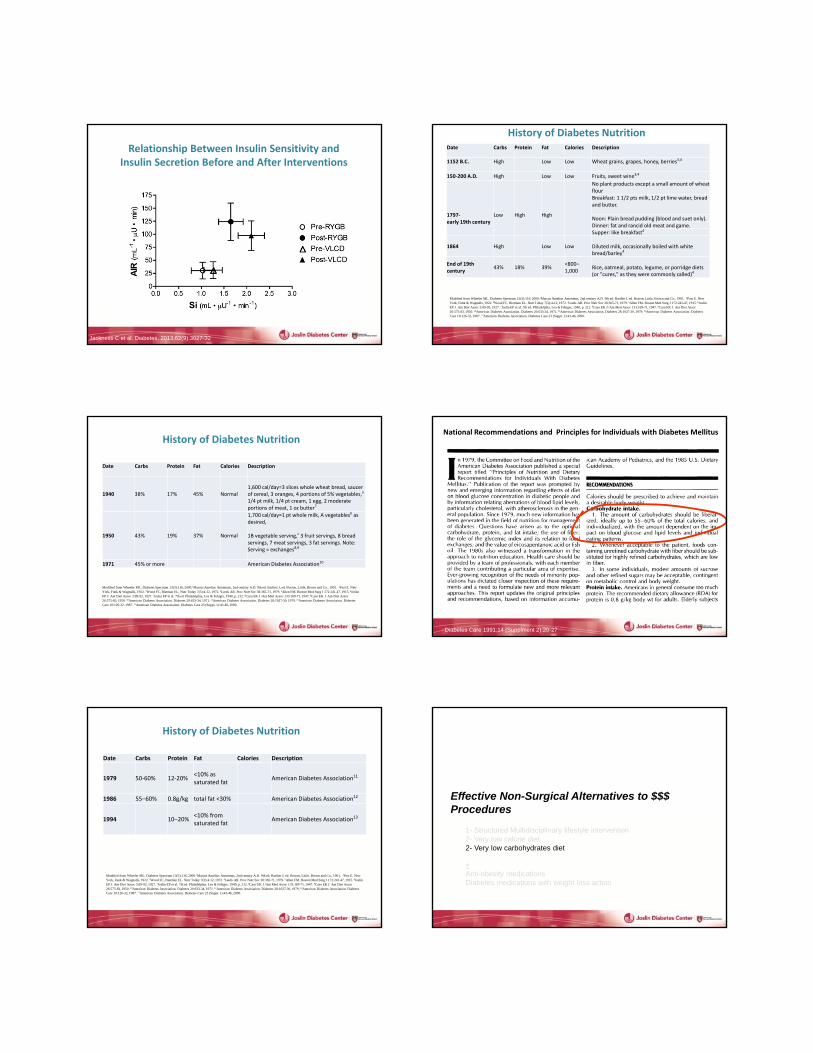
Relationship Between Insulin Sensitivity and Insulin Secretion Before and After Interventions
Jackness C et al. Diabetes. 2013;62(9):3027-32
Date Carbs Protein Fat Calories Description
1152 B.C. High Low Low Wheat grains, grapes, honey, berries3,4
150‐200 A.D. High Low Low Fruits, sweet wine3,4
1797‐early 19th century
Low High High
No plant products except a small amount of wheat flourBreakfast: 1 1/2 pts milk, 1/2 pt lime water, bread and butter.
Noon: Plain bread pudding (blood and suet only). Dinner: fat and rancid old meat and game. Supper: like breakfast4
1864 High Low Low Diluted milk, occasionally boiled with white bread/barley4
End of 19th century
43% 18% 39%<800–1,000
Rice, oatmeal, potato, legume, or porridge diets (or "cures," as they were commonly called)4
Modified from Wheeler ML. Diabetes Spectrum 13(3):116, 2000.1Marcus Aurelius Antoninus, 2nd century A.D. 9th ed. Bartlett J, ed. Boston, Little, Brown and Co., 1901. 2Post E. New York, Funk & Wagnalls, 1922. 3Wood FC, Bierman EL. Nutr Today 7(3):4-12, 1972. 4Leeds AR. Proc Nutr Soc 38:365-71, 1979. 5Allen FM. Boston Med Surg J 172:241-47, 1915. 6Joslin EP J. Am Diet Assoc 3:89-92, 1927. 7Joslin EP et al. 7th ed. Philadelphia, Lea & Febiger, 1940, p. 212. 8Caso EK J /Am Med Assoc 133:169-71, 1947. 9Caso EK J. Am Diet Assoc26:575-83, 1950. 10American Diabetes Association. Diabetes 20:633-34, 1971. 11American Diabetes Association. Diabetes 28:1027-30, 1979. 12American Diabetes Association. Diabetes Care 10:126-32, 1987. 13American Diabetes Association. Diabetes Care 23 (Suppl. 1):43-46, 2000.
History of Diabetes Nutrition
Date Carbs Protein Fat Calories Description
1940 38% 17% 45% Normal1,600 cal/day=3 slices whole wheat bread, saucer of cereal, 3 oranges, 4 portions of 5% vegetables,a
1/4 pt milk, 1/4 pt cream, 1 egg, 2 moderate portions of meat, 1 oz butter7
1950 43% 19% 37% Normal
1,700 cal/day=1 pt whole milk, A vegetablesb as desired,
1B vegetable serving,c 3 fruit servings, 8 bread servings, 7 meat servings, 3 fat servings. Note: Serving = exchanges8,9
1971 45% or more American Diabetes Association10
Modified from Wheeler ML. Diabetes Spectrum 13(3):116, 2000.1Marcus Aurelius Antoninus, 2nd century A.D. 9th ed. Bartlett J, ed. Boston, Little, Brown and Co., 1901. 2Post E. New York, Funk & Wagnalls, 1922. 3Wood FC, Bierman EL. Nutr Today 7(3):4-12, 1972. 4Leeds AR. Proc Nutr Soc 38:365-71, 1979. 5Allen FM. Boston Med Surg J 172:241-47, 1915. 6Joslin EP J. Am Diet Assoc 3:89-92, 1927. 7Joslin EP et al. 7th ed. Philadelphia, Lea & Febiger, 1940, p. 212. 8Caso EK J /Am Med Assoc 133:169-71, 1947. 9Caso EK J. Am Diet Assoc26:575-83, 1950. 10American Diabetes Association. Diabetes 20:633-34, 1971. 11American Diabetes Association. Diabetes 28:1027-30, 1979. 12American Diabetes Association. Diabetes Care 10:126-32, 1987. 13American Diabetes Association. Diabetes Care 23 (Suppl. 1):43-46, 2000.
History of Diabetes Nutrition
Diabetes Care 1991;14 (Supplment 2):20-27
National Recommendations and Principles for Individuals with Diabetes Mellitus
Date Carbs Protein Fat Calories Description
1979 50‐60% 12‐20%<10% as saturated fat
American Diabetes Association11
1986 55–60% 0.8g/kg total fat <30% American Diabetes Association12
1994 10–20%<10% from saturated fat
American Diabetes Association13
Modified from Wheeler ML. Diabetes Spectrum 13(3):116, 2000.1Marcus Aurelius Antoninus, 2nd century A.D. 9th ed. Bartlett J, ed. Boston, Little, Brown and Co., 1901. 2Post E. New York, Funk & Wagnalls, 1922. 3Wood FC, Bierman EL. Nutr Today 7(3):4-12, 1972. 4Leeds AR. Proc Nutr Soc 38:365-71, 1979. 5Allen FM. Boston Med Surg J 172:241-47, 1915. 6Joslin EP J. Am Diet Assoc 3:89-92, 1927. 7Joslin EP et al. 7th ed. Philadelphia, Lea & Febiger, 1940, p. 212. 8Caso EK J /Am Med Assoc 133:169-71, 1947. 9Caso EK J. Am Diet Assoc26:575-83, 1950. 10American Diabetes Association. Diabetes 20:633-34, 1971. 11American Diabetes Association. Diabetes 28:1027-30, 1979. 12American Diabetes Association. Diabetes Care 10:126-32, 1987. 13American Diabetes Association. Diabetes Care 23 (Suppl. 1):43-46, 2000.
History of Diabetes Nutrition
Effective Non-Surgical Alternatives to $$$ Procedures
1- Structured Multidisciplinary lifestyle intervention2- Very low calorie diet2- Very low carbohydrates diet
+Anti-obesity medicationsDiabetes medications with weight loss action
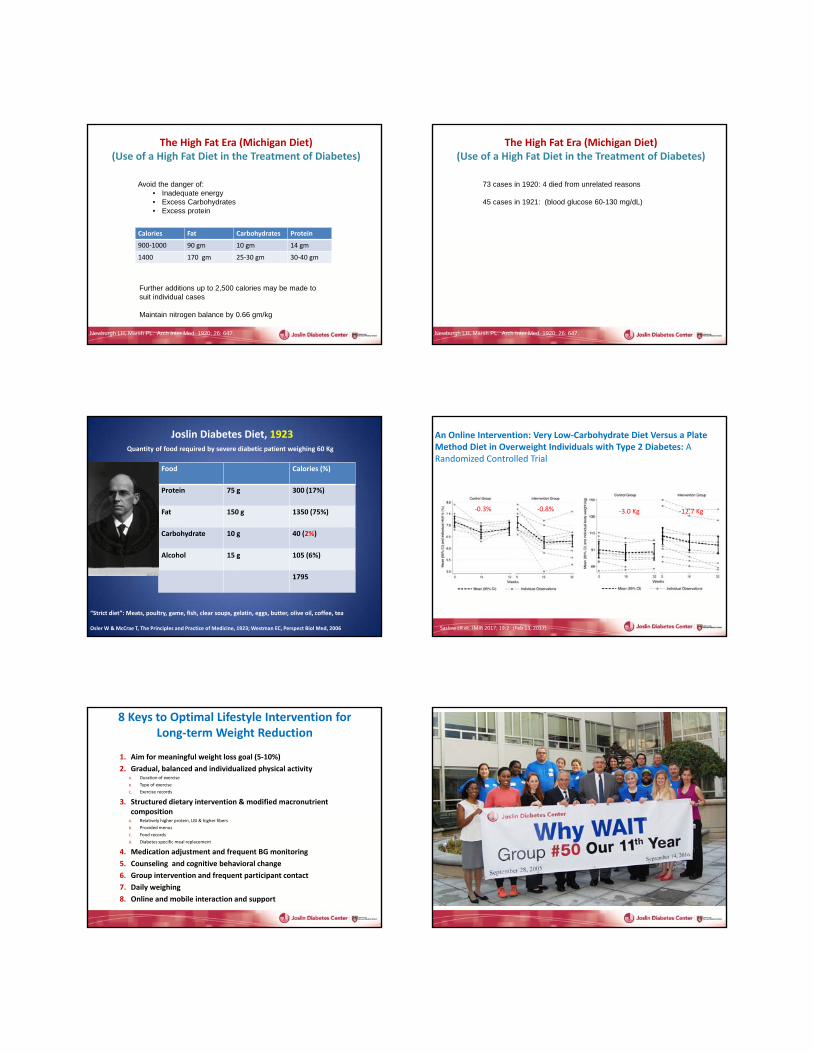
The High Fat Era (Michigan Diet)(Use of a High Fat Diet in the Treatment of Diabetes)
Diabetes Mellitus
Newburgh LH, Marsh PL. Arch Inter Med. 1920; 26: 647.
Further additions up to 2,500 calories may be made to suit individual cases
Maintain nitrogen balance by 0.66 gm/kg
Calories Fat Carbohydrates Protein
900‐1000 90 gm 10 gm 14 gm
1400 170 gm 25‐30 gm 30‐40 gm
Avoid the danger of:• Inadequate energy• Excess Carbohydrates• Excess protein
Newburgh LH, Marsh PL. Arch Inter Med. 1920; 26: 647.
73 cases in 1920: 4 died from unrelated reasons
45 cases in 1921: (blood glucose 60-130 mg/dL)
The High Fat Era (Michigan Diet)(Use of a High Fat Diet in the Treatment of Diabetes)
Diabetes Mellitus
“Strict diet”: Meats, poultry, game, fish, clear soups, gelatin, eggs, butter, olive oil, coffee, tea
Osler W & McCrae T, The Principles and Practice of Medicine, 1923; Westman EC, Perspect Biol Med, 2006
Joslin Diabetes Diet, 1923Quantity of food required by severe diabetic patient weighing 60 Kg
Food Calories (%)
Protein 75 g 300 (17%)
Fat 150 g 1350 (75%)
Carbohydrate 10 g 40 (2%)
Alcohol 15 g 105 (6%)
1795
An Online Intervention: Very Low‐Carbohydrate Diet Versus a Plate Method Diet in Overweight Individuals with Type 2 Diabetes: A Randomized Controlled Trial
‐0.3% ‐0.8% ‐3.0 Kg ‐12.7 Kg
Saslow LR et. JMIR 2017; 19:2 (Feb 13, 2017)
8 Keys to Optimal Lifestyle Intervention for Long‐term Weight Reduction
1. Aim for meaningful weight loss goal (5‐10%)
2. Gradual, balanced and individualized physical activity A. Duration of exercise
B. Type of exercise
C. Exercise records
3. Structured dietary intervention & modified macronutrient composition
A. Relatively higher protein, LGI & higher fibers
B. Provided menus
C. Food records
D. Diabetes specific meal replacement
4. Medication adjustment and frequent BG monitoring
5. Counseling and cognitive behavioral change
6. Group intervention and frequent participant contact
7. Daily weighing
8. Online and mobile interaction and support
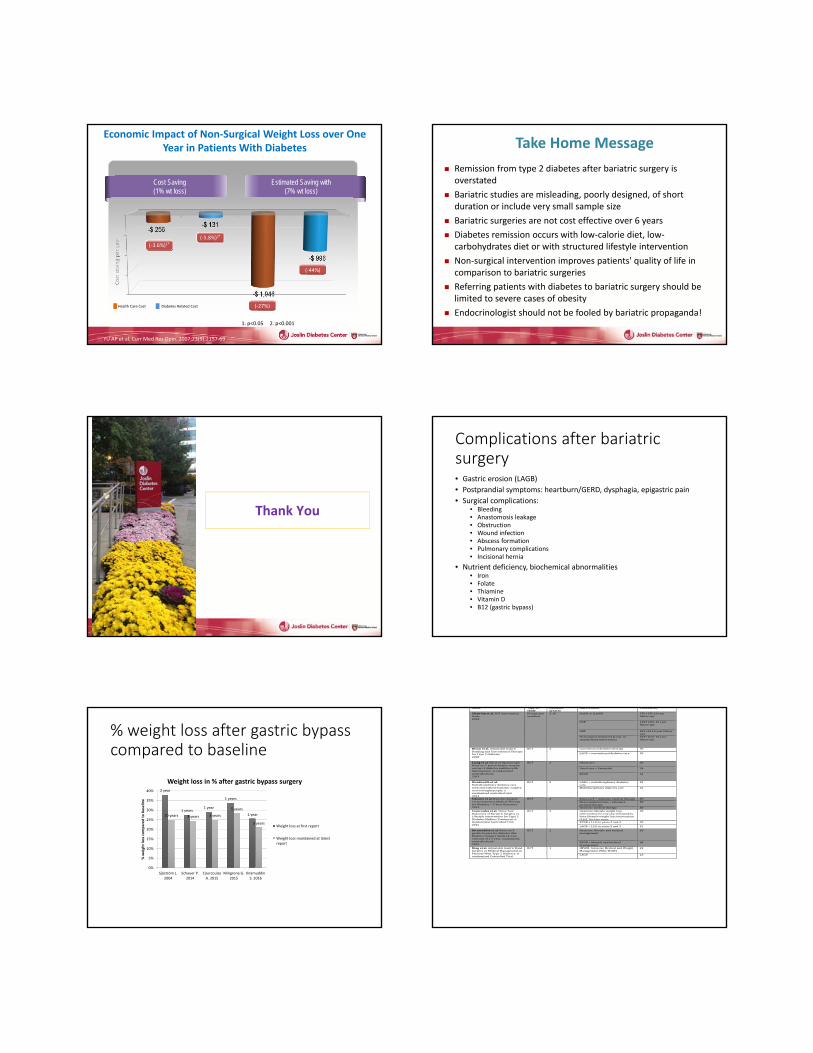
Economic Impact of Non‐Surgical Weight Loss over One Year in Patients With Diabetes
Cost Saving(1% wt loss)
Cost saving per year
(‐3.6%)1*(‐5.8%)2*
(‐27%)
(‐44%)
Estimated Saving with(7% wt loss)
YU AP et al. Curr Med Res Opin. 2007;23(9):2157‐69
Health Care Cost Diabetes Related Cost
1. p<0.05 2. p<0.001
Take Home Message
Remission from type 2 diabetes after bariatric surgery is overstated
Bariatric studies are misleading, poorly designed, of short duration or include very small sample size
Bariatric surgeries are not cost effective over 6 years
Diabetes remission occurs with low‐calorie diet, low‐carbohydrates diet or with structured lifestyle intervention
Non‐surgical intervention improves patients' quality of life in comparison to bariatric surgeries
Referring patients with diabetes to bariatric surgery should be limited to severe cases of obesity
Endocrinologist should not be fooled by bariatric propaganda!
Thank You
Complications after bariatric surgery• Gastric erosion (LAGB)
• Postprandial symptoms: heartburn/GERD, dysphagia, epigastric pain
• Surgical complications: • Bleeding• Anastomosis leakage• Obstruction• Wound infection • Abscess formation• Pulmonary complications• Incisional hernia
• Nutrient deficiency, biochemical abnormalities• Iron• Folate• Thiamine• Vitamin D• B12 (gastric bypass)
% weight loss after gastric bypass compared to baseline
2 year
1 years1 year
1 years
1 year10 years 3 years 3 years
5 years
3 years
0%
5%
10%
15%
20%
25%
30%
35%
40%
Sjöström L.2004
Schauer P.2014
CourcoulasA. 2015
Mingrone G.2015
IkramuddinS. 2016
% weight loss compared to baseline
Weight loss in % after gastric bypass surgery
Weight loss at first report
Weight loss maintained at latestreport
Name Typeofstudy
Duration(years)
Intervention Patientsno.
Sjöströmetal.SOSinterventionstudy2004
Prospectivematched
2‐10 NAGBor(L)AGB
376(15610yearfollowup)
VGB
1369(45110yearfollowup)
GBP
265(3410yearfollowup)
Nonsurgicaltreatmentgroup,nostandardizedintervention
2037(627 10yearfollowup)
Dixonetal. AdjustableGastricBandingandConventionalTherapyforType2Diabetes2008
RCT 2 Conventionaldiabetestherapy 30
LAGB+conventionaldiabetescare 30
Liangetal.EffectoflaparoscopicRoux‐en‐Ygastricbypasssurgeryontype2diabetesmellituswithhypertension:Arandomizedcontrolledtrial2013
RCT
1
Usualcare
36
Usualcare+Exenatide
34
RYGB 31
Wentworthetal.Multidisciplinarydiabetescarewithandwithoutbariatricsurgeryinoverweightpeople:arandomizedcontrolledtrial2014
RCT 2 LABG+multidisciplinarydiabetescare
25
Multidisciplinarydiabetescare 26
Schaueretal.BariatricSurgeryversusIntensiveMedicalTherapyforDiabetes–3‐YearOutcomes2014
RCT
3 Roux‐en‐Y+intensivemedicaltherapy 50Sleevegasterectomy+intensivemedicaltherapy
50
Intensivemedicaltherapy 50Courcoulasetal.ThreeYearOutcomesofBariatricSurgeryvs.LifestyleInterventionforType2DiabetesMellitusTreatment:ARandomizedControlledTrial2015
RCT 3 Intensivelifestyleweightlossinterventionforoneyearfollowedbylowelifestyleweightlossintervention(LLLI)fortwoyears
20
RYGB+LLLIinyears2and3 20
LAGB+LLLIinyears2and3 21
Ikramuddinetal.Roux‐en‐Ygastricbypassfordiabetes(theDiabetesSurgeryStudy)2‐yearoutcomeofa5‐year,randomized,controlledtrial2015
RCT 2 Intensivelifestyleandmedicalmanagement
60
RYGB+lifestyleandmedicalmanagement
60
Dingetal.AdjustableGastricBandSurgeryorMedicalManagementinPatientsWithType2Diabetes:ArandomizedControlledTrial
RCT
1
IMWM,IntensiveMedicalandWeightManagement(WhyWAIT)
22
LAGB
23