Embed Size (px)
Citation preview

De Novo Variants: Can these Inform Clinical Phenotypes?
Christine Seidman, MD Thomas W. Smith Professor of Medicine & Genetics Investigator, Howard Hughes Medical Institutes

Tetralogy of Fallot Hypoplastic Left Heart Syndrome
Transposition of Great Arteries
Schematics Courtesy of the Center for Disease Control
National Center Birth Defects/Disabilities
Prevalence:1.45/1000 children 0.4 in 1000 adults
Mean Age (2000): 17 years
11% Congenital anomaly 9-50% Neurodevelopmental deficits
(NDD)

Pediatric Cardiac Genomics Consortium
Hypothesis: De Novo Gene Mutations Cause Critical CHD Mutations are Damaging
Loss of Function (LoF): Premature Stop, Frameshift
Deleterious Missense Resides
Brigham & Women’s Hospital Children’s Hospital Boston Columbia Medical Center Children’s Hospital Philadelphia Children’s Hospital Los Angeles
Mount Sinai Medical Center Rochester Medical Center UCLA Yale School of Medicine NHLBI
Collaborating Sites: PCGC

Whole Exome Sequencing of Critical CHD Trios
1220 critical CHD Trios Exclude Syndromic Cases Unaffected parents Family history negative
vs. Observed in 900 Control Trios Unaffected parents Unaffected sibling of Autistic Child Simons Simplex Cohort Collaborators:
Matthew State, Michael Wigler, Eric Eichler
PCGC
vs. Expected Number per Exome Based on the probability of mutation at
each base, controlling for a) Local sequence context
b) Depth of coverage c) Divergences score based on human-macaque differences d) Exclude in-frame insertions/deletions e) Meta-SVM for Missense variants
(Samocha et al., Nature Genetics, 2014)

7DEOH �
7DEOH �� GH QRYR (QULFKPHQW LQ &DVHV YV� &RQWUROV
&DVHV� 1 ���� &RQWUROV� 1 ���2EVHUYHG ([SHFWHG
(QULFKPHQW S2EVHUYHG ([SHFWHG
(QULFKPHQW SQ 5DWH Q 5DWH Q 5DWH Q 5DWH
$OO JHQHV7RWDO ���� ���� ������ ���� ��� ���� ��� ���� ����� ���� ��� ����6\QRQ\PRXV ��� ���� ����� ���� ��� � ��� ���� ����� ���� ��� �0LVVHQVH ��� ���� ����� ���� ��� ���� ��� ���� ����� ���� ��� ����'�0LV ��� ���� ����� ���� ��� ���[����� ��� ���� ���� ���� ��� �����/R) ��� ���� ����� ���� ��� ������ �� ���� ���� ���� ��� ����'DPDJLQJ ��� ���� ����� ���� ��� ���[����� ��� ���� ����� ���� ��� ����
++( JHQHV7RWDO ��� ���� ����� ���� ��� ���[����� ��� ���� ����� ���� ��� ����6\QRQ\PRXV �� ���� ����� ���� ��� ���� �� ���� ���� ���� ��� ����0LVVHQVH ��� ���� ����� ���� ��� ������� ��� ���� ����� ���� ��� ���'�0LV �� ���� ���� ���� ��� ���[����� �� ���� ���� ���� ��� ����/R) �� ���� ���� ���� ��� ���[����� �� ���� ���� ���� ��� ����'DPDJLQJ ��� ���� ���� ���� ��� ���[����� �� ���� ���� ���� ��� ����
/+( JHQHV7RWDO ��� ���� ����� ���� ��� � ��� ���� ����� ���� ��� ����6\QRQ\PRXV ��� ���� ����� ���� ��� � ��� ���� ����� ���� ��� �0LVVHQVH ��� ���� ����� ���� ��� ���� ��� ���� ����� ���� ��� ����'�0LV ��� ���� ���� ���� ��� ����� �� ���� ���� ���� ��� �����/R) �� ���� ���� ���� ��� ���� �� ���� ���� ���� ��� ����'DPDJLQJ ��� ���� ����� ���� ��� ���� ��� ���� ����� ���� ��� ����
Q� 1XPEHU RI GH QRYR PXWDWLRQV� 5DWH� 1XPEHU RI GH QRYR PXWDWLRQV GLYLGHG E\ QXPEHU RI LQGLYLGXDOV LQ FRKRUW �1�� ++(� +LJK +HDUW ([SUHVVHGJHQHV �WRS TXDUWLOH RI H[SUHVVLRQ�� /+(� /RZHU +HDUW ([SUHVVHG JHQHV �ERWWRP WKUHH TXDUWLOHV RI H[SUHVVLRQ�� '�0LV� 'DPDJLQJ 0LVVHQVH SUHGLFWHGE\ 0HWD�690� 'DPDJLQJ� '�0LV � /R)� %ROG� (QULFKPHQW ! � RU S � �����
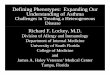
CHD Cases, N = 1220 Controls, N = 900
Homsy et al, Science 2015
Genes Highly Expressed in Developing Heart
Observed
Damaging De Novo Variants: Enriched in CHD Cases vs Expected or Observed
Observed Expected Expected Enrichment Enrichment p p

Evidence for Pathogenicity: 21 Genes with Recurrent Damaging De Novo Variants

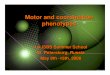
De Novo Copy Number Variants Detected by WES Glessner*, Bick,* et al, Circ Res 2014
Z-sc
ore
of N
orm
aliz
ed R
ead
Dep
th
-10
-
5
0
5 11 Targets, 105 bases (chr 22: 36013197-36156089)
O 1-00425
RBFOX2
De Novo RBFOX2 LoF Variants 3 SNVs (frameshifts/stop) 1 CNV(del) 4 De Novo vs expected: p=1.60E-8 All with HLHS

De Novo Copy Number Variants Detected by WES Glessner*, Bick,* et al, Circ Res 2014
RBFOX2
RBFOX2 : Binds mRNA splicing enhancer element (UGCAUG) Contributes to tissue-specific exon splicing in pre-mRNAs Highly expressed in heart (>250 reads/million) Targets ~7% Human ES cell Genes (Yeo et al; Nat Struct Molec Bio, 2009)

Genotype:Phenotype Assessments: De Novo, Damaging Variants Enriched in CHD Subsets
Extra: Non-cardiac Congenital Anomaly NDD: Neurodevelopmental Delay/Deficits
Homsy et al, Science 2015

Genes Harboring De Novo Variants: Common to Both CHD and NDD Cohorts
Homsy et al, Science 2015
Known NDD Genes HHE & NDD Genes
Enric
hmen
t

Functional Annotation of Genes with De Novo, Damaging Variants
2. Cardiovascular Developmental Processes (p=8.6x10-8) 3. Anatomic Structure Morphogenesis Modification (p=1.1 x 10-14)
1. Neurologic Development (p=1.8 x10-5)
4. Chromatin Modification (p=7.5x10-20)
Homsy et al, Science 2015

Evidence/Support that De Novo Variants are not VUS
Ø Unlikely Chance Co-Occurrence of De Novo, Damaging Mutations in “Constrained” Residues and Critical CHD
Ø Genes with De Novo Variants: Highly Expressed in Affected Tissues Ø Additional (Unappreciated) Clinical Phenotypes are “Explained” by
De Novo Variants Ø Recurrent De Novo, Damaging Gene Variants among Probands with
“Like” phenotypes Ø Proteins encoded by Genes with De Novo Variants, like Familial
Mutations Function in Related Biologic Pathways
Familial CHD: Cardiac TxF

Evidence/Support that Damaging De Novo Variants do Not Fully Cause Clinical Phenotypes
Ø 69 Genes with De Novo Mutations (n=85) were shared in CHD and
NDD cohorts. Highly UNLIKELY that NDD-ascertained patients with these variants had severe CHD.
Ø Not all CHD patients with De Novo Mutations in Genes identified in NDD-ascertained patients have NDD
Ø Mutations = Definitive Causes of Disease: Asymmetric Limb Phenotypes in CHD patients
Ø Can Clinical Identification of De Novo Mutations be Diagnostic in Single Patients?

Strategies to Functionally Annotate CHD Mutations: Define Cardiac Developmental Transcription in Single Cells
Delaughter et al, in Review

A1
A2
KCNN3 WNT2 TNNI3
Atrial Cardiomyocytes Ventricular Cardiomyocytes
1
2
3
Acadl Mlf1 Cav1 Gja1 Casq2 Kcnk3 Dhrs7 Ckm Cox8b Mt1 Nfia Slc24a5 Sdpr Mgp Mgst1 Ckb Ddt Hmga2 Wnt2 Tagln Acta2 Gm100 Tnni3 Ndufa5 Pam Cox6a2 Smpx Fxyd1 Nppa Sln
Strategies to Functionally Annotate CHD Mutations: Define Cardiac Developmental Transcription in Single Cells
Delaughter et al, in Review

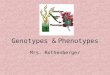
Modeling Human Mutations in Isogenic iPSC-derived Cardiomyocytes
iPSC-derived Cardiomyocytes
Adult Human Myocyte
iPSC-CM

KDM5B (1341)
KDM5A^ (452)
CHD7 (471)
115
200
125 171
136
20
834
KDM5B (2244)
KDM5A^ (858)
CHD7 (1051)
296
508
124
56
170
191
1270
Transcriptional Differences between Isogenic WT and CHD-mutant Cardiomyocytes
Increased Decreased
^KDM5A+/R1508W & KDM5A+/- >90%Congruent

hES-CM (1 yr)
Developmental age of Cardiomyocytes Differentiated from Mouse/Human Embryonic Stem Cells
Delaughter et al, in Review

E9.5 E14.5
-0.10 0.0
20
30
40
P0
10
20
30
40
10
20
30
40
10
P21
E14.5
20
30
40
10
0.05 -0.05
P0
P21 %
Cel
ls
A2
0%
50%
100%
E14.5 P0 P7 P21
*** **
WT Nkx2-5+/-
*** **
0.10
------- WT Nkx2-5
Developmental Delay in Cardiomyocytes from Nkx2-5 Mice
Delaughter et al, in Review

CHD Genetics Jason Homsy James Ware David McKean Michael Parvenof Steve DePalma Alireza Haghighi Alex Bick Akl Fahed Karou Ito
iPS-Cardiomyocytes Travis Hinson Calvin Sheng Tarsha Ward Navid Nafissi Warren Tai David Conner
RNAseq Studies Dan Delaughter Alex Bick Arin Kim
Pediatric CV Genetics Consortia Boston Children’s Hospital: Jane Newburger, Amy Roberts Children’s Hospital of Pennsylvania: Elizabeth Goldmuntz Columbia: Wendy Chung Icahn School of Medicine at Mt Sinai: Bruce Gelb Yale: Martina Brueckner & Richard Lifton NIH: Jonathan Kaltman and Charlene Shramm