Embed Size (px)
Citation preview
De-escalating Challenging Interactions with Students
A Review of the Literature
Dorje Jennette, PsyD | Melody Fo, PsyD | Gary Dunn, PhD | Mary Knudtson, DNSc, NP, FAAN
Student Health Services
University of California, Santa Cruz
Agenda / Purpose / ObjectivesPresenter: Mary Knudtson, Executive Director
• Who’s here? What roles are represented in the audience?
• Purpose: Understand research-driven responses to disruptive students
• Objectives:• Understand the consequences of disruptive behavior
• List possible causes of disruptive behavior
• Describe continuum of disruptive behavior
• Explain how to respond to disruptive behavior
• Implementation
What roles are represented in the audience?Presenter: Mary Knudtson, Executive Director
• Primary care provider
• Pharmacist
• Nurse
• Psychiatrist
• Psychologist/Psychotherapist
• Technician
• Dietician
• Medical assistant
• Health promotion
• Other roles?
• Also in role of interacting with students waiting in reception area?
Who has an example of disruptive behavior to share?Presenter: Mary Knudtson, Executive Director
• Student yelling in the waiting area
• Student throwing things and shoving furniture
• Student refusing to leave
• Student is verbally threatening
Honegger (2012)
Quiz: Disruptive Behavior in HealthCarePresenter: Mary Knudtson, Executive Director
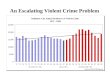
• Compared to the average worker in the US, how many times more likely is a worker in health care and social assistance to be the victim of a non-fatal assault or violent act?
A. 2B. 3C. 5D. 10
• What percent of all non-fatal injuries from occupational assaults and violent acts occurred in the healthcare setting?
A. 25%B. 33%C. 49%D. 60%
• Which group of healthcare workers are most frequently assaulted?A. NursingB. Primary Care ProvidersC. Social Service WorkersD. Administrative Staff
Elliott. (1997) Lanza. (1992)US Bureau of Labor and Statistics. (2010)
Quiz: Disruptive Behavior toward Nurses(from National Survey of RNs, 2008)Presenter: Mary Knudtson, Executive Director
• What percentage of nurses reported verbal abuse from patients within the year?A. 15%B. 30%C. 50%D. 59%
• What percentage of nurses reported physical abuse (e.g., grabbed, scratched, kicked) within the year?A. 16%B. 26%C. 36%D. 46%
• In their work as a nurse, what percentage experienced sexual harassment or hostile environment?A. 13%B. 23%C. 33%D. 43%
•According to research literature, which characteristics place nurses at higher risk for being victims of violence? (select all that apply)A. Minority groupB. Younger, less experiencedC. WomenD. Men
Buerhaus, Donelan, ResRoches, & Hess. (2009)Wang et al. (2008)
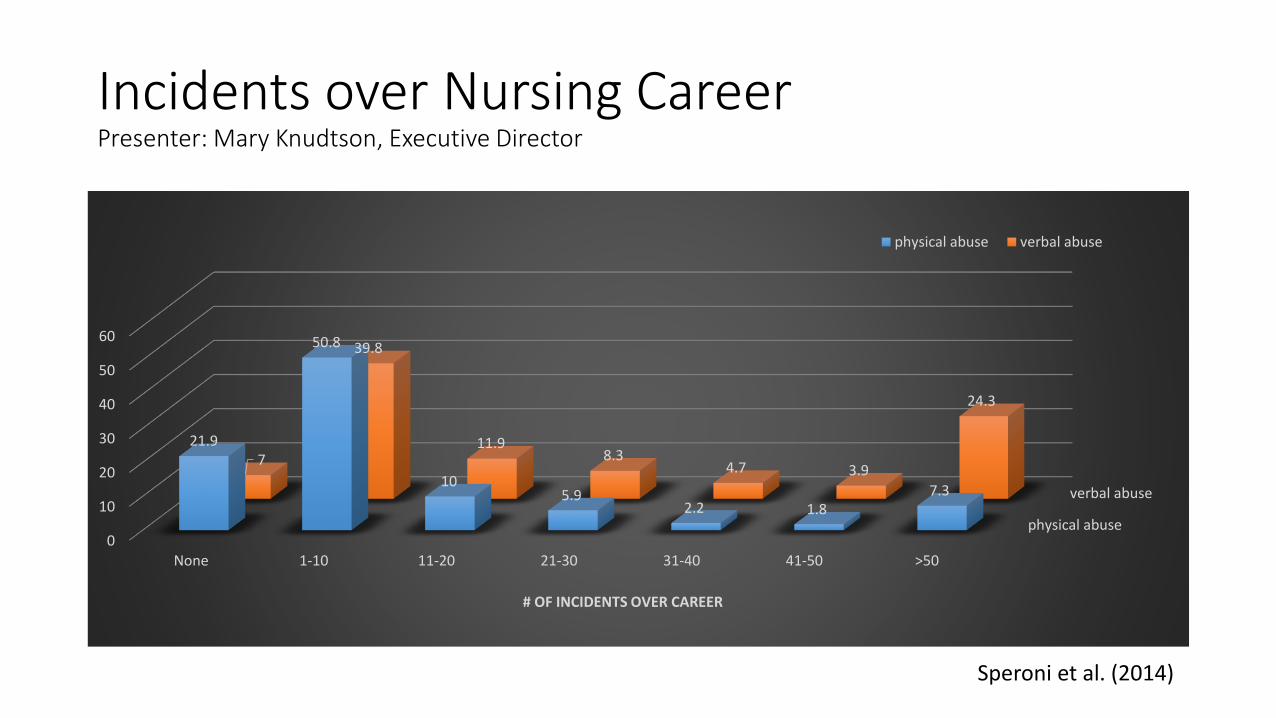
Incidents over Nursing CareerPresenter: Mary Knudtson, Executive Director
physical abuse
verbal abuse
0
10
20
30
40
50
60
None 1-10 11-20 21-30 31-40 41-50 >50
21.9
50.8
105.9
2.2 1.87.3
7
39.8
11.98.3
4.7 3.9
24.3
# OF INCIDENTS OVER CAREER
physical abuse verbal abuse
Speroni et al. (2014)
State of the ResearchPresenter: Mary Knudtson, Executive Director
• Nursing is a primary focus of research
• Lack of agreement on what constitutes aggression and violence
• Methodological limitations: typically small and/or self-selected sample, small-scale settings, self-assessment
• Under-reporting• Stigma, isolation, and fear of judgement may inhibit reporting of disruptive behavior
• Approximately 80% of incidents may not be reported
• Administrative or staff resistance to accurate reporting• Apathy
• Private trainings/manuals—authority-based, without publications
• Government sourcesRippon. (2000)Wang et al. (2008)
CostsPresenter: Mary Knudtson, Executive Director
• 25.7% of nurses report receiving no training
• Physical, personal, emotional, professional, organizational consequences (e.g., triggers can invoke reactions to past events)
• Job performance, productivity, job satisfaction, staff retention, staff morale
• Because of violence where they work:• 63.3% considered leaving their workplace
• 8.8% considered leaving the nursing profession altogether
• 6.3% considered changing jobs
Speroni et al., 2014
Evidence about TrainingPresenter: Mary Knudtson, Executive Director
• INTACT Program: 2-days of mandatory aggression management training with group work, role-plays, self-defense techniques, and aggression management manual (Ilkiw-Lavalle, Grenyer, & Graham, 2002)• Knowledge improvement for first-time participants as well as those with prior training.
• Shorter more frequent training programs likely beneficial
• Significant differences in pre/post scores based on occupation suggesting training should be tailored to the needs of staff.
• All staff highly satisfied with training and relevance of material. Requests for ongoing education and learning negotiation skills
• Summary of findings from other studies:• Regular, ongoing education helps staff maintain skills and increases confidence• Training increased sense of safety, confidence, self-efficacy. Greater confidence with more modules
completed.• Improved attitudes toward working with aggressive patients. Decline in perceived severity of incidents.• Decreased burnout and staff turnover, negative attitudes, and increased concern for patient care
Goodykoontz & Henrick. (1990)Grenyer et al. (2004)Wang et al. (2008)
Disruptive Behavior ContinuumPresenter: Dorje Jennette, CAPS Clinical Director
• Disruptive – any incident in which the delivery of care or services is interrupted or impeded.
• Threat – any verbal or non-verbal expression of an intention to inflict pain or injury or to cause annoyance or alarm.
• Violence – any physical force exerted to violate, damage, or abuse another person, equipment, or property.
VA Office of Inspector General. (2013)
Precipitating FactorsPresenter: Dorje Jennette, CAPS Clinical Director
• Loss of personal power• Delays in service access
• Need to maintain self-esteem/“save face”
• Fear• Feelings of uncertainty or confusion• Feeling pressured to make decisions
• Frustration
• Attention-seeking
• Psychological/physiological causes• Personality disorder• Psychosis• Pain/hunger/insomnia• Influence of alcohol or other drugs• Neurological impairment
Note: Beware of the Fundamental Attribution Error; situation often trumps personality
Some categories informed by Nonviolent Crisis Intervention® training program
PreventionPresenter: Dorje Jennette, CAPS Clinical Director
• Rational Detachment
• Exceptional Customer Service
• Assess Your Environment
• Assess Yourself
Denver VA. (2009)
Signs and Symptoms of StressPresenter: Dorje Jennette, CAPS Clinical Director
• Noticeable shift in behavior
• Difficulty taking in information/instructions
• Decreased awareness of surroundings
• Pacing, finger drumming, hand wringing
• Staring off into space or looking “dazed”
• Fearful or anxious presentation
Denver VA. (2009)
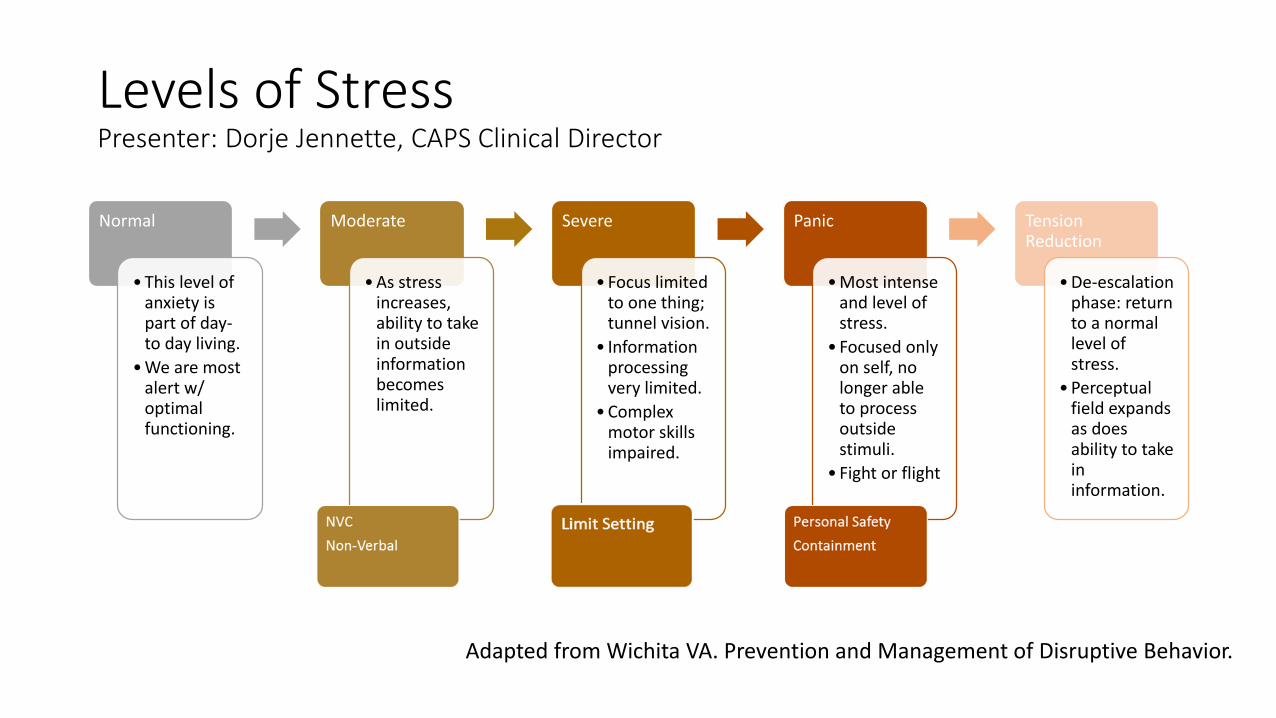
Levels of StressPresenter: Dorje Jennette, CAPS Clinical Director
Normal
• This level of anxiety is part of day-to day living.
• We are most alert w/ optimal functioning.
Moderate
• As stress increases, ability to take in outside information becomes limited.
Severe
• Focus limited to one thing; tunnel vision.
• Information processing very limited.
• Complex motor skills impaired.
Panic
• Most intense and level of stress.
• Focused only on self, no longer able to process outside stimuli.
• Fight or flight
Tension Reduction
• De-escalation phase: return to a normal level of stress.
• Perceptual field expands as does ability to take in information.
Adapted from Wichita VA. Prevention and Management of Disruptive Behavior.
Image adaptation courtesy of Kendra Morgan: https://www.webjunction.org/news/webjunction/approaching-conflict-as-an-opportunity-for-growth.html
Registration staff calls you to assist with a student who is demonstrating challenging behavior in the waiting room.Presenter: Melody Fo, Behavioral Health Consultant
• What are your initial reactions?• Emotions?• Attitudes?• Thoughts/beliefs/assumptions?• Behaviors?• Physiological response?
• What do you look like (facial expression, posture, etc.) when you are distressed by an interpersonal conflict?
• How might your initial reactions change if you were being called to assist with a student with pain, high anxiety, psychosis?
Personal ReactionsPresenter: Melody Fo, Behavioral Health Consultant
• Freeze, fight, flight
• Physiological stress response
• “Negative emotions”: anger, fear, disgust, sadness, despair
• Question own competence
• Judgements and assumptions about student and situation
Farrell & Salmon. (2010)Farrell, Touran, & Salmon. (2010)
How might our personal reactions affect further interactions with the student?Presenter: Melody Fo, Behavioral Health Consultant
• Compromised judgement, communication, reasoning. Stress response may re-escalate student
• Self-fulfilling prophecy• Inadvertently trigger, maintain, or exacerbate disruptive behavior by
behaving less sensitively• Uncaring behavior in an attempt to protect self from distress and/or feelings of
inadequacy• Hostility, coercion, or engaging in power struggle in response to threats to
competence
• Fail to consider functions disruptive behavior may have for students• Fundamental attribution error
Farrell & Salmon. (2010)Farrell, Touran, & Salmon. (2010)Richter. (2006)
Student Behaviors in ContextPresenter: Melody Fo, Behavioral Health Consultant
• Staff can influence disruptive student behaviors by perceiving and labeling behavior as such
• Feeling empathy for student is the best predictor of staff readiness to help with disruptive behavior
• Staff training to build understanding of:• Behavior toward students that is affected by values (or attitudes), emotional
reactions, skills in interaction
• Student’s perspective
• Environment (cultural, physical) influences on staff-student interactions
Dagman & Cairns. (2005)Farrell & Salmon. (2010)
Defusing Difficult SituationsPresenter: Melody Fo, Behavioral Health Consultant
• Verbal intervention as a first step• Maintain calm • Attitude of willingness to help• Use simple sentences• Use paraphrasing to convey understanding• Acknowledge student’s opinion/position (“I see what you mean,” “I’d like to hear more about it”)• Convey expectation that student can control their behavior• Use “I statements” rather than “you”
• Re-stabilize the situation once emotional tension is no longer driving the interaction• Lead the conversation back to the initial issue (“could we talk about . . . again?”)• Allow time for responses (“Take your time,” “Think carefully . . .”)• Sophisticated giving in (“You’re right, one can see it from this point of view, but we should talk about . . . “)• Avoid “why-questions” as they are often perceived as reprimanding• Open-ended questions are preferable to closed questions
Denver VA. (2009)Phillips, Stinson, Strickler. (2014) Richter. (2006)
Defusing Difficult Situations (cont)Presenter: Melody Fo, Behavioral Health Consultant
• Listen for content and meaning (if confusing, listen for bigger universal emotional experience)
• Control the situation rather than the student• Conflict management with goal of win-win situation for both parties
• Gain time for de-escalation• Take a few breaths or look out the window for a few seconds when feeling pressured to respond
• Demonstrate balance of self-confidence and certainty without being provocative• Too much complacency can be interpreted as arrogant or provocative• Too little self-confidence may suggest staff are not able to resolve the situation• Avoid complementary or reciprocal escalation
• Avoid power plays between staff and students (back out and take team approach, defer to a different point person/team lead)
• Permit verbal venting, when possible• Listen for peak and valleys
Defusing Difficult Situations (cont)Presenter: Melody Fo, Behavioral Health Consultant
• Paraverbal communication• Facial expression and body language congruent with verbal message• Check the appropriateness of your volume and tone• Use even rate and rhythm• Personal space (at least three feet, but can vary culturally)• Utilize supportive stance• Lowered, uncrossed arms with open hands show we are not aggressive• Empathic listening conveyed by subtle tilt of head, nodding, and maintaining eye contact
without staring• Slow and gentle movements• Do not block access to escape routes (only police would prevent leaving)
• If at panic level of stress, utilize therapeutic containment• Isolate student• May involve moving other students and extraneous objects
Limit SettingPresenter: Melody Fo, Behavioral Health Consultant
• Set limits on behaviors rather than feelings
• Keep limits simple, reasonable, clear, and enforceable
• Offer alternative choice before the consequence
• Ignore challenging questions by redirecting and restating your request
“Please come back to the waiting area with me and I’ll be sure your provider meets with you as soon as possible. If you try to enter the restricted area again, I’ll have to call campus police.”
Nonviolent Communication (NVC) ProcessPresenter: Gary Dunn, CAPS Director
• Developed by Dr. Marshal Rosenberg: psychologist, educator, global conflict mediator
• 4 stage process promoting effective communication and conflict management.• Clear observations without mixing in evaluations
• Emotional response to situation without critical judgments
• Investigation of needs that may or may not have been met
• Presenting clear, non-demanding requests in a respectful, non-coercive manner
Nosek, Gifford, & Kober. (2014)
Nonviolent (Empathic) Communication for Health Care ProvidersPresenter: Gary Dunn, CAPS Director
“The purpose of Nonviolent (Empathic) Communication is to facilitate the flow of information necessary for health care providers to demonstrate their care and treat their patients effectively, as well as to work cooperatively and resolve differences effectively. It also helps identifying when a patient(s) needs empathy, and what might be interfering with our ability to respond to another person’s needs for caring at a given moment (our own emotions, preoccupations for diagnostics or treatment, etc).” (Rosenberg & Molho, 1998)
Nonviolent (Empathic) Communication for Health Care ProvidersPresenter: Gary Dunn, CAPS Director
Empathy in healthcare:
• Increases patient satisfaction
• Improves compliance
• Enhances provider ability to diagnose and treat patients
• Positively impacts providers’ experiences of interactions with patients and colleagues
• Providers who demonstrate empathic behaviors have a significantly reduced risk of litigation
Rosenberg & Molho. (1998)
NVC PracticePresenter: Gary Dunn, CAPS Director
NVC suggests that our paraphrasing take the form of questions that reveal our understanding, with questions focusing on:
• What you are observing: • “Are you reacting to the request to fill out the green sheet?”
• How others are feeling and the needs generating their feelings: • “Are you feeling worried because you were asked to wait for an
appointment?”
• What others are requesting: • “Are you wanting me to tell you my reasons for saying what I did?”
• “Would you like it if I let your PCP know your concerns?”
NVC PracticePresenter: Gary Dunn, CAPS Director
• Making a request (vs. demand)• “Would you be willing to lower your voice or talk later?”
• Specific
• Concrete
• Achievable
• Current
Role-play practicePresenter: Gary Dunn, CAPS Director
Respond to the following scenarios (and what impulses would you likely experience?):
• During a blood draw, a student says, “Let me out of here.”
• Despite being referred to the nearest pain clinic for any additional pain medication prescriptions, a student refuses to leave until his Norco prescription is refilled.
• In the waiting room, a student reacts to an unanticipated delay by becoming furious and yelling that everyone is incompetent.
Organizational Interventions and ConsiderationsPresenter: Gary Dunn, CAPS Director
• Organizational factors conducive to violence:• Understaffing, excessive workload• Detached, impersonal, restrictive and authoritarian organizational culture likely to increase student frustration• Workplace changes or restructuring • Climate of high co-worker support and harmony reduces risk of violence
• Clear organizational policy toward workplace violence speaks to management’s commitment reducing violence
• Responsibilities and standards of acceptable practice should be explicit for employer as well as employee• Most programs place the burden on staff to acquire skills to manage challenging behavior
• Zero-Tolerance Policies• May negatively influence aggression management efforts by implying attitude of punishment toward any aggressive
behavior• May alter tendency of health care staff to place the patient’s needs first• Assumption that all aggressive behaviors are inappropriate may lead to unnecessary, immediate, high intensity interventions• Negative impact on staff confidence and skills in dealing with aggression• Does not appear to increase nurses’ perception of organization’s commitment to take action against perpetrators• Reduced level of violence associated with both zero-tolerance policies and a clear outline of prohibited behaviors.
Wang et al. (2008)
Post-Incident StrategiesPresenter: Gary Dunn, CAPS Director
• Direct resources toward post-event programs that are preventative and reduce the impact of an event that has occurred
• Continuous monitoring of events promote better understanding of challenging encounters and establishment of prevention programs• Violent Incident Form (VIF): checklist that includes verbal threats, aggression, time, place,
perpetrator, activity, consequences • Accurate documentation promotes identification of action plans and justification for further
programs/training
• Structured Interventions:• Timely, informal debriefing sessions for all staff focused on VIF content, how situation was
handled, victim reaction, and whether incident could have been avoided or mitigated.• Resulted in better awareness of risk situations, how to avoid potentially dangerous situations, dealing
with aggressive patients (Arnetz & Arnetz, 2000)• Psychological Debriefing is categorized by APA Div. 21 as having “no research
support/treatment is potentially harmful” (see Cochrane, 2002). Research suggests Trauma Focused CBT may be better approach (Cochrane, 2010).
Wang et al. (2008)
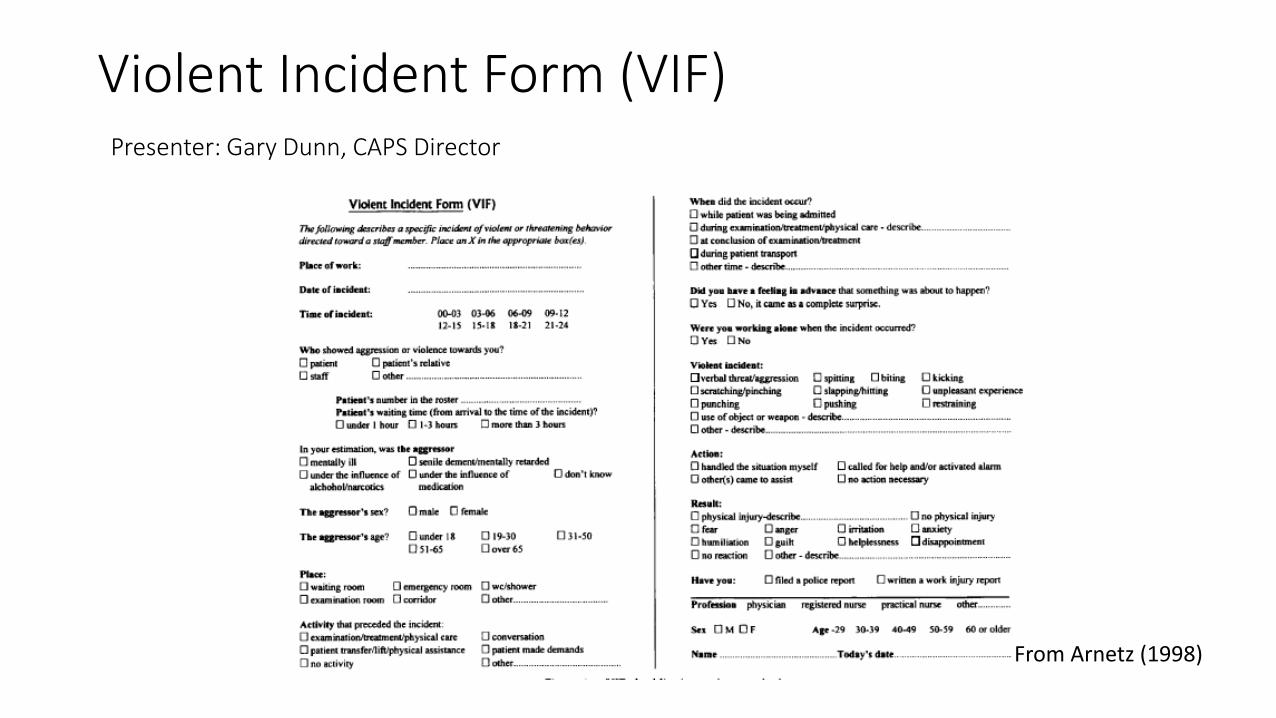
Violent Incident Form (VIF)Presenter: Gary Dunn, CAPS Director
From Arnetz (1998)
Training Development ResourcesPresenter: Gary Dunn, CAPS Director
• Arnetz, J. (1998). The Violent Incident Form (VIF): A practical instrument for the registration of violent incidents in the health care workplace. Work and Stress, 12, 17-28.
• ASIS International Healthcare Security Council. (2011). Managing disruptive behavior and workplace violence in healthcare. http://www.g4s.us/~/media/Files/USA/PDF-Articles/Hospitals%20and%20Healthcare/Council_Healthcare_WorkplaceViolence.ashx
• California Division of Occupational Safety and Health. Cal/OSHA Guidelines for Workplace Security. http://www.dir.ca.gov/dosh/dosh_publications/worksecurity.html.
• California Division of Occupational Safety and Health. Guidelines for Security and Safety of Health Care and Community Service Workers. http://www.dir.ca.gov/dosh/dosh_publications/hcworker.html.
• Center for Disease Control and Prevention. Workplace Violence Prevention for NursesCDC Course No. WB1865 - NIOSH Pub. No. 2013-155. http://www.cdc.gov/niosh/topics/violence/training_nurses.html
• Denver VA. (2009). Prevention and management of disruptive behavior. http://www.denver.va.gov/DENVER/clinicaltrainee/09medicalcenterpreventiondisruptivebehavior.doc.
• Farrell & Salmon. (2009). Challenging behavior: An action plan for education and training. Contemporary Nurse, 34(1), 110-118.
• Farrell, Shafiei, & Salmon. (2010). Facing up to ‘challenging behavior’: a model for training in staff-client interactions. Journal of Advanced Nursing, 1644-1655.
• Oregon OSHA. Violence Prevention Program – Online. https://www4.cbs.state.or.us/exs/osha/training/training/workshop/index.cfm
• Richter, D. (2006). Nonphysical conflict management and de-escalation. In D. Richter and R. Whittington (Eds.), Violence in mental health settings: Causes, consequences, management (125-144). Springer, New York.
• Wang, S., Hayes, L., & O’Brien-Pallas, L. (2008). A review and evaluation of workplace violence prevention programs in the health sector. Nursing Health Services Research Unit. Retrieved from http://www.nhsru.com/wp-content/uploads/2010/11/NHSRU-U-of-T-Site-EVPP-Study-Final-Report-July-081.pdf
• Wichita VA. Prevention and management of disruptive behavior. http://www.wichita.va.gov/documents/8_PMDB_substitute_110112.pdf?trk=profile_certification_title.
ReferencesBuerhaus,P., Donelan, K., ResRoches, C., & Hess, R. (2009). Still making progress to improve the hospital workplace environment: Results from the 2008 National Survey of Registered Nurses, Sept/Oct 2009.
Dagman, D., & Cairns, M. (2005). Staff judgements of responsibility for the challenging behaviour of adults with intellectual disabilities. Journal of Intellectual Ability Research, 49.
Denver VA. (2009). Prevention and management of disruptive behavior. Retrieved from http://www.denver.va.gov/DENVER/clinicaltrainee/09medicalcenterpreventiondisruptivebehavior.doc.
Farrell, G. & Salmon, P. (2010). Challenging behavior: An action plan for education and training. Contemporary Nurse, 34(1), 110-118.
Farrell, Shafiei, & Salmon. (2010). Facing up to ‘challenging behavior’: a model for training in staff-client interactions. Journal of Advanced Nursing, 1644-1655.
Goodykoontz, L. & Herrick, C. (1990). Evaluation of an in-service education program regarding aggressive behaviour on a psychiatric unit. The Journal of Continuing Education in Nursing, 21, 129-133.
Grenyer, B., Ilkiw-Lavalle, O., Biro, P., Middleby-Clements, J., Comninos, A., & Coleman, M. (2004). Safer at work: Development and evaluation of an aggression and violence minimization program. Australian and New Zealand Journal of Psychiatry, 38, 804-810.
Nosek, M., Gifford, G., & Kober, B. (2014). Nonviolent communication (NVC) training increases empathy in baccalaureate nursing students: A mixed method study. Journal of Nursing Education and Practice, 4(10).
ReferencesIlkiw-Lavalle, O., Grenyer, B., & Graham, L. (2002). Does prior training and staff occupation influence knowledge acquisition from an aggression management training program? International Journal of Mental Health Nursing, 11, 233-239.
Phillips, J., Stinson, K., & Strickler, J. (2014). Avoiding eruptions: De-escalating agitated patients. Nursing, April.
Richter, D. (2006). Nonphysical conflict management and de-escalation. In D. Richter and R. Whittington (Eds.), Violence in mental health settings: Causes, consequences, management (125-144). Springer, New York.
Rippon, T. (2000). Aggression and violence in health care professions. Journal of Advanced Nursing, 31(2), 452-460.
Rosenberg, M. & Molho, P. (1998). Nonviolent (empathic) communication for health care providers. Hemophilia, 4, 335-340.
Speroni, K., Fitch, T., Dawson, E., Dugan, L., & Atherton, M. (2014). Incidence and cost of nurse workplace violence perpetrated by hospital patients or patient visitors. Journal of Emergency Nursing, 40(3).
Honegger, T. (2012). Intervention strategies for potentially dangerous patients [power point slides].
US Bureau of Labor and Statistics. (2010). Compensation and working conditions.
VA Office of Inspector General. (2013). Management of Disruptive Patient Behavior at VA Medical Facilities
Wang, S., Hayes, L., & O’Brien-Pallas, L. (2008). A review and evaluation of workplace violence prevention programs in the health sector. Nursing Health Services Research Unit. Retrieved from http://www.nhsru.com/wp-content/uploads/2010/11/NHSRU-U-of-T-Site-EVPP-Study-Final-Report-July-081.pdf
Wichita VA. Prevention and management of disruptive behavior. Retrieved from http://www.wichita.va.gov/documents/8_PMDB_substitute_110112.pdf?trk=profile_certification_title.
Contact us
• Dorje Jennette, PsyDCAPS Associate Director for Clinical [email protected]
• Melody Fo, PsyDCAPS Psychologist, Behavioral Health [email protected]
• Gary Dunn, PhDCAPS [email protected]
• Mary Knudtson, DNSc, NP, FAANExecutive [email protected]
Acknowledgement: Anna Iversen was consulted for this presentation.