Embed Size (px)
Citation preview

DAVID A. HOOKER, MDBMH-DESOTO ASST. ED MEDICAL
DIRECTOR
EMS Management of Acute Stroke

Pop-Quiz
1. What is the most important historical information relating to a stroke patient? a. History of stroke previously b. History of diabetes c. Time of symptom onset (Last known well)d. Recent use of drugs or alcohol
2. At what level should blood pressure be reduced in the pre-hospital setting?
a. 140/90 b. 180/105 c. 220/120 d. Never reduce BP in the pre-hospital setting unless per medical command physician
3. Which of the following is NOT an important component of pre-hospital stroke patient care?
a. Determine the time of symptom onset (Last known well)b. Call the destination hospital early c. Acquire a 12-lead EKGd. Transfer the patient as soon as possible

Objectives
Understand the epidemiology surrounding the mortality and morbidity of stroke in the U.S.
Understand the two major types of strokesRecognize 5 stroke signs/symptomsLearn risk factors for strokeUnderstand treatment options for strokeUnderstand the role of TPA in the treatment
of acute ischemic strokeUnderstand the importance of EMS in the
stroke system of care

Financial Disclosures
None (unfortunately)

Stroke Mortality
Stroke is the 4th leading cause of death, killing over 160,000 Americans annually
Approximately 795,000 strokes occurs in the United States each year
Someone in the U.S. has a stroke every 40 seconds
Someone in the U.S. dies of a stroke every 4 minutes

Burden of Stroke
Stroke is the number one reason for nursing home admission
7 million survivors of stroke >20 years oldUp to 74% of stroke survivors require
assistance with activities of daily living from informal caregivers
Direct / indirect costs of stroke in 2010 in the U.S. were estimated at $73.7 BILLION dollars

Personal Impact of Stroke

EMS and Outcomes
Diagnoses in which EMS plays huge part in patient outcomes Major Trauma Cardiac Arrest Acute MI Stroke

Types of Stroke
Ischemic Clot/plaque blocks flow
Hemorrhagic Blood vessel leaks =
bleeding

Mimics of Stroke
Alcohol intoxicationIntracranial or systemic infectionsMedication reactionsLow or high blood surgarMigrainesEpilepsyTumorsDementiaMultiple Sclerosis

Types of Stroke

Transient Ischemic Attacks (TIAs)
Commonly called “mini-strokes”200,000 – 500,000 in the U.S. per yearIncidence increased with ageSymptoms are same as for stroke, but are
temporary and resolve without detectable tissue damage
9% - 20% will go on to have stroke within 90 days
Immediate medical attention required

Modifiable Risk Factors
HTNCAD/Carotid Disease/PVDAtrial FibrillationDiabetesObesityHigh Cholesterol/DietLack of exerciseETOH/Drug abuseCoagulopathy- Cancer, Sickle Cell AnemiaPFO- Patent Foramen Ovale

Non-modifiable Risk Factors
Age->55Race: African Americans have 2x the risk of
death and disability. Asians have 1.4x the risk of death and disability.
Sex: 9% greater chance in men. 61% of stroke deaths occur in women Kills more women than breast, ovarian, uterine and
cervical cancer combinedPrevious Stroke or TIAFamily History of Stroke

Not Just For Old People
Prevalence of hospitalization for AIS increased significantly in those <44 years old 53% increase med 15 – 34 47% increase in men 35 – 44 36% increase in women 35 – 44
Nearly 25% of strokes occur in people <65 years old

Ischemic Stroke
87% of strokesOccurs when a blood vessel supplying
the brain becomes blockedWithout oxygen cells in the brain
began to die in minutesWithout reversal of the occlusion over
time more cells die and brain function in that area is permanently lost

Signs and Symptoms of AIS
Weakness (hemiparesis) of the face, arm or leg – especially on one side of the body (unilateral)
Unilateral sensory deficitVisual deficits (blindness, gaze palsy, diplopia)Speech (slurred – a motor dysfunction)Language (aphasia – damage to the brain’s
speech center)Ataxia (lack of coordinated movement)Cognitive impairment

Selected Stroke Syndromes
Anterior (ACA) Contralateral hemiparesis (maximal in the leg), urinary incontinence, apathy, confusion, poor judgment, mutism, grasp reflex, gait apraxia
Middle (MCA) (most common) Contralateral hemiparesis (worse in the arm and face than in the leg), dysarthria, hemianesthesia, contralateral homonymous hemianopia, aphasia (if the dominant hemisphere is affected) or apraxia and sensory neglect (if the nondominant hemisphere is affected)
Posterior (PCA) Contralateral homonymous hemianopia, unilateral cortical blindness, memory loss, unilateral 3rd cranial nerve palsy, hemiballismus

Selected Stroke Syndromes
Ophthalmic artery (branch of the MCA)
Monocular loss of vision (amaurosis)
Vertebrobasilar system Unilateral or bilateral cranial nerve deficits (eg, nystagmus, vertigo, dysphagia, dysarthria, diplopia, blindness), truncal or limb ataxia, spastic paresis, crossed sensory and motor deficits*, impaired consciousness, coma, death (if basilar artery occlusion is complete), tachycardia, labile BP
Lacunar infarcts Absence of cortical deficits plus one of the following:Pure motor hemiparesis Pure sensory hemianesthesiaAtaxic hemiparesisDysarthria–clumsy hand syndrome

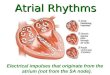
Time is Brain!!
Penumbra is a potentially
salvageable area the surrounds the core infarct zone
The core infarct zone expands over time
Every hour without treatment in AIS causes 120 million neurons to be lost and ages the brain by 3.6 years

Time frame Neurons lost Ages the brain by
Every second 32,000 8.7 hours
Every minute 1.9 million 3.1 weeks
Every hour 120 million 3.6 years
10 hours† 1.2 billion 36 years
Time is Brain!!

Hemorrhagic Stroke
13% of strokesCerebral blood vessel ruptures or
leaksNon-traumatic causes
Hypertension Subarachnoid hemorrhage Anticoagulant therapy Clotting disorders
More likely to result in death or severe disability
35-52% dead within 1 month (½ of those within 48 hours)
Only 10% living independently in 1 month; improves to only 20% within 6 months


Risk Factors for Hemorrhagic Stroke
HypertensionAdvancing ageCoagulation disorders & therapyETOH abuseDrug use (meth, cocaine, crack, etc.)Ischemic stroke—hemorrhagic transformation

Signs and Symptoms Hemorrhagic Stroke
Presentation can be identical to ischemic stroke
Sudden—signs over minutes to hoursHeadache (SAH thunderclap, worse headache
of life)Nausea and vomitingDecreasing LOCExtremely elevated blood pressure

Subarachnoid Hemorrhage
Acute bleeding around the outside of the brain and into the subarachnoid space
Usually from an aneurysm or arteriovenous malformation.
Statistics: 50% are fatal 1-15% die before reaching the hospital Those who survive are often impaired 1-7% of all strokes
Treatment is neurosurgery

AIS vs. Hemorrhagic Stroke
often high BPrare ↓LOCrare or vague H.A.rare nausea &
vomitingoften wake up with
the symptoms
usually very high BP↓ LOC~ 50% of the
time H.A.~ 40% of the
timeVomiting~50% of
timewake up with
symptoms only ~15%FINAL DIAGNOSIS MADE BY CT!!!

EMS and Stroke
50% of stroke patients call 911Ability to asses stroke vs. mimics
HypoglycemiaCollection of key information which guide
treatment Onset (Time Last Known Well) Meds (Anticoagulants) Blood pressure
Direct patient destinationActivate the stroke teamPrehospital Management and Stabilization

EMS and Stroke: Time is Brain
NAEMSP believes that: Expeditious EMS dispatch and response should occur. EMS personnel should be knowledgeable in the assessment,
management and triage of suspected stroke patients. Personnel should be skilled in the performance of pre-hospital stroke screening and in determining the timing, onset and nature of symptoms.
EMS personnel should communicate with the receiving facilities as soon as possible.
Evidence-based EMS protocols should be consistent with local/regional resources.
EMS systems and medical directors should develop local/regional strategies for treating, triaging and transporting patients with acute stroke symptoms -- including the identification of stroke-ready centers and criteria for patients who should be transported to such centers

EMS Treatment Recommendations
Dispatch Time Turnout Time Travel Time On-scene Time
Time call received to time
EMS unit notified to respond
Time EMS unit notified to time wheels move
Time until EMS arrives on scene
Time spend with patient before
start of transport
<1 minute <1 minute =Time for trauma or
MI calls
<15 minutes
Dispatch Diagnosis of stroke by emergency medical dispatchers and its
impact on the prehospital care of patients Caceres, et al. J Stroke Cerebrovasc Dis. 2013 Nov;22(8):e610-4.
67,844 strokes identified by EMS (52.5 % by dispatch) Advanced Life Support dispatched Help and Instructions offered to caller Arrived at facility in shorter time

EMS Treatment Recommendations
CABs Oxygen as needed & reduce hypercapnea (↑CO2 = ↑
ICP) Prevent aspiration (Remember: 50% of ICH patients
vomit and have ALOC)Establish / record time Last Known WellBring witness, family member or caregiver to hospital.
If not, get name and cell number of witness or family – even if “coming right on”
Bring or record all medications. Especially any “blood thinners”

Cincinnati Pre-hospital Stroke Scale
Most widely used system to assess for stroke in the pre-hospital setting
Test includes Facial droop – ask patient to smile – abnormal if one side does
not move as well Arm drift – ask patient to hold both arms out for 10 seconds -
abnormal if one arm drifts compared to other or doesn’t move Slurred speech – ask patient to repeat simple sentence –
abnormal if speech is slurred, inappropriate or mute Time last known well / Time to get to stroke-ready hospital
Sensitivity of one deficit for acute stroke is 66%, all three 87%
Formal screening algorithm can increase paramedic detection of stroke to >90%

EMS Treatment of Stroke
Rapid transport to closest stroke-ready hospital Guidelines support bypassing hospitals without stroke
resources if stroke center is within reasonable transport range
Air transport when indicatedAlert receiving ED as soon as possibleCheck & record blood glucose en routeCheck & monitor blood pressure en routeCardiac monitor, IV access en routeSeizures can be treated with valium or ativan

Radio Report ED Handoff
Keep it briefCode Stroke
Symptom CSS
LKWTVital Signs
SymptomsLKWT
Instead of time of symptom onset
Onset is often unknown Witnesses, contact info
Pertinent PMHxVital Signs, GlucoseExam
Stroke Handoff

Stroke Hospitals
Primary stroke center (PSC) Acute stroke teams, stroke units, written care protocols and
an integrated emergency response system Support services including 24/7 CT (including interpretation)
and rapid lab testing 2011 Brain Attack Coalition guidelines reiterate EMS
transport to nearest PSCComprehensive stroke center
Personnel with specific expertise in many disciplines including neurosurgery and vascular neurology
Advanced neuroimaging such as MRI and cerebral angiography
Surgical and endovascular techniques ICU and stroke registry

Stroke Hospitals
Telestroke hub or spoke Uses technology to connect patients & physicians to
remote specialists via: Telephone/Internet connection Videoconferencing Teleradiology
Telestroke is the use of telemedicine for stroke care Neurologists use an audio/video connection to evaluate
and recommend treatment for patients in a remote ED

Mississippi Certified Primary Stroke Centers
Anderson Memorial Hospital (Meridian)Memorial Hospital at GulfportMiss. Baptist Medical Center (Jackson)North Miss. Medical Center (Tupelo)Singing River Hospital (Pascagoula)St. Dominic (Jackson)UMMC (Jackson)MEMPHIS: Baptist Memphis, UT Methodist,
St. Francis

The Thrombolytic Timeline
0 10 20 30 40 50 60 70 80 90
911

Use of Thrombolytics in AIS
TPA (Alteplase) is FDA approved and indicated for the management of acute ischemic stroke
FDA approval is for treatment initiated within 3 hours of onset of symptoms ECASS-III study has shown TPA may be beneficial
up to 4.5 hours after onset of symptoms with additional restrictions; is not currently FDA approved
Patient must meet strict inclusion and exclusion criteria
Requires a rapid, coordinated response

Thrombolytics for AIS Inclusion Criteria
18 years or olderDemonstrate a measurable neurologic deficit
as defined by the National Institute of Health Stroke Scale (NIHSS)
Confirmed diagnosis of acute ischemic strokeCan be treated with 3 hours of stroke
symptom onset Recent ECASS-III shows up to 4.5 hours with
additional exclusion criteria

Thrombolytics for AIS Exclusion Criteria
Evidence of ICH on CTSuspicion of SAH on pretreatment evaluationSerious head trauma or stroke (prior 3 months)Recent intracranial or intraspinal surgery (past 2
weeks)History of ICH (ever)Arterial puncture in a noncompressible site within
past 7 daysMultilobar infarction on CT (>1/3 cerebral territory)Uncontrolled hypertension at time of treatment (SBP
> 185 mm/Hg or DBP > 110mm/Hg) despite 2 doses of medications

Thrombolytics for AIS Exclusion Criteria
Seizure at onset of strokeActive internal bleedingIntracranial neoplasm, arteriovenous
malformation, or aneurysmKnown bleeding diathesis
Platelet count <100K Heparin within last 48 hours with elevated aPTT Current use of Xa inhibitors Current use of anticoagulant with INR > 1.7 or PT >
15 secsBlood glucose <50 mg/dL or >400 mg/dL

Thrombolytics Warnings
Minor or rapidly improving neurological deficitsPregnancyMajor surgery or serious trauma with previous 14
daysSevere neurological deficit (NIHSS > 22 at
presentation)GI/Urinary tract hemorrhage within previous 21
daysAcute MI within past 3 months

NIHSS
Level of Consciousness A) LOC Responsiveness B) LOC Questions C) LOC Commands
Horizontal Eye Movement Visual field test Facial Palsy Motor Arm Motor Leg Limb Ataxia Sensory Language Speech Extinction and Inattention
Score [3] Stroke Severity
0 No Stroke Symptoms
1-4 Minor Stroke
5-15 Moderate Stroke
16-20Moderate to Severe
Stroke
21-42 Severe Stroke

Thrombolytics Outcomes in AIS
The NINDS tPA study was the landmark study that use of thrombolytics in AIS is based
Thrombolytics showed statistically significant improvement on all 4 outcome measures in Part 2 of NINDS
Patients treated with thrombolytics were at least 33% more likely to achieve minimal or no neurologic disability at 90 days versus those given placebo
AIS patients given thrombolytics had 6.4% incidence of intracranial hemorrhage vs. 0.65% in the placebo group
Mortatlity at 90 days was 17.3% in the thrombolytic group vs. 20.5% in the placebo group

Intra-arterial Treatment of AIS
Endovascular therapyPerformed by neuro-interventionalistDevices that actually remove the clot
from the artery MERCI, Penumbra, Solitaire, Trevo
Can be considered in patients in which TPA contraindicated TPA is not successful or predicted not to be
successful Past TPA timeline – up to 8 hours

Clot Retrieval

In Summary
Dispatch rapidly with pre-arrival instructionsRespond rapidlyMinimize on-scene timeHistory of event, preferably with a witnessBrief assessment such as the Cincinnati ScaleTriage, stabilize and treat the stroke patientMaintenance of circulation, airway and breathingHigh-priority transport – air transport when indicatedAppropriate destination – closest stroke-ready hospitalEarly notification of receiving ERPresent patient to ED with reportThe best stroke care is a coordinated multi-disciplinary
approach

Questions