Embed Size (px)
Citation preview

DATA QUALITY MANAGEMENT CONTROL
PROGRAM
Data Quality Section, PASBA

2
Overview
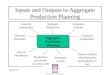
Regulatory Guidance Program Management Organizational Factors System Inputs, Processes, and Outputs
CHCS ADM MEPRS/EAS TPOCS MEWACS
Patient Records Accountability
Coding Audits Sampling Size and Techniques Inpatient Records Outpatient Records
Workload Comparison System Security System Design,
Development, Operations, and Education and Training

Regulatory GuidanceDODI 6040.40
Military Health System Data Quality Management Control Procedures
3
Department of Defense
INSTRUCTION

Regulatory GuidanceDODD 6040.41
Medical Records Retention and Coding at Military Treatment Facilities
4
Department of Defense
DIRECTIVE

Regulatory GuidanceDODD 6040.42
Medical Encounter and Coding at Military Treatment Facilities
5
Department of Defense
DIRECTIVE

Regulatory GuidanceDODD 6040.43
Custody and Control of Outpatient Medical Records
6
Department of Defense
DIRECTIVE

Program Management
Data Quality Manager Data Quality Assurance Team Intermediate Command DQ Manager Service Data Quality Manager DQMC Review List Commanders Monthly Data Quality
Statement (internet based)
7

System Inputs, Processes, and Outputs
Composite Health Care System (CHCS) Armed Forces Health Longitudinal
Technology Application (AHLTA) Ambulatory Data Module (ADM) Medical Expense and Performance
Reporting System (MEPRS) / Expense Assignment System (EAS)
MEPRS Early Warning and Control System (MEWACS)
Defense Medical Human Resources System –Internet (DMHRS-i)
Third Party Outpatient Collection System (TPOCS)
8

Data InputMEPRS/EAS, ADM, CHCS, TPOCS Written Procedures Current Versions Upgrades & Updates Rejected Records End of Day Processing
Percentage of Clinics Percentage of Appointments
Timely Coding Completion
9

Commander’sData Quality Statement
Q. 1. What percentage of appointments was closed in meeting your “End of Day” processing requirements, “Every appointment – Every day?” (B.5.)
10

Commander’sData Quality Statement
Q. 2. In accordance with legal and medical coding practices, have all of the following occurred: a) What percentage of Outpatient Encounters,
other than APVs, have been coded within 3 business days of the encounter? (B.6.(a))
b) What percentage of APVs have been coded within 15 days of the encounter? (B.6.(b))
c) What percentage of Inpatient records have been coded within 30 days after discharge? (B.6.(c))
11

Data OutputMEPRS/EAS, ADM, CHCS, TPOCS
EAS Financial Reconciliation Inpatient and Outpatient Workload
Reconciliations MEWACS Review Timely Data Transmittal Workload Comparison
12

Commander’sData Quality Statement
Q. 3. Medical Expense and Performance Reporting System for Fixed Military Medical and Dental Treatment Facilities Manual (MEPRS Manual) DoD6010-13-M, dated April 7, 2008, paragraph C3.3.4, requires report reconciliation (C.1.)
a) Was monthly MEPRS/EAS financial reconciliation process completed, validated and approved prior to monthly MEPRS transmission?
13

Commander’sData Quality Statement
Q. 3. Medical Expense and Performance Reporting System for Fixed Military Medical and Dental Treatment Facilities Manual (MEPRS Manual) DoD6010-13-M, dated April 7, 2008, paragraph C3.3.4, requires report reconciliation (C.1.)
b) Were the data load status, outlier/variance, WWR-EAS IV, and allocations tabs in the MEWACS document reviewed and explanations provided for flagged data anomalies?
14

Commander’sData Quality Statement
Q. 3. Medical Expense and Performance Reporting System for Fixed Military Medical and Dental Treatment Facilities Manual (MEPRS Manual) DoD6010-13-M, dated April 7, 2008, paragraph C3.3.4, requires report reconciliation (C.1.)
c) For DMHRS-i, what is the percentage of timecards submitted by the suspense date?
d) For DMHRS-I, what is the percentage of approved timecards by the suspense date?
15

Data OutputMEPRS/EAS, ADM, CHCS, TPOCS CHCS
Duplicate Records Timely Data Transmittal
Standard Inpatient Data Record (SIDR) Worldwide Workload Report
Inpatient Records Accountability Documentation Coding SIDRs completed (in a “D” status)
Workload Comparison
16

Commander’sData Quality Statement
Q. 4. Compliance with TMA or Service-Level guidance for timely submission of data (C.3.).
a) MEPRS/EAS (45 calendar days)
17

Commander’sData Quality Statement
Q. 4. Compliance with TMA or Service-Level guidance for timely submission of data (C.3.).
- b) SIDR/CHCS (5th and 20th calendar day of the month)
18

Commander’sData Quality Statement
Q. 4. Compliance with TMA or Service-Level guidance for timely submission of data (C.3.).
- c) WWR/CHCS (10th calendar day following month)
19

Commander’sData Quality Statement
Q. 4. Compliance with TMA or Service-Level guidance for timely submission of data (C.3).
d) SADR/ADM (daily)
20

Data Output
A minimum of 30 records/encounters should be pulled randomly from the entire population of MTF inpatient medical records for the audit data month.
A random audit of 30 records per MTF will provide a statistical confidence level of 90%, with a confidence interval/sampling error range of plus or minus 15%.
The PASBA is generating a monthly DD Form 2569 audit pull-list for auditing of other health insurance .
21

Data OutputInpatient Coding
Coding DRG Codes Related Data Elements (C.5)
All Diagnoses Any Procedures Sex Age Discharge/Disposition
Percentage of SIDRs Completed (D-Status)
22

Commander’sData Quality Statement
Q. 5. Outcome of monthly inpatient coding audit: (C.5.c.f.g,h,i,j)
a) What percentage of inpatient records
whose assigned DRG codes were correct?
23

Commander’sData Quality Statement
Q. 5. Outcome of monthly inpatient coding audit: (C.5.c.f.g,h,i,j)
b) Inpatient Professional Services Rounds encounters E & M codes audited and deemed correct?
24

Commander’sData Quality Statement
Q. 5. Outcome of monthly inpatient coding audit: (C.5.c.f.g,h,i,j)
c) Inpatient Professional Services Rounds encounters ICD-9 codes audited and deemed correct?
25

Commander’sData Quality Statement
Q. 5. Outcome of monthly inpatient coding audit: (C.5.c.f.g,h,i,j)
d) Inpatient Professional Services Rounds encounters CPT codes audited and deemed correct?
26

Data OutputMEPRS/EAS, ADM, CHCS, TPOCS
ADM Timely Data Transmittal
Standard Ambulatory Data Record (SADR) Error Logs Workload Comparison
27

Data OutputOutpatient Coding
Sample Size Accountability
Percentage Located or Properly Checked Out Checked-out Over 30-Days?
DD Form 2569 (Third Party Insurance Information)
28

Commander’sData Quality Statement
Q.6. Outpatient Records. (c.6.a,b,c,d,e,f)
a) Is the documentation of the encounter selected to be audited available? Documentation includes documentation in medical record, loose (hard copy) documentation or an electronic record of the encounter in AHLTA?
29

Data OutputOutpatient Coding
E&M Codes ICD-9 Codes CPT Codes
30

Commander’sData Quality Statement
Q. 6. Outpatient Records.
b) What is the percentage of E & M codes deemed correct? (E & M code must comply with current DoD guidance.)
31

Commander’sData Quality Statement
Q. 6. Outpatient Records.
c) What is the percentage of ICD-9 codes deemed correct?
32

Commander’sData Quality Statement
Q. 6. Outpatient Records.
d) What was the percentage of CPT codes deemed correct? (CPT code must comply with current DoD guidance.)
33

Commander’sData Quality Statement
Question 7 Ambulatory Procedure Visits (C.7.a,b,c)
Questions 7.a,b,c, are the same as Questions 6.a,c,d,,
34

Commander’sData Quality Statement
Q. 8. Outcome of monthly inpatient audit: (C.8a,b,c,d,e,f)
a) What percentage of completed and current (signed within the past 12 months) DD Form 2569s are available for audit?
b) What percentage of available, current and complete DD Form 2569s are verified to be correct in the Patient Insurance Information (PII) module in CHCS?
35

Commander’sData Quality Statement
Q. 8. Outcome of monthly outpatient audit: (C.8a,b,c,d,e,f)
c) What percentage of completed & current (signed within the past 12 months) DD Form 2569s (TPC Insurance Info) are available for audit?
d) What percentage of available, current and completed DD Form 2569s are verified to be correct in the Patient Insurance Information (PII) module in CHCS?
36

Commander’sData Quality Statement
Q. 9. Comparison of reported workload data (C.9).
a) # SADR Encounters (count only visits / # WWR visits
b) # SIDR Dispositions / # WWR Dispositions c) # EAS Visits / # WWR Visits d) # EAS Dispositions / # WWR Dispositions e) # IPSR SADR encounters (FCC=A***)/# Sum
WWR (Total Bed Days + Total Dispositions + Live Births + Bassinet Days)
Note: Question e, FY11 Goal is 80%.
37

Data OutputWorkload Comparison
Q.9a SADR Visits / WWR Visits
Should have an equal number of visits. Encounters – Omit Appt. Status of “No-
Shows,” “Canceled,” and Disposition Code “Left Without Being Seen”.
Encounters – Include Appt. Status “TelCon” Only SADR Records Marked with an Appt.
Status of “C” (complete) Are To Be Included. Only “count” encounters are included.
38

Data OutputWorkload Comparison
Q.9b SIDR Dispositions / WWR Dispositions
Must Match Only SIDRs With a Disposition of Status of “D”
Are To Be Included SIDRs – Exclude Carded for Record Only (CRO)
and Absent Sick Records
39

Data OutputWorkload Comparison
Q. 9c EAS Visits / WWR Visits
Must Match Include MEPRS Functional Cost Code B**
(Outpatient) and FBN (Hearing Conservation) Include APVs
40

Data OutputWorkload Comparison
Q. 9d EAS Dispositions / WWR Dispositions
Must Match Only SIDRs with a Disposition Status of “D”
are to be included
41

Data OutputWorkload Comparison
Q. 9e IPSR encounters (FCC=A***)/# Sum WWR (Total Bed Days + Total Dispositions + Live Births + Bassinet Days) Must Match Only SIDRs with a Disposition Status of “D” are
to be included. Insure WWR calculation includes live births
(section 01) and Bassinet Days (section 00).
Note: FY11 Goal is 80%
42

Commander’sData Quality Statement
Q.10. - System Design, Development, Operations and Education/Training (E.4.i).
# AHLTA SADR encounters/# of Total SADR encounters
Note: FY11 compliance goal is 95%.. (* It is understood that not all clinical
modules are deployed in the current version of AHLTA.)
43

Commander’sData Quality Statement
Q.11.- CHCS software used during the data month to identify duplicate patient registration records. (C.2a)
- What was the number of potential duplicate records in the reporting month?
44

Commander’sData Quality Statement
Q.12.- Provide the number of incomplete and non-transmitted SIDRs for the month. (F.1)
Note: This question on the DQ Statement is only a requirement for Army sites and will not be reported to TMA.
45

Commander’sData Quality Statement
Q.13.a.- Provide the number of loose forms/documents/papers that are currently waiting to be filed, either electronically or in the hard-copy medical record. (F.2.a)
Note: This question on the DQ Statement is only a requirement for Army sites and will not be reported to TMA.
46

Commander’sData Quality Statement
Q.13.b.- Provide the number of loose forms/documents/papers that are currently waiting to be filed, either electronically or in the hard-copy medical record, 30 days after an active duty soldier has retired or separated from the service. (F.2.b)
Note: This question on the DQ Statement is only a requirement for Army sites and will not be reported to TMA.
47

Commander’sData Quality Statement
Q. 14. – I am aware of data quality issues identified by the completed Commander’s Statement and Review List and when needed, have incorporated monitoring mechanisms and have taken corrective actions to improve the data from my facility.
48

Security
Are there internal controls and procedures in place to approve and manage assignment of security key privileges?
Have all security key holders been identified and their need for security key privileges validated by the CIO or designee?
49

System Design, Operations, and Education/Training
System Administrator Appointed In Writing for Each System
Training and Education Procedures and Documentation
System Change Request Process System Incident Report Routine Maintenance Points of Contact for Equipment Failure
Issues Contingency Plans Trouble tickets
50

52
BACKUP SLIDES

53
METRIC MANIA
Department of Army
Strategic Readiness System(SRS)
Review &
Analysis
TMA metrics
BALANCED SCORECARD
- Promote, Sustain and Enhance Soldier Health- Train, Develop and Equip a Medical Force that Supports Full Spectrum Operations - Deliver Leading Edge Health Services to Our Warriors and Military Family to Optimize Outcomes
For more information go to: https://ke2.army.mil/bscThis is a dynamic, living document
America’s Premier Medical Team Saving Lives and Fostering Healthy and Resilient PeopleArmy Medicine…Army Strong!
Pat
ien
t/C
ust
om
er/
Sta
keh
old
er CS 6.0 Inspire Trust in
Army Medicine
CS 4.0 Responsive Battlefield
Medical Force
CS 1.0 Improved Healthy and Protected
Families, Beneficiaries and
Army Civilians
CS 3.0 Improved Healthy and Protected Warriors
CS 5.0 Improved Patient and Customer
Satisfaction
IP 10.0 Optimize Medical
Readiness
IP 13.0 Build Relationships and Enhance Partnerships
LG 18.0 Improve Training and Development
IP 11.0 Improve Information
Systems
CS 2.0 Optimized Care and Transition of Wounded, Ill, and
Injured Warriors
IP 12.0 Implement
Best Practices
IP 14.0 Improve Internal and
External Communication
LG 20.0 Improve Knowledge
Management
LG 17.0 Improve Recruiting and
Retention of AMEDD Personnel
Inte
rna
l P
roce
ssL
ea
rnin
g
an
d G
row
th
LG 19.0 Promote and Foster a
Culture of Innovation
Maximize Value in Health Services
Provide Global Operational Forces Build the Team Balance Innovation
with StandardizationOptimize Communication and
K nowledge Management
Fee
db
ack
Ad
jus
ts R
eso
urc
ing
De
cisi
on
s
IP 8.0 Improve Quality,
Outcome-Focused Care and Services
IP 7.0 Maximize Physical and Psychological
Health Promotion and Prevention
IP 9.0 Improve Access and Continuity of
Care
IP 16.0 Synchronize
Army Medicine to Support Army
Stationing & BRAC
R 21.0 Optimize
Resources and Value
R 22.0 Optimize Lifecycle Management
of Facilities and Infrastructure
R 23.0 Maximize
Human Capital
EN
DS
ME
AN
SW
AY
S
Re
sou
rce
IP 15.0 Leverage Research,
Development and Acquisition
= CofS Accountability
OTSG
Command Management System(CMS)
Why should you care? What can you do to help?

54
MEDCOM STRATEGY MAP
GOALS:
• Improve overall health & wellness of enrolled beneficiaries.
• Improve patient access and satisfaction.
• Improve effectiveness of peacetime direct care system.

55
KEYS TO SUCCESS
• Improve Data Quality Efforts
• Cultural Change
• Improve Access to Care
• Tie Financing to PerformancePBAM – Performance Based Adjustment Model

Army Health System
MedicalGreen-Suit
Military
Total MEDCOMDHP Human Resources
WT Population ~ 12,000
Population Requiring Healthcare (Demand)
MEDCOM Capacity (Human Capital)
MEDCOM direct care capacity cannot meet the Healthcare demand of the around 3 million eligible beneficiaries (MEDCOM cares for 1.414 million enrolled & 300K users)
Reasons include: -Population dispersion (especially among Retirees & their Families) -Efficiency demands (numerous small population centers) -Military structure supports Readiness – not peacetime healthcare
AD
ADFM
65+
Ret/RetFM (<65)
Army Health System

23% 63% 1%24% 67% 7%24% 63% 11%24% 65% 9%25% 66% 6%26% 67% 7%27% 62% 9%27% 61% 9%28% 63% 8%28% 65% 6%28% 61% 9%30% 59% 9%30% 62% 6%31% 61% 7%32% 61% 6%33% 60% 7%33% 59% 7%33% 58% 7%35% 61% 4%38% 58% 4%
47% 48% 4%61% 36% 3%Tricare/military
Kaiser PermanenteAARP
MedicareMedicaid
BCBS of MichiganCare first BCBS
PacifiCare/ SecureHumana
Medicare and Part DOther health plan
AnthemHighmark
Blue Cross & Blue ShieldWellPoint
UnitedHealthecare-NetBCBS of Illinois
CoventryAetnaCigna
Health Care Services CorpUnitedHealcare
Highly satisfied Satisfied Dissatisfied Highly dissatisfied
Overall satsfation with health plan
Overall Satisfaction With Health Plans
“And the Winner is…” Managed Care Magazine, September 2008 pp 41-46
Data -Wilson Health Information LLC Annual Survey Jan-Feb 2008

58
DATA QUALITY
• Increased emphasis on MTF submissions
• Improved reporting timeliness
• Improved accuracy SIDRs
SADRs
MEPRS

59
• Combines Multiple Data Systems• Current Enrollment (ECM)- Assumes Historical Space-A
work• Potential Enrollment (MTF Business Plans)• EBSM- Forecast population changes• Ops- UNCLASSIFIED Deployments and Redeployments by
location by month• ARTS- Deployed personnel from MTF
• Provides Adjusted Enrollment for those Active duty deployed, and redeploying
• Adjusts MTF enrollment capacity based on deployed PCMs (1000/Per deployed PCM)
• Future Development to include:• Adjustments for Backfilling PCMs from another MTF• Forecast ARTS deployments- (Pending Deployments)• Deployment to CMS
Enrollment Capacity Forecast Model (ECFM)

60
USE OF THE DATA
TMA = Gospel
“Garbage In, Garbage Out”
OTSG = Disaster
MTF = Nuclear Fire Storm

61
• The data matter
• Cultural shift
• Use the CMS
• Ask: What are we asking our staff to do?
Priorities

62
Standardize Core R&A for Medical Treatment Facilities
• No standard R&A approach in MEDCOM
• MTF Cdrs create their own “TOC”
• MTF’s spend a lot of time designing/developing
the “TOC”
• Cdrs and staffs learn together at the expense
of
Organizational Performance
• R&A provides the Azimuth….critical to direction
and success

63
Core Measures for MTFs
• Enrollment
• Productivity
• Access
• Patient Satisfaction
• Coding Accuracy
• Prevention/HEDIS

64
End-of-Day (EOD) Processing MTF staff will determine the status of each appointment as accurately as possible. EOD processing will be correctly completed at the end of each business day.
Pending: The MTF appointment information system assigns this initial status for an appointment that has been booked for a patient for a future date or time. All pending appointments must be changed to one of the final encounter statuses in order to complete End-of-Day processing.
Kept: The patient has a booked appointment, arrives at the MTF/clinic, and is treated by provider.
Walk-in: The patient does not have a scheduled appointment, arrives at the clinic, and is assigned a time to see the provider the same day. This status will not be changed at End-of-Day processing.
Sick Call: An Active Duty member arrives at a clinic for a pre-arranged block of time for care. This status will not be changed at End-of-Day processing.

65
End-of-Day (EOD) ProcessingPatient Cancellation: A patient with a scheduled appointment notifiesThe MTF in accordance with local procedures that they will not keep the appointment.
No-Show: A scheduled appointment that the patient does not keep. Determinations of no-shows will be in accordance with local procedures.
Facility Cancellation: The MTF cancels an available/open appointmentor cancels a patient’s scheduled appointment.
Left Without Being Seen: The patient has a booked appointment, arrivesat the clinic, and is checked in, but decides to leave without seeing the provider.
Admin: The admin status is used on appointments or telephone consultsthat do not represent actual contact with a patient. The status must beAssigned in End-of-Day processing. A transaction with this status will not bepassed to ADM or AHLTA and will not be coded or included in SADR.

66
End-of-Day (EOD) ProcessingOccasions of Service: This status on a patient appointment indicates nomedical decision was made by a privileged provider who is directly Responsible for the management of care for the patient. This status willno longer be used on telephone consults. This transaction will pass fromCHCS to the Ambulatory Data Module (ADM), is always non-count, and maybe used to assess level of effort. ADM and AHLTA do not recognize this status as an appointment for completion. Therefore this status will NOT prompt the provider to code the encounter and will avoid generating a Standard Ambulatory Data Record (SADR).
Telephone Consultation: When a provider answers a telephone consult inAHLTA, the provider will be asked by the system, “Does this meet the out-patient visit criteria?” If the provider is a technician, nurse, or other non-count provider or the clinic is a non-count clinic, the workload type responsewill be defaulted to No (non-count) and cannot be changed in AHLTA. If the provider is a privileged provider and the clinic is a count clinic, the defaultwill be Yes (count). The provider should change the response to No if it does not meet the visit criteria.

67
Walk-ins 1. A walk-in is a patient who seeks care without a scheduled appointment,Arrives at the clinic, and is assigned a time to see the provider the same day.
2. There is no ATC Standard for walk-in appointments.
3. Walk-ins are not designed for use as a schedulable event.
4. High utilization of walk-ins can create data quality challenges for the MTF and make the process of measuring/explaining access, and assessing demand more complex.
5. High rates of walk-ins may also make business plan targeting difficult since theyare unplanned events.
6. Excessive walk-in activity can reduce the appointments available to patientsrequesting care on the telephone.
7. However, if clinics utilize the walk-in function to get patients seen in a manner that is more timely/convenient for the patients, this is recognized as good customerservice from the patient’s perspective.

68

69
Medical Expense and Performance Reporting System (MEPRS)
1. The DoD Manual 6010.13-M, MEPRS for Fixed Medical and Dental TreatmentFacilities. Provides a definition of MEPRS codes (also know as functional costcodes, FCC).
2. Define your CHCS File-and-Build Hospital Locations so that each clinic has only one associated MEPRS code.
3. Ensure that each MEPRS code has the four characteristics of: a. A defined physical space (e.g., square footage) b. Associated expenses (e.g., supplies) c. Associated personnel time (e.g., work hours) and d. Associated workload (e.g., visits, procedures, etc.)
4. Manual provides definition and criteria of a visit (count vs. non-count)
5. Defense Medical Human Resources System – internet (DMHRS-i), there has been significant improvement in timecard reporting. Need to pay attention to the accuracy of the information being entered into the system.

70https://pasba3.amedd.army.mil/login/login.fcc

71

72

73

74

75

76

77

78

79
1) In the data month (include only B*** and FBN* accounts): a) What percentage of appointments were closed in meeting your “End of Day” processing requirements, “Every appointment – Every day?”
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 100% 100%
ERMC 99% 99%
0606 - HEIDELBERG 100% 100%
0607 - LANDSTUHL 99% 99%
0609 - VILSECK 100% 100%
NRMC 100% 100%
0037 - WASHINGTON DC 100% 100%
0061 - FT. KNOX 100% 100%
0069 - FT. MEADE 99% 100%
0086 - WEST POINT 100% 100%
0089 - FT. BRAGG 100% 100%
0121 - FT. EUSTIS 100% 100%
0122 - FT. LEE 100% 100%
0123 - FT. BELVOIR 99% 100%
0330 - FT. DRUM 100% 100%
PRMC 100% 100%
0052 - FT. SHAFTER 100% 100%
0610 - CAMP ZAMA 100% 100%
0612 - SEOUL 100% 100%
SRMC 100% 100%
0001 - REDSTONE ARSENAL 100% 100%
0003 - FT. RUCKER 100% 100%
0047 - FT. GORDON 100% 100%
0048 - FT. BENNING 100% 100%
0049 - FT. STEWART 100% 100%
0060 - FT. CAMPBELL 100% 100%
0064 - FT. POLK 100% 100%
0098 - FT. SILL 100% 100%
0105 - FT. JACKSON 100% 100%
0109 - FT. SAM HOUSTON 100% 100%
0110 - FT. HOOD 100% 100%
WRMC 100% 100%
0005 - FT. WAINWRIGHT 99% 99%
0008 - FT. HUACHUCA 100% 100%
0032 - FT. CARSON 100% 100%
0057 - FT. RILEY 100% 100%
0058 - FT. LEAVENWORTH 99% 99%
0075 - FT. LEONARD WOOD 100% 100%
0108 - FT. BLISS 100% 100%
0125 - FT. LEWIS 100% 100%
0131 - FT. IRWIN 100% 100%
Legend: N/A 95% - 100% 80% - 94% 0% - 79% or No Response

80
2) In accordance with legal and medical coding practices, have all of the following occurred (see applicable DoDD/DoDI on Medical Records Retention and Coding): a) What percentage of Outpatient Encounters, other than Ambulatory Patient Visits (APVs), have been coded within 3 business days of the encounter (e.g., if the day of encounter is Monday, then coding must be completed by the third business day, Thursday, close of business)?
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 92% 93%
ERMC 96% 96%
0606 - HEIDELBERG 94% 96%
0607 - LANDSTUHL 98% 98%
0609 - VILSECK 93% 93%
NRMC 92% 93%
0037 - WASHINGTON DC 89% 89%
0061 - FT. KNOX 96% 91%
0069 - FT. MEADE 92% 93%
0086 - WEST POINT 81% 85%
0089 - FT. BRAGG 95% 97%
0121 - FT. EUSTIS 93% 95%
0122 - FT. LEE 97% 96%
0123 - FT. BELVOIR 90% 92%
0330 - FT. DRUM 93% 96%
PRMC 88% 89%
0052 - FT. SHAFTER 88% 89%
0610 - CAMP ZAMA 95% 98%
0612 - SEOUL 90% 90%
SRMC 92% 93%
0001 - REDSTONE ARSENAL 91% 92%
0003 - FT. RUCKER 96% 97%
0047 - FT. GORDON 93% 94%
0048 - FT. BENNING 96% 97%
0049 - FT. STEWART 93% 91%
0060 - FT. CAMPBELL 97% 96%
0064 - FT. POLK 91% 95%
0098 - FT. SILL 94% 96%
0105 - FT. JACKSON 93% 96%
0109 - FT. SAM HOUSTON 84% 85%
0110 - FT. HOOD 91% 91%
WRMC 92% 94%
0005 - FT. WAINWRIGHT 88% 90%
0008 - FT. HUACHUCA 95% 96%
0032 - FT. CARSON 94% 96%
0057 - FT. RILEY 98% 98%
0058 - FT. LEAVENWORTH 96% 98%
0075 - FT. LEONARD WOOD 97% 99%
0108 - FT. BLISS 89% 92%
0125 - FT. LEWIS 88% 89%
0131 - FT. IRWIN 95% 96%
Legend: N/A 95% - 100% 80% - 94% 0% - 79% or No Response

81
0 1 2 3 4 5 6-7 8-1415-21
22-2829-60
61-9091-120
>120
0%
20%
40%
60%
80%
100%
120%
Time to Completion of Outpatient Encounters - FY 2009(Overall)
1st Quarter (2008/10-2008/12) 2nd Quarter (2009/01-2009/03) 3d Quarter (2009/04-2009/06) 4th Quarter (2009/07-2009/09)
Time (Days) to Completion
% E
ncou
nter
s Com
plet
ed in
Tim
e In
terv
al
see detail of percentage encoun-ters closed after 2 weeks...

82
8-14
15-21
22-28
29-60
61-90
91-120
>120
93.0%
94.0%
95.0%
96.0%
97.0%
98.0%
99.0%
100.0%
Time to Completion of Outpatient Encounters(among encounters lasting more than 1 week)
1st Quarter (2008/10-2008/12) 2nd Quarter (2009/01-2009/03) 3d Quarter (2009/04-2009/06) 4th Quarter (2009/07-2009/09)
Time (Days) to Completion
% E
ncou
nter
s Com
plet
ed in
Tim
e In
terv
al

83
2) In accordance with legal and medical coding practices, have all of the following occurred (see applicable DoDD/DoDI on Medical Records Retention and Coding): b) What percentage of APVs has been coded within 15 calendar days of the encounter?
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 94% 93%
ERMC 98% 98%
0606 - HEIDELBERG 75% 82%
0607 - LANDSTUHL 100% 100%
0609 - VILSECK
NRMC 97% 98%
0037 - WASHINGTON DC 95% 97%
0061 - FT. KNOX 100% 100%
0069 - FT. MEADE 99% 97%
0086 - WEST POINT 90% 90%
0089 - FT. BRAGG 100% 99%
0121 - FT. EUSTIS 100% 100%
0122 - FT. LEE
0123 - FT. BELVOIR 100% 100%
0330 - FT. DRUM 22% 78%
PRMC 97% 96%
0052 - FT. SHAFTER 97% 96%
0610 - CAMP ZAMA
0612 - SEOUL 99% 95%
SRMC 86% 94%
0001 - REDSTONE ARSENAL
0003 - FT. RUCKER
0047 - FT. GORDON 46% 96%
0048 - FT. BENNING 100% 100%
0049 - FT. STEWART 92% 93%
0060 - FT. CAMPBELL 98% 100%
0064 - FT. POLK 87% 81%
0098 - FT. SILL 99% 95%
0105 - FT. JACKSON 96% 98%
0109 - FT. SAM HOUSTON 85% 87%
0110 - FT. HOOD 98% 99%
WRMC 98% 84%
0005 - FT. WAINWRIGHT 99% 100%
0008 - FT. HUACHUCA
0032 - FT. CARSON 99% 99%
0057 - FT. RILEY 99% 100%
0058 - FT. LEAVENWORTH 100% 99%
0075 - FT. LEONARD WOOD 100% 100%
0108 - FT. BLISS 95% 95%
0125 - FT. LEWIS 99% 64%
0131 - FT. IRWIN 89% 88%
Legend: N/A 95% - 100% 80% - 94% 0% - 79% or No Response

84
2) In accordance with legal and medical coding practices, have all of the following occurred (see applicable DoDD/DoDI on Medical Records Retention and Coding): c) What percentage of inpatient records has been coded within 30 calendar days after discharge (for MTFs with inpatient capability)?
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 86% 95%
ERMC 100% 100%
0606 - HEIDELBERG 0% 0%
0607 - LANDSTUHL 100% 100%
0609 - VILSECK 0% 0%
NRMC 98% 98%
0037 - WASHINGTON DC 97% 100%
0061 - FT. KNOX 100% 100%
0069 - FT. MEADE 0% 0%
0086 - WEST POINT 100% 100%
0089 - FT. BRAGG 93% 90%
0121 - FT. EUSTIS 0% 0%
0122 - FT. LEE 0% 0%
0123 - FT. BELVOIR 100% 100%
0330 - FT. DRUM 0% 0%
PRMC 100% 100%
0052 - FT. SHAFTER 100% 100%
0610 - CAMP ZAMA 0% 0%
0612 - SEOUL 100% 100%
SRMC 78% 98%
0001 - REDSTONE ARSENAL 0% 0%
0003 - FT. RUCKER 0% 0%
0047 - FT. GORDON 99% 93%
0048 - FT. BENNING 100% 100%
0049 - FT. STEWART 100% 100%
0060 - FT. CAMPBELL 100% 100%
0064 - FT. POLK 100% 99%
0098 - FT. SILL 100% 99%
0105 - FT. JACKSON 99% 100%
0109 - FT. SAM HOUSTON 0% 93%
0110 - FT. HOOD 0% 100%
WRMC 81% 85%
0005 - FT. WAINWRIGHT 100% 100%
0008 - FT. HUACHUCA 0% 0%
0032 - FT. CARSON 100% 100%
0057 - FT. RILEY 100% 100%
0058 - FT. LEAVENWORTH 0% 0%
0075 - FT. LEONARD WOOD 100% 100%
0108 - FT. BLISS 66% 97%
0125 - FT. LEWIS 99% 0%
0131 - FT. IRWIN 0% 100%
Legend: N/A 95% - 100% 80% - 94% 0% - 79% or No Response

85
Auditing for DD Form 2569, Other Health Insurance
• Non active duty only.
• MEPRs FCC of “B” and “FBN”.
• Eliminated all “B” MEPRS which have a fourth
level code of 2.
• Minimum of 50 encounters for SADRs, SIDRs,
APVs. (Encounters for parent and child MTF)
• Increased number of encounters pulled for MTFs
when requested.
• Randomly selected encounters.

86
8.a) INPATIENT DISPOSITIONS: What percentage of completed and current (signed within the past 12 months) DD Form 2569s (Third Party Collection Insurance Info) is available for audit (non-active duty encounters only)? (See DoD 6010.15-M, MTF UBO Manual)
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 96% 95%
ERMC 100% 98%
0606 - HEIDELBERG 0% 0%
0607 - LANDSTUHL 100% 98%
0609 - VILSECK 0% 0%
NRMC 95% 87%
0037 - WASHINGTON DC 97% 73%
0061 - FT. KNOX 100% 97%
0069 - FT. MEADE 0% 0%
0086 - WEST POINT 0% 100%
0089 - FT. BRAGG 83% 80%
0121 - FT. EUSTIS 0% 0%
0122 - FT. LEE 0% 0%
0123 - FT. BELVOIR 100% 97%
0330 - FT. DRUM 0% 0%
PRMC 100% 98%
0052 - FT. SHAFTER 100% 97%
0610 - CAMP ZAMA 0% 0%
0612 - SEOUL 100% 100%
SRMC 92% 99%
0001 - REDSTONE ARSENAL 0% 0%
0003 - FT. RUCKER 0% 0%
0047 - FT. GORDON 80% 100%
0048 - FT. BENNING 100% 100%
0049 - FT. STEWART 79% 100%
0060 - FT. CAMPBELL 100% 100%
0064 - FT. POLK 100% 100%
0098 - FT. SILL 100% 97%
0105 - FT. JACKSON 100% 100%
0109 - FT. SAM HOUSTON 100% 92%
0110 - FT. HOOD 100% 100%
WRMC 98% 99%
0005 - FT. WAINWRIGHT 100% 100%
0008 - FT. HUACHUCA 0% 0%
0032 - FT. CARSON 100% 93%
0057 - FT. RILEY 100% 100%
0058 - FT. LEAVENWORTH 0% 0%
0075 - FT. LEONARD WOOD 85% 100%
0108 - FT. BLISS 98% 94%
0125 - FT. LEWIS 98% 100%
0131 - FT. IRWIN 100% 100%
Legend: N/A 95% - 100% 80% - 94% 0% - 79% or No Response

87
8.c) OUTPATIENT ENCOUNTERS: What percentage of completed and current (signed within the past 12 months) DD Form 2569s (TPC Insurance Info) is available for audit (non-active duty encounters only)? (See DoD 6010.15-M, MTF UBO Manual)
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 81% 83%
ERMC 82% 75%
0606 - HEIDELBERG 87% 90%
0607 - LANDSTUHL 95% 85%
0609 - VILSECK 67% 62%
NRMC 78% 86%
0037 - WASHINGTON DC 23% 56%
0061 - FT. KNOX 97% 96%
0069 - FT. MEADE 87% 94%
0086 - WEST POINT 74% 71%
0089 - FT. BRAGG 52% 62%
0121 - FT. EUSTIS 90% 96%
0122 - FT. LEE 95% 95%
0123 - FT. BELVOIR 90% 95%
0330 - FT. DRUM 91% 91%
PRMC 90% 86%
0052 - FT. SHAFTER 90% 83%
0610 - CAMP ZAMA 100% 100%
0612 - SEOUL 81% 75%
SRMC 88% 79%
0001 - REDSTONE ARSENAL 100% 97%
0003 - FT. RUCKER 82% 74%
0047 - FT. GORDON 100% 78%
0048 - FT. BENNING 100% 93%
0049 - FT. STEWART 100% 75%
0060 - FT. CAMPBELL 100% 46%
0064 - FT. POLK 93% 90%
0098 - FT. SILL 96% 60%
0105 - FT. JACKSON 63% 70%
0109 - FT. SAM HOUSTON 42% 68%
0110 - FT. HOOD 92% 95%
WRMC 79% 82%
0005 - FT. WAINWRIGHT 100% 95%
0008 - FT. HUACHUCA 68% 70%
0032 - FT. CARSON 90% 90%
0057 - FT. RILEY 100% 100%
0058 - FT. LEAVENWORTH 58% 62%
0075 - FT. LEONARD WOOD 85% 80%
0108 - FT. BLISS 42% 36%
0125 - FT. LEWIS 64% 100%
0131 - FT. IRWIN 88% 94%
Legend: N/A 95% - 100% 80% - 94% 0% - 79% or No Response

88
8.e) APVs: What percentage of the completed and current DD Form 2569s (TPC Insurance info.) is available for audit (non-active duty encounters only)? (See DoD 6010.15M, MTF UBO Manual)
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 96% 92%
ERMC 103% 98%
0606 - HEIDELBERG 85% 100%
0607 - LANDSTUHL 96% 96%
0609 - VILSECK 0% 0%
NRMC 87% 81%
0037 - WASHINGTON DC 67% 24%
0061 - FT. KNOX 100% 100%
0069 - FT. MEADE 86% 94%
0086 - WEST POINT 0% 100%
0089 - FT. BRAGG 80% 90%
0121 - FT. EUSTIS 90% 92%
0122 - FT. LEE 0% 0%
0123 - FT. BELVOIR 97% 97%
0330 - FT. DRUM 100% 44%
PRMC 92% 93%
0052 - FT. SHAFTER 90% 87%
0610 - CAMP ZAMA 0% 0%
0612 - SEOUL 93% 100%
SRMC 100% 99%
0001 - REDSTONE ARSENAL 0% 0%
0003 - FT. RUCKER 0% 0%
0047 - FT. GORDON 100% 100%
0048 - FT. BENNING 100% 100%
0049 - FT. STEWART 100% 97%
0060 - FT. CAMPBELL 100% 100%
0064 - FT. POLK 100% 100%
0098 - FT. SILL 100% 100%
0105 - FT. JACKSON 100% 100%
0109 - FT. SAM HOUSTON 100% 90%
0110 - FT. HOOD 100% 100%
WRMC 97% 97%
0005 - FT. WAINWRIGHT 100% 100%
0008 - FT. HUACHUCA 0% 0%
0032 - FT. CARSON 92% 96%
0057 - FT. RILEY 100% 100%
0058 - FT. LEAVENWORTH 100% 100%
0075 - FT. LEONARD WOOD 100% 100%
0108 - FT. BLISS 96% 86%
0125 - FT. LEWIS 86% 98%
0131 - FT. IRWIN 100% 100%
Legend: N/A 95% - 100% 80% - 94% 0% - 79% or No Response

89
10. a) Number of AHLTA SADR encounters / number of total SADR encounters.
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 91% 92%
ERMC 96% 96%
0606 - HEIDELBERG 100% 100%
0607 - LANDSTUHL 92% 92%
0609 - VILSECK 100% 100%
NRMC 95% 94%
0037 - WASHINGTON DC 97% 97%
0061 - FT. KNOX 92% 86%
0069 - FT. MEADE 97% 97%
0086 - WEST POINT 94% 93%
0089 - FT. BRAGG 92% 93%
0121 - FT. EUSTIS 97% 98%
0122 - FT. LEE 100% 100%
0123 - FT. BELVOIR 98% 99%
0330 - FT. DRUM 92% 91%
PRMC 93% 93%
0052 - FT. SHAFTER 91% 91%
0610 - CAMP ZAMA 99% 100%
0612 - SEOUL 98% 99%
SRMC 88% 90%
0001 - REDSTONE ARSENAL 97% 99%
0003 - FT. RUCKER 98% 99%
0047 - FT. GORDON 83% 87%
0048 - FT. BENNING 99% 98%
0049 - FT. STEWART 91% 92%
0060 - FT. CAMPBELL 91% 94%
0064 - FT. POLK 100% 100%
0098 - FT. SILL 78% 89%
0105 - FT. JACKSON 85% 87%
0109 - FT. SAM HOUSTON 98% 98%
0110 - FT. HOOD 78% 79%
WRMC 90% 92%
0005 - FT. WAINWRIGHT 95% 97%
0008 - FT. HUACHUCA 97% 100%
0032 - FT. CARSON 99% 100%
0057 - FT. RILEY 74% 79%
0058 - FT. LEAVENWORTH 99% 100%
0075 - FT. LEONARD WOOD 99% 98%
0108 - FT. BLISS 81% 82%
0125 - FT. LEWIS 90% 91%
0131 - FT. IRWIN 97% 100%
Legend: N/A 95% - 100% 80% - 94% 0% - 79% or No Response

90
11) Use CHCS during the data month to identify potential duplicate patients and appointments. a) For CHCS/AHLTA hosts only, what was the number of potential duplicate records in the data month for all MTFs under the host?
Reporting Month Dec 2010 Jan 2011
Data Month Oct 2010 Nov 2010
Army 866 421
ERMC 31 32
0606 - HEIDELBERG
0607 - LANDSTUHL 31 32
0609 - VILSECK
NRMC 44 62
0037 - WASHINGTON DC
0061 - FT. KNOX 17 24
0069 - FT. MEADE
0086 - WEST POINT 2 13
0089 - FT. BRAGG 25 25
0121 - FT. EUSTIS
0122 - FT. LEE
0123 - FT. BELVOIR 0 0
0330 - FT. DRUM 0 0
PRMC 72 37
0052 - FT. SHAFTER 32 26
0610 - CAMP ZAMA
0612 - SEOUL 40 11
SRMC 380 182
0001 - REDSTONE ARSENAL 0 0
0003 - FT. RUCKER 122 121
0047 - FT. GORDON 14 11
0048 - FT. BENNING 15 8
0049 - FT. STEWART 5 15
0060 - FT. CAMPBELL 0 0
0064 - FT. POLK 162 0
0098 - FT. SILL 8 8
0105 - FT. JACKSON
0109 - FT. SAM HOUSTON
0110 - FT. HOOD 54 19
WRMC 339 108
0005 - FT. WAINWRIGHT 2 5
0008 - FT. HUACHUCA 10 3
0032 - FT. CARSON 18 21
0057 - FT. RILEY 58 2
0058 - FT. LEAVENWORTH 3 1
0075 - FT. LEONARD WOOD 30 33
0108 - FT. BLISS 197 22
0125 - FT. LEWIS 19 19
0131 - FT. IRWIN 2 2

91
Questions ??
??
?
?
?
?
?
?
?
?
?
?
?
?