Embed Size (px)
Citation preview

Michael K. W. Lichtenberg MD, FESC
Data on treatment of iliofemoral DVT with mechanical thrombectomy

Conflict of Interest - Disclosure
Within the past 12 months, I or my spouse/partner have had a financial
interest/arrangement or affiliation with the organization(s) listed below.
Affiliation/Financial Relationship Company
1. Honoraria for lectures: CR Bard, Boston Scientific AB Medica, Volcano,
Optimed GmbH, Straub Medical, Terumo, Biotronik, Veryan
2. Honoraria for advisory board activities: Veniti, Optimed GmbH, Straub
Medical, Biotronik, Veryan, Boston Scientific, Philips
3. Participation in clinical trials: Biotronik, CR Bard, Veryan, Straub Medical,
Veniti, Boston Scientific, LimFlow,Terumo, Philips, Optimed, IPmedical
4. Research funding: Biotronik, Boston Scientific, Veryan, Veniti, AB Medica,
Philips, CRBard, Optimed

• Frequent, but underestimated chronic
complication after iliofemoral DVT
• > 25% at risk for developing PTS following an
acute iliofemoral DVT (ATTRACT 28%)
• 5-10% severe PTS
White RH. The epidemiology of venous thromboembolism. Circulation 2003;107 (23 Suppl 1): I4-8.
Akesson H, Brudin L, Dahlstrom JA, Eklöf B, Ohlin P, Plate G. Venous function assessed during a 5 year period after acute ilio-femoral venous thrombosis treated with anticoagulation. Eur J Vasc Surg 1990;4(1):43-48.
Meissner M, Gloviczki P, Comerota A, Dalsing MC, Eklof BG, Gillespie DL et al. Early thrombus removal strategies for acute deep venous thrombosis: Clinical practice guidelines of the society for vascular surgery and the American venous forum. J Vasc Surg 2012; 55:1449-462.

22 y, female, acute onset of symptoms

Descending DVT in May – Thurner syndrome. Transpopliteal access, 10 F Aspirex®
8 F: blood volume aspiration up to 75 ml/min
10 F: blood volume aspiration up to 130 ml/min

EVIDENCE / GUIDELINES
Antithrombotic Therapy for VTE Disease Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of
Chest Physicians Evidence-Based Clinical Practice Guidelines Clive Kearon , MD , PhD ; Elie A. Akl , MD , MPH , PhD ; Anthony
J. Comerota , MD ; Paolo Prandoni , MD , PhD ; Henri Bounameaux , MD ; Samuel Z. Goldhaber , MD , FCCP ; Michael E. Nelson ,
MD , FCCP ; Philip S. Wells , MD ; Michael K. Gould , MD , FCCP ; Francesco Dentali , MD ; Mark Crowther, MD ; and Susan R.
Kahn , MD

ATTRACT trial
Outcome (24 mo)PCDT
(n=336)no PCDT(n=335)
P value
Any PTS 46,7 % 48,2% 0.56
Recurrent VTE 12,5% 8,5% 0.09
Generic QOL (SF-36 PCS) 11,8 10,1 0.37
VENOUS QOL (VEINES) 27,7 23,5 0.08
Moderate or Severe PTS 17,9% 23,7% 0.035
MS-PTS IFDVT 18,4% 28,2%
MS-PTS FPDVT 17,1% 18,1%
Major bleed 1,7% 0,3% 0.049
Any bleed 4,5% 1,7% 0.049
N Engl J Med. 2017 Dec 7;377(23):2240-2252

ATTRACT subgroup analysis

PCTD arm

CDT not sufficient

Patient outcomes (efficacy analysis)
Villalta 24 months: PCTD 3.95 vs 5.54 non-PCTD, p = 0.0033
VCSS 24 months: PCTD 1.98 vs 2.80 non-PCDT, p = 0.018
Veines 24 months: PCTD 28.63 vs 23.02 non-PCDT, p = 0.029

SAFETY REPORTING
Bleeding complication
PEARL Registry: 4.5% (minor/major)
Venous Registry: 11% major,16% minor
CAVENT (CDT arm): 22% (minor/major)

Thrombolysis vs PMT for iliofemoral DVT:A systemic review and metaanalysis
M. Lichtenberg, R. de Graaf, K. Kolosa, D. Golicki (Arnsberg, Warsaw)
• Database: MEDLINE• Keywords:
– deep vein thrombosis, deep venous thrombosis– iliofemoral– Additionaly in updating search 2: AngioJet, Penumbra, Aspirex
• Publication years:– search 1: 1946 – 4th December 2018– search 2: 1946 – 12th December 2018
• Inclusion criteria:– deep vein thrombosis (DVT)– iliofemoral arteries– Interventions:
• Catheter-directed thrombolysis (CDT), systemic thrombolysis, ultrasound-accelerated CDT
• Pharmacomechanical thrombectomy (PMT) with AngioJet, Penumbra Indigo or Aspirex device
1
3

Methods in studies
• Thrombolysis
– catheter-directed thrombolysis (CDT)
– ultrasound-accelerated CDT
– CDT + baloon
– systemic thrombolysis
• PMT
– AngioJet
– AngioJet/Trellis
– standard multi-sidehole catheter/AngioJet/Trellis
– AngioJet + direct stent
– AngioJet + CDT + staged stent
14

Included Literature for Metaanylsis1
5

Lysis grade II/III
CDT
PMT
n.s.

Recurrent DVT
CDT
PMT
n.s.

Overall PTS rate
n.s.
CDT
PMT

Moderate/Severe PTS

Reflux rate
PMT

Adjunctive angioplasty and stenting
CDT
PMT
n.s.

Safety: Major bleeding complications
Significantly
favours PMT

Pulmonary embolism

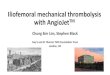
AngioVac Indigo Aspirex
Argon Penumbra Straub
no GW no GW 0,018 GW
Separator 0,025 GW
OTW
22F 3,4F, 5F, 6F, 8F 6F, 8F, 10F
75, 120 cm 85,115, 135, 150 cm 85, 95, 110 cm
Aspiration Aspiration Aspiration
Mechanical thrombectomy devices


Mechanical thrombectomy: Clearlumen (Walkvascular)

Conclusion
• Real advantage for PMT is safety (significant lower bleeding complications)
– Trend towards lower pulmonary embolism
• PMT and CDT are quite similar in efficacy
– Trend towards lower overall PTS and reflux with PMT
CDT must be stopped for
treatment of iliofemoral DVT

Michael K. W. Lichtenberg MD, FESC
Data on treatment of iliofemoral DVT with mechanical thrombectomy