Embed Size (px)
Citation preview
MYCOBACTERIAL DISEASES
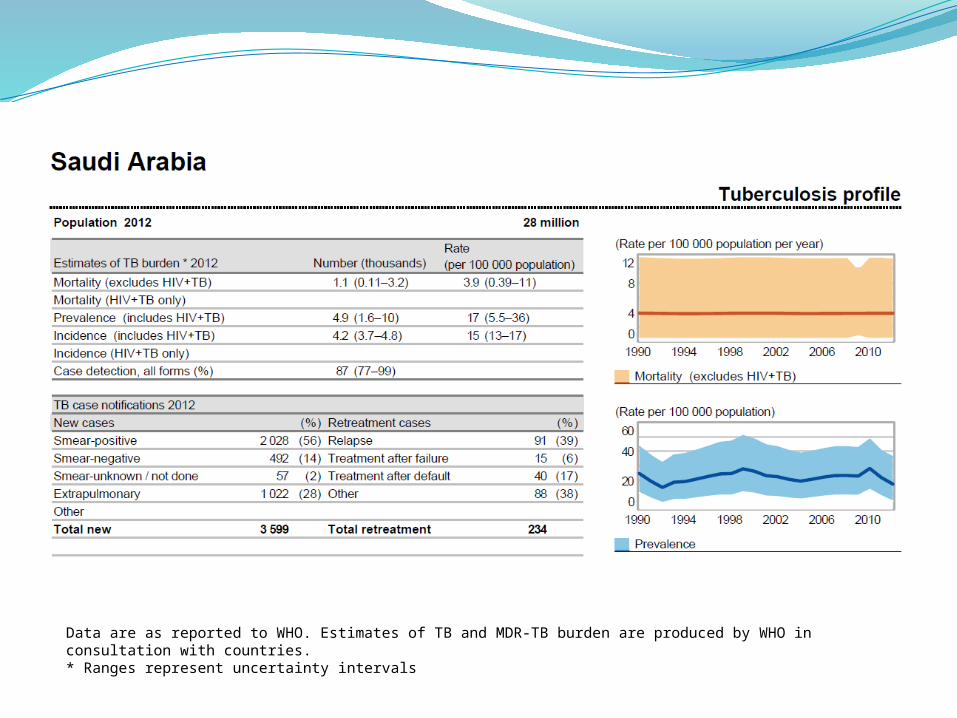
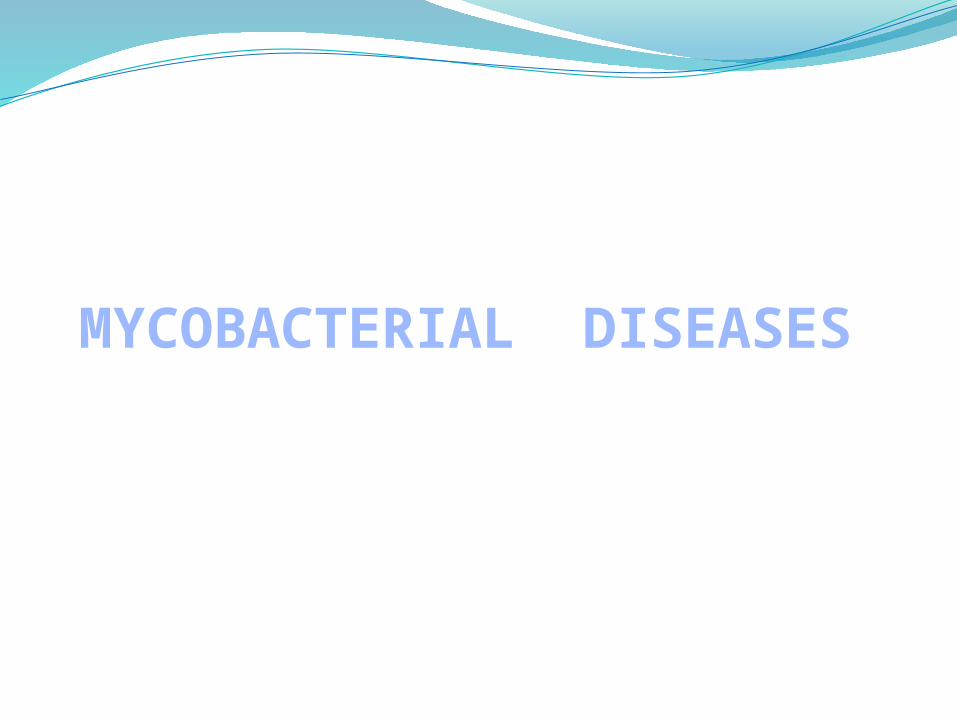
Data are as reported to WHO. Estimates of TB and MDR-TB burden are produced by WHO in consultation with countries.* Ranges represent uncertainty intervals
Mycobacterium tuberculosis
Obligate aerobe acid-fast rods
TUBERCULOSIS OVERVIEW, CAUSE, AND PATHOGENESIS
Tuberculosis, MTB, or TB (short for tubercle bacillus)
common, and in many cases lethal infectious disease
caused by various strains of mycobacteria
usually Mycobacterium tuberculosis
Mycobacterium tuberculosis, was identified and described on 24 March 1882 by Robert Koch
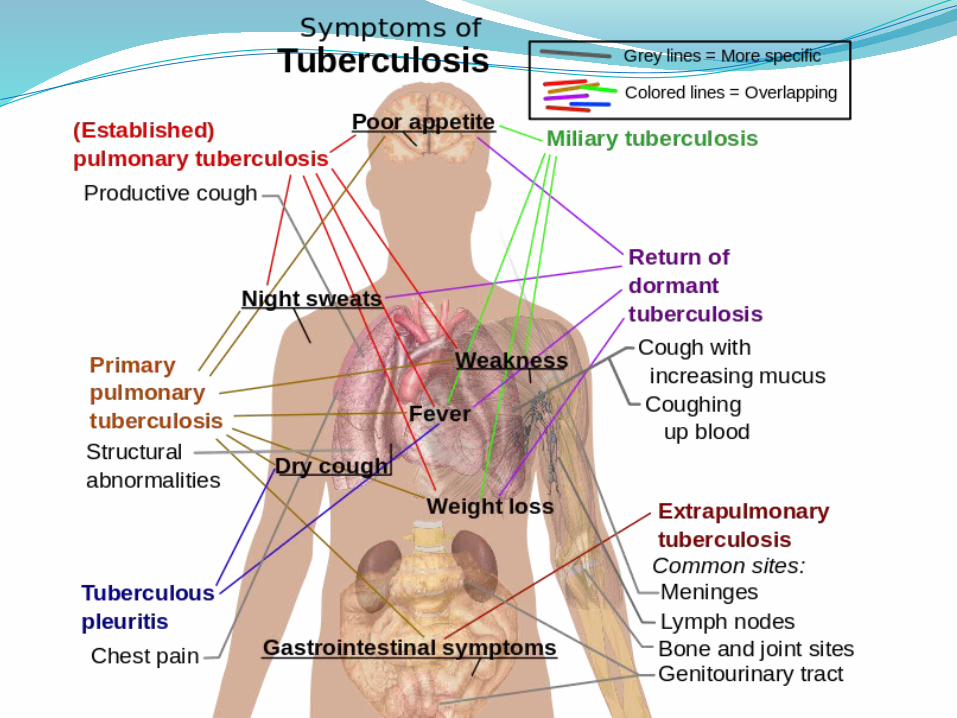
Tuberculosis may infect any part of the body
most commonly occurs in the lungs
pulmonary tuberculosis
Tuberculosis holds a special place in medical history
Can humble master clinicianschallenge public health authoritiestreatable and preventable
WHO (TB) data2 million deaths occur worldwide, each year Over 8 million cases, each year
In 2012, nearly 9 million people around the world became sick around 1.3 million TB-related deaths worldwide
≤ 33% of world’s population have silent latent infection
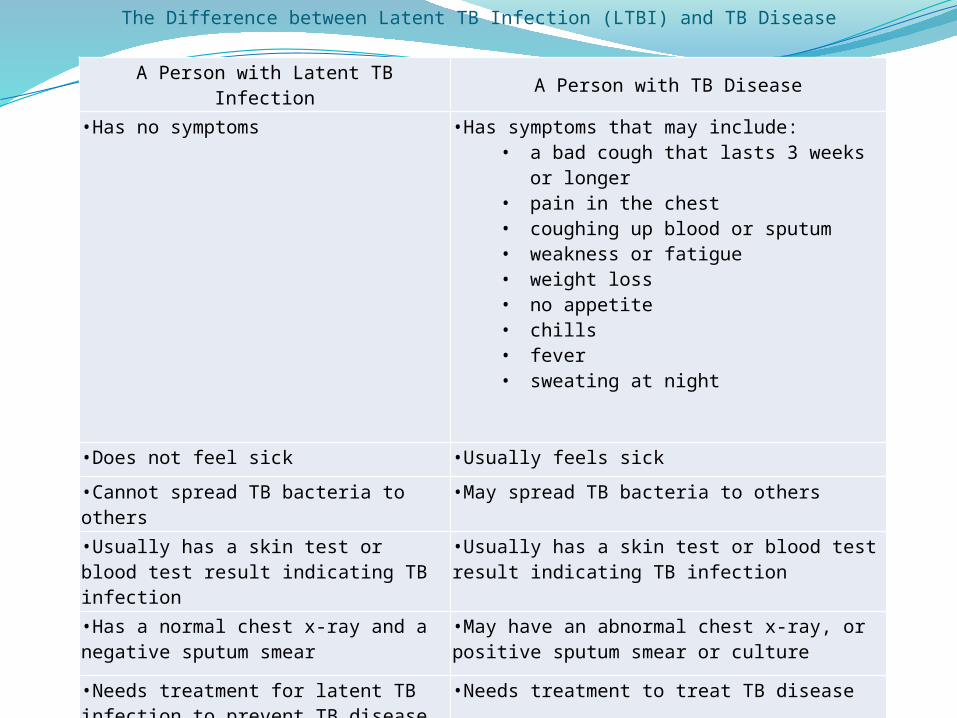
A Person with Latent TB Infection A Person with TB Disease
•Has no symptoms •Has symptoms that may include:• a bad cough that lasts 3 weeks or
longer• pain in the chest• coughing up blood or sputum• weakness or fatigue• weight loss• no appetite• chills• fever• sweating at night
•Does not feel sick •Usually feels sick
•Cannot spread TB bacteria to others •May spread TB bacteria to others
•Usually has a skin test or blood test result indicating TB infection
•Usually has a skin test or blood test result indicating TB infection
•Has a normal chest x-ray and a negative sputum smear
•May have an abnormal chest x-ray, or positive sputum smear or culture
•Needs treatment for latent TB infection to prevent TB disease
•Needs treatment to treat TB disease
The Difference between Latent TB Infection (LTBI) and TB Disease
Tuberculosis in the United States is now largely a disease of the disadvantaged
In 2006, there were 13,767 reported cases of TB in the United Statescases were reported in every statedrug-resistant casesco-infection with M. tuberculosis and HIVestimated 10 to 15 million persons remain latently
infected
A total of 9,945 TB cases were reported in the United States in 2012
Both the number of TB cases reported and the case rate decreased this represents a 5.4% and 6.1% decline, respectively,
compared to 2011
Mycobacterium tuberculosisslightly curved or straight rod-shaped bacillusrequires special acid-fast stains to be
visualized
It is closely related to M. bovisprimarily pathogen of cattle and related
animals
M. tuberculosis is also related to M. lepraeleprosy
Mycobacterium tuberculosis
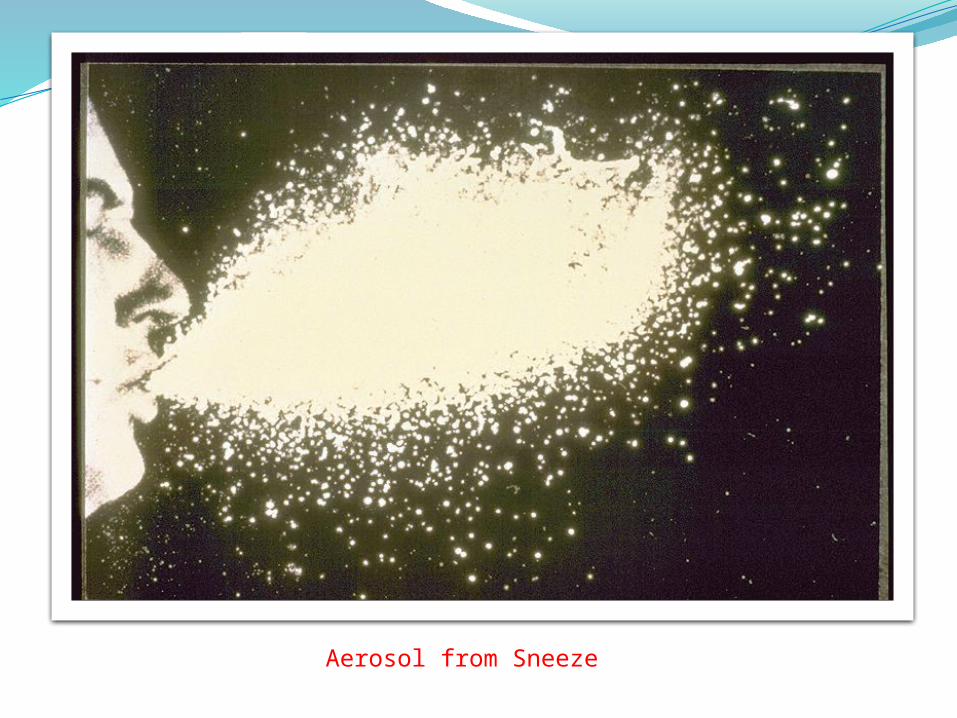
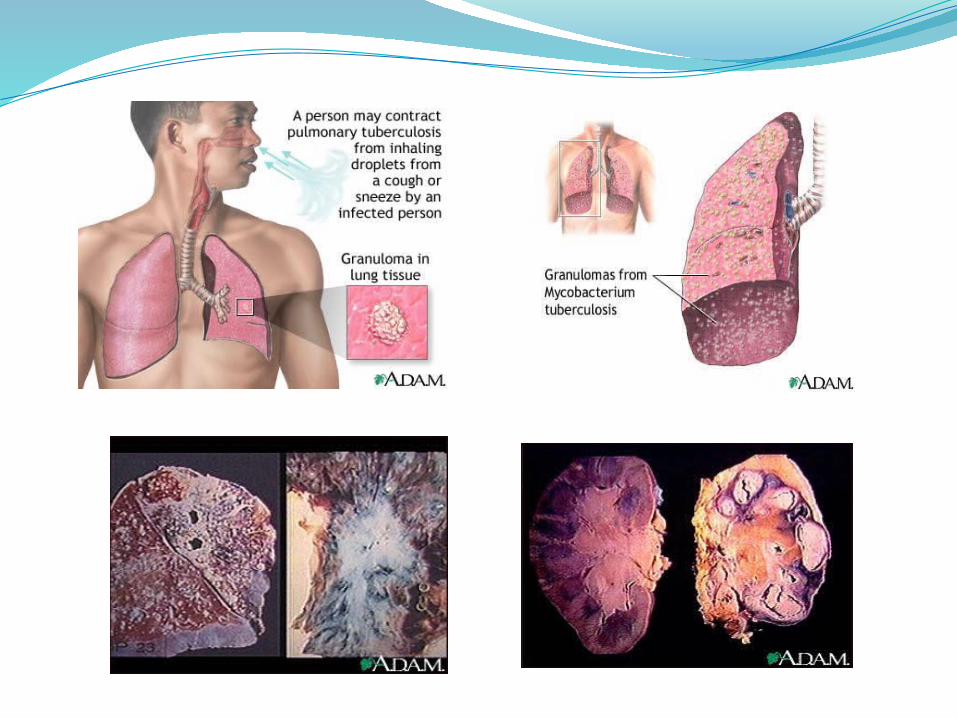
Tuberculosis is spread from person to personthrough the air by droplet nuclei1 to 5 m in diameter that have been expulsed into the air
Cough is the primary means by which tubercle bacilli are aerosolizedsinging, sneezing, or speaking may contribute to a lesser
extent
Droplet nucleismall enough to remain suspended in the air for long time
The probability of transmission depends on numerous factorssource caseexposed contactair space shared
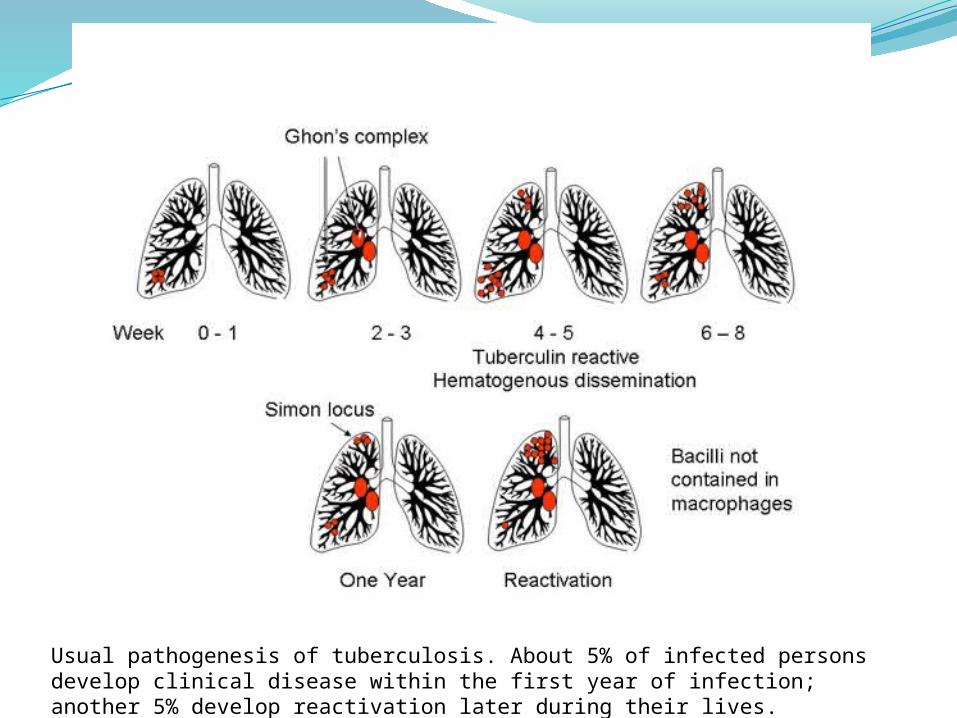
Usual pathogenesis of tuberculosis. About 5% of infected persons develop clinical disease within the first year of infection; another 5% develop reactivation later during their lives.
TB pathogenesis begins when a droplet containing viable tubercle bacilli is inhaled
Bacilli then spread through the pulmonary lymphaticsreach lymph nodesmay become enlarged
Efferent lymphatics then carry bacilli into the systemic circulation lungs, brain, kidneys, and bones
Tubercle bacilli replicate relatively slowlydividing time within 18 to 24 hours20 minutes for most common pathogens
Thus, the process of local, lymphatic, and eventual systemic spread described above typically requires several weeks
PULMONARY TUBERCULOSISWorldwide, tuberculosis remains the most common
cause of death
Pulmonary tuberculosis is the most common manifestation and the form of the disease usually responsible for its transmission
The usual patient with pulmonary tuberculosis presents with a history of several weeks of a progressive illness
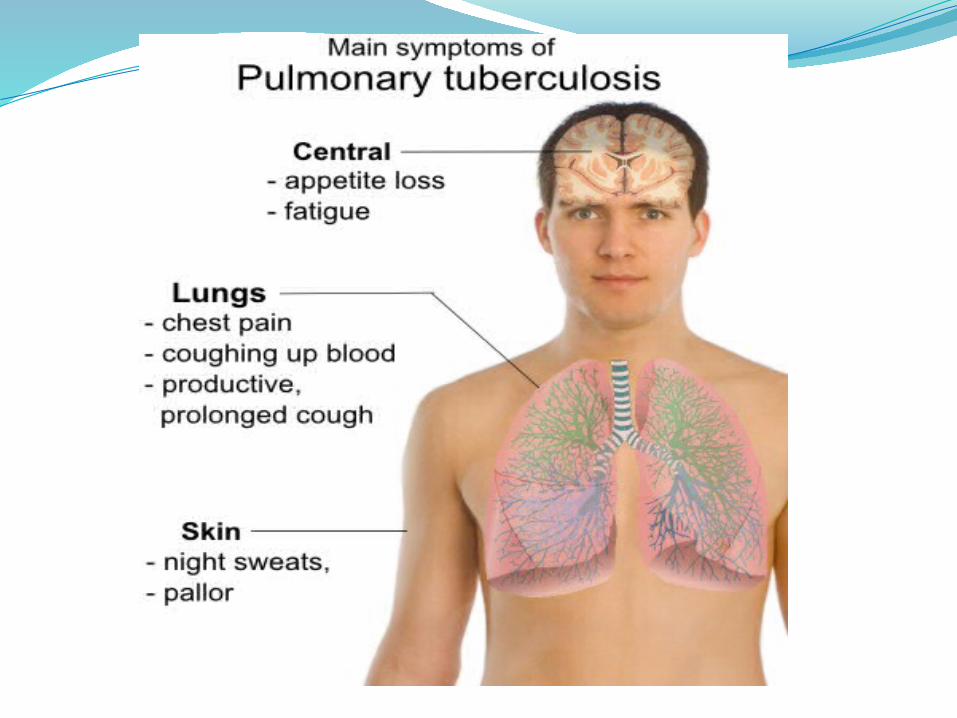
The most important pulmonary symptom is cough
Constitutional complaints coexist and may predominatefever, chills, night sweats, weight loss, appetite loss, and
easy fatigability
HIV and TB
HIV has greatly increasing the risk of TB
Diagnosis of TB in patients with HIV can be difficult
Suspicion of TB is an indication for HIV antibody testing
Laboratory diagnosis1- Mantoux skin test (Tuberculin)
2- Chest X-ray
3- Isolation of Mycobacterium speciesLöwenstein–Jensen medium (L.J. medium)microscopic positive results for acid-fast bacilli
4- Identification of microbial genetic materialmolecular methods such as PCR
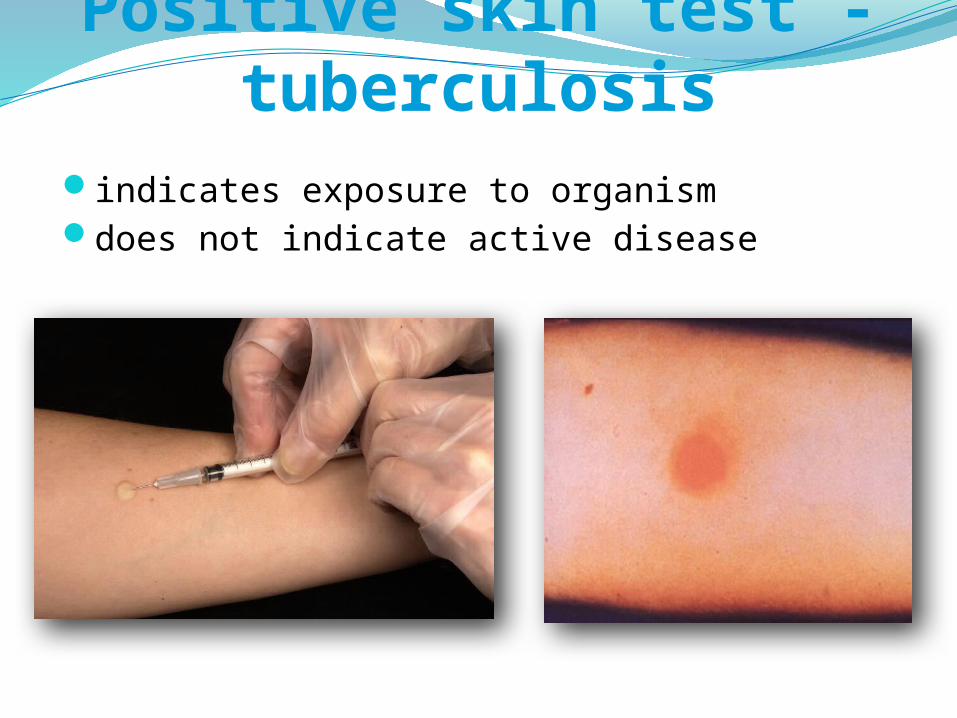
Positive skin test - tuberculosisindicates exposure to organismdoes not indicate active disease

The Mantoux skin test consists of an intradermal injection of one-tenth of a milliliter (ml) of PPD tuberculin.
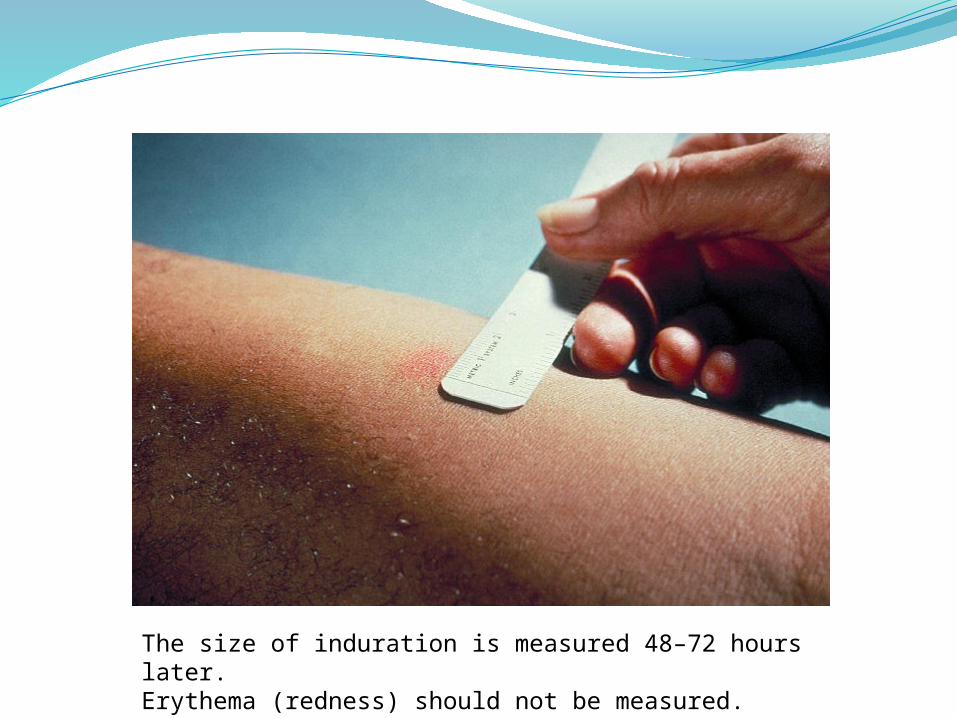
The size of induration is measured 48–72 hours later.Erythema (redness) should not be measured.
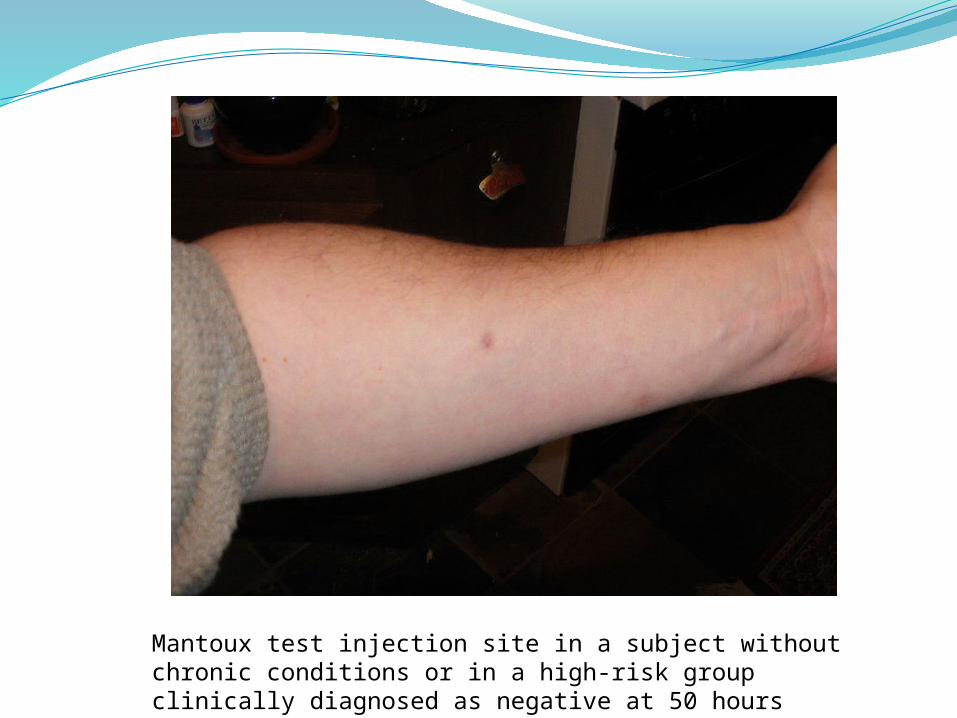
Mantoux test injection site in a subject without chronic conditions or in a high-risk group clinically diagnosed as negative at 50 hours
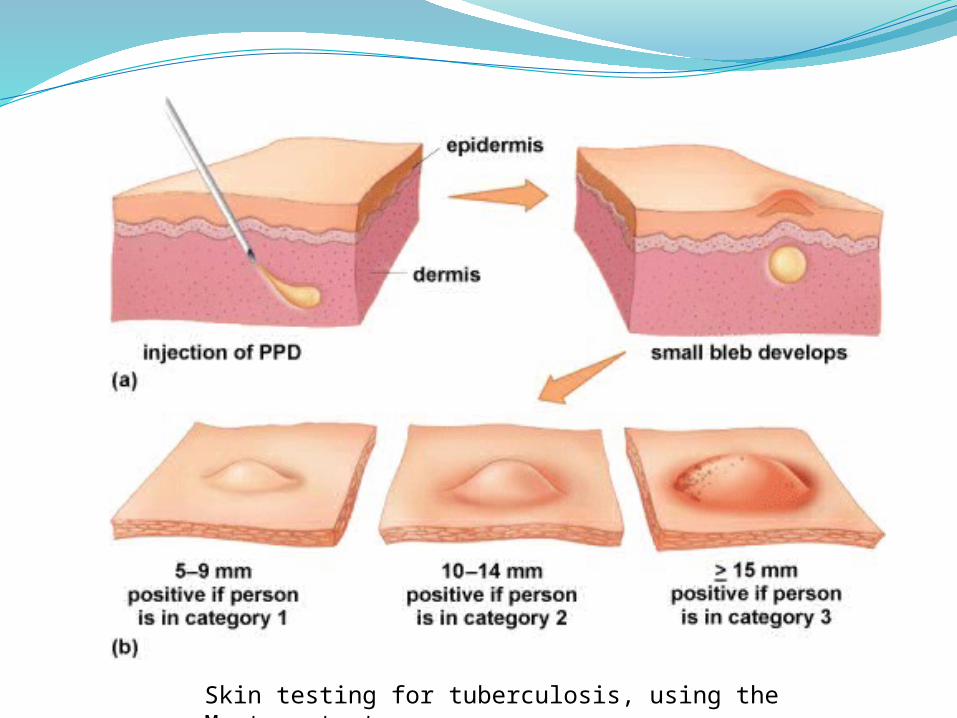
Skin testing for tuberculosis, using the Mantoux test.
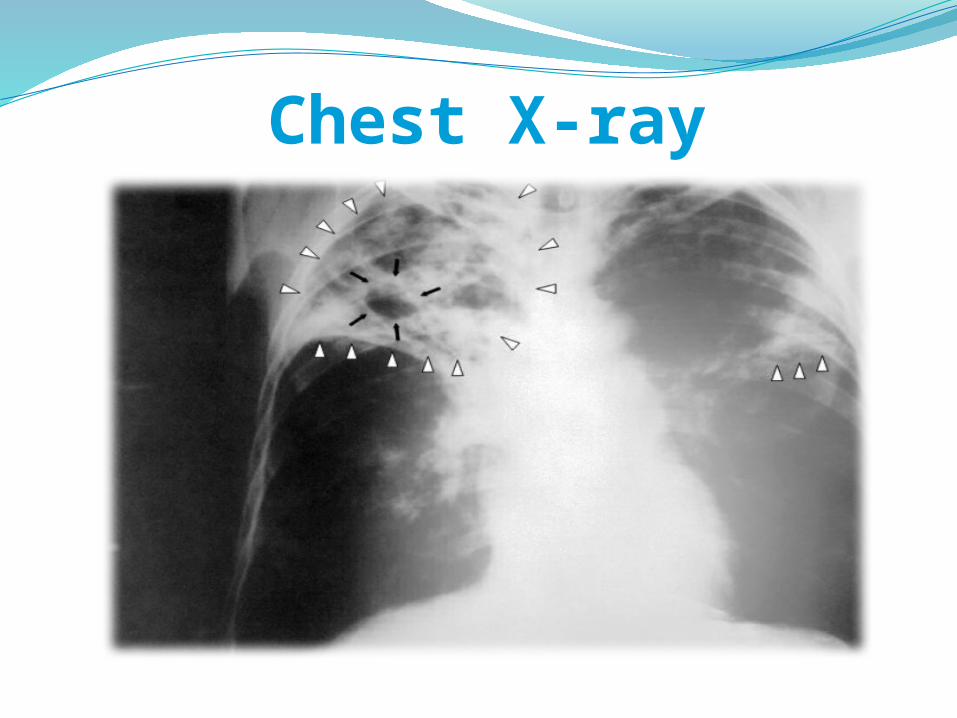
Chest X-ray
Microscopic Examination of Mycobacterium
The Mycobacteria are aerobic acid fast, non-motile, non-spore forming rods
M. tuberculosis is a non capsulated straight or slightly curved rod, measuring 1-4µm x 0.2-0.6 µm
The most common pathogens that cause disease to man areM. tuberculosis, M. bovis, M. africanum, and M.microti
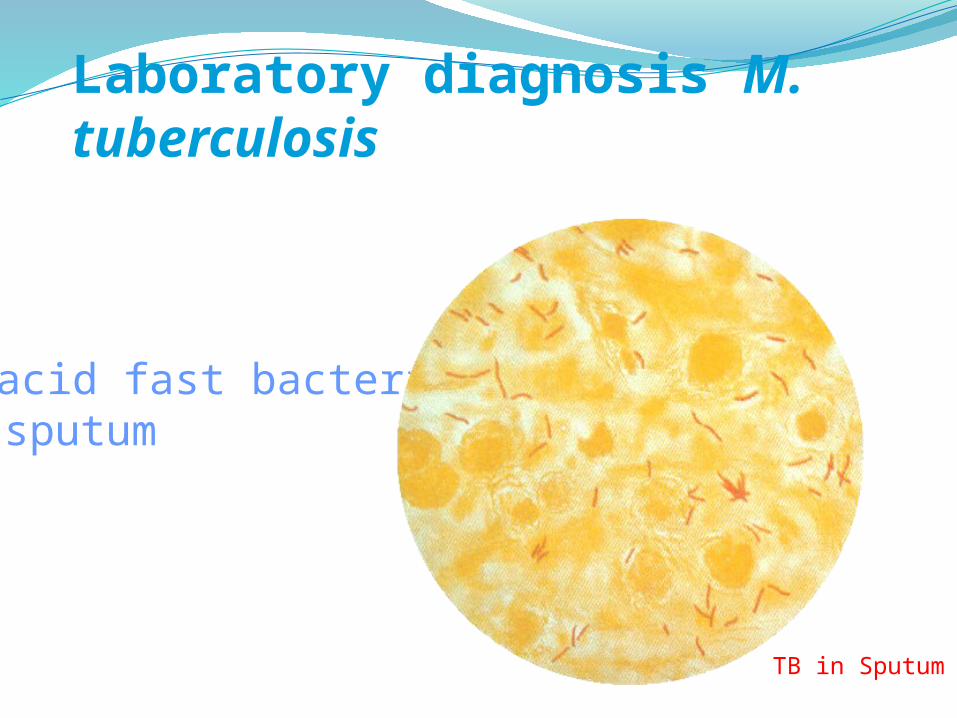
Laboratory diagnosis M. tuberculosis
• acid fast bacteria – sputum
TB in Sputum
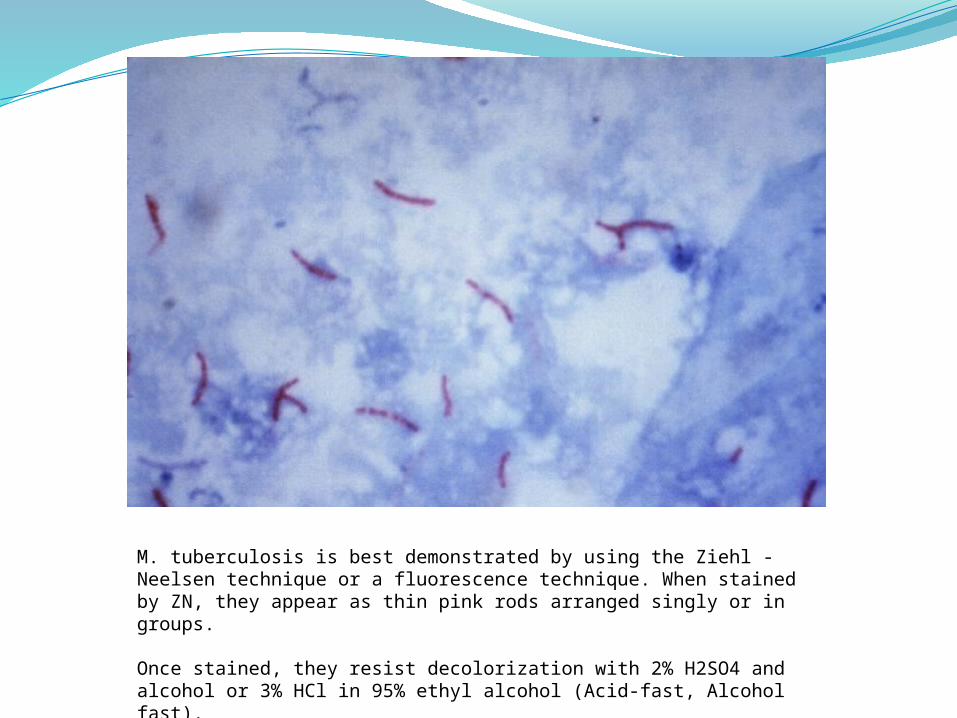
M. tuberculosis is best demonstrated by using the Ziehl -Neelsen technique or a fluorescence technique. When stained by ZN, they appear as thin pink rods arranged singly or in groups.
Once stained, they resist decolorization with 2% H2SO4 and alcohol or 3% HCl in 95% ethyl alcohol (Acid-fast, Alcohol fast).
Cultural Characteristics and colony morphology
M. tuberculosis is strict aerobicgrows very slowly (2-4 weeks)egg enriched medium
Lowenstein-Jensen medium giving dry creamy colored colonies
Other selective media as Middlebrook 7H10, 7H11 agar and 7H9 brothused for primary isolationantibiotic susceptibility testing
M. tuberculosis is a non chromogendoes not grow on media contain p-nitrobenzoic acidthese characteristics help to differentiate them from
M. avium, M. intracellulare, and M. kansasii
The optimum temperature for growth is at 37C
The culture must be incubated up to 12 weeks
M. tuberculosis produces rough, and tough colonies on glycerol and pyruvate egg media
They are niacin producers and grow under aerobic conditions at 37 C
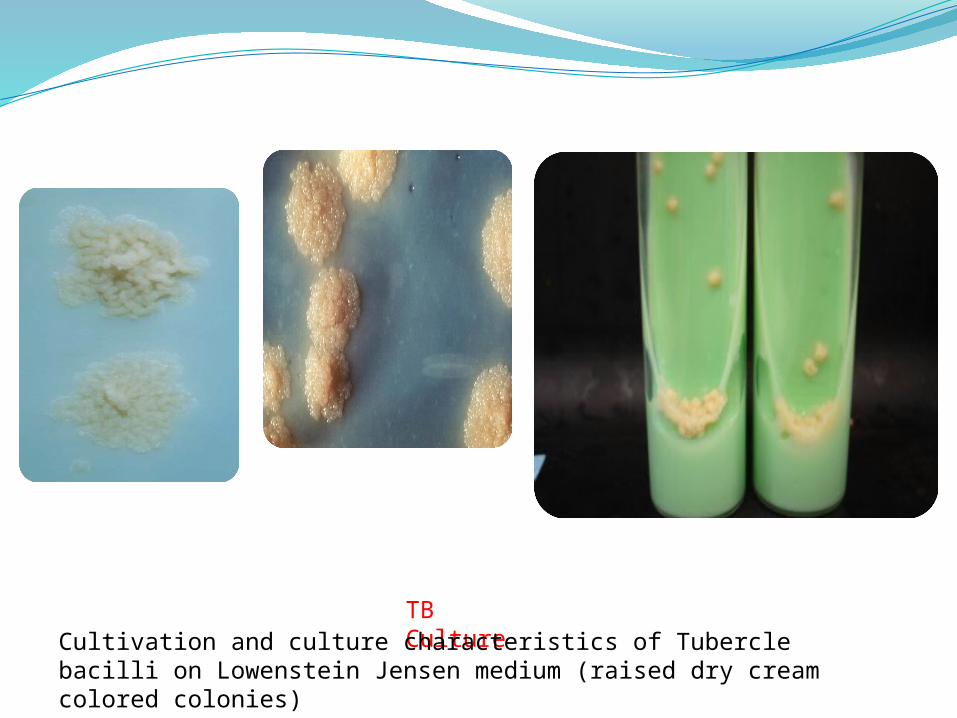
TB CultureCultivation and culture characteristics of Tubercle bacilli on
Lowenstein Jensen medium (raised dry cream colored colonies)
Tuberculosispolymerase chain amplificationrapid diagnosis
Antibotic treatment - tuberculosisextensive time periods (e.g. 9 months)organism grows slowly, or dormanttwo or more antibiotics
e.g. rifampin and isoniazidresistance minimized
Tuberculosis and Drug resistance
Multiple drug resistant (MDR)Resistant to first line drugs
Extremely drug resistant (XDR) Resistant to some of the second line drugs
Nearly un-treatable
Transmission - tuberculosisM. tuberculosis is carried in airborne particles,
called droplet nuclei, of 1– 5 microns in diameter
Depending on the environment, these tiny particles can remain suspended in the air for several hours
M. tuberculosis is transmitted through the air, not by surface contact
Transmission occurs when a person inhales droplet nuclei containing M. tuberculosistraverse the mouth or nasal passages, upper
respiratory tract, and bronchireach the alveoli of the lungs
Vaccination• BCG vaccine – an attenuated strain of M. bovis – not effective
• in US, – incidence is low– vaccination not practiced– immunization interferes with diagnosis
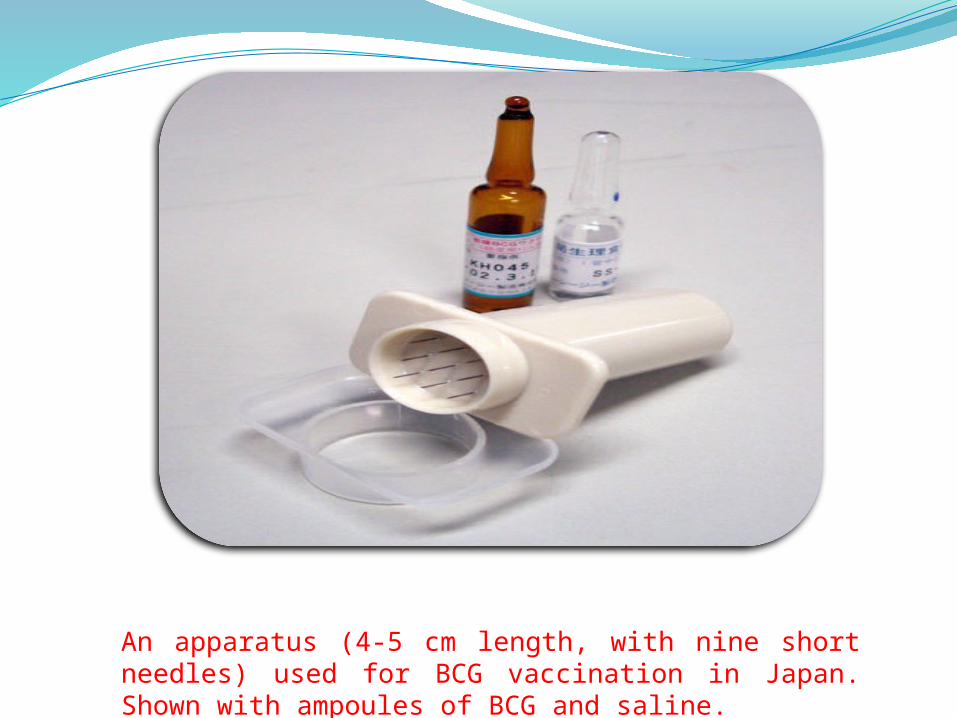
An apparatus (4-5 cm length, with nine short needles) used for BCG vaccination in Japan. Shown with ampoules of BCG and saline.
M. avium - M. intracellulare complex (M. avium)
• non-AIDS– infection almost never
• AIDS – major bacterial opportunist
• multiple drug-resistance
• spread from cattle
• infected cattle are culled– positive skin test
• rarely seen in US
M. bovis

M. lepraeleprosymajor disease of third worldrare in US
A 24-year-old man from Norway, infected with leprosy, 1886.
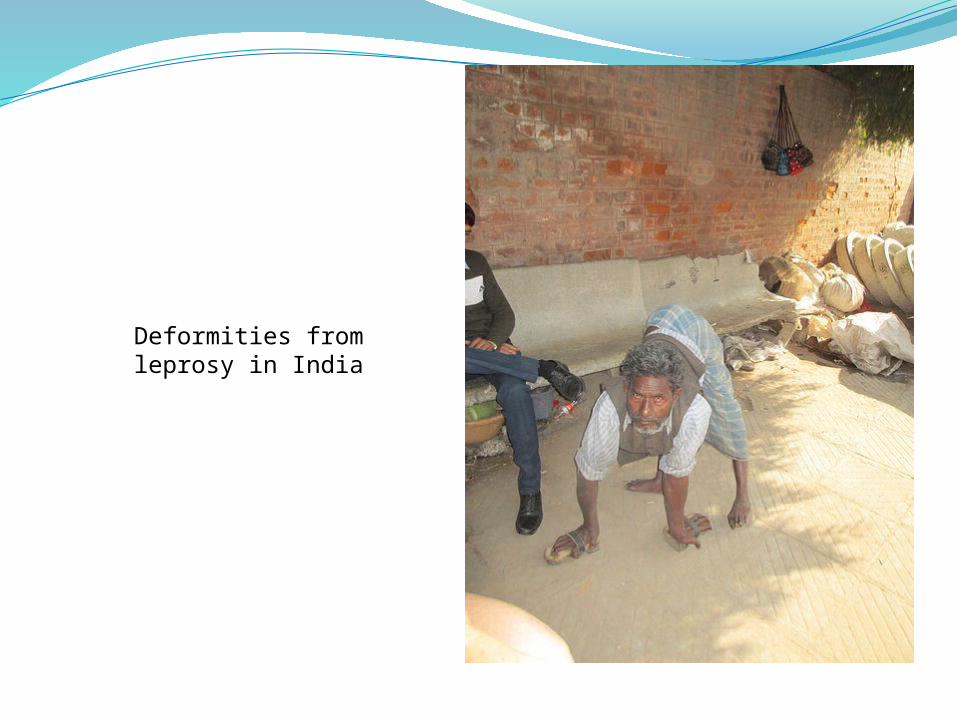
Deformities from leprosy in India