Embed Size (px)
Citation preview

Dartmouth Biomedical LibrariesLibrary Grand Rounds
Palliative and End-of-Life Care Information Resources
A Case-Based Presentation
December 16, 2004

Ira Byock, M.D.Director, Palliative Care Program
Dartmouth-Hitchcock Medical Center
Cindy Stewart, M.L.S.Associate Director/Health Sciences Library
Dartmouth Biomedical Libraries
Objectives
Introducing participants to readily available web-based information resources for “just-in-time” education and practical management of palliative care issues.
Familiarizing participants with the Palliative Care Program at DHMC.
Providing selected clinical pearls related to therapeutic use of communication in palliative aspects of care.

Palliative Care -- definition
Interdisciplinary care for persons with life-threatening illness or injury which addresses physical, emotional, social and spiritual needs and seeks to improve quality of life for the ill person and his or her family.
SocialWorkerSocialWorker
PalliativeMedicinespecialist
PalliativeMedicinespecialist
HospicePhysician
& RNs
HospicePhysician
& RNs
HospitalNursing
HospitalNursingPT/OT/RT
TherapistsPT/OT/RTTherapists
ClinicalPharmacist
ClinicalPharmacist
PCPPCP
DieticianDietician
VolunteerCoordinatorVolunteer
Coordinator
PastoralCare
PastoralCare
HospitalCRC-Discharge
Planner
HospitalCRC-Discharge
Planner
Patient & Family

Palliative Care
Hospice Care
Hospice and Palliative Care
Byock I. Hospice and Palliative Care: A Parting of Ways or a Path to the Future?
Journal of Palliative Medicine. 1998;1(2):165-176.

An interdisciplinary team 24/7 availability Ongoing communication Advanced care planning Formal symptom assessment & treatment Crisis prevention & early crisis management Care coordination Spiritual care Anticipatory guidance Bereavement support
Typical Services of Hospice & Palliative Care

PhysiciansIra Byock, M.D.Frances Brokaw, M.D.Diane Palac, M.D.Thomas Prendergast, M.D.
Nurse PractitionersLisa Szczepaniak, MSN, ARNPMarie Bakitas, MSN, ARNPPeggy Bishop, MS, ARNP
Network and Program DevelopmentYvonne Corbeil
Administrative AssistantGeri Barden 650-5402
Palliative Care at DHMC

Goals of care clarification Pain & Symptom assessment & treatment Family support Counseling & Anticipatory Guidance
Adaptation to illness & prognosis Issues of life completion & closure Discharge planning Planning for home care Transition to home hospice
Palliative Care in the Hospital

Access To Tools Where to go for definitions and basic information
Glossaries Web-based resources – quick information
re palliative treatments and clinical tips Textbooks Journals

www.stoppain.org
www.growthhouse.org

www.nhpco.org

www.PromotingExcellence.org

www.PromotingExcellence.org

www.PromotingExcellence.org

www.PromotingExcellence.org

www.PromotingExcellence.org

www.PromotingExcellence.org

Up To Date www.utdol.com

Up To Date www.utdol.com

MDConsult

MDConsult

www.growthhouse.org

Print resources from Dartmouth Libraries

Print resources from Dartmouth Libraries

Print resources from Dartmouth Libraries

eJournals

eJournals

eJournals

The case…
Mrs. Smith is a 72 year old Caucasian woman from upstate New York with who is admitted to DHMC with acute dyspnea, altered mental status and low grade fever.

Mrs. Smith – Medical History
She has been treated for Stage IIA (T1N1M0) adenocarcinoma of the right upper lung diagnosed in March 2003.
She completed neo-adjuvant chemotherapy and radiation therapy followed by lobectomy in April 2003.
Post-op course was complicated by R lower extremity deep vein thrombosis. A Greenfield filter was placed.

Mrs. Smith – Social History
Mrs. Smith and her 79 yo husband moved from Rochester, NY 2 years ago to a small home in Milford, NH to be closer to family. Her husband has mild memory loss and confusion and requires her assistance to maintain daily activities.
Their daughter, Ann, who is the durable power of attorney for health care (DPOAHC) for both her parents, lives in Nashua. She apparently was the person who called the ambulance this morning.
The couple’s son lives in Boston. He is an attorney with the an oil company and often travels overseas.

Mrs. Smith – case unfolds
Ann Smith arrives at the hospital 3 hours after the patient is admitted, saying that her mother hadn’t answered the phone that morning and she had arrived at their home and found her mother in bed, confused. She had been incontinent and had no memory of last night.

Mrs. Smith – case unfolds
Her father was sitting at the kitchen table, looking bewildered. He had been trying to make breakfast for Mrs. Smith and himself. The refrigerator door was open and various containers scattered around the counters and kitchen table.
Ann hastily arranged for a neighbor to stay with her father for the day before driving to DHMC.

CBC, electrolytes, calcium, BUN are all wnl CXR shows a LUL infiltrate and signs of
previous RUL surgery. Cranial MRI reveals a large frontal and
smaller parietal cerebral metastases.
imagesMD
Mrs. Smith – case unfolds

NSCLC Cerebral metastasis Possible seizure Probable aspiration pneumonia
Mrs. Smith – Diagnoses

Patient’s daughter, Ann, asks your advice. She just spoke with her brother who is in London on business. He is emotionally struggling with their mother’s illness and is not acknowledging the seriousness of her condition.
He is flying home and will be coming to the hospital within 36 hours.
She asks you to meet with her and her brother to discuss her mother’s prognosis and to assist her and her brother in making decisions that are in their parents’ best interests.
Mrs. Smith – case unfolds

Management Resources
Clinical Guidelines Hospice organizations Communication resources

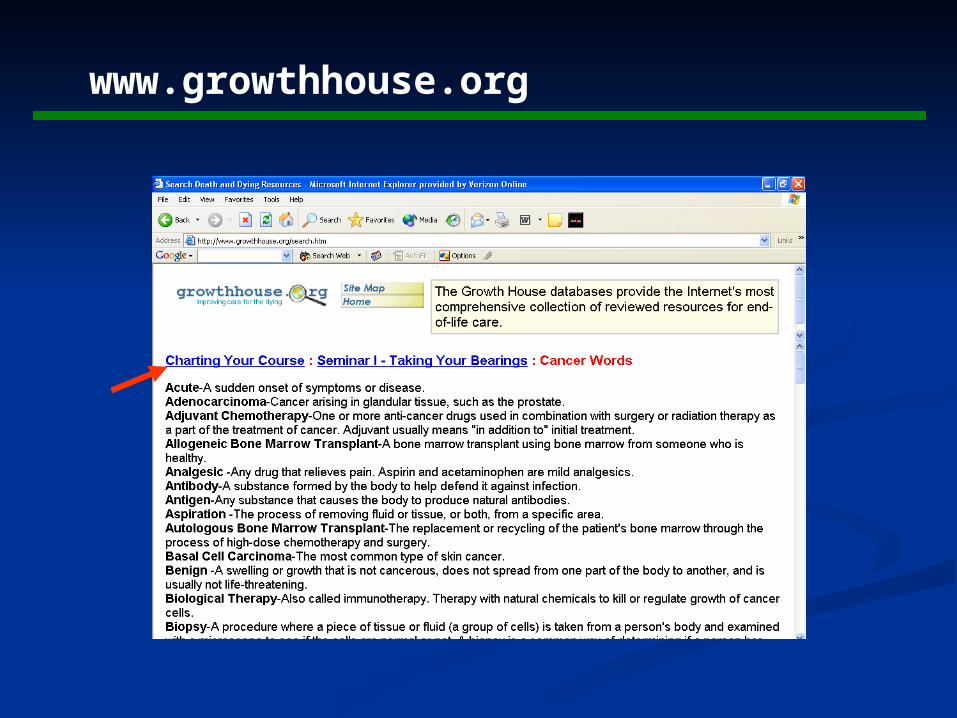
EPERC: End of Life & Palliative Education Resource Center
EPERC: End of Life & Palliative Education Resource Center

EPERC: End of Life & Palliative Education Resource Center

National Guidelines Clearinghouse

National Guidelines Clearinghouse
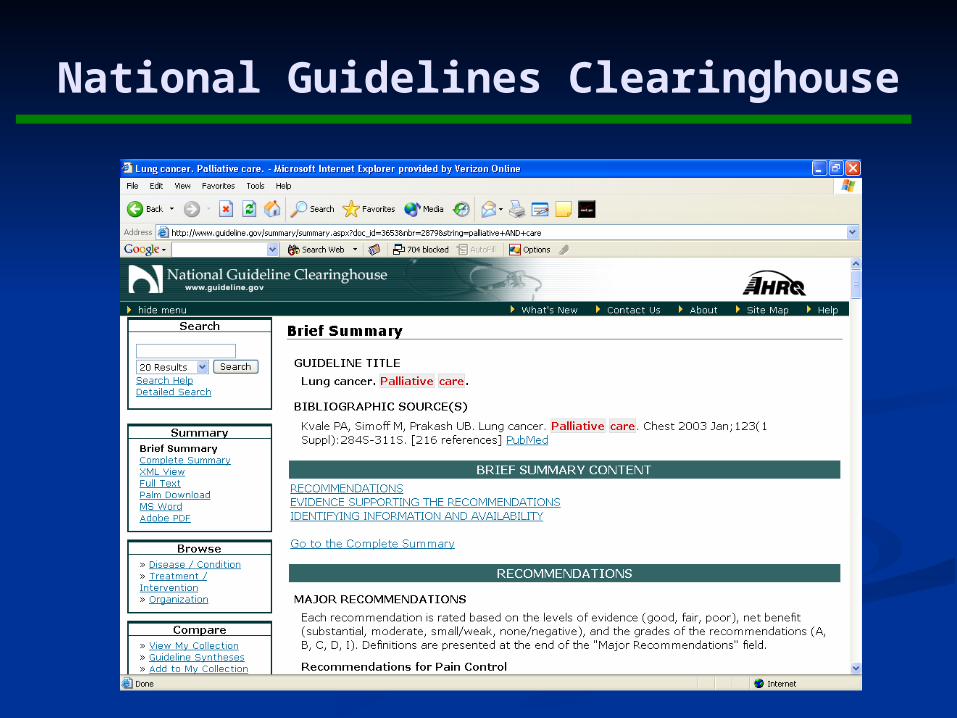
National Guidelines Clearinghouse

Decision-making and Communication

Decision-making and Communication

Pitfalls in care planning for patients w/o decision-making capacity
Failure to reach shared appreciation of pt’s condition and prognosis
Failure to apply substituted judgment Offering choice between care and no care, rather
than between prolonging life and quality of life Too literal interpretation of an isolated, out-of-
context, earlier statement Failure to address the full range of decisions &
options
Lang F, Quill T. Making decisions with families at the end of life.
Am Fam Physician. 2004. 70(4):719-723.

eJournals
Decision-making and Communication

eJournals
Prendergast TJ, Puntillo KA. Withdrawal of life support: intensive caring at the end of life.
JAMA Dec 4 2002;288(21):2732-2740.
Decision-making and Communication

eJournals
Prendergast TJ, Puntillo KA. Withdrawal of life support: intensive caring at the end of life.
JAMA Dec 4 2002;288(21):2732-2740.
Decision-making and Communication

eJournals
Prendergast TJ, Puntillo KA. Withdrawal of life support: intensive caring at the end of life.
JAMA Dec 4 2002;288(21):2732-2740.
Decision-making and Communication

The next day Mrs. Smith is more alert, but slightly confused. She complains only of a moderate headache.
Two days after admission, Mrs. Smith is fully oriented with intact cognitive and motor function.
In discussion with her medical oncologist and the in-patient attending, she declines whole brain radiation, and chemotherapy.
When CPR is discussed, she firmly requests that a DNR order be written.
Mrs. Smith – case unfolds

Mrs. Smith’s daughter is willing to take her parents to her and her husband’s home in Nashua. She asks about hospices in the area.
She is also worried about controlling pain in their home.
She asks what she should do if a seizure occurs.
Mrs. Smith – Discharge planning issues

Locating a hospice program

Locating a hospice program

Locating a hospice program

Home Health & Hospice Care (Nashua)
Locating a hospice program

Locating a hospice program
Home Health & Hospice Care (Nashua)
Advance directives – Are the couple’s NY advance documents valid?
If she didn’t have a DPOAHC, where could we find one?
Advance Directives

Advance Directives

Advance Directives

Advance Directives
www.Partnershipforcaring.org OR www.growthhouse.org

Advance Directives
www.Partnershipforcaring.org OR www.growthhouse.org

Home care for Seizures
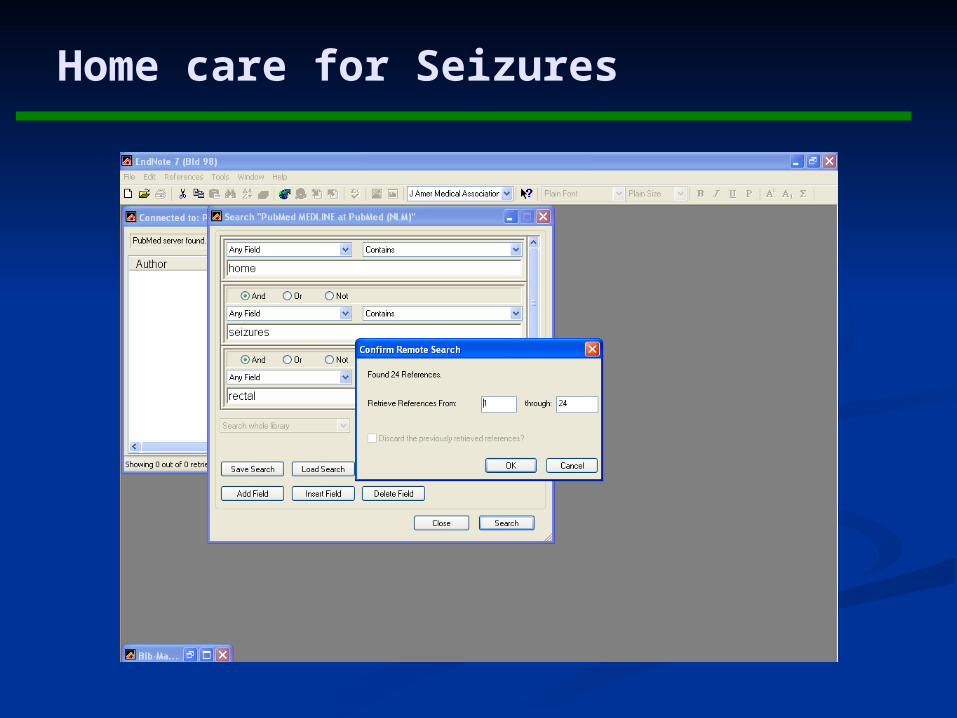
Home care for Seizures

Home care for Seizures

Home care for Seizures

Home care for Seizures

Home care for Pain

Home care for Pain

Home care for Pain

Home care for Pain

Resources for Communication & Counseling

7-steps for structuring communication regarding care at the end of life
Prepare by confirming facts & establishing environment Establish what the patient (and family) knows Determine how information is to be handled Deliver information in sensitive, straightforward manner Respond to emotions of patients, parents, & families Establish goals for care and treatment priorities Establish an overall plan
von Gunten CF, Ferris FD, Emanuel LL Ensuring competency in end-of-life care: communication & relational skills.
JAMA 2000;284(23):3051-3057.
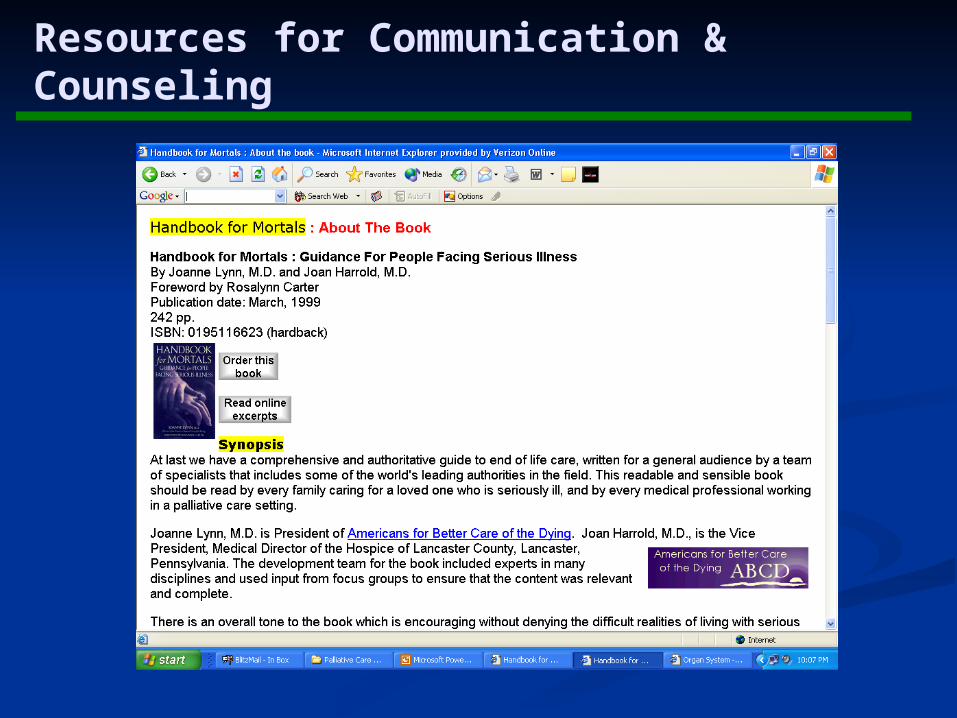
Resources for Communication & Counseling

Patient information: MedlinePlusMedlinePlus Handbook for MortalsHandbook for Mortals ENABLE – ENABLE – Charting Your CourseCharting Your Course Completing a LifeCompleting a Life Dyingwell.orgDyingwell.org
Resources for Communication & Counseling

Resources for Communication & Counseling
Resources for Communication & Counseling

Dartmouth
Project ENABLE – Charting Your Course
Resources for Communication & Counseling

Resources for Communication & Counseling

Resources for Communication & Counseling

Resources for Communication & Counseling
http://commtechlab.msu.edu/sites/completingalife/
Resources for Communication & Counseling
http://commtechlab.msu.edu/sites/completingalife/

Resources for Communication & Counseling
www.dyingwell.org

Resources for Communication & Counseling
www.dyingwell.org

Two months after discharge, you receive a call
from the Nashua hospice program saying that Mrs. Smith died comfortably at her daughter’s home with her extended family present.
Two weeks later Ann Smith sends a card expressing her and her family’s appreciation for the care you gave her mother and the support of their family.
Mrs. Smith – Case Concludes